Embed Size (px)
DESCRIPTION
Citation preview

1
16 February 200516 February 2005
FDA Advisory Committee MeetingFDA Advisory Committee Meeting
Cardiovascular Safety of CelecoxibCardiovascular Safety of Celecoxib
& &
Risk-Benefit Assessment Risk-Benefit Assessment

A2
DelegationDelegation
Dr Jeffrey BorerDr Jeffrey Borer CardiologyCardiologyDr Andrew Dannenberg Dr Andrew Dannenberg GastroenterologyGastroenterologyDr Gerry FaichDr Gerry Faich Epidemiology/Drug SafetyEpidemiology/Drug SafetyDr Norman GitlinDr Norman Gitlin GastroenterologyGastroenterologyDr Gary Koch Dr Gary Koch StatisticianStatisticianDr Bernard LevinDr Bernard Levin OncologyOncologyDr Scott LippmanDr Scott Lippman Oncology Oncology Dr Nancy NussmeierDr Nancy Nussmeier AnesthesiologyAnesthesiologyDr Lee SimonDr Lee Simon RheumatologyRheumatologyDr Vibeke Strand Dr Vibeke Strand RheumatologyRheumatologyDr Andrew WheltonDr Andrew Whelton NephrologyNephrology Dr William WhiteDr William White HypertensionHypertension

A3
Overall ConclusionsOverall Conclusions
There are few therapeutic alternatives for patients with There are few therapeutic alternatives for patients with chronic arthritis-related painchronic arthritis-related pain
– Patients who discontinue celecoxib will likely turn to Patients who discontinue celecoxib will likely turn to NSAIDsNSAIDs
Celecoxib provides improved GI safety compared to NSAIDsCelecoxib provides improved GI safety compared to NSAIDs All lines of evidence show the CV safety of celecoxib is All lines of evidence show the CV safety of celecoxib is
similar to NSAIDs for up to 1 yr; similar to NSAIDs for up to 1 yr;
– beyond 1 yr little is known for any of these agentsbeyond 1 yr little is known for any of these agents
– evidence for COXIB vs NSAID class effect on CV safety evidence for COXIB vs NSAID class effect on CV safety is not establishedis not established
– rofecoxib is distinct from celecoxib and NSAIDs rofecoxib is distinct from celecoxib and NSAIDs Only further study of NSAIDs/COXIBs will define the longer-Only further study of NSAIDs/COXIBs will define the longer-
term CV risks against the known risks of GI ulcer term CV risks against the known risks of GI ulcer complicationscomplications

A4
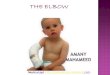
Census data for 1999.CDC. MMWR Morb Mortal Wkly Rep. 2001;50:120-125.
% All Disabilities
Stroke
Blindness or Vision
Diabetes
Mental or Emotional
Limb/Extremity Stiffness
Deafness or Hearing
Lung or Respiratory
Heart Trouble, Hardening of the Arteries
Back or Spine
Arthritis
0 2 4 6 8 10 12 14 16 18
2.8%
3.3%
3.4%
3.7%
4.2%
4.4%
4.7%
7.8%
16.5%
17.5%
Arthritis is a Leading Cause of Disability
About 39 million physician visits/ yr1
More than 500,000 hospitalizations/ yr1
1 CDC, Arthritis Foundation. National Arthritis Action Plan: A Public Health Strategy. 1999.

A5
Efficacy in OA Efficacy in OA
NSAIDs are an important treatment optionNSAIDs are an important treatment option
Pincus et al. Arthritis Rheum 2001;44:1587-1598Pincus et al. Arthritis Rheum 2001;44:1587-1598* p<0.05 vs acetaminophen * p<0.05 vs acetaminophen
00
2525
3030
3535
4040
4545
5050
JJ
JJ
JJJJ
JJ
JJ
JJJJ
acetaminophenacetaminophen
diclofenac + diclofenac + misoprostolmisoprostol acetaminophenacetaminophen
diclofenac + diclofenac + misoprostolmisoprostol
WO
MA
C T
arg
et J
oin
t S
core
(m
m)
WO
MA
C T
arg
et J
oin
t S
core
(m
m)
00 66 00 66
washout washout &&
crossovercrossover
washout washout
Acetaminophen 1000 mg qidAcetaminophen 1000 mg qidDiclofenac 75 mg/misoprostol 200 Diclofenac 75 mg/misoprostol 200 g bid g bid N=227N=227
**
**
GreaterGreaterimprovementimprovement
WeeksWeeks

A6
Age Group (yrs)Age Group (yrs)
00
55
1010
1515
2020
2525
15-1
915
-19
20-2
420
-24
25-2
925
-29
30-3
430
-34
35-3
935
-39
40-4
440
-44
45-4
945
-49
50-5
450
-54
55-5
955
-59
60-6
460
-64
65-6
965
-69
70-7
470
-74
75-7
975
-79
80-8
480
-84
85+
85+
Non-users MenNon-users Men
Non-users WomenNon-users Women
Current users Men Current users Men
Current users WomenCurrent users Women
Saskatchewan, Canada Saskatchewan, Canada
Per
100
0 P
t-yr
sP
er 1
000
Pt-
yrs
Perez-GutthaPerez-Gutthannn et al. Epidemiology 1997;8:18-24n et al. Epidemiology 1997;8:18-24
Incidence of Hospitalization for GI Bleeding or Incidence of Hospitalization for GI Bleeding or PerforationsPerforations

A7
Arachidonic AcidArachidonic Acid
COX-1COX-1(Constitutive)(Constitutive)
COX-2COX-2(Inducible)(Inducible)
StomachStomachIntestineIntestineKidneyKidneyPlateletPlatelet
Disease Targets:Disease Targets:• Arthritis, PainArthritis, Pain
xx
COX-2 Inhibitor Hypothesis: COX-2 Inhibitor Hypothesis: 19921992
NSAIDsNSAIDs
COX-2 inhibitorCOX-2 inhibitor

A8
Clinical Effects of Celecoxib in RAClinical Effects of Celecoxib in RA
**p**p <0.001 vs other treatments <0.001 vs other treatments
****
Pat
ien
ts w
ith
Ulc
er (
%)
Pat
ien
ts w
ith
Ulc
er (
%)
Celecoxib Celecoxib (mg bid)(mg bid)
Naproxen Naproxen (mg bid)(mg bid)
2525
00
55
1010
1515
2020
PlaceboPlacebo 200200 400400 500500 100100
AC
R 2
0 R
esp
on
der
s A
CR
20
Res
po
nd
ers
(%)
(%)
00
1010
2020
3030
4040
5050
100100 200200 400400 500500
CelecoxibCelecoxib(mg bid)(mg bid)
NaproxenNaproxen(mg bid)(mg bid)
****
****
PlaceboPlacebo
Simon et al. JAMA 282 20:1921-1928, 1999Simon et al. JAMA 282 20:1921-1928, 1999 *p*p <0.001 vs placebo <0.001 vs placebo
CelecoxibCelecoxibNaproxen Naproxen
Placebo Placebo N =1149N =1149
EfficacyEfficacy Upper GI SafetyUpper GI Safety

