Embed Size (px)
DESCRIPTION
Biomechanics of the lumbar disc and effects of its derangement on spine.Dr.Sushil vijay,
Citation preview
BIOMECHANICS OF LUMBAR DISC DERANGEMENTS & LUMBAR
SPINE INJURIES.
Dr. Sushil VijayPG Student, D.orthSantosh Medical college & Hospital, GZB
GOALS OF THIS PRESENTATION
Understand the functional anatomy of the spine especially lumbar spine
Understand the load bearing properties of lumbar structures
Understand the strain of traditional and back sparing exercises/movements on the spine
DISCUSSION POINTS :-
Basic Anatomy & Functional Units of the lumbar spine &
the biomechanics :-
Functional UnitsDifferent stresses on the lumbar discApplied BiomechanicsBiomechanics of Lumbar spine MovementsBiomechanics of lumbar spine InjuriesBiomechanics of lumbar disc degenerationProphylaxis
The spinal column
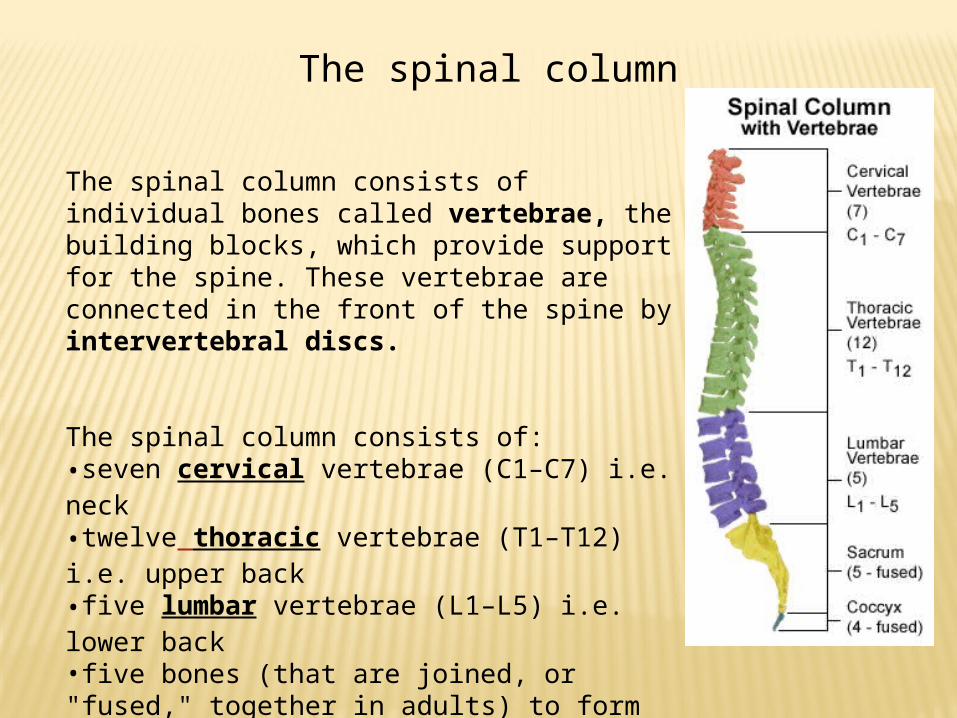
The spinal column consists of individual bones called vertebrae, the building blocks, which provide support for the spine. These vertebrae are connected in the front of the spine by intervertebral discs.
The spinal column consists of:•seven cervical vertebrae (C1–C7) i.e. neck•twelve thoracic vertebrae (T1–T12) i.e. upper back•five lumbar vertebrae (L1–L5) i.e. lower back•five bones (that are joined, or "fused," together in adults) to form the bony sacrum • three to five bones fused together to form the coccyx or tailbone
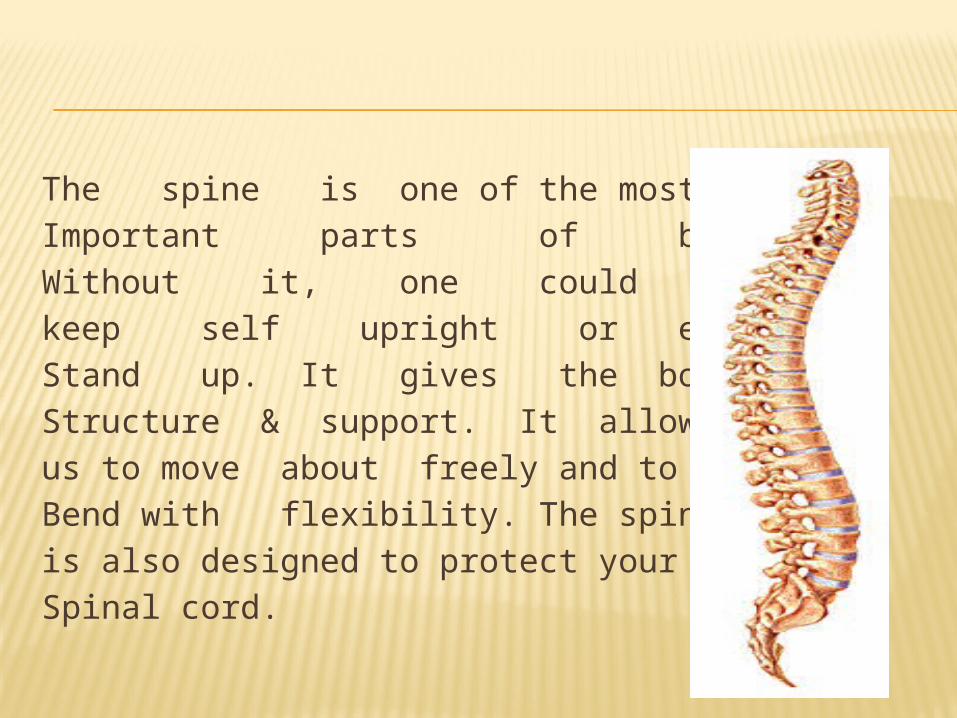
The spine is one of the most Important parts of body. Without it, one could not keep self upright or even Stand up. It gives the body Structure & support. It allowsus to move about freely and to Bend with flexibility. The spineis also designed to protect yourSpinal cord.
THE VERTEBRAL COLUMN
Great Strength Size and architecture
of bones Strong ligaments Powerful, enduring
muscles Strength combined
with great flexibility Many joints close
together Joints allow
movement in two or more planes
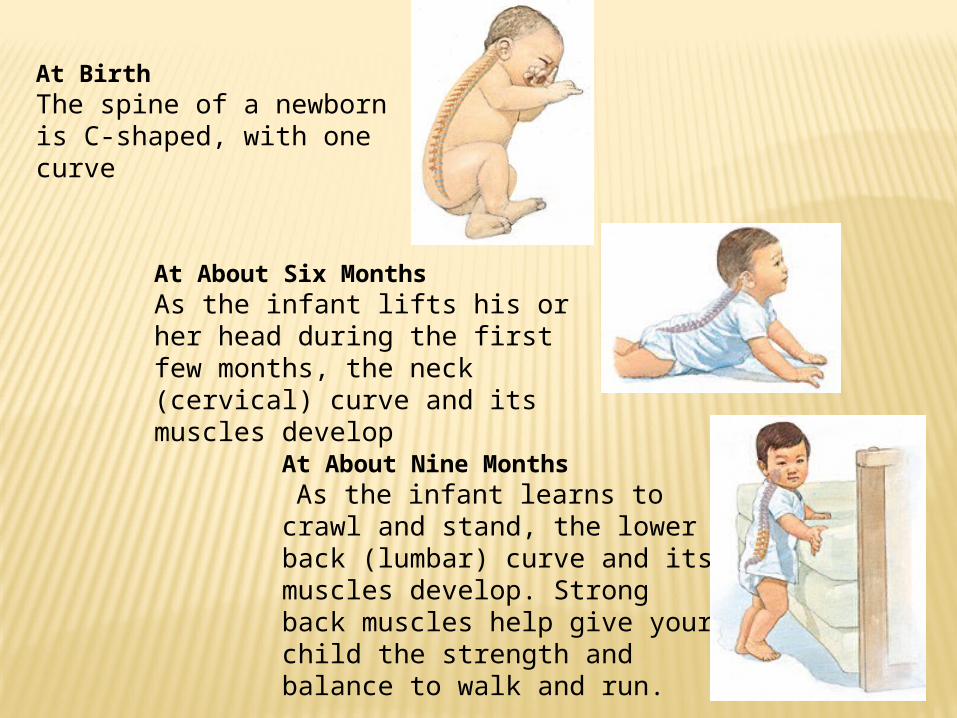
At BirthThe spine of a newborn is C-shaped, with one curve
At About Six MonthsAs the infant lifts his or her head during the first few months, the neck (cervical) curve and its muscles develop
At About Nine Months As the infant learns to crawl and stand, the lower back (lumbar) curve and its muscles develop. Strong back muscles help give your child the strength and balance to walk and run.
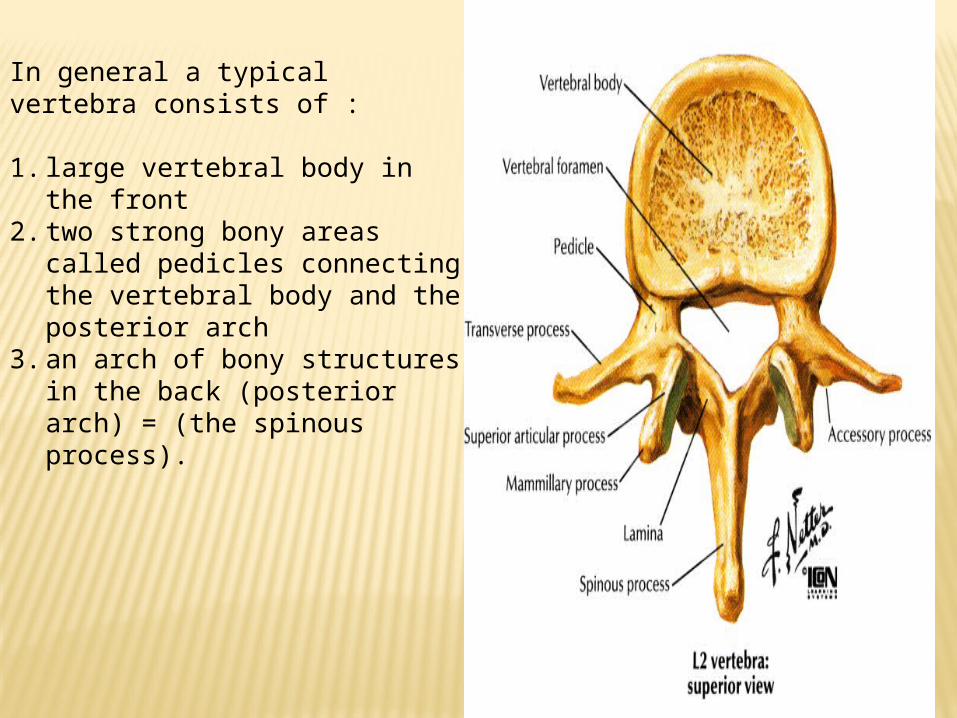
In general a typical vertebra consists of :
1. large vertebral body in the front
2. two strong bony areas called pedicles connecting the vertebral body and the posterior arch
3. an arch of bony structures in the back (posterior arch) = (the spinous process).
FUNCTIONAL UNITS OF SPINE
The functional unit is composed of three segments:
Anterior segment containing two adjacent vertebral bodies, one superincumbent upon the other, separated by an intervertebral disc,
Middle segment containing pedicle and IV foramen and
Posterior neural elements segment.
