Embed Size (px)
Citation preview

PfA
DP
R
A
r
m
m
t
a
n
i
a
t
C
o
p
s
p
t
3
Ipcag
FeCGUtaAitIsrp
MO
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S V O L . 1 , N O . 1 , 2 0 0 8
© 2 0 0 8 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N I S S N 1 9 3 6 - 8 7 9 8 / 0 8 / $ 3 4 . 0 0
P U B L I S H E D B Y E L S E V I E R D O I : 1 0 . 1 0 1 6 / j . j c i n . 2 0 0 7 . 1 0 . 0 0 1
ercutaneous Coronary Interventionor Chronic Stable AnginaReassessment
avid R. Holmes, JR, MD, FACC,* Bernard J. Gersh, MB, CHB, DPHIL, FACC,*atrick Whitlow, MD, FACC,† Spencer B. King III, MD, MACC,‡ James T. Dove, MD, FACC§
ochester, Minnesota; Cleveland, Ohio; Atlanta, Georgia; and Springfield, Illinois
s it approaches its fourth decade, percutaneous coronary intervention (PCI) is now the most widely used
evascularization strategy around the world and has been tested in multiple clinical scenarios against both
edical and surgical therapies. For each patient group and clinical scenario setting, the goals of therapy
ust be specifically defined and clearly understood as an integral component of the process of selecting
he optimal strategy for the individual patient. In patients with chronic stable, often mild angina, the major
chievable goals of PCI are to affect symptoms, either by decreasing them or preventing them, reduce the
eed for subsequent procedures, and relieve ischemia. Achievement of these goals has been documented
n multiple randomized trials of PCI versus medical therapy. In these trials of patients with stable coronary
rtery disease (CAD), however, no reduction in death and myocardial infarction has been observed, and
hese limitations of PCI in this clinical setting need to be emphasized. Given the typically diffuse nature of
AD and the fact that PCI only treats a segment within a coronary artery, this is not surprising. Although
ptimal medical therapy forms the cornerstone of management for any patient with CAD, among stable
atients who do fail medical therapy, percutaneous coronary revascularization plays a well-documented
ignificant role in improving symptoms and preventing the subsequent need for revascularization. The ap-
ropriate utilization rates of PCI in patients with chronic stable angina and preserved left ventricular func-
ion should lead to more cost-effective care of patients with stable CAD. (J Am Coll Cardiol Intv 2008;1:
4–43) © 2008 by the American College of Cardiology Foundation
bsttui
bvvuAtmsdpp
t has been 30 years since Gruentzig first used aercutaneous procedure to treat a patient withoronary artery disease (CAD) (1,2). In that initialpplication, a 37-year-old male with unstable an-ina pectoris of recent onset underwent successful
rom the *Department of Cardiology, Division of Cardiovascular Dis-ase and Internal Medicine, Mayo Clinic, Rochester, Minnesota; †Theleveland Clinic, Cleveland, Ohio; ‡Fuqua Heart Center, Atlanta,eorgia; and §Prairie Cardiovascular Consultants, Southern Illinoisniversity School of Medicine, Springfield, Illinois. Dr. Gersh serves on
he Data Safety and Monitoring Board of Boston Scientific Corporationnd on the member advisory boards for Cardiovascular Therapeutics,straZeneca, and Bristol-Myers Squibb. Dr. Whitlow has participated
n research studies with Abbot, Boston Scientific, and Cordis and is onhe board of directors for Medlogics, Inc.; is a scientific advisor for Icon,nc.; and is a stockholder (�$50,000) with Medtronic, Inc. Dr. Kingerves on the medical advisory board for Medtronic, Inc. and has receivedoyalties from Cordis. Peter Berger, MD, served as Guest Editor for thisaper.
eanuscript received August 28, 2007; revised manuscript receivedctober 9, 2007, accepted October 26, 2007.
alloon dilatation of a proximal left anterior de-cending lesion. In 2000, at the age of 61 years,hat patient had recurrent chest pain for the firstime since the initial procedure. Angiography doc-mented no significant stenosis at the site treatedn 1977.
Over the course of the past 3 decades, there haveeen major advances in nonsurgical coronary re-ascularization, and percutaneous coronary inter-ention (PCI) has now become the most widelysed revascularization procedure around the world.lthough a substantial part of this growth has been
he consequence of the well-documented improve-ent in outcomes of patients with the broad
pectrum of acute ischemic syndromes who un-ergo PCI versus medical therapy (3–7), it isrimarily the result of the application of PCI inatients with chronic coronary disease who have
ither stable angina or a positive functional test
wuth(toosmaamwascttia
ccntamgilt
gsptvrmcpmidn
siiisof
oasabbntmsiCbdasaa(
PdcPlptteqmfebenNstv1is
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 1 , N O . 1 , 2 0 0 8
F E B R U A R Y 2 0 0 8 : 3 4 – 4 3
Holmes, Jr. et al.
