Embed Size (px)
Citation preview
Pediatric Cardiology ECHO Clinic:Patient and Staff Scheduling Analysis
Angie Adams, Clinic Office Manager, Pediatric Cardiology ECHO ClinicRichard J. Coffey, Director, Program & Operations Analysis
Program & Operations Analysis Department
Final Report
December 15, 2005
Project Team:Kristin BankerStephanie Buck
Savitha ChelladuraiLindsey Selander
Ic
Table of Contents
Executive Summary .4Introduction 6Background 6
Scope (Included) 7Scope (Excluded) 7Project Deliverables 7
Approach and Methodology 8Interviews 8Scheduling at Other ECHO Clinics 8Literature Search 8Quantitative Data Collection 8Simulation 9
Results and Conclusions 9Interviews of UHMS Staff 9
Technicians: Add-on and late patients create scheduling backups 9Nurses and Outpatients Office Assistants: Queue for ECHO common occurrence. 10Administrative Staff High patient scheduling at peak hours 10
Scheduling at Other ECHO Clinics 11University of Chicago Corner Children ‘s Hospital: Pulifrom a List ofPatients 11Cincinnati Children ‘s Hospital: Enforce a late policy 11Cleveland Clinic Children Hospital: Stagger patient schedule times 11Children ‘s Hospital Boston: Employ many technicians 12
Literature Search 12Simulation to find solutions to patient waits 12Service time standard deviation 12Staffscheduling, changing work hours per day 12Solutions to delay problems: alter the service, arrival, and queueing processes 12
Quantitative Data Analysis 14Variations in procedure time 14Percentage of types ofECHOs 15Percentage ofECHOs by times lot 15Number ofECHOs per hour 16Total ECHOs per day 17ECHOs by type 19
Recommendations 20Create patient list to pullfrom, stagger technician lunches 20Enforce late penalties 20Change prescheduling process 21
Expected Impact 21Appendices 23
2
List of Tables and Figures
Table 1: Time needed to perfonTi an ECHO based on type 15Table 2: Percentage of ECHOs, per time slot, 2005 fiscal year 16Table 3: Overall Findings of Simulation (Based on 2005 Fiscal Data) 22
Figure 1: Average time needed to perform an ECHO based on type 14Figure 2: Percentage of ECHOs, per type, in one week 15Figure 3: ECHOs performed per hour (2005 Fiscal Year) 16Figure 4: ECHOs per hour by type (2005 Fiscal Year) 17Figure 5: Total ECHOs per day (2005 Fiscal Year) 1 8Figure 6: ECHOs per Day (Recorded October 4 — November 4) 18Figure 7: ECHOs per Day by Type (2005 Fiscal Year) 19Figure 8: Type of ECHOs performed per year (2005 Fiscal Year) 20
3
Executive Summary
The Pediatric Cardiology Echocardiogram Clinic Office Manager, Ms. Adams, perceivesa problem with the current scheduling of the Pediatric Cardiology EchocardiogramClinic. Her concerns include long wait times for patients and large amounts of downtimeand overtime by the technicians. The office manager would like to know if there is abetter way to schedule patients or technicians to prevent waiting and overtime.
There are a total of 6 technicians and 2 nurses available to perform echocardiograms. Thescheduling of current technicians and nurses is based on 8 hours per day, Mondaythrough Friday from 8am to 5pm with an hour lunch at noon. The PC ECHO Clinic has 6ECHO exam rooms with 1 extra machine for emergencies or bedside procedures. ECHOsare scheduled for 1-hour blocks but can take 20 to 90 minutes. The office managerreports that the ECHO Clinic has large backups of patients on certain days, particularlyTuesdays and Fridays, but on other days the clinic has gaps in its schedule. Patientsinclude inpatients, outpatients, new patients, and discharges. Patients between the ages of1 month and 2 years must be sedated which requires an additional 30 minutes for theprocedure.
MethodologyThe clinic was analyzed to identify the cause of these concerns and to find a feasiblesolution. The team worked on improving the efficiency of the scheduling of the full timeECHO technicians to achieve a balanced workload. Numerical and interview data wereexamined to produce a scheduling solution for the office manager.
To collect data, our team used five main methods. We conducted interviews with keystaff members of the clinic, collected data on ECHO times from the lab technicians,collected information on how other hospitals run their ECHO labs, conducted a literaturesearch, and analyzed the data collected with respect to the data received for an entirefiscal year.
Data AnalysisBased on 426 ECHOs collected from October 4th, 2005 to November 4th , 2005, theaverage time for an ECHO is 56.1 minutes, with a 23.1 minute standard deviation. If theprocedures are separated by type, Portable, Sedation, Fetal and Inpatient/Outpatient(Non-Sed), based on data analysis, sedation ECHOs require 20 more minutes to performthan the average time.
Other ECHO procedures are the most frequent with 67% of ECHOs in a one week timeperiod, followed by Portable at 24%. Based on this, the 60-minute time slots for ECHOsmay be most suited for the lab, but Fetal ECHOs may be able to be scheduled for shortertime slots and Sedation ECHOs must be allowed more time.
Based on Fiscal Year 2005 data, the clinic has been successful in spreading its patientload throughout the week. This consistency in scheduling is contrary to concernsexpressed by the office manager. This shows that the scheduling problems were not the
4
scheduling itself but the add-ons, patients who are added to the schedule last minute, thatcaused the greatest problems in schedule backups.
Conclusions and RecommendationsTo create better scheduling, one patient list should be created, which has 5 patientsscheduled per hour from 8am .- 11am and from 1pm - 3pm. This patient list will allow foran absent technician on any given day without a negative effect on the scheduling. Thetechnicians should be assigned patients using a pull system, where the next freetechnician is given the next available patient. The order of which technician is deemedfirst would rotate. This rotation among technicians would even out much of the work loadvariations between different technicians in this system. Technician’s lunches could alsobe staggered so that some technicians would always be on duty. This staggering is easilyincorporated into the recommended patient pull system and should prevent techniciansfrom having to move back their lunches when patients arrive during the normal lunchbreak
Our team created a simulation of staffing and scheduling changes, and according to thesimulation these changes would improve both technician utilization and patient waittimes. The simulation was performed assuming that 35 patients would be seen per day.The patient intake was based on the largest ECHO time in order for personal allowance.
Based on practices of other ECHO clinics, scheduling is organized in the simulation suchthat patients are pulled by the technicians as each is ready to take another patient. Fivepatients are scheduled per hour starting at 8am and ending at 3pm. The type of ECHO israndomized based on 2005 fiscal year data. This process will only work if the clinic canget patients scheduled; however, there is allowance for ‘surprise’ patients in the scheduleat the end of the day. This simulation also includes time at the end of each procedure,allowing procedures to run over. Also, the pull system allows for one ECHO to run overor under and not interfere too greatly with those scheduled. The 5 patients per hourallows for an absent technician, unknown patient flow, or extra long ECHO times. Theimprovements made by these recommendations include a decrease in patient wait time(11.4% decrease), increase in the number of patients seen per day (from 27.5 to 35patients), and an increase in technician utilization (from 55.92% to 76.91%).
5
Introduction
The Pediatric Cardiology Echocardiogram Clinic Office Manager, Ms. Adams, perceivesa problem with the current scheduling of the Pediatric Cardiology EchocardiogramClinic. Her concerns include long wait times for patients and large amounts of downtimeand overtime by the technicians. She would like to know if there is a better way toschedule patients or technicians to prevent waiting and overtime. The team analyzed theclinic to identify the cause of these complaints and find a feasible solution. The analysisincluded collecting of data from technicians by interviews and logging. The teamexamined the data to produce a scheduling solution for the clinic office manager.
Background
The University Medical Health Systems (UMHS) Pediatric Cardiology (PC)Echocardiogram (ECHO) Clinic and its 6 Full Time Equivalent (FTE) ECHO techniciansscan an average of 29 patients per day (a combination of inpatients and outpatients),Monday through Friday (holidays excluded). On Saturdays and Sundays, the ECHOactivity is greatly decreased, and physicians instead of technicians perform 1 to 4 ECHOsper day. The clinic also employs two nurses to assist in performing sedations for patientsbetween the ages of 2 months and 2 years. The scheduling of current technicians andnurses is based on 8 hours per day, Monday through Friday from 8am to 5pm with anhour lunch at noon.
The PC ECHO Clinic has 6 ECHO exam rooms with 1 extra machine for emergencies orbedside procedures. These machines require upgrading every 6 months and repair asneeded by a contractor. ECHOs are scheduled for 1-hour blocks but can take 20 to 90minutes
Patients include inpatients, outpatients, new patients, and discharges. These patients aremostly pediatric, but some PC ECHOs are performed on adults and fetuses. Outpatientsare prescheduled, but most inpatients cannot be scheduled in advance and are “forced”into the schedule as needed. Since many patients are from out-of-state or overseas, theycannot be asked to “come back later;” priority must be given to discharge patients tomake room for new patients in the hospital.
Patients between the ages of 2 months and 2 years must be sedated which requires anadditional 30 minutes for the procedure. Technicians also spend time waiting forinpatients due to scheduling conflicts within the hospital. The schedule also has gaps dueto cancellations and no shows of scheduled appointments.
Some ECHOs for returning outpatients are prescheduled by physicians and others are notprescheduled. New patients and non-prescheduled return visits are added to the schedulebefore or after clinic appointments. Inpatients are added to the schedule as necessarysince they can be called from the floor as needed. The current patient scheduling processcauses long wait times and disjointed scheduling due to its unpredictable nature.
6
Inpatients take priority over outpatients, causing longer wait times for outpatients wheninpatients have to be scheduled on short notice.
According to the Pediatric Cardiology Echocardiogram Clinic Office Manager, on somedays (especially Tuesdays and Fridays) the ECHO Clinic often has up to 5 patientswaiting. This backlog causes long patient wait times and sometimes results in techniciansworking overtime. On other days, only 2 ECHOs are scheduled in an 8 hour period.
Our task was to analyze the Pediatric Cardiology ECHO Clinic process and statisticallypredict its patient demand. Based on this predicted patient demand, our team developedrecommendations to improve patient wait times, clinic efficiency, staff efficiency, andstaff/patient flow.
Scope (Included)The scope of the project was limited to:
• The Pediatric Cardiology ECHO Clinic, its technicians, and its nurses• ECHOs performed primarily in the ECHO Clinic• ECHOs also performed in the Emergency Room and at bedside in the pediatric
and adult patient rooms.• All congenital disease patients who began their treatment within the Pediatric
Cardiology department (including adult patients if they were previous pediatricpatients who chose to continue their treatment with the clinic)
• Pregnant mothers who are having fetal ECHOs performed• Patients are classified as inpatient, outpatient, new patient, and discharge
Scope (Excluded)The scope of the project excluded was:
• The amount of time patients spend with the physician before the ECHO isperformed
• Any other time the patient spends within the hospital (aside from wait time for theECHO).
• The amount of time necessary to analyze the written ECHO reports.• Trans-esophagus ECHOs, the Into-catheter ECHOs, and the Echo-interpretations
for uncommon ECHOs
Project DeliverablesThis report presents the following information:
• A summary of our literature search• A flowchart of current clinic system• A summary of our statistic study• A summary of our scheduling simulation• A written report detailing recommended changes
7
Approach and Methodology
To determine a more efficient method of scheduling, our team conducted interviews withkey staff members of the clinic, collected data on ECHO times from the lab technicians,collected information on how other hospitals run their ECHO labs, conducted a literaturesearch, and analyzed the data collected over our time period and compared it with to thedata received for fiscal year 2005.