FUNCTIONAL UNITS
AnteriorMiddlePosterior
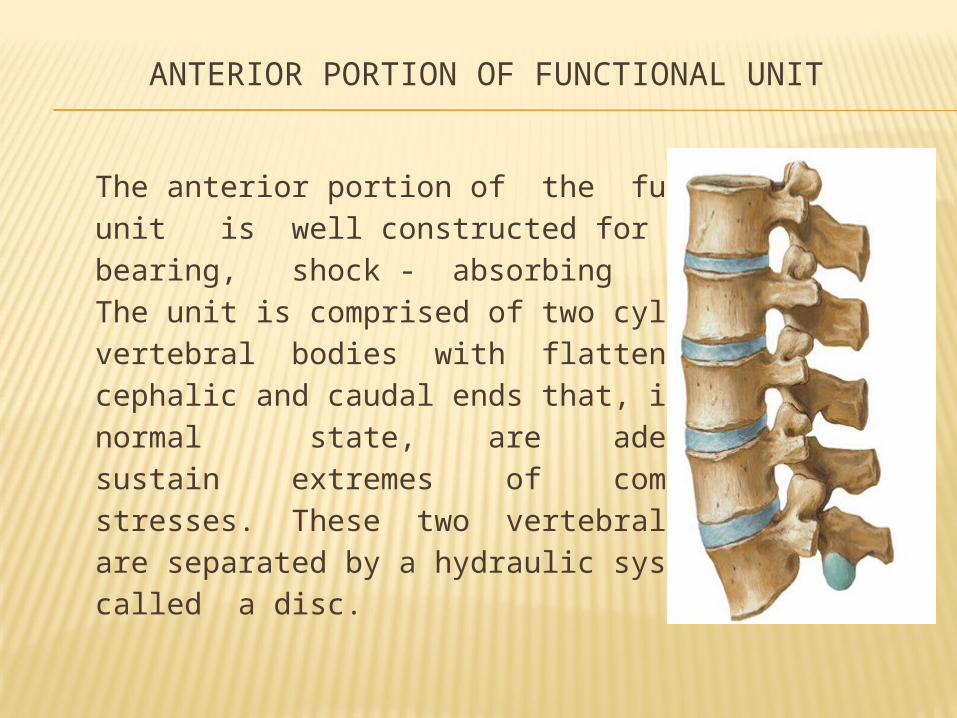
ANTERIOR PORTION OF FUNCTIONAL UNIT
The anterior portion of the functional unit is well constructed for its weight- bearing, shock - absorbing function. The unit is comprised of two cylindrical vertebral bodies with flattened cephalic and caudal ends that, in their normal state, are adequate to sustain extremes of compressive stresses. These two vertebral bodies are separated by a hydraulic system called a disc.
INTERVERTEBRAL DISC
Anatomical considerations
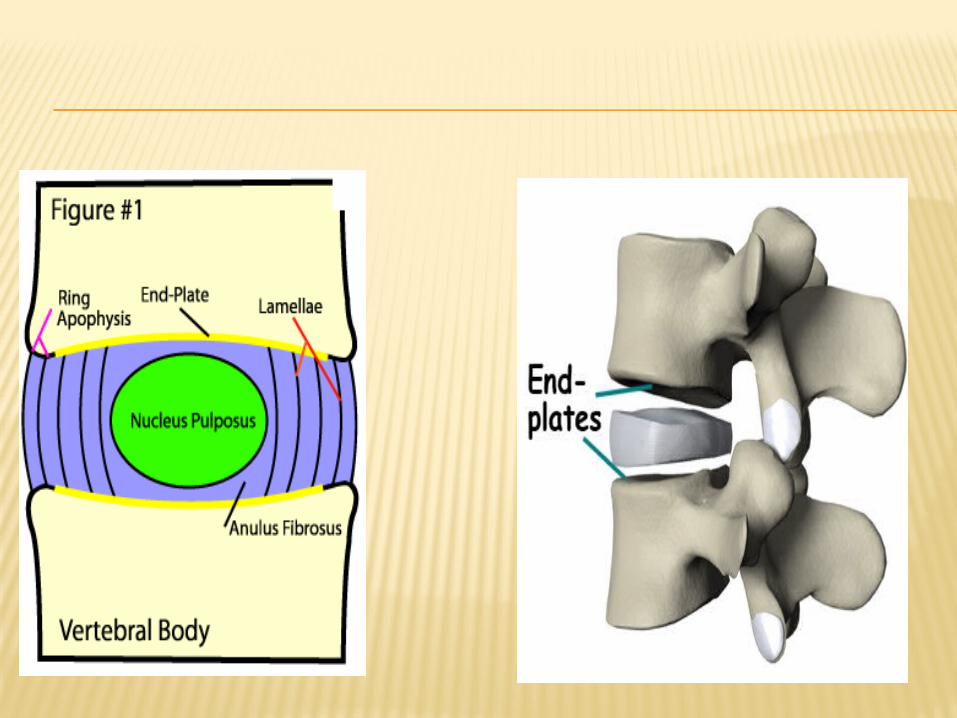
The disc is made up of inner gelatinous nucleus pulpous and outer fibrous casing -- annulus fibrosus.
The disc is a self-contained fluid system that absorbs shock, permits transient compression, and, owing to fluid displacement within an elastic container, allows movement. It is quite evident then that the disc is a mechanical "shock absorber.“
The upper and the lower plates of the disc are the end plates of the vertebral bodies. These plates are articular hyaline cartilage in direct contact and adherent to the underlying resilient bone of the vertebral body. In their normal state these end plates are firm, flat, circular, inflexible surfaces that form the cephalad and caudal portions of the disc and to which is attached the encircling annulus fibrosus.
NUCLEUS PULPOSUS
The nucleus pulposus is a colloidal gel, a muco polysaccharide that has a physical-chemical action. In a "young" and in an undamaged disc the nucleus is 88 percent water. Due to its colloidal chemical nature it can imbibe external fluids and maintain its intrinsic fluid balance.
Diffusion of solutes occurs via the central portion of the end plates and through the annulus.
Increased intradiscal pressure probably also forces fluid through minute foramina in the end plates. When pressure is released or decreased, fluid returns into the disc by imbibition. As the nucleus ages, it loses its water-binding capacity and looses its expansion capability.
During first two decades the nucleus water content decreases from its early 88 percent because its water-binding capacity has been decreased. In the aging process there is a decrease in the protein polysaccharide with an additional loss of osmotic and imbibition properties.
The intervertebral disc has a vascular supply that disappears after the second decade. By the third decade the disc, now avascular, receives its nutrition by diffusion of lymph through the vertebral end plates and by virtue of the physical-chemical imbibitory characteristics of the nucleus colloidal gel. The ability of an injured disc to regain its elasticity is bound to be stronger in the young. Resistance to stress by the vertebral column is further augmented by the vertebral ligaments. The ligaments run longitudinally along the vertebral column and by their attachments restrict excessive movement of the unit in any direction and prevent any significant shearing action.
The ligaments, by their position and attachments, encase the disc and reinforce the annulus yet do not detract from its physiologic elasticity. Viewed at the level of the functional unit, the entire disc is enclosed anteriorly by the anterior longitudinal ligament and posteriorly by the posterior longitudinal ligament

NUCLEUS PULPOSUS
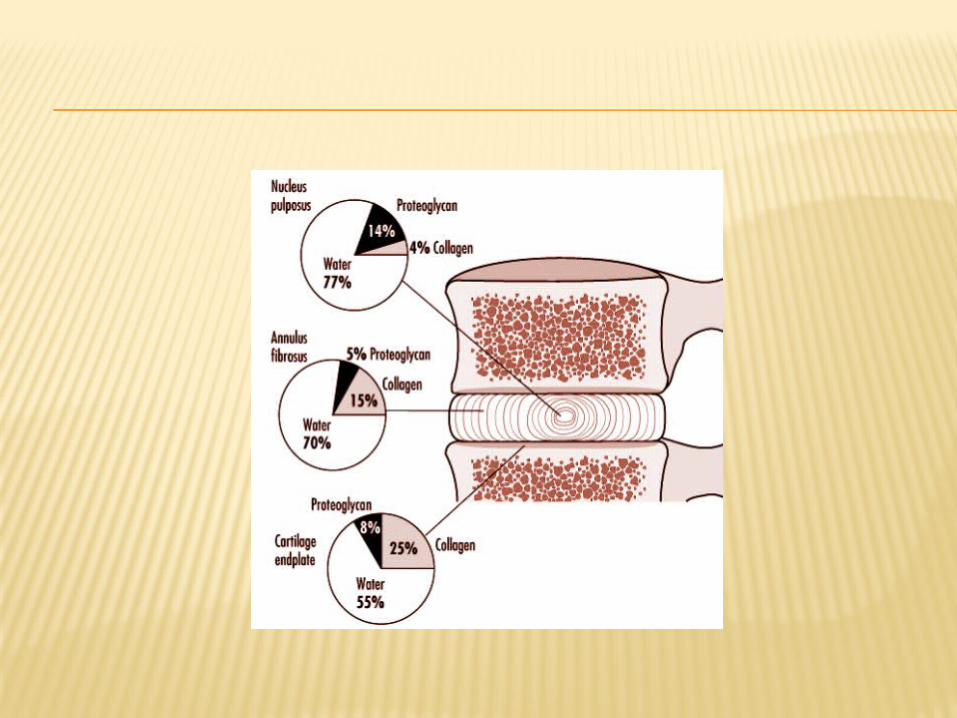
The nucleus pulposus consists of a gelatinous mucoprotein and mucopolysaccharide structure located posteriorly in the lumbar part of the spine, between the cartilaginous end-plates, and is surrounded by the annulus fibrosis.
The polysaccharides give the nucleus a water-imbibing ability. The water content within the nucleus ranges from 85 to 90 percent of the total nucleus at birth to 70 percent in later years
ABOUT PRESSURE AT NUCLEUS PULPOSUS Pressure within the center of the
normal nucleus is never zero, because of a pre existing tension even when the disk is unloaded. This characteristic is known as preload. The preload mechanism in the nucleus allows greater resistance to applied forces.
MOVEMENTS OF NUCLEUS PULPOSUS
Great controversy prevails about the amount of movement of the nucleus during spinal motions. A normally functioning disk is already located posteriorly in the lumbar part of the spine, so there will be a tendency for further posterior displacement with forward spinal movements. For example, spinal flexion would result in partial absorption and distribution of the load by the nucleus, with some backward displacement of the nucleus.
ANNULUS FIBROSUS
The annulus fibrosis is the laminated, fibrocartilaginous structure encapsulating the nucleus. In this structure, two sets of fibers cross obliquely to each other at about ±30 degrees in relation to the disk.
The annulus may be further divided into three layers, the peripheral portion being attached directly to the cortex of the vertebral body by Sharpey‘s fibers and the intermediate and inner portions being attached to the cartilaginous end-plates. Annulus fibers are thicker and more numerous anteriorly than posteriorly. The posterior and posterior lateral fibers have a more parallel alignment than do the anterior fibers. The posterior annulus fibers are also attached to the posterior longitudinal ligament, which is thinner in the lumbar region than in other spinal regions.
