Embed Size (px)
Citation preview
PLATELET TRANSFUSION
IN ONCOHAEMATOLOGY
Dr.René TARDIVELEtablissement Français du Sang
9th Maghreb Haematology Conference
Sousse 25-26 May 2012
Page 2
Indications for platelet transfusion
Central thrombocytopenia together with treatment of the cause
Thrombopathy, occasional
Peripheral thrombocytopenia, exceptional
Page 3
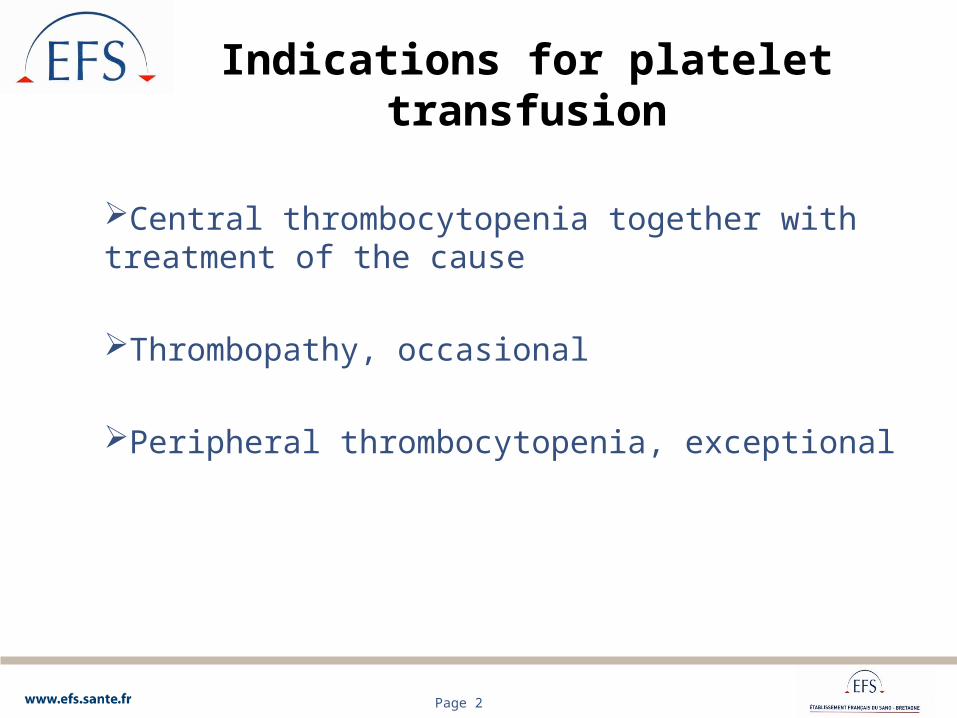
Platelet concentrates (1)
APC RPP
Origin Cell separatorsFrom total blood
CLP or BC
Composition 1 donation 4 to 6 donations
Quantity of platelets in 1011 2 to 8 3 to 5
Volume/ml 200-400 or more 200-350
Principal characteristics

Page 4
Platelet concentrates (2)
APC RPP
Separators•Haemonetics MCS ++•Terumo BCT Trima•Fenwal Amicus•Fresinus Comtec
Several program options by separators
2 products:• PRP• CLP or BC
2 techniques:• manual• automatic-Orbisac-TACSI
Principal characteristics

