Embed Size (px)
Citation preview
Practical Spine Biomechanics for
Clinical Practice
2012 CNS Annual Meeting October 6-10 in Chicago, Illinois.
1
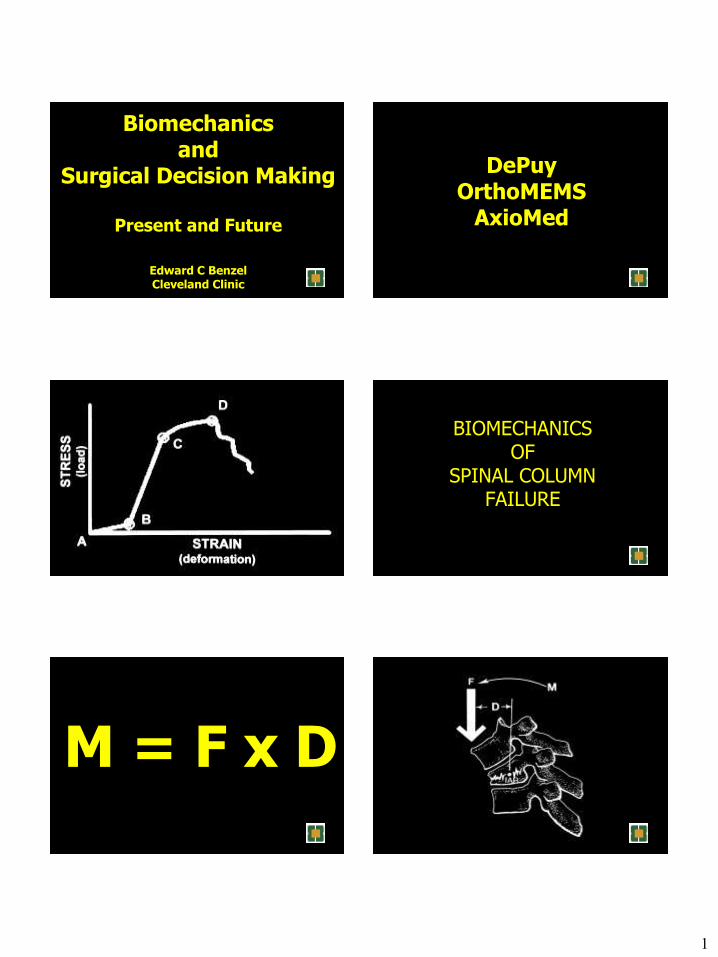
Biomechanics and
Surgical Decision Making
Present and Future
Edward C Benzel Cleveland Clinic
DePuy OrthoMEMS
AxioMed
BIOMECHANICS OF
SPINAL COLUMN FAILURE
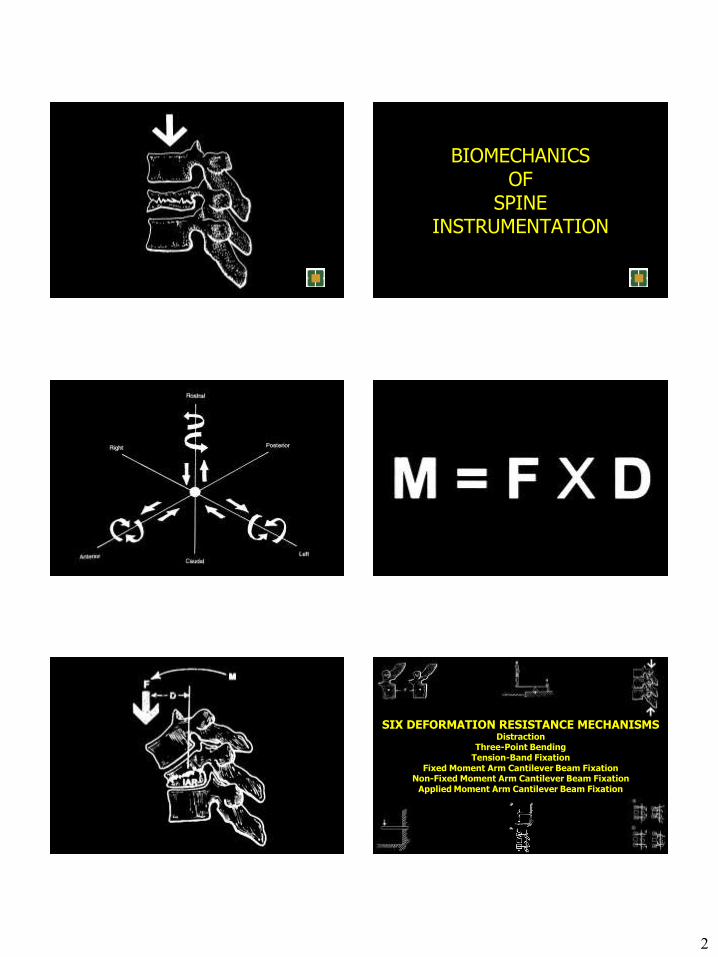
M = F x D
2
BIOMECHANICS OF
SPINE INSTRUMENTATION
SIX DEFORMATION RESISTANCE MECHANISMS Distraction
Three-Point Bending Tension-Band Fixation
Fixed Moment Arm Cantilever Beam Fixation Non-Fixed Moment Arm Cantilever Beam Fixation
Applied Moment Arm Cantilever Beam Fixation
3
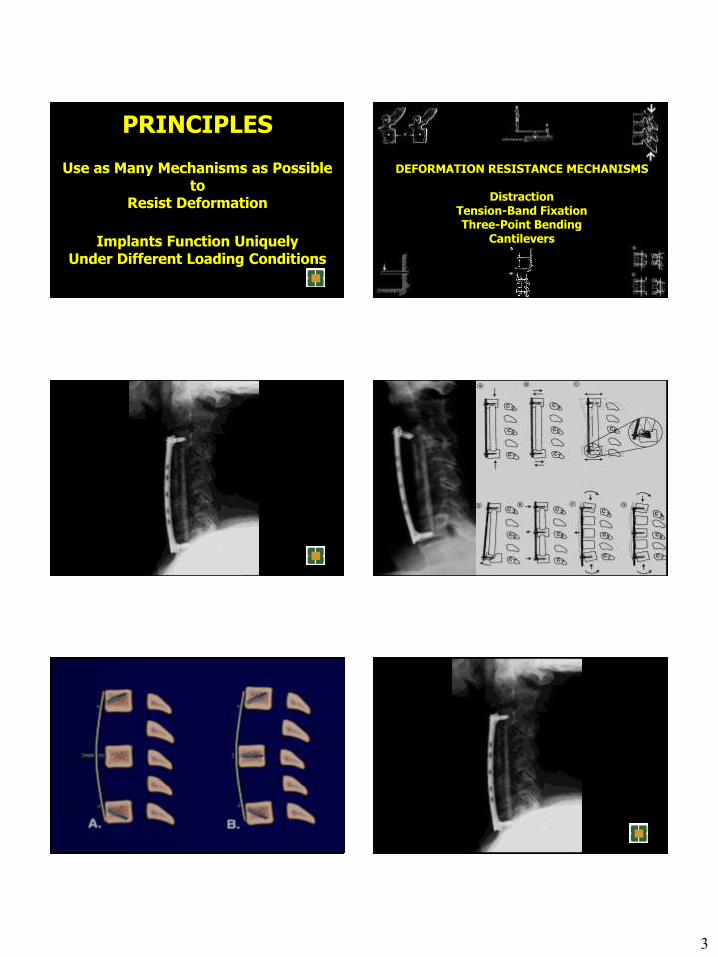
PRINCIPLES
Use as Many Mechanisms as Possible to
Resist Deformation
Implants Function Uniquely
Under Different Loading Conditions