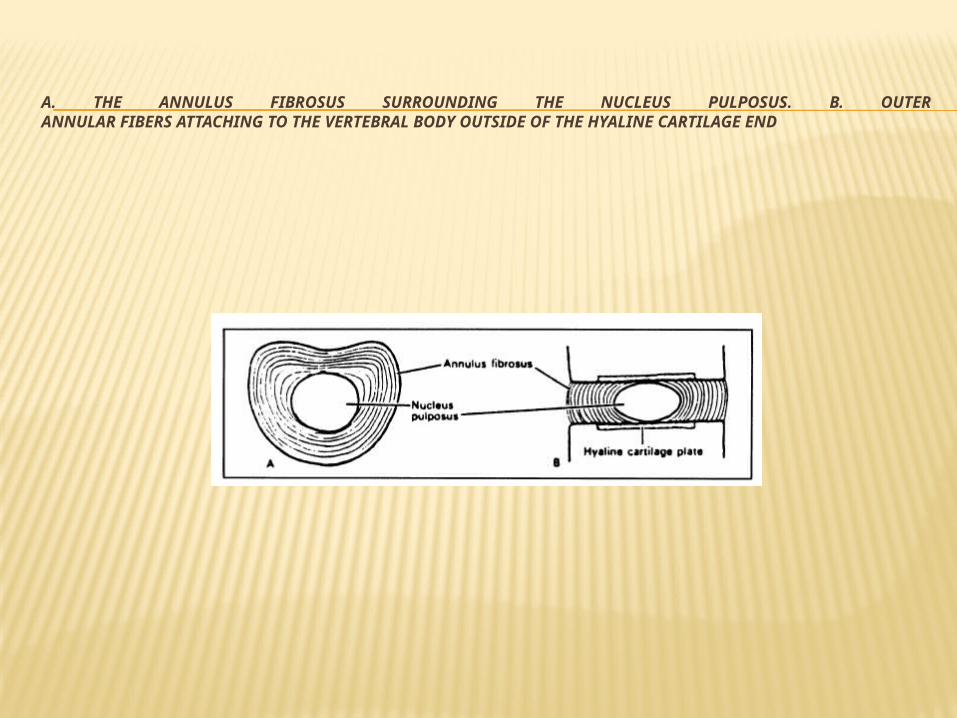
A. THE ANNULUS FIBROSUS SURROUNDING THE NUCLEUS PULPOSUS. B. OUTERANNULAR FIBERS ATTACHING TO THE VERTEBRAL BODY OUTSIDE OF THE HYALINE CARTILAGE END
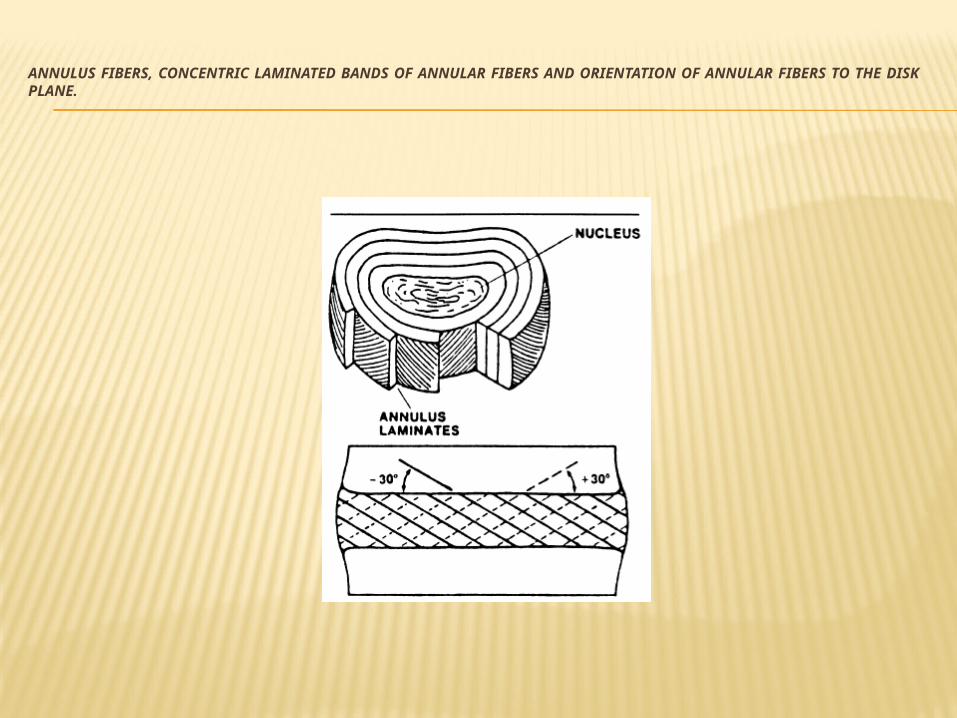
ANNULUS FIBERS, CONCENTRIC LAMINATED BANDS OF ANNULAR FIBERS AND ORIENTATION OF ANNULAR FIBERS TO THE DISKPLANE.
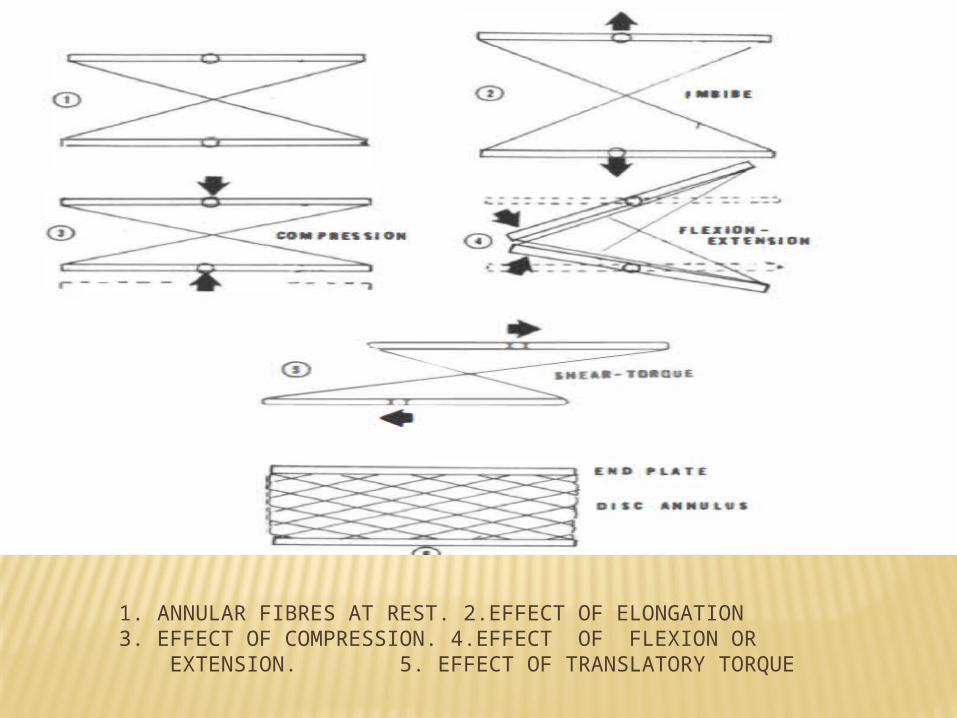
1. ANNULAR FIBRES AT REST. 2.EFFECT OF ELONGATION3. EFFECT OF COMPRESSION. 4.EFFECT OF FLEXION OR EXTENSION. 5. EFFECT OF TRANSLATORY TORQUE
END PLATES
The disk is separated from adjacent vertebral bodies by articular hyaline cartilage or cartilage endplates.
After the age of eight, the cartilaginous end-plates lose their blood supply, leaving holes from the blood vessels. These holes allow for the diffusion of metabolites but cause structural weakness.
Thus, the lumbar disk has some inherent structural features predisposing it to possible mechanical malfunction such as the parallel arrangement of the posterior annulus fibers, the posterior location of the nucleus, the thickness of the posterior fibers, and the holes in the cartilaginous end-plates.
PROPERTIES OF IV DISC
A normal intervertebral disk is an anisotropic structure, with a self-limiting elastic container, capable of absorbing shock and allowing movement.
The anisotropic property means the disk demonstrates mechanical properties that vary with spatial orientation and that allow the disk both elasticity and stiffness. The annulus functions as a fibroelastic mesh surrounding a colloidal gel, the nucleus.
The fibroelastic mesh not only retains the nucleus and provides the disk with hydraulic properties but gives resistance to tensile forces as well. As long as the nucleus remains well hydrated and the annulus fibers are well nourished and not damaged, the disk will function normal.
HYDRAULIC MECANISM OF INTERVERTEBRAL DISC
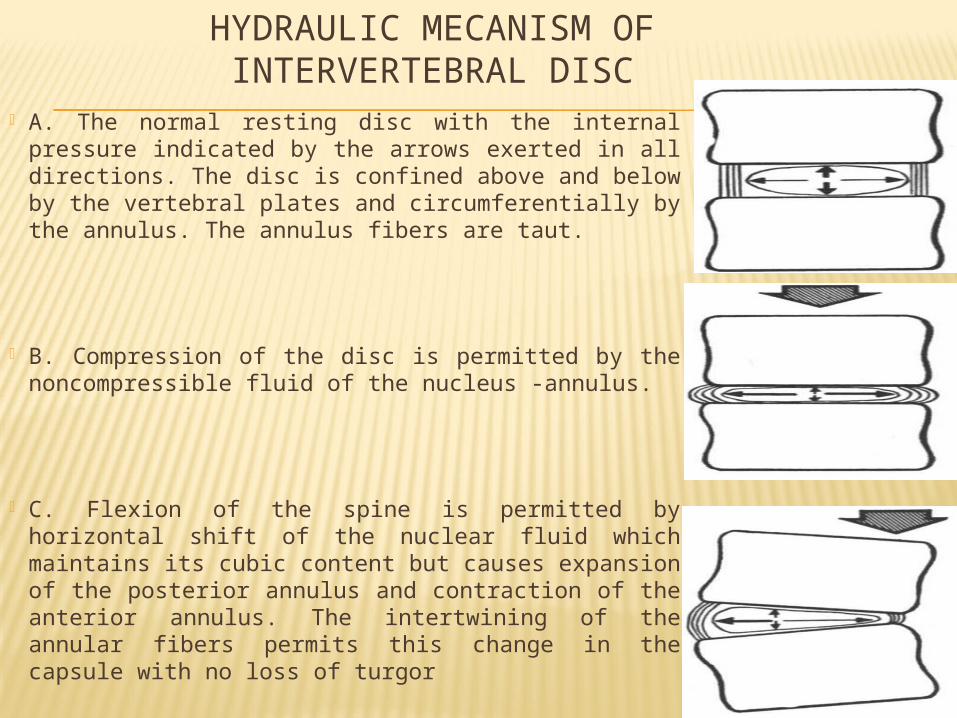
A. The normal resting disc with the internal pressure indicated by the arrows exerted in all directions. The disc is confined above and below by the vertebral plates and circumferentially by the annulus. The annulus fibers are taut.
B. Compression of the disc is permitted by the noncompressible fluid of the nucleus -annulus.
C. Flexion of the spine is permitted by horizontal shift of the nuclear fluid which maintains its cubic content but causes expansion of the posterior annulus and contraction of the anterior annulus. The intertwining of the annular fibers permits this change in the capsule with no loss of turgor
An abnormally functioning disk degenerates either through aging or trauma. The result is a loss of both hydraulic and elastic properties of the disk through
1. a decrease in the water content and therefore a lessening of the preload effect of the nucleus, 2. a decrease in the elastic collagen tissue in the annulus with replacement of large fibrous inelastic bands and 3.cartilage degeneration in the end-plates.
Traumatic incidents such as single high-level loads can also create ruptures in the annulus fibers. These ruptures are first seen at about the age of 25. Consistent softening of the posterior part of the annulus has been found as part of the aging process after the age of 45, with total annular lamellae disorganization by the age of 70-80 years.
POSTERIOR PORTION OF FUNCTIONAL UNIT
The posterior portion of the unit is composed of the two vertebral arches. two transverse processes, a central posterior spinous process, and paired articulations, inferior and superior, known as facets.
The processes of the posterior arch, the transverse and the posterior spinous, are the sites of muscular attachment. Because of the origin and insertion of muscles from one process to another, movement of the spine is possible. Because of the contractility and the elasticity of the muscles, a large range of motion is possible, and the manner of attachment and interspinous bridging provides balance of the static spine and strength for the kinetic spinal column. Maintenance of the erect posture is in part achieved by the sustained tonus of the muscles acting on these bony prominences. Motion and locomotion are also dependent on these muscles playing synchronously between their points of bony attachment.
The articulations, or facets, pilot the direction of movement between two adjacent vertebrae. By their directional planes they simultaneously prevent or restrict movement in a direction contrary to the planes of the articulation. They may be compared to the movement of wheels on railroad tracks in which forward and backward movement is possible but sideway movement is prevented.