Page 5
Platelet concentrates (3)
Storage5 days (7 days in certain countries in the event of bacterial detection or attenuation of pathogens)Continuous agitation20-24 °Cconcentration: 1.2-1.5.106/mm3 (recommendations)
Page 6
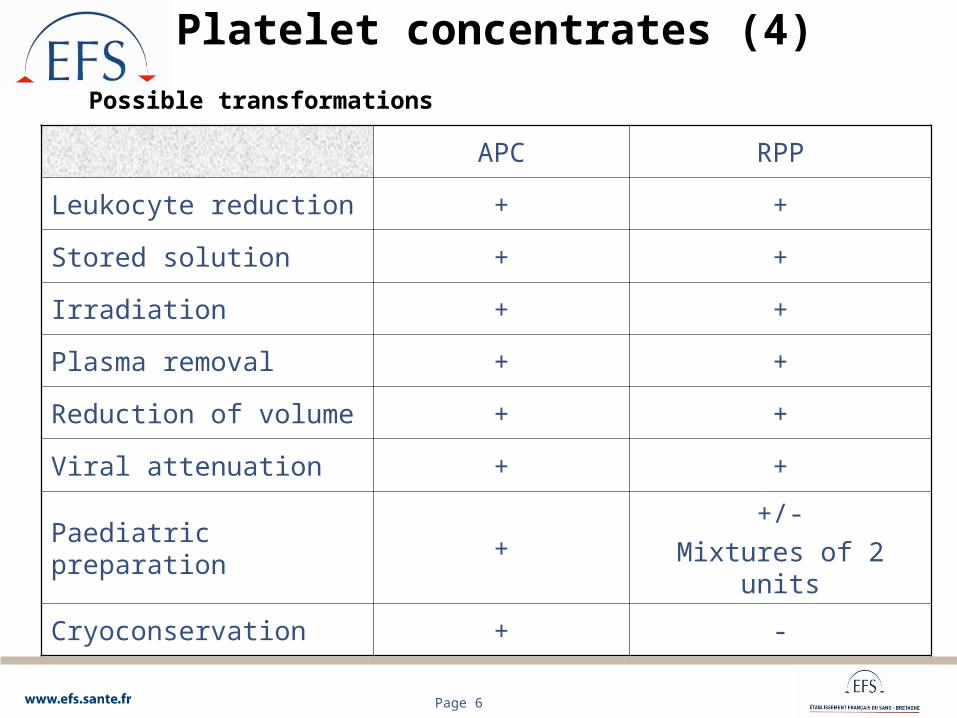
Platelet concentrates (4)
APC RPP
Leukocyte reduction + +
Stored solution + +
Irradiation + +
Plasma removal + +
Reduction of volume + +
Viral attenuation + +
Paediatric preparation ++/-
Mixtures of 2 units
Cryoconservation + -
Possible transformations
Page 7
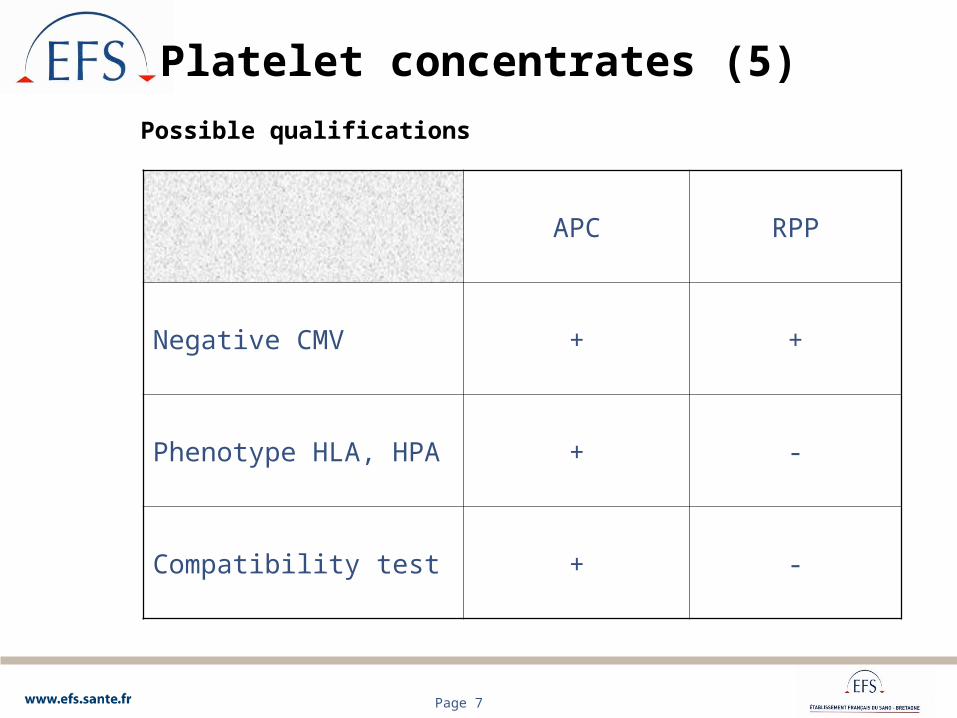
Platelet concentrates (5)
APC RPP
Negative CMV + +
Phenotype HLA, HPA + -
Compatibility test + -
Possible qualifications
Page 8
Platelet concentrates (6)
CPA or RPP
No difference in effectiveness
No difference in frequency of immunization
No product superior to another, but one may be better adapted to the patient

Page 9
Platelet transfusion indication
Preventive or curative?