DEFORMATION RESISTANCE MECHANISMS
Distraction Tension-Band Fixation Three-Point Bending
Cantilevers
4
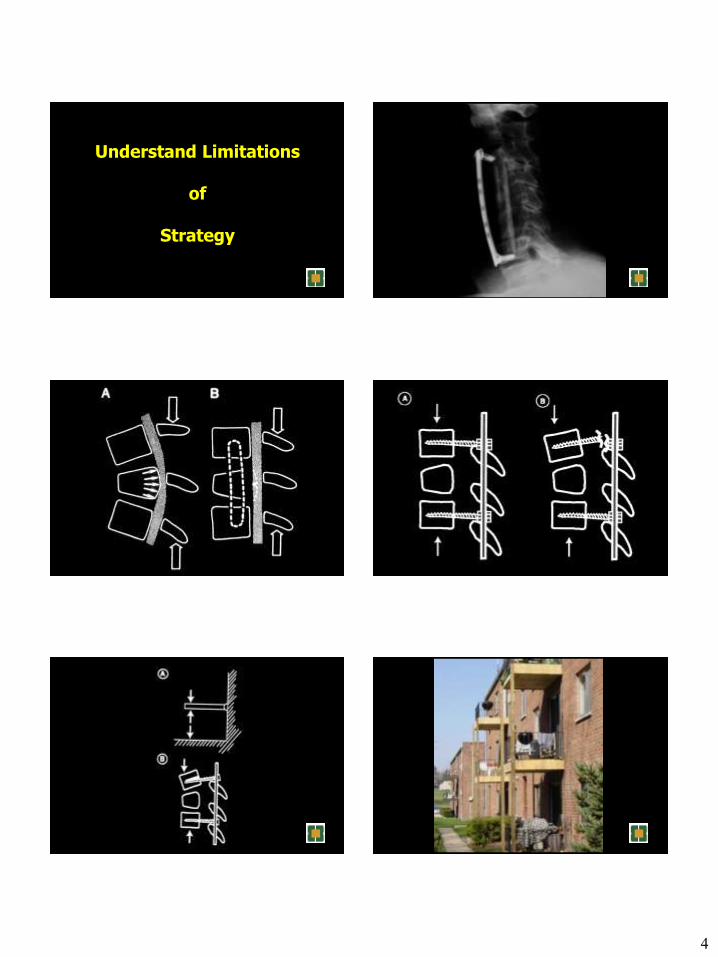
Understand Limitations
of
Strategy

5
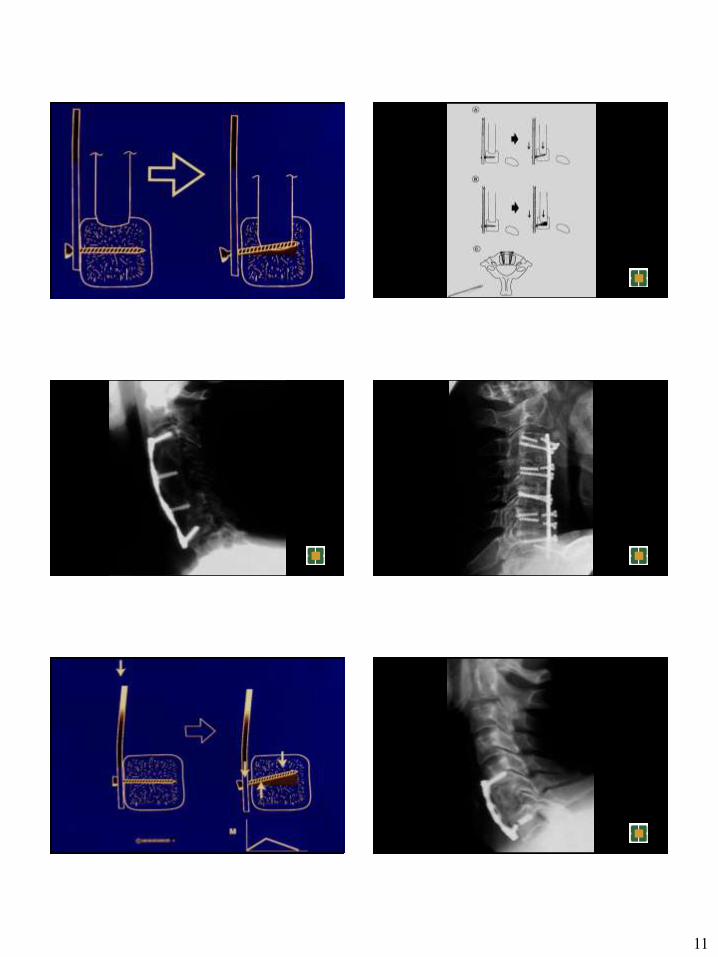
Dynamic Fixation
Wolff’s Law
Every change in the form and function of a bone, or of
function alone, is followed by specific definitive change in its
internal architecture and equally definitive secondary
changes in its external configuration, in accordance with
mathematical laws.
“Structure is nothing else than the physical expression of
function… under pathologic conditions the structure and
form of the parts change according to the abnormal
conditions of force transmission”

6
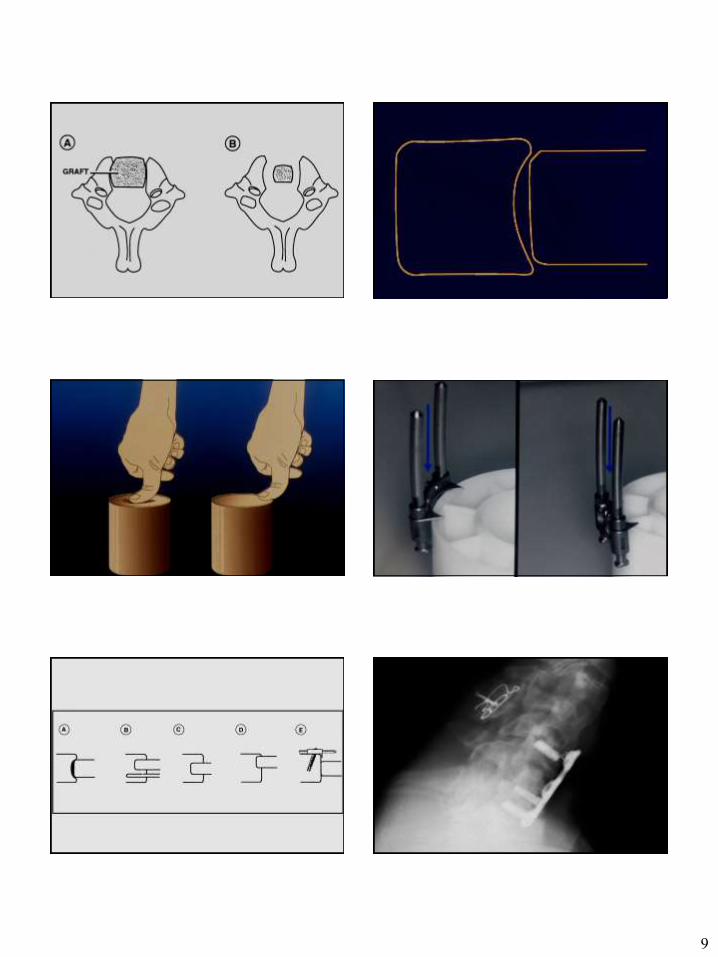
LOADING THE BONE GRAFT
Significant Loading and Unloading in
