Embed Size (px)
Citation preview

JMed Genet 1997;34:917-923
Syndrome of the month
Prader-Willi syndrome
Suzanne B Cassidy
AbstractPrader-Willi syndrome is a complex dis-order affecting multiple systems withmany manifestations relating to hypotha-lamic insufficiency. Major findings in-clude infantile hypotonia, developmentaldelay and mental retardation, behaviourdisorder, characteristic facial appear-ance, obesity, hypogonadism, and shortstature. Obesity and the behaviouralproblems are the major causes ofmorbid-ity and mortality.Prader-Willi syndrome is caused by
abnormalities of the imprinted region ofproximal 15q and results from absence ofthe normally active paternal genes in thisregion. Such absence results from pater-nal interstitial deletion, maternal unipa-rental disomy, or a mutation or otherabnormality in the imprinting process.Diagnostic identification of all causes
has become available in recent years, per-mitting early detection and institution ofappropriate management. This testinghas permitted recent identification ofsome phenotypic differences among af-fected subjects of different race andbetween those with deletions and unipa-rental disomy as a cause.(3Med Genet 1997;34:917-923)
Keywords: Prader-Willi syndrome; imprinting; proxi-mal 15q; uniparental disomy
Department ofGenetics and Centerfor Human Genetics,Case Western ReserveUniversity andUniversity Hospitals ofCleveland, 11100Euclid Avenue,Lakeside 1500,Cleveland, OH 44106,USAS B Cassidy
Prader-Willi syndrome (PWS) is a complex,multisystem disorder first described in 1956.'Twenty-five years later it captured the interestof geneticists because it was the first recognisedmicrodeletion syndrome identified by highresolution chromosome analysis.2 PWS is nowknown to be one of the most commonmicrodeletion syndromes, one of the most fre-quent disorders seen in genetics clinics, and themost common recognised genetic form ofobesity. It is also the first recognised humangenomic imprinting disorder and the firstrecognised as resulting from uniparentaldisomy.' PWS thus occupies an importantplace in the contemporary history of humangenetic disorders. It is, in addition,distinguished by being a syndrome caused byseveral different genetic alterations of proximal
1 5q (genetic heterogeneity) and it is typified bya distinctive behavioural phenotype."7Approximately 1 in 10 000-15 000 subjects
is diagnosed with PWS8 and it occurs in bothsexes and all races. Unfortunately, diagnosis isstill delayed in many cases despite the availabil-ity of clinical diagnostic criteria.' Appropriatemanagement can have a significant positiveimpact on health and quality of life, butcontrolling the characteristic obesity and diffi-cult behaviour constitutes a major challenge,requiring cooperative input from geneticists,primary care physicians, endocrinologists, nu-tritionists, psychologists, psychiatrists, andteachers, as well as families and other caregivers.
Clinical findings and natural historyAlthough many of the manifestations of PWSare related to functional hypothalamic defi-ciency, the clinical appearance in infancydiffers considerably from that in childhood andadulthood.4"
HYPOTONIAHypotonia ofprenatal onset is nearly uniformlypresent and is probably the cause of decreasedfetal movement, frequent abnormal fetal posi-tion, and difficulty at the time of delivery oftennecessitating caesarean section.4 The neonatalcentral hypotonia is almost invariably associ-ated with poor sucking, with consequent failureto thrive and the necessity for nasogastric orother special feeding techniques. Infantile leth-argy, with decreased arousal and weak cry, arealso prominent findings, leading to the neces-sity to awaken the child to feed. A gastrostomytube is rarely necessary since this problem istransient. Reflexes may be decreased or absent.Neuromuscular electrophysiological and bi-opsy studies are normal or non-specific and thehypotonia gradually improves. Motor mile-stones are delayed and average age of sitting is12 months and walking is 24 months. Adultsremain mildly hypotonic with decreased mus-cle bulk and tone.
HYPOGONADISMHypogonadism is prenatal in onset' and is evi-dent at birth as genital hypoplasia, It ismanifested by cryptorchidism, scrotal hypopla-sia (small, hypopigmented, and poorly rug-ated), and sometimes a small penis in males,
917 on N
ovember 9, 2020 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.34.11.917 on 1 Novem
ber 1997. Dow
nloaded from

918
.--
*.... ......
