Embed Size (px)
Citation preview
Remedy Publications LLC., | http://clinicsinsurgery.com/
Clinics in Surgery
2016 | Volume 1 | Article 12681
Coronary Artery Bypass Surgery vs. Percutaneous Coronary Intervention: Current Status
OPEN ACCESS
*Correspondence:Yadava OP, Department of Cardiac
Surgery, National Heart Institute, 49-50, Community Centre, East of Kailash,
New Delhi - 11 00 65, India,E-mail: [email protected]
Received Date: 07 Nov 2016Accepted Date: 23 Dec 2016Published Date: 28 Dec 2016
Citation: Yadava OP. Coronary Artery Bypass Surgery vs. Percutaneous Coronary
Intervention: Current Status. Clin Surg. 2016; 1: 1268.
Copyright © 2016 Yadava OP. This is an open access article distributed under
the Creative Commons Attribution License, which permits unrestricted
use, distribution, and reproduction in any medium, provided the original work
is properly cited.
Review ArticlePublished: 28 Dec, 2016
AbstractBoth coronary artery bypass surgery and percutaneous interventions are competing for numero-uno position for coronary revascularisation. Though there have been significant advances in percutaneous interventions, yet they have not been perfected enough to give results equivalent to CABG in all clinical and anatomical scenarios and infact are not universally applicable also. There are guidelines, yet those are being flouted and certain ambiguities are exploited by either side to suit the procedure, not to the patient but to the doctor delivering it. This critical review thus looks at bypass surgery and PCI in light of currently available data and highlights the pitfalls in the available therapies. Certainly PCI is evolving and has come a long way and for simpler coronary anatomies may be the preferred line of myocardial revascularisation, but certainly it has not replaced bypass surgery. The two infact should be viewed as complementary to each other with each having its niche area and domain.
Keywords: Coronary artery bypass surgery; Percutaneous coronary
Yadava OP*
Department of Cardiac Surgery, National Heart Institute, India
IntroductionEver since 1977 when Gruentzig performed the first percutaneous coronary angioplasty
(PTCA) [1], its scope has been gradually widened. It is now being applied to more complex and multi vessel lesions. Even coronary artery bypass surgery (CABG) has seen dramatic advances since its introduction in 1967 by Favalaro [2]. Infact lately CABG has become less invasive and, notwithstanding the raging debate between off pump versus pump surgery [3], over 99% of coronary work in our centre is being performed off pump, while cardiologists are becoming more invasive. There is obviously a keen tussle between the two procedures and it’s time to relook at the current status of each in light of its counterpart.
Till date all randomized controlled trials (RCTs) that have looked at CABG versus Percutaneous Interventions (PCI) have come to a common conclusion that there is no difference between the two with regard to early mortality and myocardial infarction (MI) but angina relief and rates of repeat revascularization are overwhelmingly in favour of CABG. Introduction of Drug Eluting Stents (DES) and more recently the biodegradable stents, have given further impetus to PCI with the hope that with reduction in the rates of restenosis, the latter two disadvantages of PCI would be eliminated. However, this hope is based on a faulty premise as coronary artery disease (CAD) is not a localized pathology but is segmental in nature and as against PCI, which addresses a discrete localized lesion, CABG bypasses the whole diseased segment, and therefore intuitively speaking also, CABG is likely to be more effective than PCI [4]. This prompted Spencer B King III to comment, ”Five years after stent implantation almost twice as many events are related to factors other than restenosis.” Infact some of these factors may be natural history-driven [5]. Let’s look at some of these issues more closely.
Is Angioplasty Applicable Universally?Angioplasty is not universally applicable and if we look at RCTs between PTCA and CABG
in multivessel CAD, one finds that barely half of the patients who required revascularisation were eligible for either procedure that is PTCA or CABG. The rest of the patients were not suitable for PTCA because they either suffered from diffused atherosclerosis, multiple lesions, chronic total occlusion, calcified lesions, type C lesions, small size of the coronary vessels, severe LV dysfunction, and presence of LV clot/LV aneurysm, presence of peripheral vascular disease or other associated anomalies. In these kinds of lesions, usually PTCA is not possible but with modern technology and improvement in hardware as well as the experience gained over last decade, most of these

Yadava OP Clinics in Surgery - Cardiovascular Surgery
Remedy Publications LLC., | http://clinicsinsurgery.com/ 2016 | Volume 1 | Article 12682
lesions may now be tackled, albeit with suboptimum outcomes [6]. In the pivotal SYNTAX Trial, which compared DES with CABG, 35% of patients were rejected for PTCA because of unsuitable coronary anatomy [7].
Has the Restenosis been Eliminated?Though the DES have revolutionized PCI and compared to
Bare Metal Stents (BMS), the restenosis rates have come down dramatically, but they are still significant. Currently accepted figures are 8.9% at 8 months with Sirolimus eluting stents (SES) [8]. 7.9% at 9 months with Paclitaxel eluting stents (PES) [9] and 15.3% at 8 months with Zotarolimus eluting stents (ZES) [9,10]. The 4.7% restenosis at 8 months and improved MACE at 2 years reported in the SPIRIT III Trial [11,12], for Everolimus eluting stents (EES) was for a very limited subset of patients. Here lesions more than 28mm in length and vessel size <2.5 mm were excluded and the angiographic follow up was done in only 50% of patients [11]. Besides lesion length and lesion type (B2/C), smaller vessel size is a strong predictor of TLR [13]. Even in chronic total occlusion, the results of PCI are suboptimum. Besides technical failure (38.7% in New York PCI Registry), even if one successfully opens the artery, the binary restenosis was 22.6% for the entire treated segment in the ACROSS/TOSCA - 4 Trial with 16% incidence of stent fractures and 25% of these needing TLR within the first six months [14], besides a host of other serious complications like increased coronary perforation (RR 5.0; p< 0.001) and cardiac tamponade (RR 5.0; p< 0.01) [15].
Even the next generation Bioresorbable (BRS) stents have not tilled now achieved the desired goal. There are issues related to radial strength, dilatation range, visibility on imaging, thick struts, deliverability etc. The binary restenosis in the ABSORB Study was 12% at one year [16]; overall TLR was 45% at 12 months with Bioabsorbable magnesium stents in the PROGRESS Study [17] and 13% in the GENOUS Healing Stent Trial with antibody coated stents to capture endothelial progenitor cells [18]. Even in the ISAR TEST IV Study at 4-12 months follow up, binary restenosis was 12% with SES with disappearing polymer [19] Drug eluting balloons too have not survived the scrutiny at 9 months. In the PEPCAD III Trial, instent late loss with drug eluting balloons was 0.41, MI at 9 months 4.6%, stent thrombosis 2.0% and target vessel revascularisation (TVR) 13.8%, all of which parameters were statistically significantly higher than with DES [20].
These results have improved only marginally, if at all, over time. Raungaard et al. [21], comparing Biodegradable Polymer Versus durable Zotarolimus Eluting Stents found no difference in primary end points of mortality, MI and TLR at 12 months (5.0 Versus 5.3%). Even in ABSORB Japan Study [22] barely equivalency of results was achieved with Cobalt Chromium Everolimus Eluting Stents. To the contrary, in ABSORB III study [23] TLF was 7.8% with BRS platform as compared to 6.1% for durable platform (p-0.007). So the dream of zero restenosis has not been achieved till now. More over restenosis is not a benign event & may present as Acute Coronary Syndrome in upto two thirds of patients with increased mortality - HR 1.23; p-0.02 [24,25].
Then there is the problem of catch up restenosis [26]. This late luminal creep begins to come at around 6 months and goes on till two years, and translates into increased clinical events and TLR at 2 years of up to 24.1% with Taxus stents, 18.8% with Cypher stents and 17.4% with ISAR stents. Similar late catch up phenomenon has been reported with Xience stents at 6 and 24 months in the Spirit II Trial
[27] and continues unabated with BRS platform. Infact Zhang et al. [28], in an OCT Study of ABSORB Cohort B, found edge vascular response, at both proximal and distal edges, which was progressive till at least 3 years and Cassese et al. [29,30] found late lumen loss at 6 months to be higher with BRS platform (0.30+0.59 mm) as compared to DES (0.22+0.48; p-0.035), a finding confirmed by the ABSORB II [31] - 3 year results presented at TCT meet at Washington in November 2016.
No wonder then, that 30 days readmission rates with PCI despite all the advances in stent technology, have not come down - 16.1% in 2000 and 15.4% in 2012, with 4 times higher mortality in these patients [30].
Completeness of RevascularisationTamburino et al. [32] achieved complete revascularization in only
41.7% of patients with multi vessel disease undergoing PCI with DES. They also found that complete revascularization reduced cardiac death (hazard ratio 0.37; p=0.03), death and MI (hazard ratio 0.34; p=0.008) and repeat revascularization (hazard ratio 0.45; p=0.0003) and were corroborated by Garcia et al. [33]. In SYNTAX trial [34] complete revascularization was achieved in 63.2% in CABG group as against 56.7% with PCI (p=0.005) and in the ACUITY Study [35], 60% had incomplete revascularisation following PCI with 18.7% having a residual SYNTAX Score of >18.7% translating into incrementally higher event rates proportionate to residual SYNTAX Score with each one point increase contributing to 6% increase in cardiac mortality, 2% increase in MI and 4% in TVR.
It is therefore not surprising to note that Curtis et al. [36] in their review of 3, 15, 241 patients in 1,108 hospitals performing >50 angioplasties per year, found a readmission rate of 14.6% with PCI at 30 days. One fifth of these readmissions were for acute events like MI, unstable angina, arrhythmias and heart failure and nearly 27.5% of these patients needed repeat revascularisation.
Diabetes Mellitus & Other Co-morbiditiesDiabetic patients are altogether different ball game clinically,
anatomically, etiopathologically, biologically, angiographically and rheologically. They have small caliber and diffusely diseased vessels, which are involved more distally with poor collaterals and a milieu interior of increased thrombogenecity, endothelial dysfunction and altered platelet function [37]. They also have associated co morbidities like renal dysfunction, peripheral and carotid vascular disease and pan microvascular dysfunction.
From the historical BARI Trial [38], through the ARTS [39] and Northern New England Cardiovascular Disease [40] studies, the VA Cards Study [41], Cardia Trial [42], ASCERT Study [43] to the contemporary FREEDOM Trial [44], that one groups of patients where consensus is unanimous that CABG is the preferred mode of myocardial revascularisation.