Flexion and
Extension
Buffered by Dynamic Implant
DiAngelo and Foley
7
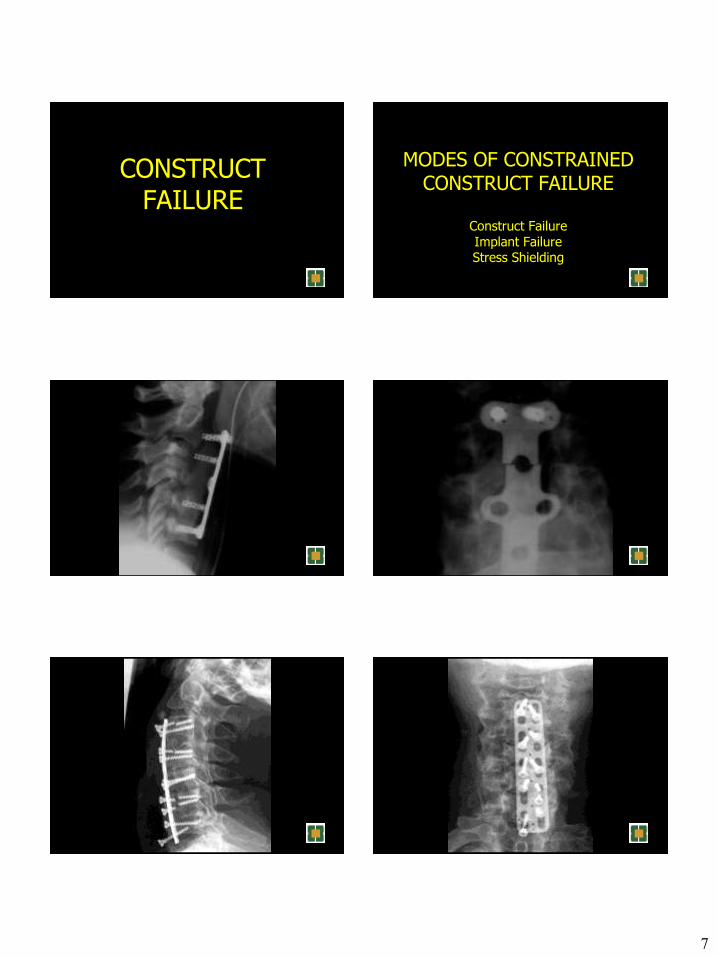
CONSTRUCT FAILURE
MODES OF CONSTRAINED CONSTRUCT FAILURE
Construct Failure Implant Failure Stress Shielding
8
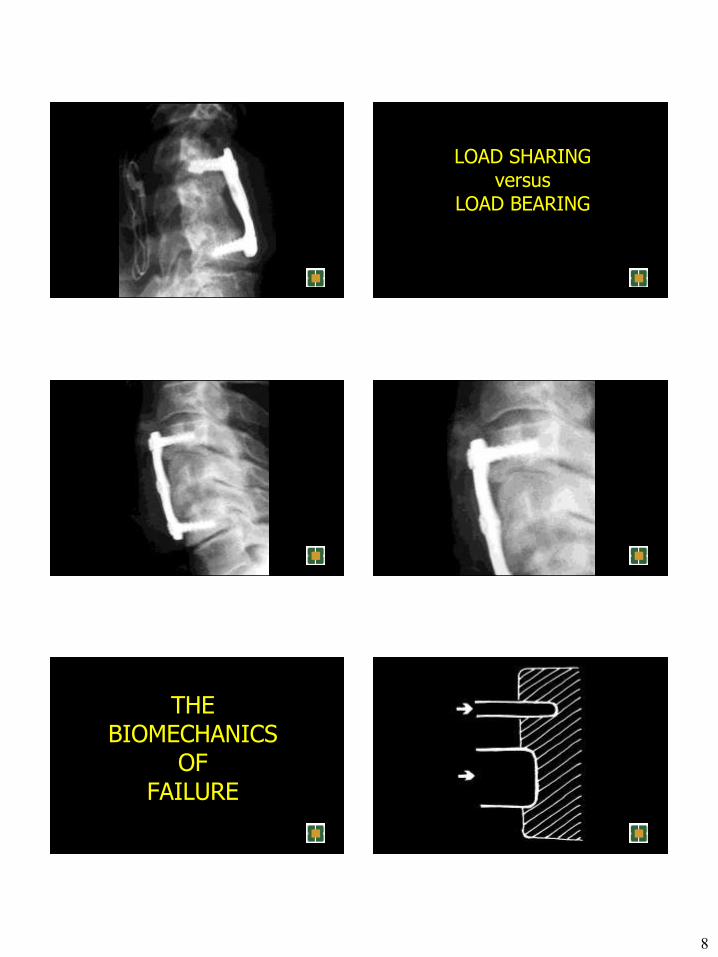
LOAD SHARING versus
LOAD BEARING
THE BIOMECHANICS
OF FAILURE
9

10
11
12
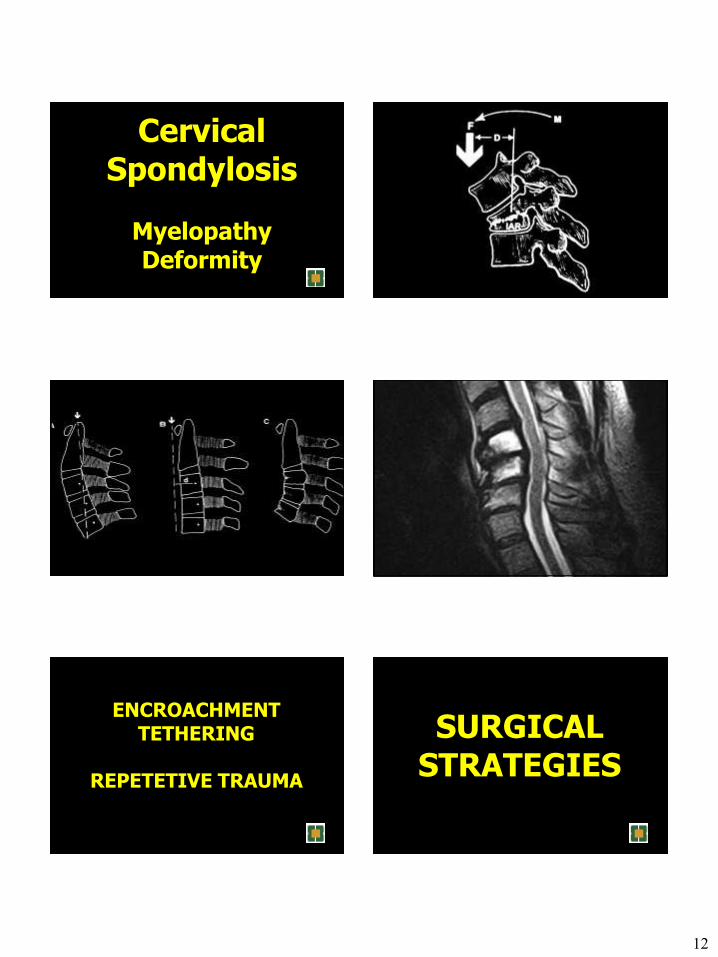
Cervical Spondylosis
Myelopathy Deformity
ENCROACHMENT TETHERING
REPETETIVE TRAUMA
SURGICAL
STRATEGIES
13
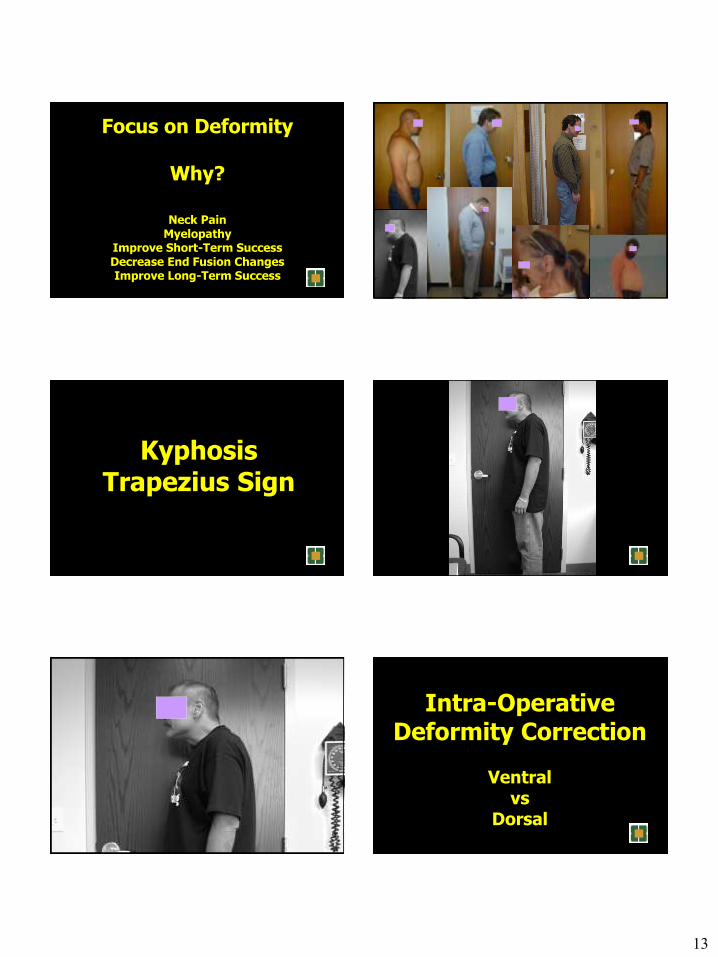
Focus on Deformity
Why?
Neck Pain Myelopathy
Improve Short-Term Success Decrease End Fusion Changes Improve Long-Term Success
Kyphosis Trapezius Sign
Intra-Operative Deformity Correction
Ventral
vs Dorsal
14
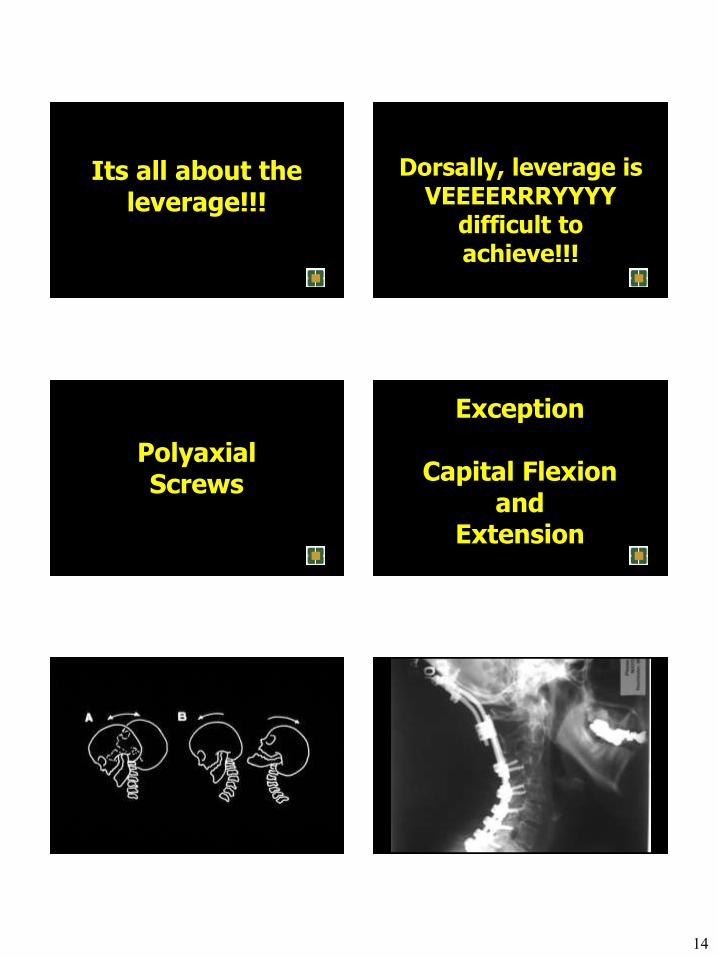
Its all about the leverage!!!