0
*. ~':3
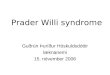
Figure 1 Evolution of the phenotype ofPWS in a patient with a lSq deletion: (A) 11 months, (B) 2½12years, (C) 3¼12years, (D) 7years, (E) 13years,(F) 27years. See text for description ofphenotypicfindings. (All photographs reproduced with permission.)
and by hypoplasia of the labia minora andclitoris in females. These findings persistthroughout life, though spontaneous descent oftestes has been observed up to adolescence.Hypogonadism is also evident in abnormal
pubertal development. While pubic and axil-lary hair may develop early or normally, theremainder of pubertal development is delayedand usually incomplete. Adult males onlyoccasionally have voice change, male bodyhabitus, or substantial facial or body hair. Infemales, breast development generally beginsat a normal age, but there is usually amenor-rhoea or oligomenorrhoea. Menarche mayoccur as late as the 30s, particularly inassociation with significant weight loss. In bothmales and females, sexual activity is rare andinfertility is the rule.The hypogonadism is hypothalamic in origin
and gonadotrophins, oestrogen, and testoster-one are generally deficient.4 9 Since the pitui-tary gland and gonads are normal but under-
stimulated, treatment with pituitary or gonadalhormones can improve secondary sexcharacteristics.49
HYPERPHAGIA AND OBESITYThe proportion of fat mass to lean body mass ishigh even in thin infants with PWS,'0presumably because of hypotonia and the sub-sequent decreased muscle bulk. However,significant obesity generally begins after hyper-phagia has its onset, often between the ages of1 and 6 years. Food seeking behaviour, withhoarding of or foraging for food, eating ofunappealing substances such as garbage, petfood, and frozen food, and stealing of food ormoney to buy food, are common. A highthreshold for vomiting may complicate binge-ing on spoiled food from the garbage or suchitems as boxes of sugar or frozen uncookedmeat, and toxicity from ineffective Ipecac usedto induce vomiting has occurred. The obesity iscentral in distribution with relative sparing of
A..
.s~~~~~~~~~~~~..
xl,
v;.4
SW
',.,.. ss KSX r:-
I E ..... ,- g 'S. i:s, a i:
.|w w
Cassidy
... d.,
#.b
zrIim
i.-. -
.i..
I
-.-I.-
1:1 1-
on Novem
ber 9, 2020 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.34.11.917 on 1 N
ovember 1997. D
ownloaded from

Prader- Willi syndrome
SHORT STATUREBirth weight and length are usually within nor-mal limits, but the early period of failure tothrive may result in both weight and lengthbeing below the 3rd centile. Short stature, ifnot apparent in childhood, is almost alwayspresent by the second half of the seconddecade, associated with lack of a pubertalgrowth spurt. Average height is 155 cm formales and 148 cm for females. African-Americans tend to be taller.'9 Growth hormonedeficiency has been shown in most testedpatients with PWS, and treatment with growthhormone increases height and lean body mass,often resulting in decreased body massindex.9 22
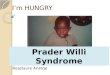
Figure 2 A 41 year old with PWS. See textfor descriptionofphenotypic findings.
the distal extremities, and even subjects whoare not overweight tend to deposit fat on theabdomen, buttocks, and thighs (figs 1 and 2).
Obesity is the major cause of morbidity andmortality in PWS and longevity may be nearlynormal if it is avoided. 12 13 Cardiopulmonarycompromise results from excessive obesity, as
can type II diabetes mellitus, hypertension,thrombophlebitis, and chronic leg oedema.Sleep apnoea occurs at increased frequency.The hyperphagia is the result of a hypotha-
lamic abnormality resulting in lack ofsatiety.'4 '1 In addition, there is a decreasedcaloric requirement,'6 probably related tohypotonia and decreased activity.
DYSMORPHIC APPEARANCE
Characteristic facial features, including narrowbifrontal diameter, almond shaped palpebralfissures, narrow nasal bridge, and downturnedmouth with a thin upper lip, are either presentfrom birth or evolve over time'7 (figs 1 and 2).Small, narrow hands with a straight ulnar bor-der and sometimes tapering fingers, and short,often broad feet are usually present by the age
of 10, with an average adult foot length of 20.3cm in females and 22.3 cm in males.'8 African-Americans are less likely to have small handsand feet.'9 A characteristic body habitus,including sloping shoulders, heavy mid section,and genu valgum with straight lower legborders, is usually present from toddlerhood(figs 1 and 2). Hypopigmentation for the fam-ily, manifested as fairer skin, hair, and eye col-our, occurs in about a third of affectedsubjects.20 Strabismus is often present.2'Scoliosis/kyphosis are common, the formeroccurring at any age, and the latter developingin early adulthood (fig 2).