A9
Relative Risk (95%CI)Relative Risk (95%CI)
GI Safety Profile of Celecoxib GI Safety Profile of Celecoxib Meta Analysis of Arthritis RCTsMeta Analysis of Arthritis RCTs
0.35 (0.22, 0.56)0.35 (0.22, 0.56)
Reductions in Hgb > 2g/dL Reductions in Hgb > 2g/dL
Symptomatic ulcers/GI bleeding Symptomatic ulcers/GI bleeding
Withdrawal due to GI intolerance Withdrawal due to GI intolerance
Celecoxib (200/400 mg) vs NSAIDs Celecoxib (200/400 mg) vs NSAIDs
Celecoxib (any dose) vs NSAIDs Celecoxib (any dose) vs NSAIDs
Celecoxib (200/400 mg) vs NSAIDs Celecoxib (200/400 mg) vs NSAIDs
Celecoxib (any dose) vs NSAIDs Celecoxib (any dose) vs NSAIDs
Celecoxib (200/400 mg) vs NSAIDs Celecoxib (200/400 mg) vs NSAIDs
Celecoxib (any dose) vs NSAIDs Celecoxib (any dose) vs NSAIDs
0.61 (0.46, 0.81)0.61 (0.46, 0.81)
0.71 (0.55, 0.91)0.71 (0.55, 0.91)
0.72 (0.56, 0.92)0.72 (0.56, 0.92)
0.70 (0.60, 0.80)0.70 (0.60, 0.80)
0.75 (0.70, 0.80)0.75 (0.70, 0.80)
Favors NSAIDsFavors NSAIDs
0.500.500.250.25 1.01.00.750.75 1.251.25
Favors celecoxibFavors celecoxib
0.00.0
Moore et al. Arthritis Research & Therapy 2005: (Feb) Moore et al. Arthritis Research & Therapy 2005: (Feb)
39,605 OA/RA patients; mean exposure ~7 mo39,605 OA/RA patients; mean exposure ~7 mo

A10
3.03.0
4.04.0
1.91.9
11
22
33
44
55
66
77
Ad
just
ed
Ra
te R
ati
oA
dju
ste
d R
ate
Ra
tio
00Non-useNon-use celecoxibcelecoxib rofecoxibrofecoxib diclo+misodiclo+miso NSAIDsNSAIDs
Mamdani et al. BMJ 2002;325(7365):624-7Mamdani et al. BMJ 2002;325(7365):624-7
1.01.01.01.0
Risk of Hospitalization for Upper GI Risk of Hospitalization for Upper GI Bleeding with COXIBsBleeding with COXIBs
>55% women>55% womenMean age >75 yrsMean age >75 yrs>1% with Hx of GI bleed >1% with Hx of GI bleed >16% Use of gastroprotective agent>16% Use of gastroprotective agent>12% Use of aspirin>12% Use of aspirin
100,000 (2.2)*100,000 (2.2)* 18,908 (3.6)*18,908 (3.6)* 14,583 (7.3)*14,583 (7.3)* 5,087 (9.6)*5,087 (9.6)* 5,391 (12.6)*5,391 (12.6)*
*n (no. upper GI bleeds per 1000 person-yrs)*n (no. upper GI bleeds per 1000 person-yrs)

A11
3.33.3
1.31.3
2.12.1
1.01.0
00
11
22
33
44
55
Non-useNon-use celecoxibcelecoxib rofecoxibrofecoxib NSAIDsNSAIDs
Ad
just
ed
Od
ds
Ra
tio
Ad
just
ed
Od
ds
Ra
tio
Risk of Hospitalization of Upper GI Risk of Hospitalization of Upper GI Bleeding in High Risk PatientsBleeding in High Risk Patients
NNøøggåård et al. Aliment Pharmacol Ther 2004;19:817-25rd et al. Aliment Pharmacol Ther 2004;19:817-25
Patients with prior gastrointestinal diseasesPatients with prior gastrointestinal diseases
46% female 46% female Mean age >68 yrsMean age >68 yrs>22% with Hx of non-bleeding GI ulcer >22% with Hx of non-bleeding GI ulcer >70% Use of gastroprotective agent>70% Use of gastroprotective agent>21% Use of aspirin>21% Use of aspirin

A12
GI Safety Benefit - ConclusionsGI Safety Benefit - Conclusions
Medical need for improved GI safety is fulfilled Medical need for improved GI safety is fulfilled with celecoxib with celecoxib – Randomized Controlled TrialsRandomized Controlled Trials
Celecoxib has a favorable GI safety profile Celecoxib has a favorable GI safety profile vs NSAIDsvs NSAIDs
– Epidemiology StudiesEpidemiology Studies Celecoxib is associated with a lower risk Celecoxib is associated with a lower risk
of hospitalization due to GI bleeding than of hospitalization due to GI bleeding than NSAIDsNSAIDs

A13
Thromboembolic CV Adverse Events:Thromboembolic CV Adverse Events:VIGOR and CLASS StudiesVIGOR and CLASS Studies
DaysDays00 4040 8080 120120 160160 200200 240240 280280 320320 360360
VIGORVIGOR
PPPPPPPPPPPPPPPPPP
PPPPPPPPPPPPPPPPPPPPPPPPPPPPPP
RR
RRRR
RRRRRRRRRRRRRR
RRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRR
RRRRRRRRRRRRRRRRRRRRRRRRRR00
0.50.5
1.01.0
1.51.5
2.02.0
2.52.5
RR Rofecoxib 50 mg qd (n=4047)Rofecoxib 50 mg qd (n=4047)
Naproxen 500 mg bid (n=4029)Naproxen 500 mg bid (n=4029)QQ
p < 0.05p < 0.05
White et al. Am J Cardiol;2002:89:425-430White et al. Am J Cardiol;2002:89:425-430 www.fda.gov/ohrms/dockets/ac/01/briefing/3677b2_6_cardio.docwww.fda.gov/ohrms/dockets/ac/01/briefing/3677b2_6_cardio.doc
% o
f P
atie
nts
% o
f P
atie
nts
JJ Celecoxib 400 mg bid (n=3987)Celecoxib 400 mg bid (n=3987)
PP NSAIDs (n=3981)NSAIDs (n=3981)
CLASSCLASS
JJJJJJJJJJJJJJ
JJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJJ
PPPPPPPPPPPPPPPP
PPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPP
PPPPPPPPPPPPPPPPPPPPPPPPPP00
0.50.5
1.01.0
1.51.5
2.02.0
2.52.5
pp = 0.973= 0.973
DaysDays00 4040 8080 120120 160160 200200 240240 280280 320320 360360
PPPP
% o
f P
atie
nts
% o
f P
atie
nts

