Embed Size (px)
Citation preview

23BLEEDING FROM THE LOWER GENITAL TRACT
A. Duncan and C. von Widekind
INTRODUCTION
In the first comprehensive English Languagetextbook on the subject, William Smellie, in his1752 Treatise on the Theory and Practise of Mid-wifery1, correctly identifies the atonic uterus as amajor cause of postpartum hemorrhage with hisstatement ‘This dangerous efflux is occasioned byevery thing that hinders the emptied uterus fromcontracting’. Although he refers to vaginal pack-ing with Tow or linen rags (dipped in astringentssuch as oxycrate, red tart wine, alum orSacchar-saturni), he does not specifically referto bleeding from the lower genital tract. Becausethis omission was repeated in subsequent yearsby many standard textbooks and reviews ofpostpartum hemorrhage, it is not surprising thatthe present evidence base is poor, and a 2005MESH search in PubMed of the NationalLibrary USA combining the terms ‘Postpartumhemorrhage’ AND ‘Lacerations’ OR ‘Rupture’NOT ‘Uterine rupture’ came up with only 28publications.
Maternal deaths specifically from lower geni-tal tract bleeding as the cause of postpartumhemorrhage are rare in the developed world.The 2000–2002 United Kingdom ConfidentialEnquiries2 reported only one death from thiscause. World-wide, no accurate figures exist,but it is likely that the numbers are significant,particularly where there is significant co-morbidity and a poorly resourced maternityinfrastructure3.
CLASSIFICATION
Possible sources of bleeding from the lowergenital tract include:
(1) Cervical tears;
(2) Vaginal tears (above and below the levatorani muscle, see Figure 1);
(3) Vulva and perineal tears;
(4) Episiotomies.
With the exception of cervical tears withoutvaginal extension, all of the above can lead toparavaginal hematomas, which in turn can bedivided into those above and below the levatorani muscle (Figure 1). Infralevator hematomasinclude those of the vulva, perineum, para-vaginal space and ischiorectal fossa. Supra-levator bleeding is more dangerous, as it is moredifficult to identify and control the source ofbleeding, and blood loss into the retroperitonealspace can be massive.
INCIDENCE
In the UK, postpartum hemorrhage of morethan 500 ml occurs in between 5 and 17% of alldeliveries and postpartum hemorrhage of morethan 1000 ml in 1.3% of deliveries.
Cervical tears
Minor cervical tears are common and are likelyto remain undetected. However, bleeding whichoccurs despite a well-contracted uterus and whichdoes not appear to be arising from the vaginaor perineum is an indication for examining thecervix. Numerous cases have been described ofwomen dying from hemorrhage due to a cervicaltear, following operative vaginal delivery.
Postpartum hematoma
Because there is no agreed definition, thereis no consensus as to the incidence. After
194
216Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:20:58
Color profile: Generic CMYK printer profileComposite Default screen

195
Bleeding from the lower genital tract
Figure 1 Paravaginal hematomas. (a) The hematoma lies beneath the levator ani muscle; (b) thehematoma lies above the levator ani and is spreading upwards into the broad ligament. H, hematoma;LA, levator ani, U, uterus; P, pelvic peritoneal reflection
217Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:20:59
Color profile: Generic CMYK printer profileComposite Default screen

spontaneous delivery, up to 50% of parturientsdevelop a minor self-limiting infralevator/vulvahematoma5. In contrast, the formation of a sig-nificant postpartum hematoma is an uncommonbut serious complication after delivery, with thereported incidence of around 1 in 500–700deliveries6. Major pelvic (supralevator) hema-tomas are rare, with widely varying reportedincidence of between 1 in 500 and 1 in 20 0007.
Episiotomy
An episiotomy can bleed heavily, and, althoughthere are no data on the incidence of hemor-rhage from this cause alone, observational stud-ies suggest that the relative risk of postpartumhemorrhage is increased four to five times if anepisiotomy is performed8.
RISK FACTORS
The major causes of postpartum hemorrhageare uterine atony, retained placental fragments,morbid adherence of the placenta and lowergenital tract lacerations. Data from the NorthWest Thames District of the UK (Table 1)reviewed the obstetric factors associated with ablood loss of more than 1000 ml and appor-tioned a relative risk to each factor4. Of these,assisted delivery (forceps or vacuum extrac-tion), prolonged labor, maternal obesity (andassociated large baby) and episiotomy weremost relevant to the risks of lower genital tracthemorrhage. It is worth noting that episiotomy,
with a relative risk of 5, carried the same weightas a cause of postpartum hemorrhage as didmultiple pregnancy and retained placenta.Rotational forceps are a particular risk factor forspiral vaginal tears9.
