Embed Size (px)
Citation preview
Osteopathic Medicine
The Lumbar Spine
Grégoire Lason & Luc Peeters
2
The Lumbar Spine
Grégoire Lason & Luc Peeters All rights reserved. Osteo 2000 bvba © 2013. No part of this e-book may be reproduced or made
public by printing, photocopying, microfilming, or by any means without the prior written permission of the publisher.
Contact: Osteo 2000, Kleindokkaai 3-5, B – 9000 Ghent, Belgium
Mail: [email protected]
Web: http://osteopedia.iao.be and www.osteopathie.eu
Tel: +32 9 233 04 03 - Fax: +32 55 70 00 74
ISBN: 9789074400411
The International Academy of Osteopathy – I.A.O.
3
Content Content ....................................................................................................................... 3
1. Introduction ............................................................................................................ 7
2. Biomechanics ........................................................................................................ 8 2.1. General ............................................................................................................. 8 2.2. Motions in the sagittal Plane .......................................................................... 8
2.2.1. Neutral Position (N) .................................................................................... 8 2.2.2. Flexion (F) .................................................................................................. 9
2.2.2.1. Moderate Flexion ................................................................................. 9 2.2.2.2. More Flexion ........................................................................................ 9
2.2.3. Extension .................................................................................................. 11 2.2.3.1. Moderate Extension ........................................................................... 11 2.2.3.2. More Extension .................................................................................. 11
2.3. Motions in the Frontal Plane ........................................................................ 13 2.3.1. Sidebending .............................................................................................. 13
2.3.1.1. Neutral Position .................................................................................. 13 2.3.1.2. Flexion ............................................................................................... 14 2.3.1.3. Extension ........................................................................................... 15
2.4. Motions in the Horizontal Plane ................................................................... 16 2.4.1. Rotation .................................................................................................... 16
3. Lesion Mechanics ................................................................................................ 17 3.1. Group Lesion in NSRRL ................................................................................. 20 3.2. Monolytic Lesion in FRSR ............................................................................. 21 3.3. Monolytic Lesion in ERSR ............................................................................. 22
4. Low Back Pain related to the lumbar Spine ...................................................... 23 4.1. General ........................................................................................................... 23 4.2. Possible Causes of Low Back Pain ............................................................. 27
4.2.1. Lumbar spinal Stenosis ............................................................................ 27 4.2.2. Ankylosing Spondylitis .............................................................................. 28 4.2.3. Scheuermann’s Disease ........................................................................... 29 4.2.4. Disc Disease ............................................................................................. 30
4.2.4.1. Degenerative ...................................................................................... 30 4.2.4.2. Acute Disc Prolapse ........................................................................... 32 4.2.4.3. Cauda Equina Syndrome ................................................................... 33 4.2.4.4. Annular Fissure .................................................................................. 33 4.2.4.5. Discitis ................................................................................................ 34
4.2.5. Osteoarthritis ............................................................................................ 38 4.2.6. Facet Joint Arthropathy ............................................................................ 39 4.2.7. Facet Joint synovial Cysts ........................................................................ 41 4.2.8. Ligamentum Flavum Hypertrophy ............................................................ 42 4.2.9. Spondylolysis ............................................................................................ 43
4
4.2.10. Spondylolysthesis or Anterolysthesis ..................................................... 44 4.2.11. Scoliosis ................................................................................................. 45 4.2.12. Lumbosacral transitional Malformation ................................................... 46 4.2.13. Fractures ................................................................................................ 47 4.2.14. Osteomyelitis .......................................................................................... 48
5. Examination ......................................................................................................... 49 5.1. Provocation Tests for Inflammation ............................................................ 49