Page 10
Platelet transfusion indication (1)
Curative
Patient presenting a haemorrhage

Page 11
Platelet transfusion indication (2)
Preventive
To prevent bleeding associated with thrombocytopenia and/or thrombopathy in a curable patient or a patient with a prolonged life expectancy (bone-marrow transplant, induction of L A,…)
Page 12
Platelet transfusion - PreventiveDose (1)
Numerous studies seems to show the advantage of strong doses of 4 to 5 10 11
Norol F and coll: Platelet transfusion has dose response study Blood 1998; 98:1448 - 1453Klumpp TR and coll: Clinical consequences of alterations in platelet transfusion dose: prospective, randomized, double-blind trial transfusion 1999; 39:674 - 681Sensebe et al: The efficacy of high-dose patient transfusions of platelets in hematology thrombocytopenic patients: result of prospective, randomized, open blinded end point (PROBE) study Blood 2005 105: 862-864

Page 13
Platelet transfusion - PreventiveDose (2)
However, other studies show that a low dose 2-3 1011 can also be effectiveTinmouth A et al: Low-dose prophylactic platelet transfusions in recipients of an autologous peripheral blood progenitor cell transplant and patients with acute leukemia: a randomized controlled trial with sequential Bayesian design. Transfusion 2004; 44: 1711-1719.Heddle NR et al (Best ISBT Working party) Study STOP low dose 1.5 -3.1011 versus standard amounts 4-6.1011. Study stopped in 2008 because of the higher frequency of haemorraging in the low-dose group Slichter S et al: Dose of Prophylactic Platelet Transfusions and Prevention of Hemorrhage N England journal of medicine 2010; 362:600 - 613
Page 14
Platelet transfusion - PreventiveDose (3)
Study PLADO (Optimal Platelet Dose Strategy for Management of Thrombocytopenia)
3 doses of platelets: 1.1-1011/m2
2.2-1011/m2
4.4-1011/m2
Low doses involve a reduction in the transfused platelets but increases the number of transfusions (5 versus 3 for average and high doses)Weak or strong doses do not have an effect on the frequency of the bleedingsNo significant difference when with the number of days before appearance of grade 2 bleeding or higher, no matter what the dose
Page 15
Platelet transfusion - Preventivetransfusional thresholds (1)
Pietersz R.N.I International Forum –Prophylactic platelet transfusion – Vox Sanguins 2012
14 responses by different countries
In the absence of risk factor10.109/l (except Russia and in certain indications from Japan
and the Netherlands: 5-109/l
Page 16
Platelet transfusion - Preventivetransfusional thresholds (2)
In the event of risk factors
Fever >38.5°C, evolutionary sepsis, coagulation anomaly, thrombopathy, anaemia, mucite, extensive purpura, haemorrhage inside the eye, HTA, anatomical lesions
Threshold up to 20.109/l

Page 17
Platelet transfusion - Preventivetransfusional thresholds (3)
Other situations
Invasive techniques: catheter, implantable chamber, fibroscopy, biopsy, broncho-alveolar washingSurgery, severe haemorrhage ,DIVC,…
Threshold raised to 50.109/l or above

Page 18
Platelet transfusion Dose in practice
Recommendation AFSSaPS or ANSM
• 0.5.1011 for every 7 kg of patient weight
• (or average dose suggested in PLADO study)

Page 19
Platelet transfusion
Evaluation of effectiveness
- Curative: Stopping bleeding
- Preventive: Increase in platelet count after transfusion Duration of transfusional effectiveness (3-4 days) Prevention of thrombocytopenia-related
haemorrhages
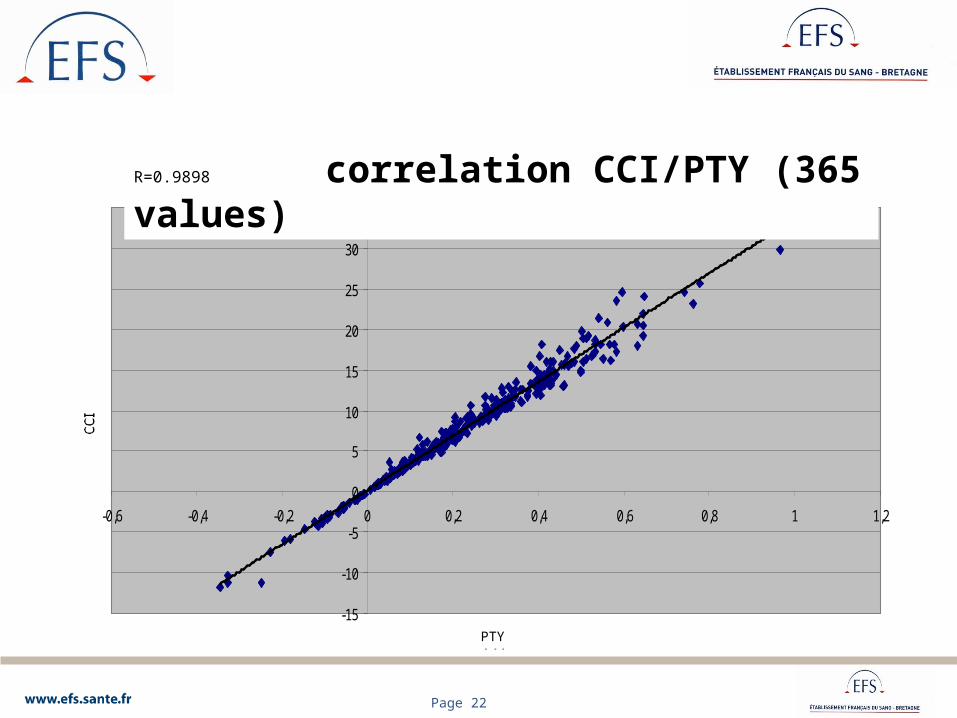
RTP > 20% and/or CCI > 7