The facets are arthrodial joints that function on a gliding basis. Lined with synovial tissue, they are separated by synovial fluid which is contained within an articular capsule. The plane of the facets, in their relation to the plane of the entire spine, determines the direction in which the two vertebrae will move. The direction, or plane, of the facets in any segment of the spine will determine the direction of movement permitted to that specific segment of the spine. The plane of the facets will simultaneously determine the direction of movement not permitted that spinal segment.
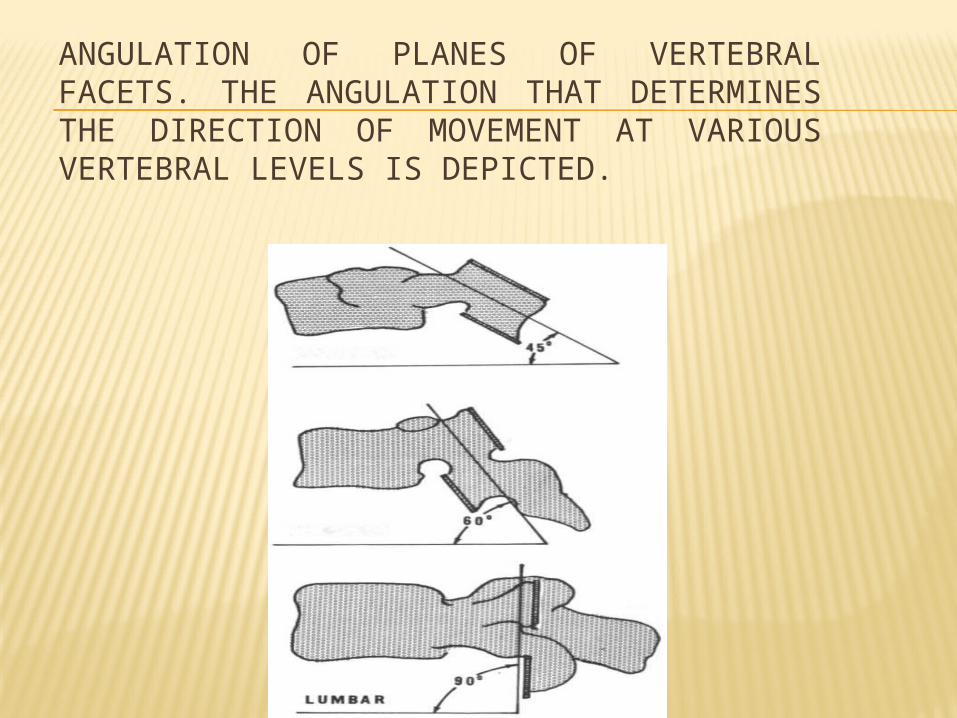
ANGULATION OF PLANES OF VERTEBRAL FACETS. THE ANGULATION THAT DETERMINES THE DIRECTION OF MOVEMENT AT VARIOUS VERTEBRAL LEVELS IS DEPICTED.
FACET JOINTS : MOVEMENT In the thoracic spine the facets are convex-concave and lie essentially
in a horizontal plane. Movement permitted by this facet plane in the thoracic spine is lateral flexion, such as side bending and rotation about a vertical line. A combined movement of lateral flexion and rotation occurs here, for, in spinal column movement, no pure lateral bending is possible without some rotation and no true rotation is possible without some lateral flexion. Due to this facet plane, no significant flexion or extension movement in an anterior posterior plane is possible in the adult thoracic-spine segment.
In brief, the direction of the facet plane that exists between two adjacent vertebrae in a functional unit determines the direction of movement of those two vertebrae. As the facets of the lumbar spine are vertical-sagittal in an anterior plane, movement of the lumbar spine exists in an anterior-posterior flexion-extension direction. The planes of the thoracic spine relegate to this segment all significant lateral flexion such as side bending and rotation of the total spine. All other
SPINE AS A TOTAL:-
The total vertebral column can now be visualized as the sum total of all the functional units, superimposed one upon the other, in an erect jointed column balanced against gravity and capable of movement.
All three curves--the lumbar, the thoracic, and the cervical-in their ascent, must meet in a midline center of gravity to balance the weight distribution of the curve and to counter the eccentric loading of each curve. The side view of the three physiologic curves in the erect position may be considered as posture
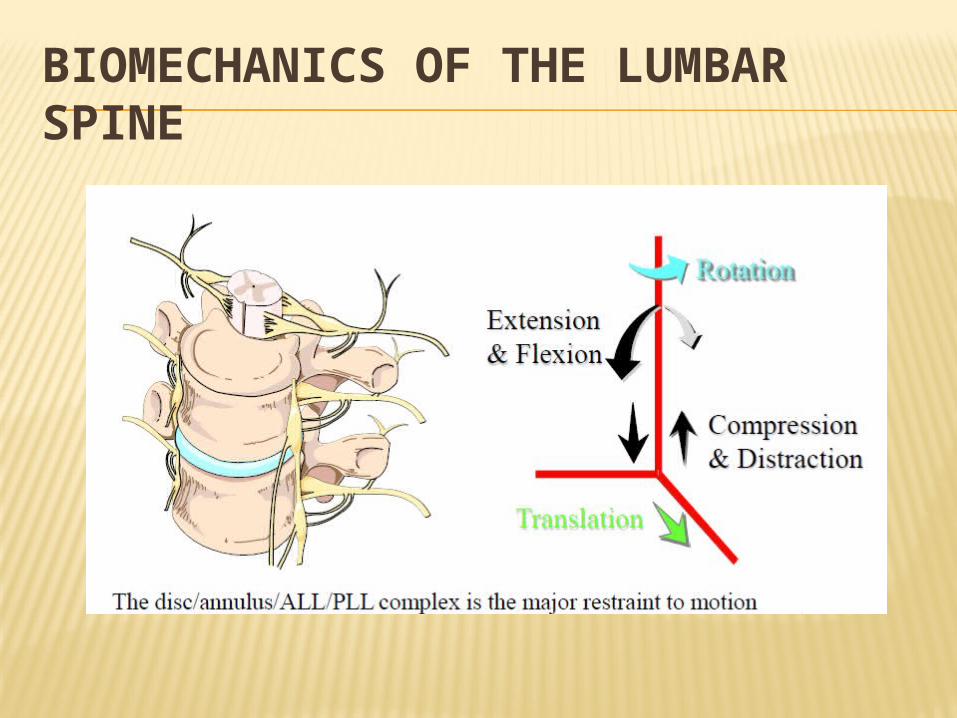
BIOMECHANICS OF THE LUMBAR SPINE
MECHANICS
The axis of thoracic & lumbar spinal motion is located in the disc, but the center of gravity is anterior to the vertebral body. Therefore, even with erect standing, a bending moment is generated in the spine that must be resisted by the intervertebral discs, spinal ligaments, and spinal extensor muscles. Greatest loads are seen in the lumbar region. The bending moment is markedly increased when an individual is lifting or carrying an object in front of the body. Flexion and torsional movement also greatly increase pressure in the lumbar disc.
BIOMECHANICS
Definition :- Mechanics, the study of forces and their effects
when applied to humans, is called biomechanics. It is difficult, however, to begin to apply biomechanical principles to clinical situations without understanding the terminology involved. For example, what is meant by load, strain, stress, and shear and how do they relate to tension, compression, bending, and torsion!
- Load is a general term describing the application of a force to a structure. A load results in a distribution of stresses and strains in a structure.
- Strain is defined as the physical deformation of a structure, resulting in either a longitudinal strain (change in unit length) or an angular deformation.
- Stress is the internal force per unit area produced. A load can produce two types of stress, normal or shear. A normal stress is the force per unit area acting perpendicular to the area, and shear stress is the force per unit area acting parallel to the considered area.
Mechanical stresses, unlike strains, are not measurable in any structure; therefore, mechanical stresses are measured by comparing the strain to the load, where the strain is measured by assuming it to be proportional to the load.
The ratio of change in stress to change in strain (in the direction of the load) identifies the elastic modulus of a structure commonly known as Young's modulus.
Materials with a large elastic modulus are considered stiff and require greater stresses to produce a given strain than do materials that are less stiff. For example, steel has a larger elastic modulus than rubber. The result of the same stress on each results in a large strain in the rubber and a small strain in the steel.`
Tension and compression are both normal stress. Tension represents collinear forces, acting in opposite directions, which tend to separate; compression represents colinear forces, which tend to push together.
Tension differs from compression only in the direction in which the load is applied.
Loads may be applied either directly, through a single axis of a structure, resulting in either compression or tension stress, or indirectly. When a force is applied indirectly, at an angle to the axis of a structure,a multiaxial situation results, producing a bending or torsion stress.The load on the structure applied
in a multiaxial situation is called torque and results in torsion from the application of twisting or rotating movements. In a straight structure, all areas experience the same torque; however, in a curved structure, because the load is applied at a point away from the neutral axis and not directly supported, the result is both torque and bending.The vertebral column is a structure that supports a load. In the spine, an externally applied load produces stresses and strains of the vertebral body or disk, or both. The vertebral body, composed of a stiffer material, has a greater elastic modulus than does the disk. Therefore, strains can be produced much more easily in the disk, which in turn must distribute the resultant forces.
Compression &
Tension Stresses on the IV Disk
NORMAL LUMBAR DISK
In the normal lumbar disk, it is not herniation that is seen with high compressive loads, but failure of the vertebral body, resulting in collapsed cartilaginous end-plates. This type of collapsing demonstrates that, with direct, single axis compressive loading, as opposed to indirect or multiaxial loading, a spine with normal intervertebral disks is relatively strong. In the normal disk, a compressive load increases the internal pressure of the disk and stretches the annulus fibers. The resultant stresses are directed radially to the end-plates and annulus. The inner layers of the annulus are subjected to a small compressive stress, which is transferred to other vertebrae by the fluid pressures of the nucleus. The outer annulus layers are subjected to tensile stress without transference. However, because of their alignment, the outer layers of annulus fibers are capable of absorbing the tensile stress. The magnitude of tensile stresses depends on the thickness of the annulus fibers. Thetensile stresses on the thinner, more parallel posterior fibers of the lumbar part of the spine are four to five times as great as the applied load.
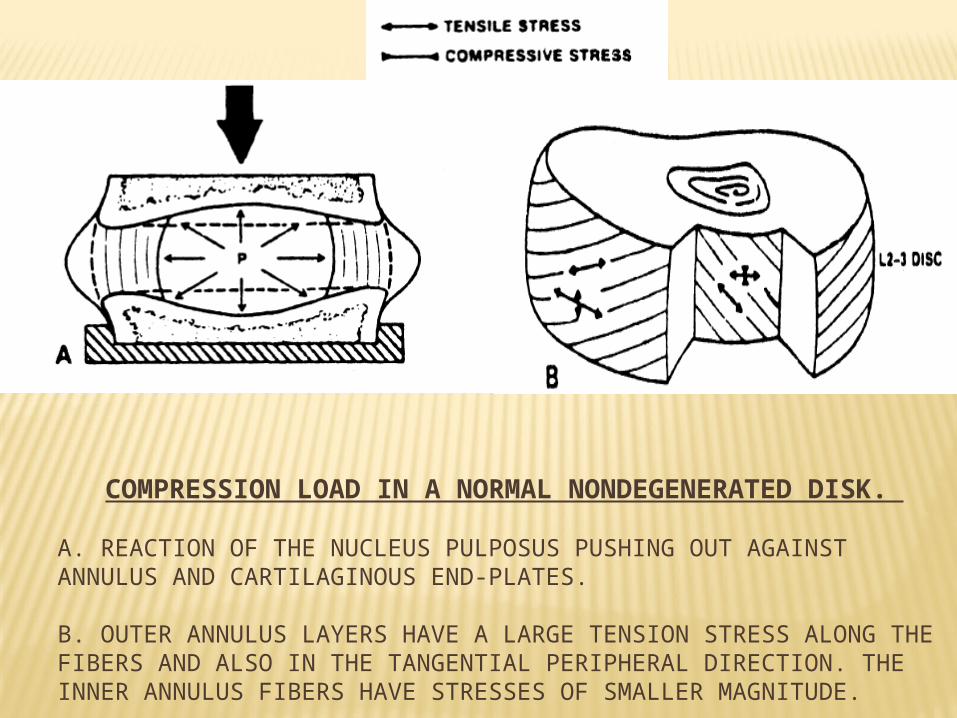
COMPRESSION LOAD IN A NORMAL NONDEGENERATED DISK.