5.1.1. Heel Compression .................................................................................... 49 5.1.2. Compression Test (sitting) ........................................................................ 50 5.1.3. Compression Test of the Facet Joints and Rozet Test ............................. 51 5.1.4. Traction Test ............................................................................................. 51
5.2. Test for Amplitude ........................................................................................ 52 5.2.1. Schober Test ............................................................................................ 52 5.2.2. Finger to Toe Test .................................................................................... 52
5.3. Phalen’s Test for lumbar Stenosis .............................................................. 53 5.4. Leg Extension Test ....................................................................................... 53 5.5. Neurological Tests ........................................................................................ 54
5.5.1. Checklists for neurological Examination of the lumbar and sacral Plexuses ............................................................................................................................ 54 5.5.2. Reflex Adductor Tendon ........................................................................... 56 5.5.3. Patella Reflex (Knee Jerk Response) ....................................................... 56 5.5.4. Patella Reflex – Jendrassik Test .............................................................. 57 5.5.5. Tibialis Anterior Reflex .............................................................................. 57 5.5.6. Tibialis Posterior Reflex ............................................................................ 58 5.5.7. Achilles Tendon ........................................................................................ 58 5.5.8. Testing Muscle Force ............................................................................... 59 5.5.9. Testing Sensibility ..................................................................................... 59 5.5.10. Babinski Reflex ....................................................................................... 60 5.5.11. Straight Leg Rise Test (SLR) .................................................................. 61 5.5.12. Hoover Test ............................................................................................ 63 5.5.13. Kernig Test ............................................................................................. 63 5.5.14. Millgram Test .......................................................................................... 64 5.5.15. Beevor’s Test .......................................................................................... 64
5.6. Mobility Testing ............................................................................................. 65 5.6.1. Active Flexion ........................................................................................... 65 5.6.2. Active Extension ....................................................................................... 65 5.6.3. Active Sidebending ................................................................................... 66 5.6.4. Oscillation Test (sitting) ............................................................................ 66 5.6.5. Oscillation Test (prone) ............................................................................ 67 5.6.6. Passive Flexion Test ................................................................................ 67 5.6.7. Passive Extension Test ............................................................................ 68 5.6.8. Passive Sidebending Test ........................................................................ 68
6. Techniques ........................................................................................................... 69
5
6.1. Mobilisations ................................................................................................. 69 6.1.1. General ..................................................................................................... 69 6.1.2. Flexion – Extension Mobilisation .............................................................. 70 6.1.3. Flexion Mobilisation .................................................................................. 70 6.1.4. Extension Mobilisation .............................................................................. 71 6.1.5. Sidebending Mobilisation .......................................................................... 71 6.1.6. Sidebending Mobilisation .......................................................................... 72 6.1.7. Rotation Mobilisation ................................................................................ 72 6.1.8. Rotation Mobilisation ................................................................................ 73 6.1.9. Stretch of the Iliolumbar Ligaments .......................................................... 73
6.1.9.1. Note on the Iliolumbar Ligaments ...................................................... 74 A. Development ........................................................................................... 74 B. Anatomy .................................................................................................. 74 C. Biomechanics of the Iliolumbar Ligaments ............................................. 77 D. Pathology ................................................................................................ 81 E. Provocation and palpation ...................................................................... 82