PCI for Chronic Stable Angina
35
ith ischemia. On one hand, the burgeoning use of PCI isnderstandable because of major technological advances inhe field, but it should be appreciated that, although PCIas taken the place of coronary artery bypass graftingCABG) as the most widely used mode of revascularization,he major increase in the utilization of PCI has been becausef its use in patients formerly treated with medical therapynly. Patients and physicians frequently view coronary arterytenosis as a mechanical problem to be “fixed” by mechanicaleans. Nonetheless, during the last few decades, there have
lso been profound improvements in approaches to primarynd secondary prevention, and these sentinel advances inedical therapy have generated new questions abouthether PCI may be overused as the initial therapeutic
pproach to patients with stable CAD and relatively mildymptoms. The consistent findings in generations of trialsomparing PCI and surgical revascularization with medicalherapy, together with recent advances in secondary preven-ion, set the stage for a reappraisal of the critically importantssue of optimal management of patients with chronic stablengina.
This discussion of therapeutic modalities needs to beonsidered in relation to the overall goals of therapy inhronic CAD. In this respect, the chronicity and progressiveature of the disease processes are of paramount impor-ance. Coronary disease is not cured by any currentlyvailable therapies, but the natural history and prognosisay be modified. This is germane to all therapeutic strate-
ies, namely medical therapy, PCI, and surgical revascular-zation. Potential targets of therapy include both short- andong-term goals that vary from prevention of clinical eventso the treatment of symptoms (Table 1).
The application of PCI in an attempt to achieve theseoals depends upon many factors, including the extent andeverity of the CAD, the baseline demographics of theatient (including comorbidities), and the patient’s presen-ation (e.g., an acute ischemic syndrome versus stable anginaersus asymptomatic ischemia). The benefits of coronaryevascularization in patients with ST-segment elevationyocardial infarction (STEMI) and non–STEMI acute
oronary syndromes (ACS) have been the subject of multi-le trials, with the general consensus favoring an aggressiveechanical approach in patients with these syndromes and,
n particular, among those at higher risk (3–7). The presentiscussion will focus on patients with chronic stable angina,ot on patients with ACS.Irrespective of whether revascularization is performed
urgically or percutaneously, the landscape has changedrrevocably in that aggressive secondary prevention is anntegral aspect of management. This has been an area ofntense investigation, and there are robust evidence-basedets of data that have been used to formulate guidelines forptimal care, which emphasize the benefits of aggressive risk
actor modification with diet, exercise, and treatment of ibesity, diabetes, hypertension, and hyperlipidemia, as wells tobacco cessation. Specific adjunctive medical therapieshould include administration of statins, aspirin, anngiotensin-converting enzyme (ACE) inhibitor in manyut not all patients, and the judicious use of nitrates andeta-blockers and calcium chan-el blockers in symptomatic pa-ients. Blood pressure controlay require multiple drugs, and
ome lipid abnormalities requirenterventions beyond statins.ontrol of hyperglycemia haseen proved critical in managingiabetes. New antianginal agentsre under development, and oneuch drug, ranolazine, has beenpproved recently by the Foodnd Drug AdministrationFDA) (8–10).
Consideration of the goals ofCI must take into account theescription of what would beonsidered to be “optimalCI.” The technological revo-
ution, dominated by stent im-lantation and advances in an-ithrombotic and antiplateletherapies, is continuouslyvolving. As a direct conse-uence, there has been a dra-atic decrease in the need for urgent CABG surgery
ollowing PCI because the problem of acute or threat-ned closure has been almost eliminated. In addition,are-metal stents (BMS) have reduced, although notliminated, clinical or angiographic restenosis and theeed for repeat revascularization procedures (11–14).onetheless, it should be emphasized that two decades of
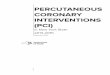
tudies have not shown that conventional percutaneousransluminal coronary angioplasty (PTCA) improves sur-ival in comparison with medical therapy (15–20) (Fig.). Given the change from balloon dilatation to stentmplantation, it is important to evaluate the effect oftenting on the hard end points of death and myocardial
Table 1. Goals of Treatment
Relief or decrease of angina and ischemia
Prevention of progression of disease
Prevention of complications of disease including
Myocardial infarction
Worsening left ventricular function or development of congestive heart failure
Cardiovascular death
Sudden cardiac death or arrhythmias
Abbreviationsand Acronyms
ACE � angiotensin-converting enzyme
ACS � acute coronarysyndromes
BMS � bare-metal stent(s)
CABG � coronary arterybypass grafting
CAD � coronary arterydisease
DES � drug-eluting stent(s)
FDA � Food and DrugAdministration
LV � left ventricular
MI � myocardial infarction
PCI � percutaneouscoronary intervention
PTCA � percutaneoustransluminal coronaryangioplasty
STEMI � ST-segmentelevation myocardialinfarction
nfarction (MI). Two separate m
eta-analyses have been
pdaStdnhev
dpcssbcs
1
2
3
4
5
adratpd
[gAmatpfi
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 1 , N O . 1 , 2 0 0 8
F E B R U A R Y 2 0 0 8 : 3 4 – 4 3
Holmes, Jr. et al.