Though the use of DES [45-47] and Glycoprotein IIb IIIa inhibitors [48] have been shown to bring the restenosis rates down, Insulin treated diabetics still do less well with PCI as compared to non insulin treated diabetics [47]. In Swedish Registry [49,50], besides incomplete revascularization with PCI, Insulin dependent DM had higher restenosis (HR 1.54) and stent thrombosis (HR 1.56). When we compare the results of PCI Vs CABG, certainly CABG scores over PCI for both Non Insulin Dependent DM (HR 1.46) and Insulin dependent DM (HR 1.21). BARI 2D Study clearly showed that the

Yadava OP Clinics in Surgery - Cardiovascular Surgery
Remedy Publications LLC., | http://clinicsinsurgery.com/ 2016 | Volume 1 | Article 12683
mortality and early MACE were exactly the same with CABG and PCI but CABG decreased cardiovascular event rates and CABG in insulin sensitive group fared the best (p=0.01) [51]. Even in head to head comparison between PCI and CABG in diabetics in the Cardia Trial, though the one year primary end points of mortality, MI and stroke were the same in both the groups (10.5% in CABG Group and 13.0% in the PCI group (p=0.39), revascularization was 9.9% in the PCI group Vs 2% with CABG (p=0.001) and composite MACE was 19.3% with PCI Vs 11.3% with CABG (p=0.02) [52]. In the SYNTAX Diabetes Sub study (n=452), repeat revascularization at one year with PES was 20.3% as against 6.4% with CABG (p< 0.001) [53] with an overall MACE of 26% and 14.2% respectively (p=0.0025). Besides there may be mortality benefit for CABG as shown by Tu et al. [54] and FREEDOM Study [55] - 5 yr all cause mortality 16.3% in PCI group versus 10.9% in CABG (p-0.005). These results were confirmed in a number of studies [56] and meta-analyses [57,58].
Even the newer DES have not made much impression in diabetic population [59] and in SPIRIT IV [60], ENDEAVOR IV [61] and the COMPARE Trials [62] results of EES & ZES were the same as PES in diabetics though the former two had improved outcomes over PES in non diabetics. Therefore Boden and Taggart writing an editorial for the BARI 2D Trial commented, “….. when revascularization is indicated, both BARI 2D and other studies support the use of CABG as the preferred approach, unless and until future studies indicate otherwise” [63].
CABG is the preferred mode of revascularisation in presence of other co-morbidities as PCI under performs in situations of chronic kidney disease [64,65], LV dysfunction [66] and Hypothyroidism [67].
Does Surgery Confer a Survival Advantage over PCI?
The answer to this question is a categorical ‘Yes’. It has been demonstrated quite conclusively in a number of studies that CABG gives survival advantage which PCI is not able to provide. In the SOS Trial [68] at 6 years, mortality was 10.9% with PCI, as against 6.8% with CABG, p=0.002. Even in the New York Registry data published by Hannan et al. [69], there was statistically significant increase in both survival and MI free survival at 18 months with bypass surgery as against DES. Similar findings were reported in a propensity score matched analysis of 105,106 patients by Hlatky et al. [70], where an 8% decrease in mortality was demonstrated with CABG over PCI on a 5 year follow up. Even Trikalinos et al. [71], in a meta analysis of 61 randomized trials of PCI including 25,388 patients over a 20 years period, reported, ‘Cumulative advances in PCI have not translated into an improvement in survival or a reduction in MI’, a statement finding resonance in SYNTAX Trial [72] and large databases like ACCF Registry and STS National Database [43], and this survival gets magnified as we follow patients longer and longer with survival curves still diverging at 5 years [43].
This survival advantage get larger in diabetics (one year mortality 12.5% with PES Vs 5.7% with CABG and cardiac death 10.2% with PES Vs 3.4% with CABG) and in those with Syntax Score >33, (one year mortality was 13.5% with PES Vs 4.1% with CABG) [53]. In the BARI 2D Study too, the mortality at five years was lowest in the CABG strata followed by optimum medical therapy and highest in the PCI strata [51]. This survival advantage of CABG over PCI gets magnified with multi arterial CABG (p< 0.001). Comparison of 9-year
propensity-matched reintervention-free survival data for both PCI treatment cohorts with each separately compared with SA-CABG and MA-CABG surgery: (A) BMS-PCI versus SA-CABG; (B) BMS-PCI versus MA-CABG; (C) DES-PCI versus SA-CABG; and (D) DES-PCI versus MA-CABG. The p values were derived by log-rank test. SA-Single arterial; MA-Multi arterial [73].
Are Drug Eluting Stents Entirely Safe?Though the brouhaha raised during the World Congress in
Barcelona was over hyped and not called for and the relative safety of DES have been demonstrated by the Bern-Rotterdam Registry, SCAAR Registry, Dynamic Registry and the Basket - Late Trials, yet there are a lot of safety concerns with DES. Togni et al. [74] have very conclusively demonstrated that DES induced endothelial dysfunction and they also lead to an impaired coronary vasomotor response also shown by Kim et al. [75] and very recently Tsuburaya et al. [76] Even with BRS platform Serruys et al. [31] found no improvement in vaso-motor tone of the stented vessel at a time when BRS should have disappeared and tone normalised. Not only do they affect the stented segment, but contributed to acceleration of atherosclerosis even in non stented coronary segments leading some times to MI - ‘Pro Inflammatory’ effect of the DES [77]. Renu Virmani, Aloke Finn and Joner have been demonstrating and espousing the negative effects of DES for long [78]. They have conclusively shown that DES lead to decreased neo-intima formation with exposed struts, malapposition and macrophage infiltration and they do lead to formation of vulnerable plaques. Late aneurysm formation has been reported in as many as 1.25% [79] cases and stent malapposition in 10-25% [80]. Terminologies like malapposition and edge dissection actually came into vogue only after the introduction of DES and may occur late [80,81]. Late thrombosis is another major issue with DES and in most studies has been shown to be around 0.6% - 1% per year out to 3-5 years (ERACI III Study [82], Bern - Rotterdam Registry [83], ESTROFA Study [84] and D-DELTA Reg [85]. Infact Serruys et al. [86] in their comparison of ARTS II DES with ARTS I CABG have reported an incidence of definite, probable or possible stent thrombosis (ST) according to the ARC definition of 9% at 5 years. Even in D-DELTA Registry [85], it was 5% & may occur as late as 7.3 years [87]. Taniwaki et al. [88] in an OCT based study propounded multiple mechanisms for ST like strut mal-apposition (34.5%); neo-atherosclerosis (27.6%); uncovered stent, stent under expansion etc & found more than one mechanism responsible for ST in 55% of patients. Similar findings were reported by Souteyrand et al. [89] in PESTO Reg.
BRS platform provide no respite. Infact to the contrary Puricel et al. [90] reported 1 year ST of 3% in a series of 1305 patients with 52% presenting as MI and 17% having sudden cardiac death. Increased tendency of BRS platform for ST has been confirmed in Med Star CV Research Network meta-analysis [91] (p-0.02) and Lancet meta-analysis [92] (p-0.02), besides large registries like German/Swiss Registry [90] (3% at 12 months) and ISAR - ABSORB Registry [93] (2.6% at 12 months) with poor outcomes.
This is certainly a cause of concern, especially for patients who are either resistant or recalcitrant to usage of antiplatelet medicines. Antiplatelet resistance has been reported in 5-45% of cases and MACE increases many folds in these patients [94,95]. Diabetic subjects have a higher number of Clopidogrel non responders (p=0.04) and increased platelet reactivity leading to increased atherothrombotic risks [96]. Further 32.4% of the patients taking antiplatelets experience bleeding

Yadava OP Clinics in Surgery - Cardiovascular Surgery
Remedy Publications LLC., | http://clinicsinsurgery.com/ 2016 | Volume 1 | Article 12684
and 11.1% sufficient to force the individual to stop the antiplatelet medication [97], thus predisposing to late stent thrombosis. In the ADAPT-DES Study [98], those who bled had a higher mortality of 13% versus 3.2% in those, who did not (HR 5.03; p< 0.0001). Also should a person need non cardiac surgery during the first one year, and then he is faced with the difficult choice of managing bleeding versus antiplatelet medications.
DES also led to reduce collateral growth and therefore any subsequent coronary event is likely to be serious [99]. It may be for this reason that death/MI beyond 6 months was 9.1% after DES versus 3.8% with BMS (p=0.009) at 3 years in the BASKET Trial [100].
New disease pathologies keep emerging as we follow patients longer following PCI like neoatherosclerosis [101] and vulnerable plaques, concertina effect [102] and Kounis Syndrome [103] - a continuous, chronic repetitive, hypersensitivity induced inflammation of coronaries producing acute coronary syndrome. Post PCI, OCT & IVUS have given us new insights. Seoda et al. [104] in the MGH-OCT Registry of 786 patients found incomplete stent apposition in 39.1%, stent edge dissection in 30% (only 1.4% picked up on cine angio), irregular protrusions in 53.8% and disrupted fibrous tissue in 61% patients, leading to device oriented clinical end points of 4.2% at 1 year. Stent fractures were demonstrated in 22% stents by Kan et al. [105] translating into instent restenosis (42.1%), increased TLR (24.8%) and definitive ST in 4.6%.
In BRS platform, there are additional technical difficulties due to thick struts and imaging and deliverability issues. In ABSORB II Study [106], barely 8% of BRS and 20% of Everolimus Eluting Stents had optimum device expansion with both asymmetric (p-0.007) and eccentric (p< 0.004) implants leading to MACE. Similarly Gori et al. [107] demonstrated evagination in 54% BRS and periscaffold aneurysm in 4% in an OCT based study.
Quality of Life and Cost ConsiderationsOne has to keep in mind the social obligations that we have to
our relatively impoverished society. Cost considerations cannot be ignored and DES, not only in a scenario of multi vessel CAD [108,109], but also in single vessel LAD stenosis [110,111], is not cost effective. Even in Syntax subset of patients, when quality of life and economics were analysed, it was found that at one year angina relief was much better with CABG and in patients with Syntax score of >33, CABG was cost effective. Also the follow up costs with PCI were much higher [112]. These are data for western patients and calculated according to western criteria, while in developing world, this cost consideration gets overwhelmingly weighted in favour of bypass surgery. Early short term gains of PCI get neutralized by 3 years and there was no difference in quality of life between PCI & CABG in diabetics [113].
Long Term Safety and Performance Profile of DES
These issues are essentially subjudice and as against CABG where almost 20-30 year results are now available, we barely have five year results with evidence of late ‘catch up’ restenosis manifesting at around two years [26, 27]. Philpott et al. [114] have clearly shown that the reduced restenosis benefit of DES, present in the first year, is lost by the third year and survival between BMS and DES at 3 years is equivalent [67]. In COURAGE Trial also, early gains of PCI were lost by 3 years [115].