Page 20
• Platelet transfusion yield (PTY)
[PC after transfusion-PC before transfusion] X weight (kg) X 0.075
PTY =
Number of platelets transfused (X 1011)
PC: platelet count
Page 21
• Corrected Count Increment (CCI)
[PC after transfusion - PC before transfusion] X body surface area (m2) X 100
CCI=
Number of platelets transfused (X 1011)
PC: platelet count
Page 22
correlation CCI / PTY (365 valeurs)
-15
-10
-5
0
5
10
15
20
25
30
35
-0,6 -0,4 -0,2 0 0,2 0,4 0,6 0,8 1 1,2
PTY
CCI
R = 0,9898
R=0.9898 correlation CCI/PTY (365 values)
PTY

Page 23
Data EFS BretagneCHU Rennes
Oncohaematology(Pr. Thierry Lamy)
Follow-up of the output of platelet transfusion
Page 24
Study of transfusion efficiency after transfusions of single donor-apheresis platelet concentrates
and random-donor platelet concentrates
J.VASSE, R.TARDIVEL, S.GAUCHERON, G.ANDREU,
G.SEMANAJune 2007

Page 25
RESULTS (1)
• From 05/05/2005 to 09/04/2007• 3496 platelet transfusions• 2354 SD-APC • 1141 RD-PC
Page 26
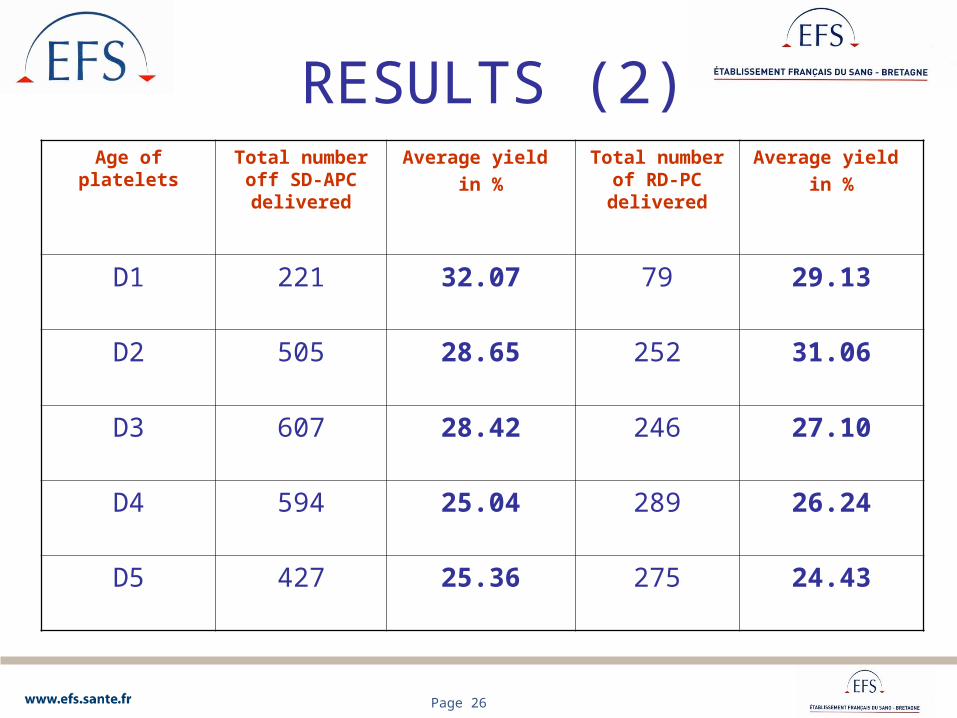
RESULTS (2)Age of
plateletsTotal number
off SD-APC delivered
Average yield in %
Total number of RD-PC delivered
Average yield in %
D1 221 32.07 79 29.13
D2 505 28.65 252 31.06
D3 607 28.42 246 27.10
D4 594 25.04 289 26.24
D5 427 25.36 275 24.43
Page 27
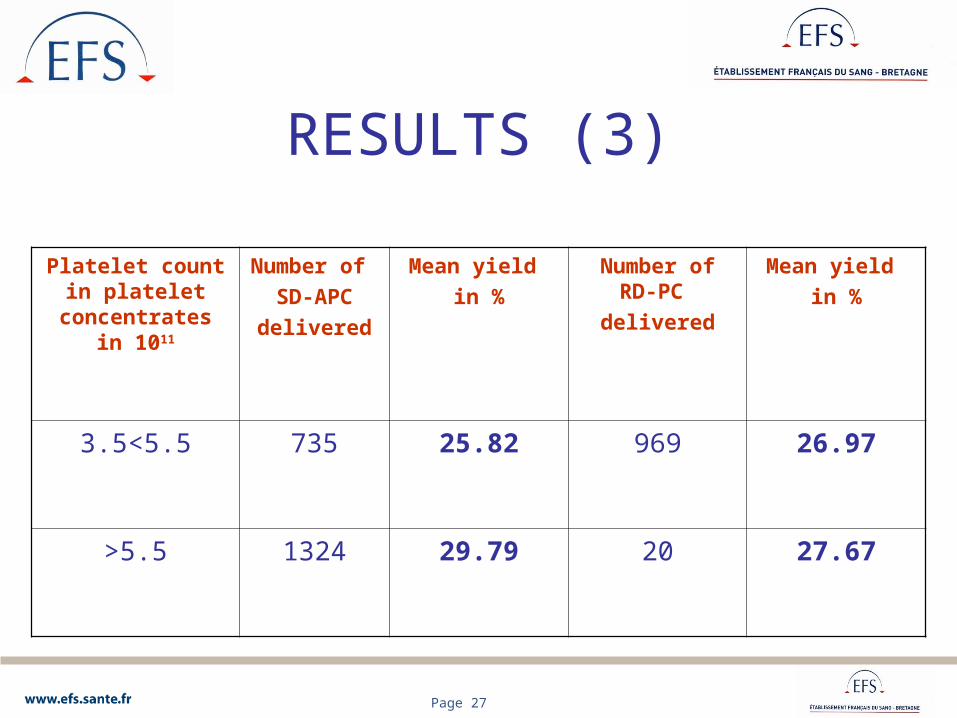
RESULTS (3)
Platelet count in platelet
concentrates in 1011
Number of SD-APC
delivered
Mean yield in %
Number of RD-PC
delivered
Mean yield in %
3.5<5.5 735 25.82 969 26.97
>5.5 1324 29.79 20 27.67