6.1.10. Mobilisation for Anterolisthesis ............................................................... 84 6.2. ‘Osteopathic Manipulative Techniques’ ...................................................... 85
6.2.1. General ..................................................................................................... 85 6.2.2. Standard Manipulation of an ERSR Lesion ............................................... 88 6.2.3. Standard Manipulation of a FRSR Lesion ................................................. 89 6.2.4. Manipulation in Shift of an ERSR Lesion ................................................... 89 6.2.5. Manipulation in Shift of an ERSR Lesion ................................................... 90 6.2.6. Manipulation in Shift of a FRSR Lesion ..................................................... 90 6.2.7. Manipulation of an Anterolisthesis ............................................................ 91 6.2.8. Manipulation of an Anterolisthesis – Second Technique .......................... 91 6.2.9. Manipulation of the underlying Facets into Divergence ............................ 92 6.2.10. Manipulation of an ERSR Lesion (Sitting) ............................................... 93 6.2.11. Manipulation of the Thoracolumbar Junction .......................................... 94 6.2.12. Manipulation of the Thoracolumbar Junction – Second Technique ........ 94 6.2.13. Manipulation of the Thoracolumbar Junction – Third Technique ............ 95
6.3. ‘Muscle Energy Techniques’ (M.E.T.) .......................................................... 96 6.3.1. General ..................................................................................................... 96 6.3.2. Correction of a FRSR Lesion ..................................................................... 98 6.3.3. Correction of an ERSR Lesion .................................................................. 98 6.3.4. Correction of a NSLRR Lesion ................................................................... 99 6.3.5. Correction of a Lesion of L4 in FRSR ........................................................ 99 6.3.6. Correction of a Lesion of L4 in ERSR ...................................................... 100 6.3.7. Stretch of the Quadratus Lumborum ...................................................... 100 6.3.8. Stretch of the Quadratus Lumborum - Second Technique .................... 101 6.3.9. Stretch of the Paravertebral Muscles ..................................................... 101 6.3.10. Stretch of the Right Internal Oblique .................................................... 102 6.3.11. Stretch of the Psoas Major ................................................................... 102
6.4. ‘Strain and Counterstrain’ Techniques ..................................................... 103
6
6.4.1. General ................................................................................................... 103 6.4.2. Extension Lesion of L1 and L2 ................................................................. 103 6.4.3. Extension Lesion of L3, L4 and L5 ............................................................ 104 6.4.4. Atypical Lesion of L5 ............................................................................... 104 6.4.5. Flexion Lesion of L1 ................................................................................ 105 6.4.6. Flexion Lesion of L2 ................................................................................ 105 6.4.7. Atypical Lesion of L2 ............................................................................... 106 6.4.8. Flexion Lesion of L3 and L4 ..................................................................... 106 6.4.9. Flexion Lesion of L5 ................................................................................ 107
7. Bibliography ....................................................................................................... 108
8. About the Authors ............................................................................................. 113
9. Acknowledgment ............................................................................................... 114
10. Osteopathic terminology ................................................................................ 115 10.1. The three anatomical Axes ....................................................................... 115 10.2. The three anatomical Planes .................................................................... 116 10.3. Spinal Biomechanics ................................................................................ 117 10.4. General Abbreviations .............................................................................. 119 10.5. Specific Terms ........................................................................................... 120
11. All Video’s ........................................................................................................ 121
8
2. Biomechanics (Benzel 2001, Carlson 2003, Fryette 1942, 1988, Gray 1995, 2000, Grant 2004, Hall-Craggs 1995, Harrison et al 1999, Kapandji 2001, King & Yang 1986, Lovett 1905, Moore & Dalley 1999, Netter 2003, Panjabi & White 2001, Pearcy & Tibrewel 1984, Romanes 1972, Shellshear & Macintosh 1949, Snell 1995, Sobotta 2001, Vicenzino & Twomey 1993, White & Panjabi 1990, Woodburne & Burkel 1988, Wood & Jones 1953)
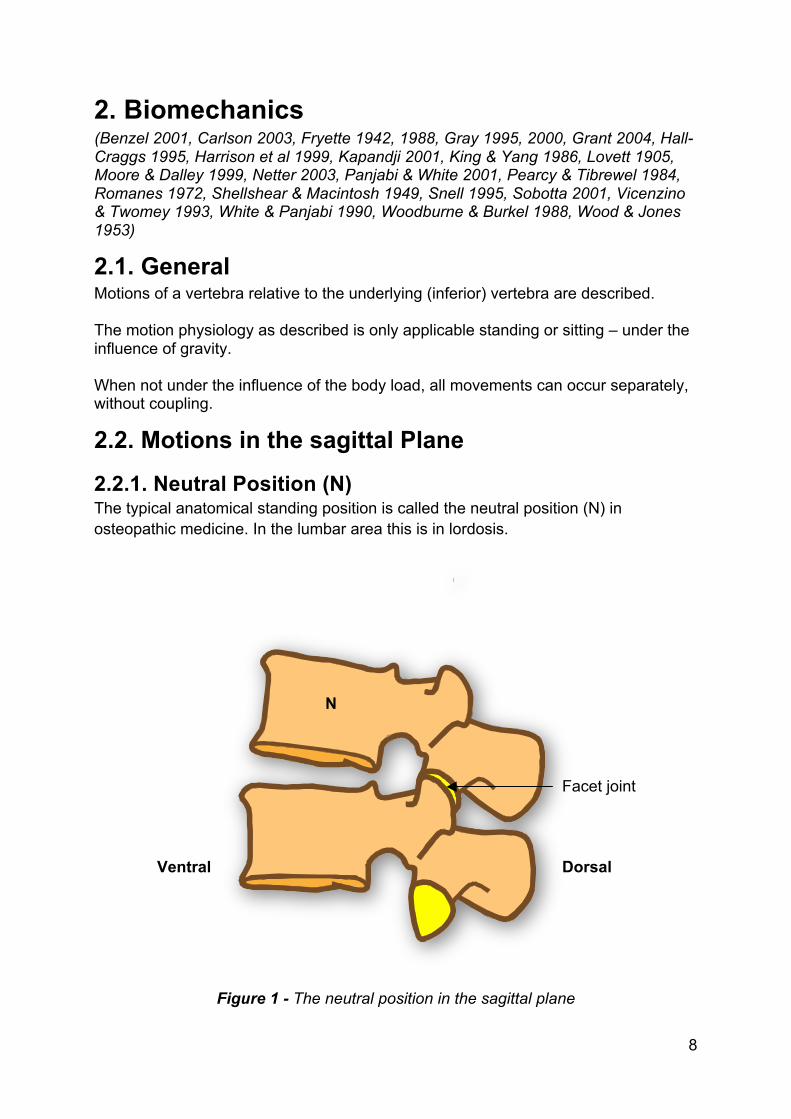
2.1. General Motions of a vertebra relative to the underlying (inferior) vertebra are described. The motion physiology as described is only applicable standing or sitting – under the influence of gravity. When not under the influence of the body load, all movements can occur separately, without coupling.
2.2. Motions in the sagittal Plane
2.2.1. Neutral Position (N) The typical anatomical standing position is called the neutral position (N) in osteopathic medicine. In the lumbar area this is in lordosis.
