Embed Size (px)
Citation preview

PATHOPHYSIOLOGY OF LIPOPROTEIN(A) ATHEROSCLEROSIS, THROMBOSIS, AND MORE
Sergio Fazio, MD, PhDWilliam and Sonja Connor Chair of Preventive CardiologyProfessor of Medicine and Physiology & PharmacologyDirector of Preventive CardiologyKnight Cardiovascular InstituteOregon Health and Science University

Structure of Lipoprotein (a)
Leibundgut et al JACC 2012 and JLR 2013, Rao ATVB 2015

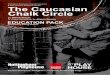
Apo(a) isoform distribution –Dallas Heart Study
Tsimikas S et al. Circulation 2009;119:1711–9
200
150
100
50
0100
755025
05040302010
011 13 177 9 19 21 2315 25 27 29 31 3533 37 4139
Number of kringles
Num
ber o
f sub
ject
s
Black
White
Hispanic
Lp(a
), nm
ol/L
100
7050
30
20
1012‒20 21‒26 27‒41
Number of kringles
Black
White
Hispanic

Mean Lp(a) concentration based on number of KIV repeatsLp
(a) m
g dL
–1
Number of KIV repeats11–16
70
10
30
40
20
50
0
60
17–19 20–22 23–25 26–28 29–31 32–34 35–37 >37
Low High
49 5260
Molecular weight of Apo(a)
1915 14 12
7 5
Kronenberg and Utermann J Int Med 2013;1:6–30

Prevalence of Elevated Lp(a) Levels Based on Distribution of Lipoprotein(a) Levels in the
Copenhagen General Population Study (6000 subjects)
Nordestgaard et al. European Heart Journal 2010:31;2844–2853
Lp(a) distribution in general population extrapolated from the graph
Lp(a) Level
Prevalence 20% 5% 1% 0.2% 0.02%
Number (US) 60,000,000 15,000,000 3,000,000 600,000 60,000
Number (EU) 100,000,000 25,000,000 5,000,000 1,000,000 100,000
Globally 1,400,000,000 350,000,000 70,000,000 14,000,000 1,400,000

Prevalence of Elevated Lp(a) Levels in 629,858 Subjects from a Referral Laboratory Population in the US
White et al AHA 2015
Health Diagnostic Laboratory referral dataset (2010-2014)
Median age 56. Both genders (54% women) Mean±SD = 31±38 mg/dL Median (IQR) = 15 (7-43) mg/dL Range = 0-571 mg/dL. Lp(a) percentiles:
75% >43 mg/dL 80% >55 mg/dL 90% >85 mg/dL 95% >109 mg/dL 99% >169 mg/dL
Lp(a) >30 mg/dL = 32nd percentile Lp(a) >50 mg/dL = 22nd percentile
6

Prevalence of Elevated Lp(a) Levels at a Tertiary Academic Medical Center
UCSD Database, Courtesy of Sam Tsimikas
7
43% of subjects referred to UCSD for dyslipidemia had Lp(a) >50 mg/dL

Genetic Determinants of CAD63,746 cases and 130,681 controls
Identified 46 loci and 104 independent variants for CADThe most significant are genes involved in lipid metabolism and inflammation
CARDIoGRAMplusCAD Consortium Nature Genetics Jan 2013
LPA Gene

Human, Chimp, Bonobo, Gorilla, Orangutan - KIV and KV
Baboon, Cynomolgus, Rhesus - KIV
European hedgehog - KIII
Leibundgut et al JLR 2013
Only human Lp(a) has immunoreactive OxPL
Lp(a) is Present in Humans, Apes and Monkeys, but the OxPL on Human Lp(a) is Unique to Humans Only

What Makes the Relationship Between Lp(a) and OxPL Uniquely Human?

Apo(a) secreted in the media contains OxPL, but only if KIV-10 is intact
Leibundgut et al JLR 2013

OxPL are present in purified human Lp(a) extracted with 2:1 chloroform:methanol
Leibundgut et al JLR 2013

Lp(a) and OxPL induce macrophage apoptosis
Koschinsky and Marcovina AJC 1998Seimon Cell Metabolism 2010

Hazard ratios for incident cardiovascular events per SD increase in log-transformed Lp(a) levels in the Atherosclerosis Risk In Communities (ARIC) study. Data are shown for African American (solid line) and Caucasian (dotted line) populations separately
Virani et al and Ridker et al Circulation 2012
Elevated Lp(a) as CVD risk factor
14
CVD
African American
Caucasian
CHD
African American
Caucasian
Stroke
African American
Caucasian
Hazard ratio per standard deviation increase in log-transformed Lp(a) levels
0.8 1.00.9 1.1 1.2 1.41.3
14