Left Main Stenosis – Is it a Surgical Bastion?Certainly not anymore! After the LE MANS Registry [116]
showed improved outcomes with DES in left main, the Syntax trial has conclusively shown that in isolated left main and when associated with single vessel disease, the results of angioplasty are quite satisfactory
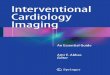
Figure 1: Pair wise PCI Versus CABG Comparisons of Match-Adjusted Unplanned Reintervention.
Yadava OP Clinics in Surgery - Cardiovascular Surgery
Remedy Publications LLC., | http://clinicsinsurgery.com/ 2016 | Volume 1 | Article 12685
[7]. Also osteal and mid shaft lesions with low Syntax Score do fairly well with angioplasty. However, distally located lesions [117] (more than 60-70%), high Syntax Score >33 [118], those associated with double or triple vessel CAD (67.5%) [7] And LV dysfunctions are still in the surgical domain [119].
PCI in distal LM has issues both when the bifurcation angle is shallow [120] and when it is steeper [121] leading to increased atherosclerosis. Restrictive bifurcation angle was an independent predictor of MACE (HR 2.65; p< 0.001) even in the SYNTAX-LM Sub study [121].
MAIN COMPARE [122], PRECOMBAT [123] and other studies have shown that early events like death, MI and stroke are exactly the same between stent and CABG but repeat revascularization is much higher with stents as compared to CABG. In CREDO-KYOTO Registry [124], surgery was superior and even in matters of CVA it was equivalent to PCI at 5 years. In EXCEL Trial [125] however PCI fared better than CABG in low and intermediate SYNTAX scores with 39% reduction in mortality, MI and strokes (HR 0.61; p-0.008) at 30 days but there were higher catch up primary end points at 3 years (11.5% Vs 7.9% with CABG; p-0.02) - Ref. (Figure 1).
NOBLE Trial [126] however showed higher MACCE at 5 years with PCI (28.9%) as compared to CABG (19.1%). In a subgroup analysis of PRE COMBAT and SYNTAX Cohorts, Cavalcante et al. [127] too demonstrated 5 years MACE of 23.0% with CABG as against 28.3% with PCI (HR 1.23) mainly driven by repeat revascularisation (HR 1.85, p< 0.001).
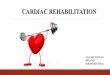
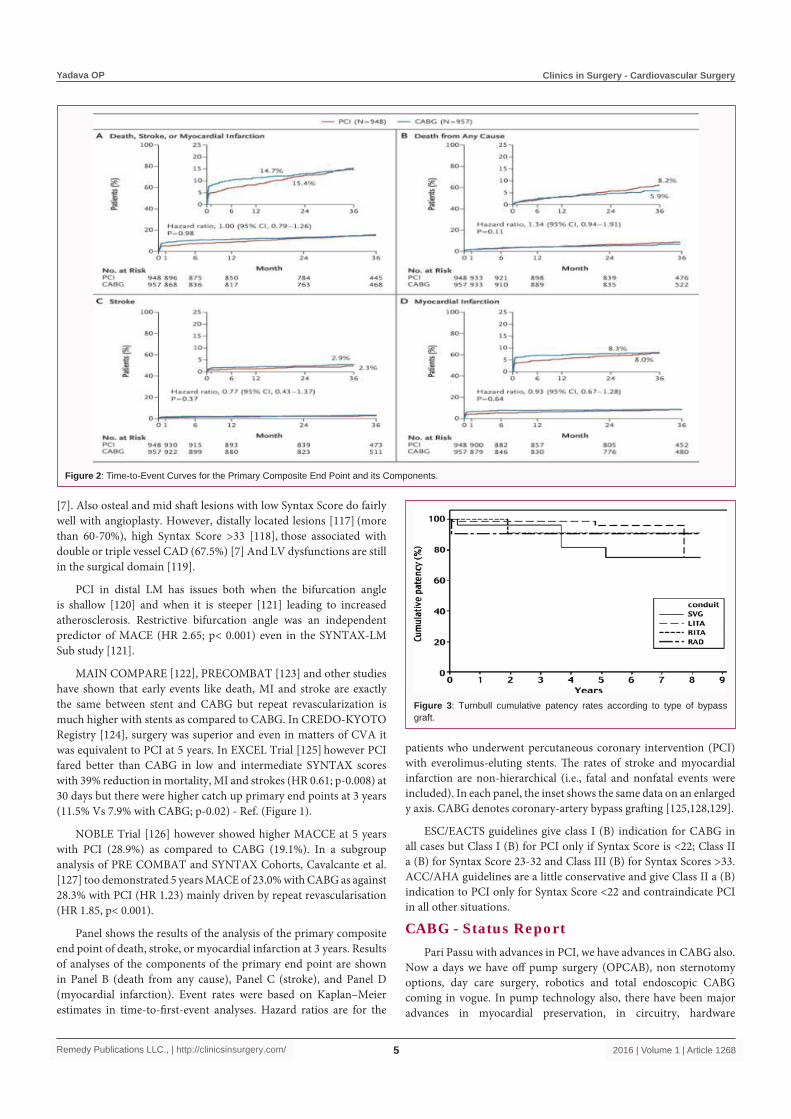
Panel shows the results of the analysis of the primary composite end point of death, stroke, or myocardial infarction at 3 years. Results of analyses of the components of the primary end point are shown in Panel B (death from any cause), Panel C (stroke), and Panel D (myocardial infarction). Event rates were based on Kaplan–Meier estimates in time-to-first-event analyses. Hazard ratios are for the
patients who underwent percutaneous coronary intervention (PCI) with everolimus-eluting stents. The rates of stroke and myocardial infarction are non-hierarchical (i.e., fatal and nonfatal events were included). In each panel, the inset shows the same data on an enlarged y axis. CABG denotes coronary-artery bypass grafting [125,128,129].
ESC/EACTS guidelines give class I (B) indication for CABG in all cases but Class I (B) for PCI only if Syntax Score is <22; Class II a (B) for Syntax Score 23-32 and Class III (B) for Syntax Scores >33. ACC/AHA guidelines are a little conservative and give Class II a (B) indication to PCI only for Syntax Score <22 and contraindicate PCI in all other situations.
CABG - Status ReportPari Passu with advances in PCI, we have advances in CABG also.
Now a days we have off pump surgery (OPCAB), non sternotomy options, day care surgery, robotics and total endoscopic CABG coming in vogue. In pump technology also, there have been major advances in myocardial preservation, in circuitry, hardware
Figure 2: Time-to-Event Curves for the Primary Composite End Point and its Components.
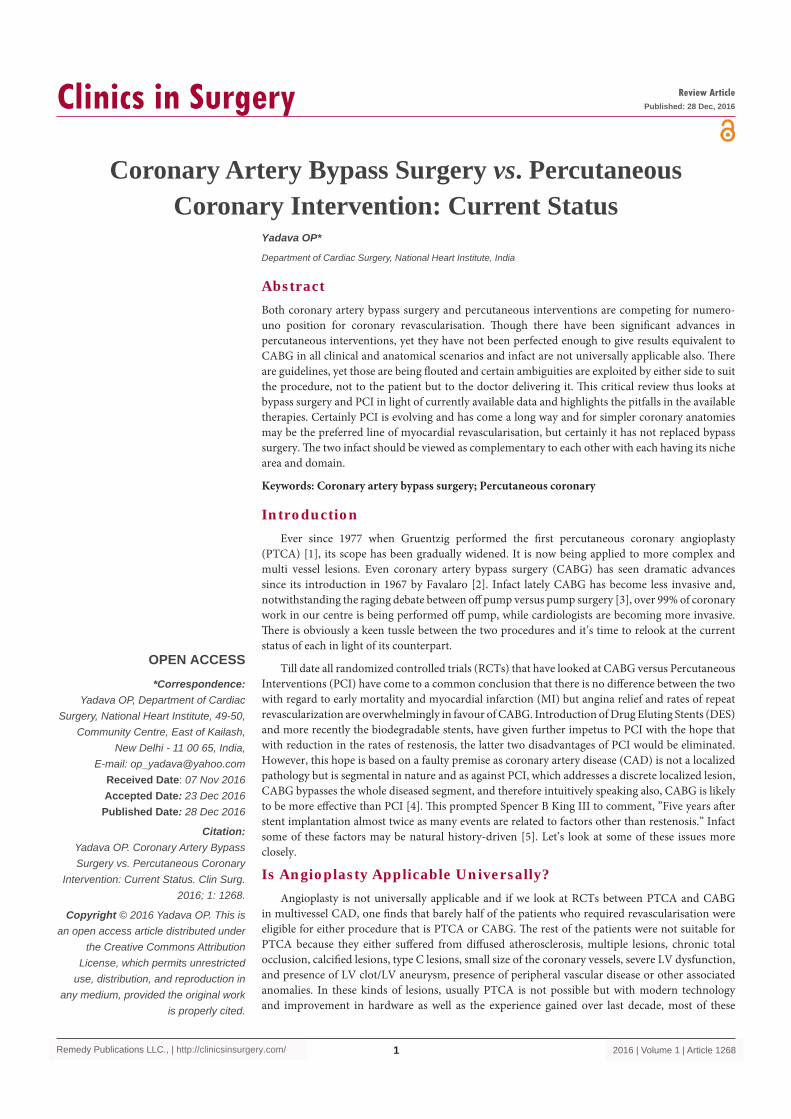
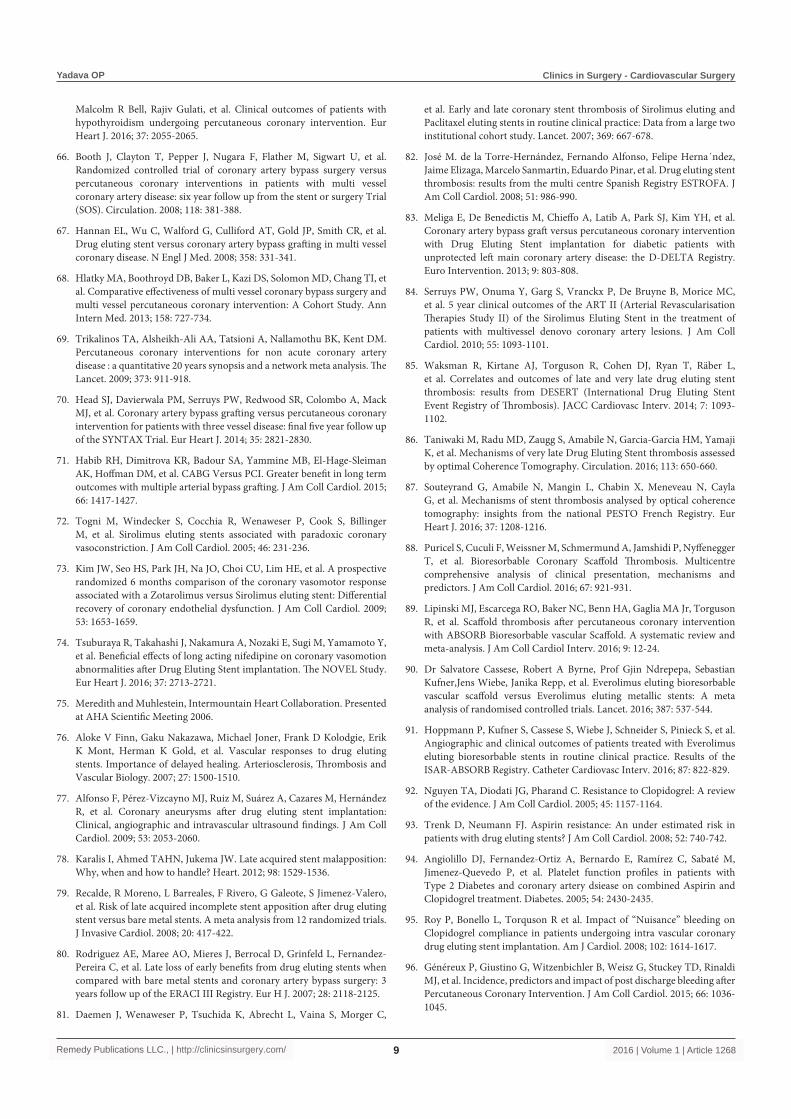
Figure 3: Turnbull cumulative patency rates according to type of bypass graft.