InterviewsTo determine how the staff of the clinic viewed the problem, the team interviewed thefollowing individuals: the six ECHO technicians; the two clinic nurses; the clinic cleric;the Director of Pediatric Cardiology, Dr. Albert Roccini; the Director of the PediatricECHO Laboratory, Dr. Gregory Ensing; and the two outpatient office assistants. Theseinterviews largely pertained to the areas of lab efficiency, procedures, and any thoughtsthat the interviewee may have had for improvement. Interview questions can be found inAppendix D.
Scheduling at Other ECHO ClinicsA number of other hospitals in the country run Pediatric ECHO clinics. The teaminterviewed personnel from University of Chicago Corner Children’s Hospital, CincinnatiChildren’s Hospital, Cleveland Clinic Children’s Hospital, and Children’s HospitalBoston. These interviews were performed in order to determine if these clinics hadscheduling methods that prevented patient waits and technician overtime.
Literature SearchA literature search has been completed using the following information sources:University of Michigan’s Library Journals and Newspapers, the Journal of IndustrialTechnology, the Journal of Industrial Economics, and other selected journals thatregularly publish papers regarding scheduling. The search was performed in order todetermine how other systems with similar problems have changed their schedulingmethods.
Quantitative Data CollectionWe collected data from the ECHO technicians about the time to complete different typesof ECHOs. The team created data collection sheets, and the six technicians were asked tofill them out. The technicians noted the type of ECHO procedure completed as well as itsstart and finish time. The team members then collected these data sheets. The data aboutthe times were then entered and analyzed as they were received. The data collection wasconducted from October 4th to November 4th with which 24 days and 426 ECHOs wereobserved. Log sheets created by the team can be found in Appendix E.
The Clinic Office Manager, Angie Adams, also provided us with information about thenumber, type, and time that ECHOs occurred for the 2005 fiscal year. This data wascompared to what we collected to see how the newly collected data compared to the year,as a whole.
8
Simulation
A simulation was performed by our team to test the recommended schedule. Given thescheduling recommendations, the simulation was developed assuming that 35 patientswould be seen per day. The patient intake was based on the largest ECHO time in orderfor personal allowance. The scheduling was based off of the 2005 fiscal year, and thetype of ECHO was randomized based on this year’s data. Lunches were scheduled for thetechnicians in blocks as close to one hour as possible.
The scheduling is performed such that patients are pulled by the technicians as theybecome available again. Five patients are scheduled per hour, on the hour, starting at8am and ending at 3pm. The type of ECHO is randomized based on percentagesdetermined using 2005 fiscal year data. This scheduling system will only work if theECHO clinic can get patients scheduled; however, this system has an allowance for‘surprise’ patients in the schedule at the end of the day. This simulation also includestime at the end of each procedure, allowing procedures to run over. Also, first availableallows for one ECHO to run over or under and not interfere too greatly with thosescheduled. A simulation of scheduling 5 patients per hour allows for an absenttechnician, unknown patient flow, or extra long ECHO times. This simulation wasperformed for both a lab running with six technicians as well as one with five, to allowfor one absent technician.
Results and Conclusions
Both qualitative and quantitative data have been analyzed to describe the current situationand determine possible improvements. Qualitative data was collected through interviewsof UHMS ECHO staff and personnel from other hospitals, as well as a literature search.Data on the time of day in which ECHOs were performed from the 2005 fiscal year havebeen analyzed, as well as the logging data collected from the ECHO lab. Results fromthese analyses are discussed below.
Interviews of UHMS StaffTo better understand the current situation, the team interviewed all of the ECHO lab staff;the Director of Pediatric Cardiology, Dr. Albert Roccini; and two outpatient officeassistants. A summary of these interviews follows.
Technicians: Add-on and late patients create scheduling backupsNone of the six technicians reported feeling overworked due to the current scheduling ofthe clinic. However, all technicians reported there were days that they felt eitheroverworked or under-worked, and that these days balanced each other. Technicians alsoreported that they did not take overtime at the end of the day but consistently missedlunch to finish patients’ scans. Two of the six technicians felt very strongly that lunchshould not be missed during their day. These missed lunches are considered overtime.Technicians also reported seeing on average 4-6 patients per day and spending 45-60minutes with each patient.
9

Technicians answered similarly to one another on questions about procedures and feltthat there were time and procedure differences depending on each patient, and they feltthat these could vary greatly if a patient with a “complicated” case was scheduled.
Four out of six technicians did not have a problem with the current system and often feltthat uncertainty and scheduling problems were the nature of the lab and that nothingcould be done about it. Those technicians that did report being unhappy with the currentsituation identified the scheduling as the source of the problem. Among technicians,patients that were added to the schedule last minute, add-ons, and patients that arrivedlate were identified as the major problems. The clinic currently takes late patients inahead of other patients that have been waiting. This system of accepting late patientscauses even longer wait times for the patients that had arrived before them.
All technicians were also open to working hours other than 8 am to 5 pm, 5 days perweek. They have tried to implement a 10 hour a day, 4 days per week schedule, but thedoctors were not open to it due to their own clinic schedules.
Nurses and Outpatients Office Assistants: Queuefor ECHO common occurrenceOne nurse interviewed reported feeling a little under-worked and under-utilized, whereasthe other has more responsibilities and performs other tasks outside the ECHO lab. Theywere both comfortable with different working hours and schedules. Both outpatient officeassistants reported feeling a little overworked but their scheduling is out of our scopesince the assistants work for both the ECHO and regular PC lab. The assistants wereinterviewed because they are essential to patient flow from the outpatient clinics. Bothassistants also reported that ECHOs get backed up every day; depending on the day theback up averages 20-3 0 minutes or up to an hour. One assistant reported that the ECHOflow seemed to be a problem with technicians not being assigned to patients who werealready waiting in the clinic; the technicians were therefore free even though there was aqueue of patients for ECHOs in the PC waiting room. An assistant stated that patients arecalled the day before to be reminded of their appointment and this procedure has reducedno shows to some extent.
Administrative Staff High patient scheduling atpeak hoursAdministrative staff believes that too many patients are scheduled during peak hours andtoo few patients at other times. Staff has stated that too many patients are added to theschedule at the last minute, add-ons, due to clinics. These staff members also suggestedthat lunches should be staggered to allow for technicians to take their lunch break andstill meet the patient flow needs. One staff member also suggested scheduling moreelective ECHOs for non-peak hours. Another staff member and a doctor suggestedsetting aside blocks of time for add-ons from clinics which often add-on, if there is aprospective number based on historical data. The staff also stated that chaos occurs in theECHO lab when technicians are out on vacation or call in sick. One staff member statedthat the desired 4 days per week, 10 hour each day is probably not an option because itwould increase this chaos, and is not needed from the administrative point of view. Onedoctor claims that adding more technicians will not solve this problem since 7.5 yearsago the ECHO clinic employed 3 technicians with half the business.
10
One staff member stated lack of communication and understanding as main problemswithin the ECHO lab. Another concern voiced by two of the staff members is who getsprecedence, inpatients or outpatients.
Based on these staff interviews a flowchart of the current clinic system is included inAppendix A.
Scheduling at Other ECHO ClinicsA number of other hospitals in the country run Pediatric ECHO clinics. The teaminterviewed personnel from these hospitals in order to determine if these clinics hadscheduling methods that prevent patient waits and technician overtime.
University of Chicago Corner Children ‘s Hospital: Pullfrom a List ofPatientsCurrently University of Chicago’s Pediatric Cardiology ECHO lab would like to hire oneadditional technician. This need for an additional technician has caused backups thatwould not normally occur. The lab usually employs three technicians and a coordinator,who also performs procedures. The lab is separated into inpatient and outpatient labs. Allinpatient procedures are performed in the patient rooms although they have a room forprocedures which is rarely used, The outpatient lab has two procedure rooms from whichtwo of the technicians work. The other technicians perform the portable ECHOs forinpatients. Approximately 20 ECHOs are performed each day. All are scheduled with onelist containing outpatients and one containing inpatients. As the technicians finish withone patient they pull the next patient on the list. Patients are not scheduled to a specifictechnician.
Cincinnati Children’s Hospital: Enforce a late policyThe ECHO lab at Cincinnati Children’s Hospital reports the average patient wait times tobe 10-15 minutes for ECHOs. The lab has four rooms for procedures and employs eighttechnicians, with one technician performing fetal ECHOs only. The lab servicesinpatients and outpatients, but inpatients are done only by portable, unless the patientrequires sedation; if sedation is necessary the inpatient is brought to the lab. The lab seesan average of 32 to 36 patients per day. The lab enforces a strict late policy: if a patient is20 minutes late they get pushed to the bottom of the list; if they are an hour late they arerescheduled to another day.
Cleveland Clinic Children ‘s Hospital: Stagger patient schedule timesCleveland Clinic ECHO lab employs six technicians and contains three rooms forprocedures. The lab reports there is more demand than rooms to accommodate thepatients; however, they rarely experience backups. The lab sees an average of 20 to 25patients per day of which 3 to 10 per day are portables. Procedures are scheduled in 45-minute time blocks and patients’ times are staggered. Late patients are fit into theschedule once they arrive.
11
Children ‘s Hospital Boston: Employ many techniciansThe ECHO lab has 18 technicians and 8 rooms. The lab sees 40 to 50 scheduled patientsand 20 to 30 add-on patients per day. Inpatient add-ons are mainly done by portable. Sixof the eight rooms are scheduled with the other two rooms left for outpatient added-ons.
Literature SearchA literature search, focusing on appointment systems and scheduling of staff in healthcare, supports the methodology of this project and provides some suggestions forscheduling.
Simulation to find solutions to patient waitsOne simulation-based study of a walk-in clinic in the United Kingdom1used similarmeans of data collection for their simulation as well as similar sample sizes. The studyused both historical and collected data and ran a simulation based on both. Thesimulation was also done for a worst case scenario when appointments took longer thanthe scheduled block time. In addition, “probability distributions were used to mimic theway in which inter-arrival times and service times vary about their average values fromcase to case.” The Centre was also concerned with coordinating multiple clinics as occursin the ECHO lab with x-ray. “Since the study was primarily concerned with reducing thenumber of people in the waiting room, it seemed sensible to investigate whethertimetabling short-running clinics (i.e. clinics that did not run all day) at less busy timeswould be feasible and effective.” This idea of timetabling short-running clinics is out ofour scope, but a thought for further study. This study focused on the simulation model butused discussion and observation to find a solution to patient wait times. The study alsosuggested “advertising” quieter times which can be applied to the ECHO lab in terms ofprescheduling during times that are known to be slower, such as 8 am on Mondaymornings.
Service time standard deviationAn article by Kiassen and Rohleder5suggested methods for Scheduling OutpatientAppointments in a Dynamic Environment, such as the ECHO lab. They found “bestresults can be obtained in all cases if clients with large service time standard deviationsare scheduled toward the end of the appointment session.”
