Embed Size (px)
Citation preview

Acute Inflammation

"Inflammation is one of the most important and most useful of our host defense mechanisms, and without an adequate inflammatory response none of us or our patients would be living.
It is not a disease but a manifestation of a disease
Ironically it is also one of the most common means whereby our own tissues are injured."
Inflammation

GENERALITIES REGARDING THE INFLAMMATORY RESPONSE:
process involves multiple participants.Inflammation is the reaction of vascularized living tissues to local injuryfairly stereotypicalIt is a series of events which overlap and form a continuum in the terminal vascular bed, in blood and in connective tissues It is a response to an initiating event a defense mechanism.purpose is to eliminate the offending irritant and to repair the damaged tissue.It can be harmful.

Roles of Inflammation:
Protection -Contain and isolate the injury -Destroy invading organisms and inactive toxins
Achieve healing and repair -ideally tissue should return to normal -abscess formation may occur -persistent infection -chronic infection -scar formation-may distort tissue and alter their function

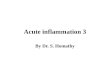
Outcome of Acute Inflammation
INJURYMediators
Acute inflammation
Resolution
Abscess formation
HealingRegeneration
ScarringChronic inflammationMediators
Persistent infectionPersistent toxinsAutoimmune diseases

Inflammation
“Is a reaction of a tissue and its microcirculation to a pathogenic insult”
It is characterized by the generation of inflammatory mediators and movement of fluid & leukocytes from the blood into extravascular tissues.

Causes of Inflammation
Microbial Infections – pyogenic bacteria, virusHypersensitivity reactions – parasites, TBPhysical agents – trauma, radiation, heat, coldChemicals – corrosives,bacterial toxinsTissue necrosis - infarction

ACUTE INFLAMMATION
Cardinal Signs
Redness (rubor)
Swelling (tumor)
Heat (calor)
Pain (dolor)
Loss of function (functio laesa)

Phases of Acute Inflammation
1- Initiation: 1- Stimulation (injury) with changes in microvasculature2- Structural changes leading to fluid extravasation3- Emigration of WBCs to the site of injury
2- Amplification:Both soluble mediators and cellular inflammatory systems are activated and amplified
3- Termination:Specific inhibition or dissipation of the mediators

Acute InflammationAcute inflammation involves several processes:
Vascular component- Alterations in vascular caliber leading to increased blood flowExudative component- Changes in the micro-vasculature causing protein rich fluid to leave circulationCellular component- recruitment and emigration of the leukocytes outside circulation and accumulation in the focus of injuryProliferative component- resulting in tissue regeneration,granulation tissue and healing

Acute Inflammation-Vascular events

Components of the vascular response
Vascular Changes - Vasodilation (change in caliber and flow) - increased vascular permeability - acute local active hyperemia
Cellular Events - Movement from capillaries and post
capillary venules - emigration -Accumulation of leukocytes at sites of
injury - migration -Activation of inflammatory cells

Sequence of events
Increased Vascular permeability
Escape of protein rich fluid into extravascular space
-immunoglobulins
-coagulation factors
-fibrinogen
Results in edema

InflammationPathogenesis of Edema
Inflammatory edema:
1. Direct, irreversible injury - all vessels (burns)
2. Transient increase in vascular permeability, i.e., the effect of mediators on post-capillary venules
3- Increased hydrostatic pressure

EDEMA -TRANSUDATEEDEMA -TRANSUDATE
(protein content low –(protein content low –
few cells-few cells-
specific gravity <1.012)specific gravity <1.012)
HydrostaticHydrostatic
pressurepressure
OncoticOncotic
pressurepressure
Inflammation Increased Hydrostatic Pressure

EDEMA -EXUDATE (protein content high: numerous neutrophils: specific gravity >1.020)
HydrostaticHydrostatic
pressurepressure
OncoticOncotic
pressurepressure
Inflammation Increased Vascular Permeability
Diapedesis

Mechanisms of increased vascular permeability
1- Formation of endothelial gaps in post capillary venules2- Direct injury to endothelial cell3-Leukocyte Dependent Endothelial Injury4-Increased Transcytosis5- Leakage from new capillaries

COMPONENTS OF THE INFLAMMATORY RESPONSE
Vascular Changes - Vasodilation (change in caliber and flow) -Increased Vascular Permeability – Acute Local Active Hyperemia
Cellular Events - Movement from capillaries and post
capillary venules - emigration -Accumulation of leukocytes at sites of
injury - migration -Activation of inflammatory cells

Cellular component
Accumulation of neutrophil polymorphs in the extracellular space is the diagnostic histologic feature of acute inflammation

Post capillary venules Concentration of RBC’s
increases as fluid decreases Blood flow decreases (slows-
stasis) Leucocytes interact with
endothelium Margination
Slowing and stagnation of blood flowWBC’s fall out of the central columnTumble slowly and roll along the endothelium of venules
Pavementing endothelium appears to be essentially
lined by white cells
Increased Permeability

Adhesion and Emigration
Prerequisite for cells to get to site of inflammation through endothelium.Leukocyte-Endothelial interaction –importantLeukocyte aggregation – WBC stick to endothelium and to each other.Adhesion molecules- molecular surface of WBC’s and endothelium.- Bind together to allow WBC’s to adhere.