Yadava OP Clinics in Surgery - Cardiovascular Surgery
Remedy Publications LLC., | http://clinicsinsurgery.com/ 2016 | Volume 1 | Article 12686
and instrumentation. OPCAB avoids the damaging effects of cardiopulmonary bypass, thereby providing better LV protection, reduced hospital stay, reduced morbidity and mortality Ref. (Figure 2), especially in high risk patients [130] with overall reduction in the cost of surgery. OPCAB has been validated even by angiography, both early [131] and at long term, [132] though there are some concerns raised by western literature, they seem to be nullified by Lamy et al. [133] Time is not far when these procedures will be offered as day case procedures especially when totally Endoscopic & Robotically controlled CABG become a ubiquitous reality.
Pedicled LIMA - LAD graft is the gold standard with patency rates upwards of 90% at 20 years [134] and patency of RIMA, Radial Artery (RA) and Right Gastro-Epiploeic Artery (RGEA) [135] is excellent at mid to long term. Angiographic patency estimates at 5 years were 95.9% for LIMA, 91.2% for RIMA, 90.6% for RA and 81.8% for Saphenous Vein [136] Ref. (Figure 3). Comparable patencies and clinical outcomes at 5 years using alternative conduits have been validated even in the RAPCOS Trial [137].
In a meta analysis [138] looking at CABG Vs PCI for multi vessel disease, the MACE for PCI was 42.8% as against 20.8% for CABG at 5 years and repeat revascularization was 30% with PCI Vs 7.4% with CABG. Similar results have been published by Daemen et al. [139], Takagi et al. [140], Park et al. [141] and Bangalore et al. [142]. In the ACUITY Trial [143] PCI decreased bleeding, blood transfusion & acute kidney injury but at cost of increased repeat revascularisation (19.5 versus 5.2%); mortality, MI and CVA remaining neutral. However in a meta-analysis of SYNTAX and BEST Trials, Chang et al. [144] found CABG superior for mortality (HR 0.65; p-0.039); MI (HR 0.40; p< 0.001) and repeat revascularisation (HR 0.55; p< 0.001) and neutral for CVA (HR 1.1; p-0.714).
Total arterial revascularization (TAR) provides survival benefits unmatched by PTCA. Eight year event free survival rate was 80.2+7.3% in the experience of Angela et al. [145] and actuarial freedom from cardiac death (including hospital death) was 97.6% at 9 years with TAR [146]. Similar long term survival is a rule rather than exception with TAR. Bergsma [147] reported 7 years survival of 91%, Nishida [148] described a 7 year survival of 88% and Tavilla [149] reported a 10 year survival of 87%. Locker et al. [150] from Mayo Clinic demonstrated 8 years survival benefit for multi arterial CABG over PCI with DES (87% versus 70%; p< 0.001).
Minimally Invasive CABG is establishing itself lately and provides invasiveness equivalent to PCI with improved outcomes. Holzhey et al. [151] in a large series reported an early operative mortality of 0.8%; peri-operative CVA 0.4% & early graft patency of 95.5%. Complete revascularisation was achieved in 95% patients [152]. MIDCAB too has been validated against PCI for LAD stenosis [153,154].
Also the oft heard premise that let us try PCI first and if it fails, CABG can always be offered, is not valid. PCI is not entirely benign and infact increases mortality and peri-operative complications 4during subsequent CABG [155].
Heart Team ConceptThough mandated as a Cl I (c) indication by all guidelines, it
is not implemented in true spirit for various reasons both ethical & unethical. As a consequence over 70% patients are both ill & misinformed into believing that PCI will prevent MI and increase survival [156] and barely 1% correctly understood the benefit of
PCI and as a consequence nearly one thirds of patients with Class I indications for CABG are subjected to PCI [156]. Patient awareness, self regulation by physicians and strict legislation may help correct this anomaly but real disruptive game changer will be when the gate keeper role moves from a cardiologist to an imaging specialist, so that unbiased decisions are taken by a neutral authority.
ConclusionBoth PTCA and CABG have improved over the last ten years. The
restenosis with DES has come down dramatically compared to BMS but is still in the range of 5-10% at 3 months and though the safety of DES has been proven, but the recurrence of angina and repeat revascularisation are still much higher than CABG. Besides that DES are costly, but to their advantage, they are patient and user friendly with early return to work and no cosmetic stigma attached. Similarly CABG too has improved and with off pump techniques, the mortality has come down to below 1% and the stroke rates too are falling to around 1%. The long term results of CABG are superior and it is cost effective, more so in scenarios of diabetes mellitus, multi vessel disease, chronic total occlusions and diffuse atherosclerosis. Therefore it is important that we combine the two technologies for the benefit of our patients and customize the treatment according to their needs. Whenever we have a simple coronary anatomy, be it single or double or triple vessel disease with a low SYNTAX score (<22 for multi vessel disease and <33 for left main disease), then angioplasty may still be considered for a patient, but if the anatomy is complex, then there is no question, CABG is the preferred choice. Both procedures are there to stay and will give good results if use for appropriate indications. Infact hybrid revascularization using Pedicled LIMA – LAD and stenting to the back of the heart arteries performed in composite operation suites may soon become the norm of the day. By the same token, one must not forget that both these procedures are palliative in nature and are likely to become obsolete at some stage, that is when either genetics takes over or some causative agent for CAD can be identified and curative pharmaco-therapeutic agent found for the same. Till such time, both will continue to exist and both will be required in a complementary fashion.
References1. Gruntzig A. Transluminal dilation of coronary artery stenosis. Lancet.
1978; 1: 263.
2. Favaloro RG. Saphenous vein autograft replacement of severe segmental coronary artery occlusion: operative technique. Ann Thorac Surg. 1968; 5: 334-339.
3. Yadava OP, Kundu A. 'On' or 'Off' pump coronary artery bypass grafting. Is the last word out? Ind Heart J. 2013; 65: 187-190.
4. Wasilewski J, Niedziela J, Osadnik T, Duszańska A, Sraga W, Desperak P, et al. Predominant location of coronary artery atherosclerosis in the Left Anterior Descending Artery. The impact of septal perforators and the myocardial bridging effect. Kardiochir Torakochirugia Pol. 2015; 12: 379-385.
5. Leon MB, Allocco DJ, Dawkins KD, Baim DS. Late clinical events after drug eluting stents: the interplay between stent related and natural history driven events. JACC Cardiovasc Interv. 2009; 2: 504-512.
6. Hannan EL, Zhong Y, Jacobs AK, Stamato NJ, Berger PB, Walford G, et al. Patients with chronic total occlusion undergoing percutaneous coronary interventions: Characteristics, success and outcomes. Circ Cardiovasc Interv. 2016: 9: e003586.
7. Serruys PW, Morice MC, Kappetein AP, Colombo A, Holmes DR, Mack

Yadava OP Clinics in Surgery - Cardiovascular Surgery
Remedy Publications LLC., | http://clinicsinsurgery.com/ 2016 | Volume 1 | Article 12687
MJ, et al. Percutaneous Coronary Intervention versus Coronary Artery Bypass Grafting for severe Coronary Artery Disease. New Engl J Med. 2009; 360: 961-972.
8. Jeffrey J Popma, Martin B Leon, Jeffrey W Moses, David R Holmes, Nicholas Cox, Michelle Fitzpatrick, et al. SIRIUS Investigators. Quantitative assessment of angiographic restenosis after Sirolimus Eluting Stent implantation in native coronary arteries. Circulation. 2004; 110: 3773-3780.
9. Gregg W Stone, Stephen G Ellis, David A Cox, James Hermiller, Charles O'Shaughnessy, James Tift Mann, et al. TAXUS IV Investigators. A polymer based, paclitaxel eluting stent in patients with coronary artery disease. N Engl J Med. 2004; 350: 221-231.
10. Leon MB, Mauri L, Popma JJ, Cutlip DE, Nikolsky E, O'Shaughnessy C, et al. ENDEAVOR IV Investigators. A randomized comparison of the endeavor zotarolimus eluting stent versus the TAXUS Paclitaxel eluting stent in denovo coronary lesions 12 month outcomes from the ENDEAVOR IV Trial. J Am Coll Cardiol. 2010; 55: 543-554.
11. Stone GW, Midei M, Newman W, Sanz M, Hermiller JB, Williams J, et al. Spirit III Investigators. Comparison of an everolimus eluting stent and a paclitaxel eluting stent in patients with coronary artery disease: a randomized trial. JAMA. 2008; 299: 1903-1913.
12. Stone GW, Midei M, Newman W, Sanz M, Hermiller JB, Williams J, et al. Spirit III Investigators. Randomized comparison of everolimus eluting and paclitaxel eluting stents. Two year clinical follow up from the Clinical Evaluation of the Xience V Everolimus eluting coronary stent system in the treatment of patients with denovo native coronary artery lesions (SPIRIT) III Trial. Circulation. 2009; 119: 680-686.