Dorsally, leverage is VEEEERRRYYYY
difficult to achieve!!!
Polyaxial Screws
Exception
Capital Flexion and
Extension
15
16
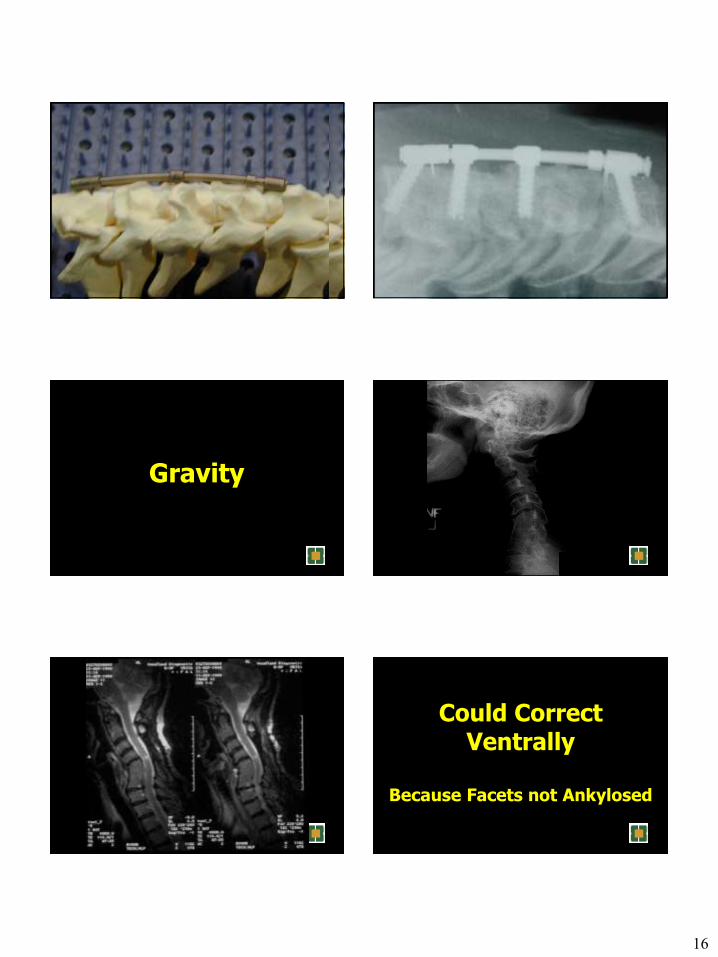
Gravity
Could Correct Ventrally
Because Facets not Ankylosed

17
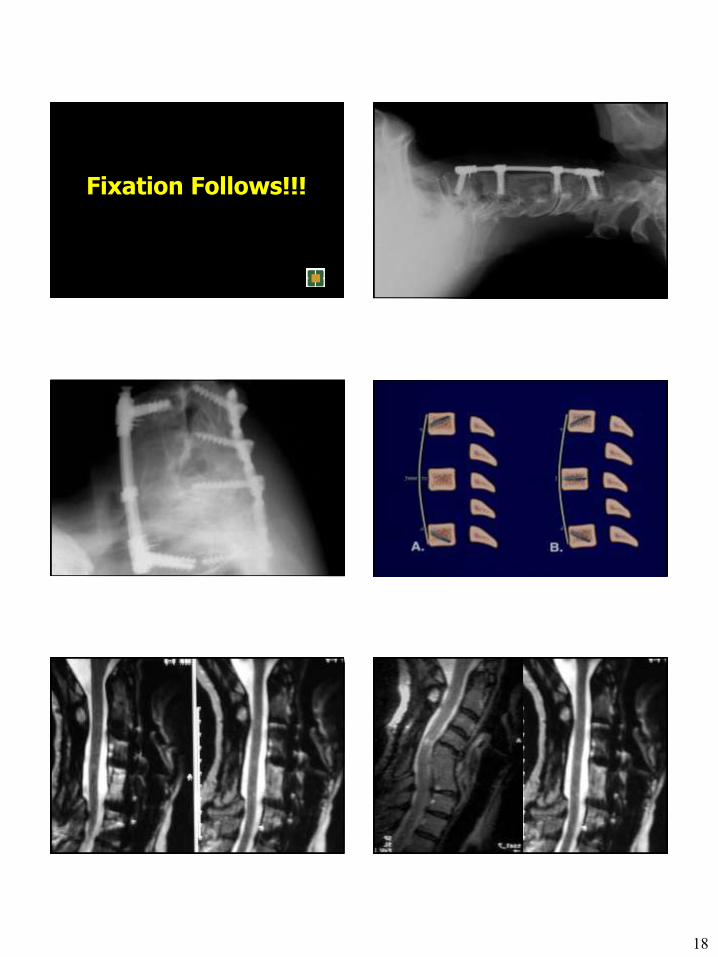
Its all about leverage!!!
18
Fixation Follows!!!
19
