Embed Size (px)
Citation preview

Tal Geva, MDTal Geva, MDDepartment of CardiologyDepartment of CardiologyChildren’s Hospital BostonChildren’s Hospital Boston
Overview of Progress in Overview of Progress in Pediatric CardiologyPediatric Cardiology
Food and Drug AdministrationFood and Drug AdministrationPediatric Advisory Subcommittee MeetingPediatric Advisory Subcommittee Meeting
February 3, 2004February 3, 2004

OutlineOutline
• Scope of congenital heart disease (CHD)Scope of congenital heart disease (CHD)
• Trends in CHD outcomesTrends in CHD outcomes
• Trends in managementTrends in management
• Trends in imaging of pediatric and adult CHDTrends in imaging of pediatric and adult CHD
• Gaps in knowledgeGaps in knowledge
Tal Geva 2/04

Scope of Congenital Heart DiseaseScope of Congenital Heart Disease
• AHA*: 8 per 1,000 live births (~40,000/year), AHA*: 8 per 1,000 live births (~40,000/year),
~10~1066 Americans currently living with CHD Americans currently living with CHD
• Hoffman and KaplanHoffman and Kaplan†† (review of 62 studies (review of 62 studies
published since 1955)published since 1955)::– – 4 to 50 per 1,000 live births4 to 50 per 1,000 live births– – Incidence depends primarily on number Incidence depends primarily on number
of small VSDs included in seriesof small VSDs included in series
– – Moderate and severe CHD: 6 per 1,000 Moderate and severe CHD: 6 per 1,000 without BAV and 19 per 1,000 with BAVwithout BAV and 19 per 1,000 with BAV
* www.americanheart.org/presenter.jhtml?identifier=1477* www.americanheart.org/presenter.jhtml?identifier=1477† † JACCJACC 2002;39:1890-9002002;39:1890-900 Tal Geva 2/04

Types of Congenital Heart DiseaseTypes of Congenital Heart Disease(median incidence per 10(median incidence per 1066 live births; excluding non-stenotic BAV and silent PDA) live births; excluding non-stenotic BAV and silent PDA)
VSD* 2,829
PDA 567
ASD 564
PS 532
Coarc 356
TOF 356
AVC 340
D-TGA 303
AS 256
HLHS 226* Excluding tiny VSDs
DORV 127
Truncus 94
Tri atresia 92
TAPVC 91
Single V 85
PA/IVS 83
Ebstein 40
All cyanotic 1,270
All CHD 7,699
BAV 9,244Tal Geva 2/04Source: JACC 2002;39:1890-900

Outcomes of CHD: MortalityOutcomes of CHD: Mortality
Source: Boneva et al. (CDC) Circulation 2001;103:2376-81Source: Boneva et al. (CDC) Circulation 2001;103:2376-81
• 1995-97: CHD contributed to 5822 deaths/year
Tal Geva 2/04

Outcomes of CHD: MortalityOutcomes of CHD: Mortality
Source: Boneva et al. (CDC) Circulation 2001;103:2376-81Source: Boneva et al. (CDC) Circulation 2001;103:2376-81
• 51% of deaths in infants; 7% in 1-4 years• ~19% higher mortality in blacks compared
with whites
Tal Geva 2/04

0
200
400
600
800
1000
1200
1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
0.00%
1.00%
2.00%
3.00%
4.00%
5.00%
6.00%
Mo
rta
lity
Pe
rce
nta
ge
Children’s Hospital Boston: CICU MortalityChildren’s Hospital Boston: CICU Mortality
Tal Geva 2/04

Source: Sadr et al. Am J Cardiol 2000;86:577-9
Despite an overall in mortality, some pockets of resistance persist…
Tal Geva 2/04

