Embed Size (px)
DESCRIPTION
pictotrans - julie, gabsy, toy, mia (with labels!! ^_^)
Citation preview

PATHOLOGY OF THE BREAST AND THE MALE GENITAL TRACTpictotrans - prepared by julie, gabsy, toy, & mia

DISCLAIMER All the slides are available for viewing in Pathology Department. Structures and labels found in the succeeding photomicrographs are all based on the transcribers interpretation of microscopic findings as indicated in the case described.The labeling of the photomicrographs were all done by the transcribers, mistakes might be present. Feel free to make corrections.

GYNECOMASTIA
A 38-year-old male noted a palpable non-painful mass on his right breast. There are no other symptoms noted. Physical Examination a non-tender, fairly circumscribed 1.5cm x 1.5cm mass on the lower outer quadrant. He underwent core needle biopsy of the mass.
The specimen submitted consisted of several cream-white to yellow soft tissue strips with an aggregate diameter of 0.8cm.
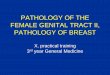
Microscopic sections showed mammary ducts lined by single to stratified epithelium. The epithelial cells are regular cooking and composed to cuboidal to low columnar cells. No lobular formation is seen. Surrounding the ducts are fibrosis and hyalinization.
Key words: Hyalinization FibrosisKey concepts Terminal duct lobular unit Estrogen excess Male breast anatomy

LPOGynecomastia
mammary duct
blood vessels - not ducts!!!
note the surrounding fibrosis and hyalinization
No lobules present

LPOGynecomastia
mammary ductsagain,note the surrounding fibrosis and hyalinization
single layer of epithelium
No lobules present
HPO

photomicrograph downloaded from www.pathguy.com/lectures/breast.htm
mammary ducts
with surrounding fibrosis and hyalinization No lobules present
LPOGynecomastia

CHRONIC MASTITIS, NON-SPECIFICA 72-year-old woman felt a small lump in her left breast while
taking a bath. This was not accompanied by any other symptoms. She consulted at the OPD clinic where physical examination showed a 2cm x 2cm movable nontender nodule in the outer upper quadrant of her left breast. A core needle biopsy was done and was submitted to the surgical pathology section.
Grossly, the specimen consisted of few cream-grey elongated thin tissue fragments having an aggregate dimension of 1.2 x 0.5 x 0.4cm. All were submitted for processing.
Microscopically, sections show aggregates of small lymphocytes surrounding a small duct. In the immediate background is mild fibrosis. Other portions of the tissue samples show mature adipose tissues and blood vessels.
Key words Small lymphocytic infiltrates Fibrous breast parenchymaKey concepts Incidental/conincidental findings Non-specific findings Reactive changes

LPOChronic Mastitis
fibrous breast parenchyma

HPO of fibrotic parenchymaChronic Mastitis
fibrous tissue
note the elongated nuclei

LPOChronic Mastitis
lymphocytic infiltrates

HPO of lymphocytic infiltratesChronic Mastitis
lymphocytes

INVASIVE DUCTAL CARCINOMAA 65-year-old female was admitted for a non-healing ulcer on the
right breast. Three years before admission, she noted a small, non-tender, firm nodule in the upper outer right quadrant of her right breast. This was excised but the excision wound did not heal. On admission, there was a small, superficial ulcer in the upper outer quadrant about 2cm above the nipple. There was another 1cm diameter small, firm mass just lateral to the base of the ulcer. Excision biopsy was done.
The specimen consisted of a firm, reddish purple, 1.5cm diameter, rounded mass which was covered by a 2 x 1.6cm elliptical ulcerated skin flap. The cut surface retracted and presented yellowish-white granular gritty adipose tissue. The skin was markedly adherent to the underlying tissue.
Microscopically, the infiltrating irregular nests and cords of polyhedral cells have hyperchromatic nuclei and prominent nucleoli and contain ample eosinophilic cytoplasms. Tumor cells fill dilated ducts, may of which exhibit central necrosis (“comedones”). Dense sclerotic connective tissue surround tumor nests (tumor desmoplasia). A cribriform pattern may also be seen. A few normal breast acini are seen in the periphery.