Figure 1 - The neutral position in the sagittal plane
Facet joint
Dorsal Ventral
N
9
2.2.2. Flexion (F)
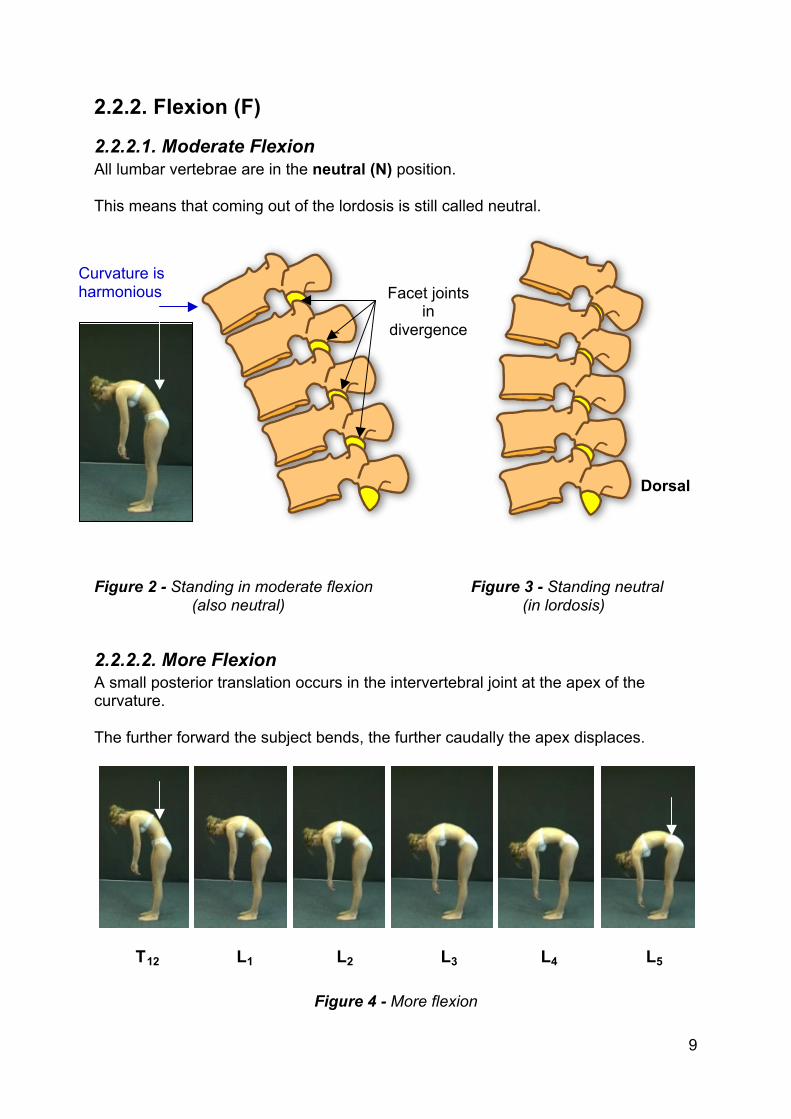
2.2.2.1. Moderate Flexion All lumbar vertebrae are in the neutral (N) position. This means that coming out of the lordosis is still called neutral.
Figure 2 - Standing in moderate flexion Figure 3 - Standing neutral (also neutral) (in lordosis)
2.2.2.2. More Flexion A small posterior translation occurs in the intervertebral joint at the apex of the curvature. The further forward the subject bends, the further caudally the apex displaces.
Figure 4 - More flexion
T12 L1 L2 L3 L4 L5
Curvature is harmonious Facet joints
in divergence
Dorsal
10
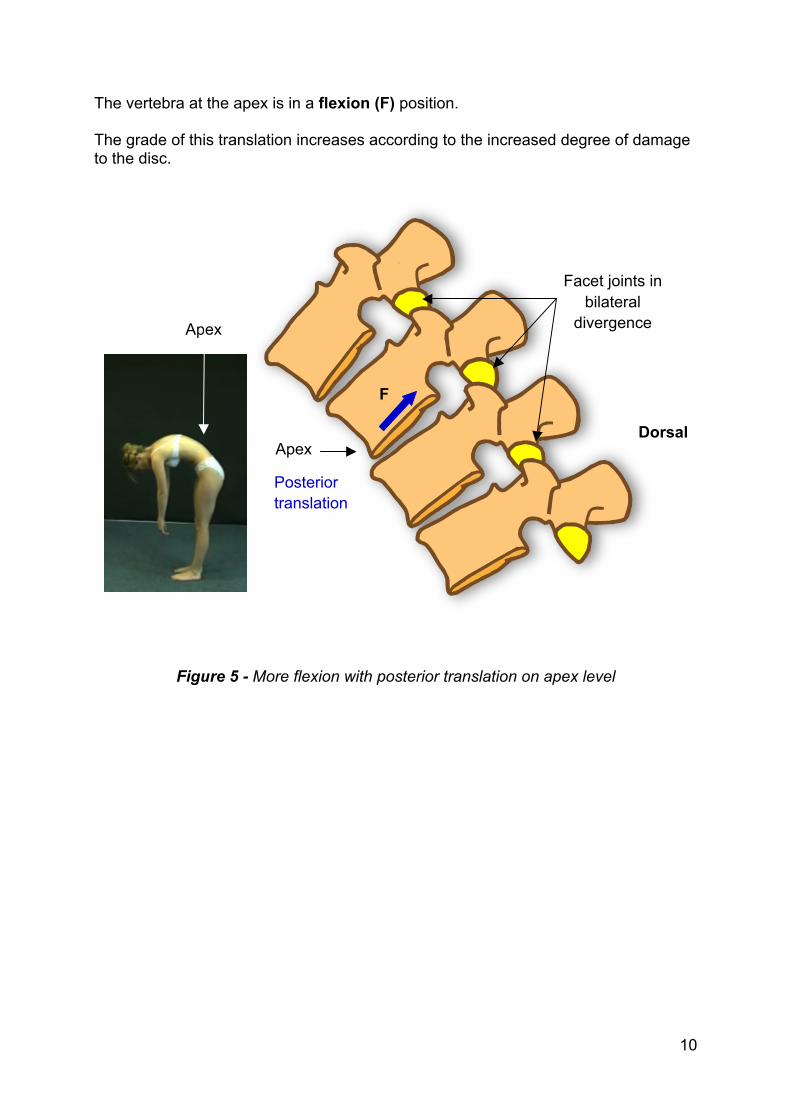
The vertebra at the apex is in a flexion (F) position. The grade of this translation increases according to the increased degree of damage to the disc.