Staffscheduling, changing work hours per dayA study by George, et al titled A Simulation Study to Evaluate Hospital Operating RoomPerformance2,found that changing the staffing schedule from 5-8 hour days to 4-10 hourdays did not improve utilization because the number of patients and the number of staff atpeak times did not change. For the ECHO lab, since the limiting factor is the number ofexam rooms which is currently limited to 6, changing the scheduling of staff from 8-hourwork days to 10-hour work days will not change the situation.
Solutions to delay problems: alter the service, arrival, and queueing processesModeling Patient Flows Through the HEALTHARE System (Chapter l) includes a casestudy of a LA County/USC health center which shows that health care delays can bereduced “through awareness of best practices, application of quantitative methods, and a
12

commitment to change.” This method of delay reduction requires the cooperation of allinvolved parties to share practices and coordinate activities. The text also suggests that“solutions to delay problems come in three forms: alter the service, arrival, and queueingprocesses”. All three areas should be addressed to find success in the new ECHOscheduling procedure. Hall also refers to the negative effect that absenteeism has onscheduling. Absenteeism is a problem the ECHO lab faces when the lab is short staffeddue to vacation time or sick leave. Other problems that can occur include delay intransportation of patients due to the large demand on the transport system of the hospital.The text also recommended forming a diverse team, pulling from all parts of the hospitaland from all disciplines that can see the process as a whole and make improvements overthe entire system. These changes should take the form of a hospital-wide schedulingsystem and simulation tools to forecast changes before final decisions are made.
Other resources cited provided similar insights to the above mentioned articles. A list ofreferences can be found in Appendix F.
13
Quantitative Data Analysis
Two types of data were analyzed for the purpose of our study, data collected fromOctober 4thi to November 4th, 2005 and Fiscal Year 2005 data. Findings from this datumwere used to create a scheduling recommendation and a simulation to model therecommendation.
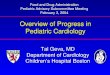
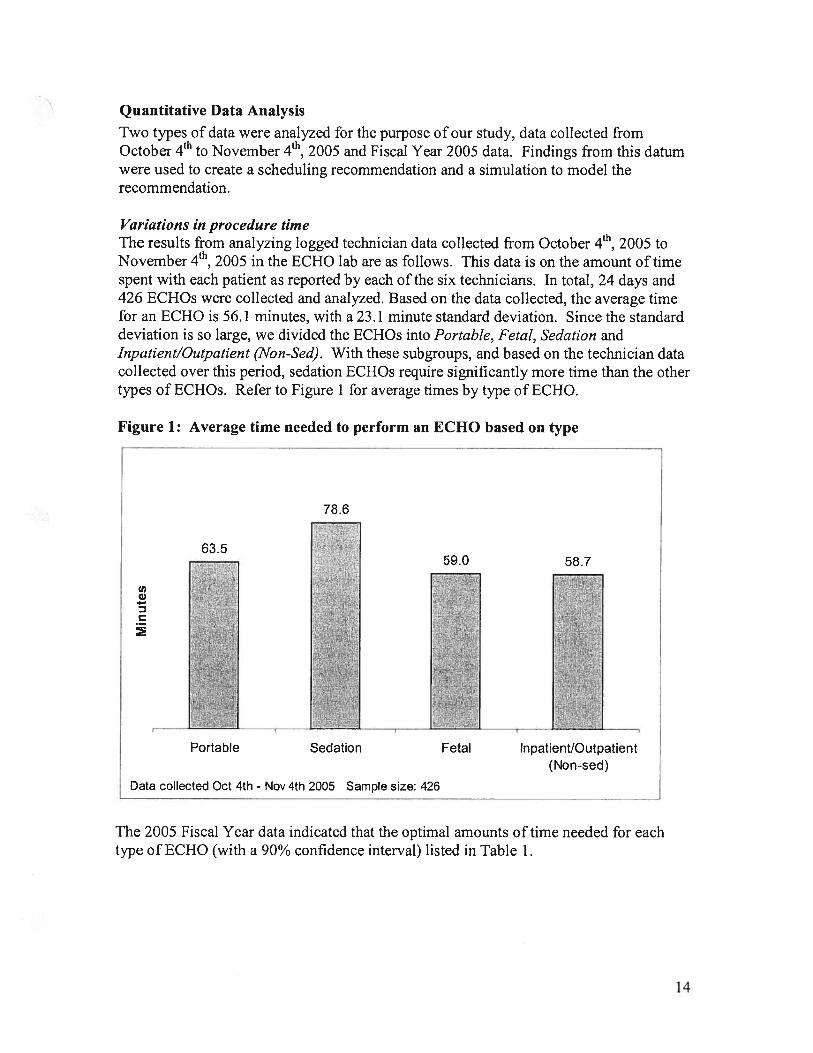
Variations in procedure timeThe results from analyzing logged technician data collected from October 4th, 2005 toNovember 4th, 2005 in the ECHO lab are as follows. This data is on the amount of timespent with each patient as reported by each of the six technicians. In total, 24 days and426 ECHOs were collected and analyzed. Based on the data collected, the average timefor an ECHO is 56.1 minutes, with a 23.1 minute standard deviation. Since the standarddeviation is so large, we divided the ECHOs into Portable, Fetal, Sedation andInpatient/Outpatient (Non-Sed). With these subgroups, and based on the technician datacollected over this period, sedation ECHOs require significantly more time than the othertypes of ECHOs. Refer to Figure 1 for average times by type of ECHO.
Figure 1: Average time needed to perform an ECHO based on type
The 2005 Fiscal Year data indicated that the optimal amounts of time needed for eachtype of ECHO (with a 90% confidence interval) listed in Table 1.
78.6
63.5
cnC,4-
D
59.0 58.7
Data collected Oct 4th - Nov 4th 2005 Sample size: 426
Portable Sedation Fetal Inpatient/Outpatient(Non-sed)
14
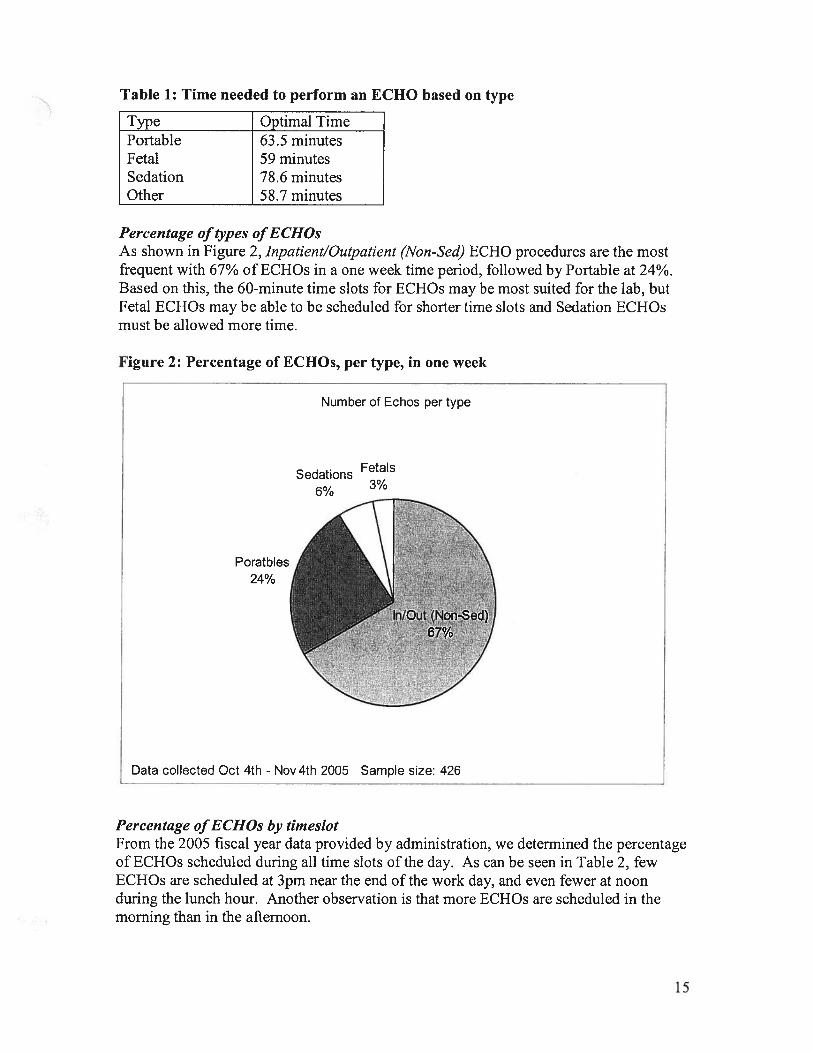
Table 1: Time needed to perform an ECHO based on type
Type Optimal TimePortable 63.5 minutesFetal 59 minutesSedation 78.6 minutesOther 58.7 minutes
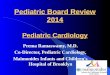
Percentage of types ofECHOsAs shown in Figure 2, Inpatient/Outpatient (Non-Sed) ECHO procedures are the mostfrequent with 67% of ECHOs in a one week time period, followed by Portable at 24%.Based on this, the 60-minute time slots for ECHOs may be most suited for the lab, butFetal ECHOs may be able to be scheduled for shorter time slots and Sedation ECHOsmust be allowed more time.
Figure 2: Percentage of ECHOs, per type, in one week
Percentage ofECHOs by timeslotFrom the 2005 fiscal year data provided by administration, we determined the percentageof ECHOs scheduled during all time slots of the day. As can be seen in Table 2, fewECHOs are scheduled at 3pm near the end of the work day, and even fewer at noonduring the lunch hour. Another observation is that more ECHOs are scheduled in themorning than in the afternoon.
Number of Echos per type
FetalsSedations3%6%
Poratbles24%
Data collected Oct 4th - Nov 4th 2005 Sample size: 426
15
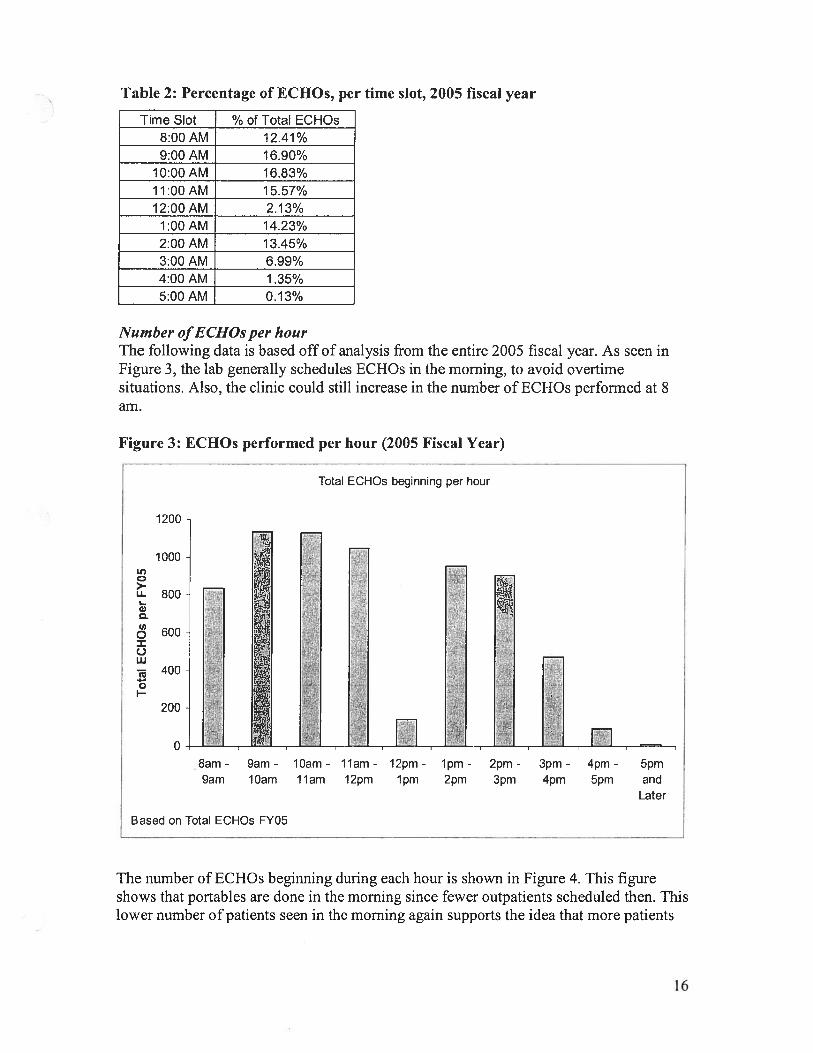
Table 2: Percentage of ECHOs, per time slot, 2005 fiscal year
Time Slot % of Total ECHOs8:00AM 12.41%9:00AM 16.90%
10:00AM 16.83%11:00 AM 15.57%12:00AM 2.13%
1 :00 AM 14.23%2:00AM 13.45%3:00 AM 6.99%4:00 AM 1 .35%5:00AM 0.13%
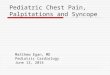
Number ofECHOs per hourThe following data is based off of analysis from the entire 2005 fiscal year. As seen inFigure 3, the lab generally schedules ECHOs in the morning, to avoid overtimesituations. Also, the clinic could still increase in the number of ECHOs performed at 8am.