PCI for Chronic Stable Angina
36
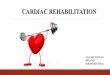
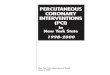
ublished (Figs. 2 and 3). Brophy et al. (21) found noifference in death or MI between balloon angioplastynd stenting in 29 trials involving 9,918 patients. Aluwaidi et al. (22) performed another meta-analysis of 23rials that included 10,347 patients. This meta-analysisemonstrated no significant difference between the tech-iques in the frequency of death or MI. There was,owever, a significant reduction in major adverse cardiacvents. This was solely the result of a reduction in targetessel revascularization.
The subsequent development and widespread adoption ofrug-eluting stents (DES) further improved the outcome ofercutaneous procedures by significantly reducing restenosisompared with BMS. In multiple series, the need forubsequent procedures with DES has been reduced toingle-digit frequency. Recently, the issues of stent throm-osis have attracted considerable attention and generatedontroversy (23–28). However, the data as a whole stillupport the following conclusions (Figs. 4 and 5):
. Drug-eluting stents significantly reduce restenosis com-pared with BMS.
. Overall stent thrombosis rates are low and occur withboth BMS and DES.
. The timing of stent thrombosis appears to vary; stentthrombosis with DES appears to occur somewhat laterthan with BMS and may continue for a longer period oftime. Moreover, stent thrombosis is an unpredictableevent and is associated with severe consequences. Cessationof clopidogrel is an important precipitating factor, but othermechanisms must be operative in many patients.
. In carefully selected patient populations in the random-ized trials leading to FDA approval, there was nodifference in death or MI during follow-up, irrespective
Figure 1. Results of a Meta-Analysis of Studies on theEffect of PCI Versus Medical Therapy on Cardiac Death or MI
CI � confidence interval; PCI � percutaneous coronary intervention;pt � patients. Data from Katritsis et al. (15).
of whether BMS or DES were placed. This, however, is
not a universal finding, and there appear to be differencesbetween trial and registry populations, particularly thoseincluding patients with non–FDA-approved indicationsfor DES. For example, the DEScover registry enrolled6,906 patients undergoing PCI at 140 medical centersfrom January 2005 to June 2005. At 1 year, there was nodifference in the adjusted risk of death or MI betweenDES and BMS. There were, however, no differencesin the rate of stent thrombosis. This is in contrast tothe Swedish Registry, which did not find a differencein death and MI during 3 years of follow-up. How-ever, there was a difference in the temporal profile,with more adverse events in the first 6 months withBMS and more events after 6 months with DES.More data are needed particularly among higher-riskpatients who were excluded from the initial random-ized trials.
. The optimal duration of dual antiplatelet therapy withclopidogrel needs to be determined.
Optimal percutaneous approaches demand attention tontithrombotic and antiplatelet therapies (both periproce-ural and after discharge) and multiple technical issueselated to the placement of the stent; these include theppropriate size and length, selection of equipment, implanta-ion techniques, and an awareness of comorbidities and theirotential interactions with the procedure (e.g., renal failure,iabetes, and severe left ventricular [LV] dysfunction).Recent trials of PCI versus medical therapy (COURAGE
Clinical Outcomes Utilizing Revascularization and Ag-ressive DruG Evaluation]) and the MASS (Medicine,ngioplasty, or Surgery Study)-2 trial of PCI, CABG, andedical therapy have generated considerable interest and
gain draw attention to the issue of the appropriate indica-ions for coronary revascularization and particularly PCI inatients with chronic stable angina. In many respects, thendings of these contemporary trials should not come as a
Figure 2. Meta-Analysis of Stents Versus Conventional PTCAon Rate of Death or MI, Angiographic Restenosis, and Repeat PTCA
MI � myocardial infarction; PTCA � percutaneous transluminal coronary
angioplasty. Data from Brophy et al. (21).
smrit
moctahmatmqad
tafdrwtaCttvPatoirs
Cssssatsdctamw
opbfniP
prrdcmwacrdwts
T
AmmCamrbciona1o1g
tEtaeehef
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 1 , N O . 1 , 2 0 0 8
F E B R U A R Y 2 0 0 8 : 3 4 – 4 3
Holmes, Jr. et al.
PCI for Chronic Stable Angina
37
urprise because these are entirely consistent with theajority of prior trials over a 20- to 30-year period. In this
espect, a review of the results of previous randomized trialsn patients with chronic stable angina may help in placinghe recent trials into perspective.
Early trials in the 1970s and 1980s of CABG versusedical therapy compared CABG during the learning curve
f this procedure with medical therapy that would beonsidered entirely inadequate by today’s standards. None-heless, the evidence-based data from these trials suggested
survival benefit only for surgery patients at medium origher risk, including those with LV dysfunction andultivessel disease. In patients with preserved LV function
nd stable angina Canadian Cardiovascular Society Class 1o 2, there was no mortality benefit with surgery overedical therapy. Subsequent registry studies demonstrated
uite clearly the survival benefits of revascularization onlymong patients with severe symptoms and multivesselisease irrespective of LV function (29).The next series of trials compared PTCA with medical
herapy in patients with stable angina. A recent meta-nalysis demonstrated a lack of benefit in death and MIrom PCI (15,18,19,30) (Fig. 1). Nonetheless, these studiesid convincingly identify greater relief of symptoms withevascularization. More recent studies that included patientsith stents were TIME (Trial of Invasive versus Medical
herapy in Elderly patients) in elderly patients with severengina randomized to revascularization with either PCI orABG versus intensive medical therapy (31); the MASS-2
rial, which had three arms (CABG, PCI, or medicalherapy) (32); and the AVERT (Atorvastatin VErsus Re-ascularization Treatments) trial of medical therapy versusCI (19). In the AVERT trial, lipid lowering was lessggressively performed in the interventional arm. None ofhe trials demonstrated an advantage of revascularizationver medical therapy in regard to death and MI. However,n many trials, up to 50% of patients “crossed over” toevascularization with PCI or CABG due to persistentymptoms that were refractory to antianginal drug therapy.