13. Gershlick A, Kandzari DE, Leon MB, Wijns W, Meredith IT, Fajadet J, et al. Zotarolimus eluting stents in patients with native coronary artery disease: Clinical and angiographic outcomes in 1,317 patients. Am J Cardiol. 2007; 100: 45M-55M.
14. Kandzari DE, Rao SV, Moses JW, Dzavik V, Strauss BH, Kutryk MJ, et al. ACROSS/TOSCA – 4 Investigators. Clinical and angiographic outcomes with Sirolimus eluting stents in total coronary occlusions: the ACROSS/TOSCA-4 (Approaches to chronic occlusions with Sirolimus eluting stents/Total Occlusion Study of Coronary Arteries – 4) Trial. JACC Cardiovasc Interv. 2009; 2: 97-106.
15. Khan MF, Brilakis ES, Wendel CS, Thai H. Comparison of procedural complications and in-hospital clinical outcomes between patients with successful and failed percutaneous intervention of coronary chronic total occlusions: A meta-analysis of observational studies. Cath Cardiovasc Interv. 2015; 85: 781-794.
16. Ormiston JA, Serruys PW, Regar E, Dudek D, Thuesen L, Webster MW, et al. A bioabsorbable everolimus eluting coronary stent system for patients with single denovo coronary artery lesions (ABSORB): a prospective open label trial. Lancet. 2008; 371: 899-907.
17. Erbel R, Di Mario C, Bartunek J, Bonnier J, de Bruyne B, Eberli FR, et al. PROGRESS AMS (Clinical Performance and Angiographic Results of Coronary Stenting with Absorbable Metal Stents) Investigators. Temporary scaffolding of coronary arteries with bioabsorbable magnesium stents: a prospective, non randomized multi centre trial. Lancet. 2007; 369: 1869-1875.
18. Mig Lionico M, Patti G, D’Ambrosio A, Di Sciascio G. Percutaneous coronary intervention utilizing a new endothelial progenitor cells antibody coated stent: a prospective single centre registry in high risk patients. Cath Cardiovasc Interv. 2008; 71: 600-604.
19. Byrne RA, Kastrati A, Kufner S, Massberg S, Birkmeier KA, Laugwitz KL, et al. Intracoronary stenting and angiographic results: Test efficacy of 3 Limus Eluting Stents (ISAR-TEST 4) Trial. Eur H J. 2009; 30: 2441-2449.
20. Hamm et al - for PEPCAD 3 Investigators. Drug eluting balloons versus Stents. Presented at the AHA Annual Scientific meeting Nov. 2009.
21. Raungaard B, Jensen LO, Tilsted HH, Christiansen EH, Maeng M, Terkelsen CJ, et al. Zotarilimus - Eluting durable-polymer coated stent versus a Biolimus-eluting biodegradable polymer coated stent in unselected patients undergoing percutaneous coronary intervention (SORT OUT VI): a randomised non-inferiority trial. Lancet. 2015; 385: 1527-1535.
22. Kimura T, Kozuma K, Tanabe K, Nakamura S, Yamane M, Muramatsu T, et al. A randomized trial evaluating everolimus-eluting Absorb bio-resorbable scaffolds versus everolimus-eluting metallic stents in patients with coronary artery disease: ABSORB Japan. Eur Heart J. 2015; 36: 3332-3342.
23. Ellis SG, Kereiakes DJ, Metzger DC, Caputo RP, Rizik DG, Teirstein PS, et al. Everolimus-Eluting Bioresorbable scaffolds for coronary artery disease. N Engl J Med. 2015; 373: 1905-1915.
24. Marco A Magalhaes, Sa'ar Minha, Fang Chen, Rebecca Torguson, A Fazir Omar, Joshua P Loh, Ricardo O Escarcega, et al. Clinical presentation and outcomes of coronary in-stent restenosis across 3 stent generations. Circ Cardiovasc Interv. 2014; 7: 768-776.
25. Byrne RA, Raisuke LR, Mehilli J et al. Durability of anti restenotic efficacy in drug eluting stents with and without permanent polymer. JACC Cardiovasc Interv. 2009; 2: 291-299.
26. Claessen BE, Beijk MA, Legrand V, Ruzyllo W, Manari A, Varenne O, et al. Two year clinical, angiographic and intravascular ultrasound follow up of the XIENCE V everolimus eluting stent in the treatment of patients with denovo native coronary artery lesions: the SPIRIT II Trial. Circl Cardiovascular Interv. 2009; 2: 339-347.
27. Zhang YJ, Iqbal J, Nakatani S, Bourantas CV, Campos CM, Ishibashi Y, et al. Sccaffold and edge vascular response following implantation of everolimus eluting bioresorbable vascular scaffold: a 3 year serial optical coherence tomography study. J Am Coll Cardiol Interv. 2014; 7: 1361-1369.
28. Cassese S, Hoppmann P, Kufner S, Byrne RA, Wiebe J, Colleran R, et al. Intra individual comparison of Everolimus-eluting Bioresorbable vascular scaffolds versus Drug eluting metallic stents.Circ Cardiovasc Interv. 2016; 9: e003698.
29. Mc Neely C, Markwell S, Vassileva C. Readmission after inpatient percutaneous coronary interventions in the Medicare population from 2000 to 2012. Am Heart J. 2016; 179: 195-203.
30. Serruys PW, Chevalier B, Sotomi Y, Cequier A, Carrié D, Piek JJ, et al. Comparison of an everolimus-eluting bioresorbable scaffold with an everolimus-eluting metallic stent for the treatment of coronary artery stenosis (ABSORB II): a 3 year, randomized controlled single-blind, multi center trial. Lancet. 2016; 388: 2479-2491.
31. Tamburino C, Angiolillo DJ, Capranzano P, Dimopoulos K, La Manna A, Barbagallo R, et al. Complete versus incomplete revascularization in patients with multi vessel disease undergoing percutaneous coronary interventions with drug eluting stent. Cather Cardiovasc Interv. 2008; 72: 448-456.
32. Garcia S, Sandoval Y, Roukoz H, Adabag S, Canoniero M, Yannopoulos D, et al. Outcomes after complete versus incomplete revascularisation in patients with multi vessel coronary artery disease: A meta analysis of 89,833 patients - enrolled in randomised clinical trials and observational studies. J Am Coll Cardiol. 2013; 62: 1421-1431.
33. Serruys PW, Morice MC, Kappetein AP, Colombo A, Holmes DR, Mack MJ, et al. SYNTAX Investigators. Percutaneous coronary interventions versus coronary artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009; 360: 961-972.
34. Généreux P, Palmerini T, Caixeta A, Rosner G, Green P, Dressler O, et al. Quantification and impact of untreated coronary artery disease after percutaneous coronary intervention. The residual SYNTAX (Synergy between PCI with Taxus and Cardiac Surgery) Score. J Am Coll Cardiol. 2012; 59: 2165-2174.

Yadava OP Clinics in Surgery - Cardiovascular Surgery
Remedy Publications LLC., | http://clinicsinsurgery.com/ 2016 | Volume 1 | Article 12688
35. Curtis JP, Schreiner G, Wang Y, Chen J, Spertus JA, Rumsfeld JS, et al. All cause readmission and repeat revascularization after percutaneous coronary interventions in a cohort of medicare patients. J Am Coll Cardiol. 2009; 54: 903-907.
36. Steffenino G, LaScala E, Riva L, Minardi E. Coronary angioplasty in diabetic patients. Ital H J Suppl. 2002; 3: 9-15.
37. The BARI Investigators seven year outcome in the Bypass Angioplasty Revascularization Investigation (BARI) by treatment and diabetic status. J Am Coll Cardiol. 2000; 35: 1122-1129.
38. Abizaid A, Costa MA, Centemero M, Abizaid AS, Legrand VM, Limet RV, et al. Clinical and economic impact of diabetes mellitus on percutaneous and surgical treatment of multi vessel coronary disease patients: Insight from the Arterial Revascularization Therapy Study (ARTS) Trial. Circulation. 2001; 104: 533-538.
39. Niles NW, McGrath PD, Malenka D, Quinton H, Wennberg D, Shubrooks SJ, et al. for the Northern New England Cardiovascular Disease Study Group. Survival of patients with diabetes and multi vessel coronary artery disease after surgical or percutaneous coronary revascularization: results of a large regional prospective study. J Am Coll Cardiol. 2001; 37: 1008-1015.
40. Kamalesh M, Sharp TG, Tang XC, Shunk K, Ward HB, Walsh J, et al. Percutaneous Coronary Intervention versus Coronary Bypass Surgery in United States veterans with diabetes. J Am Coll Cardiol. 2013; 61: 808-816.
41. Kapur A, Hall RJ, Malik IS, Qureshi AC, Butts J, de Belder M, et al. Randomised comparison of percutaneous coronary intervention with coronary artery bypass grafting in diabetic patients: 1 year results of the CARDIA (Coronary Artery Revascularisation in Diabetes) Trial. J Am Coll Cardiol. 2010; 55: 432-440.
42. Weintraub WS, Grau-Sepulveda MV, Weiss JM, O'Brien SM, Peterson ED, Kolm P, et al. Comparative effectiveness of revascularisation strategies. N Engl J Med. 2012; 366: 1467-1476.
43. Farkouh M, Domanski M, Fuster V. Revascularisation strategies in patients with diabetes. N Engl J Med. 2013; 368: 1455-1456.
44. Dibra A, Kastrati A, Mehilli J, Pache J, Schühlen H, von Beckerath N, et al. Paclitaxel eluting or Sirolimus eluting stents to prevent restenosis in diabetic patients (ISAR DIABETES Study). New Engl J Med. 2005; 353: 663-670.
45. Sabaté M, Jiménez-Quevedo P, Angiolillo DJ, Gómez-Hospital JA, Alfonso F, Hernández-Antolín R, et al. for the DIABETES Investigators. Randomized comparison of Sirolimus eluting stent versus standard stent for percutaneous coronary revascularization in diabetic patients. (DIABETES Trial). Circulation. 2005; 112: 2175-2183.
46. Bangalore S, Bhagwat A, Pinto B, Goel PK, Jagtap P, Sathe S, et al. Percutaneous coronary intervention in patients with Insulin treated and non insulin treated diabetes mellitus. Secondary analysis of the TUXEDO Trial. JAMA Cardiol. 2016; 1: 266-273.
47. Mehilli J, Kastrati A, Schuhlen H et al - ISAR SWEET Study Investigators. Randomized clinical trial of Abciximab in diabetic patients undergoing elective percutaneous coronary intervention after treatment with a high loading dose of Clopidogrel. Circulation. 2004; 110: 3627-3635.