The number of ECHOs beginning during each hour is shown in Figure 4. This figureshows that portables are done in the morning since fewer outpatients scheduled then. Thislower number of patients seen in the morning again supports the idea that more patients
Figure 3: ECHOs performed per hour (2005 Fiscal Year)
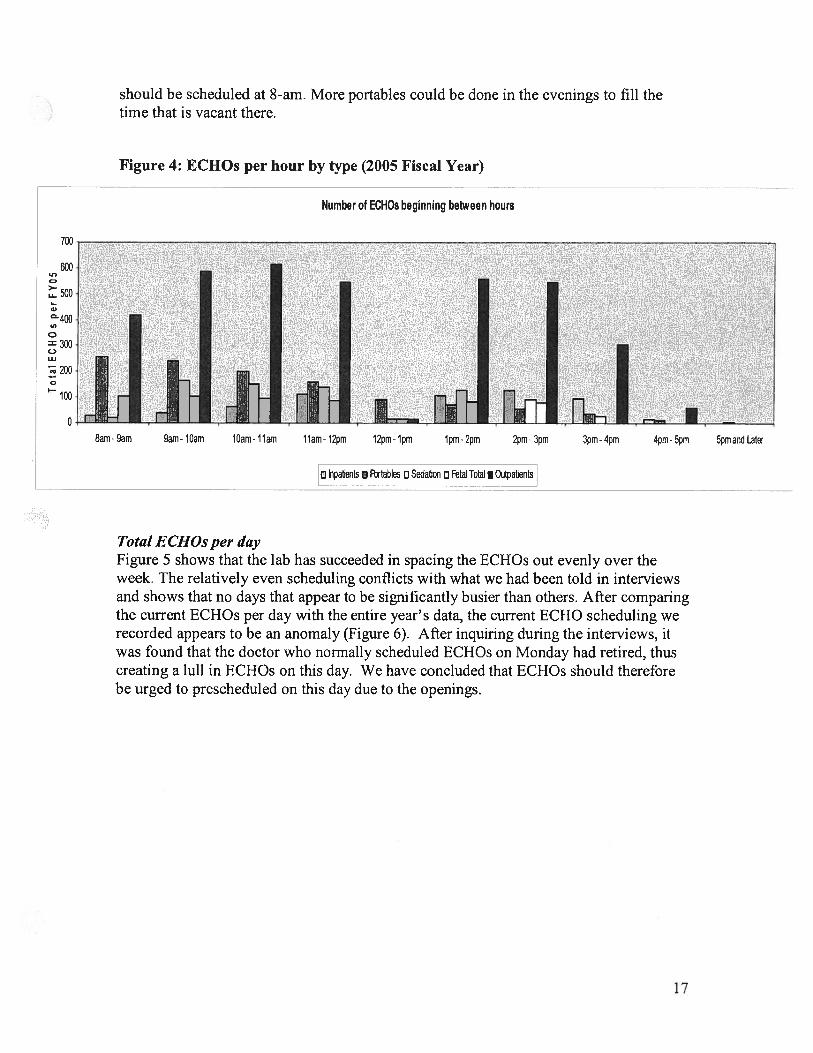
should be scheduled at 8-am. More portables could be done in the evenings to fill thetime that is vacant there.
Figure 4: ECHOs per hour by type (2005 Fiscal Year)
a pabents a Fectabes a Sedation a Fetal Total I Outpaents
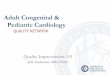
Total ECHOs per dayFigure 5 shows that the lab has succeeded in spacing the ECHOs out evenly over theweek. The relatively even scheduling conflicts with what we had been told in interviewsand shows that no days that appear to be significantly busier than others. After comparingthe current ECHOs per day with the entire year’s data, the current ECHO scheduling werecorded appears to be an anomaly (Figure 6). After inquiring during the interviews, itwas found that the doctor who normally scheduled ECHOs on Monday had retired, thuscreating a lull in ECHOs on this day. We have concluded that ECHOs should thereforebe urged to prescheduled on this day due to the openings.
Number of ECHOs beginning between hours
U,0>-Li.
a,
400a,
300C.,
Ui
200
100
8am- 9am 9am- lOam lOam- 11am 11am- 12pm 12pm- 1pm 1pm- 2pm 2pm- 3pm 3pm- 4pm 4pm- 5pm 5pmand Later
17
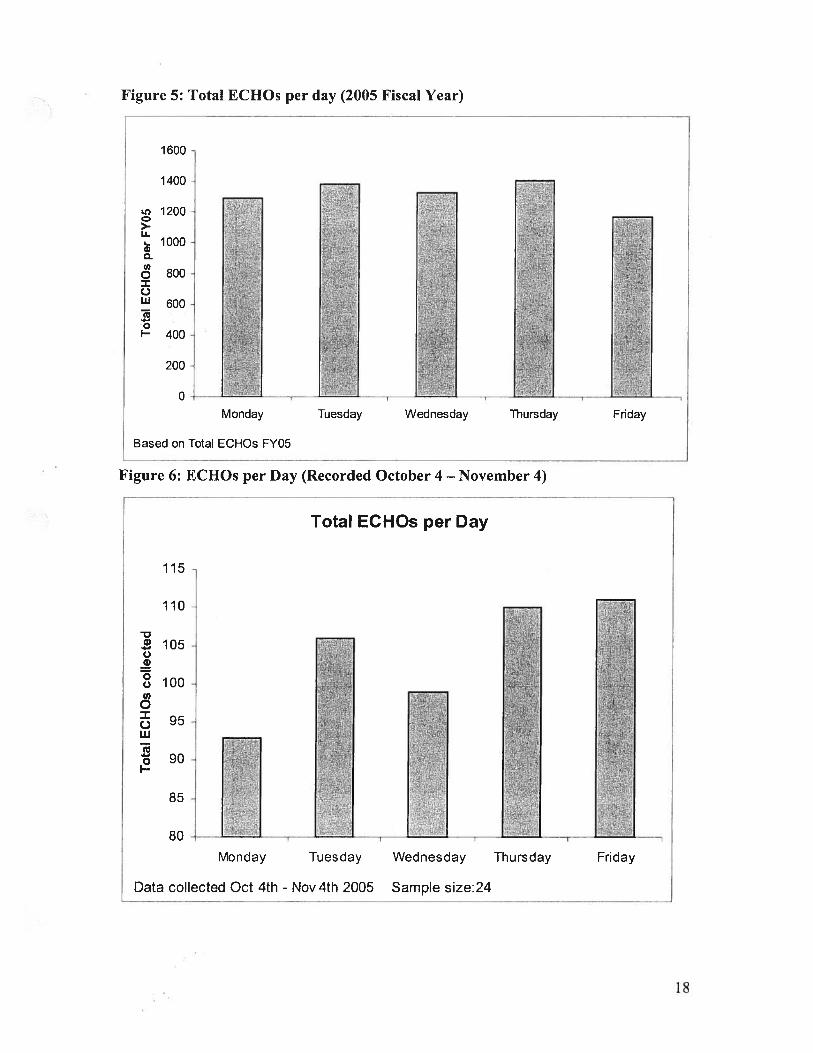
Figure 5: Total ECHOs per day (2005 Fiscal Year)
1600
1400
1200
___
>-Li.10o0 -
U,o 800 /
W 600
I— 400
200
0 —
________
——___________
________
. - - —-_______
Monday Tuesday Wednesday Thursday Friday
Based on Total ECHOs FY05
Figure 6: ECHOs per Day (Recorded October 4 — November 4)
Total ECHOs per Day
115
110
-
___
-:W inic . -
o 100.
0
I.Ll -
.o -•- ..
.._:.
I- .- -.
85- .
80- I I —
Monday Tuesday Wednesday Thursday Friday
Data collected Oct 4th - Nov 4th 2005 Sample size:24
18
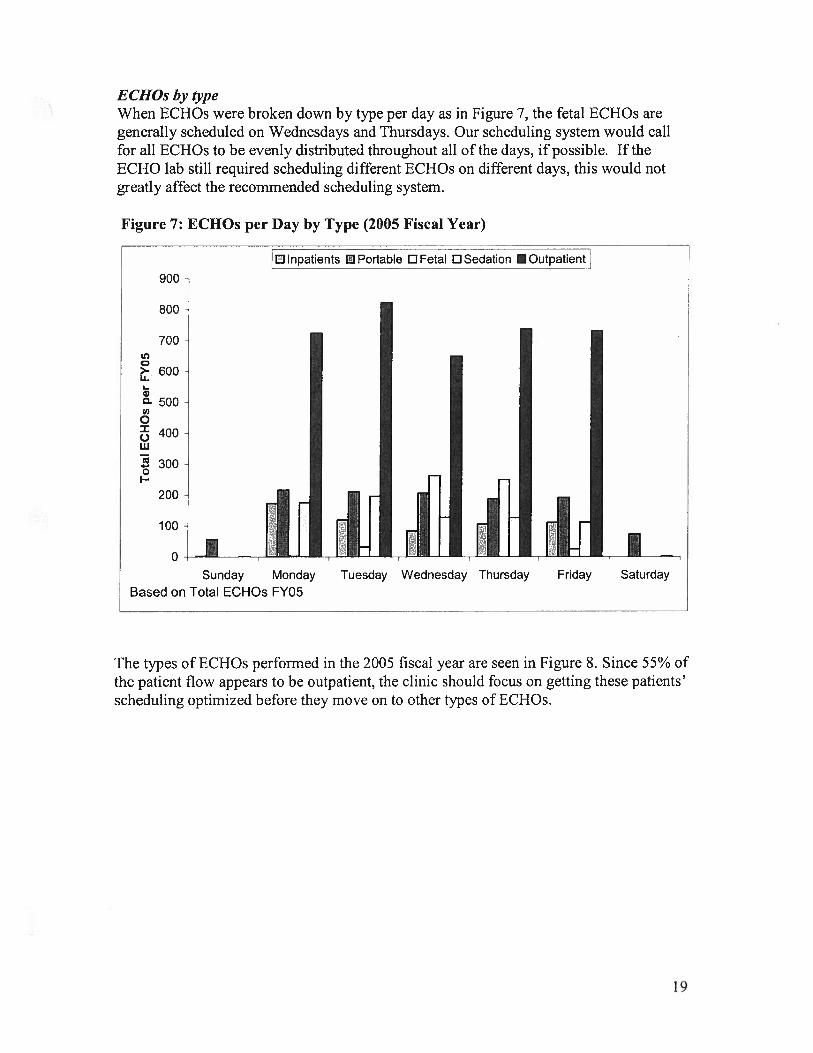
ECHOs by typeWhen ECHOs were broken down by type per day as in Figure 7, the fetal ECHOs aregenerally scheduled on Wednesdays and Thursdays. Our scheduling system would callfor all ECHOs to be evenly distributed throughout all of the days, if possible. If theECHO lab still required scheduling different ECHOs on different days, this would notgreatly affect the recommended scheduling system.