An important early trial was the ACIP (Asymptomaticardiac Ischemia Pilot) study of 558 patients with clinically
table, angiographically documented CAD who were judgeduitable for revascularization after being diagnosed withilent ischemia on 48-h Holter monitoring (33). Threetrategies were tested: 1) angina-guided medical therapy; 2)ngina plus ischemia-guided therapy; and 3) revasculariza-ion using either surgery or PTCA. In contrast to thetudies above, total mortality, the combined end point ofeath or MI, and the end point of death, MI, or recurrentardiac hospitalization were significantly decreased in pa-ients undergoing revascularization. This was a pilot studynd emphasizes the importance of designing and imple-enting larger adequately powered trials. Similar results
ere found in the SWISSI II (Swiss Interventional Study wn Silent Ischemia Type II) trial, a small trial of 201atients with a prior MI and silent ischemia, which found aenefit for PCI in regard to recurrent events over a 10-yearollow-up period (34). Thus, it may be that, among the largeumber of patients with stable CAD, those with silent
schemia may be a high-risk group that can benefit fromCI.In summary, the evidence-based message concerning
atients with chronic stable angina is clear and consistent: 1)evascularization is associated with greater symptomaticelief but there are no differences in the “hard” end points ofeath and MI; and 2) in patients on medical therapy,rossover to revascularization is frequent. Therefore, inany patients, a trial of medical therapy is very appropriate,ith the understanding that if symptoms and quality of life
re not improved, the option of revascularization may behosen, and the price to be paid is not that of an increasedate of death or MI. These data set the stage for a criticaliscussion of the most recent trial (COURAGE) (35),hich has generated considerable emotion and some con-
roversy. The question to be addressed is whether the resultshould have come as a surprise.
he COURAGE Trial
s has been true with almost all randomized trials ofedical therapy versus a revascularization strategy, manyore patients were screened than randomized. In theOURAGE trial, 35,539 patients were initially screened,
nd 3,071 met eligibility criteria; of these 3,071 patientseeting eligibility criteria, 2,287 were enrolled. It must be
emembered that all randomized trials are subject to “entryias.” This precept stands in contrast to registries, which areharacterized by “selection bias.” The underlying hypothesisn the COURAGE trial was that a strategy of PCI withptimal medical therapy would reduce the risk of death andonfatal reinfarction compared with optimal medical ther-py alone. The 3-year event rates were projected to occur in6.4% of the PCI plus medical therapy group versus 21.0%f the medical therapy group. The actual event rates were9% in the PCI group and 18.5% in the medical therapyroup.
Crucial to the understanding of this trial is an apprecia-ion of the baseline characteristics of the patients enrolled.ven though not all patients enrolled were at very low risk,
he trial was aimed at patients with stable disease and notcute ischemic syndromes. Baseline characteristics of thenrolled patients included: 1) 42% to 43% of patients hadither no angina or only class 1 angina; 2) 30% of patientsad single-vessel disease, and approximately 35% had dis-ase involving the left anterior descending; 3) the ejectionraction was approximately 61% in both groups; and 4) DES
ere not routinely available.
utycmss
rCledtM
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 1 , N O . 1 , 2 0 0 8
F E B R U A R Y 2 0 0 8 : 3 4 – 4 3
Holmes, Jr. et al.
PCI for Chronic Stable Angina
38
In a patient such as was recruited for this trial, it isnlikely that any revascularization strategy would improvehe rate of death and MI. With an 8% mortality rate at 5ears and only 27% of those deaths being due to cardiacauses, it would also be unlikely to show or expect aortality difference. Moreover, the rate of death, MI, and
troke is approximately 20% and very unlikely to demon-
Figure 3. Evaluation of the Effects of Routine Stenting Versus Conventiona
(A) Effects on death; (B) effects on reinfarction. AS � Angioplasty or Stent; BEBOSS � Balloon Optimization versus Stent Study; CADILLAC � Controlled Abc� Doppler Endpoint Stenting International Investigation; EPISTENT � EvaluatioStenting in Acute Coronary Occlusions; FROST � French Optimal Stenting Triacoronary Stenting or Angioplasty for Restenosis Reduction in Small Arteries; MCoronary Balloon Angioplasty With Provisional Stenting Versus Primary Stent; OWith Routine Stent Strategy; OR � odds ratio; PASTA� Primary Angioplasty VeAngioplasty after Recanalization of Chronic Coronary Occlusions; SISA � StentTotal Occlusion; Stent-PAMI � Stent Primary Angioplasty in MI; STENTUIM � Imwith Conventional Balloon Angioplasty in Acute Myocardial Infarction; TOSCAfrom Brophy et al. (22).