Evidence Base for Lp(a) as an Independent, Causal, Genetic Risk Factor for CVD
© 2015 DIA, Inc. All rights reserved.
Nonfatal MI and coronary death(9318 cases)
Ris
k ra
tio (9
5% C
I)
Usual Lp(a), Geometric Mean, mg/dL3 6 12 24 48 96 192
1.8
1.4
1.2
1.6
1.0
0.9
0.8
Adjustment for age and sex only Multivariableand KIV-2 adjusted
Hazard Ratio (95% CI)
P<.002
0.8 21 4
2 variant alleles
1 variant allele
0 variant alleles
Geometric Mean Lp(a) Lipoprotein (mg/dL)0 25 50 75 100 125
8.0
4.0
2.0
1.0
0.0
Odd
s ra
tio fo
r cor
onar
y di
seas
eLp(a)
mg/dL
>117
77‐117
30‐76
5‐29
<5
Erqou et al JAMA 2009:302:412-23 Kamstrup et al JAMA 2009:301;2331-9 Clarke et al NEJM 2009:361:2518-28

40% of patients reclassified to higher or lower risk category based on Lp(a) information

Is Lp(a) a Risk Factor In Patients On Long-Term Statin Therapy?
Tsimikas CV Endo Diab Obes 2016

Proposed Pathogenic Mechanisms for Lp(a)
Spence and Koschinsky (2012) ATVB 32:1550-1551; Koschinsky & Marcovina (2004) Curr. Opin. Lipidol. 15: 167-74

Change in Lp(a) with therapeutic agents
Tsimikas CV Endo Diab Obes 2016

Genetic Association of Lp(a) and Calcific AS
Thanassoulis G et al. NEJM 2013;368(6):503–512
20
Lp(a) SNP rs10455872
Genome wide significance
level

Risk of aortic valve replacement as a function of elevated Lp(a) levels
1 2 543Hazard ratio (95% CI) for
aortic valve stenosis
<22
22–66
67–89
90–95
Lp(a)percentile
>95
mg/dL
11 (7–17)
40 (30–51)
80 (63–95)
3 (2–4)
124 (104–148)
Participantsn
13,053
6,677
1,728
6,123
1,435
Eventsn
127
87
27
53
30
Age and sex adjusted
Trend: p<0.001
1 2 543Hazard ratio (95% CI) for
aortic valve stenosis
Multivariable adjusted
Trend: p<0.001
1. Kamstrup PR et al. J Am Coll Cardiol. 2013 Oct 10. doi: 10.1016/j.jacc.2013.09.038. [Epub ahead of print]
Lp(a): lipoprotein(a); CI, confidence interval; HDL, high density lipoproteinAnalyses were adjusted for age and sex, or multivariable adjusted additionally for total cholesterol, HDL cholesterol, systolic blood pressure, smoking, and diabetes; Lp(a) in mg/dL is shown as median (interquartile range)
Total: 29,026 324--(1.1%)--

Lp(a) and OxPL-apoB Levels Predict Progression of Aortic Stenosis
22
Capoulade et al. JACC 2015

Risk of Rapid AS Progression According to Levels of Lp(a) and OxPL-apoB
23
Capoulade et al JACC 2015

Statins do not improve progression of aortic valve disease
24
Hung and Tsimikas Curr Opin Lipid 2014

Clinical Event Rates: AVR or CV death
Models adjusted for age, male gender and baseline Vpeak
Capoulade et al. JACC 2015

Change in Lp(a) and OxPL-apoB Levels from Baseline to 1-year with Rosuvastatin in ASTRONOMERPotential Explanation of the failure of statins in AS
26
Capoulade et al. JACC 2015

Clin Chem 2010; 8: 1252-1260
Lp(a)

Lancet Diabetes Endocrinol 2013; 1: 220-227

Kamstrup & Nordestgaard. Lancet Diabetes Endocrinol 2013; online August 27
Instrumental Variable Analysis