Outcomes of CHD: MorbidityOutcomes of CHD: Morbidity
Tal Geva 2/04
The majority of therapeutic interventions for The majority of therapeutic interventions for CHD do not lead to “cure”CHD do not lead to “cure”
• Residual anatomic abnormalitiesResidual anatomic abnormalities
• Residual hemodynamic abnormalitiesResidual hemodynamic abnormalities
• Neurodevelopmental abnormalitiesNeurodevelopmental abnormalities
• Social and insurability issuesSocial and insurability issues

Tal Geva 2/04
As survival of patients with CHD improved, As survival of patients with CHD improved, attention shifted from getting patients out of attention shifted from getting patients out of the hospital to improving their functional, the hospital to improving their functional, psychological, and social outcomes psychological, and social outcomes

Tal Geva 2/04
Neurodevelopmental OutcomesNeurodevelopmental Outcomes
D-TGAD-TGA
Circulatory arrest v. low-flow CPB trialCirculatory arrest v. low-flow CPB trialWypij et al. J Thorac Cardiovsc Surg 2003;126:1397Wypij et al. J Thorac Cardiovsc Surg 2003;126:1397

Tal Geva 2/04
S/p FontanS/p FontanNeurodevelopmental OutcomesNeurodevelopmental Outcomes
Source: Goldberg et al. J Ped 2000;137:646Source: Goldberg et al. J Ped 2000;137:646

Tal Geva 2/04
Neurodevelopmental OutcomesNeurodevelopmental Outcomes

Tal Geva 2/04
Dunbar-Masterson et al.Dunbar-Masterson et al.Circulation 2001;104:1138Circulation 2001;104:1138

Outcomes of CHD: MorbidityOutcomes of CHD: Morbidity
Tal Geva 2/04
• Residual anatomic abnormalitiesResidual anatomic abnormalities
• Residual hemodynamic abnormalitiesResidual hemodynamic abnormalities
• Neurodevelopmental abnormalitiesNeurodevelopmental abnormalities
• Social and insurability issuesSocial and insurability issues

Tal Geva 2/04
Even when we think treatment leads to cure…Even when we think treatment leads to cure…
22 year-old woman, s/p coarctation repair in infancy22 year-old woman, s/p coarctation repair in infancy

Tal Geva 2/04
Residual hemodynamic burden is common
S/p TOF repair
QuickTime™ and aSorenson Video 3 decompressorare needed to see this picture.

Tal Geva 2/04
Trends in Management of CHDTrends in Management of CHD

Tal Geva 2/04
Many variables account for the dramatic Many variables account for the dramatic progress in outcomes of CHDprogress in outcomes of CHD
• Better understanding of anatomy, embryology, Better understanding of anatomy, embryology, genetics, pathophysiology, and natural genetics, pathophysiology, and natural
historyhistory
• Improved diagnosisImproved diagnosis
• Support technology (e.g., cardiorespiratory Support technology (e.g., cardiorespiratory support and monitoring technology in the OR support and monitoring technology in the OR
and CICU, ECMO, mechanical assist and CICU, ECMO, mechanical assist devices)devices)
• Pharmacotherapy (e.g., pressors, ACE Pharmacotherapy (e.g., pressors, ACE inhibitors, inhibitors, -blockers, NO, Sildenofil, -blockers, NO, Sildenofil,
Bosentan)Bosentan)
• Surgical techniquesSurgical techniques
• Transcatheter therapyTranscatheter therapy

Tal Geva 2/04
Many variables account for the dramatic Many variables account for the dramatic progress in outcomes of CHDprogress in outcomes of CHD
• Better understanding of anatomy, embryology, Better understanding of anatomy, embryology, genetics, pathophysiology, natural historygenetics, pathophysiology, natural history
• Improved diagnosisImproved diagnosis
• Support technology (e.g., cardiorespiratory Support technology (e.g., cardiorespiratory support and monitoring technology in the OR support and monitoring technology in the OR
and CICU, ECMO, mechanical assist and CICU, ECMO, mechanical assist devices)devices)
• Pharmacotherapy (e.g., pressors, ACE Pharmacotherapy (e.g., pressors, ACE inhibitors, inhibitors, -blockers, NO, Sildenofil, -blockers, NO, Sildenofil,
Bosentan)Bosentan)
• Surgical techniquesSurgical techniques
• Transcatheter therapyTranscatheter therapy