A. REACTION OF THE NUCLEUS PULPOSUS PUSHING OUT AGAINST ANNULUS AND CARTILAGINOUS END-PLATES.
B. OUTER ANNULUS LAYERS HAVE A LARGE TENSION STRESS ALONG THE FIBERS AND ALSO IN THE TANGENTIAL PERIPHERAL DIRECTION. THE INNER ANNULUS FIBERS HAVE STRESSES OF SMALLER MAGNITUDE.
IN DEGENERATED LUMBAR DISK
Under the same compressive load, the nucleus of a degenerated disk will not absorb some of the stress and transfer the remainder to the annulus and end-plates; instead, the increased load is distributed to the annulus.
Under these circumstances the outer annulus fibers receive a large tensile stress without the fiber mechanism to absorb the stress or the hydrostatic nucleus to distribute the forces radially.
Consequently, the inner fibers receive a large compressive stress. Nachemson measured pressures in the nucleus pulposus of moderately degenerated disks and found these pressures to be 30 percent lower than pressure in a normal disk. This decreased pressure further causes a significant increase in the vertical load placed on the annulus in a degenerated disk
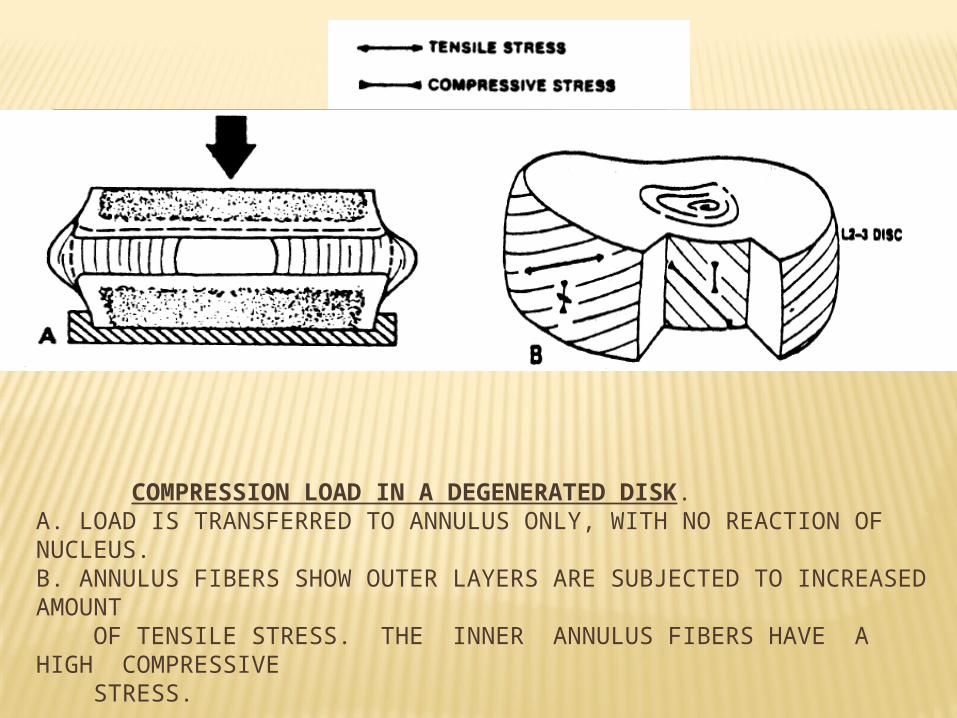
COMPRESSION LOAD IN A DEGENERATED DISK. A. LOAD IS TRANSFERRED TO ANNULUS ONLY, WITH NO REACTION OF NUCLEUS.B. ANNULUS FIBERS SHOW OUTER LAYERS ARE SUBJECTED TO INCREASED AMOUNT OF TENSILE STRESS. THE INNER ANNULUS FIBERS HAVE A HIGH COMPRESSIVE STRESS.
BENDING AND TORSION STRESSES
Functional movement in the vertebral column is a combination of direct and indirect loading. In the spine the stresses most likely to produce trauma are bending and torsion, which reflect the combinations of shear, compression, and tension forces.
Bending involves simultaneous tension, compression, and some shear stresses at different locations in the disk. Bending in forward flexion, lateral flexion, or extension of the spine results in a tensile stress on the convex side of the annulus and a compressive stress, caused by the body weight, on the concave side. The side of the annulus under tension stretches, while the side under compression bulges. Whenundergoing bending, a structure will have maximum stress at the outer surface. In the vertebral column this means the outer peripheral surfaces of the annulus will be subjected to the highest tensile stresses on the convex side and the highest compressive stresses on the concave side
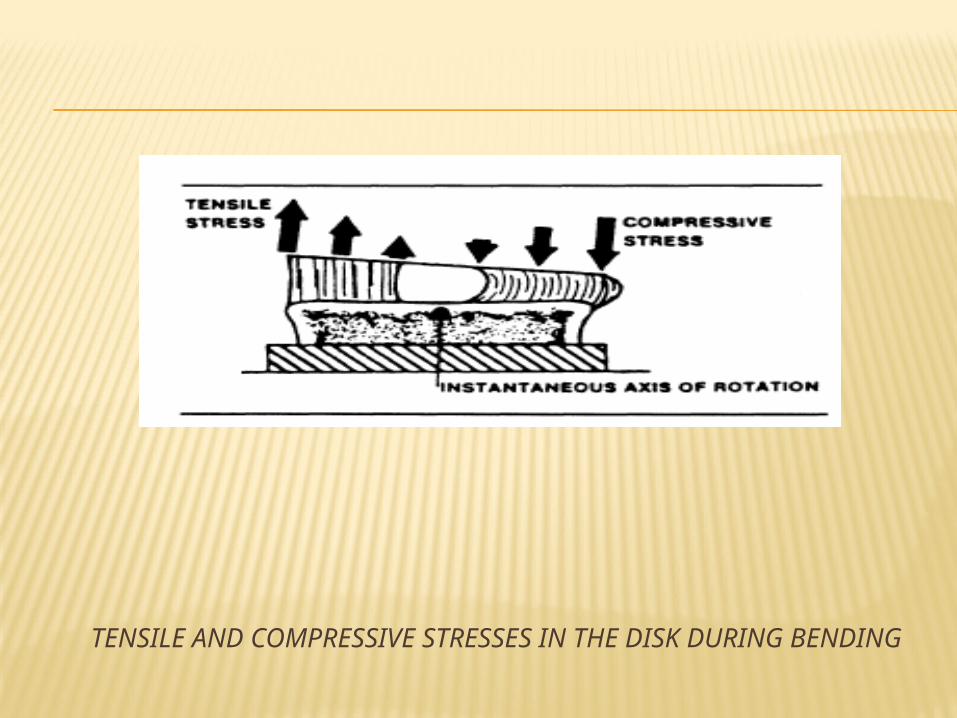
TENSILE AND COMPRESSIVE STRESSES IN THE DISK DURING BENDING
Torsion stress in the spine comes from twisting or rotating on the long axis.
The motion of one vertebra on another produces both tensile and shear stresses in the annulus. The shear stresses take place in the horizontal plane about the rotational axis. Because the annulus fibers cross at oblique angles to the horizontal plane, torsion results in tensile stresses in the fibers resisting rotation.
Shear stresses, however, also exist perpendicular to the annulus fiber direction. Because the bond between parallel fibers is relatively weak, these shear stresses may cause failure in the annulus.
The peripheral surface structures are subjected to the largest stresses and subsequently develop the greatest strains. The magnitude of the strain is proportional to the distance from the peripheral annulus to the axis of rotation. In the disk, this stress is maximal at the posterolateral angles of the annulus where there is already structural weakness
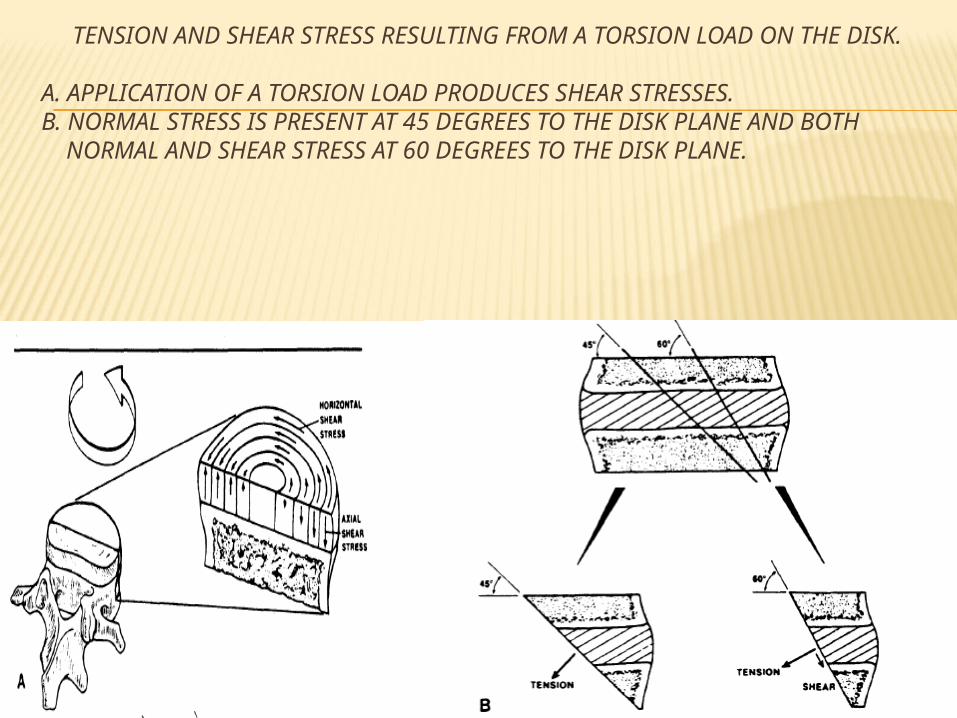
TENSION AND SHEAR STRESS RESULTING FROM A TORSION LOAD ON THE DISK.
A. APPLICATION OF A TORSION LOAD PRODUCES SHEAR STRESSES. B. NORMAL STRESS IS PRESENT AT 45 DEGREES TO THE DISK PLANE AND BOTH NORMAL AND SHEAR STRESS AT 60 DEGREES TO THE DISK PLANE.
Thus, combinations of movements such as twisting, bending, and bending with rotation will result in increased stresses and strains on the disk, especially with a superimposed load. These stresses alone can account for disk injury; in the presence of any disk degeneration, the stresses are only magnified.
How then do these biomechanical principles relate to normal daily activities in the patient with disk pathology?
LUMBAR DISK : APPLIED BIOMECHANICS
Applied biomechanics in relation to Posture Work, & Exercise
POSTURE
Usually a patients comes with a complaint of pain brought on by sitting and relieved by lying supine is a frequent complaint from a patient with a disk problem.
A series of studies was done and it was shown that two top risk factors for a herniated lumbar disc are sedentary occupation and driving motor vehicle, followed by lifting, bending or prolonged standing or sitting.
In Subjects who used to alternatively sat and stood incidence was low.
The intradiscal pressures of the third lumbar disk documented the high disk loads in sitting.