trate a difference because neither noncardiac mortality nor t
ates of stroke would be expected to be reduced by PCI.onsequently, the only modifiable hard end point would
ikely be MI and probably Q-wave MI because biomarkerlevation occurs frequently after stenting. As previouslyiscussed, only in patients at higher risk does revasculariza-ion with PCI or CABG result in a reduction in death and
I. Even with the advent of DES, multiple randomized
A on Death and Reinfarction
NT � Belgian Netherlands Stent Study; BESMART � Bestent in Small Arteries;and Device Investigation to Lower Late Angioplasty Complications; DESTINIlatelet IIb/IIIa Inhibitor for Stenting; FRESCO � Florence Randomized ElectiveMI � Gianturco-Roubin in Acute Myocardial Infarction; ISAR-SMART � Intra-Mayo-Japan Investigation for Chronic Total Occlusion; OCBAS � Optimal
� Optimum Percutaneous Transluminal Coronary Angioplasty Comparedtent Implantation in Acute Myocardial Infarction; SARECCO � Stent orSmall Arteries; SPACTO � Stent versus Percutaneous Angioplasty in Chroniciate Coronary Angioplasty with Elective Wiktor Stent Implantation Comparedal Occlusion Study of Canada; other abbreviations as in Figure 2. Reprinted
l PTC
NESTEiximabn of Pl; GRAAJIC �
PUSrsus Sing inmed
� Tot
rials and registry studies have not documented a reduction

iB
ardawr“ooiaorgBc
rtbCrraorbSPt
pvtt
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 1 , N O . 1 , 2 0 0 8
F E B R U A R Y 2 0 0 8 : 3 4 – 4 3
Holmes, Jr. et al.
PCI for Chronic Stable Angina
39
n the hard end points of death or infarction compared withMS (23–25).Given the inability of PCI to dramatically decrease death
nd MI in this patient population with stable symptoms,elief of symptoms and prevention of the need for clinicallyriven subsequent procedures remain more important frompatient standpoint. In the COURAGE trial, angina reliefas better and quicker in the PCI group. Subsequent
evascularization in the medical group was performed forangina that was unresponsive to maximal medical therapyr when there was objective evidence of worsening ischemian non-invasive testing.” Any subsequent revascularizationn this trial was therefore clinically driven and not related toprotocol requirement. PCI showed a significant advantagever medical therapy, with a subsequent revascularizationate of 21.1% versus 32.6% in the optimal medical therapyroup (hazard ratio 0.60, 95% CI 0.51 to 0.71, p � 0.001).ased on the documented reduction of restenosis with DES
Figure 3. Continued.
ompared with BMS, it is reasonable to speculate that the c
evascularization rates in the PCI group of the COURAGErial would have been likely significantly less had DESeen used. What was surprising and gratifying in theOURAGE trial, however, was the high rate of angina
elief among medically treated patients. This may be theesult of superb adherence to protocol-driven medical ther-py. In the optimal medical therapy group, at 3 years, 75%f patients were on an ACE inhibitor or angiotensineceptor blocker, 92% were on a statin, 86% were on aeta-blocker, and 50% were on a calcium channel blocker.imilar adherence to medical therapy was also present in theCI group. This degree of adherence to evidence-based
herapy is infrequent in registry series (36).Accordingly, we could conclude that in the group of
atients with stable angina and generally well-preservedentricular function (ejection fraction approximately 61%),he application of PCI in addition to optimal medicalherapy results in improvement of symptoms and a signifi-
ant decrease in the need for subsequent revascularization in
mbr
1
2
3
4
5
Pct
culari
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 1 , N O . 1 , 2 0 0 8
F E B R U A R Y 2 0 0 8 : 3 4 – 4 3
Holmes, Jr. et al.
PCI for Chronic Stable Angina
40
any patients. There are several explanations for the lack ofenefit of PCI in the COURAGE trial and other trials ineducing death or MI:
. Cardiac mortality rates in patients with stable angina inthe current era are low.
. It is possible that drug therapy and secondary preventionimprove endothelial function and stability over the longterm.
. The potential benefits of PCI of the culprit lesion orlesions are diluted by the effects of disease progression inother vessels or the failure to provide complete revascu-larization initially.
Figure 4. Analysis of Randomized Trials of Sirolimus Versus BMS on Death
BMS � bare-metal stent; MI � myocardial infarction; TLR � target lesion revas
Figure 5. Analysis of Randomized Trials of Paclitaxel Versus BMS on Death
Abbreviations as in Figure 4. Reprinted from Stone et al. (23).
. In patients with severe stenoses treated medically, col-lateralization may play a role in alleviating symptoms,although collaterals are generally an indication of severeischemia.