Sequential involvement of adhesion molecules
Central Axial StreamCentral Axial Stream
Rolling Adhesion Transmigration
SELECTINS (E&P) INTEGRINS & Ig-LIKE MOLECULES (ICAM, VCAM)
Qualitative and Quantitative Endothelial and PMN Changes

EMIGRATION
Process by which leukocytes escape from their location in the blood to reach the perivascular tissues, (sometimes referred to as Diapedesis…)

Emigration - Process
1. After adhesion - leukocytes move along the endothelial surface2. Insert large cytoplasmic extension pseudopodia into endothelial gaps3. Gaps created by actions of histamine and other chemical mediators as well as by the leukocytes themselves4. PECAM – adhesion molecule is important in this process5. Entire cell passes through once pseudopodia are through6. Collagenase excreted - breakdown basement membrane

SEQUENCE OF LEUKOCYTE EVENTS
MarginationPavementingEmigrationChemotaxisPhagocytosis and Synthesis of biochemical MediatorsIntracellular DegradationExtracellular Release of Leukocyte Products

Phases of Acute Inflammation
1- Initiation: 1- Stimulation (injury) with changes in microvasculature2- Structural changes leading to fluid extra-vasation3- Emigration of WBCs to the site of injury
2- Amplification:Both soluble mediators and cellular inflammatory systems are activated and amplified
3- Termination:Specific inhibition or dissipation of the mediators

Regulation of Leucocyte Recruitment
Binding of chemical agents to specific receptors of leukocyte cell membranes stimulates a variety of events including chemotaxis

Chemotaxis
Chemotaxis: Directional migration in response to a chemical gradient of chemoattractant.It is a dynamic and energy dependent activity –
-process is receptor mediated.
-implies directed locomotion
Chemotaxins and Chemokines:
- mediators which make leukocytes travel
- chemoattractants

Mechanisms of Chemotaxis
Leukocytes crawl - require adhesive surface
Undergo morphological shape changes
Migrate towards the highest concentration of chemoattractant (Adherence, secretion and locomotion)

Inflammation Chemotaxis
1. Exogenous mediators, e.g.:a- N-formyl methionine terminal amino acids
from bacteria
b- Lipids from destroyed or damaged membranes (including LPS)
2. Endogenous mediators, e.g.:a- Complement proteins (C5a)
b- Chemokines, particularly IL-8
c- Arachidonic acid products (LTB4)

Chemotacticfactors (eg. c5a)
Chemotacticfactors (eg. c5a)
Tissue injury
Tissue injury
Vasoactivemediators(eg. histamine)
Vasoactivemediators(eg. histamine)
Increased vascularpermeability
Increased vascularpermeability
Recruitment of inflammatory cells
Recruitment of inflammatory cells
EdemaEdema PMNsPMNs MonosMonos
Production of inflammatory
mediators
Production of inflammatory
mediators
Acute inflammation
Acute inflammation
Chronic inflammation
Chronic inflammation

CHEMICAL MEDIATORS OF INFLAMMATION
· Production of active mediators is triggered by microbial products or host proteins.
· Most require binding to specific receptors on target cells for biologic activity.
· Some have direct enzymatic activity,
· One mediator can stimulate the release of other mediators by target cells- amplification
· May have different affects on different cells.
· Most are short lived.
· Many have the potential to be harmful.

CHEMICAL MEDIATORS OF INFLAMMATION
General Principles:
Originate from plasma and cells.
When in plasma are found in inactive state and must be activated.
When in cells are often within granules and are synthesized in response to a stimulus.

InflammationChemical Mediators of Inflammation
Cellular mediatorsPreformed1. Vasoactive amines2. Proteases – lysosomal
constituentsNewly synthesized1. Arachidonic acid
metabolites2. Platelet activating factor3. Cytokines4. Nitric oxide5. Oxygen-derived free
radicals
Plasma mediators1. Complement system2. Kinin system3. Coagulation and
fibrinolytic pathway

1 - Plasma Factors
Four enzymatic cascade and interrelated systems, important in the inflammatory response are found within plasma. These systems include the1. complement,
2. kinins
3. coagulation and system



2.1- HistamineFound in mast cells, basophils and plateletsReleased in response to stimuli Promotes arteriolar dilation and venular endothelial contraction results in widening of interendothelial cell junctions with increased vascular permeability
2.2- SerotoninVasoactive effects similar to histamineFound in platelets
Vasoactive amines
Inflammation2 - Chemical Mediators released from Cells

The following agents can stimulate release of histamine from mast cells:* Physical injury, mechanical trauma, heat, chemical agents, Snake venoms, toxins, bile salts, ATP* Immune reactions involving binding of antibodies to mast cells* Fragments of complement called anaphylatoxins (C3a and C5a)* Histamine-releasing factors from neutrophils, monocytes, and platelets* Cytokines (interleukin-1, IL-8)
InflammationChemical Mediators released from Cells