Figure 7: ECHOs per Day by Type (2005 Fiscal Year)
The types of ECHOs performed in the 2005 fiscal year are seen in Figure 8. Since 55% ofthe patient flow appears to be outpatient, the clinic should focus on getting these patients’scheduling optimized before they move on to other types of ECHOs.
900
800
Dinpatients PortabIe DFetaI DSedation iOutpatientj
700
600
500
C>-U..
a)c.U,0
0Ui
4-0
400
300
200
100
0
Sunday MondayBased on Total ECHOs FY05
Tuesday Wednesday Thursday Friday Saturday
19
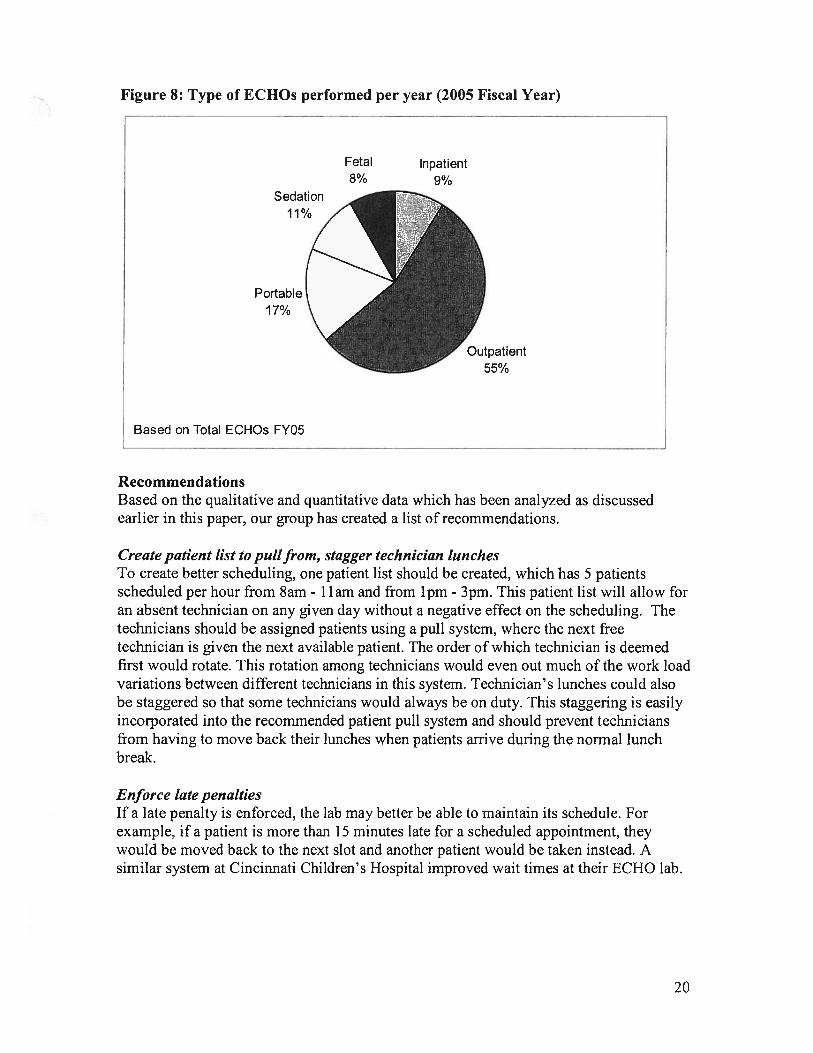
Figure 8: Type of ECHOs performed per year (2005 Fiscal Year)
RecommendationsBased on the qualitative and quantitative data which has been analyzed as discussedearlier in this paper, our group has created a list of recommendations.
Create patient list to pullfrom, stagger technician lunchesTo create better scheduling, one patient list should be created, which has 5 patientsscheduled per hour from 8am 11am and from 1pm - 3pm. This patient list will allow foran absent technician on any given day without a negative effect on the scheduling. Thetechnicians should be assigned patients using a pull system, where the next freetechnician is given the next available patient. The order of which technician is deemedfirst would rotate. This rotation among technicians would even out much of the work loadvariations between different technicians in this system. Technician’s lunches could alsobe staggered so that some technicians would always be on duty. This staggering is easilyincorporated into the recommended patient pull system and should prevent techniciansfrom having to move back their lunches when patients arrive during the normal lunchbreak.
Enforce late penaltiesIf a late penalty is enforced, the lab may better be able to maintain its schedule. Forexample, if a patient is more than 15 minutes late for a scheduled appointment, theywould be moved back to the next slot and another patient would be taken instead. Asimilar system at Cincinnati Children’s Hospital improved wait times at their ECHO lab.
Fetal8%
Inpatient9%
Sedation11%
Portable17%
Based on Total ECHOs FY05
Outpatient55%
20
Change prescheduling processWe recommend that doctors preschedule and inform the lab of possible ECHO patients aday in advance. This information would allow for shorter patient wait times because thepatient’s appointment would be scheduled in advance instead of pushed into the existingschedule. In addition, leaving some time blocks open for any last minute outpatientswould allow flexibility in scheduling.
Prescheduling advance ECHOs for Mondays at 8 am would allow for more ECHOs to beadded to the schedule without creating delays for other patients since early morningECHOs are less frequent.