. Acute coronary syndromes secondary to ruptured plaquesoccurs frequently at sites separate from areas of severestenosis, regardless of initial PCI. This observation isalso true for patients receiving optimal medical therapyalone.
otential for overuse of PCI. Given that PCI in patients withhronic stable angina is very effective in improving symp-oms but has not been shown to decrease death or MI, why
nd TLR
zation. Reprinted from Stone et al. (23).
and TLR
, MI, a
, MI,

homipt1tvdopoiav
Nualtap
atlcmWndi
diTltgnaNta
hctiira
etps1tc
C
WegaddaAtmccdttta
siTsa
wnwtTCipqdat
RDR
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 1 , N O . 1 , 2 0 0 8
F E B R U A R Y 2 0 0 8 : 3 4 – 4 3
Holmes, Jr. et al.
PCI for Chronic Stable Angina
41
as there been such controversy about the potential forveruse? Data from both Europe and the U.S. demonstratearked regional variations in the rates of PCI use, suggest-
ng that factors other than “evidence-based” medicine arelaying a role. For example, in a recent study of 11 states inhe U.S., variations in procedures performed per capita were.83-fold for PCI and 1.54-fold for CABG. Variations inhe rate of cardiac catheterization accounted for 68% of theariability in rates of revascularization, and major indepen-ent determinants of catheterization rates were the numberf cardiac surgeons and interventional cardiologists in aarticular state (37). Thus, it seems that this complex issuef potential overuse of PCI has multiple components,ncluding overuse of angiography, noninvasive coronaryngiography, fear of litigation, financial incentives for pro-iders, and self-referrals.
The variability in the rates of coronary angiography inorth America and Europe is also quite striking. A single
nified explanation to account for this is not readily avail-ble (38–40). Reasons may include access to catheterizationaboratories and availability of cardiologists, patient expec-ations, the preference of the primary caregiver, the extentnd application of specific screening approaches, and im-lementation of evidence-based guidelines.Patient desire for a “quick fix,” defensive medicine, and
lack of understanding of therapeutic choices are addi-ional confounders. This issue may become more prob-ematic with the increased application of noninvasiveomputed tomography-based coronary angiography thatay identify lesions in patients who are asymptomatic.hen lesions have been identified with noninvasive coro-
ary angiography and patient reassurance becomes moreifficult, this can be the catalyst for a cascade of events
ncluding coronary angiography and intervention.Prior to invasive coronary angiography, there is often a
iscussion with the patient regarding the course of therapyn the event that a significant lesion or lesions are found.he scene is often set for percutaneous treatment if the
esion is deemed suitable. From the patient’s standpoint,his makes intuitive sense to combine the diagnostic angio-ram and the intervention in a single setting. This “conve-ient” approach to treat what is there has become ingrainednd is part of both patients’ and physicians’ expectations.onetheless, the consequence may be the lost opportunity
o discuss all the therapeutic options in a less urgent settingnd with all the information at hand.
To further complicate matters, payers in some regionsave insisted that only interventionalists perform diagnosticatheterizations so that any lesion found may be stented athe time of the diagnostic procedure. The complex but realssues of financial incentives and self-referral cannot begnored and are an integral part of this discussion. Self-eferral eliminates some of the checks and balances that are
healthy aspect of the decision to choose among manyffective options. Likewise, cost-effectiveness is an impor-ant component. Claude et al. (41) analyzed this in elderlyatients with chronic angina. Patients undergoing an inva-ive approach had higher 30-day costs but lower 2- to2-month hospital and interventional costs than medicallyreated patients. Medical patients had higher practitionerharges.
onclusions
hat then can be said about the role of PCI in the currentra? First and foremost, in patients with stable angina and ineneral well-preserved LV function who are beginning orre already on optimal medical therapy, application of PCIoes not reduce the frequency of subsequent MI or cardiaceath; it does, however, significantly reduce angina. PCIlso reduces the need for subsequent additional procedures.n appropriate approach is to initiate a trial of medical
herapy and aggressive risk factor reduction in patients withild stable angina who are amenable to this strategy,
ushioned by the security of knowing that a subsequentrossover to PCI does not come at the price of increasedeath or MI. A crucial aspect of this discussion is ahorough understanding of the patient’s realistic expecta-ions: the impact of angina upon lifestyle and the ability toolerate medical therapy. Moreover, comprehensive second-ry prevention remains the bedrock of both strategies.
Second, DES have been found to be associated withignificant reduction in restenosis and thereby may furthermprove anginal relief in both stable and unstable patients.he issue of stent thrombosis continues to require further
tudy, as does the most appropriate duration of dualntiplatelet therapy.
Finally, the appropriate rates of use are a major concernith important socioeconomic implications. What iseeded is to establish whether use is appropriate, and, if not,hy not? It is up to the cardiovascular community to ensure
hat evidence-based medicine dominates clinical practice.he Clinical Competence Statement on Interventionalardiology of the American College of Cardiology, Amer-
can Heart Association, and Society for Cardiac Angiogra-hy and Interventions advances suggestions for maintaininguality and ensuring appropriate selection of these proce-ures (42). The credibility of what we as cardiologists dond how we implement coronary revascularization placeshe onus of responsibility on us.
eprint requests and correspondence: Dr. David R. Holmes, Jr.,epartment of Cardiology, Mayo Clinic, 200 First Street SW,ochester, Minnesota 55905. E-mail: [email protected].