The disk pressures during unsupported sitting were one-third greater than during standing and were directly related to the body weight above the level of the disk measured.
Leaning forward 20 degrees increases the load or pressure 30 percent, and lifting a 20-kg (44.1-lb) load in this position increases the load or pressure 100 percent, with a 40 percent increase in tensile stress on the posterior aspect of the annulus
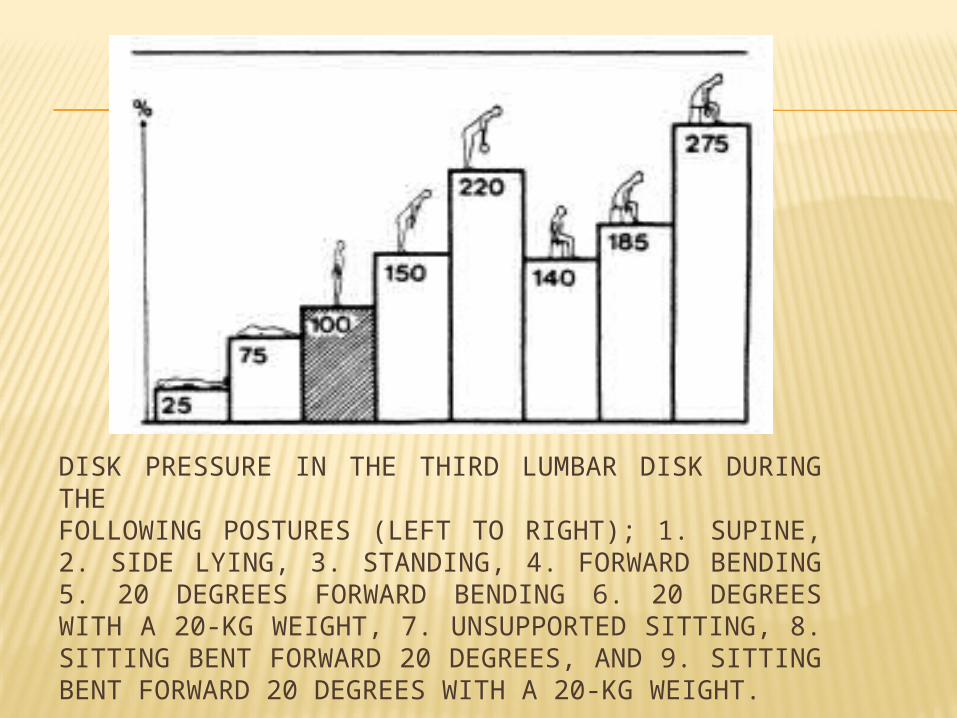
DISK PRESSURE IN THE THIRD LUMBAR DISK DURING THEFOLLOWING POSTURES (LEFT TO RIGHT); 1. SUPINE, 2. SIDE LYING, 3. STANDING, 4. FORWARD BENDING 5. 20 DEGREES FORWARD BENDING 6. 20 DEGREES WITH A 20-KG WEIGHT, 7. UNSUPPORTED SITTING, 8. SITTING BENT FORWARD 20 DEGREES, AND 9. SITTING BENT FORWARD 20 DEGREES WITH A 20-KG WEIGHT.
It has been studied that pressure in a normal disk measures only one-half of the externally applied load, but that the pressure in a moderately degenerated disk is equal to the full external load
The intradiscal pressure is distinctly lower in the standing position than in the sitting position. The decreased EMG activity in the psoas major muscle during standing indicates that this muscle may be responsible for this decreased intradiskal pressure. In the sitting position, however, the psoas muscle stabilizes and compresses the lumbar part of the spine, thus increasing the intradiskal pressure. The intradiskal load may be further decreased while in standing by flexing one hip and resting the foot of the flexed leg on a surface elevated about 6 to 12 inches. The slight elevation of the foot reduces the load even more by decreasing the tension on the psoas muscle. The least heavy loads were found in the lumbar part of the spine in the supine position (25 kg/cm2) or in the semi-Fowler's position with hips and knees flexed (35 kg/cm2
LOWEST LOAD ON LUMBAR SPINE
In a study the lowest load in sitting was found to be with a backrest inclination of 120 degrees and a lumbar support 5 cm (2 in) in depth. This position gave both the lowest electromyographic reading for back muscles and the lowest intradiskal pressures.
Intradiskal pressure further decreased when a subject sat in a chair providing arm and thigh supports and adequate space to change positions.
The highest disk pressures were found when chairs with no lumbar support and a 90-degree inclination (straight back) were used. In this rightangled sitting position, the pelvis rotates and causes obliteration of the lumbosacral curve.
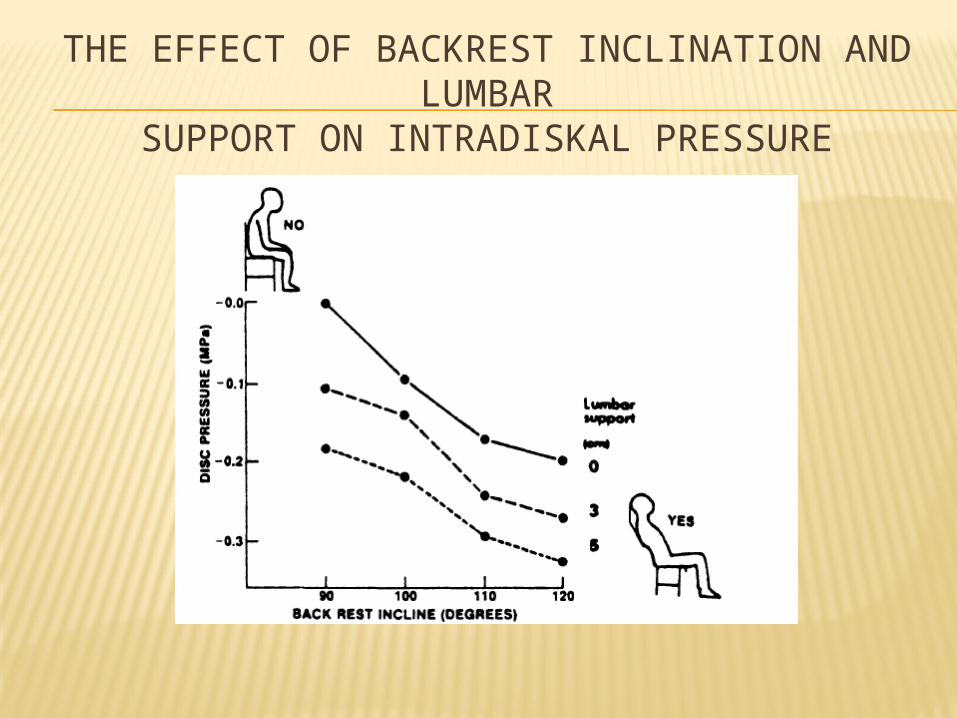
THE EFFECT OF BACKREST INCLINATION AND LUMBAR
SUPPORT ON INTRADISKAL PRESSURE
WORK
The onset of low back pain is often attributed to heavy work involving static loading positions combined with lifting in the forward stooping position.
Lifting while stooping increased the disk pressure by two-thirds and caused a tensile stress on the posterior annulus close to a rupturing force (100 kg/cm2) of the annulus.
The disk pressure increase was related more to the distance the load was held from the body than from lifting with a bent back in a stooped position versus lifting with a straight back in a crouched position. Another factor to consider in lifting in the stooped position is the complete obliteration of the lumbosacral curve, resulting in hydraulic pressure directed posteriorly at the disk
PUSHING VS PULLING :-
A load held at a distance from the body results in a larger bending moment and consequently produces a greater shear stress on the spine. Lifting at a distance from the body requires greater muscle force and therefore increases intradiskal pressures and the reactions of the spinal joint. The same principle may also be applied to pushing and pulling an object. Pushing an object generates a smaller load on the disk because the rectus abdominis muscle, with a large lever arm, counterbalances the moment arm. When an object is pulled, the erector spinae muscles work with a short lever arm in order to resist the bending moment, thereby generating a greater load.
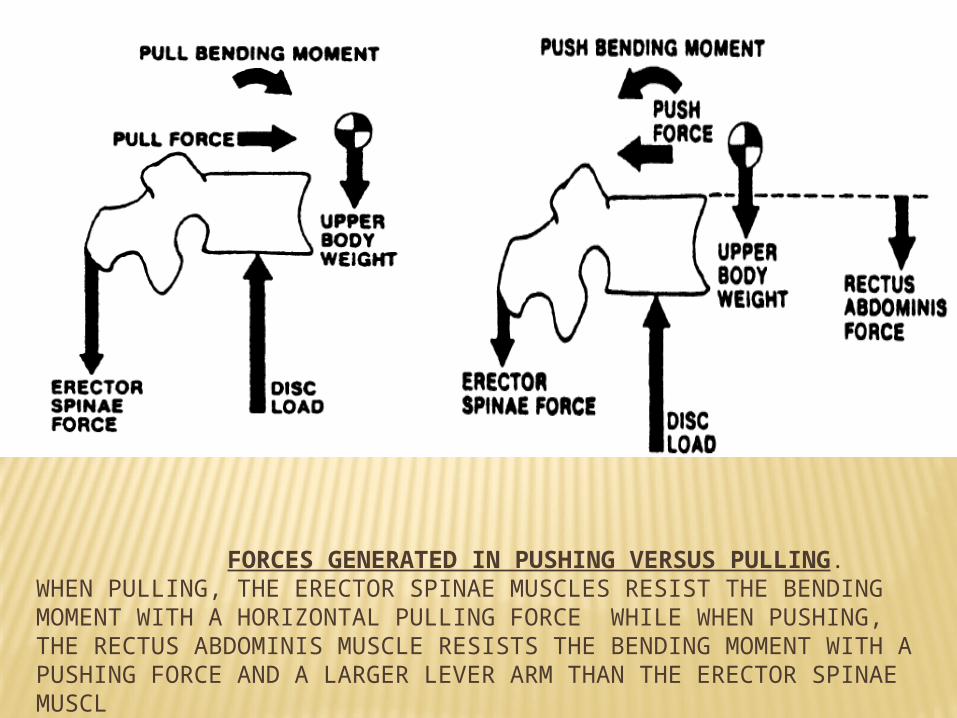
FORCES GENERATED IN PUSHING VERSUS PULLING. WHEN PULLING, THE ERECTOR SPINAE MUSCLES RESIST THE BENDING MOMENT WITH A HORIZONTAL PULLING FORCE WHILE WHEN PUSHING, THE RECTUS ABDOMINIS MUSCLE RESISTS THE BENDING MOMENT WITH A PUSHING FORCE AND A LARGER LEVER ARM THAN THE ERECTOR SPINAE MUSCL
LIFTING WEIGHTS FROM GROUND
Three methods of lifting from the squat position: 1) with both knees up off the ground, 2) with both knees down on the ground, and 3) in an oblique position with one knee off and one knee on the ground. The lift done with both knees down on the ground produced less spinal stress than the other two. However, toward the end of the lift with both knees down, the trunk was well forward of the knees and in an unstable posture.

The oblique lift with one knee down and one up seemed to be a compromise between the other two positions, with early spinal stress and a more stable posture for progressing to the upright position. Also, an analysis of the speed of the lift demonstrated that a slow lift produced less intradiskal pressure than did a fast lift.
EFFECT OF ROTATION
Studies show that even three degrees of rotation can disrupt the annulus fibers at their weakest point, that is, where the fibers attach to the bone.
At 15 degrees of rotation, a total breakdown in the annulus occurs.
Disk alone receives 50 percent of the torque; the facets, which function to prevent torsion, receive the other 50 percent.
Therefore, a dangerous position for the spine is flexion, which opens the facet joints, followed by rotation, because the disk will not have the protection ordinarily provided by the facets.
EXERCISE
Most of us assume that exercise will make backs stronger and eliminate symptoms, yet there is no conclusive evidence that strong muscles protect the back from painful episodes.