In the future, the team recommends doing a statistical analysis of what percentage ofpatients each doctor adds on for ECHOs after their clinics. Based on this data the ECHOclinic will be able to leave open a certain amount of procedure slots each day toaccommodate the predicted number of add ons by doctors.
Expected Impact
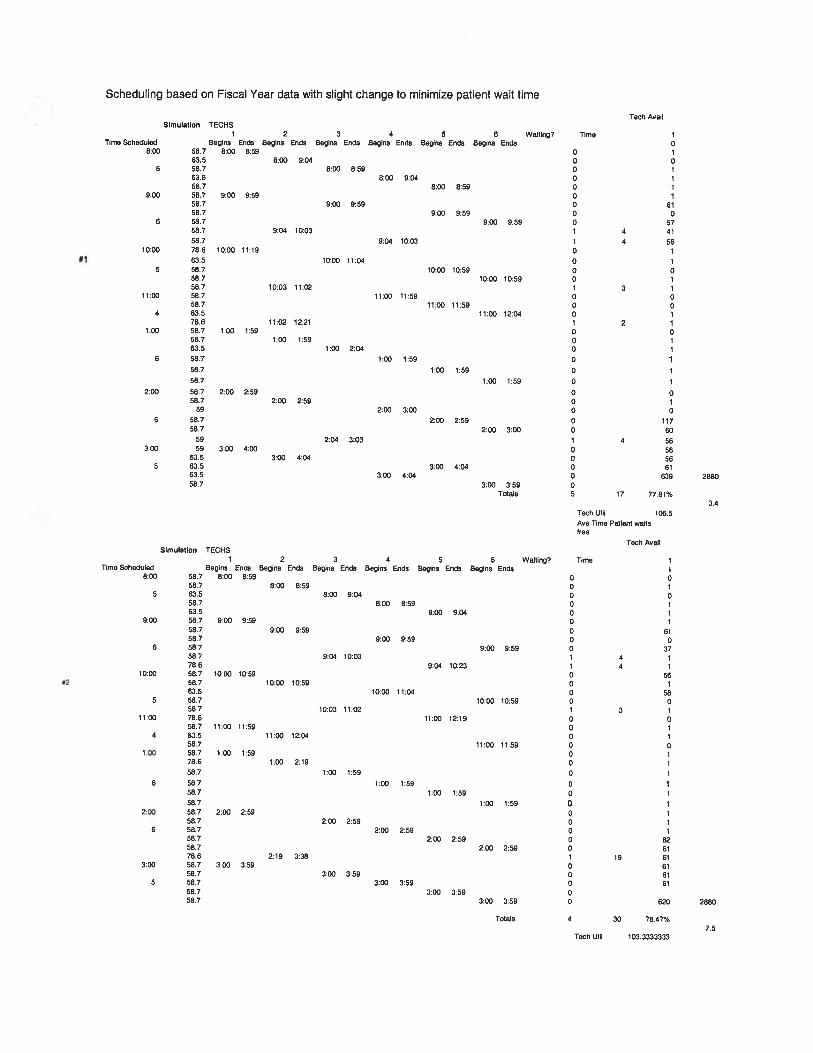
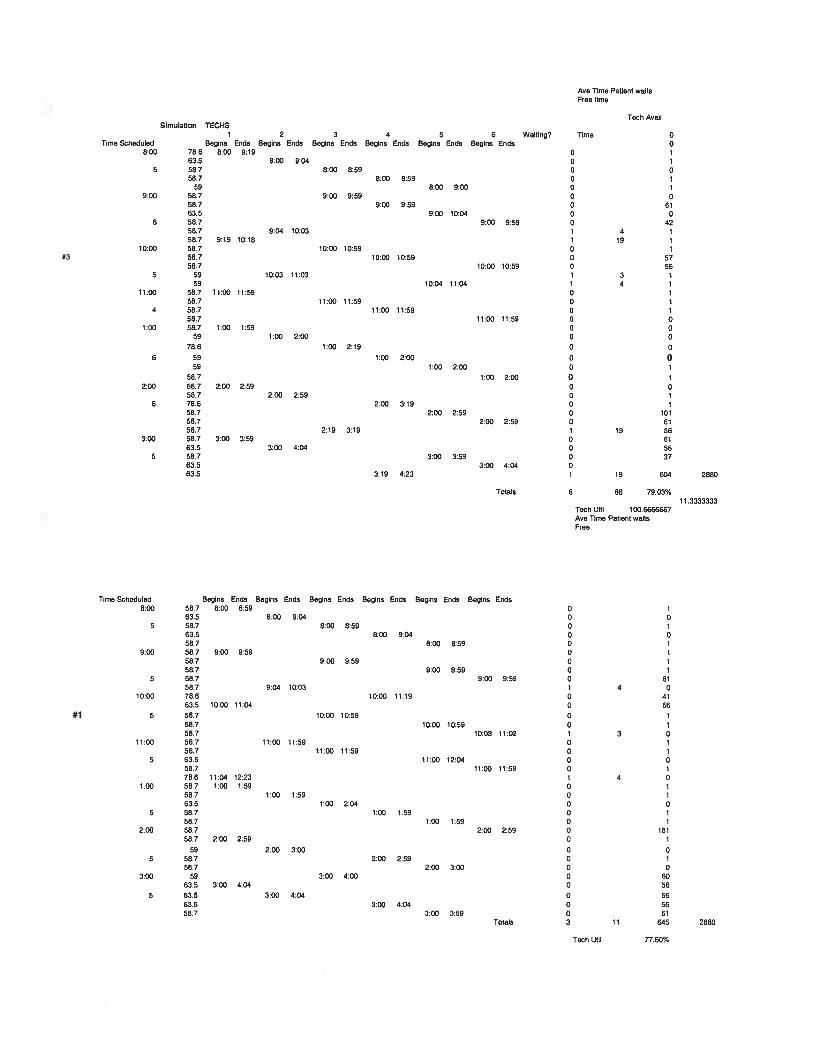
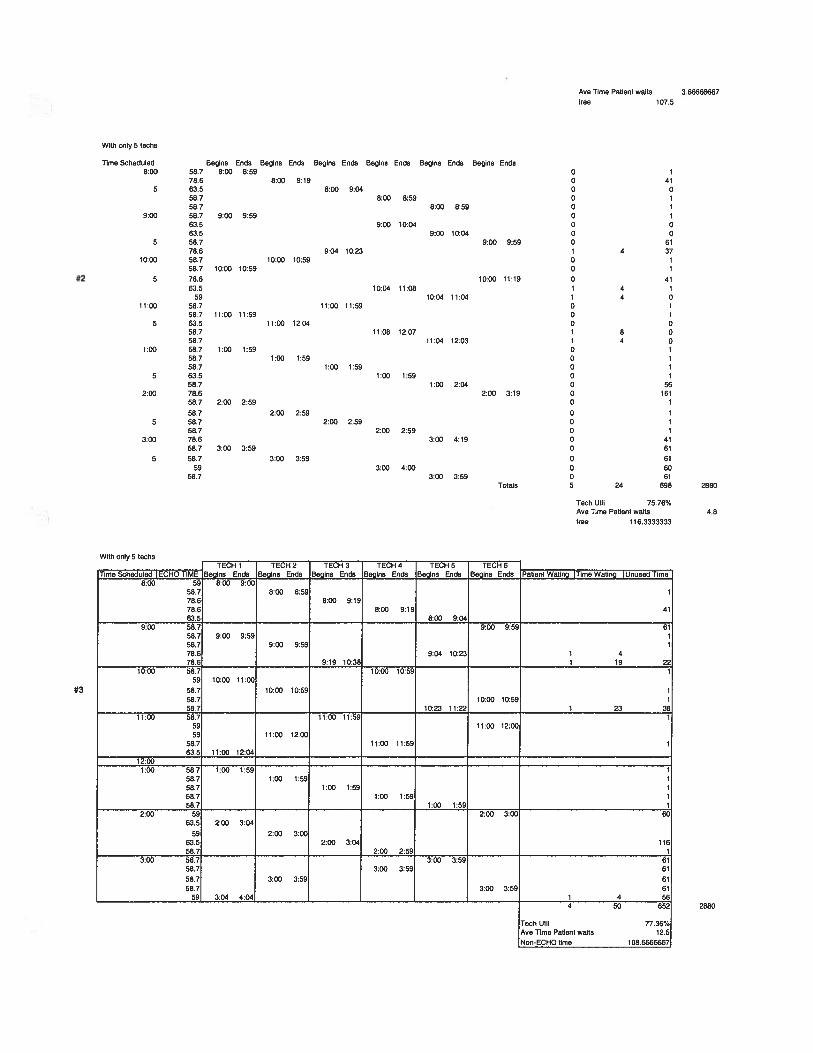
Based on a simulation which our team has performed of staffing and scheduling changes,there would be improvements made in both technician utilization and patient wait times.The simulation can be found in Appendix B. This was performed assuming that 35patients would be seen per day. Lunches were scheduled for the technicians in blocks asclose to one hour as possible.
The scheduling is performed such that patients are pulled by the technicians as theybecome available again. Five patients are scheduled per hour starting at 8am and endingat 3pm. This scheduling system will only work if the ECHO clinic can get patientsscheduled; however, this system has an allowance for ‘surprise’ patients in the scheduleat the end of the day. This simulation also includes time at the end of each procedure,allowing procedures to run over. Also, this pull system allows for one ECHO to run overor under and not interfere too greatly with those scheduled. The simulation of 5 patientsper hour allows for an extra technician to be gone in the case of emergencies, unknownpatient flow, or extra long ECHO times.This simulation was performed for both a lab running with six technicians as well as onewith five, to allow for one absent technician. Table 3 summarizes these findings.
21
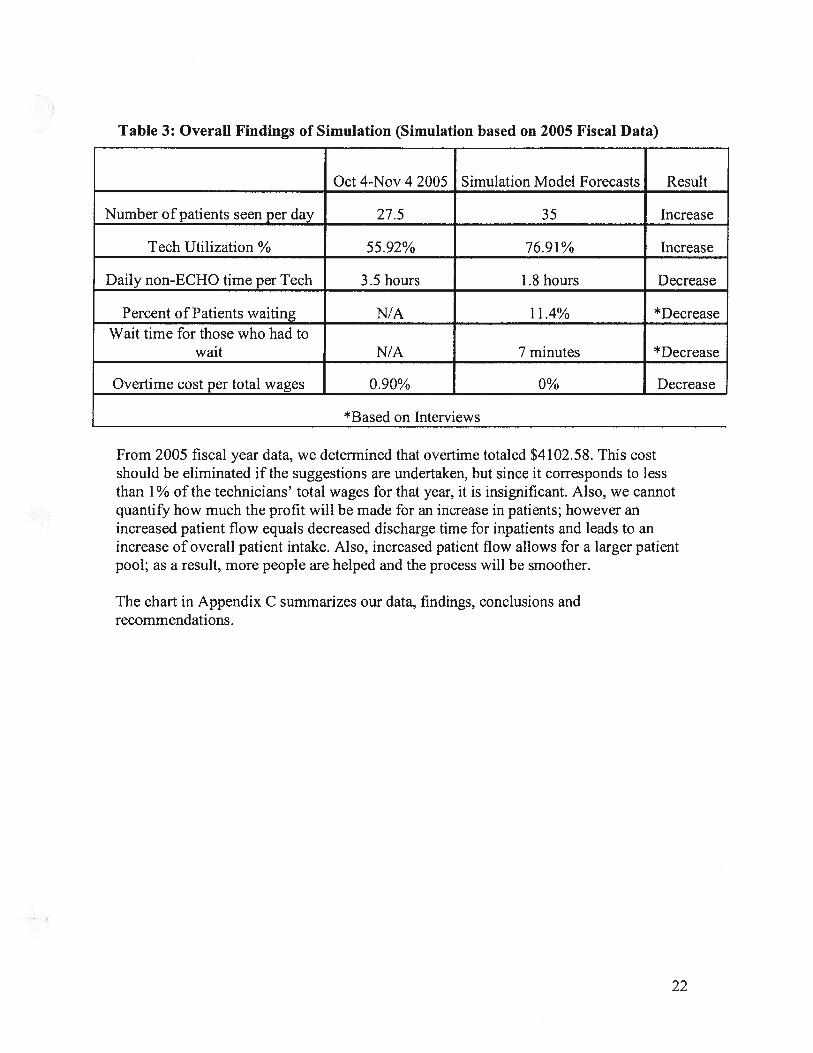
Table 3: Overall Findings of Simulation (Simulation based on 2005 Fiscal Data)
Oct 4-Nov 4 2005 Simulation Model Forecasts Result
Number of patients seen per day 27.5 35 Increase
Tech Utilization % 55.92% 76.9 1% Increase
Daily non-ECHO time per Tech 3.5 hours 1.8 hours Decrease
Percent of Patients waiting N/A 11.4% *Decrease
Wait time for those who had towait N/A 7 minutes *Decrease
Overtime cost per total wages 0.90% 0% Decrease
*Based on Interviews
From 2005 fiscal year data, we determined that overtime totaled $4102.58. This costshould be eliminated if the suggestions are undertaken, but since it corresponds to lessthan 1% of the technicians’ total wages for that year, it is insignificant. Also, we cannotquantify how much the profit will be made for an increase in patients; however anincreased patient flow equals decreased discharge time for inpatients and leads to anincrease of overall patient intake. Also, increased patient flow allows for a larger patientpool; as a result, more people are helped and the process will be smoother.
The chart in Appendix C summarizes our data, findings, conclusions andrecommendations.