A14
Overview Overview
Celecoxib - CV safety vs placebo Celecoxib - CV safety vs placebo
– Longer-term studiesLonger-term studies
Celecoxib – CV safety vs NSAIDsCelecoxib – CV safety vs NSAIDs
– Meta analysis of RCTs Meta analysis of RCTs
– Risk factorsRisk factors
– Epidemiology studiesEpidemiology studies
– Considerations of mechanism Considerations of mechanism
Conclusions: Risk-benefitConclusions: Risk-benefit

A15
Overview Overview
Celecoxib - CV safety vs placebo Celecoxib - CV safety vs placebo
– Longer-term studiesLonger-term studies
Celecoxib – CV safety vs NSAIDsCelecoxib – CV safety vs NSAIDs
– Meta analysis of RCTs Meta analysis of RCTs
– Risk factorsRisk factors
– Epidemiology studiesEpidemiology studies
– Considerations of mechanism Considerations of mechanism
Conclusions: Risk-benefitConclusions: Risk-benefit

A16
CV Event DefinitionsCV Event Definitions APTC* composite endpoint APTC* composite endpoint
– non-fatal myocardial infarctions, non-fatal myocardial infarctions, – non-fatal strokes,non-fatal strokes, or or – vascular deathsvascular deaths ( (all deaths attributed to cardiac, all deaths attributed to cardiac,
cerebral, hemorrhagic,cerebral, hemorrhagic, embolic, other vascular, embolic, other vascular, or unknown causes)or unknown causes)
Meta-analysis – similar construct to APTC; based Meta-analysis – similar construct to APTC; based upon investigator reports of serious adverse eventsupon investigator reports of serious adverse events
Epidemiologic studies - hospitalization for acute MI alone Epidemiologic studies - hospitalization for acute MI alone or plus coronary death (1 study with APTC endpoint)or plus coronary death (1 study with APTC endpoint)
*Antiplatelet Trialists Collaboration. *Antiplatelet Trialists Collaboration. BMJBMJ. 1994;308:81-106. 1994;308:81-106

A17
Sporadic Adenoma Prevention Trials (SAP)Sporadic Adenoma Prevention Trials (SAP)
Colorectal adenomas: precursors of colon cancerColorectal adenomas: precursors of colon cancer Over-expression of COX-2 (pre-cancer, cancer, Over-expression of COX-2 (pre-cancer, cancer,
metastatic disease)metastatic disease) Two celecoxib SAP trials (still ongoing)Two celecoxib SAP trials (still ongoing)
– APC (005) & PreSAP (018)APC (005) & PreSAP (018)– 3 year placebo controlled RCTs3 year placebo controlled RCTs– Hypothesis: celecoxib will reduce polyp Hypothesis: celecoxib will reduce polyp
recurrence by >35% in a high risk cohort recurrence by >35% in a high risk cohort (prior adenoma).(prior adenoma).
Setting allowed for first longer-term placebo comparison; Setting allowed for first longer-term placebo comparison; Celecoxib - agent of choice based on GI safety Celecoxib - agent of choice based on GI safety

A18
APCAPC Pre-SAP Pre-SAP
Study DescriptionStudy Description
Number of patientsNumber of patients 20352035 15611561
Pt-yearsPt-years 47784778 39393939
Mean exposure (yrs)Mean exposure (yrs) 2.32.3 2.52.5
Number of CV eventsNumber of CV events 4141 3131
Mean age (yrs)Mean age (yrs) 6060 6161
Hx of hypertensionHx of hypertension 41%41% 35%35%
Hx of CHDHx of CHD 39%39% 48%48%
Concomitant aspirinConcomitant aspirin 30%30% 16%16%
Sources Available to Evaluate CV Safety Sources Available to Evaluate CV Safety of Celecoxibof Celecoxib
Patient PopulationPatient Population

A19
Alzheimer’s Disease Anti-Inflammatory Alzheimer’s Disease Anti-Inflammatory Prevention Trial (ADAPT)Prevention Trial (ADAPT)
RCT evaluating celecoxib 200 mg bid or RCT evaluating celecoxib 200 mg bid or naproxen 220 mg bid vs placebo naproxen 220 mg bid vs placebo – Elderly population (>70 yrs) at risk for AD Elderly population (>70 yrs) at risk for AD
(first degree relative with the disease)(first degree relative with the disease)– Except for uncontrolled hypertension, no other Except for uncontrolled hypertension, no other
restrictions for CV diseaserestrictions for CV disease– Hypothesis: celecoxib will reduce the incidence Hypothesis: celecoxib will reduce the incidence
of AD by >30% in a high risk cohort.of AD by >30% in a high risk cohort.
First longer-term placebo-controlled trial with an NSAIDFirst longer-term placebo-controlled trial with an NSAID

A20
APCAPC Pre-SAP Pre-SAP ADAPTADAPT
Study DescriptionStudy Description
Number of patientsNumber of patients 20352035 15611561 24632463
Pt-yearsPt-years 47784778 39393939 38883888
Mean exposure (yrs)Mean exposure (yrs) 2.32.3 2.52.5 1.61.6
Number of CV eventsNumber of CV events 4141 3131 ~70~70
Mean age (yrs)Mean age (yrs) 6060 6161 >70>70
Hx of hypertensionHx of hypertension 41%41% 35%35% n/an/a
Hx of CHDHx of CHD 39%39% 48%48% n/an/a
Concomitant aspirinConcomitant aspirin 30%30% 16%16% n/an/a
Sources Available to Evaluate CV Safety Sources Available to Evaluate CV Safety of Celecoxibof Celecoxib
Patient PopulationPatient Population

A21
CV Safety of Chronic Celecoxib vs Placebo – CV Safety of Chronic Celecoxib vs Placebo – Conclusions: Longer-term StudiesConclusions: Longer-term Studies
Three longer-term placebo-controlled trials with Three longer-term placebo-controlled trials with celecoxibcelecoxib
– APC - showed a CV risk with celecoxib vs APC - showed a CV risk with celecoxib vs placebo after ~1 yr of continuous treatmentplacebo after ~1 yr of continuous treatment
– Pre-SAP - no differences observed with Pre-SAP - no differences observed with continuous treatment of celecoxib up to 3 yrs continuous treatment of celecoxib up to 3 yrs
– ADAPT - Naproxen showed a CV risk (over 1.5 yrs) ADAPT - Naproxen showed a CV risk (over 1.5 yrs) vs placebo, in contrast to celecoxibvs placebo, in contrast to celecoxib
Celecoxib requires further study to estimate longer-term Celecoxib requires further study to estimate longer-term CV risks; an NSAID comparator in such a trial is critical CV risks; an NSAID comparator in such a trial is critical