48. Ritsinger V, Saleh N, Lagerqvist B, Norhammar A. High event rates after a first percutaneous coronary intervention in patients with diabetes mellitus. Results from the Swedish Coronary Angiography and Angioplasty Registry. Circ Cardiovasc Interv. 2015; 8.
49. Dangas GD, Farkouh ME, Sleeper LA, Yang M, Schoos MM, Macaya C, et al. Long term outcome of PCI versus CABG in insulin and non insulin treated diabetic patients. Results from the FREEDOM Trial. J Am Coll Cardiol. 2014; 64: 1189-1197.
50. Frye RL, August P, Brooks MM, Hardison RM, Kelsey SF, MacGregor JM
et al. A randomized trial of therapies for Type 2 Diabetes and coronary artery disease. The BARI 2D Study Group. N Engl J Med. 2009; 360: 2503-2515.
51. Kapur A, Hall RJ, Malik IS, Qureshi AC, Butts J, de Belder M, et al. Randomized comparison of percutaneous coronary intervention with coronary artery bypass grafting in diabetic patients. 1 year results of the CARDia (Coronary Artery Revascularization in Diabetes) Trial. J Am Coll Cardiol. 2010; 55: 432-440.
52. Banning AP, Westaby S, Morice MC, Kappetein AP, Mohr FW, Berti S, et al. Diabetic and non diabetic patients with left main and/or 3 vessel coronary artery disease: Comparison of outcomes with cardiac surgery and Paclitaxel eluting stents. J Am Coll Cardiol. 2010; 55: 1067-1075.
53. Tu B, Rich B, Labos C, Brophy JM. Coronary Revascularisation in diabetic patients: A systematic review and Bayesian Network Meta-analysis. Ann Intern Med. 2014; 161: 724-732.
54. Farkouh ME, Domanski M, Sleeper LA, Siami FS, Dangas G, Mack M, et al. Strategies for multivessel revascularisation in patients with diabetes. New Engl J Med. 2012; 367: 2375-2384.
55. Mancini GB, Farkouh ME, Brooks MM, Chaitman BR, Boden WE, Vlachos H, et al. Medical treatment and Revascularization options in patients with type 2 Diabetes and coronary disease. J Am Coll Cardiol. 2016; 68: 985-995.
56. De Luca G, Schaffer A, Verdoia M, Suryapranata H. Meta analysis of 14 trials comparing bypass grafting versus drug eluting stents in diabetic patients with multivessel coronary artery disease. Nutr Metab Cardiovasc Dis. 2014; 24: 344-354.
57. Deb S, Wijeysundera HC, Ko DT, Tsubota H, Hill S, Fremes SE. Coronary artery bypass graft surgery Versus percutaneous interventions in coronary revascularization. A systematic review. JAMA. 2013; 310: 2086-2095.
58. Fröbert O, Lagerqvist B, Carlsson J, Lindbäck J, Stenestrand U, James SK. Differences in restenosis rate with different drug eluting stents in patients with and without diabetes mellitus: A report frm the SCAAR (Swedish Angiography and Angioplasty Registry) J Am Coll Cardiol. 2009; 53: 1660-1667.
59. Clinical evaluation of the Xience V Everolimus eluting coronary stent system in the treatment of patients with denovo native coronary artery lesions IV (SPIRIT IV) Presented at Transcatheter Cardiovascualr Therapeutics meeting (TCT 2009), San Francisco CA, Sept 23, 2009.
60. Kirtane AJ, Patel R, O'Shaughnessy C, Overlie P, McLaurin B, Solomon S, et al. Clinical and angiographic outcomes in diabetics from the ENDEAVOR IV Trial: randomized comparison of Zotarolimus and Paclitaxel eluting stents in patients with coronary artery disease. JACC Cardiovasc Interv. 2009; 2: 967-976.
61. Kedhi E, Joesoef KS, McFadden E, Wassing J, van Mieghem C, Goedhart D, et al. Second generation everolimus eluting and paclitaxel eluting stents in real life practice (COMPARE): a randomized trial. Lancet. 2010; 375: 201-209.
62. Boden WE, Taggart DP. Diabetes with coronary disease–A moving target amid evolving therapies? Editorial N Engl J Med. 2009; 360: 2570-2572.
63. Baber U, Farkouh ME, Arbel Y, Muntner P, Dangas G, Mack MJ, et al. Comparative efficacy of coronary artery bypass surgery versus percutaneous coronary intervention in patients with diabetes and multi-vessel coronary artery disease with or without chronic kidney disease. Eur Heart J. 2016.
64. Mamas MA, Anderson SG, O'Kane PD, Keavney B, Nolan J, Oldroyd KG, et al. Impact of left ventricular function in relation to procedural outcomes following percutaneous coronary intervention: insights from the British Cardiovascular Intervention Society. Eur Heart J. 2014; 35: 3004-3012a.
65. Ming Zhang, Jaskanwal D S Sara, Yasushi Matsuzawa, Hossein Gharib,
Yadava OP Clinics in Surgery - Cardiovascular Surgery
Remedy Publications LLC., | http://clinicsinsurgery.com/ 2016 | Volume 1 | Article 12689
Malcolm R Bell, Rajiv Gulati, et al. Clinical outcomes of patients with hypothyroidism undergoing percutaneous coronary intervention. Eur Heart J. 2016; 37: 2055-2065.
66. Booth J, Clayton T, Pepper J, Nugara F, Flather M, Sigwart U, et al. Randomized controlled trial of coronary artery bypass surgery versus percutaneous coronary interventions in patients with multi vessel coronary artery disease: six year follow up from the stent or surgery Trial (SOS). Circulation. 2008; 118: 381-388.
67. Hannan EL, Wu C, Walford G, Culliford AT, Gold JP, Smith CR, et al. Drug eluting stent versus coronary artery bypass grafting in multi vessel coronary disease. N Engl J Med. 2008; 358: 331-341.
68. Hlatky MA, Boothroyd DB, Baker L, Kazi DS, Solomon MD, Chang TI, et al. Comparative effectiveness of multi vessel coronary bypass surgery and multi vessel percutaneous coronary intervention: A Cohort Study. Ann Intern Med. 2013; 158: 727-734.
69. Trikalinos TA, Alsheikh-Ali AA, Tatsioni A, Nallamothu BK, Kent DM. Percutaneous coronary interventions for non acute coronary artery disease : a quantitative 20 years synopsis and a network meta analysis. The Lancet. 2009; 373: 911-918.
70. Head SJ, Davierwala PM, Serruys PW, Redwood SR, Colombo A, Mack MJ, et al. Coronary artery bypass grafting versus percutaneous coronary intervention for patients with three vessel disease: final five year follow up of the SYNTAX Trial. Eur Heart J. 2014; 35: 2821-2830.
71. Habib RH, Dimitrova KR, Badour SA, Yammine MB, El-Hage-Sleiman AK, Hoffman DM, et al. CABG Versus PCI. Greater benefit in long term outcomes with multiple arterial bypass grafting. J Am Coll Cardiol. 2015; 66: 1417-1427.
72. Togni M, Windecker S, Cocchia R, Wenaweser P, Cook S, Billinger M, et al. Sirolimus eluting stents associated with paradoxic coronary vasoconstriction. J Am Coll Cardiol. 2005; 46: 231-236.
73. Kim JW, Seo HS, Park JH, Na JO, Choi CU, Lim HE, et al. A prospective randomized 6 months comparison of the coronary vasomotor response associated with a Zotarolimus versus Sirolimus eluting stent: Differential recovery of coronary endothelial dysfunction. J Am Coll Cardiol. 2009; 53: 1653-1659.
74. Tsuburaya R, Takahashi J, Nakamura A, Nozaki E, Sugi M, Yamamoto Y, et al. Beneficial effects of long acting nifedipine on coronary vasomotion abnormalities after Drug Eluting Stent implantation. The NOVEL Study. Eur Heart J. 2016; 37: 2713-2721.
75. Meredith and Muhlestein, Intermountain Heart Collaboration. Presented at AHA Scientific Meeting 2006.
76. Aloke V Finn, Gaku Nakazawa, Michael Joner, Frank D Kolodgie, Erik K Mont, Herman K Gold, et al. Vascular responses to drug eluting stents. Importance of delayed healing. Arteriosclerosis, Thrombosis and Vascular Biology. 2007; 27: 1500-1510.
77. Alfonso F, Pérez-Vizcayno MJ, Ruiz M, Suárez A, Cazares M, Hernández R, et al. Coronary aneurysms after drug eluting stent implantation: Clinical, angiographic and intravascular ultrasound findings. J Am Coll Cardiol. 2009; 53: 2053-2060.
78. Karalis I, Ahmed TAHN, Jukema JW. Late acquired stent malapposition: Why, when and how to handle? Heart. 2012; 98: 1529-1536.
79. Recalde, R Moreno, L Barreales, F Rivero, G Galeote, S Jimenez-Valero, et al. Risk of late acquired incomplete stent apposition after drug eluting stent versus bare metal stents. A meta analysis from 12 randomized trials. J Invasive Cardiol. 2008; 20: 417-422.
80. Rodriguez AE, Maree AO, Mieres J, Berrocal D, Grinfeld L, Fernandez-Pereira C, et al. Late loss of early benefits from drug eluting stents when compared with bare metal stents and coronary artery bypass surgery: 3 years follow up of the ERACI III Registry. Eur H J. 2007; 28: 2118-2125.
81. Daemen J, Wenaweser P, Tsuchida K, Abrecht L, Vaina S, Morger C,
et al. Early and late coronary stent thrombosis of Sirolimus eluting and Paclitaxel eluting stents in routine clinical practice: Data from a large two institutional cohort study. Lancet. 2007; 369: 667-678.
82. José M. de la Torre-Hernández, Fernando Alfonso, Felipe Herna´ndez, Jaime Elizaga, Marcelo Sanmartin, Eduardo Pinar, et al. Drug eluting stent thrombosis: results from the multi centre Spanish Registry ESTROFA. J Am Coll Cardiol. 2008; 51: 986-990.
83. Meliga E, De Benedictis M, Chieffo A, Latib A, Park SJ, Kim YH, et al. Coronary artery bypass graft versus percutaneous coronary intervention with Drug Eluting Stent implantation for diabetic patients with unprotected left main coronary artery disease: the D-DELTA Registry. Euro Intervention. 2013; 9: 803-808.
84. Serruys PW, Onuma Y, Garg S, Vranckx P, De Bruyne B, Morice MC, et al. 5 year clinical outcomes of the ART II (Arterial Revascularisation Therapies Study II) of the Sirolimus Eluting Stent in the treatment of patients with multivessel denovo coronary artery lesions. J Am Coll Cardiol. 2010; 55: 1093-1101.