INVASIVE DUCTAL CARCINOMA Key words Polyhedral cells in tumor nests Central necrosis (“comedones”) Tumor desmoplasiaKey concepts Hormones and carcinogenesis Grading and staging Tumor angiogenesisTips On scan, note the disorganized architecture and loss of lobularity.

central necrosis – comedones
dense sclerotic CT – tumor desmoplasia
LPOInvasive Ductal Carcinoma

Invasive Ductal CarcinomaHPO showing polyhedral
cells
Note:hyperchromatic nuclei prominent nucleoli eosinophilic cytoplasm

photomicrograph downloaded from www.pathguy.com/lectures/breast.htm
LPOInvasive Ductal Carcinoma
central necrosis – comedones
dense sclerotic CT – tumor desmoplasia

photomicrograph downloaded from www.pathguy.com/lectures/breast.htm
LPOInvasive Ductal Carcinoma
central necrosis – comedones
dense sclerotic CT – tumor desmoplasia

photomicrograph downloaded from www.pathguy.com/lectures/breast.htm
LPOInvasive Ductal Carcinoma
cribriform pattern

PHYLLODES TUMOR, LOW GRADEA 49-year-old female was admitted for a right breast mass. This
started as a small and painless mass 9 years ago and grew to its present size. On admission, there was a large, globular, movable, 10cm in diameter mass in the upper quadrant of the right breast. There was no palpable axillary lymph node. Simple mastectomy was done.
The specimen consisted of the right breast which, upon cutting, revealed a globular, well-circumscribed, doughy, pale, pearly-white, rubbery mass 8cm in diameter. The cut surface of the mass was bulging with a leaf-like clefts and excluded slimy material.
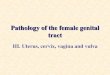
Microscopic sections revealed cystic and cleft-like spaces lined by cuboidal and myoepithelial cells. The stroma is rather cellular with spindle cells and congested vessels and has a sprinkling of lymphocytes. The stroma shows polypoid invaginations (stromal nodules) into the clefts and cysts.
Key words Cystic/cleft-like spaces Cuboidal epithelium Cellular stroma Polypoid invaginationsKey concept Mitotic (proliferative) index

LPOPhyllodes Tumor
we really don’t have an idea on this one… we can’t find a clear structure showing a “leaflike pattern”

photomicrograph downloaded from www.pathguy.com/lectures/breast.htm
LPOPhyllodes Tumor

INVASIVE LOBULAR CARCINOMAA 63-year-old menopausal call center agent felt an ill-defined
thickened area over the left breast. She noted mild tightness of the skin overlying the breast. She sought consult at the Breast Clinic where physical examination showed a 2 x 2cm “mass” in the upper inner quadrant of the left breast. Skin was dimpled and nipple retraction was noted. The “mass” was rubbery in consistency and tender on palpation. Biopsy was performed.
Gross, the specimen consisted of several tan brown, soft to firm,
irregularly shaped tissue fragments with an aggregate diameter of 2cm. All were submitted for processing.
Microscopically, sections showed an infiltrating carcinoma
composed of tumor cells arranged in “targetoid” fashion. Closer view shows that the tumor cells are disposed into “Indian files” dissecting and infiltrating breast stroma and adipose tissue. No ductal formations are seen.
On HPO, tumor cells are uniform in size. Nuclei are atypical and
hyperchromatic. Pleomorphism and mitotic activity are not pronounced.

INVASIVE LOBULAR CARCINOMA Key words “Targetoid” arrangement “Indian” filing Uniformly sized tumor cells
Key concepts Terminal Ductal-Lobular Unit of the Breast Lobular VS Ductal Carcinoma of the Breast

linear arrangement of cells“Indian” filing
LPOInvasive Lobular Carcinoma

linear arrangement of cells“Indian” filing
LPOInvasive Lobular Carcinoma

HPOInvasive Lobular Carcinoma
cells uniform in sizenuclei atypical and hyperchromatic

Invasive Lobular Carcinoma
HPO
infiltration of stroma

photomicrograph downloaded from www.pathguy.com/lectures/breast.htm
LPOInvasive Lobular Carcinoma
“Indian” filing

photomicrograph downloaded from www.pathguy.com/lectures/breast.htm
“Indian” filing
HPOInvasive Lobular Carcinoma
cells uniform in sizenuclei atypical and hyperchromatic

FIBROCYSTIC DISEASE
A 28-year-old female was seen for a right breast mass of 4 months duration which had been slowly enlarging. Examination showed a 2.5 diameter mass, slightly tender, firm, movable, with indistinct borders.
Grossly, the mass was 3cm in diameter, rubbery and round. Cut section showed cystic cavities (blue dome cysts) averaging 2cm in diameter.
Microscopically, multiple cystic ducts are lined by cuboidal to
columnar epithelium which is multilayered in some areas. They are flattened in the larger cystic areas and taller, apocrine-like in others. The stroma varies from loose to densely sclerotic.