Association of Lp(a) levels with incident T2D and CHD in the EPIC-Norfolk study
Lp(a): lipoprotein(a); CHD, coronary heart disease; T2D, type 2 diabetes; Confidence intervals (CIs) were calculated using a floating absolute risk technique; Hazard ratios were adjusted for age as underlying timescale, sex, BMI, alcohol, smoking status, systolic and diastolic blood pressure, physical activity, education level, and family history of diabetes (only for T2D) or family history of CHD (only for CHD);
2.0
1.5
1.0
0.5
0.0
Ha
zard
ra
tio
(95%
CI)
1 2 3 4 5 6 7 8 9 10
Decile of baseline Lp(a) levels
(2–3.9) (3.9–5.3) (5.3–7.1) (7.1–9.1) (9.1–11.6) (11.6–15.4) (15.4–21.8) (21.8–35.4) (35.4–53.5) (53.5–175.0)Lp(a)mg/dL
Ye Z et al. Diabetes 2013 Oct 2.
30
: CHD; : T2D

Risk of T2DM with Lp(a) concentrations below vs above 10 mg dL–1
31
Incident WHS(1670/25076)
2.5
1.0
1.5
0.5
0.0
2.0
Prevalent WHS(797/25076)
Prevalent WHS(419/9233)
Risk for T2DM for individuals with Lp(a) <10 mg dL–1 versus ≥10 mg dL–1
1.57(1.23–2.01)
HR
2.29(1.59–3.28)
OR1.54
(1.14–2.08)OR
Kronenberg and Uterman J Int Med 2013;1:6–30
31

Lp(a)LDLapo(a)
assembly
LDL‐receptorsPlasminogen receptors
PCSK9 inhibitors
Model for receptor-mediated catabolism of apo(a) and Lp(a)
From Romagnuolo R et al. J Biol Chem 2015;290:11649‐62
Supraphysiological levels
LDL

AIM-HIGH: Lp(a) remains a predictor of CVD events in patients with LDL-C of 54 mg/dl
Albers et al JACC 2013
33
Statin + placebo Statin plus niacin
Q4 of Lp(a): >125 nmol/L (50 mg/dL)

Effect of Alirocumab on Lp(a) levels150 mg Q2W on Lp(a)
All patients Baseline
Lp(a) >30 mg/dLn=51n=31n=102n=74
Median (Q1:Q3) % change from baseline, mITT population
‐30.3% (‐50.0, ‐19.4)
‐0.3% (‐16.7, 11.5)
‐28.3% (‐37.1, ‐19.4)
‐4.4% (‐15.3, 10.8)
BaselineLp(a) ≤30 mg/dL
n=43 n=51
‐37.5% (‐57.1, ‐7.4)
0.0% (‐16.7, 17.2)

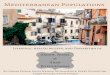
R‐square: 0.0463Spearman’s correlation coefficient: 0.2236p=0.0298
50
0
‐100
Lp(a) %
cha
nge from
baseline
‐40
LDL‐C % change from baseline
‐50
‐80 ‐60
FitIndividual measurements 95% prediction limits95% confidence limits
Lp(a) change from baseline (%) vs. LDL-C change from baseline in alirocumab treatment group

R‐square: 0.0463Spearman’s correlation coefficient: 0.2236p=0.0298
50
0
‐100
Lp(a) %
cha
nge from
baseline
‐40
LDL‐C % change from baseline
‐50
‐80 ‐60
FitIndividual measurements 95% prediction limits95% confidence limits
Lp(a) change from baseline (%) vs. LDL-C change from baseline in alirocumab treatment group

Reduction in Lipoprotein(a) With PCSK9Monoclonal Antibody Evolocumab

Correlation between Lp(a) and LDL-C changes induced by Evolocumab

Correlation between Lp(a) and LDL-C changes induced by Evolocumab

CETP Inhibitor Anacetrapib
ParameterLS Mean Percent (95% CI) Placebo-Adjusted
Change from Baseline
Week 24 Week 76
Non-HDL-C -31.7* (-33.6, -29.8) -29.4* (-31.6, -27.3)
Apo B -21.0* (-22.7, -19.3) -18.3* (-20.2, -16.4)
Apo A-1 44.7* (42.8, 46.5) 42.3* (40.5, 44.1)
TC 13.7* (12.0, 15.3) 15.6* (13.8, 17.3)
TG -6.8 (-9.9, -3.9) -5.3 (-8.9, -1.7)
Lp(a) -36.4 (-40.7, -32.3) -38.8 (-44.5, -33.9)
ApoE 29.2* (24.7, 33.7) 35.3* (30.6, 40.1)
*p<0.001; mean for all variables except for triglyceride and lipoprotein(a), for which median is shown