Page 28
Distribution of the platelets transfused according to age
(N = 11207)(08/02/2010-13/05/2012)
J1 J2 J3 J4 J5
3.3% 20.5% 28% 34% 14.2%
Distribution CPA/MCPCPA: 41%MCP: 59%
Page 29
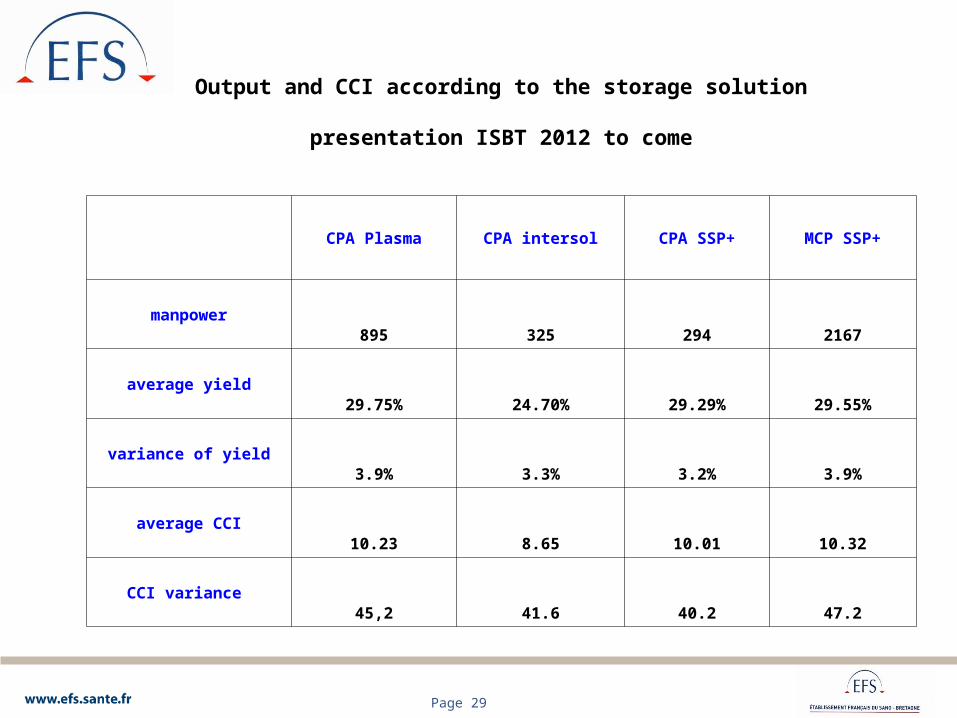
Output and CCI according to the storage solution
presentation ISBT 2012 to come
CPA Plasma CPA intersol CPA SSP+ MCP SSP+
manpower895 325 294 2167
average yield29.75% 24.70% 29.29% 29.55%
variance of yield3.9% 3.3% 3.2% 3.9%
average CCI10.23 8.65 10.01 10.32
CCI variance 45,2 41.6 40.2 47.2

Page 30
Output according to the storage solution
presentation ISBT 2012 to come (4459 PC Transfusions)
CPA Plasma CPA intersol CPA SSP+ MCP SSP+
Manpower 923 519 453 2564
average yield 29,42% 23,8% 28,10% 28,6%
variance of yield 3.8% 3.3% 3.2% 3.9%

Page 31
Tests de Comparaison des moyennes : utilisation du t de Student. La valeur de ce test doit être supérieure à 1.96 pour accepter à 95% l’hypothèse selon laquelle les moyennes observées sont différentes. Statistiquement, nous pouvons appliquer ce test de Student après avoir vérifié l’homogénéité des variances. Le test de Fischer-Snedecor nous permet de valider cette homogénéité car dans chacun des cas, le rapport de la variance la plus élevée sur la variance la plus faible est inférieur à la valeur théorique de 1.57.
Comparaisons des moyennes : CPA Intersol et CPA Plasma : F=1.15 et t=5.5 les moyennes sont différentes. CPA SSP+ et CPA Plasma : F=1.18 et t=1.2 les moyennes sont identiques. CPA SSP+ et MCP SSP+ : F=1.22 et t=0.5 les moyennes sont identiques. MCP SSP+ et CPA Plasma : F=1.03 et t=1.1 les moyennes sont identiques.
Nbre Receveurs
Rendement Moyen
Variance du rendement
CPA Intersol 519 23,79% 3,3%
CPA Plasma 923 29,42% 3,8%
CPA SSP+ 453 28,10% 3,2%
MCP SSP+ 2 564 28,60% 3,9%

Page 32
En jaune, les moyennes significativement différentes : J5 rendement moindre que J4 pour CPA PlasmaCPA/MCP SSP+ : les moyennes de rendement à 1 jour près peuvent sembler décroître selon l’ancienneté du PSL, mais statistiquement ces moyennes comparées au jour près sont identiques et ne présentent pas de différence.
La valeur du t de Student ici compare le rendement moyen de l’âge du PSL sur la ligne concernée avec la ligne juste au dessus : ex : J5 vs J4
type pslAge du P.S.L.
Nbre Receveurs
Rendement Moyen
Variance du rendement
t de Student
1 29 28,5% 5,3%2 88 25,5% 4,1% 0,6 3 141 23,6% 3,5% 0,7 4 179 23,6% 2,9% 0,0 5 73 21,6% 2,4% 0,9 1 56 32,3% 3,6%2 151 29,4% 3,7% 1,0 3 235 28,9% 3,7% 0,3 4 299 31,4% 4,3% 1,5 5 154 24,8% 2,8% 3,7 1 30 32,6% 4,9%2 92 29,4% 3,3% 0,7 3 129 28,9% 3,4% 0,2 4 140 26,4% 2,7% 1,2 5 55 25,7% 3,0% 0,2 1 27 33,9% 6,0%2 475 30,4% 3,9% 0,7 3 814 29,0% 4,1% 1,2 4 920 27,4% 3,7% 1,7 5 273 27,7% 4,1% 0,2
CPA Intersol
CPA Plasma
CPA SSP+
MCP SSP+
Page 33
Results
4459 PC Transfusions
1219 Recipients
2264 yeld > 20% ( 60% PC Transfusions)