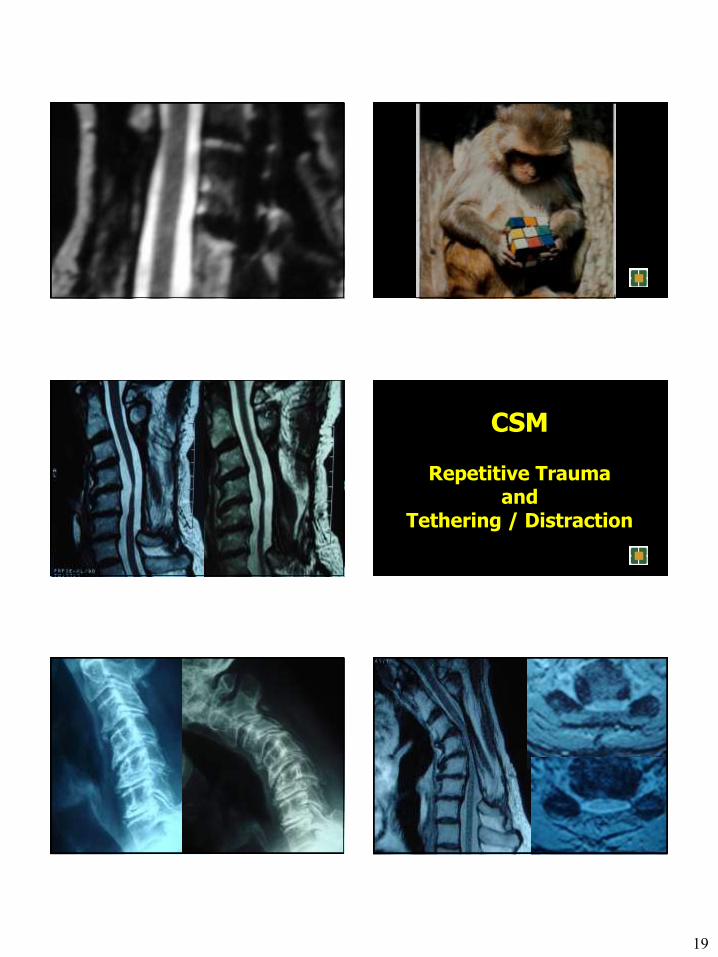
CSM
Repetitive Trauma and
Tethering / Distraction
20
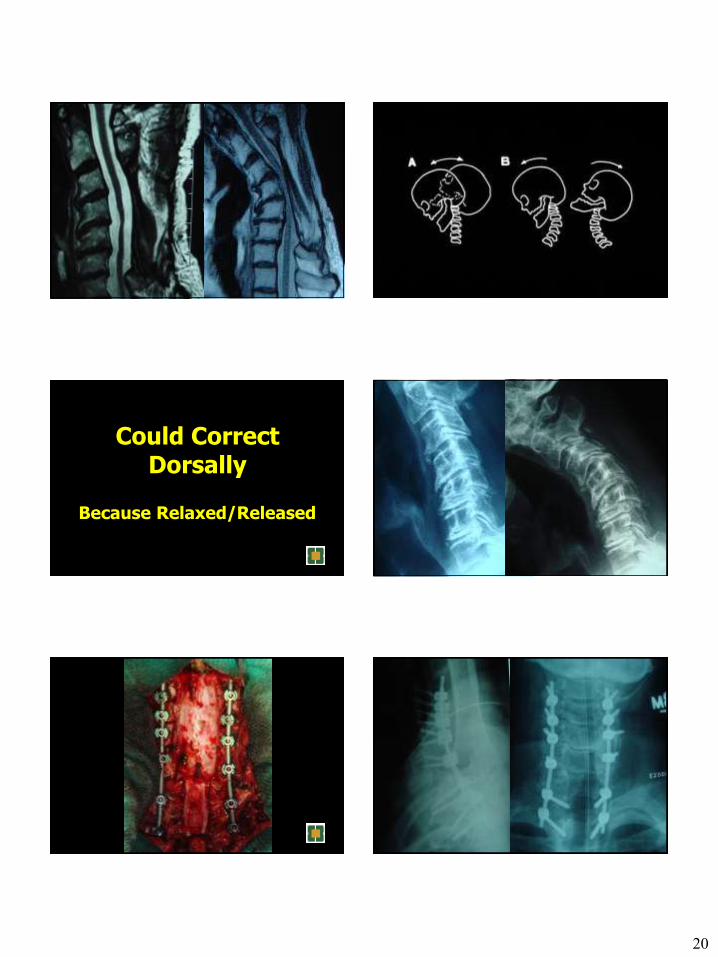
Could Correct Dorsally
Because Relaxed/Released
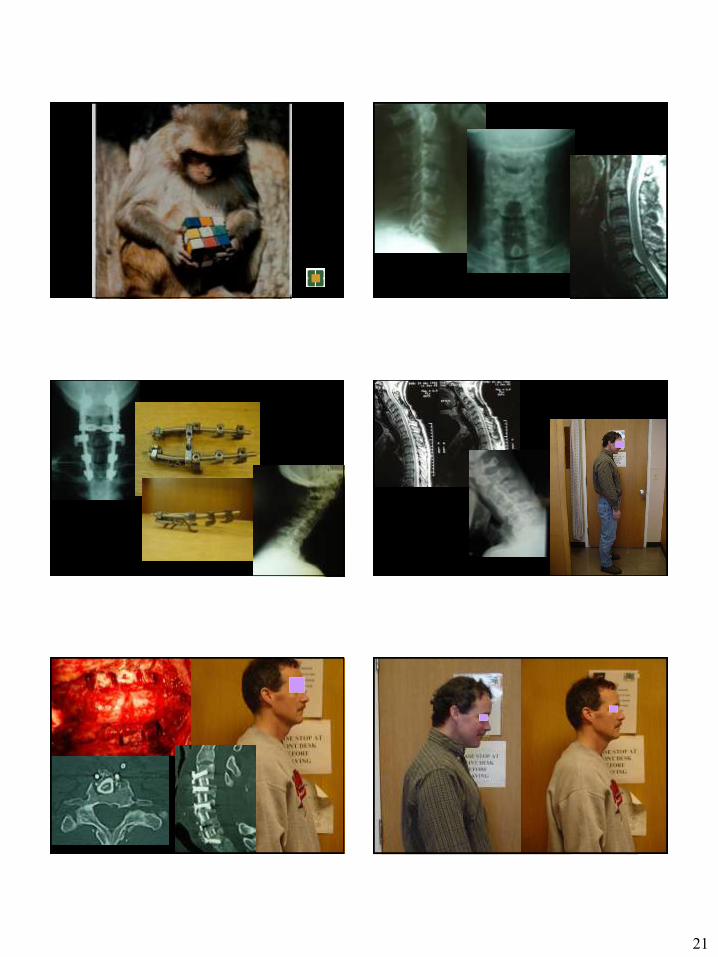
21

22
Correct at
Another Level
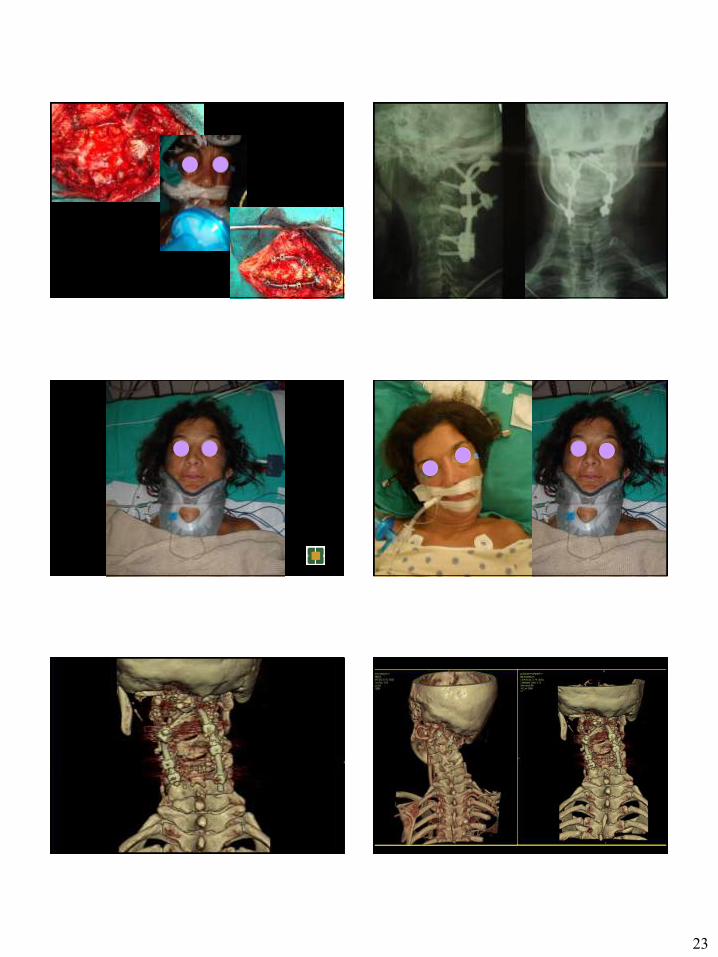
23
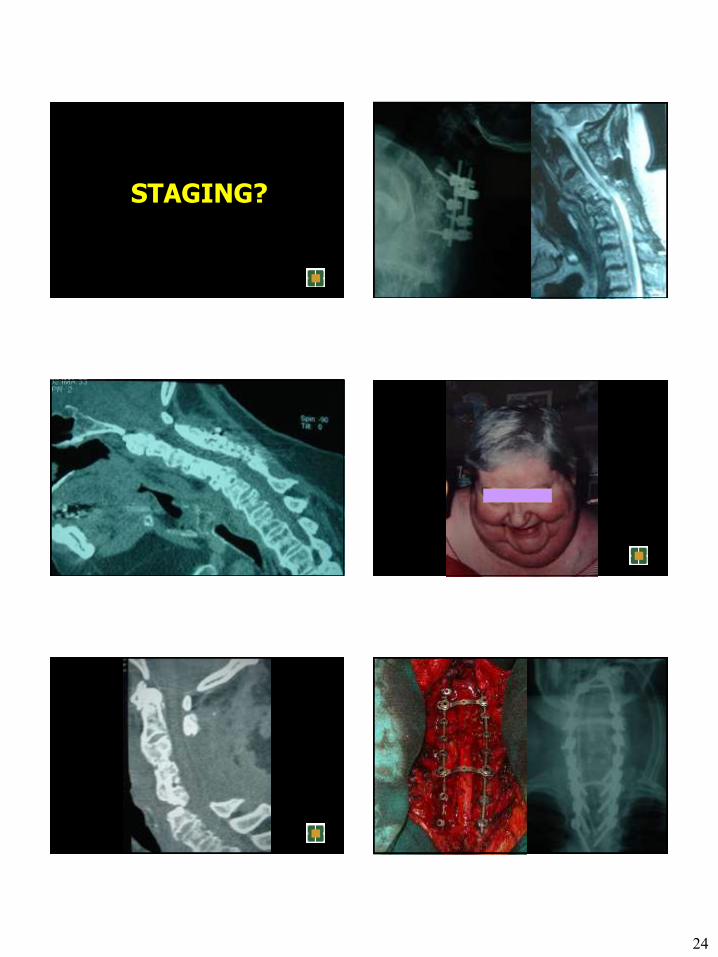
24
STAGING?