Figure 5 - More flexion with posterior translation on apex level
Dorsal
Apex
Apex
F
Facet joints in bilateral
divergence
Posterior translation
49
5. Examination (Kuchera & Kuchera 1996, 2001, Lee & Vleeming 2004, Paris 1997, Saal 2002, Stern et al 2006, Wadell et al 1982, Wilson 2008)
5.1. Provocation Tests for Inflammation An inflamed joint can be provoked on pain when compressed. After compression, often the pain persists for seconds.
The compression can be provoked mechanically by coughing or sneezing.
5.1.1. Heel Compression This test is done with the patient supine. The osteopath taps the calcaneus of the patient’s straightened leg in axial direction (towards the spine). The test can also be performed by asking the standing patient to stand on his/her toes and to fall on the heels. This test compresses the discs and the facet joints and provokes pain in the case of intra-articular inflammation, discitis or facet inflammation. Discitis or facet inflammation is also painful when coughing or sneezing. The provoked pain will be sharp.
50
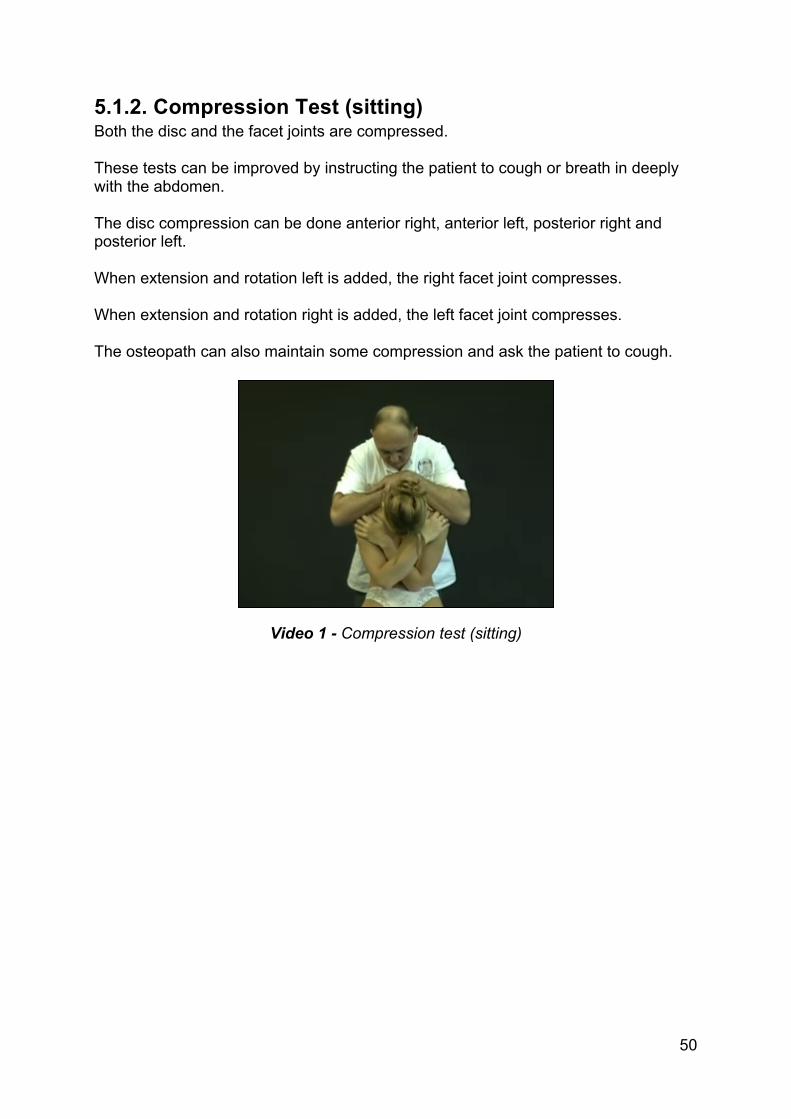
5.1.2. Compression Test (sitting) Both the disc and the facet joints are compressed. These tests can be improved by instructing the patient to cough or breath in deeply with the abdomen. The disc compression can be done anterior right, anterior left, posterior right and posterior left. When extension and rotation left is added, the right facet joint compresses. When extension and rotation right is added, the left facet joint compresses. The osteopath can also maintain some compression and ask the patient to cough.