22
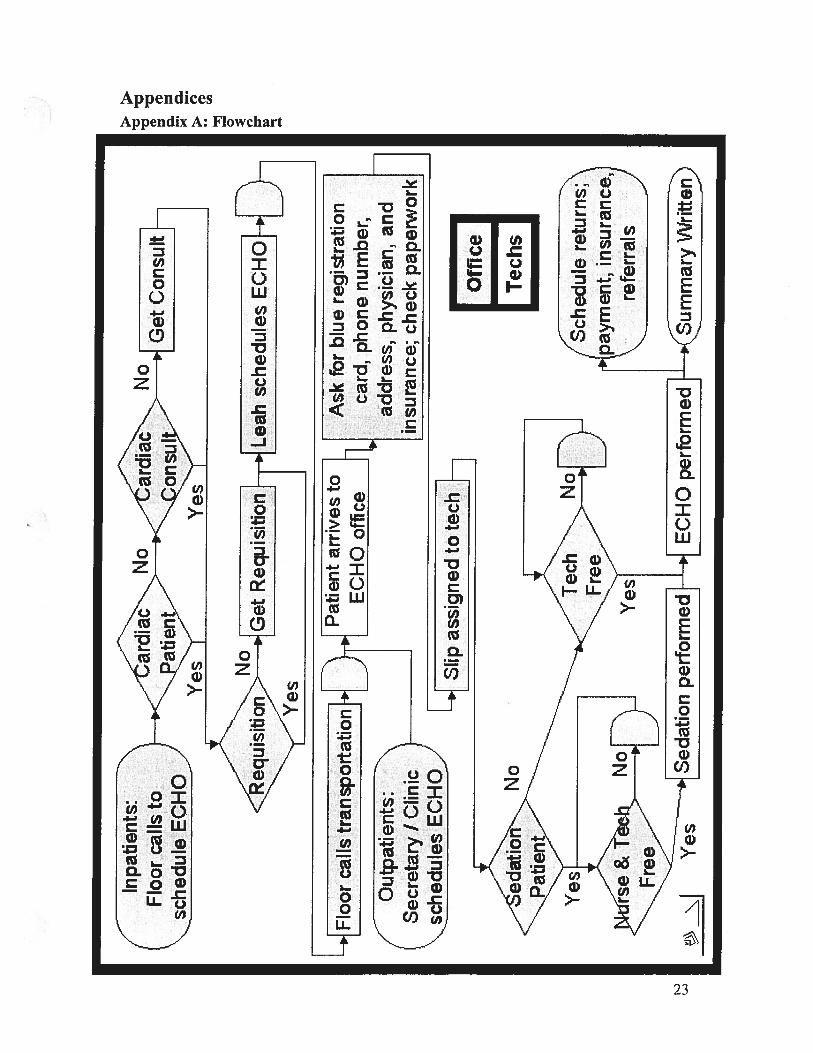
AppendicesAppendix A: Flowchart
Cl)
C.,
Oi
23
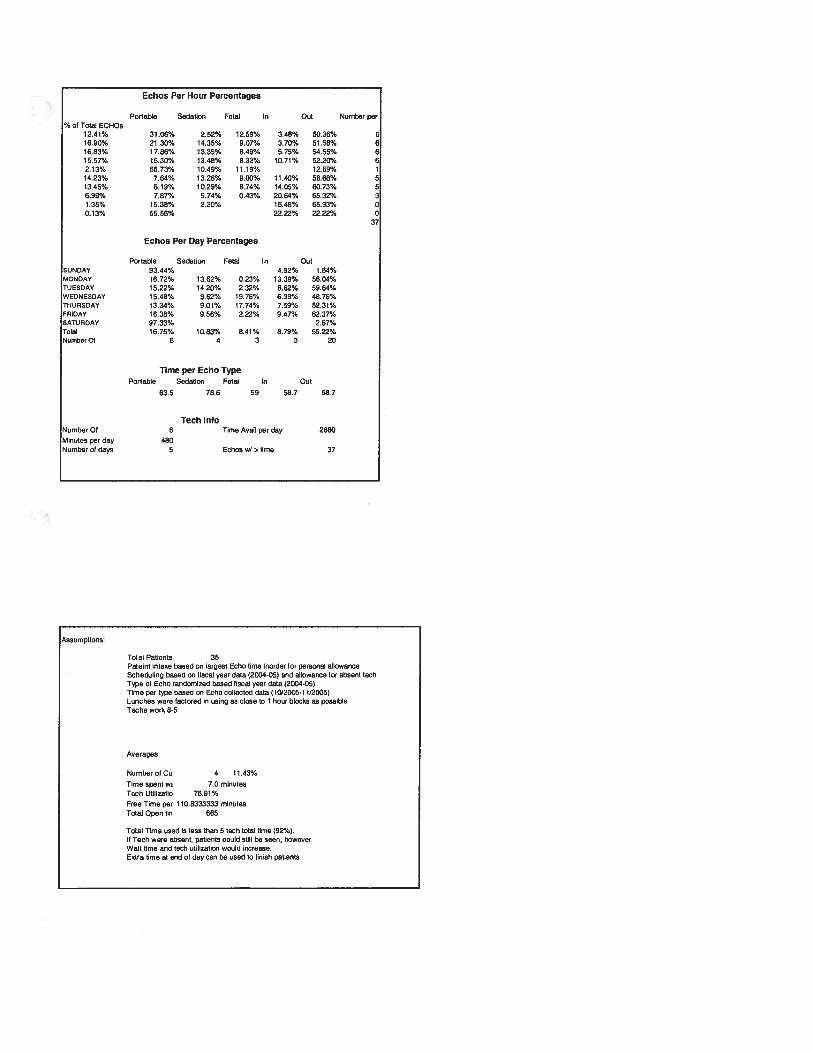
Echos Per Hour Percentages
Portable Sedation Fetal In Out Number per% ot Total ECHOS
12.41% 31.06% 2.52% 12.59% 3.48% 50.36% 516.90% 21.30% 14.35% 9.07% 3.70% 51.58% 616.83% 17.86% 13.35% 8.49% 5.75% 54.55% 615.57% 15.30% 13,48% 8.32% 10.71% 52.20% 62.13% 65.73% 10.49% 11.19% 12.59%14.23% 7.64% 13.28% 9.00% 11.40% 58.68% 513.45% 6.19% 10.29% 8.74% 14.05% 60,73% 56.99% 7.87% 5,74% 0.43% 20.64% 65.32% 31.35% 15.38% 2.20% 16.48% 65.93% 00.13% 55.56% 22.22% 22.22% 0
37
Echos Per Day Percentages
Portable Sedation Fetal In OutSUNDAY 93.44% 4.92% 1.64%MONDAY 16.72% 13.62% 0.23% 13.39% 56.04%TUESDAY 15.22% 14 20% 2.32% 8.62% 59.64%WEDNESDAY 15.48% 962% 19.76% 6.39% 48 76%THURSDAY 13.34% 9.01% 17.74% 7.59% 52.31%FRIDAY 16.38% 9.56% 2.22% 9.47% 62.37%SATURDAY 97.33% 2.67%TetI 16.75% 10.83% 8.41% 8.79% 55.22%NU,nbnrOt 6 4 3 3 20
Time per Echo TypePortable Sedation Fetal In Out
63.5 78.6 59 58.7 58.7
Tech InfoNumber Of 6 Time Avail per day 2880
Minutes per day 480Number of days 5 Echos w/ s lime 37
Assumptions:
Total Patients 35Pateint intake based on largest Echo lime inorder or personal allowanceScheduhng based on fiscal year data (2004-05) and allowance tsr absent techType ot Ocho randomized based fiscal year data (2004-05)Time per type based on Echo collected data (10/2005.1112005)Lunches were factored in using as close 10 1 hour blocks as possibleTechs work 8-5
Averages
Number of Cu 4 11.43%
TIme spent wt 7.0 minutesTech Utilizatio 76.91%
Free Time per 110.8333333 minutesTotal Open tin 665
Total Time used is less than 5 tech total time (92%).It Tech were absent, patients could stilt be seen, howeverWait time and loch utilization would increase.Extra time at end of day can be used to finish patients
Simulation
58.758763558 763 558.758 756 758 758 778 658,758 763.558.758.778 658 763.558 758.778.658.7
58.758 7
58.758.758 758 758.758 778.658.758 758 758 758.7
TECHS1 2 3 4 5 6
Begins Ends Begins Ends Begins Ends Begins Ends Begins Ends Begins Ends8:00 859
8.00 8.598:00 9:04
8.00 8.598.00 9.04
900 9599:00 9:59
900 9’59
9:04 10:03
Tech Avail
Time 10
0 10 00 1o0 10 10 610 00 571 4 41
1 4 560 1
o 10 00 11 3 10 00 00 11 2 10 00 10 10 10 1
0 1
0 00 10 00 117o 601 4 560 560 560 610 639
3:00 3:59 0Totals 5 17 77.81%
TectiUlil 1065Ave Time Pahent wallstree
Tech Avail
Waiting? Time 1
0 00 10 00 10 10 1o 610 0
9:00 9:59 0 371 4 11 4 10 560 10 580 01 3 10 000 10 00 10 10 1
0 10 1
1:00 1:59 0 10 10 10 1o 82
2:00 259 0 6119 61
0 610 610 61
300 359 0 620
Totals 4 30 78 47%
Tech Util 103.3333333
#1
Scheduling based on Fiscal Year data with slight change to minimize patient wait time
Simulation TBCHS1 2 3 4 5 6 Waiting7
Time Scheduled Begins Ends Begina Enda Begins Ends Begins Ends Begins Ends Begins Ends8.00 58.7 8:00 859
63.5 8:00 9:045 58.7 8:00 8 59
63.5 8:00 9.0458.7 8:00 8:59
9:00 58.7 9.00 9:5958.7 9:00 9:5958.7 900 9:59
6 58.7 9:00 95958.7 9:04 10:03587 904 1003
1000 786 1000 1119
635 1000 11:045 587 1000 1059
587 10:00 10:5988.7 10.03 11:02
11:00 587 11:00 11.5958.7 t1:00 11.89
4 63.5 11:00 12:0478.6 11:02 12:21
1:00 587 100 15958.7 1:00 1:5963.5 1:00 2:04
6 58.7 1:00 1:59
58.7 1:00 1:59
58.7 1:00 1:592:00 58.7 2.00 2:59
58.7 2:00 2:5959 2:00 300
6 58.7 2:00 2:5958 7 2:00 3:00
59 2:04 3:03300 59 300 4.00
63 5 300 4.045 63.5 3:00 4.04
63 5 3.00 4.0458 7
#2
Time Scheduled8:00
5
9’OO
6
10:00
5
11.00
4
1:00
6
2.00
6
300
10:00 1059
11:00 11.59
1:00 159
904 10:23
10:03 11:02
10:00 10.59
11.00 12.04
100 2:19
2880
34
2880
7.5
10:00 11.04
1.00 1.59
2.00 259
300 3 59
1:00 1:59
200 2:592 00 2 59
2.19 3:383.00 359
300 359
10’OO 1059
11:00 12.19
11:00 11:59
1.00 1.59
200 259
3:00 3:59
Ave Time Patient waitsFree time
Tech AvailSimulation TECHS
1 2 3 4 5 6 Waiting? Time 0Time Scheduled Begins Ends Begins Ends Begins Ends Begins Ends Begins Ends Begins Ends 0
800 786 800 919 0 163.5 8.00 9.04 0 1
5 587 8:00 8:59 0 0587 8.00 859 0 1
59 600 900 0900 58 7 9.00 9 59 0 0
58.7 900 9 59 0 6163 5 9:00 10:04 0 0
6 58.7 9:00 959 0 42587 9:04 1003 1 4 158.7 919 10:18 1 19 1
10:00 58.7 10:00 10:59 0 1#3 58.7 10:00 10:59 0 57
587 10.00 10:59 0 565 59 10:03 11:03 1 3 1
59 10:04 1104 1 4 111.00 58.7 11:00 11:59 0 1
58.7 11:00 11:59 0 14 58.7 11:00 11:59 0 1
58.7 11.00 11:59 0 01.00 58,7 1:00 1:59 0 0
59 1:00 200 0 078.6 1:00 2.19 0 0
5 59 1:00 2.00 0 059 1:00 2:00 0 1
587 100 200 0 12:00 587 2:00 2:59 0 0
58,7 2:00 2:59 0 16 78.6 2:00 3:19 0
58.7 2:00 2:59 0 10158.7 2.00 2.59 0 61587 2:19 3:19 1 19 56
3:00 58.7 3:00 3:59 0 6163 5 300 404 0 56
5 587 3:00 3:59 0 3763 5 3:00 4:04 063.5 3:19 4:23 1 19 604 2880
Totals 6 68 79.03%11.3333333
Tech Util 100.6666667Ave Time Patient WaitsFree
Time Scheduled Begins Ends Begins Ends Begins Ends Begins Ends Begins Ends Begins Ends800 587 800 859 0 1
635 8.00 9:04 0 05 587 800 8:59 0 1
635 800 904 0 0587 8.00 859 0 1
900 587 900 959 0 1587 900 9:59 0 158.7 9.00 9:59 0 1
5 58.7 9.00 9.59 0 61587 9.04 10:03 1 4 0
1000 786 10:00 1119 0 41635 1000 11:04 0 56
#1 5 58.7 1000 1059 0 158,7 10:00 10:59 0 1587 10:03 11:02 1 3 0
1100 587 11:00 11:59 0 158.7 11.00 11.59 0 1
5 63.5 11:00 12.04 0 0587 11,00 11.59 0 1786 1104 12:23 1 4 0
100 587 100 159 (3 1587 100 1.59 0 1635 100 204 0 0
5 58.7 1.00 1.59 0 158.7 100 1 59 0 1
200 587 200 2:59 0 18158.7 200 2.59 0 1
59 2.00 300 0 05 58.7 200 259 0 1
58.7 2:00 300 0 03 00 59 3,00 4.00 0 60
63 5 3:00 404 0 56
5 63.5 3.00 4:04 0 56635 3:00 404 0 56587 3:00 359 0 61
Totals 3 11 645 2880
Tech Util 77,60%
107.53 66666667Ave Time Patient waits
free
652
77.36%12.5
With only 5 techs
Time Scheduled8:00
5
9:00
5
1000
5
11:00
5
1:00
5
2:00
5
3:00
5
With only S techs
Begins Ends Begins Ends Begins Ends Begins Ends Begins Ends Begins Ends58,7 8:00 8:59 0 178.6 8:00 9:19 0 4163.5 8:00 9:04 0 058.7 8:00 8:59 0 158.7 8:00 8:59 0 158.7 9:00 9:59 0 163.5 9:00 10:04 0 0635 9:00 10:04 0 058.7 9 00 9.59 0 6178.6 9:04 10:23 1 4 3755.7 10:00 10.59 0 155.7 10:00 10:59 0 1
78.6 10:00 11:19 0 4163.5 10:04 11:08 1 4 1
59 10:04 11:04 1 4 0587 11:00 11:50 0 1587 11:00 11:59 0 1635 11:00 12:04 0 0587 1108 1207 1 8 058.7 11:04 12:03 1 4 058.7 1:00 1:59 0 1587 1:00 1:59 058.7 1:00 1:59 0 163.5 1:00 1:59 0 158.7 1:00 2:04 0 5678.6 2:00 3:19 0 16158.7 2:00 2:59 0 1