R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 1 , N O . 1 , 2 0 0 8
F E B R U A R Y 2 0 0 8 : 3 4 – 4 3
Holmes, Jr. et al.
PCI for Chronic Stable Angina
42
EFERENCES
1. Gruntzig A. Transluminal dilatation of coronary-artery stenosis. Lan-cet 1978;1:263.
2. Gruntzig AR, Senning A, Siegenthaler WE. Nonoperative dilation ofcoronary artery stenosis: percutaneous transluminal coronary angio-plasty. N Engl J Med 1979;301:61–8.
3. Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelinesfor the management of patients with ST-elevation myocardial infarc-tion—executive summary: a report of the American College of Cardi-ology/American Heart Association Task Force on Practice Guidelines(Writing Committee to Revise the 1999 Guidelines for the Manage-ment of Patients with Acute Myocardial Infarction) (erratum in J AmColl Cardiol 2005;45:1376). J Am Coll Cardiol 2004;44:671–719.
4. Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intrave-nous thrombolytic therapy for acute myocardial infarction: a quantita-tive review of 23 randomised trials. Lancet 2003;361:13–20.
5. Fragmin and Fast Revascularisation during InStability in Coronaryartery disease Investigators. Invasive compared with non-invasivetreatment in unstable coronary-artery disease: FRISC II prospectiverandomized multicentre study. Lancet 1999;354:708–15.
6. Fox KA, Poole-Wilson PA, Henderson RA, et al. Interventional versusconservative treatment for patients with unstable angina or non–ST-elevation myocardial infarction: the British Heart Foundation RITA 3randomised trial: Randomized Intervention Trial of Unstable Angina.Lancet 2002;360:743–51.
7. Mehta SR, Cannon CP, Fox KA, et al. Routine vs selective invasivestrategies in patients with acute coronary syndromes: a collaborativemeta-analysis of randomized trials. JAMA 2005;293:2908–17.
8. Chaitman BR, Pepine CJ, Parker JO, et al. Effects of ranolazine withatenolol, amlodipine, or diltiazem on exercise tolerance and anginafrequency in patients with severe chronic angina: a randomized con-trolled trial. JAMA 2004;291:309–16.
9. Chaitman BR, Skettino SL, Parker JO, et al. Anti-ischemic effects andlong-term survival during ranolazine monotherapy in patients withchronic severe angina. J Am Coll Cardiol 2004;43:1375–82.
0. Chaitman BR. Ranolazine for the treatment of chronic angina andpotential use in other cardiovascular conditions. Circulation 2006;113:2462–72.
1. McGrath PD, Malenka DJ, Wennberg DE, et al. Changing outcomesin percutaneous coronary interventions: a study of 34,752 procedures innorthern New England, 1990 to 1997. Northern New England Cardio-vascular Disease Study Group. J Am Coll Cardiol 1999;34:674–80.
2. Seshadri N, Whitlow PL, Acharya N, et al. Emergency coronary arterybypass surgery in the contemporary percutaneous coronary interventionera. Circulation 2002;106:2346–50.
3. Williams DO, Holubkov R, Yeh W, et al. Percutaneous coronaryintervention in the current era compared with 1985–1986: the NationalHeart, Lung, and Blood Institute Registries. Circulation 2000;102:2945–51.
4. Rankin JM, Spinelli JJ, Carere RG, et al. Improved clinical outcomeafter widespread use of coronary artery stenting in Canada. N EnglJ Med 1999;341:1957–65.
5. Katritsis DG, Ioannidis JP. Percutaneous coronary intervention versusconservative therapy in nonacute coronary artery disease: a meta-analysis. Circulation 2005;111:2906–12.
6. King SB 3rd. Angioplasty is better than medical therapy for alleviatingchronic angina pectoris. Arch Intern Med 2005;165:2589–92.
7. Shroff AR, Cohen DJ. Does stenting save lives? Understanding thestrengths and limitations of meta-analysis. Am Heart J 2004;147:756–8.
8. Parisi AF, Folland ED, Hartigan P. A comparison of angioplasty withmedical therapy in the treatment of single-vessel coronary arterydisease. N Engl J Med 1992;326:10–16.
9. Pitt B, Waters D, Brown WV, et al. Aggressive lipid-lowering therapycompared with angioplasty in stable coronary artery disease. N EnglJ Med 1999;341:70–76.
0. Henderson RA, Pocock SJ, Clayton TC, et al. Seven-year outcome inthe RITA-2 trial: coronary angioplasty versus medical therapy. J Am
Coll Cardiol 2003;42:1161–70.1. Brophy JM, Belisle P, Joseph L. Evidence for use of coronary stents. Ahierarchical Bayesian meta-analysis. Ann Intern Med 2003;138:777–86.
2. Al Suwaidi J, Holmes DR Jr, Salam AM, et al. Impact of coronaryartery stents on mortality and nonfatal myocardial infarction: meta-analysis of randomized trials comparing a strategy of routine stentingwith that of balloon angioplasty. Am Heart J 2004;147:815–22.