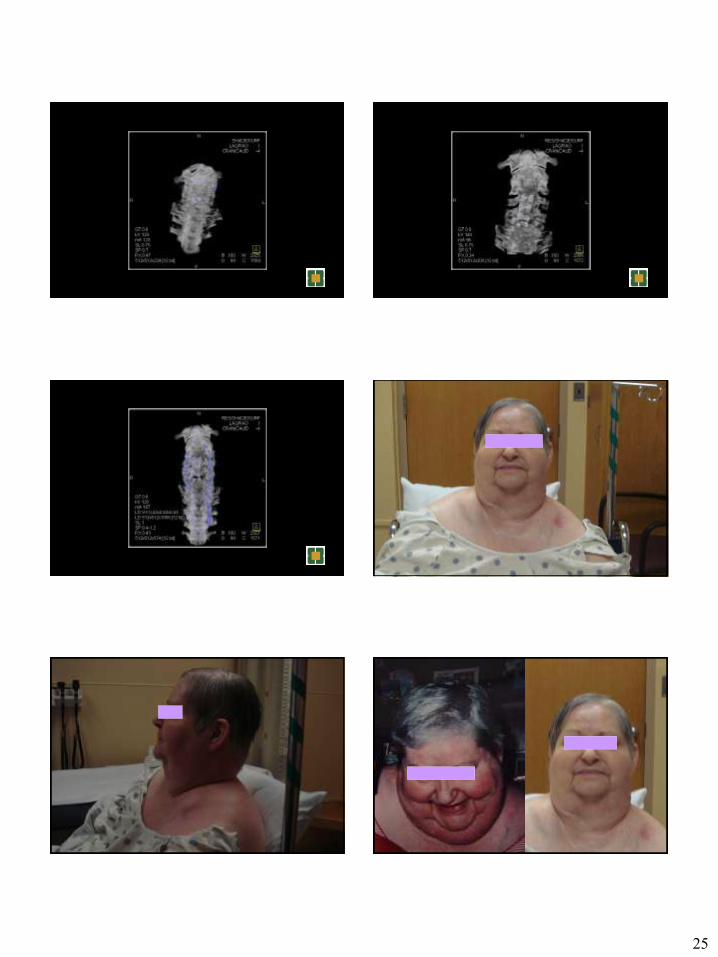
25

26
Dorsal Releasing (eg Osteotomy)
Fixation
Ventral Releasing Fixation
Correction
Posture Posture
Back Pain
Back Pain
Fundamentals Fundamentals
27
Rocket Science Rocket Science Innovation Drives Research
Innovation Drives Research
Research Drives Innovation Research Drives Innovation
Fusion
Motion Preservation Technologies
Assessment Strategies
Fusion
Motion Preservation Technologies
Assessment Strategies
“The treatment of back pain falls primarily in the non-operative domain. Surgical management for such a malady, therefore, should be a relative exception.”
Deep, Agonizing Pain Worsened with Loading
Improved with Unloading
28
MOTION
PRESERVATION
Interspinous Spacers (Motion Preservation)
Interspinous Spacers (Motion Preservation)
X-Stop (St. Francis Medical) X-Stop (St. Francis Medical)
Wallis (Spine Next, Bordeaux) Wallis (Spine Next, Bordeaux)
Diam (Medtronic) Diam (Medtronic)
Dynamic Stabilization (Motion Preservation or Fusion Enhancement)
Dynamic Stabilization (Motion Preservation or Fusion Enhancement)

29
TDA
Pain Generator ???????????
30
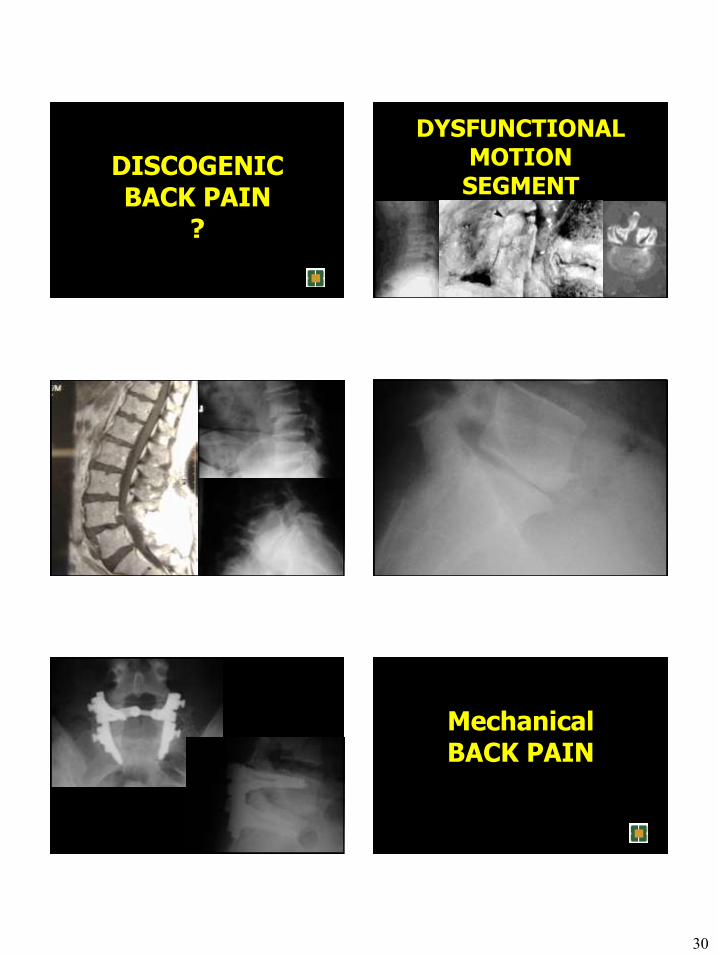
DISCOGENIC BACK PAIN
?
DYSFUNCTIONAL MOTION SEGMENT
Mechanical BACK PAIN
31
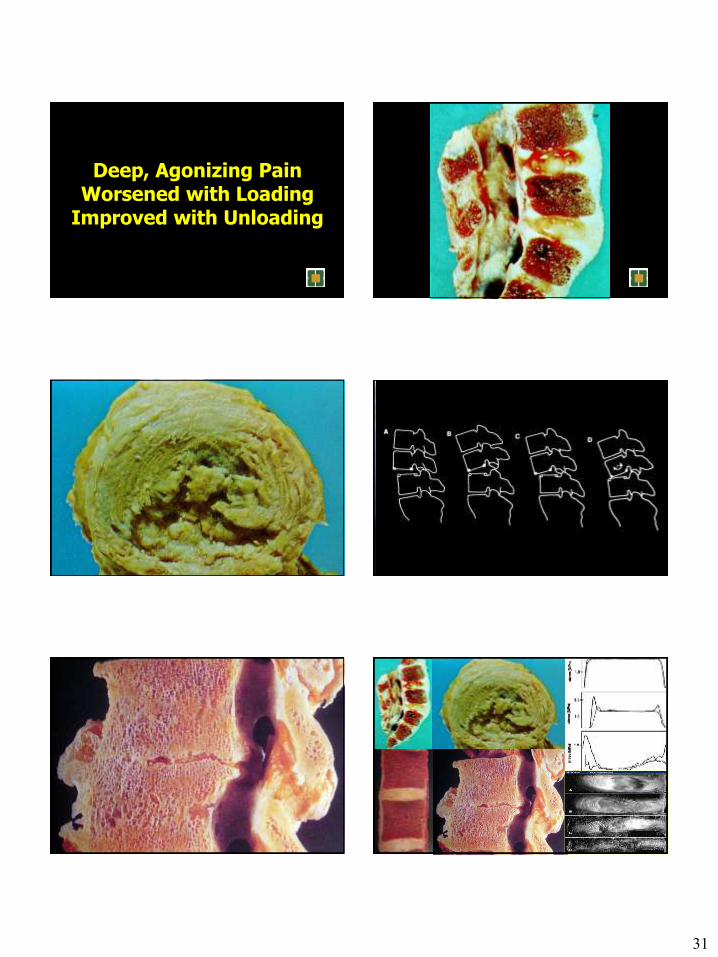
Deep, Agonizing Pain Worsened with Loading
Improved with Unloading

32
ATTRIBUTES
Replicates Anatomy Replicates Motion
Replicates Mechanics Minimal Complications
Acceptable Revision Strategies Longevity
Retardation of Degenerative Changes Symptom Relief
REPLICATES ANATOMY
Disc Interspace Height Disc Interspace Angle
REPLICATES MOTION
Translation Angular
Axial
Coronal
Sagittal
In Which Plane?
Axial? Translational?
Bending?