85. Waksman R, Kirtane AJ, Torguson R, Cohen DJ, Ryan T, Räber L, et al. Correlates and outcomes of late and very late drug eluting stent thrombosis: results from DESERT (International Drug Eluting Stent Event Registry of Thrombosis). JACC Cardiovasc Interv. 2014; 7: 1093-1102.
86. Taniwaki M, Radu MD, Zaugg S, Amabile N, Garcia-Garcia HM, Yamaji K, et al. Mechanisms of very late Drug Eluting Stent thrombosis assessed by optimal Coherence Tomography. Circulation. 2016; 113: 650-660.
87. Souteyrand G, Amabile N, Mangin L, Chabin X, Meneveau N, Cayla G, et al. Mechanisms of stent thrombosis analysed by optical coherence tomography: insights from the national PESTO French Registry. Eur Heart J. 2016; 37: 1208-1216.
88. Puricel S, Cuculi F, Weissner M, Schmermund A, Jamshidi P, Nyffenegger T, et al. Bioresorbable Coronary Scaffold Thrombosis. Multicentre comprehensive analysis of clinical presentation, mechanisms and predictors. J Am Coll Cardiol. 2016; 67: 921-931.
89. Lipinski MJ, Escarcega RO, Baker NC, Benn HA, Gaglia MA Jr, Torguson R, et al. Scaffold thrombosis after percutaneous coronary intervention with ABSORB Bioresorbable vascular Scaffold. A systematic review and meta-analysis. J Am Coll Cardiol Interv. 2016; 9: 12-24.
90. Dr Salvatore Cassese, Robert A Byrne, Prof Gjin Ndrepepa, Sebastian Kufner,Jens Wiebe, Janika Repp, et al. Everolimus eluting bioresorbable vascular scaffold versus Everolimus eluting metallic stents: A meta analysis of randomised controlled trials. Lancet. 2016; 387: 537-544.
91. Hoppmann P, Kufner S, Cassese S, Wiebe J, Schneider S, Pinieck S, et al. Angiographic and clinical outcomes of patients treated with Everolimus eluting bioresorbable stents in routine clinical practice. Results of the ISAR-ABSORB Registry. Catheter Cardiovasc Interv. 2016; 87: 822-829.
92. Nguyen TA, Diodati JG, Pharand C. Resistance to Clopidogrel: A review of the evidence. J Am Coll Cardiol. 2005; 45: 1157-1164.
93. Trenk D, Neumann FJ. Aspirin resistance: An under estimated risk in patients with drug eluting stents? J Am Coll Cardiol. 2008; 52: 740-742.
94. Angiolillo DJ, Fernandez-Ortiz A, Bernardo E, Ramírez C, Sabaté M, Jimenez-Quevedo P, et al. Platelet function profiles in patients with Type 2 Diabetes and coronary artery dsiease on combined Aspirin and Clopidogrel treatment. Diabetes. 2005; 54: 2430-2435.
95. Roy P, Bonello L, Torquson R et al. Impact of “Nuisance” bleeding on Clopidogrel compliance in patients undergoing intra vascular coronary drug eluting stent implantation. Am J Cardiol. 2008; 102: 1614-1617.
96. Généreux P, Giustino G, Witzenbichler B, Weisz G, Stuckey TD, Rinaldi MJ, et al. Incidence, predictors and impact of post discharge bleeding after Percutaneous Coronary Intervention. J Am Coll Cardiol. 2015; 66: 1036-1045.
Yadava OP Clinics in Surgery - Cardiovascular Surgery
Remedy Publications LLC., | http://clinicsinsurgery.com/ 2016 | Volume 1 | Article 126810
97. Meier P, Zbinden R, Togni M, Wenaweser P, Windecker S, Meier B, et al. Coronary collateral function after drug eluting stent implantation. J Am Coll Cardiol. 2007; 49: 15-20.
98. Pfisterer M, Brunner-La Rocca HP, Rickenbacher P, Hunziker P, Mueller C, Nietlispach F, et al. Long term benefit risk balance of drug eluting versus bare metal stents in daily practice. Does stent diameter matter? Three year follow up of BASKET. Eur H J. 2009; 30: 16-24.
99. Lee SY, Hur SH, Lee SG, Kim SW, Shin DH, Kim JS, et al. Optical coherence tomographic observation of Instent neoatherosclerosis in lesions with more than 50% neointimal area stenosis after second generation drug eluting stent implantation. Circ Cardiovasc Interv. 2015; 8: e001878.
100. Shand JA, Ramsewak A, Hanratty CG, et al. The 'Concertina effect' and the limitations of current Drug Eluting Stent: is it time to revisit and prioritize stent design over efficacy? Interv Cardiol. 2012; 4: 325-335.
101. Memon S, Chhabra L, Masrur S, Parker MW. Allergic acute coronary syndrome (Kounis Syndrome) Proc (Bayl Univ Med Cent). 2015; 28: 358-362.
102. Soeda T, Uemura S, Park SJ, Jang Y, Lee S, Cho JM, et al. Incidence and clinical significance of Post-Stent OCT Findings: One year follow up study from a multicenter registry. Circulation. 2015; 132: 1020-1029.
103. Kan J, Ge Z, Zhang JJ, Liu ZZ, Tian NL, Ye F, et al. Incidence and clinical outcomes of stent fractures on the basis of 6,555 patients and 16,482 Drug Eluting Stents from 4 centers. J Am Coll Cardiol Interv. 2016; 9: 1115-1123.
104. Suwannasom P, Sotomi Y, Ishibashi Y, Cavalcante R, Albuquerque FN, Macaya C, et al. The impact of post procedural asymmetry, expansion and eccentricity of bioresorbable Everolimus Eluting Scaffold and metallic Everolimus eluting stent on clinical outcomes in the ABSORB II Trial. JACC Cardiovasc Interv. 2016; 9: 1231-1242.
105. Gori T, Jansen T, Weissner M, Foin N, Wenzel P, Schulz E, et al. Coronary evaginations and peri-scaffold aneurysms following implantation of bioresorbable scaffolds: Incidence, outcome and optical coherence tomography analysis of possible mehcanisms. Eur Heart J. 2016; 37: 2040-2049.
106. Griffin SC, Barber JA, Manca A, Sculpher MJ, Thompson SG, Buxton MJ, et al. Cost effectiveness of clinically appropriate decisions on alternative treatments for angina pectoris: prospective observational study. BMJ. 2007; 334: 624-628.
107. Bach RG. PCI was not as effective as CABG for severe coronary artery disease at 5 years. Ann Intern Med. 2013; 159: JC4-JC5.
108. Aziz O, Rao C, Panesar SS, Jones C, Morris S, Darzi A, et al. Meta analysis of minimally invasive internal thoracic artery bypass versus percutaneous revascularization for isolated lesions of the left anterior descending artery. BMJ. 2007; 334: 617-620.
109. Rao C, Aziz O, Panesar SS, Jones C, Morris S, Darzi A, et al. Cost effectiveness analysis of minimally invasive internal thoracic artery bypass versus percutaneous revascularization for isolated lesions of the left anterior descending artery. BMJ. 2007; 334: 621-623.
110. Cohen DJ, Lavelle TA, Serruys FW, Li H, Lei Y, Wang K, et al. Health related quality life and US economic outcomes of PCI with drug eluting stent versus bypass surgery: 1 year results from the SYNTAX Trial. Presented at ACC Annual Meeting, March, 2009.
111. Abdallah MS, Wang K, Magnuson EA, Spertus JA, Farkouh ME, Fuster V, et al. Quality of life after PCI Vs CABG among patients with diabetes and multi vessel Coronary Artery Disease. A Randomized Clinical Trial. JAMA. 2013; 310: 1581-1590.
112. Philpott AC, Southern DA, Clement FM, Galbraith PD, Traboulsi M, Knudtson ML, et al. for the APPROACH Investigators. Long term outcomes of patients receiving drug eluting stents. Can Med Assn J. 2009; 180: 167-174.
113. Weintraub WS, Spertus JA, Kolm P, Maron DJ, Zhang Z, Jurkovitz C, et al. Effect of PCI on quality of life in patients with stable coronary disease. N Engl J Med. 2008; 359: 677-687.
114. Buszman PE, Buszman PP, Kiesz RS, Bochenek A, Trela B, Konkolewska M, et al. Early and long term results of unprotected left main coronary artery stenting. The LE MANS (Left Main Coronary Artery Stenting) Registry. J Am Coll Cardiol. 2009; 54: 1500-1511.
115. Valgimigli M, Malagutti P, Rodriguez-Granillo GA, Garcia-Garcia HM, Polad J, Tsuchida K, et al. Distal left main coronary disease is a major predictor of outcome in patients undergoing percutaneous interventions in the drug eluting stent era: An integrated clinical and angiographic analysis based on the Rapamycin eluting stent evaluated at Rotterdam Cardiology Hospital (RESEARCH) and Taxus stent evaluated at Rotterdam Cardiology Hospital (T-SEARCH) registries. J Am Coll Cardiol. 2006; 47: 1530-1537.
116. Morice MC, Serruys PW, Kappetein AP, Feldman TE, Ståhle E, Colombo A, et al. Five year outcomes in patients with left main disease treated with either Percutaneous Coronary Intervention or Coronary Artery Bypass Grafting in the synergy between Percutaneous Coronary Intervention with TAXUS and Cardiac Surgery Trial. Circulation. 2014; 129: 2388-2394.
117. Zheng Z, Xu B, Zhang H, Guan C, Xian Y, Zhao Y, et al. Coronary artery bypass graft surgery versus percutaneous coronary intervention in patients with unprotected left main coronary artery disease. J Am Coll Cardiol Interv. 2016; 9: 1102-1111.
118. Kang SJ, Mintz GS, Kim WJ, Lee JY, Oh JH, Park DW, et al. Changes in left main bifurcation geometery after a single stent cross over technique: an intravascular ultrasound study using direct imaging of both the LAD and the Left Circumflex Coronary Artery before & after intervention. Circ Cardiovasc Interv. 2011; 4: 355-361.
119. Girasis C, Farooq V, Diletti R, Muramatsu T, Bourantas CV, Onuma Y, et al. Impact of 3 dimensional bifurcation angle on 5 year outcome of patients after percutaneous coronary intervention for left main coronary artery disease. A substudy of the SYNTAX Trial. JACC Cardioasc Interv. 2013; 6: 1250-1260.
120. Seung KB, Park DW, Kim YH, Lee SW, Lee CW, Hong MK, et al. Stents versus coronary artery bypass grafting for left main coronary artery disease. N Engl J Med. 2008; 358: 1781-1792.