A22
Overview Overview
Celecoxib - CV safety vs placebo Celecoxib - CV safety vs placebo
– Longer-term studiesLonger-term studies
Celecoxib – CV safety vs NSAIDsCelecoxib – CV safety vs NSAIDs
– Meta analysis of RCTs Meta analysis of RCTs
– Risk factorsRisk factors
– Epidemiology studiesEpidemiology studies
– Considerations of mechanism Considerations of mechanism
Conclusions: Risk-benefitConclusions: Risk-benefit

A23
Cardiovascular Safety of Celecoxib: Meta-analysis of RCTs
41 completed randomized controlled trials and a total of 44,307 treated patients (>91% OA/RA) – 24,932 celecoxib-treated patients– 4,057 placebo-treated patients– 15,318 patients treated with active comparators
Celecoxib doses; 50 – 800 mg daily Primary NSAIDs – naproxen, ibuprofen, diclofenac Study duration – 2 wks to 1 yr
Celecoxib exposureCelecoxib exposure >> 3 months – 11206 (55%) of patients 3 months – 11206 (55%) of patients>> 9 months – 2472 (12%) of patients 9 months – 2472 (12%) of patients>> 1 yr – 803 (4%) of patients 1 yr – 803 (4%) of patients

A24
Meta-analysis: CV Endpoints
Composite endpoint of any CV death, non-fatal MI or non-fatal stroke– Any CV death– Non-fatal MI – Non-fatal stroke

A25
APCAPC Pre-SAP Pre-SAP ADAPTADAPT Meta-analysis of RCTsMeta-analysis of RCTs
2 wks – 1 yr2 wks – 1 yr
Study DescriptionStudy Description
vs. vs. PlaceboPlacebo
vs. vs.
NSAIDs NSAIDs
Number of patientsNumber of patients 20352035 15611561 24632463 1151911519 3376333763
Pt-yearsPt-years 47784778 39393939 38883888 18531853 1003710037
Mean exposure (yrs)Mean exposure (yrs) 2.32.3 2.52.5 1.61.6 0.160.16 0.300.30
Number of CV eventsNumber of CV events 4141 3131 ~70~70 3131 111111
Mean age (yrs)Mean age (yrs) 6060 6161 >70>70 5959 6060
Hx of hypertensionHx of hypertension 41%41% 35%35% n/an/a 45%45% 25%25%
Hx of CHDHx of CHD 39%39% 48%48% n/an/a 22%22% 10%10%
Concomitant aspirinConcomitant aspirin 30%30% 16%16% n/an/a 13%13% 11%11%
Sources Available to Evaluate CV Safety Sources Available to Evaluate CV Safety of Celecoxibof Celecoxib
Patient PopulationPatient Population

A26
CV Death, MI and Stroke:CV Death, MI and Stroke:Celecoxib vs. NSAIDs Celecoxib vs. NSAIDs
CelecoxibCelecoxib 200 mg 200 mgN=19773N=19773
NSAIDsNSAIDs
N=13990N=13990
Patient-yearsPatient-years 56515651 43864386
Mean exposure/patient (mos.)Mean exposure/patient (mos.) 3.43.4 3.83.8
CV death, MI, strokeCV death, MI, stroke 57 (1.0)57 (1.0) 54 (1.2)54 (1.2)
CV deathCV death 15 (0.3)15 (0.3) 19 (0.4)19 (0.4)
MIMI 35 (0.6)35 (0.6) 19 (0.4)19 (0.4)
StrokeStroke 7 (0.1)7 (0.1) 16 (0.4)16 (0.4)
n (events per 100 patient-years)n (events per 100 patient-years)

A27
0.86 (0.59, 1.26)0.86 (0.59, 1.26)
0.72 (0.37, 1.39)0.72 (0.37, 1.39)
1.49 (0.82, 2.70)1.49 (0.82, 2.70)
Celecoxib daily dose Celecoxib daily dose >> 200 mg 200 mg
0.33 (0.14, 0.78)0.33 (0.14, 0.78)
CV death, MI, or strokeCV death, MI, or stroke
CV deathCV death
MIMI
StrokeStroke
Favors celecoxibFavors celecoxib Favors NSAIDsFavors NSAIDs
0.1 1.0 10.00.30.3 3.03.0
Relative Risk (95%CI)Relative Risk (95%CI)
CV Death, MI and Stroke:CV Death, MI and Stroke:Celecoxib vs. NSAIDs Celecoxib vs. NSAIDs

A28
1.26 (0.57, 2.80)
0.86 (0.59, 1.26)
0.81 (0.49, 1.35)
0.88 (0.43, 1.82)
Celecoxib daily dose > 200 mg
1.11 (0.41, 3.01)
vs. Placebo
vs. NSAID
vs. Naproxen
vs. Diclofenac
vs. Ibuprofen
0.1 1.0 10.0
Favors celecoxib Favors comparator
0.3 3.0
Relative Risk (95%CI)Relative Risk (95%CI)
CV Death, MI and Stroke:Celecoxib vs. Pbo, NSAIDs Combined & Individually

A29
0.86 (0.59, 1.26)0.86 (0.59, 1.26)
0.93 (0.52, 1.68)0.93 (0.52, 1.68)
0.75 (0.34, 1.67)0.75 (0.34, 1.67)
0.91 (0.53, 1.58)0.91 (0.53, 1.58)
200 mg200 mg
200 mg200 mg
400 mg400 mg
800 mg800 mg
Favors celecoxibFavors celecoxib Favors NSAIDsFavors NSAIDs
0.10.1 1.01.0 10.010.00.30.3 3.03.0
CV Death, MI and Stroke:CV Death, MI and Stroke:Celecoxib vs. NSAIDs: By Dose Celecoxib vs. NSAIDs: By Dose
Relative Risk (95%CI)Relative Risk (95%CI)

A30
CV Death, MI and Stroke:CV Death, MI and Stroke:CLASS and CAESAR StudiesCLASS and CAESAR Studies
PPPP PP
PP JJ
PP PP
PPPP PP
PP PPPPPP
PPPPPP PPPP PP PP PPPP
PP PP PPPPPPPP
PP PPPP
PP
PPPP
JJJJ JJ
JJ
JJ
JJ
JJ
JJJJ
JJ
JJ
JJJJ
JJJJ JJ
JJ JJJJ
JJ
JJ JJ
JJJJJJ JJJJ
JJ
3.03.0
2.02.0
1.01.0
00 3030 6060 9090 120120 150150 180180 210210 240240 270270 300300 330330 360360 390390
Celecoxib 200 – 800 mg daily, n=4445Celecoxib 200 – 800 mg daily, n=4445
NSAIDs (diclofenac, ibuprofen), n=4439NSAIDs (diclofenac, ibuprofen), n=4439
% o
f P
atie
nts
% o
f P
atie
nts
DaysDays
PP
JJ
p = 0.601, by log rank testp = 0.601, by log rank test
JJ
00
JJ