Tal Geva 2/04
Trends in Surgical Management of CHDTrends in Surgical Management of CHD
— — Staged palliative Staged palliative approach with approach with emphasis on Rx. of emphasis on Rx. of symptomssymptoms
Early anatomic repair Early anatomic repair with emphasis on with emphasis on restoration of normal restoration of normal physiologyphysiology
— — Improved protection of vital organsImproved protection of vital organs• Circulatory arrest v. low-flow bypassCirculatory arrest v. low-flow bypass• Improved myocardial protectionImproved myocardial protection• Improved OImproved O22 delivery: pH stat v. delivery: pH stat v. stat stat
— — Minimally invasive surgeryMinimally invasive surgery• Video-assisted thoracoscopic surgeryVideo-assisted thoracoscopic surgery• Robotic surgeryRobotic surgery

Coarctation repair by Coarctation repair by robotic surgeryrobotic surgeryQuickTime™ and a
YUV420 codec decompressorare needed to see this picture.
Tal Geva 2/04

Tal Geva 2/04
Many variables account for the dramatic Many variables account for the dramatic progress in outcomes of CHDprogress in outcomes of CHD
• Better understanding of anatomy, embryology, Better understanding of anatomy, embryology, genetics, pathophysiology, natural historygenetics, pathophysiology, natural history
• Improved diagnosisImproved diagnosis
• Support technology (e.g., cardiorespiratory Support technology (e.g., cardiorespiratory support and monitoring technology in the OR support and monitoring technology in the OR and CICU, ECMO, mechanical assist and CICU, ECMO, mechanical assist
devices)devices)
• Pharmacotherapy (e.g., pressors, ACE Pharmacotherapy (e.g., pressors, ACE inhibitors, inhibitors, blockers, NO, Sildenofil, blockers, NO, Sildenofil,
Bosentan)Bosentan)
• Surgical techniquesSurgical techniques
• Transcatheter therapyTranscatheter therapy

Tal Geva 2/04
Transcatheter Management of CHDTranscatheter Management of CHD
• Valve and vessel stenosisValve and vessel stenosis— — balloon dilationballoon dilation— — stentsstents— — radiofrequency energyradiofrequency energy
• Occlusion proceduresOcclusion procedures— — ASD, VSD, PDA, collaterals, fistulaeASD, VSD, PDA, collaterals, fistulae— — variety of occluding devices and coilsvariety of occluding devices and coils
• Arrhythmia therapy (ablation)Arrhythmia therapy (ablation)
• Fetal interventionFetal intervention

Tal Geva 2/04
Cardiac Catheterization LaboratoryCardiac Catheterization Laboratory
Annual Case VolumeAnnual Case Volume

Tal Geva 2/04
Many variables account for the dramatic Many variables account for the dramatic progress in outcomes of CHDprogress in outcomes of CHD
• Better understanding of anatomy, embryology, Better understanding of anatomy, embryology, genetics, pathophysiology, natural historygenetics, pathophysiology, natural history
• Improved diagnosisImproved diagnosis
• Support technology (e.g., cardiorespiratory Support technology (e.g., cardiorespiratory support and monitoring technology in the OR support and monitoring technology in the OR and CICU, ECMO, mechanical assist and CICU, ECMO, mechanical assist
devices)devices)
• Pharmacotherapy (e.g., pressors, ACE Pharmacotherapy (e.g., pressors, ACE inhibitors, inhibitors, blockers, NO, Sildenofil, blockers, NO, Sildenofil,
Bosentan)Bosentan)
• Surgical techniquesSurgical techniques
• Transcatheter therapyTranscatheter therapy