121. Ahn JM, Roh JH, Kim YH, Park DW, Yun SC, Lee PH, et al. Randomised trial of stents versus bypass surgery for Left Main Coronary Artery Disease: 5 year outcomes of the PRECOMBAT STUDY. J Am Coll Cardiol. 2015; 65: 2198-2206.
122. Shiomi H, Morimoto T, Furukawa Y, Nakagawa Y, Sakata R, Okabayashi H, et al. Comparison of percutaneous coronary intervention with coronary artery bypass grafting in unprotected left main coronary artery disease - 5 year outcome from CREDO-KYOTO PCI/CABG Registry Cohort 2. Circ J. 2015; 79: 1282-1289.
123. Stone GW, Sabik JF, Serruys PW, Simonton CA, Généreux P, Puskas J, et al. Everolimus Eluting stents or Bypass Surgery for Left Main Coronary Artery Disease. New Engl J Med. 2016; 375: 2223-2235.
124. Mäkikallio T, Holm NR, Lindsay M, Spence MS, Erglis A, Menown IB, et al. Percutaneous Coronary Angioplasty versus Coronary Artery Bypass grafting in treatment of unprotected left main stenosis (NOBLE): a prospective randomized, open-label, non inferiority trial. Lancet. 2016; 388: 2743-2752.
125. Cavalcante R, Sotomi Y, Lee CW, Ahn JM, Farooq V, Tateishi H, et al. Outcomes after percutaneous coronary intervention or coronary artery bypass surgery in patients with unprotected left main disease. J Am Coll Cardiol. 2016; 68: 999-1009.
126. Authors/Task Force members, Windecker S, Kolh P, Alfonso F, Collet JP, Cremer J, et al. 2014 ESC/EACTS Guidelines on myocardial revascularisation. Eur Heart J. 2014; 35: 2541-2619.
Yadava OP Clinics in Surgery - Cardiovascular Surgery
Remedy Publications LLC., | http://clinicsinsurgery.com/ 2016 | Volume 1 | Article 126811
127. Fihn SD, Blankenship JC, Alexander KP, Bittl JA, Byrne JG, Fletcher BJ et al. 2014 ACC/AHA/AATS/PCNA/SCAI/STS Focussed update of the guideline for the diagnosis and management of patients with stable ischaemic heart disease. J Am Coll Cardiol. 2014; 64: 1929-1949.
128. Møller CH, Perko MJ, Lund JT, Andersen LW, Kelbaek H, Madsen JK, et al. No major differences in 30 day outcomes in high risk patients randomized to off pump versus on pump coronary bypass surgery. The Best Bypass Surgery Trial. Circulation. 2010; 121: 498-504.
129. Kim KB, Kim JS, Kang HJ, Koo BK, Kim HS, Oh BH, et al. Ten year experience with off pump coronary artery bypass grafting: Lessons learned from early post operative angiography. J Thorac Cardiovasc Surg. 2010; 139: 256-262.
130. Angelini GD, Culliford L, Smith DK, Hamilton MC, Murphy GJ, Ascione R, et al. Effects of on and off pump coronary artery surgery on graft patency, survival and health related quality of life: Long term follow up of two randomized controlled trials. J Thorac Cardiovasc Surg. 2009; 137: 295-303.
131. André Lamy, P.J. Devereaux, Dorairaj Prabhakaran, David P.Taggart, Shengshou Hu, Zbynek Straka, et al. Five year outcomes after Off-Pump or On Pump coronary artery bypass grafting. New Engl J Med. 2016.
132. Cleveland Clinic data, 1972 to 1999. Quoted from Kirklin/Barratt-Boyes Cardiac Surgery Vol.1, 3rd Edn; Churchill Livingstone. 2003; 401.
133. Suma H. Gastro epiploeic artery graft in coronary artery bypass grafting. Ann Cardiothorac Surg. 2013; 2: 493-498.
134. Shah PJ, Bui K, Blackmore S, Gordon I, Hare DL, Fuller J, et al. Has the insitu right internal thoracic artery been overlooked ? An angiographic study of the radial artery, internal thoracic arteries and saphenous vein graft patencies in symptomatic patients. Eur J Cardiothorac Surg. 2005; 27: 870-875.
135. Hayward PA, Gordon IR, Hare DL, Matalanis G, Horrigan ML, Rosalion A, et al. Comparable patencies of the radial artery and right internal thoracic artery or saphenous vein beyond 5 years: results from the radial artery patency and clinical outcomes trial. J Thorac Cardiovasc Surg. 2010; 139: 60-67.
136. Athappan G, Vinodhkumaradithyaa A, Srinivasan M, Jeyaseelan L, Ponniah T. Meta analysis of 5 year outcomes of CABG Vs PCI with stenting in patients with multi vessel disease. Minerva Cardioangiol. 2008; 56: 453-460.
137. Daemen J, Boersma E, Flather M, Booth J, Stables R, Rodriguez A, et al. Long term safety and efficacy of percutaneous coronary intervention with stenting & coronary artery bypass surgery for multi vessel coronary artery disease : a meta analysis with five year patient level data from the ARTS, ERACI II, MASS II and SOS Trials. Circulation. 2008; 118: 1146-1154.
138. Takagi H, Kawai N, Umemoto T. Meta analysis of 4 randomized controlled trials on long term outcomes of coronary artery bypass grafting versus percutaneous coronary interventions with stenting for multi vessel coronary artery disease. Am J Cardiol. 2008; 101: 1259-1262.
139. Park SJ, Ahn JM, Kim YH, Park DW, Yun SC, Lee JY, et al. Trial of Everolimus Eluting Stents or Bypass Surgery for Coronary Artery Disease. New Engl J Med. 2015; 372: 1204-1212.
140. Bangalore S, Guo Y, Samadashvili Z, Blecker S, Xu J, Hannan EL. Everolimus eluting stent or Bypass Surgery for Multi vessel Coronary Artery Disease. N Engl J Med. 2015; 372: 1213-1222.
141. Ben-Gal Y, Mohr R, Feit F, Ohman EM, Kirtane A, Xu K, et al. Surgical versus percutaneous coronary revascularsisation for multivessel disease in diabetic patients with non ST-segment elevation acute coronary syndrome. Analysis from the Acute Catheterisation and Early Intervention Triage Strategy Trial.Circ Cardiovasc Interv. 2015; 8: e002032.
142. Chang M, Ahn JM, Lee CW, Cavalcante R, Sotomi Y, Onuma Y, et al. Long term mortality after coronary revascularisation in non diabetic
patients with multivessel disease. J Am Coll Cardiol. 2016; 68: 29-36.
143. Iacò AL, Teodori G, Di Giammarco G, Di Mauro M, Storto L, Mazzei V, et al. Radial artery for myocardial revascularisation: Long term clinical and angiographic results. Ann of Thorac Surg. 2001; 72: 464- 468.
144. Formica F, Ferro O, Greco P, Martino A, Gastaldi D, Paolini G. Long term follow up of total arterial myocardial revascularization using exclusively Pedicle bilateral internal thoracic artery and right gastro epiploeic artery. Eur J Cardiothoracic Surg. 2004; 26: 1141-1148.
145. Bergsma TM, Grandjean JG, Voors AA, Boonstra PW, den Heyer P, Ebels T. Low recurrence of angina pectoris after coronary artery bypass graft surgery with bilateral internal thoracic and right gastro epiploeic arteries. Circulation. 1998; 97: 2402-2405.
146. Nishida H, Tomizawa Y, Endo M, Koyanagi H, Kasanuki H, et al. Coronary artery bypass with only in situ bilateral internal thoracic arteries and right gastro epiploeic artery.Circulation. 2001; 104: 761-780.
147. Tavilla G, Kappetein AP, Braun J, Gopie J, Tjien ATJ, Dion RAE. Long term follow up of coronary artery bypass grafting in three vessel disease using exclusively pedicle bilateral internal thoracic artery and right gastro epiploeic artery. Ann Thorac Surg. 2004; 77: 794-799.
148. Locker C, Schaff HV, Daly RC, Dearani JA, Bell MR, Frye R, et al. Multiple arterial grafts improve survival with coronary artery bypass graft surgery versus conventional coronary artery artery bypass grafting compared with percutaneous coronary intervention. J Thorac Cardiovasc Surg. 2016; 152: 369-379.
149. Holzhey DM, Cornely JP, Rastan AJ, Davierwala P, Mohr FW. Review of a 13 years single center experience with minimally invasive direct coronary artery bypass as the primary surgical treatment of coronary artery disease. Heart Surg Forum. 2012; 15: E61-E68.
150. McGinn JT Jr, Usman S, Lapierre H, Pothula VR, Mesana TG, Ruel M. Minimally inasive coronary artery bypass grafting: Dual center experience in 450 consecutive patients. Circulation. 2009; 120: S78-S84.
151. Harskamp RE, Williams JB, Halkos ME, Lopes RD, Tijssen JG, Ferguson TB, et al. Meta analysis of minimally invasive coronary artery bypass versus drug eluting stent for isolated Left anterior descending coronary artery disease. J Thorac Cardiovasc Surg. 2014; 148: 1837-1842.
152. Blazek S, Rossbach C, Borger MA, Fuernau G, Desch S, Eitel I, et al. Comparison of Sirolimus Eluting Stenting with Minimally Invasive Bypass Surgery for stenosis of the Left Anterior Descending Coronary Artery: 7 year follow up of a randomized trial. J Am Coll Cardiol Interv. 2015; 8: 30-38.
153. Bonaros N, Hennerbichler D, Friedrich G, Kocher A, Pachinger O, Laufer G, et al. Increased mortality and peri operative complications in patients with previous elective percutaneous coronary intervention undergoing coronary artery bypass surgery. J Thorac Cardiovasc Surg. 2009; 137: 846-852.
154. Hannan EL, Racz MJ, Gold J, Cozzens K, Stamato NJ, Powell T, et al. Adherence of Catheterization Laboratory Cardiologists to American College of Cardiology/American Heart Association Guidelines for Percutaneous Coronary Intervention and Coronary Artery Bypass Graft Surgery: What happens in actual practice? Circulation. 2010; 121: 267-275.
155. Kureshi F, Jones PG, Buchanan DM, Abdallah MS, Spertus JA. Variation in patients' perceptions of elective percutaneous coronary intervention in stable coronary artery disease: Cross Sectional Study. Br Med J. 2014; 349.
156. From AM, Badarin FJA, Cha SS, Rihal CS. Percutaneous coronary intervention with drug eluting stent versus coronary artery bypass surgery for multi vessel coronary artery disease: A meta analysis of available data from the ARTS II, SYNTAX, CARDia and ERACI III studies and a review of literature. Circulation. 2009; 120: 5940-5941.