InflammationChemical Mediators released from Cells
2.3 - Arachidonic acid metabolitesThese lipid mediators are short-range hormones -formed rapidly - exert their effects locally and are then inactivated.
1. Synthesized from cell membrane phospholipids through the action of phospho-lipases (inhibited by corticosteroids)
2. Form leukotrienes via 5-lipoxygenase
3. Form prostaglandins and thromboxane A2 via cyclo-oxygenase (COX-1 inhibited by aspirin and indomethacin )

2.4 - Platelet activating factor-Produced by a variety of cells, including platelets, basophils, mast cells, neutrophils, monocytes,macrophages and endothelial cells * Platelet aggregation and release* Vasodilation and increased vascular permeability (100-10,000 X histamine)* Increased leukocyte adhesion to endothelium
InflammationChemical Mediators released from Cells


Morphology and function of inflammatory cells

Inflammation Inflammatory Cell Activation
Polymorphonuclear cells are activated by many substances:
1. The Fc portion of IgM and IgG molecules
2. C5a, C3b, and iC3b
3. Leukotriene B4
4. Cytokines (TNF-)5. Formylated chemotactic peptides
derived from bacteria

InflammationActivation of Inflammatory Cells
Macrophages are activated by many substances:
1. Lipopolysaccharide (LPS), found in Gram-negative bacteria
2. Platelet activating factor (PAF)3. Cytokines produced by T-cells,
particularly interferon gamma (IFN-)4. Fibronectin, a component of
extracellular matrix

PHAGOCYTOSIS AND INTRACELLULAR DEGRADATION
Purpose- engulf, kill and degrade bacteriaRecognise the enemyEngulf itFuse with enzymesBest when coated with opsoninsImportant Opsonins
i. Antibody (Fc fragment) ii. Fibronectin iii. C3b

Engulfment Phagolysosome formation
- Small cytoplasmic extensions or pseudopods extended by cell- Flow around the attached particle until it is engulfed- Cytoplasmic processes pinch together, meet, and fuse - Form a phagosomeFusion of lysosomal granules with phagosomeDegranulation of lysosomes into phagosomeCellular mechanisms similar to that of chemotaxis

Intracellular killing and degradation
Two categories of bactericidal mechanisms are recognized
1) Oxygen-dependent H2O2 – Myeloperoxidase-Halide system Nitric Oxide - Peroxynitrite Haber-Weiss reaction - Hydroxyl ion
2) Oxygen-independent

Oxygen Independent MechanismsSubstances within granules
Lysozyme- attacks bacterial cell walls- especially gram + bacteriaBacterial permeability increasing protein (BPI)- activates phospholipase degrades cell membranesLactoferrin- Iron binding glycoproteinDefensins- Cytotoxic to microbes and certain mammalian

Termination of the acute inflammatory response· Mediators have short half lives· Mediators are degraded after release· Produced in short bursts when stimulus persists· Switch to anti-inflammatory lipoxins from arachidonic acid· Production of anti-inflammatory cytokines (TGF-•)· Inhibit the production of TNF in macrophages

Inflammation - Systemic
Manifestations• Fever - clinical hallmark of inflammation
- Endogenous pyrogens: IL-2 ,TNF-• Constitutional symptoms - malaise, anorexia,nausea• Weight loss - due to negative nitrogen balance• Hyperplasia of mononuclear phagocyte system• Leukocytosis - may be neutrophils, eosinophils, or
lymphocytes• Anemia –blood loss,chronic due to toxic depression of
bone marrow• Acute Phase Reactants - non-specific elevation of
many serum proteins• marked increase in ESR• Amyloidosis – longstanding chronic infection

Inflammation
Systemic Manifestations
Leukocytosis: most bacterial infectionLymphocytosis: Infectious mononucleosis, mumps, German measlesEosinophilia: bronchial asthma, hay fever, parasitic infestationsLeukopenia: typhoid fever, infection with rickettsiae/protozoa

Systemic effects of Inflammation
Acute phase reaction/response- IL-1 and TNF- Fever- Malaise- AnorexiaBone marrow- leukocytosis- IL-1 + TNFLymphoid organs
Liver -IL-6, IL-1, TNF -Acute phase proteins
C-reactive proteinLipopolysaccharide binding proteinSerum amyloid Aa-2 macroglobulinHaptoglobinCeruloplasminfibrinogen

Suppuration-Abscess formation
Organisation-scar formation
Persistent inflammation
(chronic inflammation)

Resolution
Means complete restoration of the tissues to normal Favouring factors
Minimal cell death and tissue damageOccurrence in an organ or tissue which has regenerative capacity (eg the liver) rather than in one which cannot regenerate (eg. the central nervous system)Rapid destruction of the causal agent
(eg. phagocytosis of bacteria)Rapid removal of fluid and debris by good local vascular drainage