EchoEchoUltrasoundUltrasound
BBM-modeM-mode 2D2D ColorColor 3D TDI3D TDI
AnatomyAnatomy FunctionFunctionMRIMRIMagnetic fields and RFMagnetic fields and RF
1940 1950 1960 1970 1980 1990 20001940 1950 1960 1970 1980 1990 2000
CathCathX-raysX-rays
DiagnosticDiagnostic InterventionalInterventional
Evolution of CHD ImagingEvolution of CHD Imaging
NuclearNuclearRadioactive tracersRadioactive tracers
CTCTX-raysX-rays
SPECTSPECT 99m99mTcTc PETPET
5 min/slice5 min/slice 400 msec/slice400 msec/slice
ThalliumThalliumRadiumRadium
Tal Geva 2/04

Tal Geva 2/04
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
Echo Cath MRI Nuclear
Imaging ProceduresImaging ProceduresChildren’s Hospital Boston, 2003Children’s Hospital Boston, 2003

Tal Geva 2/04
The excellent overall survival of patients The excellent overall survival of patients with CHD and the associated high rate of with CHD and the associated high rate of residual anatomic and functional residual anatomic and functional cardiovascular impairments result in a cardiovascular impairments result in a rapidly growing population of individuals rapidly growing population of individuals with a life-long need for surveillance that with a life-long need for surveillance that includes cardiac imagingincludes cardiac imaging

Tal Geva 2/04
Echocardiography LaboratoryEchocardiography Laboratory
Annual Case VolumeAnnual Case Volume

0
100
200
300
400
500
600
1995 1996 1997 1998 1999 2000 2001 2002 2003
Cardiovascular MRI ProgramCardiovascular MRI ProgramAnnual Case VolumeAnnual Case Volume
Tal Geva 2/04

Tal Geva 2/04
Safety Issues in Pediatric Cardiac ImagingSafety Issues in Pediatric Cardiac Imaging
• SedationSedation• Inherent risks of invasive dx. proceduresInherent risks of invasive dx. procedures• Ionizing radiation exposureIonizing radiation exposure• Contrast agentsContrast agents• RadiopharmaceuticalsRadiopharmaceuticals• Auditory traumaAuditory trauma• Pharmacological testingPharmacological testing• Improper use of imaging technology, Improper use of imaging technology,
including an unfavorable risk/benefit ratioincluding an unfavorable risk/benefit ratio

Tal Geva 2/04
Safety Issues in Pediatric Cardiac ImagingSafety Issues in Pediatric Cardiac Imaging
• SedationSedation• Inherent risks of invasive dx. proceduresInherent risks of invasive dx. procedures• Ionizing radiation exposure (cath, CT)Ionizing radiation exposure (cath, CT)• Contrast agents (cath, echo, CT, MRI)Contrast agents (cath, echo, CT, MRI)• Radiopharmaceuticals (nuclear medicine)Radiopharmaceuticals (nuclear medicine)• Auditory trauma (MRI)Auditory trauma (MRI)• Pharmacological testing (cath, echo, MRI, Pharmacological testing (cath, echo, MRI,
nuclear)nuclear)• Proper use of imaging technology, including a Proper use of imaging technology, including a
favorable risk/benefit ratiofavorable risk/benefit ratio

Tal Geva 2/04

Tal Geva 2/04
Estimated Lifetime Attributable Risk of Fatal CancerEstimated Lifetime Attributable Risk of Fatal Cancer in Pediatric CTin Pediatric CT
Age at CT ExaminationAge at CT Examination
Source: Brenner. Pediatr Radiol 2002; 32: 228Source: Brenner. Pediatr Radiol 2002; 32: 228
% Risk% Risk
0
0.02
0.04
0.06
0.08
0.1
0.12
0.14
0 10 20 30 40 50 60 70 80
Abdominal
Head