3. Stone GW, Moses JW, Ellis SG, et al. Safety and efficacy of sirolimus-and paclitaxel-eluting coronary stents. N Engl J Med 2007;356:998–1008.
4. Spaulding C, Daemen J, Boersma E, Cutlip DE, Serruys PW. Apooled analysis of data comparing sirolimus-eluting stents with bare-metal stents. N Engl J Med 2007;356:989–97.
5. Kastrati A, Mehilli J, Pache J, et al. Analysis of 14 trials comparingsirolimus-eluting stents with bare-metal stents. N Engl J Med 2007;356:1030–9.
6. Lagerqvist B, James SK, Stenestrand U, Lindback J, Nilsson T,Wallentin L. Long-term outcomes with drug-eluting stents versus baremetal stents in Sweden. N Engl J Med 2007;356:1009–19.
7. Mauri L, Hsieh W, Massaro JM, Ho KKL, D’Agostino R, Cutlip DE.Stent thrombosis in randomized clinical trials of drug-eluting stents.N Engl J Med 2007;356:1020–9.
8. Holmes DR Jr., Kereiakes DJ, Laskey WK, et al. Thrombosis anddrug-eluting stents: an objective appraisal. J Am Coll Cardiol 2007;50:109–18.
9. Rihal CS, Raco DL, Gersh BJ, Yusuf S. Indications for coronary arterybypass surgery and percutaneous coronary intervention in chronic stableangina: review of the evidence and methodological considerations.Circulation 2003;108:2439–45.
0. RITA-2 Trial Participants. Coronary angioplasty versus medical ther-apy for angina: the second Randomised Intervention Treatment ofAngina (RITA-2) trial. Lancet 1997;350:461–8.
1. The TIME Investigators. Trial of Invasive versus Medical therapy inElderly patients with chronic symptomatic coronary-artery disease(TIME): a randomised trial. Lancet 2001;358:951–57.
2. Hueb W, Soares PR, Gersh BJ, et al. The Medicine, Angioplasty, orSurgery Study (MASS-II): a randomized, controlled clinical trial ofthree therapeutic strategies for multivessel coronary artery disease:one-year results. J Am Coll Cardiol 2004;43:1743–51.
3. Davies RF, Goldberg AD, Forman S, et al. Asymptomatic CardiacIschemia Pilot (ACIP) study two-year follow-up: outcomes of patientsrandomized to initial strategies of medical therapy versus revascular-ization. Circulation 1997;95:2037–43.
4. Erne P, Schoenenberger AW, Burckhardt D, et al. Effects of percuta-neous coronary interventions in silent ischemia after myocardial infarc-tion: the SWISSI II randomized controlled trial. JAMA 2007;297:1985–91.
5. Boden WE, O’Rourke RA, Teo KK, et al. Optimal medical therapywith or without PCI for stable coronary disease. N Engl J Med2007;356:1503–16.
6. Mehta RH, Roe MT, Chen AY, et al. Changing practice fornon–ST-segment elevation acute coronary syndromes: trends from theCRUSADE quality improvement initiative. Circulation 2005;112:II793.
7. Hannan EL, Wu C, Chassin MR. Differences in per capita rates ofrevascularization and in choice of revascularization procedure for elevenstates. BMC Health Serv Res 2006;6:35.
8. Hartford K, Ross LL, Walld R. Regional variation in angiography,coronary artery bypass surgery, and percutaneous transluminal coronaryangioplasty in Manitoba, 1987 to 1992: the funnel effect. Med Care1998;36:1022–32.
9. Pilote L, Califf RM, Sapp S, et al. Regional variation across the UnitedStates in the management of acute myocardial infarction. GUSTO-1Investigators. Global Utilization of Streptokinase and Tissue Plasmin-ogen Activator for Occluded Coronary Arteries. N Engl J Med1995;333:565–72.
0. Gatsonis CA, Epstein AM, Newhouse JP, Normand SL, McNeil BJ.Variations in the utilization of coronary angiography for elderlypatients with an acute myocardial infarction. An analysis using hierar-
chical logistic regression. Med Care 1995;33:625–42.
4
4
J A C C : C A R D I O V A S C U L A R I N T E R V E N T I O N S , V O L . 1 , N O . 1 , 2 0 0 8
F E B R U A R Y 2 0 0 8 : 3 4 – 4 3
Holmes, Jr. et al.
PCI for Chronic Stable Angina
43
1. Claude J, Schindler C, Kuster GM, et al. Cost-effectiveness of invasiveversus medical management of elderly patients with chronic symptom-atic coronary artery disease. Findings of the randomized Trial ofInvasive versus Medical therapy in Elderly patients with chronic angina(TIME). Eur Heart J 2004;25:2195–203.
2. King SB, Aversano T, Ballard WL, et al. ACCF/AHA/SCAI 2007
update of the clinical competence statement on cardiac interventionalprocedures: a report of the American College of CardiologyFoundation/American Heart Association/American College of Physi-cians Task Force on Clinical Competence and Training (WritingCommittee to Update the 1998 Clinical Competence Statement onRecommendations for the Assessment and Maintenance of Proficiencyin Coronary Interventional Procedures). J Am Coll Cardiol 2007;
50:82–108.