FIBROCYSTIC DISEASE
Key words “Blue dome cysts” Cystic ducts (duct ectasia) Layered epithelium Apocrine metaplasia Sclerotic stromaKey concepts Hyperplasia Atypical hyperplasia Carcinoma-in-situ spectrumTips The spectrum of changes of fibrocytic disease (also called mammary
dysplasia) includes duct ectasia, apocrince metaplasia, sclerosis and adenosis
The degree of epithelial hyperplasia and papillomatosis correlates well with the risk of malignancy.

cystic ducts – duct ectasia
Fibrocystic DiseaseLPO

HPO of cystic ductFibrocystic disease
simple cuboidal epithelium

adenosis
LPO Fibrocystic disease
sclerotic stroma

Fibrocystic DiseaseHPO
Note:apocrine metaplasia -columnar epithelium-small nuclei-eosinophilic cytoplasm
Inspissated secretions / calcifications

Note:apocrine metaplasia -columnar epithelium-small nuclei-eosinophilic cytoplasm
HPO Fibrocystic disease

photomicrograph downloaded from www.pathguy.com/lectures/breast.htm
LPO Fibrocystic disease
cystic ectasia
adenosis
sclerotic stroma

FIBROADENOMAA 26-year-old female was seen at the OPD for a movable mass of two
weeks duration in the left breast. On examination, the mass was deeply seated, firm, tender, movable, and had a diameter of 3cm. Excision of the mass was done.
The specimen consisted of disc-shaped, well-demarcated, firm, 3.5 x 2.5 x 1.5 cm mass. The cut surface was slightly bulging, yellowish-white and had small whorls and empty pinhead-sized spaces.
Microscopically, the section shows large irregular areas of loosely arranged spindly cells and fine wavy connective tissue fibers enclosing oval, round and cleft-like spaces lined by heaped and compressed cuboidal epithelium. At the periphery of this mass is a thin rim of densely packed, hyalinized fibrous connective tissue outside of which is a histologically normal breast parenchyma
Key words Spindly cells/connective tissue Cleft-like spaces Cuboidal epitheliumKey concepts Neoplasia Hormonal influences on the tumorTips Note how the lobular architecture is preserved. Margins of the tumor are pushing
rather than infiltrating.

cleft-like spaces
FibroadenomaLPO

cleft-like spaces
FibroadenomaLPO

cleft-like spaces lined by compressed cuboidal epithelium
densely packed hyalinized fibrous connective tissue
HPO Fibrocystic disease

densely packed hyalinized fibrous connective tissue
photomicrograph downloaded from www.pathguy.com/lectures/breast.htm
LPO Fibroadenoma

SQUAMOUS CELL CARCINOMAA 57-year-old male was admitted for a mass involving the penis of
approximately one year duration. On physical examination, the penis was uncircumcised and there was a large fungating mass almost involving the entire glans penis. There was bilateral inguinal lyphadenopathy. Punch biopsy of the mass revealed squamous cell carcinoma. Amputation and bilateral inguinal dissection were performed.
Microscopically, the mass lesion consists of tumor cells, discernible as squamous in nature with attempts at keratinization and having intercellular bridges infiltrating the underlying tissue. Keratin pearls are present.
Key words Attempts at keratinization Keratin pearls Infiltration of the underlying tissueKey concepts Spread of squamous cell carcinoma Degree of differentiation of squamous cell carcinoma (grading)Tips Look for abundant pinkish cytoplasm (individual cell keratinization), keratin
pearls and intercellular bridges. Invasion is based on the extension of the tumor beyond the dermo-epithelial junction.

LPO Squamous Cell Carcinoma
Keratin pearlNeoplastic squamous cells

HPO of neoplastic squamous cellsSquamous Cell Carcinoma
Intercellular bridges
photomicrograph downloaded from www.udel.edu

densely packed hyalinized fibrous connective tissue
photomicrograph downloaded fromwww.ispub.com
Squamous cell carcinoma
Note the extension of the tumor beyond the dermo-epithelial junction (invasion)
extension of neoplastic squamous cells
Keratin pearl ( with squamous neoplasia)

LYMPHATIC FILARIASISThis is an incidental autopsy finding in a patient who died of shock
secondary to perforated peptic ulcer. On autopsy, the scrotum was literally transformed to a leather bag-
like sac which on cutting showed thickened walls encasing the testis. The spermatic cord was also thickened and firbrosed.
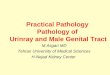
Microscopically, there is a focus of chronic granulomatous inflammation within which are cross-sections of calcified adult filariae worms. The adjacent lymphatic channels are dilated. Inflammatory cells are seen in the interstitial connective tissue. The seminiferous tubules are atrophic and surrounded by edematous interstitium likewise containing inflammatory cells.
Key words Dilated lymphatic channels Chronic granulomatous inflammation Adult filarial wormsKey concepts Host T-cell response to the filarial wormsTips The adult filarial worms inhabit the lymphatic channels. The microfilariae
immediately enter the blood stream upon their release.