Brenner et al, 2003*Brenner et al, 2003*
“ “Above doses of 50-100mSv (protracted Above doses of 50-100mSv (protracted
exposure) or 10-50 mSv (acute exposure), direct exposure) or 10-50 mSv (acute exposure), direct
epidemiologic evidence from human populations epidemiologic evidence from human populations
demonstrate the exposure to ionizing radiation demonstrate the exposure to ionizing radiation
increases the risk of some cancer.”increases the risk of some cancer.”
www.pnas.org/cgi/doi/10.1073/pnas.2235592100www.pnas.org/cgi/doi/10.1073/pnas.2235592100Tal Geva 2/04

Tal Geva 2/04
Cancer Following Cardiac Cath in ChildhoodCancer Following Cardiac Cath in ChildhoodModan et al. Int J Modan et al. Int J ofof Epidemiology 2002;29:424 Epidemiology 2002;29:424
• 674 children; cath between 1950-1970674 children; cath between 1950-1970• 28.6% had >1 cath; mean age at cath 8.9628.6% had >1 cath; mean age at cath 8.96• Mean age at f/u 37.5 yearsMean age at f/u 37.5 years• Expected number of malignancies = 4.75Expected number of malignancies = 4.75• Observed number of malignancies = 11.0Observed number of malignancies = 11.0• Standardized incidence ratio = 2.3Standardized incidence ratio = 2.3
(95% CI (95% CI 1.2-4.1)1.2-4.1)• Of the 11 malignancies, 4 were lymphomas Of the 11 malignancies, 4 were lymphomas
and 3 were melanomasand 3 were melanomas

SummarySummary
• Advances in diagnosis and management of CHD
have led to a dramatic decline in mortality (<3%)
• Rapidly expanding population of patients with
CHD (currently 1-2 million and growing)
• Patients rarely cured; frequent anatomic and
hemodynamic abnormalities requiring surveillance
(e.g., imaging)
• use of transcatheter and minimally-invasive
surgical interventions that rely on image-guidanceTal Geva 2/04

SummarySummary
• Consequently, the number of cardiovascular
imaging procedures in patients with CHD will
continue to increase
• Urgent need for research in pediatric cardiac
imaging:
– safety and efficacy of radiopharmaceuticals
– cost-risk/benefit analysis of imaging strategies
– minimizing exposure to ionizing radiation
Tal Geva 2/04

Tal Geva 2/04
Thank YouThank You

Tal Geva 2/04
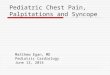
Nuclear Studies at CHB in 2003Nuclear Studies at CHB in 2003N= 515N= 515
Lung perfusionLung perfusion(n= 420; 82%)(n= 420; 82%)
Myocardial perfusionMyocardial perfusion(n= 92; 17.9%)(n= 92; 17.9%)
Shunt and EFShunt and EF(n= 3; 0.5%)(n= 3; 0.5%)

Children’s Hospital Boston 2003Children’s Hospital Boston 2003
23.2%
11.7%
27.8%
18.2%
7.7%2.0%
9.4%
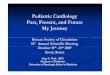
SEPTAL DEFECT:ASD Repair 10.4%VSD Repair 8.6%CAVC Repair 4.2%
CAVO-PULMONARY CONNECTION:Fenestrated Fontan 5.5%BDG 6.2%
SYSTEMIC OUTFLOW:Arterial switch operation 5.2%Coarctation repair 3.5%LVOTO 13.6%Norwood procedure 5.5%
PULMONARY OUTFLOW:Tetralogy of Fallot repair 7.9%Conduit placement / revision 4.5%Other RVOT reconstruction 5.8%
PDA Pacemaker/AICD
OTHER 8.4%Heart Tx 1.0%

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
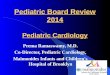
1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
CICU Age Distribution % 1992-2003
Neonate 1-12 Months 1-5 Years 5-10 Years >10 Years
Tal Geva 2/04