Embed Size (px)
Citation preview

25/5/2016
1
Principles of Physiotherapy Interventions for
Common Sport Injuries
Tan Yee Siong Sport Physiotherapist TYS Physio On Wheel
Sport Injuries PT Mx
Nature of Healing and Repair
Injury Identification
Rehabilitation Principles
Overview
Nature of Soft Tissue Healing and Repair
Terms
• Wound – Damage/disruption of normal anatomical structure and functions
• Healing – A coordinated series of events in response to an
injury/wound resulting in partial or complete repair and regeneration of the lost part
• Repair - The process of synthesizing connective tissues and its
subsequent maturation into scar tissues • Regeneration – The exact replacement of the lost cells by cells of the
same type
• Connective Tissues – A group of wide variation cells that provide the structural framework, supports, transport and energy storage within the body
Connective Tissue Proper [Areolar Tissue] The Normal Healing Cascade

25/5/2016
2
Acute Inflammation Acute Inflammation
• Local tissue reactions to injury, sometimes known as the demolition phase/clean-up process.
• Preserve and restore homeostasis, ie returning normal
tissues condition and cells environment. • 4 cardinal signs: rubor, tumor, dolor, calor [Celsus AD35] +
loss of function described by Virchow • Suffix of –itis • Prerequisite for repair and regeneration
Possible Response after Injury Regeneration
• Seen in lower vertebrates eg earthworm up to complex organism eg human.
• Human’s organs /tissues regenerative powers varies
and limited. • Certain discrepancies between the amount of
regeneration and repair. • Epithelial, connective tissues (except cartilage),
smooth muscles tissues usually regenerate well. • Muscle and neural tissues regenerate poorly.
Rate of Healing
{ { Local
Disturbed demolition phase
Vascularity
Excess movements
Foreign material
Infection/irradiation
Systemic
Malnutrition
Corticosteroids
Jaundice
Factors Influencing Wound healing

25/5/2016
3
Stress-Strain Curve
Identification of Injury
Why Examination and Ax?
Excellent in the treatment and management of MS dysfunction can only be obtained as a result of the application of a logical, systematic, careful and intellectual examination and assessment strategy.
Petty & Moore 1999
I know that you believe you understand what I said, but I am not sure you realize that what you heard is not what I meant. Maitland 1986
Key Identification from the Subjective Ax
Always listen to what patient has to say.
What are the mechanisms of injury?
Which structures could be the source of the symptom/site of injury?
What is the nature of the injury/condition?
What others factors need to be examined?
Is the condition severe and/or irritable?
Key Points in Physical Examination
Systematic and goal-oriented.
Every piece of information gather is just a clue, not the truth by itself.
Do not test for the sake of testing. The value of examination/tests carried out must be weighted.
Keep and open-mind, think logically rather quickly jumping into conclusion.
Establish comparable sign.
Common MS Lesions
Strain
Sprain
Dislocation
Subluxation
Muscle/tendon rupture
Tendinoathy/Tendinosis
Synovitis
Hemarthrosis
Contusion
Bursitis
Synovitis
Ganglion
RSI

25/5/2016
4
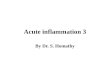
Differential Dx of Soft Tissues Disorder Synovial Fluid Inspection
Synovial Fluid Quality
Time Lapse Colour Viscosity
2 weeks Bloody red Watery
5 weeks Apricot orange Loose salivary
4 months Clear light yellow Loose salivary
8 months Clear light yellow Thick salivary
1.5 – 2.0 years Clear light yellow Thick mucus
Cartilage Flakes
White colour fragmented debris suspended in the synovial fluid.
Degree of Injury Grade 1 Grade 2 Grade 3
Pain Mild Moderate Severe
Playability Able Unable Unable
Stress Response ERP ERP Nil
Structural Integrity Preserved
Joint play increased
Laxity/ Instability
Severity of Tissue Injury
Principles of Rehabilitation
The Initial Guide where Everything Started…
Return
to Sport
§Neuromuscular
relearning §Specific Sport Drills
Aerobic
& Endurance
§ROM
§Muscular Strength §Proprioception
LL Rehabilitation RoadMap
Sorts Specific Training
Plyometric and Agility
Neuromuscular Control 3
CR Capacity
Muscles Strength and Endurance
Neuromuscular Control 2
Protection and Healing
ROM and Muscle activation
Weight Bearing and Mobility
Neuromuscular Control 1