58.7 2:00 2:59 0 158.7 2:00 2.59 0 158.7 2:00 2:59 0 175.6 3:00 4:19 0 4158.7 3:00 3:59 0 6158.7 3:00 3.59 0 61
59 3:00 4:00 0 6058.7 3:00 3:59 0 61
Totals 5 24 698
Tech Uhf 75.76%Ave Time Patient waitstree 116.3333333
lime ocneouieo I tlI1iJ I Mt
TECH 1begins Ends
TECH 2Begins Ends
TECH 3Begins Ends
TECH 4Begins Ends
TECH 5Begins Ends
TECH 6Begins Ends ralienl weang Ii me mating iijriuseo time
8.00 59 8.00 9:0058.7 8:00 8:5978.6 8:00 9:1978.6 8:00 9:19 4163.5 8:00 9:04
9:00 58.7 9:00 9:59 6158.7 900 9:59 158.7 9:00 9:59 178.6 9:04 10:23 1 478.6 9:19 10:38 1 19 22
10:00 58.7 10:00 10:5559 10:00 11:00
58.7 10:00 10:59 158.7 10:00 10:59 158.7 10:23 11:22 1 23 38
11:00 58. 11:00 11:5559 1100 12:0059 1100 12.00
58.7 11:00 11:59 163.5 11:00 12:04
12:001:00 68.7 1:00 1:59 1
58.7 1.00 1.59 158.7 1:00 1:59 1587 1:00 1:59 158.7 1:00 1:59 1
2:00 59 2:00 3:00 6063.5 2:00 3:04
59 2:00 3:0063.5 2:00 3:04 11658.7 2:00 2:59 1
3:00 58.7 3:00 3:59 6158,7 3:00 3:59 61
58.7 3:00 3:59 6158.7 3:00 3:59 61
59 3:04 4:04 ,___________ 1 4 56
2880
4.8
288050
Tech UhilAve Time Patient waits
Non-ECHO time
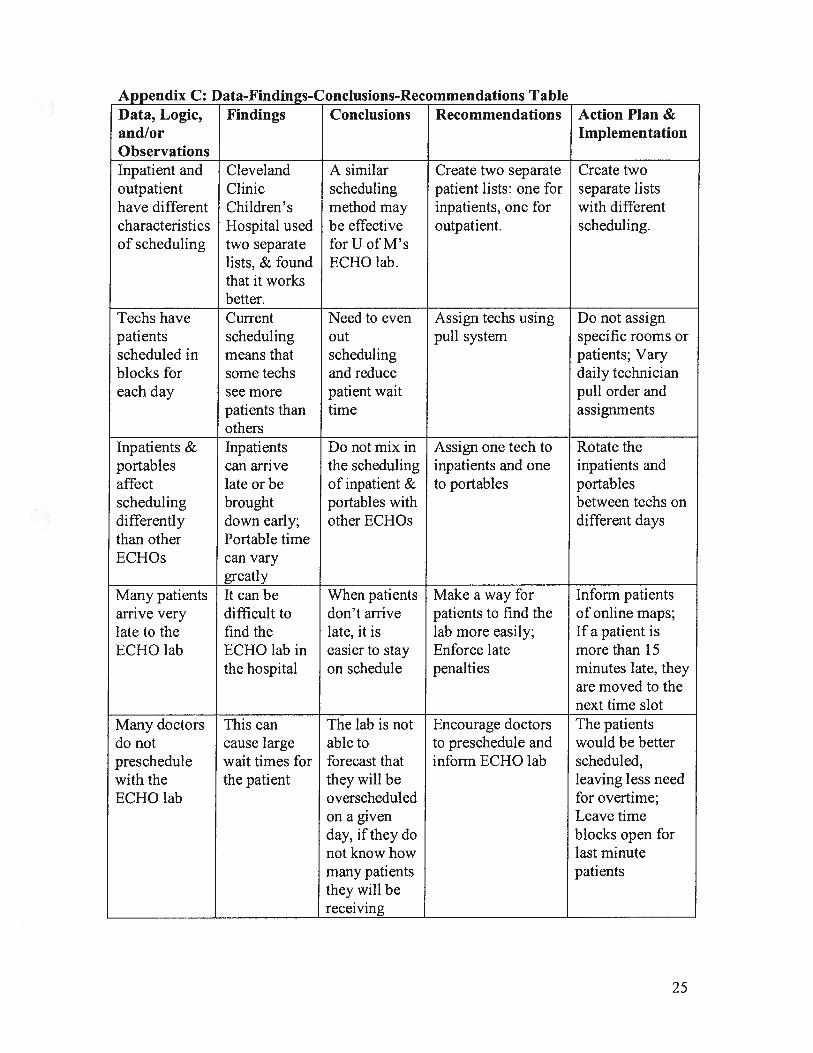
Appendix C: Data-Findings-Conclusions-Recommendations TableData, Logic, Findings Conclusions Recommendations Action Plan &and/or ImplementationObservationsInpatient and Cleveland A similar Create two separate Create twooutpatient Clinic scheduling patient lists: one for separate listshave different Children’s method may inpatients, one for with differentcharacteristics Hospital used be effective outpatient. scheduling.of scheduling two separate for U of M’s
lists, & found ECHO lab.that it worksbetter.
Techs have Current Need to even Assign techs using Do not assignpatients scheduling out pull system specific rooms orscheduled in means that scheduling patients; Varyblocks for some techs and reduce daily technicianeach day see more patient wait pull order and
patients than time assignmentsothers
Inpatients & Inpatients Do not mix in Assign one tech to Rotate theportables can arrive the scheduling inpatients and one inpatients andaffect late or be of inpatient & to portables portablesscheduling brought portables with between techs ondifferently down early; other ECHOs different daysthan other Portable timeECHOs can vary
greatlyMany patients It can be When patients Make a way for Inform patientsarrive very difficult to don’t arrive patients to find the of online maps;late to the find the late, it is lab more easily; If a patient isECHO lab ECHO lab in easier to stay Enforce late more than 15
the hospital on schedule penalties minutes late, theyare moved to thenext time slot
Many doctors This can The lab is not Encourage doctors The patientsdo not cause large able to to preschedule and would be betterpreschedule wait times for forecast that inform ECHO lab scheduled,with the the patient they will be leaving less needECHO lab overscheduled for overtime;
on a given Leave timeday, if they do blocks open fornot know how last minutemany patients patientsthey will bereceiving
25

Appendix D: Interview Questions
1. How long have you been working here as a techlnurse/administrator?2. What is the nature of your role in the lab?3. How has your role changed in that time (if it has)?4. What changes have you seen in the lab during that time?5. How many hours do you work a week?6. What days does your overtime occur on and when in the day does the overtime
occur?7. How many patients do you see in a day?8. How long on average do you spend with a patient?9. Do you feel there is a difference in how procedures are done depending on the
patient?10. Do you perceive a problem with the current system?11. What is the nature of the problem? (Their opinion)12. Do you have any resolutions for this?13. Are there days when patients are told they must come back later?14. Do you feel over or under worked?15. Please walk me through an average procedure.16. How do you feel about working different hours than 8-5, 5 days a week?17. What procedure must you go through when receiving a patient?18. What procedure must you go through when finishing with a patient?19. Do you need to go to anyone else for paperwork/approval/etc. when dealing with a
patient?20. How long does it take to reach the necessary parties when you must go for
approval/second opinion?21. How often must you sit and wait for inpatients when the lab is full (if you must
wait)?22. How long is the wait for inpatients on average?23. How often do you leave the lab for a procedure? How long does this take?
28
Appendix E: Data Collection Form
Name: Date:
Patient 1
Shift Start Time:
ECHO type
Shift End Time:
Patient In Time:Patient Out Time:Report Finished Time:
Patient 2 ECHO type
Patient In Time:Patient Out Time:Report Finished Time:
Patient 3
Patient In Time:Patient Out Time:Report Finished Time:
Patient 4
Patient In Time:Patient Out Time:Report Finished Time:
Patient 5
Patient In Time:Patient Out Time:Report Finished Time:
Patient 6
ECHO type
ECHO type
ECHO type
ECHO type
Patient In Time:
JOE 481 Team Project 5 Fall 2005Pediatric Cardiology ECHO Lab Analysis
27
Patient Out Time:Report Finished Time:
Patient 7
Patient In Time:Patient Out Time:Report Finished Time:
Patient 8
ECHO type
ECHO type
Patient In Time:Patient Out Time:Report Finished Time:
Patient 9
Patient In Time:Patient Out Time:Report Finished Time:
Patient 10
Patient In Time:Patient Out Time:Report Finished Time:
ECHO type
ECHO type
________
28
Appendix F: References
I Ashton A et al. (2005). A simulation-based study of a NHS Walk-in Centre. J Opi ResSoc 56: 153-161.
2 George SK et al. A simulation study to evaluate hospital operating room performance.http://students.washington.edu/ywl/Simulation%20study.pdf. Accessed November 2005
3 R. Hall, D. Belson, P. Murali, and M. M. Dessouky (Springer, 2006). Modeling PatientFlows through the Healthcare System. Delay Management in Health Care Systems.
4 Hashimoto F (1996). Improving outpatient clinic staffing and scheduling withcomputer simulation. J Gen Inter Med 11: 182-184.
5 Klassen K and Rohleder T (1996). Scheduling outpatient appointments in adynamic environment. J Opns Mng 14: 83-101.
6 Lane D, Monefeldt C and Rosenhead J (2000). Looking in the wrong place forhealthcare improvements: a system dynamics study of an accident and emergencydepartment. J Opi Res Soc 51: 518-531. Article.
29