When intradiskal pressures were recorded during various types of exercise, sit-ups with knees bent and active hyperextension exercises were found to produce the greatest disk pressures.
Because patients are safer biomechanically, lifting with their legs rather than their backs, exercises should focus on developing strong knee extensors, not back extensors.
Also, the ability of a patient to increase intraabdominal pressure through strong abdominal muscles will further decrease the intradiskal load and enhance lifting ability.
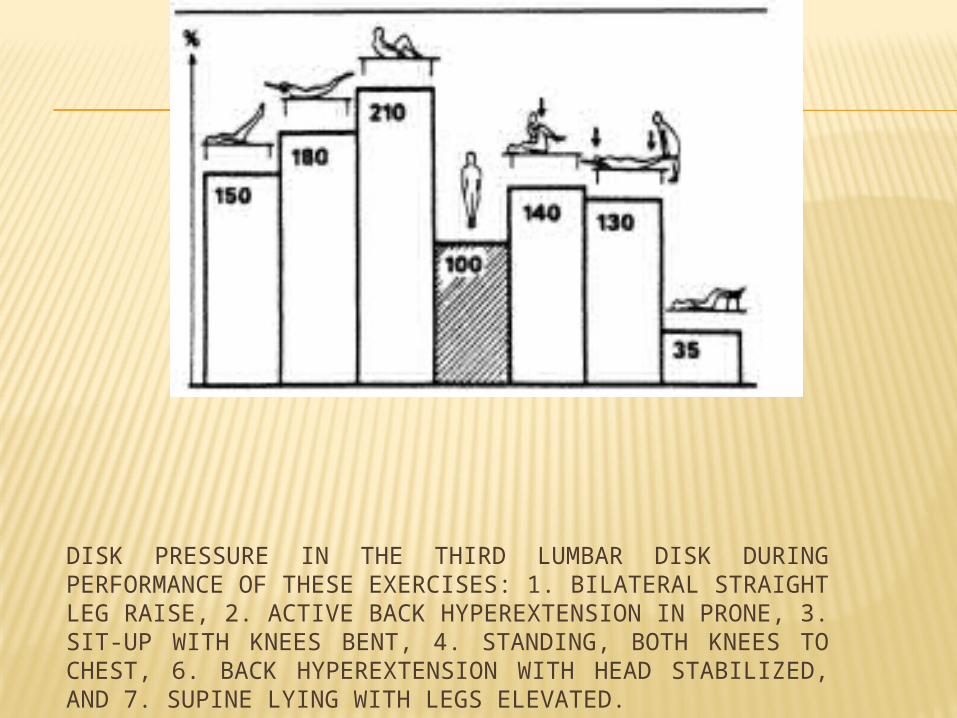
DISK PRESSURE IN THE THIRD LUMBAR DISK DURINGPERFORMANCE OF THESE EXERCISES: 1. BILATERAL STRAIGHT LEG RAISE, 2. ACTIVE BACK HYPEREXTENSION IN PRONE, 3. SIT-UP WITH KNEES BENT, 4. STANDING, BOTH KNEES TO CHEST, 6. BACK HYPEREXTENSION WITH HEAD STABILIZED, AND 7. SUPINE LYING WITH LEGS ELEVATED.
BIOMECHANICS OF MOVEMENTS OF LUMBAR SPINE
Flexion , extension, compression, axial rotation and lateral flexion are the main movements of lumbar spine.
IV Disc is the major load bearer in the lateral and posterior shear, axial compression and flexion.
Facet is the major load bearer in lumbar region in extension and flexion movement, anterior shear and axial torque which limits rotation and bending.
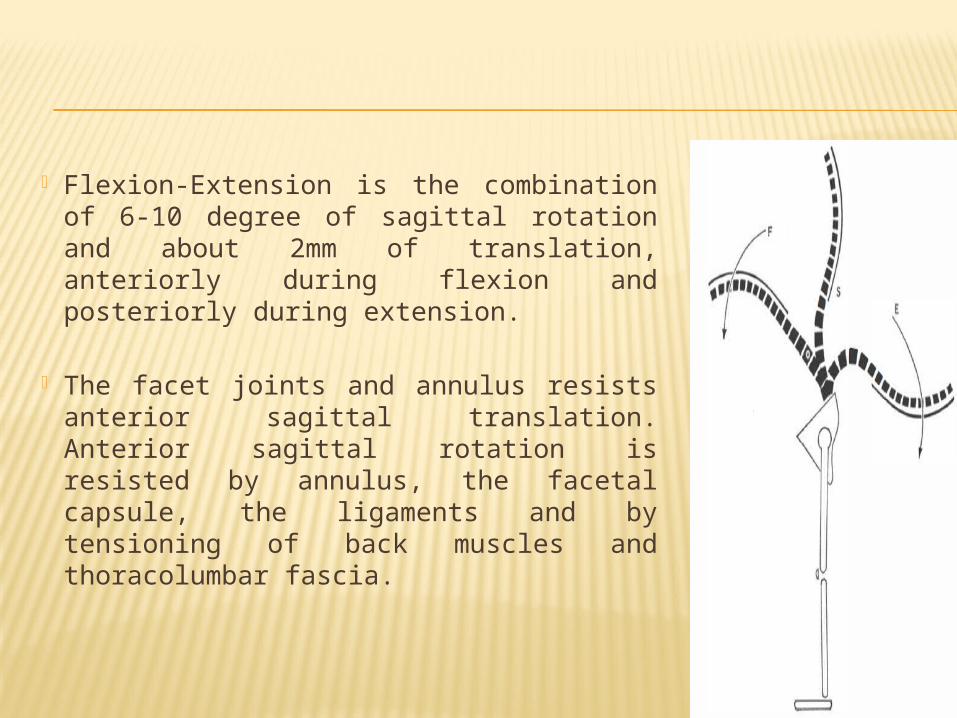
Flexion-Extension is the combination of 6-10 degree of sagittal rotation and about 2mm of translation, anteriorly during flexion and posteriorly during extension.
The facet joints and annulus resists anterior sagittal translation. Anterior sagittal rotation is resisted by annulus, the facetal capsule, the ligaments and by tensioning of back muscles and thoracolumbar fascia.
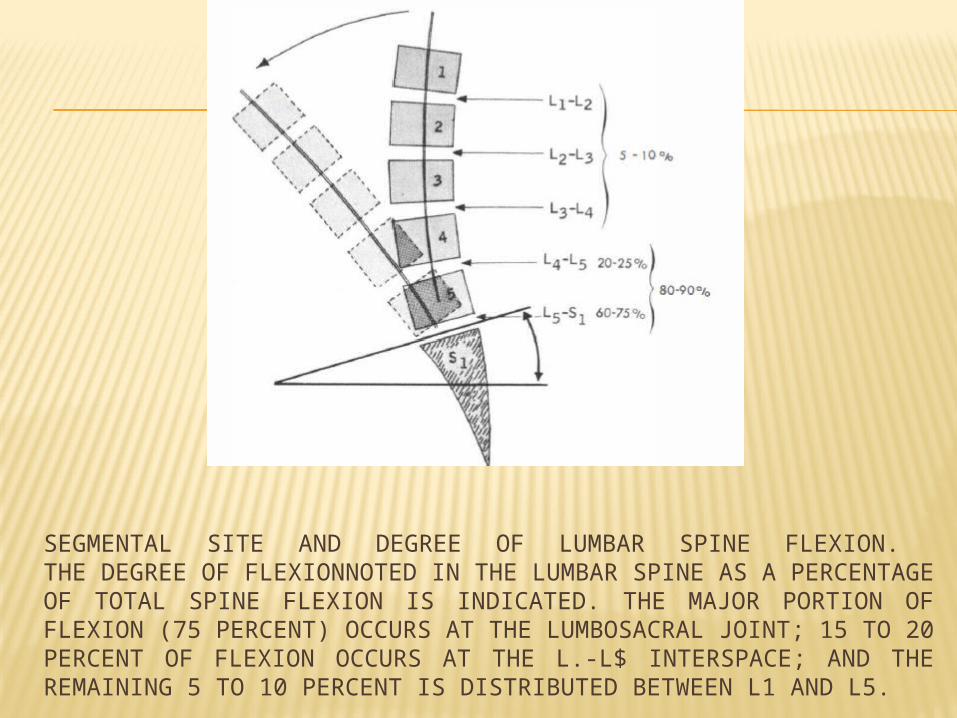
SEGMENTAL SITE AND DEGREE OF LUMBAR SPINE FLEXION. THE DEGREE OF FLEXIONNOTED IN THE LUMBAR SPINE AS A PERCENTAGE OF TOTAL SPINE FLEXION IS INDICATED. THE MAJOR PORTION OF FLEXION (75 PERCENT) OCCURS AT THE LUMBOSACRAL JOINT; 15 TO 20 PERCENT OF FLEXION OCCURS AT THE L.-L$ INTERSPACE; AND THE REMAINING 5 TO 10 PERCENT IS DISTRIBUTED BETWEEN L1 AND L5.
Compression load is largely exerted by back muscles. When a person bends forwards to lift a weight the back muscles behind the vertebrae balance the trunk weight and the weight of the object being lifted.
Studies have been performed and shown that to lift a 25 kg weight , the back muscles need 520 kg of compressive forces. About 10% compressive force is applied by the body.
Axial Rotation :- The lumbar spine does not have nay primary rotator. The axial rotation hence is directly imposed on the lumbar vertebrae and their joints. The thoracic rotation by the external and internal oblique muscles directly impose a rotatory action on the lumbar vertebrae causing on each segment a range of <3 degree.
Lateral Bending:- is a complex movement involving rotation of intervertebral joints and facet joints. Because of the complexity biomechanical analysis of this movement is lacking.
BIOMECHANICS OF LUMBAR SPINE INJURIES
1. Flexion in strict sagittal plane does not cause injury to the vertebrae before muscle injury. Muscle tears can lead to vertebral injury. Flexion prestresses the annulus fibrosus.
2. Extension :- Forceful hyperextension causes inferior articular facet to impinge like a chiesel on the lamina resulting in pars interarticularis fracture. If lamina is strong, there shall be a disruption of the facet joint capsule.
3. Flexion and torsion :- During this motion there is a series of event as the “triple joint complex” of the disc and the two facet joints. The annulus gets prestressed.
Rotation around an axis passing through the vertebral body causes disruption of ipsilateral facet capsule and compression over the contralateral facet leading to fracture of pars or articular facet. The annulus gets torn in the periphery and each event results in pain.
4. Compression injuries can take place due to excessive axial load, gravity ( as in an osteoporotic spine) or muscular action as in forward bending particularly while lifting a weight.
The critical event is that of vertebral end plate fracture which initiates the process of internal disc disruption, a process directly related to injury unrelated to age related degeneration. The annulus fails by compression and the vertebrae subluxates.
This manifest as loss of disc height and isolated disc resorption. As an alternative though rarer response, the process extend to annulus in the form of radial fissures without affecting the disc height.