Coagulation disorders, if present, are likely tosignificantly increase the risk of lower genitaltract hemorrhage and hematoma and thereforeshould always be corrected where possible. Ifvaginal lacerations require repair in this situa-tion, the threshold for the use of a vaginal packshould be low.
PREVENTION
The three main areas in which risk can bereduced all require a proactive approach:
(1) Antenatal co-morbidities such as anemiaand diabetes should be treated so thatwomen entering labor are as healthy aspossible.
(2) A consistent proactive approach is requiredin both the first and second stages of labor.Active monitoring (partogram) and earlyintervention are essential where progress isinadequate or cephalic-pelvic disproportionis diagnosed. Coagulation defects (includ-ing iatrogenic defects due to anticoagulat-ion) should be corrected where possible(see Chapter 25).
(3) Postpartum, the early identification ofexcessive blood loss and a proactiveapproach to resuscitation/fluid replacementas well as identification of the source ofbleeding and stopping it, are vital.
Because operative delivery and episiotomy areboth significant risk factors for postpartumhemorrhage from the lower genital tract, effortsto reduce the incidence of both are likely toreduce the risk of hemorrhage. Where operativevaginal delivery is required, however, thena proper technique as described in standardtextbooks10 will reduce the risk of vaginal andcervical tears.
DIAGNOSIS
Careful and well-documented observation afterdelivery is imperative as the seriousness of
196
POSTPARTUM HEMORRHAGE
AntenatalRelative
risk IntrapartumRelative
risk
Placentaprevia
Obesity
13
2
Emergency Cesareansection
Assisted deliveryProlonged labor (> 12 h)Placental abruptionMultiple pregnancyRetained placentaElective Cesarean sectionMediolateral episiotomyPyrexia in labor
9
22
1355452
Table 1 Risk factors for postpartum hemorrhageand approximate increase in risk4
218Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:20:59
Color profile: Generic CMYK printer profileComposite Default screen

concealed or persistent low-grade blood loss canbe underestimated.
Bleeding, especially after instrumentalvaginal delivery, that occurs despite a well-contracted uterus and that does not appear tobe arising from the lower vagina or perineumis an indication for examination of the uppervagina and cervix. The characteristic feature ofbleeding from upper vaginal and cervical tears isa steady loss of fresh red blood.
Exclusion of upper vaginal and cervical tearsrequires examination in the lithotomy positionwith good relaxation, good light and properassistance7. A tagged vaginal tampon to absorbblood loss from the uterine cavity and the useof flat-bladed vaginal retractors will assist invisualizing the vaginal walls.
The cervix should always be examined wherethere is continuing bleeding despite a well-contracted uterus and also after use of allrotational forceps, which are associated with asignificant increase in the risk of upper vaginaland cervical tears11. The method for doing thisis to grasp the anterior lip with one ring forcepsand to place a second ring forceps at the2-o’clock position, followed by progressively‘leap-frogging’ the forceps ahead of one anotheruntil the entire circumference has beeninspected.
TREATMENT
Hemorrhage from the lower genital tract shouldalways be suspected when there is ongoingbleeding despite a well-contracted uterus.Generally, high vaginal or cervical tears requirerepair under regional anesthesia in theater.
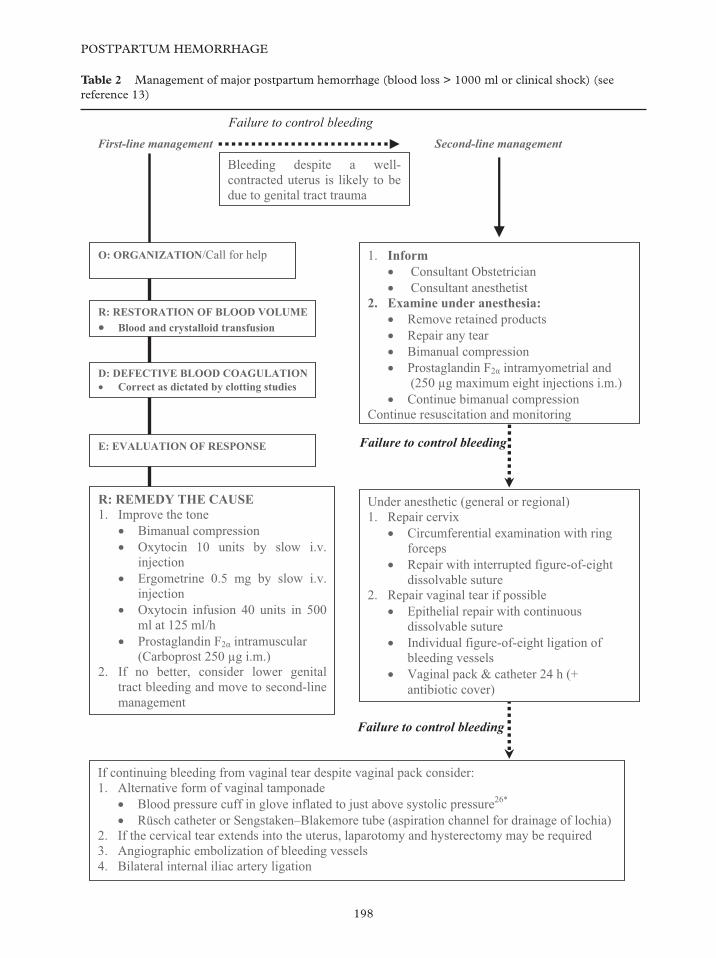
The Scottish Obstetrics Guidelines andAudit Project (SOGAP) group provides detailedguidelines on the management of postpartumhemorrhage12. A summary of the ORDERprotocol as described by Bonnar13 is shownin Table 2, with additional boxes relating tohemorrhage from the lower genital tract.