A31
CV Safety in RCTs - ConclusionsCV Safety in RCTs - Conclusions
No association for increased CV risk No association for increased CV risk detected with use of celecoxib up to 1 yr detected with use of celecoxib up to 1 yr compared to: compared to: – NSAIDs combined NSAIDs combined – naproxen, diclofenac or ibuprofen individuallynaproxen, diclofenac or ibuprofen individually
A dose-related increase in CV risk with A dose-related increase in CV risk with celecoxib is not observedcelecoxib is not observed

A32
Overview Overview
Celecoxib - CV safety vs placebo Celecoxib - CV safety vs placebo
– Longer-term studiesLonger-term studies
Celecoxib – CV safety vs NSAIDsCelecoxib – CV safety vs NSAIDs
– Meta analysis of RCTs Meta analysis of RCTs
– Risk factorsRisk factors
– Epidemiology studiesEpidemiology studies
– Considerations of mechanism Considerations of mechanism
Conclusions: Risk-benefitConclusions: Risk-benefit

A33
0.00.0
1.01.0
2.02.0
3.03.0
CV dea
th, M
I, st
roke
CV dea
th, M
I, st
roke
CV dea
th
CV dea
th MIMI
Stroke
Stroke
Eve
nts
per
100
pt
yrs
Eve
nts
per
100
pt
yrs
0.00.0
1.01.0
2.02.0
3.03.0
CV dea
th, M
I, st
roke
CV dea
th, M
I, st
roke
CV dea
th
CV dea
th MIMI
Stroke
Stroke
No Risk Factors (n = 21,974)No Risk Factors (n = 21,974)
Celecoxib Celecoxib 200 mg 200 mg NSAIDsNSAIDs
CV Death, MI and Stroke:CV Death, MI and Stroke:Celecoxib vs. NSAIDs – By CV Risk Factors*Celecoxib vs. NSAIDs – By CV Risk Factors*
*Hypertension, diabetes, hyperlipidemia, CHD *Hypertension, diabetes, hyperlipidemia, CHD
1 Risk Factor (n = 6,710)1 Risk Factor (n = 6,710) 2 Risk Factors (n = 5,079)2 Risk Factors (n = 5,079)

A34 Celecoxib daily dose Celecoxib daily dose >> 200 mg 200 mg
CV Death, MI and Stroke:CV Death, MI and Stroke:Celecoxib vs. NSAIDs – By CV Risk Factors*Celecoxib vs. NSAIDs – By CV Risk Factors*
*Hypertension, diabetes, hyperlipidemia, CHD *Hypertension, diabetes, hyperlipidemia, CHD
No CV Risk FactorsNo CV Risk Factors 1 CV Risk Factor1 CV Risk Factor 2 CV Risk Factors2 CV Risk Factors
0.10.1 1.01.0 10.010.0Favors celecoxibFavors celecoxib Favors NSAIDsFavors NSAIDs
CV death, MI, or strokeCV death, MI, or stroke
CV deathCV death
MIMI
StrokeStroke
0.10.1 1.01.0 10.010.0 0.10.1 1.01.0 10.010.0Favors celecoxibFavors celecoxib Favors NSAIDsFavors NSAIDs Favors celecoxibFavors celecoxib Favors NSAIDsFavors NSAIDs
Relative Risk (95%CI)Relative Risk (95%CI) Relative Risk (95%CI)Relative Risk (95%CI) Relative Risk (95%CI)Relative Risk (95%CI)
0.30.3 3.03.0 0.30.3 3.03.0 0.30.3 3.03.0
Cohort size = 21,974Cohort size = 21,974 Cohort size = 6,710Cohort size = 6,710 Cohort size = 5,079Cohort size = 5,079

A35
CV Death, MI and Stroke:CV Death, MI and Stroke:Celecoxib vs. NSAIDs – By Aspirin UseCelecoxib vs. NSAIDs – By Aspirin Use
Celecoxib daily dose Celecoxib daily dose >> 200 mg 200 mg
AspirinAspirinNo AspirinNo Aspirin
0.10.1 1.01.0 10.010.0
Favors celecoxibFavors celecoxib Favors NSAIDsFavors NSAIDs
0.30.3 3.03.0 0.10.1 1.01.0 10.010.00.30.3 3.03.0
0.67 (0.40, 1.13)0.67 (0.40, 1.13)
0.60 (0.29, 1.24)0.60 (0.29, 1.24)
1.17 (0.44, 3.09)1.17 (0.44, 3.09)
0.41 (0.13, 1.25)0.41 (0.13, 1.25)
CV death, MI, or strokeCV death, MI, or stroke
CV deathCV death
MIMI
StrokeStroke
1.17 (0.65, 2.12)1.17 (0.65, 2.12)
1.73 (0.31, 9.79)1.73 (0.31, 9.79)
1.74 (0.81, 3.73)1.74 (0.81, 3.73)
0.25 (0.06, 0.95)0.25 (0.06, 0.95)
Favors celecoxibFavors celecoxib Favors NSAIDsFavors NSAIDs
Relative Risk (95%CI)Relative Risk (95%CI) Relative Risk (95%CI)Relative Risk (95%CI)
Cohort size = 29,954Cohort size = 29,954 Cohort size = 3,809Cohort size = 3,809

A36
PPPP
CV Death, MI and Stroke:CV Death, MI and Stroke:CLASS StudyCLASS Study
PPPP
P0P0 PP
PPPPPPPPPPPPPP
JJ
JJJJJJJJ
JJPPJJJJJJ
6060 9090 120120 150150 180180 210210 240240 270270 300300 330330 360360 390390303000
1.01.0
2.02.0
3.03.0
PP
JJ
No AspirinNo Aspirin
4.04.0
p p = 0.333= 0.333Log-rank testLog-rank test
% o
f P
atie
nts
% o
f P
atie
nts
Celecoxib 400 mg BID (n=3105)Celecoxib 400 mg BID (n=3105)NSAIDs (n=3124)NSAIDs (n=3124)
JJ
PP
6060 9090 120120 150150 180180 210210 240240 270270 300300 330330 360360 390390303000
1.01.0
2.02.0
3.03.0
AspirinAspirin
PP
JJ
PP
JJ
PP
JJ
PPJJ
JJ
JJ
JJ
JJ
JJJJ
JJJJJJ
JJ
JJJJ
PPPPPP
PP
PP
PP
PP
JJ
4.04.0
p p = 0.666= 0.666Log-rank testLog-rank test
Celecoxib 400 mg BID (n=882)Celecoxib 400 mg BID (n=882)NSAIDs (n=857)NSAIDs (n=857)
JJ
PP PP
DaysDays

A37
Risk Factors - ConclusionRisk Factors - Conclusion
The CV safety profile of celecoxib remains The CV safety profile of celecoxib remains comparable to NSAIDs regardless of CV risk comparable to NSAIDs regardless of CV risk factors factors
– as determined by medical history or use as determined by medical history or use of low dose aspirinof low dose aspirin