DEVELOPMENTAL DELAY/MENTAL RETARDATIONIn addition to the gross motor delay describedabove, language development is also delayed.Verbal skills are an ultimate strength in mostpatients, though speech is often poorly articu-lated, having a nasal/slurred character. Cogni-tive abnormalities are evident and most pa-tients are mildly retarded (mean IQ 60s-low70s).6 23 Approximately 40% have borderlineretardation or low normal intelligence andabout 20% have moderate retardation. Aca-demic performance is poor for cognitive ability.Specific patterns of cognitive strength andweakness have begun to emerge, frequentlywith relative strength in reading, visual-spatialskills, and long term memory, and weakness inarithmetic, sequential processing, and shortterm memory.7 Coming to clinic with a book ofword search puzzles can almost be considered adiagnostic sign for PWS and unusual skill withjigsaw puzzles is common.
BEHAVIOURAL PROBLEMSA characteristic behavioural profile becomesevident in early childhood, with temper tan-trums, stubbornness, controlling and manipu-lative behaviour, obsessive-compulsive charac-teristics, and difficulty with change inroutine. 7 Lying, stealing, and aggressivebehaviour are common. True psychosis isevident in young adulthood in approximately5-10% of patients. Behavioural and psychiatricproblems interfere the most with quality of lifein adulthood.
MISCELLANEOUS CHARACTERISTICSA variety of more minor findings are unique tothis condition, including thick, viscous salivathat may predispose to dental caries andcontribute to articulation abnormalities, highpain threshold, skin picking and high thresholdfor vomiting. Sleep disturbances, especiallyexcessive daytime sleepiness and oxygen de-saturation in REM sleep, are common even inthe absence of obesity.25 Osteoporosis isfrequent.
ManagementManagement of PWS is largely problemoriented. Early intervention and special educa-tion, followed by supportive employment, areappropriate to address the developmentaldisabilities. Physical, occupational, and speech
919 on N
ovember 9, 2020 by guest. P
rotected by copyright.http://jm
g.bmj.com
/J M
ed Genet: first published as 10.1136/jm
g.34.11.917 on 1 Novem
ber 1997. Dow
nloaded from

Cassidy
PWs
cen-KD151l ZNF127 D15S11 PW71 SNRPN IPW UBE:
SIC
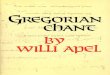
Figure 3 Genetic map of the l5qll-q13 region. Jagged,proximal and one common distal breakpoints, circles indicand bars indicate critical regions involved in PWS, Angelimprinting centre (IC), the centromere (cen), and telomerand the IC function. (Map contributed by Robert D NichCase Western Reserve University).
therapies can be bobesity can be contilow calorie diet of:regular exercise (3appropriate goal), acation, such as loc:close supervision tcfar, no medication Eness in controllingshows great benefreplacement. Sex I
improve secondarytheoretically will imtosterone treatmenwith an increase in <ucts to increase saliof benefit in treatin,ably improve dentstrict reinforcementdelineation of beh.establishment of re
improved behaviouicific serotonin reupple, fluoxetine) ofteoptimal living situalterms of behaviouihas been documentcially designated foi
Aetiology and genAlthough many ofresult from hypotstructural defect ofdocumented on
Therefore, the defibut its nature hasthe other hand, thebeen intensively inm
Prader-Willi synabsence of normallgenes at chromosornally inherited geowing to genetic im75% of patients w
there is a deletionchromosome 15qlof cases, the same 4Most of the remailuniparental disom15.' 28 29 ApproximPWS have a trans]abnormality involvhas caused either afor the critical regiGenomic imprin
explanation for th(on the clinical ou
UPD. In fact, at le.