Along Which Axis? Axial
Coronal Sagittal
REPLICATES MECHANICS
Stiffness Shock Absorption
Creep
33
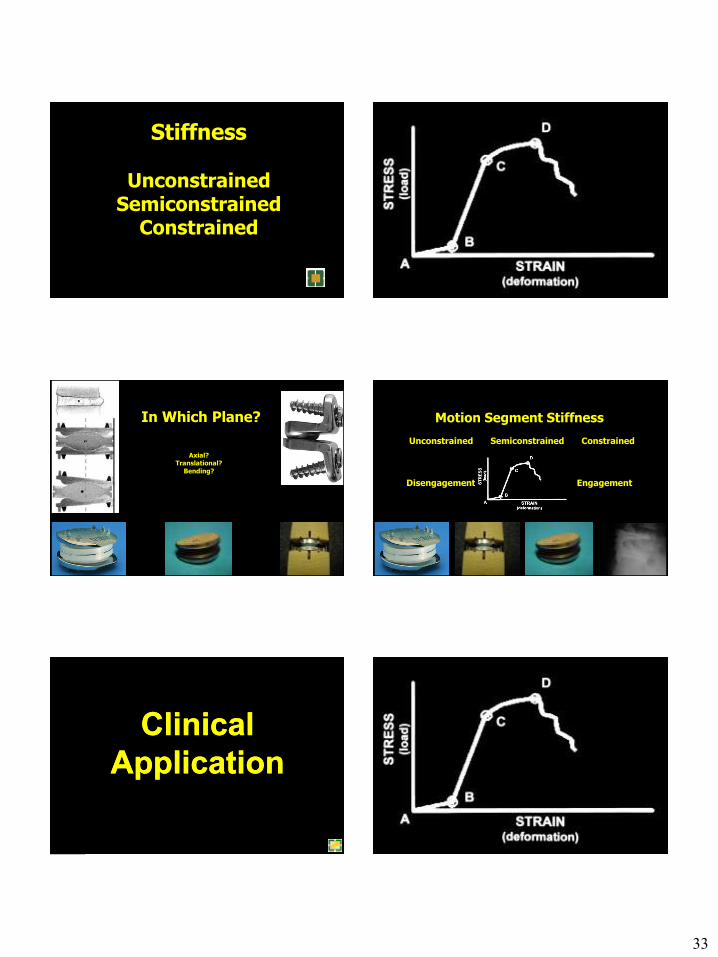
Stiffness
Unconstrained Semiconstrained
Constrained
In Which Plane?
Axial?
Translational?
Bending?
Motion Segment Stiffness
Unconstrained Semiconstrained Constrained
Disengagement Engagement
Clinical
Application
Clinical
Application
34
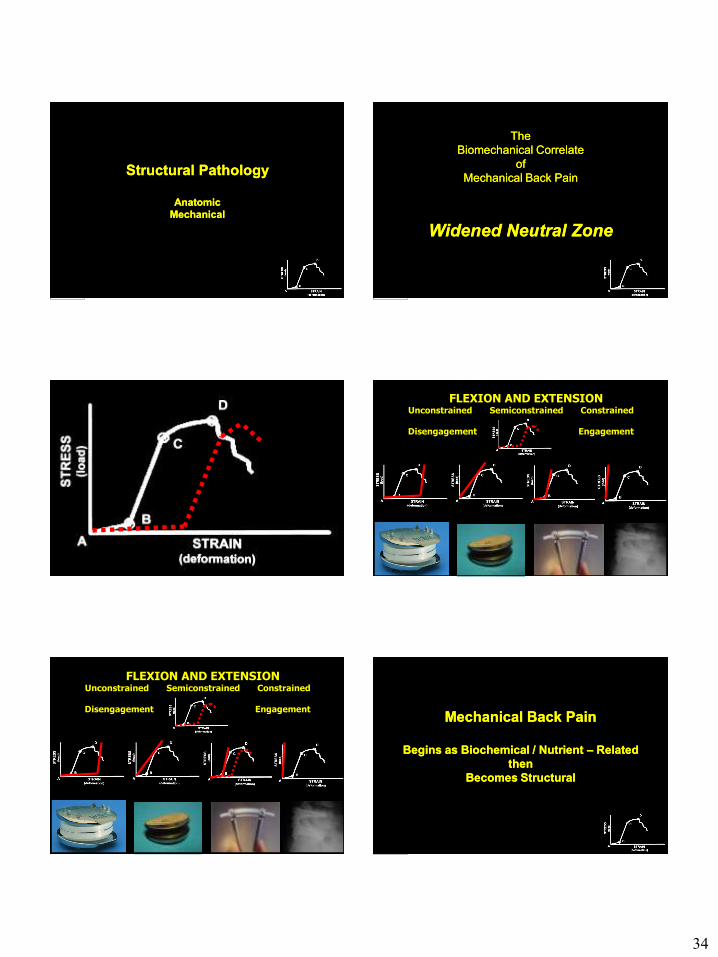
Structural Pathology
Anatomic
Mechanical
Structural Pathology
Anatomic
Mechanical
The
Biomechanical Correlate
of
Mechanical Back Pain
Widened Neutral Zone
The
Biomechanical Correlate
of
Mechanical Back Pain
Widened Neutral Zone
FLEXION AND EXTENSION Unconstrained Semiconstrained Constrained
Disengagement Engagement
FLEXION AND EXTENSION Unconstrained Semiconstrained Constrained
Disengagement Engagement
Mechanical Back Pain
Begins as Biochemical / Nutrient – Related
then
Becomes Structural
Mechanical Back Pain
Begins as Biochemical / Nutrient – Related
then
Becomes Structural
35
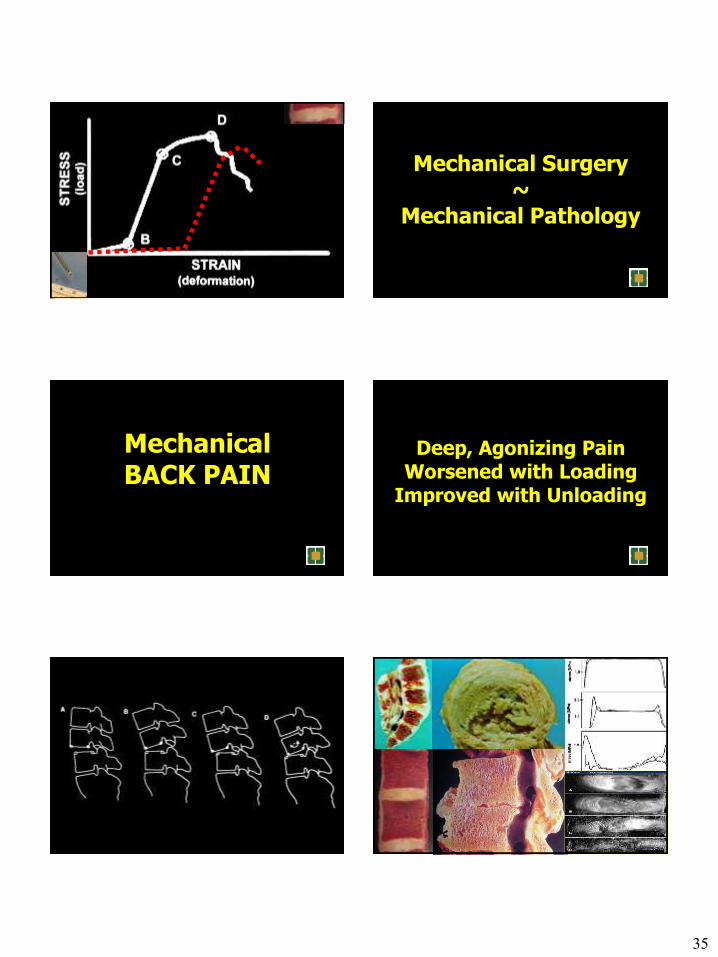
Mechanical Surgery ~
Mechanical Pathology
Mechanical BACK PAIN
Deep, Agonizing Pain Worsened with Loading
Improved with Unloading
36
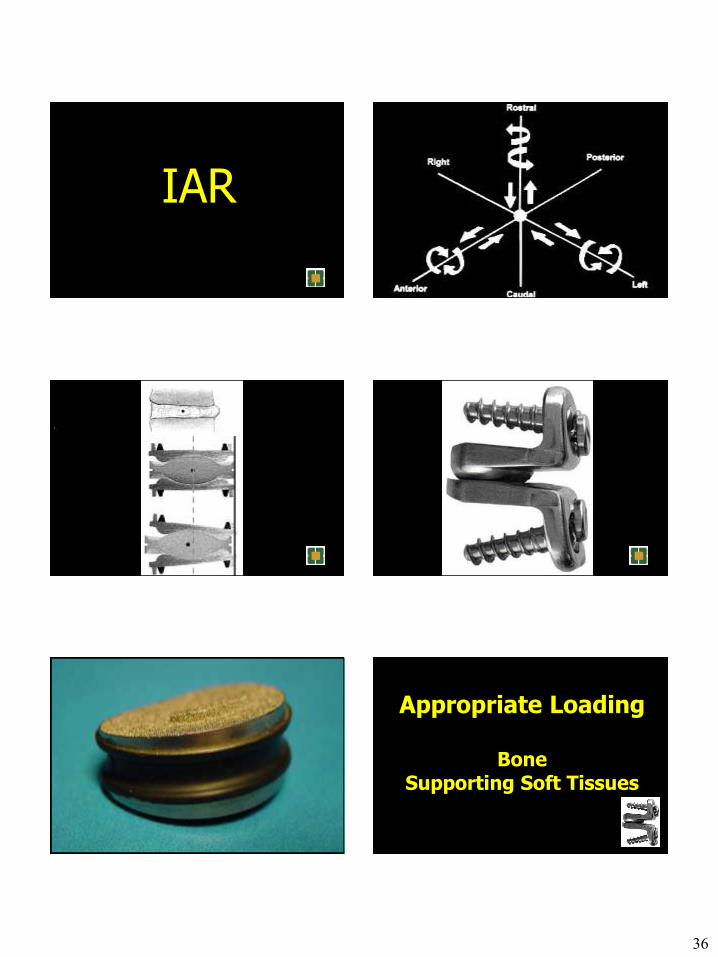
IAR
1.