A38
Overview Overview
Celecoxib - CV safety vs placebo Celecoxib - CV safety vs placebo
– Longer-term studiesLonger-term studies
Celecoxib – CV safety vs NSAIDsCelecoxib – CV safety vs NSAIDs
– Meta analysis of RCTs Meta analysis of RCTs
– Risk factorsRisk factors
– Epidemiology studiesEpidemiology studies
– Considerations of mechanism Considerations of mechanism
Conclusions: Risk-benefitConclusions: Risk-benefit

A39
Risk of Risk of MI with COXIBsMI with COXIBs
Ray WA et al. Ray WA et al. Lancet 2002Lancet 2002
Mamdani M et al. Mamdani M et al. Arch Intern Med 2003Arch Intern Med 2003
Solomon DH et al. Solomon DH et al. Circulation 2004Circulation 2004
Kimmel SE Kimmel SE et al. et al. Ann Intern Med 2005Ann Intern Med 2005
Graham DJ et al. Graham DJ et al. Lancet 2005Lancet 2005
Lévesque LE et al.Lévesque LE et al. Ann Intern Med 2005Ann Intern Med 2005
Shaya FT et al.Shaya FT et al. Arch Intern Med 2005Arch Intern Med 2005

A40
Risk of MI and UseRisk of MI and Use of COXIBs of COXIBs
Epidemiological StudiesEpidemiological Studies
Number of events*Number of events*
TotalTotal 30,36730,367
CelecoxibCelecoxib 1,0051,005
Number of patientsNumber of patients CohortCohort Case-controlCase-control
TotalTotal 2,135,8672,135,867 12,613 / 50,38012,613 / 50,380
CelecoxibCelecoxib 94,16994,169 443 / 1,802443 / 1,802
Person-yearsPerson-years
TotalTotal 2,795,4522,795,452 NANA
CelecoxibCelecoxib 12,64712,647††
Source dataSource data Cohort/nested - Mamdani M, Ray WA, Graham DJ, Shaya FT, Cohort/nested - Mamdani M, Ray WA, Graham DJ, Shaya FT, Lévesque LELévesque LECase-control - Solomon DH, Kimmel SECase-control - Solomon DH, Kimmel SE
* Ray WA and Graham DJ include MI and CHD death. Kimmel SE non-fatal MI only* Ray WA and Graham DJ include MI and CHD death. Kimmel SE non-fatal MI only
†† Person-time of exposure to celecoxib not provided in studies of Graham DJ, Shaya FT, and Lévesque LE.Person-time of exposure to celecoxib not provided in studies of Graham DJ, Shaya FT, and Lévesque LE.Number of cases exposed to celecoxib not provided in Shaya FT.Number of cases exposed to celecoxib not provided in Shaya FT.

A41
1.701.70
11
0.930.930.910.91
1.031.03
0.960.96 0.940.94
00
11
22
33
Non-useNon-use naproxennaproxen celecoxibcelecoxib
>>300mg300mgrofecoxibrofecoxib
>25mg>25mg
Ad
just
ed
Ra
te R
ati
oA
dju
ste
d R
ate
Ra
tio
Ray et al. Lancet 2002; 360:1071-73Ray et al. Lancet 2002; 360:1071-73
ibuprofenibuprofen celecoxibcelecoxib
<300mg<300mgrofecoxibrofecoxib
<<25mg25mg
Relative Risk of Relative Risk of MI/Coronary DeathMI/Coronary Death: : Use of COXIBs or NSAIDs vs. Non-useUse of COXIBs or NSAIDs vs. Non-use
mean age >60 yrsmean age >60 yrs66% women66% women37% with Hx of major CV disease 37% with Hx of major CV disease
Celecoxib Celecoxib 22,337 users22,337 users 3 months mean exposure3 months mean exposure

A42 Mamdani et al. Arch Intern Med 2003;163:481-86Mamdani et al. Arch Intern Med 2003;163:481-86
Relative Risk of Relative Risk of MIMI: : Use of COXIBs or NSAIDs vs. Non-useUse of COXIBs or NSAIDs vs. Non-use
mean age >75 yrsmean age >75 yrs>56% women>56% women>5% with Hx of MI, >5% with Hx of MI, >9% with Hx of CHD>9% with Hx of CHD
Celecoxib Celecoxib 15,271 users15,271 users 5.5 months mean follow-up5.5 months mean follow-up
1.201.201.001.00
0.900.90
1.001.0011
00
11
22
33
Non-useNon-use celecoxibcelecoxib rofecoxibrofecoxib naproxennaproxen otherotherNSAIDsNSAIDs
Ad
just
ed
Ra
te R
ati
oA
dju
ste
d R
ate
Ra
tio

A43
Non-use Non-use celecoxibcelecoxib celecoxibcelecoxib<< 200 mg 200 mg
celecoxibcelecoxib> 200 mg> 200 mg
rofecoxibrofecoxib rofecoxibrofecoxib<< 25 mg 25 mg
rofecoxibrofecoxib> 25 mg> 25 mg
Solomon et al. Circulation 2004;109:2068-73 &Solomon et al. Circulation 2004;109:2068-73 &Arthritis Rheum 2003;48 (Suppl 9) S697 (Presentation Arthritis Rheum 2003;48 (Suppl 9) S697 (Presentation ACR Oct 2003)ACR Oct 2003)
Relative Risk of Relative Risk of MIMI: : Use of COXIBs vs. Non-useUse of COXIBs vs. Non-use
1.581.58
1.141.140.940.94
1.111.11
0.930.93 0.920.9211
00
11
22
33
Ad
just
ed
Od
ds
Ra
tio
Ad
just
ed
Od
ds
Ra
tio
mean age >80 yrsmean age >80 yrs77% women77% women57% with Hx of Htn57% with Hx of Htn14% with Hx of 14% with Hx of anginaangina9% with Hx of MI 9% with Hx of MI

A44 Kimmel et al. Ann Intern Med 2005; 142:157-164Kimmel et al. Ann Intern Med 2005; 142:157-164
Relative Risk of Relative Risk of MIMI: : Use of COXIBs or NSAIDs vs. Non-useUse of COXIBs or NSAIDs vs. Non-use
Ad
just
ed
Od
ds
Ra
tio
Ad
just
ed
Od
ds
Ra
tio
0.610.610.430.43
1.161.1611
00
11
22
33
Non-useNon-use celecoxibcelecoxib rofecoxibrofecoxib NSAIDsNSAIDs
mean age >52 yrsmean age >52 yrs59% women59% women31% with Hx of Htn31% with Hx of Htn4% with Hx of angina/CHD 4% with Hx of angina/CHD