A' S virtually all families studied in which there hasbeen a recurrence of PWS, have neither
~3A GABRB3 GABRG3 )+tel deletion nor UPD, but rather have a very smallp0 - ~~~/tel
D15S10 GABRA5 PX deletion in the centre controlling imprinting
within 15ql 1-q13, the imprinting centre0 200 kb (IC).6 7 03 Methylation is one mechanism by
lines indicate the two common which genomic imprinting can occur, andate genes and reference markers, methylation has been shown for several genesfman syndrome (AS), and the identified within the PWS/AS region.27-e (tel). See text for details of genes It is of interest that a clinically very differentoils, PhD and Nancy Rebert, disorder, Angelman syndrome, is the result of
an oppositely imprinted gene in the same)eneficial at all ages. The region of chromosome 15.3 36 Thus, approxi-rolled with a well balanced mately 60% of patients with Angelman syn-about 1000-1200 kcal/day, drome have the same 1 5ql 1-qi 3 deletion, but0 minutes per day is an occurring in the maternally derived chromo-and environmental modifi- some. Paternal uniparental disomy is seen inking kitchen cabinets and 3-5%. In approximately 10% there is anZ avoid access to food. So imprinting mutation and the remaining cases, aias had long term effective- category that has not been reported in PWS,appetite. Recent evidence have a presumed single gene mutation. Re-it from growth hormone cently, mutations in the UBE3A gene haveiormone replacement will been identified in a small number of these{ sex characteristics and patients.37 38prove osteoporosis, but tes- A number of genes have been mapped withint is sometimes associated the PWS/Angelman syndrome region and oth-aggressive behaviour. Prod- ers that are not maternally imprinted have beeniva production have proved mapped between the common deletion break-g the dry mouth and prob- points (fig 3). The first mapped gene, consid-:al hygiene. Behaviourally, ered an important candidate gene, is SNRPNt of behavioural limits, clear (small nuclear ribonucleoprotein N). This geneavioural expectations, and is expressed from the paternally inheritedgular routines often lead to chromosome only39A1 and is expressed abun-r. Medications such as spe- dantly in brain. Other genes in the PWS/AS?take inhibitors (for exam- region include ZNF1 27, a zinc finger gene, and!n improve behaviour. The two additional non-coding genes (the IC tran-tion for adults with PWS in script and IPW). All these exclusively pater-r and weight management nally expressed genes and transcripts are inac--ed to be a group home spe- tivated in patients with PWS with an
r this condition.'3 26 imprinting mutation, including those patientswith a small (7-25 kb) deletion or without
ietics detected deletions.33 The non-imprinted Pthe manifestations of PWS gene, which also resides in this region, codesthalamic insufficiency, no for tyrosinase positive albinism, and its deletionthe hypothalamus has been probably causes the hypopigmentation seen inpostmortem examination. 1/3 of patients with PWS.42iciency must be functional, Recently, some clinical differences have beennot yet been identified. On reported between patients with PWS resultinggenetic basis for PWS has from deletion and UPD.1316 Perhaps the most
restigated. clinically significant of these is that patientsidrome is caused by the with UPD may lack the typical facialy active paternally inherited phenotype45 and may have delayed diagnosis.46me 1 5(ql1 -qi 3); the mater- In addition, African-Americans with PWS are
nes are normally inactive often of normal height, have normal sizedLprinting.27 In approximately hands and feet, and may also lack the typicalTith clinically typical PWS, facial phenotype.'9)f the paternally contributed1-q13.2 In the vast majority Diagnosis, differential diagnosis, and4 Mb deletion has occurred. diagnostic testingning patients have maternal Diagnostic criteria were developed by consen-
y (UPD) for chromosome sus before the availability of complete sensitiveiately 5% of patients with and specific laboratory testing.' These are stilllocation or other structural extremely valuable in suggesting the diagnosiszing chromosome 15 which and indicating the need for diagnostic testingi deletion or maternal UPD (table 1).on. The differential diagnosis for PWS in
iting in proximal 15q is the infancy includes many causes of neonatale parent of origin influence hypotonia, particularly neuromuscular disor-itcome of deletion 15q or ders. Later in childhood and adulthood, a
ast 1% of patients, including number of conditions in which mental
920
D15S13
on Novem
ber 9, 2020 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.34.11.917 on 1 N
ovember 1997. D
ownloaded from

Prader-Wilhi syndrome
Table 1 Summary of the clinical diagnostic criteria forPrader-Willi syndrome (adaptedfrom Holm et al7). Thediagnosis should be strongly suspected in children under 3years of age with five points, threefrom major criteria, or inthose above 3 years with eight points,fourfrom majorcriteria. The original diagnostic criteria, developed beforethe availability of sensitive and specific genetic testing,included a major criteria ofchromosome 15 deletion orother chromosome 15 anomaly
Major criteria (1 point each)Infantile central hypotoniaInfantile feeding problems/failure to thriveRapid weight gain between 1 and 6 years
Characteristic facial featuresHypogonadism: genital hypoplasia, pubertal deficiencyDevelopmental delay/mental retardation
Minor criteria (112 point each)Decreased fetal movement and infantile lethargyTypical behavioural problemsSleep disturbance/sleep apnoea
Short stature for the family by age 15 yearsHypopigmentationSmall hands and feet for height ageNarrow hands with straight ulnar borderEsotropia, myopiaThick, viscous salivaSpeech articulation defectsSkin picking
Supportive criteria (no points)High pain thresholdDecreased vomitingTemperature control problemsScoliosis/kyphosisEarly adrenarcheOsteoporosisUnusual skill with jigsaw puzzlesNormal neuromuscular studies
retardation/developmental delay is associatedwith obesity are included in the differentialdiagnosis, including Bardet-Biedl syndrome,Albright hereditary osteodystrophy, and Cohensyndrome.47 Mental retardation disorders inwhich obesity is an occasional finding, such as
fragile X and Angelman syndromes, may alsobe confused with PWS. Acquired hypothalamicinjury from accidents, tumours, or surgicalcomplications can closely mimic PWS.