Page 34
Platelet transfusion
Inefficiency if output < 20% or CCI <7Platelet concentrate
• Insufficient dose• Altered platelets (transport, conservation… c.f. index of
spinning)• Age of platelets• Incompatible ABO
Patient• Fever, CIVD, splenomegaly, drug • Alloimmunisation HLA or HPA = refractory state
(polytransfused, graft,…)

Page 35
Platelet transfusion
Refractory state
Output < 20% or CCI < 7 on the results of the count made 1 to 24 hrs after a second transfusion of a concentrate of platelets:
• Compatible ABO• Less than 48h of storage• Having a sufficient quantity of platelets
(0.5 * 1011/7kg)

Page 36
Antigenic systems and Antigenic systems and alloimmunisation antiplateletsalloimmunisation antiplatelets
Feverish and Feverish and allergic allergic
reactionsreactions
Post-Post-transfusional transfusional
thrombocytopenthrombocytopenic purpurasic purpuras
Refractory Refractory states poor states poor
outputsoutputs
System ABOSystem ABO ++ -- ++
System HLASystem HLA ++++ ?? ++++++
Systems HPASystems HPA ++++++ ++++++ ++++

Page 37
Causes of the refractory states Causes of the refractory states to platelet transfusions to platelet transfusions
Non alloimmuneNon alloimmuneTransfusional
• Storage• Leucocytic contamination
Clinics• Fever• splenomegaly• CIVD. MAT• CSH graft
ImmunologicalImmunological• Auto antibodyAuto antibody• Immunoallergic antibodiesImmunoallergic antibodies
AlloimmunesAlloimmunes
Anti-HLAAnti-HLA• FrequentFrequent• Anti class IAnti class I
Anti-HPAAnti-HPA• Unknown frequency, probably weak Unknown frequency, probably weak • Often not recognisedOften not recognised
Anti-ABAnti-AB• Sometimes forgottenSometimes forgotten

Page 38
Study TRAP Study TRAP (Trial to Reduce Alloimmunization to Platelets (Trial to Reduce Alloimmunization to Platelets
Study Group N. Eng. J. Med. 1997)Study Group N. Eng. J. Med. 1997)
Co-operative study 530 LAMCo-operative study 530 LAM 4 groups of patients:4 groups of patients:
1.1. Transfused with pools of concentrates of normal Transfused with pools of concentrates of normal plateletsplatelets
2.2. Transfused with pools of concentrates of Transfused with pools of concentrates of platelets treated with UV-Bplatelets treated with UV-B
3.3. Transfused with pools of concentrates of Transfused with pools of concentrates of leucocyte-reduced platelets by filtrationleucocyte-reduced platelets by filtration
4.4. Transfused with concentrates of platelets of Transfused with concentrates of platelets of apheresis with leucocytes reduced by filtrationapheresis with leucocytes reduced by filtration

Page 39
TRAP studyTRAP study (Trial to Reduce Alloimmunization to Platelets (Trial to Reduce Alloimmunization to Platelets
Study Group N. Eng. J. Med. 1997)Study Group N. Eng. J. Med. 1997)
Refractory state:Refractory state:2 consecutive ineffective transfusions,2 consecutive ineffective transfusions, CCI in the hour CCI in the hour following the transfusion < 5000/ following the transfusion < 5000/ L/m L/m22
Compatible ABOCompatible ABOAt least one of the two concentrates stored for less than 48 At least one of the two concentrates stored for less than 48 hrs.hrs.
Anti-HLA Anti-HLA MLCT sensitized by an antiglobulineMLCT sensitized by an antiglobuline60% cytotoxicity in 1 cell or 40% in 260% cytotoxicity in 1 cell or 40% in 2Tests prior to beginning of protocol and then every week for Tests prior to beginning of protocol and then every week for eight weekseight weeks
Anti-HPAAnti-HPADetection: ELISA and flow cytometryDetection: ELISA and flow cytometryConfirmation: method of capture ELISAConfirmation: method of capture ELISA