25/5/2016
5
Shoulder Rehabilitation RoadMap
Sorts Specific Training
Strength 3 [task specific]
Neuromuscular Control 3 [closed-chain stabilization]
Functional 2 [Eccentric-plyo, Total body]
ROM 2
Strength and Endurance [dynamic]
Neuromuscular Control 2 [ST and GH]
Functional 1 [ADL]
Protection and Healing
ROM 1 and Muscle activation [static– isometric]
Neuromuscular Control 1 [postural]
Nature of Injury
Healing Process – Timing
Wilhelm Roux – Law of functional adaptation
Mechanics (movement & position)
Passive and Active Stability
Associated Injuries
Governing Factors in Rehabilitation progression
Motor Tasks Taxonomy [Gentile 2000]
Acute Stage (Inflammatory Reaction) Management Guidelines
Characteristic (< 7days unless insult is perpetuated)
Vascular reaction
Exudation of cells and chemicals
Clot formation
Phagocytic, neutralization of irritants
Early fibroblastic activity
Goals
Provide reassurance and understanding
Control the effects of inflammation
Maintain soft tissue and joint integrity
Maintain function of associated areas (ROM, Muscle performance, Circulation, Function)
The initial inflammatory response is critical to the entire healing process. If this response does not accomplish what it is suppose to or if it does not subside, normal healing cannot take place.
Any movement tolerated at this stage is beneficial, but it must not increase the inflammation or pain.
Stretching and resistance exercises should not be performed over the lesion site. Active movement is usually contraindicated.
In an injured structure that is not rested and is subjected to unnecessary external stress and strains, the healing process will never really get a chance to begin.
Clinical Reminders

25/5/2016
6
Subacute Stage (Repair and Healing) Management Guidelines
Characteristics (2 – 3 weeks after injury, up to 6 weeks in tissue with limited circulation)
Decreasing or absent of inflammation
Removal of noxious stimuli
Angiogenesis
Exudate replacement by collagen formation
Tissue granulation
Myofibroblastic activity
Goals
Encourage patient to return to normal activities that do not exacerbate the symptoms. Help them to adapt to their work and recreational activities.
Monitor healing tissue response to exercise
Restore soft tissue, muscle and joint mobility and flexibility
Develop neuromuscular control, strength and endurance (including proper mechanics)
Clinical Reminders
Wound closure takes 5 to 8 days in muscle and skin and up to 6 weeks in tendons and ligaments.
Exercises and activities should be within the tolerance of the healing tissues. (non-destructive motion)
Criteria for initiating active exercises and stretching include decreased swelling, intermittent pain and pain that are not exacerbated by motion in the available range.
During this stage, the immature connective tissue is thin and unorganized. Yet proper growth and alignment can be stimulated by appropriate tensile loading in the line of normal stress of the tissue.
Clinical Reminders
Patient response is the best guide to how quickly or vigorously to progress. Any abnormal response might be the sign of chronic inflammation and intensity of exercises should be tuned-down.
Muscle weakness will set in even in the absence of muscle pathology because of restricted use of the injured region.
Be certain patient is using the correct motor pattern without substitution.
Chronic Stage (Maturation and Remodeling) Management Guidelines
Characteristic (up to 6 months and continues…)
No inflammatory sign
Balance between synthesis and degradation of collagen
Collagen oriented and increase in tensile strength in response to stresses placed on them
Adhesions and contractures
Goals
Instruct patient in biomechanically safe progression of resistance and stretching exs and how to monitor for signs of excessive stress.
Increase soft tissue, muscle and joint mobility including joint play.
Improve neuromuscular control, strength and endurance.
Improve cardiovascular endurance.
Progress functional activities.