Appropriate Loading
Bone Supporting Soft Tissues
37
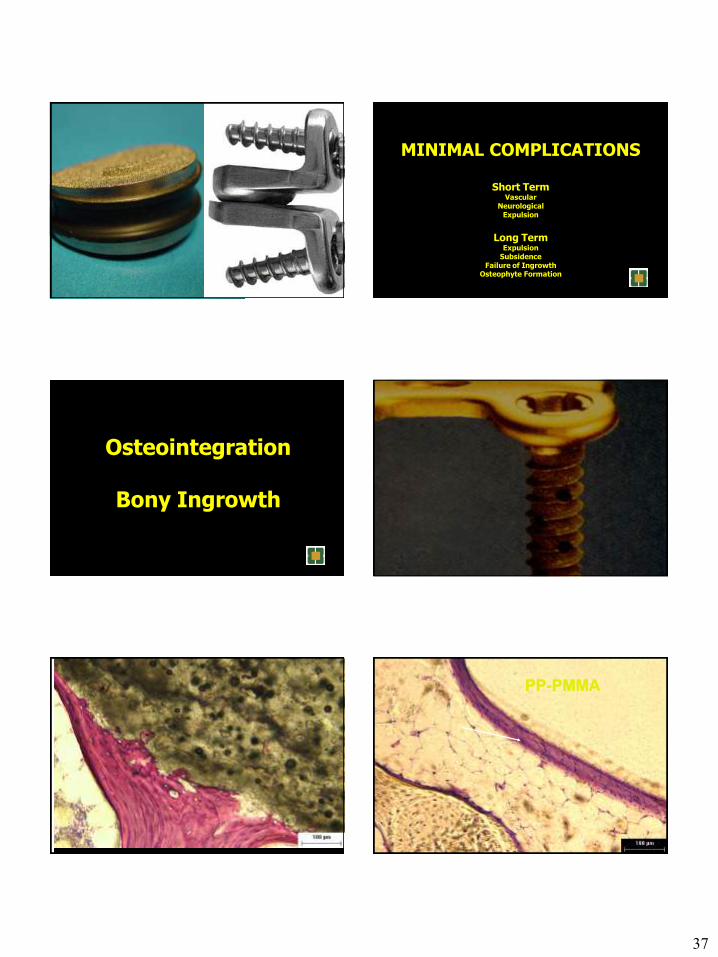
MINIMAL COMPLICATIONS
Short Term Vascular
Neurological Expulsion
Long Term
Expulsion Subsidence
Failure of Ingrowth Osteophyte Formation
Osteointegration
Bony Ingrowth
M
a
t
u
r
e
b
o
e
w
/
o
s
t
e
o
c
y
t
e
s
O
s
t
e
o
n
w
/
e
m
e
n
t
l
i
n
e
s
Paragon
X20
78 Week
PP-PMMA PP-PMMA

38
:
Large vs Small Pore Size Short - Long Term Fixation
Short Term Fixation
Intermediate Term Fixation
Long Term Fixation
ACCEPTABLE REVISION STRATEGIES
Dorsal Fusion and Instrumentation Removal?
LONGEVITY ?
RETARDATION OF DEGENERATIVE CHANGES ?
39
SYMPTOM RELIEF
Anecdotal Information Non-Inferiority ~ Inferior Device
Bias Investigator Bias
Patient Selection Bias Winner-Loser Bias
Case Against
Cervical
TDA
Case Against
Cervical
TDA
Adjacent Segment
Degeneration
Adjacent Segment
Degeneration
Adjacent Segment
Disease
Adjacent Segment
Disease
ASDeg
vs
ASDis
ASDeg
vs
ASDis

40
3 Studies – Ave Followup 4.5 Years
Prevelance of ASDis – 9-17%
Prevelance / years followed Annual Incidence of ASDis Requiring Surgery
1.5 - 4% / year
Hilibrand AS, Robbins M. Adjacent segment degeneration and adjacent segment disease: the
consequences of spinal fusion? The Spine Journal 4 (2004) 190S-194S
3 Studies – Ave Followup 4.5 Years
Prevelance of ASDis – 9-17%
Prevelance / years followed Annual Incidence of ASDis Requiring Surgery
1.5 - 4% / year
Hilibrand AS, Robbins M. Adjacent segment degeneration and adjacent segment disease: the
consequences of spinal fusion? The Spine Journal 4 (2004) 190S-194S
846 Patients – PLF – f/u 2.8 yrs
Prevalance ASDis - 9%
Annual Incidence ASDis - 3%
Henderson CM, Hennessy RG, Shuey HM, Shackelford EG. posterior lateral foraminotomy as an
exclusive operative technique for cervical radiculopathy: a review of 846 consecutively operated
cases. Neurosurgery 1983: 13(5):504-12
846 Patients – PLF – f/u 2.8 yrs
Prevalance ASDis - 9%
Annual Incidence ASDis - 3%
Henderson CM, Hennessy RG, Shuey HM, Shackelford EG. posterior lateral foraminotomy as an
exclusive operative technique for cervical radiculopathy: a review of 846 consecutively operated
cases. Neurosurgery 1983: 13(5):504-12
253 Patients ACD w and w/o F
f/u 3 years
Prevelance ASDis – 7%
Annual Incidence ASDis – 2.5%
No Difference - w and w/o
Lunsford LD, Bissonette DJ,Jannetta PJ, Sheptak PE, Zorub DS. Anterior surgery for
cervical disc disease, part 1: treatment of lateral cervical disc herniation in 253 cases. J
Neurosurg 1980:53:1-11
253 Patients ACD w and w/o F
f/u 3 years
Prevelance ASDis – 7%
Annual Incidence ASDis – 2.5%
No Difference - w and w/o
Lunsford LD, Bissonette DJ,Jannetta PJ, Sheptak PE, Zorub DS. Anterior surgery for
cervical disc disease, part 1: treatment of lateral cervical disc herniation in 253 cases. J
Neurosurg 1980:53:1-11
Hilibrand AS, Carson GD, Palumbo MA, Jones PK, Bohlman
HH. Radiculopathy and myelopathy at segments adjacent to
the site of a previous anterior cervical arthrodesis. J Bone Joint
Surg 1999; 81A(4):519-28
Hilibrand AS, Carson GD, Palumbo MA, Jones PK, Bohlman
HH. Radiculopathy and myelopathy at segments adjacent to
the site of a previous anterior cervical arthrodesis. J Bone Joint
Surg 1999; 81A(4):519-28
409 ACDF f/u 2-21 years
Prevelance ASDis – 14%
Annual Incidence ASDis – 3%
Risk Factors Neural Element Compression at Adjacent Levels
Surgery Adjacent to C56 or C67
Multilevel ACDF Lower Incidence of ASDis
(12% vs 18%, p<0.001)
409 ACDF f/u 2-21 years
Prevelance ASDis – 14%
Annual Incidence ASDis – 3%
Risk Factors Neural Element Compression at Adjacent Levels
Surgery Adjacent to C56 or C67
Multilevel ACDF Lower Incidence of ASDis
(12% vs 18%, p<0.001)
41
Back to the Basics
42
What Happens in
10, 15, 20 ….. Years?