BIOMECHANICS OF LUMBAR DISC DEGENERATION
Intervertebral disc functions between 2 balances :- chemical (swelling pressure) balance and mechanical balance. The swelling pressure balance is regulated by the nucleus pulposus composed of proteoglycan gel (which imbibes water) interwoven with collagen fibres(which resists swelling). Transdiscal pressure varies in different postures*
-------------------------------------------------------------------- *Nachemson et al 1966
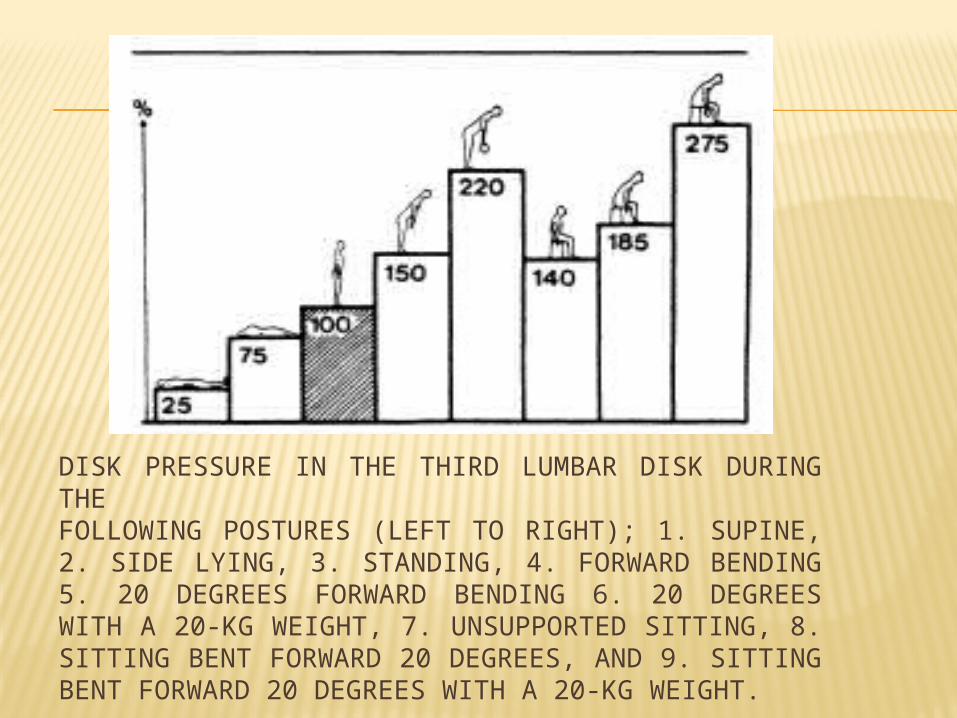
DISK PRESSURE IN THE THIRD LUMBAR DISK DURING THEFOLLOWING POSTURES (LEFT TO RIGHT); 1. SUPINE, 2. SIDE LYING, 3. STANDING, 4. FORWARD BENDING 5. 20 DEGREES FORWARD BENDING 6. 20 DEGREES WITH A 20-KG WEIGHT, 7. UNSUPPORTED SITTING, 8. SITTING BENT FORWARD 20 DEGREES, AND 9. SITTING BENT FORWARD 20 DEGREES WITH A 20-KG WEIGHT.
It is lowest in lying posture, highest in forward bending and increased in pot bellied persons, so much as that a 10cm increase in abdominal girth increases transdiscal pressure by 100lb/sq inch.
The biomechanical cause of lumbar disc derangement is the deterioration of the mechanical and chemical balance.
Although the cause of lumbar disc derangement can be implicated to a variety of etiology like ageing, Trauma, high impact activity, type of work, smoking, genetics, and obesity. The manifestation of the lumbar disc derangement can be as a mechanical disorder, neurological compressive disorder or stenotic disorder. The stages of disc degeneration * names are dysfunction, instability and stability.
STAGES OF DISC DEGENERATION
In stage of dysfunction there is swelling pressure balance deterioration , microtrauma and annulus tears and facet cartilage fissuring and synovitis.
In stage of instability , the disc height decreases , there appears a ligamentous laxity and facet joint capsule gets lax.
In the stage of stability there occurs intra discal fibrosis, peripheral osteophytosis and finally facetal subluxation and joint capsule fibrosis.
Fortunately lumbar disc degeneration routinely occurs without symptoms and whenever it is symptomatic , there is tendency for self healing.
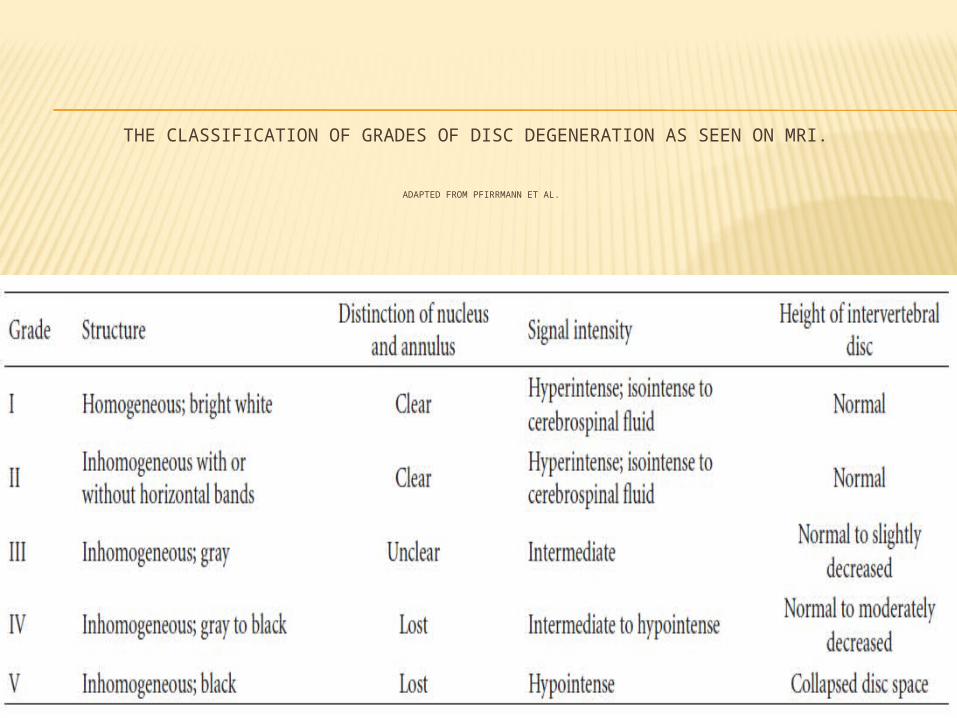
THE CLASSIFICATION OF GRADES OF DISC DEGENERATION AS SEEN ON MRI.
ADAPTED FROM PFIRRMANN ET AL.
PROPHYLAXIS
Back pain may be caused and aggravated by mechanical factors, especially by those factors related to posture. Increased emphasis on prophylaxis could well lead to a decrease in recurring back pain episodes.
POSTURAL ACTIVITIES
When a patient is suffering from back pain, sitting for long periods of time should be avoided.
If a patient must sit, proper lumbar support incorporating a back rest inclined slightly posteriorly relieves the intradiskal pressure.
WHAT IS A PROPER BACK SUPPORT?
In order to have a maximum resting effect, the lumbar support should distribute the disk pressure over the largest possible area. The support must be able to vary in size and height.The seat should tilt back slightly to accommodate the buttocks, but be high enough from the floor to prevent excessive hip flexion and eliminate the lumbar concavity.The height of the seat should allow adequate thigh support, as well as comfortable placement of the patient's feet. The free space below the seat should allow for the placement of the feet beneath the seat in rising.
Frequent change of position in sitting is important if the patient is to vary the compressive load on a degenerated disk. A chair with arm supports provides additional support and enhances the opportunity for changing positions.
WHILE LYING DOWN:-
In lying down or sleeping bending in a kyphotic posture for a prolonged period of time may cause excessive Stress on the posterior aspect of the disk. A firm mattress that prevents a flexed posture is preferable. The firmness of the mattress supports the patient's spine. The patient should rise up out of bed by rolling to his side, swinging his legs over the side of the bed, and pushing up with his arms to a sitting position, instead of sitting up directly from the lying position and twisting the body.
WORK ACTIVITIES
o While lifting weight the critical factor in lifting is to keep the load close to the body, which reduces the moment arm at the spinal joints and requires less muscle force, thereby decreasing the intradiskal pressures.
o The lift should be done with the legs, not the back
o Just before lifting, a deep breath should be taken to increase the intrathoracic and intraabdominal pressure, which in turn reduces the disk pressure.
o The load should remain close to the body in going from a flexed knee to an erect position.
o Once in the standing position, the load should be placed on the ilium, which transmits the weight to the lower extremity and bypasses the lumbar part of the spine.
An alternate method of picking up an object from the floor is to maintain a straight back and flex from the hips, then remain standing on one leg, kick the other leg out straight back, and proceed to bend over to pick up the object
If an object must be moved, pushing is preferable to pulling.
Any activity that requires lifting something and then rotating the spine, as in throwing an object, should be carefully done in two straight motions instead of a twisting motion.
Loads should not be lifted suddenly, but smoothly. Work involving contact with the floor or ground should be done in a quadrupedal position.
EXERCISE
The most important muscle groups for using proper body mechanics are the quadriceps femoris and the abdominal muscles.
Strong quadriceps femoris muscles are necessary for lifting a load in a crouched position with a straight back and bent legs.
Strong abdominal muscles help decrease intradiskal pressures. Strengthening abdominal muscles isometrically is preferable to the commonly used sit-ups because the sit-up position causes a large increase in intradiskal pressure.
A good effect for flexion exercises is that a straight or slightly kyphotic posture in the lumbar part of the spine allows for a widening of the posterior half of the intervertebral joint space and opens the foramina, thereby preventing a constriction of any disk material
Some studies support maintaining the lumbar lordorsis to keep the disk forward, as a preventive measure in patients with back pain.
Other studies suggested that if a patient must do extension exercises, he should do them from an elevated surface, where the weight of the lower limbs provides a traction effect on the lumbar part of the spine, thus decreasing the amount of compression on the disk
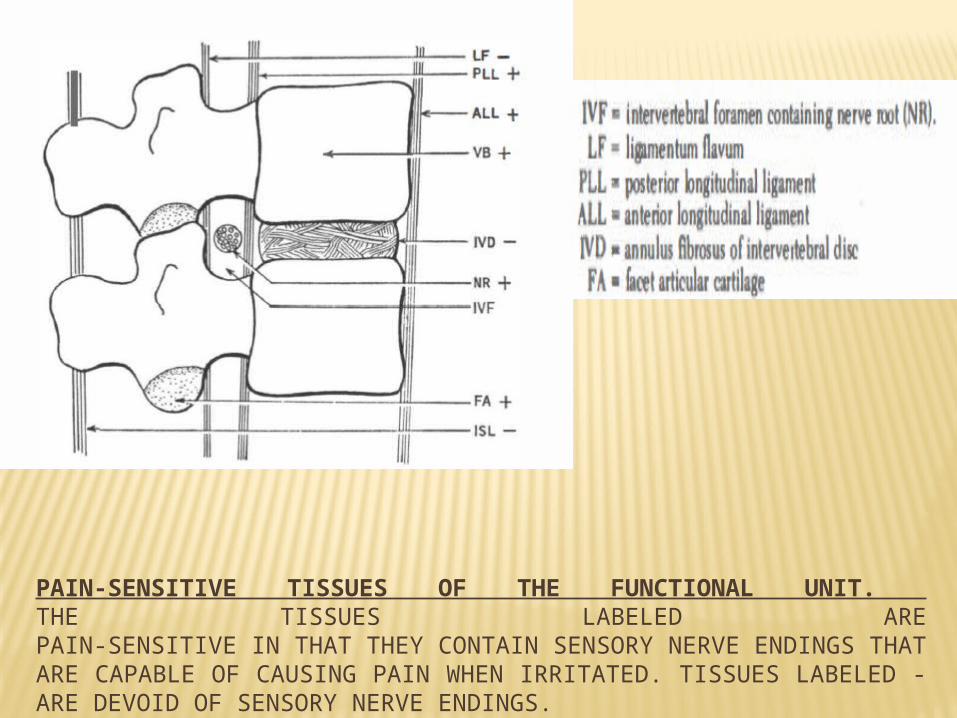
PAIN-SENSITIVE TISSUES OF THE FUNCTIONAL UNIT. THE TISSUES LABELED AREPAIN-SENSITIVE IN THAT THEY CONTAIN SENSORY NERVE ENDINGS THAT ARE CAPABLE OF CAUSING PAIN WHEN IRRITATED. TISSUES LABELED - ARE DEVOID OF SENSORY NERVE ENDINGS.