Currently, the most efficient molecular diag-nostic test for PWS is determination of theparent specific methylation imprint within thePWS/AS region using Southern hybridisationand methylation sensitive probes (SNRPN andPW7 1).34 41 48-52 If the methylation pattern ischaracteristic of maternal only inheritance,PWS is confirmed, and if not, PWS resultingfrom deletion, UPD, or an imprinting mutationis ruled out. Newer techniques using PCR to-detect the methylation status of SNRPN53 orSNRPN expression54 have been developed, butare not yet in widespread use. Determination ofwhether the PWS is the result of deletion,UPD, or an imprinting mutation is importantprimarily for genetic counselling purposes andto identify those few cases with a translocationor inherited microdeletion.High resolution cytogenetic analysis can
often detect the 15qi 1-q13 deletion; however,there is an unacceptably high false negative andfalse positive rate using this technique, and it isno longer considered sufficient for diagnosticpurposes.49 50 52 55 Fluorescence in situ hybridi-sation (FISH) using probes within thePWS/AS critical region (SNRPN or DI 5SI 1)is the definitive diagnostic test for the commonsized deletion causing PWS. It is best accom-plished in conjunction with a probe outside thecritical region, optimally a 15 centromeric
(alpha satellite) probe which can serve as acontrol, and a method to detect a cryptic trans-location involving chromosome 15 (whichwould predispose to unbalanced rearrange-ments or UPD, and thus increase the chance ofrecurrence).52
Uniparental disomy can be detected withPCR using informative microsatellite markersfrom the PWS/AS region by studying both par-ents and the child.52 56 Using additional mark-ers from other chromosomes can confirm cor-rect paternity.
Prenatal detection is possible. FISH isindicated when a cytogenetic 15q deletion issuspected on chorionic villus sampling (CVS)or amniocentesis. If trisomy 15 is detected onCVS and the fetus survives, parent of origin(methylation analysis or microsatellite marker)studies are indicated and validated.56-59 FISHand parent of origin studies are also indicated ifan inherited or de novo translocation involvingchromosome 15 is detected prenatally.
Parents should be studied in cases with anidentified imprinting mutation, since a healthyparent can carry this abnormality and be atincreased risk for recurrence.34 Prenatal detec-tion through identification of the mutation ormaternal only methylation pattern in a fetus ispossible.59The American Society of Human Genetics/
American College of Medical Genetics Testand Technology Transfer Committee hasdeveloped and published a statement regardingthe status of genetic testing for PWS andAngelman syndrome.52
Recurrence risk*PWS resulting from either the common largedeletion in the absence of a structural chromo-some abnormality or from UPD has not beenreported to recur. However, a paternal bal-anced insertion or gonadal mosaicism is possi-ble, and therefore a recurrence risk of approxi-mately 1% or less is appropriate for geneticcounselling purposes. UPD is caused bynon-disjunction, as evidenced by advancedmaternal age in this group,28 29 and by docu-mentation of trisomy 15 on CVS and maternalUPD at birth.60 Since non-disjunction canrecur, a recurrence risk of 1% is appropriate for
56 62 hsgenetic counselling purposes. In thosefamilies with a detected imprinting mutation(small deletion) or with a presumed imprintingmutation based on maternal only methylationpattern when other testing fails to indicatedeletion or uniparental disomy, a recurrencerisk of up to 50% pertains, as this is likely to bean imprinted dominant mutation, occurring inthe paternal grandmother's germline.34
ConclusionIn summary, PWS is a multisystem disorderwith considerable clinical variability. It iscaused by absence of expression of as yetunelucidated genes within 15qi 1-q13 from thenormally active paternal copy, with casesresulting from paternal interstitial deletion,maternal uniparental disomy, and imprintingmutations. Recently, testing through detectionof parent of origin of SNRPN has allowed
921
on Novem
ber 9, 2020 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.34.11.917 on 1 N
ovember 1997. D
ownloaded from

Cassidy
diagnostic confirmation in virtually all cases.Continued analysis of known but anonymousgenes within this region, and search foradditional genes, will probably provide infor-mation about genes contributing to normalhypothalamic function or regulation. Althoughsymptomatic management is available, moredefinitive treatment will probably await reversalof imprinting in this region.