Lymphatic Filariasis
adult filarial worm
photomicrograph downloaded fromwww.humpath.com

SEMINOMAA 40-year-old male consulted for an enlarging right scrotal mass of
three months duration. Physical examination revealed a well-circumscribed movable, doughy, slightly tender scrotal mass. An orchiectomy was performed.
The specimen was ovoid, well-circumscribed and measuring 7 x 5 x 5 cm. Cut surface was gray-yellowish, solid and homogenous. There was no grossly recognizable normal testicular tissue. The tunica albuginea appeared to be intact.
Microscopically, the tumor consists of poorly demarcated lobules separated by fibrous septa containing aggregates of lyphocytes. The tumor cells are polyhedral with abundant clear cytoplasm, well-defined cell margins and large central hyperchromatic nuclei. There are no residual seminiferous tubules noted.
Key words Lobules of tumor cells separated by fibrous septa containing
lymphocytes Clear cytoplasm, well-defined margins and central nucleusKey concepts Gonadal dysgenesis Histogenesis of germ cell tumors Seminoma vs. non-seminomatous germ cell tumors (NSGCT)Tips Note the uniform population of cells separated into lobules by delicate septa
containing lymphocytes. This is the classic picture of this germ cell tumor.

septa infiltrated with lymphocytes
LPOSeminoma
Note the uniform population of cells separated into lobules by delicate septa.

Seminoma photomicrograph downloaded fromupload.wikimedia.org
Polyhedral tumor cell with clear cytoplasm,
well-defined margin and central nucleus
and nucleoli
lymphocytes (the eosinophilic background is part of the extension of the
septa )

NODULAR PROSTATIC HYPERPLASIAA 55-year-old male as admitted for retention of urine. The patient
had been having diffiuculty starting urination since one year before admission. Catheterization of the bladder resulted in the evacuation of almost a liter of urine. Rectal examination revealed an enlarged, nodular and rubbery prostate. A transurethral resection prostatectomy was performed.
The specimen submitted consisted of multiple gray-tan prostatic chips 5 cm in aggregate diameter. Microscopically, the prostatic glands are of various sizes, some cystically dilated, and lined by two layers: inner columnar and outer cuboidal to flattened epithelium with intact basement membrane. The cells have small uniform nuclei and finely granular, homogenous cytoplasm. Aggregates of mononuclear cells are noted in the fibromuscular stroma.
Key words Dilated glands of various sizes Two layers of lining epitheliumKey concepts Glandular proliferation Fibromuscular proliferation Role of dihydrotestosteroneTips On scanning power, note how the lobularity of the architecture is preserved.
The fibromuscular stroma is abundant and the glands are more cystic. Look for the two cell layers of the lining epithelium. This implies the benign
nature of this lesion.

ScanningNodular Prostatic Hyperplasia
Note the prostatic glands of various sizes. The lobularity of the architecture is preserved. The firbromuscular stroma is abundant and the glands are more cystic.
Prostatic glands

HPONodular Prostatic Hyperplasia
Inner columnar cells
Outer cuboidal to flattened epithelium
Fibromuscular stroma

PROSTATIC ADENOCARCINOMAA 70-year-old male was admitted for difficulty in starting and
dribbling urination. Rectal examination showed a fixed, nodular, and stony-hard prostate, PSA level markedly elevated at 60ng/mL. A transurethral prostate biopsy showed malignancy. The patient underwent trasurethral resection prostatectomy and bilateral orchiectomy.
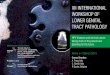
The specimen submitted consisted of several gray-yellowish, firm to hard prostatic chips, 6cm in aggregate diameter. Microscopically, the tumor is composed of closely-packed small sized glands as well as individual cells diffusely infiltrating the fibromuscular stroma.
Key words Closely-packed glands Diffuse cell infiltration of the stromaKey concepts Endocrinologic basis of prostate cancer Grading and stagingTips Note that the overall architecture is disorderly and haphazard. Glands in
prostatic carcinoma are lined by a single layer of epithelium; the outer basal layer of cells of hyperplastic glands is often absent. Observe that the glands tend to be small and tubular with scanty stroma.
Hallmark of malignancy: invasion-capsular, perineural, lymphatic/vascular.

ScanningProstatic Adenocarcinoma
Note that the overall architecture is disorderly and haphazard.

HPOProstatic Adenocarcinoma
Note the closely packed small-sized glands lined by a single layer of epithelium, as well as individual cells diffusely infiltrating the firbomuscular stroma.
Prostatic gland
Fibromuscular stroma

END OF TRANS