A45
1.301.301.601.60
11 1.231.23
0.840.84
1.141.14
3.003.00
1.061.06
00
11
22
33
44
Remote
use
Remote
use
celecoxib
celecoxib
rofe
coxib
rofe
coxib << 25 m
g
25 mg
rofe
coxib >
25 mg
rofe
coxib >
25 mg
ibupro
fen
ibupro
fen
naproxen
naproxen
indom
ethacin
indom
ethacin
diclofe
nac
diclofe
nac
Ad
just
ed
Od
ds
Ra
tio
Ad
just
ed
Od
ds
Ra
tio
Relative Risk of Relative Risk of MI/Coronary DeathMI/Coronary Death: : Use of COXIBs or NSAIDs vs. Remote-useUse of COXIBs or NSAIDs vs. Remote-use
Graham et al. Lancet 2005;365:475-481Graham et al. Lancet 2005;365:475-481
mean age >66 yrsmean age >66 yrs38% women38% women1% with Hx of MI/ 1% with Hx of MI/ revascularizationrevascularization

A46
0.990.991.091.09 1.191.1911
00
11
22
33
Non-naproxenNon-naproxenNSAIDsNSAIDs
COXIBsCOXIBs celecoxibcelecoxib rofecoxibrofecoxib
Ad
just
ed O
dd
s R
atio
Ad
just
ed O
dd
s R
atio
Relative Risk of CV Death, MI or StrokeRelative Risk of CV Death, MI or StrokeUse of COXIBs vs. Non-Use of COXIBs vs. Non-naproxennaproxen NSAIDs NSAIDs
Shaya et al. Arch Intern Med 2005;165:181-6Shaya et al. Arch Intern Med 2005;165:181-6
11% >60 yrs11% >60 yrs70% women70% women43% with Hx of Htn43% with Hx of Htn12% with Hx of CV event 12% with Hx of CV event

A47
1.061.06 1.001.0011 1.001.000.980.98
1.171.171.211.21
1.731.73
00
11
22
33
Non-use
Non-use
celecoxib
celecoxib << 200 m
g
200 mg
celecoxib >
200 mg
celecoxib >
200 mg
rofe
coxib
rofe
coxib << 25 m
g
25 mg
rofe
coxib >
25 mg
rofe
coxib >
25 mg
naproxen
naproxen
melo
xicam
melo
xicam
other N
SAIDs
other N
SAIDs
Relative Risk of Relative Risk of MIMI::Use of COXIBs or NSAIDs vs. Use of COXIBs or NSAIDs vs. NonNon-use-use
Ad
just
ed
Ra
te R
ati
oA
dju
ste
d R
ate
Ra
tio
LévesqueLévesque et al. Ann Intern Med 2005;142(7), www.annals.org et al. Ann Intern Med 2005;142(7), www.annals.org
mean age >78 yrsmean age >78 yrs67% women67% women50% with Hx of Htn50% with Hx of Htn17% with Hx of CHD 17% with Hx of CHD

A48
Non-use
Non-use
Celec
oxib
Celec
oxib <<
200
mg
200
mg
Celec
oxib >
200
mg
Celec
oxib >
200
mg
Rofeco
xib
Rofeco
xib <<
25
mg
25
mg
Rofeco
xib >
25
mg
Rofeco
xib >
25
mg
Non-use
Non-use
Celec
oxib
Celec
oxib <<
200
mg
200
mg
Celec
oxib >
200
mg
Celec
oxib >
200
mg
Rofeco
xib
Rofeco
xib <<
25
mg
25
mg
Rofeco
xib >
25
mg
Rofeco
xib >
25
mg
1.041.04 1.161.161.381.38
1.231.23 1.001.00
0.910.91 0.800.80
2.362.36
11 11
00
11
22
33
44No ASA useNo ASA use ASA useASA use
Risk of MI by Risk of MI by ASA UseASA Use Relative Risk of COXIBs vs. Non-use Relative Risk of COXIBs vs. Non-use
Ad
just
ed
Ra
te R
ati
oA
dju
ste
d R
ate
Ra
tio
LévesqueLévesque et al. Ann Intern Med 2005;142(7), www.annals.org et al. Ann Intern Med 2005;142(7), www.annals.org

A49
1.231.23
3.003.00
0.940.94
11
0.920.920.960.96
1.031.03
0.980.98
1.111.11 1.211.21
0.940.94
1.001.00
1.701.70
1.581.58
1.731.73
00
11
22
33
44
Non-use
Non-use
Ray W
A
Ray W
A
Solom
on DH
Solom
on DH
Léves
que LE
Léves
que LE
Ray W
A
Ray W
A
Solom
on DH
Solom
on DH
Léves
que LE
Léves
que LE
Graham
DJ
Graham
DJ
Ray W
A
Ray W
A
Solom
on DH
Solom
on DH
Léves
que LE
Léves
que LE
Ray W
A
Ray W
A
Solom
on DH
Solom
on DH
Léves
que LE
Léves
que LE
Graham
DJ
Graham
DJ
Low doseLow dose High doseHigh dose**
celecoxibcelecoxib rofecoxibrofecoxib celecoxibcelecoxib rofecoxibrofecoxib
Summary of MI Risk by Dose:Summary of MI Risk by Dose:Relative Risk vs. Non-use/Remote UseRelative Risk vs. Non-use/Remote Use
*High-dose: *High-dose: rofecoxib >25 mgr/day rofecoxib >25 mgr/day celecoxib >200 mg/day in Solomon DH and Lévesque LE celecoxib >200 mg/day in Solomon DH and Lévesque LE celecoxib celecoxib >> 300 mg/day in Ray WA 300 mg/day in Ray WA
Re
lati
ve
Ris
kR
ela
tiv
e R
isk

A50
CV Epidemiology Studies - ConclusionsCV Epidemiology Studies - Conclusions
The risk of MI with celecoxib as used in the The risk of MI with celecoxib as used in the real world population (dose & duration) real world population (dose & duration)
– is consistently similar to nonselective is consistently similar to nonselective NSAIDs, and non- or remote use of NSAIDs, and non- or remote use of NSAIDsNSAIDs
– These findings are in contrast to These findings are in contrast to increased risk with rofecoxibincreased risk with rofecoxib
The available data suggest that the risk of The available data suggest that the risk of MI is similar for low and high celecoxib MI is similar for low and high celecoxib dosesdoses

A51
Overview Overview
Celecoxib - CV safety vs placebo Celecoxib - CV safety vs placebo
– Longer-term studiesLonger-term studies
Celecoxib – CV safety vs NSAIDsCelecoxib – CV safety vs NSAIDs
– Meta analysis of RCTs Meta analysis of RCTs
– Risk FactorsRisk Factors
– Epidemiology StudiesEpidemiology Studies
– Considerations of MechanismConsiderations of Mechanism
Conclusions: Risk-benefitConclusions: Risk-benefit

A52
Potential Mechanism(s) of CV Risk Potential Mechanism(s) of CV Risk
Hypothesis that attributes CV risk to COXIBs only;Hypothesis that attributes CV risk to COXIBs only;
Could explainCould explain– VIGOR, APPROVe and APC results VIGOR, APPROVe and APC results
Could not explain consistent comparability Could not explain consistent comparability between celecoxib and NSAIDsbetween celecoxib and NSAIDs– meta-analysismeta-analysis– vs non-use in epidemiology studiesvs non-use in epidemiology studies
Could not explain Pre-SAP and ADAPT results Could not explain Pre-SAP and ADAPT results

A53
Potential MechanismsPotential Mechanisms
NSAIDs may not provide ‘effective’ blockade NSAIDs may not provide ‘effective’ blockade of platelets – even though TxAof platelets – even though TxA2 2 production production
is reducedis reduced Does not account for other PGs produced Does not account for other PGs produced
from COX-2 (e.g. PGEfrom COX-2 (e.g. PGE22, TxA, TxA22))
Can PGICan PGI22/TxA/TxA22 imbalance lead to imbalance lead to
prothrombotic potential?prothrombotic potential?