Video 1 - Compression test (sitting)
51
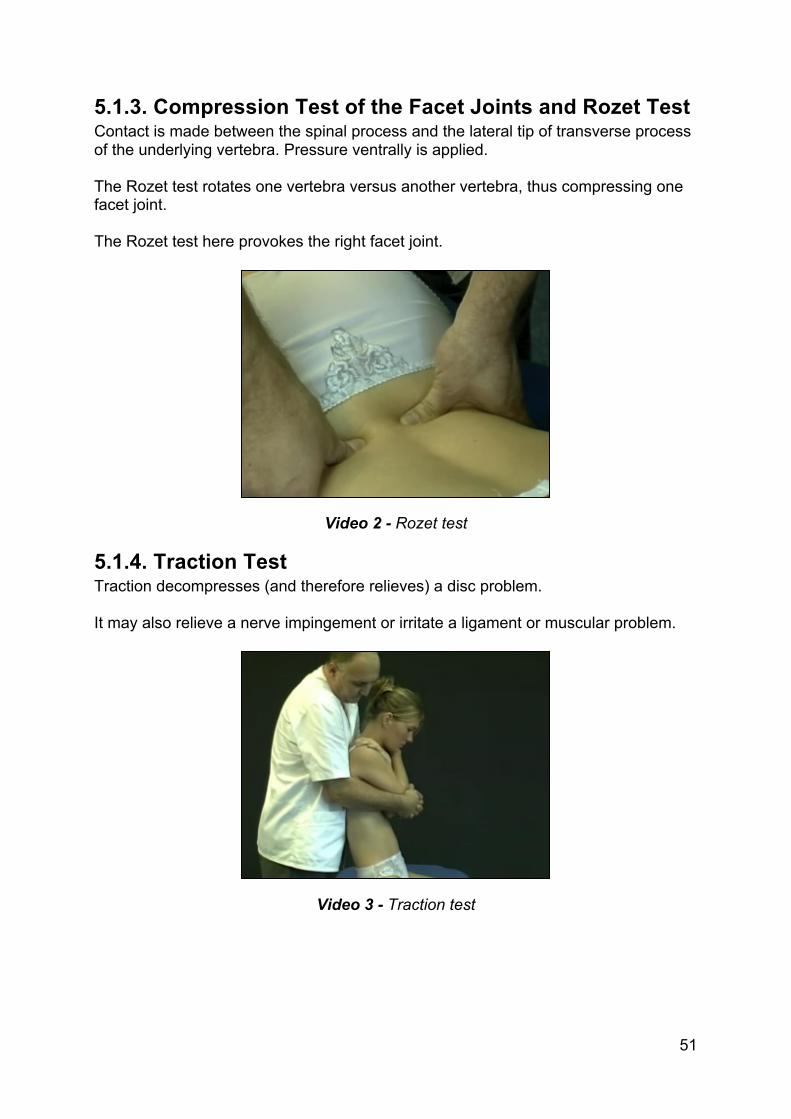
5.1.3. Compression Test of the Facet Joints and Rozet Test Contact is made between the spinal process and the lateral tip of transverse process of the underlying vertebra. Pressure ventrally is applied. The Rozet test rotates one vertebra versus another vertebra, thus compressing one facet joint. The Rozet test here provokes the right facet joint.
Video 2 - Rozet test
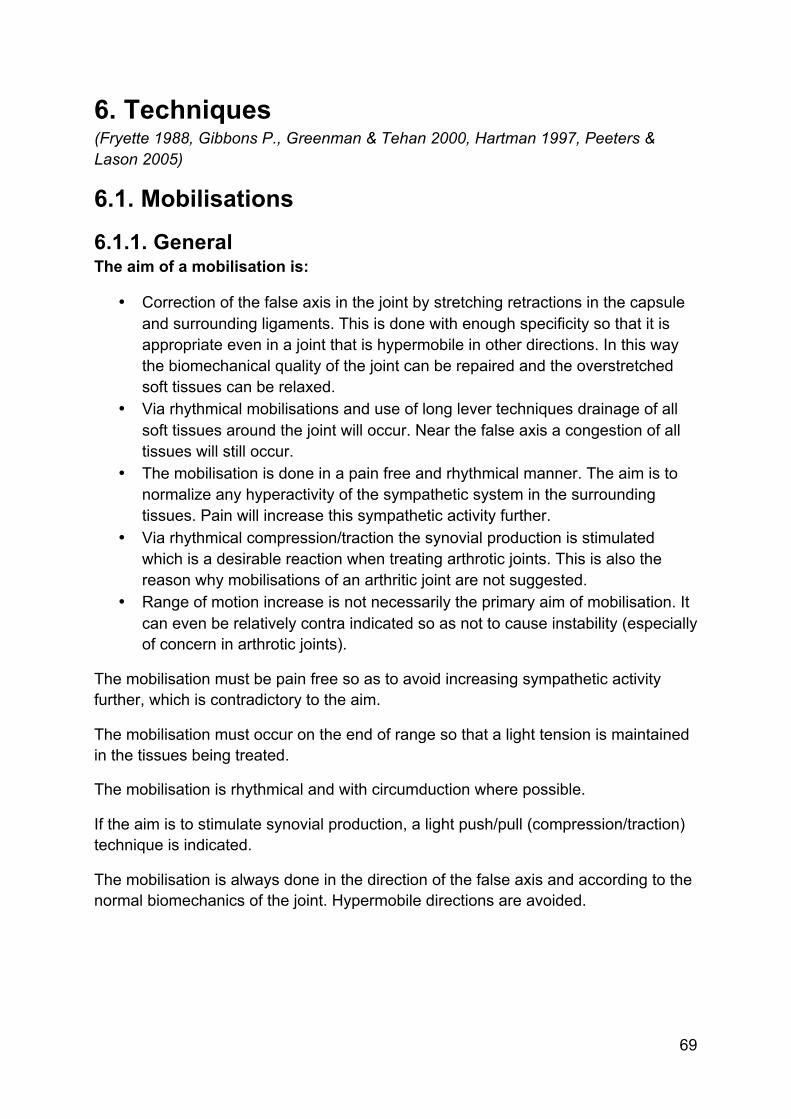
5.1.4. Traction Test Traction decompresses (and therefore relieves) a disc problem. It may also relieve a nerve impingement or irritate a ligament or muscular problem.
Video 3 - Traction test
69
6. Techniques (Fryette 1988, Gibbons P., Greenman & Tehan 2000, Hartman 1997, Peeters & Lason 2005)
6.1. Mobilisations
6.1.1. General The aim of a mobilisation is:
• Correction of the false axis in the joint by stretching retractions in the capsule and surrounding ligaments. This is done with enough specificity so that it is appropriate even in a joint that is hypermobile in other directions. In this way the biomechanical quality of the joint can be repaired and the overstretched soft tissues can be relaxed.
• Via rhythmical mobilisations and use of long lever techniques drainage of all soft tissues around the joint will occur. Near the false axis a congestion of all tissues will still occur.
• The mobilisation is done in a pain free and rhythmical manner. The aim is to normalize any hyperactivity of the sympathetic system in the surrounding tissues. Pain will increase this sympathetic activity further.