I thank Robert D Nicholls, PhD and Nathaniel Robin, MD forcritically reviewing parts of the manuscript, Nancy Rebert forproviding the gene map, and Florence Stewart for secretarialassistance. I am very appreciative of long term assistance byclinic coordinators, especially Shauna Heeger, MS, and manycollaborators. I am particularly grateful to the families ofpatients affected with PWS for their continuing support andparticipation in Prader-Willi syndrome clinics and clinicalresearch. In particular, appreciation goes to those who are will-ing to have photographs published.
1 Prader A, Labhart A, Willi H. Ein Syndrom von Adipositas,Kleinwuchs, Kryptochismus und Oligophrenie nach myot-oniertgem Zustand im Neugeborenalter. Schweiz MedWochenschr 1956;86:1260-1.
2 Ledbetter DH, Riccardi VM, Airhart SD, Strobel RJ,Keenen SB, Crawford JD. Deletions of chromosome 15 asa cause of the Prader-Willi syndrome. N EnglJ Med 1981;304:325-9.
3 Nicholls RD, Knoll JHM, Butler MG, Karam S, Lalande M.Genetic imprinting suggested by maternal heterodisomy innon-deletion Prader-Willi syndrome. Nature 1989;342:281-5.
4 Cassidy SB. Prader-Willi syndrome. Curr Probl Pediatr1984;14: 1-55.
5 Holm VA, Cassidy SB, Butler MG, et al. Prader-Willisyndrome: consensus diagnostic criteria. Pediatrics 1993;91:398-402.
6 Dykens EM, Hodapp RM, Walsh K, Nash L. Profiles,correlates and trajectories of intelligence in individuals withPrader-Willi syndrome.3Am Acad Child Adolesc Psychiatry1992;31:1125-30.
7 Dykens EM, Cassidy SB. Prader-Willi syndrome: genetic,behavioral and treatment issues. Child Adolesc Clin N Am1996;5:913-27.
8 Burd L, Vesely B, Martsolf J, Kerbeshian J. Prevalence studyof Prader-Willi syndrome in North Dakota. Am J MedGenet 1989;37:97-9.
9 Lee PDK. Endocrine and metabolic aspects of Prader-Willisyndrome. In: Management of Prader-Willi syndrome. NewYork: Springer-Verlag, 1995:32-57.
10 Schoeller DA, Levitsky LL, Bandini LG, Dretz WW, Walc-zak A. Energy expenditure and body composition inPrader-Willi syndrome. Metabolism 1988;39: 115-20.
11 Butler MG. Prader-Willi syndrome: current understandingof cause and diagnosis. Am 7Med Genet 1990;35:319-32.
12 Greenswag LR. Adults with Prader-Willi syndrome. Asurvey of 232 cases. Dev Med Child Neurol 1987;29: 145-52.
13 Cassidy SB, Devi A, Mukaida C. Aging in Prader-Willisyndrome: 232 patients over age 30 years. Proc GreenwoodGenet Center 1994;13:102-3.
14 Zipf WB, Bernston GG. Characteristics of abnormalfood-intake patterns in children with Prader-Willi syn-drome and study of effects of naloxone. Am J Clin Nutr1987;46:277-81.
15 Holland AJ, Treasure J, Coskeran P, Dallow J, Milton N,Hillhouse E. Measurement of excessive appetite and meta-bolic changes in Prader-Willi syndrome. Int J Obes1993;17:526-32.
16 Holm VA, Pipes PL. Food and children with Prader-Willisyndrome. Am _J Dis Child 1976;130:1063-7.
17 Aughton DA, Cassidy SB. Physical features of Prader-Willisyndrome in neonates. Am J Dis Child 1990;144:1251-4.
18 Hudgins LH, McKillop JA, Cassidy SB. Hand and footlengths in Prader-Willi syndrome. Am J Med Genet199 1;41:5-9.
19 Cassidy SB, Geer JS, Holm VA, Hudgins L. African-Americans with Prader-Willi syndrome are phenotypicallydifferent. Am _J Hum Genet 1996;59:A2 1.
20 Butler MG. Hypopigmentation: a common feature of thePrader-Labhart-Willi syndrome. AmJHum Genet 1 989;45:140-6.
21 Wiesner GL, Bendel CM, Olds DP, et al. Hypopigmentationin the Prader-Willi syndrome. Am 7 Med Genet 1987;40:431-42.
22 Angulo M, Castro-Magana M, Mazur B, Canas JA, VitolloPM, Sarrantonio M. Growth hormone secretion andeffects of growth hormone therapy on growth velocity andweight gain in children with Prader-Willi syndrome. J Pedi-atr Endocrinol Metab 1996;9:393-400.