25/5/2016
7
Clinical Reminders
Immature collagen molecules are held together with hydrogen bonding and can be easily remodeled in response to the stresses placed for up to 10 weeks with gentle but persistent treatment.
At 14 weeks, the scar tissue has changed to covalent bonding and is unresponsive to remodeling. Treatment under these conditions requires either adaptive lengthening in the tissue surrounding the scar or surgical release.
The progressively increasing in tensile quality may continue for 12 to 18 months. It is important to use controlled forces that duplicate the normal stresses on the tissue.
Clinical Reminders
Joint motion without adequate muscle support causes trauma to the joint as proposed by Zohn and Mennell, who recommended a muscle test grade of 4 in LL musculature before discontinuing use of assistive devices for ambulation.
Joint dynamics, muscle strength and flexibility should be balanced.
Monitoring Signs
Soreness that does not decrease after 4 hours and is not resolved after 24 hours.
Pain that comes on earlier or is increased over the previous session.
Progressive stiffness and decrease in ROM.
Inflammatory signs.
Progressive weakness.
Decreased in functional usage.
Monitoring System
McKenzie Traffic Light Procedure
If symptom increase – RED Light – STOP
If symptom unclear but not worse – AMBER Light – Try a little bit further
If symptom improve – GREEN Light – Move On
Before Injury Assessment
Equipment Removal
Only remove if it will not cause further injury, use proper cutter if needed
Athlete Positioning Comfortable and injured part supported.
For seriously injured athlete, only move unless is necessary
Ensuring Safety Protect athlete from further
harm/danger Keep the athlete calm
In The Field

25/5/2016
8
In The Field Formula for Treatments?
R.I.C.E, P.R.I.C.E, P.O.L.I.C.E, P.R.I.C.E.M.M.
Only 5% level 1 evidence.
Based on expert opinion and clinical reasoning.
Questions to Ponder in Sports Rehab
High cost incur for ACL injuries in overseas.
Only 53% of the patient return back to sport post trauma 3 – 4 years (Kvist 2005)
94% of football players went back to sport within a year.
Probable reasons for the above rehab / conditioning lack: Failure to mimic the complexity of the sport movements
during rehab.
Condition in rehabilitation is over controlled.
Gap between the rehab knowledge and athletic expertise
Outcome measures are not up to the athletic level.
Questions to Ponder in Sports Rehab
What is the nature of the sport?
How would you judge the current level of practice / training in compare to the pre-injury level?
How appropriate with the outcome measures used in relation to the sport before discharging from training / conditioning / rehab?
How do you feel during the first practice / competition and why so?
Has the rehabilitation brought patient back to the normal practice routine?
References
Kisner C, Colby LA (2007), Soft Tissue Injury, Repair and Management: Chapter 10, in Kisner C, Therapeutic Exercise – Foundation and Techniques (5th Edition, pp. 295 – 307), USA, F.A. Davis Company
Robert FD, Melissa CE (2004), Wound Healing: An Overview of Acute, Fibrotic and Delayed Healing. Frontiers in Bioscience (9), pp 283 – 289, Virginia US
Martini FH (2006), The Tissue Level of Organization: Chapter 4, in Fundamentals of Anatomy and physiology (7th Edition, pp. 118 – 137), USA, Pearson Cummings
Spector TD, Axford JS (1999), Healing and Repair: Chapter 15, in An Introduction to General Pathology (4th Edition, pp. 141 – 156), Churchill Livingstone
Bleakley CM (2013), Acute Soft Tissue Injury Management: Past, resent and Future. Physical Therapy in Sort 14 (2013), 73 – 74, Elsevier UK
Suun A et al (2010), Introduction to Sort Injuries Management: Chapter 1, in Sorts Injuries, pp 1 – 6, Open University Malaysia, Meteor Doc
PEtty NJ, Moore AP (2001), Subjective and Physical Examination: Chapter 2 – 3, in Neuromusculoskeletal Examination nd Assessment – A Handbook for Therapist, (2th Edition, pp. 5 – 107), Churchill Livingstone
Dr Arshad Puji, Sport Physician, ASIU, Orthopedic Institute HKL Dr Goh Siew Li, Sport Physician, ASIU, Orthopedic Institute HKL Dr Siti Hawa, Orthopedic Surgeon ASIU, Orthopedic Institute HKL Dr Bazam, Orthopedic Surgeon, ASIU, Orthopedic Institute HKL Mr Zahari Afandi, Sport Physiotherapist, Physiotherapy Department HKL