• Via rhythmical compression/traction the synovial production is stimulated which is a desirable reaction when treating arthrotic joints. This is also the reason why mobilisations of an arthritic joint are not suggested.
• Range of motion increase is not necessarily the primary aim of mobilisation. It can even be relatively contra indicated so as not to cause instability (especially of concern in arthrotic joints).
The mobilisation must be pain free so as to avoid increasing sympathetic activity further, which is contradictory to the aim.
The mobilisation must occur on the end of range so that a light tension is maintained in the tissues being treated.
The mobilisation is rhythmical and with circumduction where possible.
If the aim is to stimulate synovial production, a light push/pull (compression/traction) technique is indicated.
The mobilisation is always done in the direction of the false axis and according to the normal biomechanics of the joint. Hypermobile directions are avoided.
70
Contra indications
• Inflammation or infection. • A joint with intra-articular swelling.
Mobilisation will only increase and worsen the swelling. • Painful end of range. • In the direction of a structurally damaged capsule. • Directly following recent trauma.
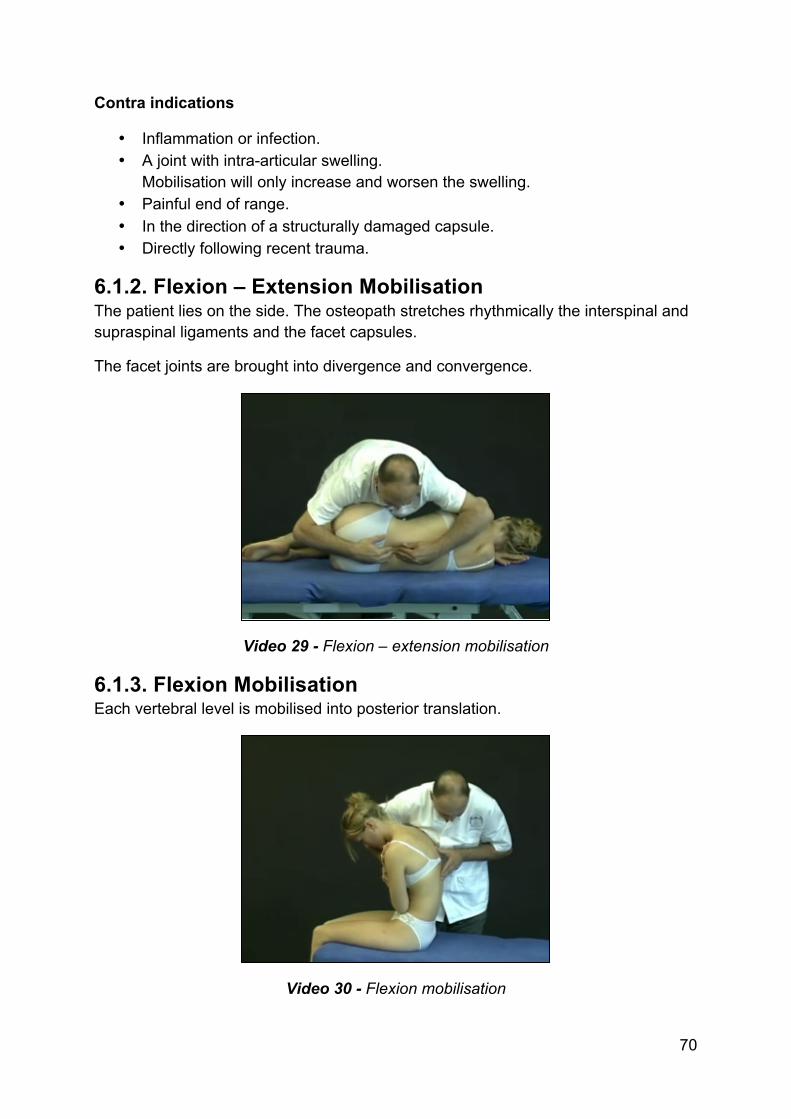
6.1.2. Flexion – Extension Mobilisation The patient lies on the side. The osteopath stretches rhythmically the interspinal and supraspinal ligaments and the facet capsules.