Page 40
TRAP StudyTRAP Study (NR. Eng.J.Med. 1997)refractory states (RS) withtransfusions of platelets
and alloimmunisationTemoins Temoins
131131UV-B 130UV-B 130 F-PC 137F-PC 137 F-AP 132F-AP 132
RS for all RS for all patientspatients
16%16%10 – 23%
10%10%6 –16%
7%7%4 –13%
8%8%4 –14%
RS and RS and previous previous pregnanciepregnanciess
32%32%21 – 47%
17%17%8 - 32%
10%10%4 – 22%
16%16%8 - 29%
Ac lymphoAc lympho
cytotoxiccytotoxic45%45%
36 –54%21%21%
15 – 30%18%18%
12 – 26%17%17%
12 – 26 %
Ac Anti -Ac Anti -plateletsplatelets
11%11% 7%7% 6%6% 7%7%
RSRS
alloimmunealloimmune13%13%
8 – 20%
5%5%2 – 11%
3%3%1 – 8%
4%4%1 – 9%
Page 41
Risk factors of Risk factors of alloimmunisationalloimmunisation
Preliminary sensitizingPreliminary sensitizingPrevious blood transfusions without leucocyte Previous blood transfusions without leucocyte reductionreductionPrevopis pregnancies 62% vs 33% of Prevopis pregnancies 62% vs 33% of immunization with/without leucocyte reduction immunization with/without leucocyte reduction (TRAP study)(TRAP study)
Pilot 32% vs 10% of immunization with products Pilot 32% vs 10% of immunization with products without leucocyte reduction vs products with without leucocyte reduction vs products with leucocyte reduction leucocyte reduction (TRAP study)(TRAP study)

Page 42
Platelet transfusion
What to do in the event of a refractory state?
search for AC anti HLA /HPA
Search for compatible platelets: phenotype CPA compatibilized cryostored
MCP
Page 43
Platelet transfusion
Other complications
Nonhemolytic feverish reactionsAnti-erythrocyte alloimmunization (rhesus)AllergyHaemolytic accidents (haemolysins)GVHDTransmission of viruses, bacteria, parasitic infectious diseasesTRALIPost-transfusional purpura

Page 44
Platelet transfusion Prevention of complications
RFNH: fresh platelets, deleucocytation, (deplasmatisation) premedication of the recipient
Alloimmunization anti D: Selection of platelets from Rh negative donor (protection
future obstétrical +++)+++) Ig anti D Passive anti D monitoring
Allergy: Prefer additive platelets in solution to platelets in plasma, (deplasmatisation?)

Page 45
Platelet transfusion
Haemolytic accidents (by AC immune ABO)Detection of haemolysinsRespect Iso group if possiblePlasma removal
GVHDIrradiation
Transmission of infectious diseases Tracking of viruses: HBV, HCV, HIV, MVC
For the bacteria: medical maintenance, good disinfection of the intake point, rules
of hygiene, information post donation

Page 46
Platelet transfusion
Transmission of infectious diseases (continued)
For parasites: exclusion for donors when returning from endemic areas
Attenuation of pathogens: Amotosalen, Riboflavin, UVC, but deterioration of the platelet function involving of the more frequent transfusions
Page 47
Platelet transfusion
TRALI
• Not-transfused male subjects• Nulliparous women• Multiparous negative ac anti HLA

Page 48
Post-transfusional purpuraPost-transfusional purpura
IdentificationIdentificationTypical form of brutal thrombocytopenia one week after the Typical form of brutal thrombocytopenia one week after the transfusion of a blood product containing of the plateletstransfusion of a blood product containing of the plateletsAtypical form: refractory thrombocytopenia with the Atypical form: refractory thrombocytopenia with the transfusions of plateletstransfusions of platelets
DiagnosisDiagnosisIn addition to frequently present anti HLA, look for anti-HPA In addition to frequently present anti HLA, look for anti-HPA interest of MAIPA with ac monoclonal suitableinterest of MAIPA with ac monoclonal suitable
TreatmentTreatmentGenerally ineffective transfusion since PR associates an anti Generally ineffective transfusion since PR associates an anti HPA reaction automatically with an allo reaction HPA reaction automatically with an allo reaction Plasma exchangePlasma exchangeIVIGIVIG

Page 49
Platelet transfusion
Conclusion
Two products with identical effectiveness: CPA and MCPPreserved in plasma or additive solution (PAS)Able to use transformations or qualifications (phenotype, test of compatibility, negative CMV) to adapt to the needs of the patientThe selection, dose, and monitoring of platelet transfusions must be subject to dialogue between the prescriber and the transfusion centre

Page 50
RemerciementsThanks
Pr. Jean-Yves MullerPr. Gilbert SemanaDr.Georges AndreuDr.Julie VasseMme Soline GaucheronMr Jean-Pierre LebaudyDistribution team