A54
PP
*Significant difference from baseline; p<0.05 *Significant difference from baseline; p<0.05
HH Celecoxib 400 mg (n=9)Celecoxib 400 mg (n=9)BB Placebo (n=7)Placebo (n=7)
JJ Celecoxib 100 mg (n=7)Celecoxib 100 mg (n=7) FF Celecoxib 800 mg (n=7)Celecoxib 800 mg (n=7)
Ibuprofen 800 mg (n=7)Ibuprofen 800 mg (n=7)
HoursHours
**
BB BBHHFF FF FF
PP
PP
-100-100
-80-80
-60-60
-40-40
-20-20
00
2020
Pre-Pre-DoseDose
22 44 6600 242488
% (
Mea
n C
han
ge
% (
Mea
n C
han
ge
S
E)
SE
)
BB JJ
Platelet AggregationPlatelet Aggregation
Pharmacologic Responses to Celecoxib Pharmacologic Responses to Celecoxib and Ibuprofen and Ibuprofen
JJHHFFPP JJ HHJJ BBPPHH
McAdam et al. PNAS 1999;96:272-277McAdam et al. PNAS 1999;96:272-277**Significantly different from placebo; p<0.05
00
2525
5050
7575
100100
125125
150150
175175
200200
4-6 hrs 6-12 hrs
Urinary PGI-M
pg
/ mg
cre
atin
ine
NRNR NRNR
******** **** **** ****
****
NR = not reported

A55
PGIPGI22 TxATxA22 PGEPGE22
MMPsMMPs
Plaque stabilityPlaque stability
Endothelial Endothelial functionfunction
Platelet Platelet aggregationaggregation
Endothelial Endothelial functionfunction
Platelet Platelet aggregationaggregation
COX-2 Prostaglandins Linked to CV DiseaseCOX-2 Prostaglandins Linked to CV Disease
COX-2 expressionCOX-2 expression

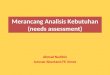
A56 Walter M et al. Atherosclerosis 177 (2004) 235-243Chikani G et al. Am J Physiol Endocrinol Metab 287 (2004): E386-E389
Rofecoxib and/or Reactive Metabolites
↑Ox-LDL↑F2-Isoprostanes
↑Blood Pressure /↑Atherothrombosis
↓Nitric Oxide Bioavailability
Putative Novel Rofecoxib Pathways Leading to Increased HTN and CV Risk

A57
24-Hour Mean SBP Change at 6 &12 Wks 24-Hour Mean SBP Change at 6 &12 Wks in OA Hypertensive Patientsin OA Hypertensive Patients
Sowers et al. Arch Int Med; 2005;165:161-168Sowers et al. Arch Int Med; 2005;165:161-168
-3-3
-2-2
-1-1
00
11
22
33
44
55
66
CelecoxibCelecoxib200 mg qd200 mg qd
n=136n=136
RofecoxibRofecoxib25 mg qd25 mg qd
n=138n=138
NaproxenNaproxen500 mg bid500 mg bid
n=130n=130
Mea
n S
BP
Ch
ang
e (m
m H
g)
Mea
n S
BP
Ch
ang
e (m
m H
g)
6 Wks6 Wks 12 Wks12 Wks 6 Wks6 Wks 12 Wks12 Wks 6 Wks6 Wks 12 Wks12 Wks
****
* p < 0.05 vs other treatments* p < 0.05 vs other treatments
SBP from ABPM dataSBP from ABPM data

A58
Mechanism SummaryMechanism Summary
It is not established that PGIIt is not established that PGI22/TxA/TxA22 imbalance imbalance
contributes to effects observed for COXIBs or contributes to effects observed for COXIBs or NSAIDsNSAIDs
Furthermore, the underlying pharmacology is Furthermore, the underlying pharmacology is more complex involving other PGs and more complex involving other PGs and pathways and raises the potential for benefit pathways and raises the potential for benefit with a COX-2 blockadewith a COX-2 blockade
Evidence for molecule-specific mechanisms is Evidence for molecule-specific mechanisms is emerging emerging

A59
Overview Overview
Celecoxib - CV safety vs placebo Celecoxib - CV safety vs placebo
– Longer-term studiesLonger-term studies
Celecoxib – CV safety vs NSAIDsCelecoxib – CV safety vs NSAIDs
– Meta analysis of RCTs Meta analysis of RCTs
– Risk FactorsRisk Factors
– Epidemiology StudiesEpidemiology Studies
– Considerations of Mechanism Considerations of Mechanism
Conclusions: Risk-benefitConclusions: Risk-benefit

A60
Summary of GI and CV Safety Summary of GI and CV Safety
Celecoxib vs NSAIDsCelecoxib vs NSAIDs– GI safetyGI safety
RCTs: lower incidence of clinically significant GI RCTs: lower incidence of clinically significant GI outcomesoutcomes
Epidemiology studies: similar risk of Epidemiology studies: similar risk of hospitalization for GI bleeding vs non-users hospitalization for GI bleeding vs non-users
– CV safetyCV safety RCTs: comparable CV safety profileRCTs: comparable CV safety profile Epidemiology studies: similar CV risk Epidemiology studies: similar CV risk
vs non-usersvs non-users

A61
Risk-Benefit of Celecoxib in Arthritis - Risk-Benefit of Celecoxib in Arthritis - ConclusionsConclusions
In the currently approved arthritis indications, In the currently approved arthritis indications, the risk-benefit of celecoxib remains positive the risk-benefit of celecoxib remains positive relative to NSAIDsrelative to NSAIDs– Comparable efficacy Comparable efficacy – GI safety benefit GI safety benefit – Comparable CV riskComparable CV risk
Shared uncertainty of the CV safety beyond Shared uncertainty of the CV safety beyond 1 year of continuous treatment 1 year of continuous treatment
Further studies are planned to evaluate the longer-term GI Further studies are planned to evaluate the longer-term GI and CV safety of celecoxib vs NSAIDs in arthritis patientsand CV safety of celecoxib vs NSAIDs in arthritis patients