23 Curfs LG. Psychological profile and behavioral characteris-tics in Prader-Willi syndrome. In: Cassidy SB, ed.Prader-Willi syndrome and other ISq deletion disorders. Berlin:Springer-Verlag, 1992:211-22.
24 Dykens EM, Cassidy SB. Correlates of maladaptive behav-ior in children and adults with Prader-Willi syndrome. AmJ7Med Genet 1995;60:546-9.
25 Hertz G, Cataletto M, Feinsilver SH, Angulo M. Develop-mental trends of sleep-disordered breathing in Prader-Willisyndrome: the role of obesity. Am J Med Genet 1995;56:188-90.
26 Greenswag LR, Alexander RA, eds. Management of Prader-Willi syndrome. 2nd ed. New York: Springer-Verlag, 1995.
27 Nicholls RD. Genomic imprinting and uniparental disomyin Angelman and Prader-Willi syndrome: a review. Am _JMed Genet 1993;46:16-25.
28 Robinson WP, Bottani A, Yagang X, et al. Molecular,cytogenetic and clinical investigations of Prader-Willisyndrome patients. Am 7 Hum Genet 1991 ;49: 1219-34.
29 Mascari MJ, Gottlieb W, Rogan PK, et al. The frequency ofuniparental disomy in Prader-Willi syndrome. N Engl JMed 1992;326:1599-607.
30 Reis A, Klein-Vogler U, Dittrich B, et al. Imprintingmutations suggested by abnormal DNA methylationpatterns in familial Angelman and Prader-Willi syndromes.Am _J Hum Genet 1994;54:741-7.
31 Sutcliffe JS, Nakao M, Christian S, et al. Deletions of a dif-ferentially methylated CpG island at the SNRPN genedefine a putative imprinting control region. Nat Genet1994;8:52-8.
32 Buiting K, Saitoh S, Gross S, et al. Inherited microdeletionsin the Angelman and Prader-Willi syndromes define animprinting centre on human chromosome 15. Nat Genet1994;9:395-400.
33 Saitoh S, Buiting K, Rogan PK, et al. Minimal definition ofthe imprinting center and fixation of a chromosome15ql1 -q13 epigenotype by imprinting mutations. Proc NatlAcad Sci USA 1996;93:7811-15.
34 Saitoh S, Buiting K, Cassidy SB, et al. Clinical spectrum andmolecular diagnosis of Angelman and Prader-Willi syn-drome imprinting mutation patients. Am J Med Genet1997;68:195-206.
35 Clayton-Smith J, Pembrey ME. Angelman syndrome. J MedGenet 1992;29:412-15.
36 Williams CA, Angelman H, Clayton-Smith J, et al.Angelman syndrome: consensus for diagnostic criteria. AmJMed Genet 1995;56:237-8.
37 Kishino T, Lalande M, Wagstaff J. UBE3A/E6-APmutationscause Angelman syndrome. Nat Genet 1997;15:70-2.
38 Matsuura T, Sutcliffe JS, Fang P, et al. De novo truncatingmutations in E6-AP ubiquitin-protein ligase gene(UBE3A4) in Angelman syndrome. Nat Genet 1997;15:74-7.
39 Ozcelik T, Leff S, Robinson W, et al. Small nuclear ribonu-cleoprotein polypeptide N (SNRPN), an expressed gene inthe Prader-Willi syndrome critical region. Nat Genet 1992;2:265-9.
40 Glenn CC, Porter KA, Jong MTC, Nicholls RD, DriscollDJ. Functional imprinting and epigenetic modification ofthe human SNRPN gene. Hum Mol Genet 1993;2:2001-5.
41 Glenn CC, Saitoh S, Jong MTC, et al. Gene structure, DNAmethylation and imprinted expression of the humanSNRPN gene. AmJMed Hum Genet 1996;58:335-46.
42 Spritz RA, Bailin T, Nicholls RD, et al. Hypopigmentationin the Prader-Willi syndrome correlates with P genedeletion but not with haplotype of the hemizygous P allele.Am3rHum Genet 1997;71:57-62.
43 Gillessen-Kaesbach G, Robinson W, Lohmann D, Kaya-Westerloh S, Passarge E, Horsthemke B. Genotype-phenotype correlation in a series of 167 deletion and non-deletion patients with Prader-Willi syndrome. Hum Genet1995;96:638-43.