The facet joints are brought into divergence and convergence.
Video 29 - Flexion – extension mobilisation
6.1.3. Flexion Mobilisation Each vertebral level is mobilised into posterior translation.
Video 30 - Flexion mobilisation
71
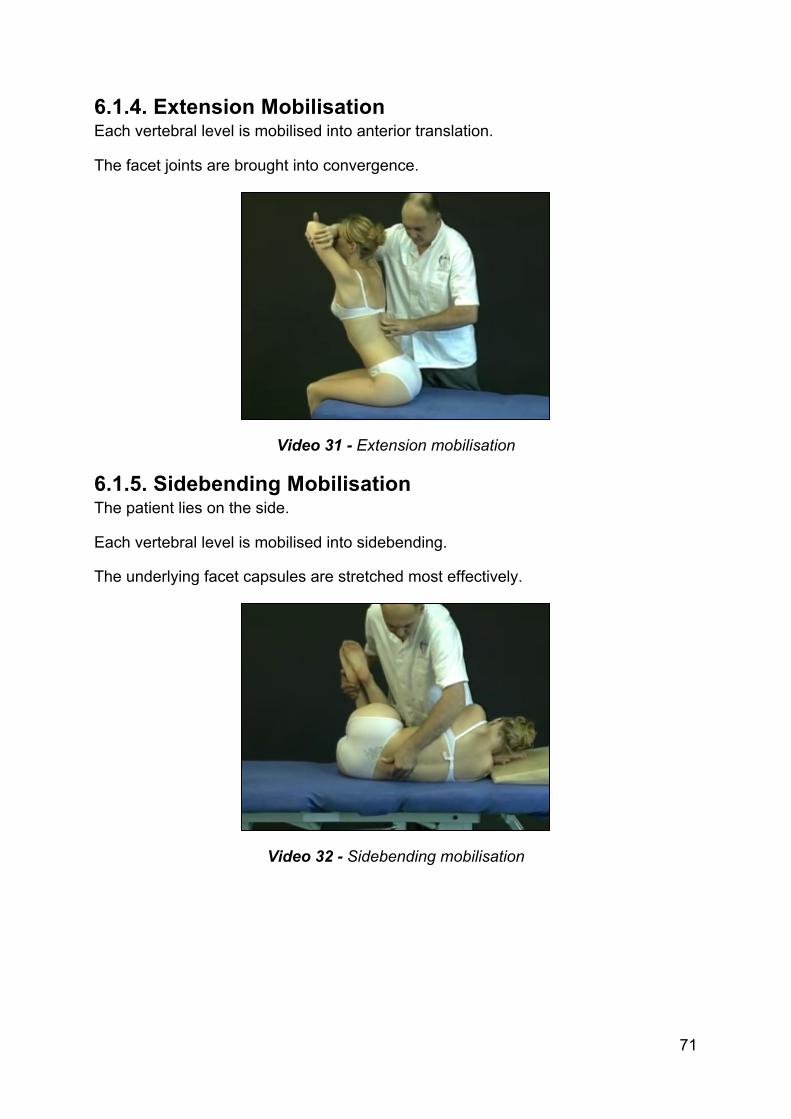
6.1.4. Extension Mobilisation Each vertebral level is mobilised into anterior translation.
The facet joints are brought into convergence.
Video 31 - Extension mobilisation
6.1.5. Sidebending Mobilisation The patient lies on the side.
Each vertebral level is mobilised into sidebending.
The underlying facet capsules are stretched most effectively.
Video 32 - Sidebending mobilisation