44 Mitchell J, Schinzel A, Langlois S, et al. Comparison of phe-notype in uniparental disomy and deletion Prader-Willisyndrome: sex specific differences. Am J Med Genet1996;65: 133-6.
45 Cassidy SB, Forsythe M, Heeger S, et al. Comparison ofphenotype between patients with Prader-Willi syndromedue to deletion 15q and uniparental disomy 15. AmJ MedGenet 1997;68:433-40.
46 Gunay-Aygun M, Cassidy SB. Delayed diagnosis in Prader-Willi syndrome due to uniparental disomy. Am _Med Genet1997;71:106-10.
47 Gunay-Aygun M, Cassidy SB, Nicholls RD. Prader-Williand other syndromes associated with obesity and mentalretardation. Behav Genet 1997;27:307-24.
48 Gillessen-Kaesbach G, Gross S, Kaya-Westerloh S, PassargeE, Horsthemke B. DNA methylation based testing of 450patients suspected of having Prader-Willi syndrome. J MedGenet 1995;32:88-92.
49 Smith A, Prasad M, Deng ZM, Robson L, Woodage T,Trent RJ. Comparison of high resolution cytogenetics,fluorescence in situ hybridisation, and DNA studies to vali-date the diagnosis of Prader-Willi and Angelman'ssyndromes. Arch Dis Child 1995;72:397-402.
50 Butler MG. Molecular diagnosis of Prader-Willi syndrome:comparison of cytogenetic and molecular genetic dataincluding parent of origin dependent methylation DNApatterns. Am_rMed Genet 1996;61:188-90.
51 Kubota T, Sutcliffe JS, Aradhya S, et al. Validation studies ofSNRPN methylation as a diagnostic test for Prader-Willisyndrome. Am _
Med Genet 1996;66:77-80.52 American Society of Human Genetics/American College of
Medical Genetics Report. Diagnostic testing for Prader-Willi and Angelman syndromes: report of the ASHG/ACMG Test and Technology Transfer committee. Am JHum Genet 1996;58:1085.
53 Kubota T, Das S, Christian SL, Baylin SB, Herman JG,Ledbetter DH. Methylation-specific PCR simplifies im-printing analysis. Nat Genet 1997;16:16-17.
922
on Novem
ber 9, 2020 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.34.11.917 on 1 N
ovember 1997. D
ownloaded from

Prader-Willi syndrome
54 Wevrick R, Francke U. Diagnostic test for the Prader-Willisyndrome by SNRPN expression in blood. Lancet 1996;348:1068-9.
55 Delach JA, Rosengren SS, Kaplan L, Greenstein RM, Cas-sidy SB, Benn PA. Comparison of high resolution chromo-some banding and fluorescence in situ hybridization(FISH) for the laboratory evaluation of Prader-Willisyndrome and Angelman syndrome. Am Med Genet1994;52:85-91.
56 Ledbetter DH, Engel E. Uniparental disomy in humans:development of an imprinting map and its implications forprenatal diagnosis. Hum Mol Genet 1995;4:1757-64.
57 Robinson WP, Langlois S, Schuffenhauer S, et al. Cytoge-netic and age-dependent risk factors associated with unipa-rental disomy 15. Prenat Diagn 1996;16:323-32.
58 Christian SL, Smith ACM, Macha M, et al. Prenataldiagnosis of uniparental disomy 15 following trisomy 15mosaicism. Prenat Diagn 1996;16:323-2.
59 Kubota T, Aradhya S, Macha M, et al. Analysis ofparent-of-origin specific DNA methylation at SNRPN and PW71 intissues: implication for prenatal diagnosis. Jf Med Genet1996;33:1011-14.
60 Cassidy SB, Lai L, Erickson RP, et al. Trisomy 15 with lossof the paternal 15 as a cause of Prader-Willi syndrome dueto maternal disomy.Am JHum Genet 1992;51:701-8.
61 Purvis-Smith SG, Saville T, Manass S, et al. Uniparentaldisomy 15 re§ulting from correction of an imitial trisomy15. Am JHum Genet 1992;50:1348-50.
62 Kennerknecht I. Differentiated recurrence risk estimationsin the Prader-Willi syndrome. Clin Genet 1992;41:303-8.
923
on Novem
ber 9, 2020 by guest. Protected by copyright.
http://jmg.bm
j.com/
J Med G
enet: first published as 10.1136/jmg.34.11.917 on 1 N
ovember 1997. D
ownloaded from