Perineal tear repair
The technique has been well described else-where14. The principles include ensuring thatthe first suture is inserted above the apex of thetear or episiotomy incision, use of a continuous
polyglactin/polyglycolic acid suture on a taper-cut needle, obliteration of dead spaces andtaking care that sutures are not inserted tootightly. If dead spaces cannot be closed securely,then a vaginal pack should be inserted.
Vaginal tear repair
The technique for repair of superficial vaginaltears is similar to that of perineal repair, asdescribed above. Use an absorbable, continuousinterlocking stitch, which must start and finishbeyond the apices of the laceration, and shouldwhere possible reach the full depth of the tearin order to reduce the risk of subsequenthematoma formation.
For deeper tears, an attempt should be madeto identify the bleeding vessel and ligate it.If there is any significant dead space or if thevagina is too friable to accept suturing, thenpacking is indicated (see below), because accessto deeper tears is usually difficult in an inade-quately anesthetized patient. Thus, repair ofsuch lacerations should be done in theater withadequate anesthesia.
Lacerations high in the vaginal vault andthose extending up from the cervix may involvethe uterus or be the cause of broad ligament orretroperitoneal hematomas. The proximity ofthe ureters to the lateral vaginal fornices, andthe base of the bladder to the anterior fornix,must be kept in mind when any extensive repairis undertaken in these areas. Poorly placedstitches can lead to genitourinary fistulas.Vaginal packing for at least 24 h is always wiseunder these conditions.
Vaginal packing using gauze is the mostcommon method to achieve vaginal tamponade.As with uterine packing, the technique ofvaginal packing involves ribbon gauze inserteduniformly side-to-side, front-to-back and top-to-bottom. Vaginal packing using thrombin-soaked packs, as described for uterine packing,can also be considered15, especially whereclosure of all lacerations has not been possible.
Because of the risk that the raw vaginal sur-face will bleed on removal of the pack, povidoneiodine-soaked double lengths of 4.5 × 48 inchpacks can be inserted inside sterile plasticdrapes (this has been well described for themanagement of uterine hemorrhage, but the
197
Bleeding from the lower genital tract
219Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:00
Color profile: Generic CMYK printer profileComposite Default screen
198
POSTPARTUM HEMORRHAGE
Failure to control bleeding
Failure to control bleeding
Failure to control bleeding
O: ORGANIZATION/Call for help
R: RESTORATION OF BLOOD VOLUMEBlood and crystalloid transfusion
1. InformConsultant Obstetrician
Consultant anesthetist 2. Examine under anesthesia:
Remove retained products Repair any tear Bimanual compression Prostaglandin F2 intramyometrial and
(250 µg maximum eight injections i.m.) Continue bimanual compression
Continue resuscitation and monitoring
D: DEFECTIVE BLOOD COAGULATIONCorrect as dictated by clotting studies
First-line management Second-line management
R: REMEDY THE CAUSE 1. Improve the tone
Bimanual compression Oxytocin 10 units by slow i.v. injection Ergometrine 0.5 mg by slow i.v.injection Oxytocin infusion 40 units in 500ml at 125 ml/h Prostaglandin F2 intramuscular
(Carboprost 250 µg i.m.) 2. If no better, consider lower genital
tract bleeding and move to second-line management
Under anesthetic (general or regional) 1. Repair cervix
Circumferential examination with ring forcepsRepair with interrupted figure-of-eight dissolvable suture
2. Repair vaginal tear if possible Epithelial repair with continuous dissolvable suture Individual figure-of-eight ligation of bleeding vessels Vaginal pack & catheter 24 h (+ antibiotic cover)
Bleeding despite a well-contracted uterus is likely to be due to genital tract trauma
E: EVALUATION OF RESPONSE
If continuing bleeding from vaginal tear despite vaginal pack consider: 1. Alternative form of vaginal tamponade
Blood pressure cuff in glove inflated to just above systolic pressure26*
Rüsch catheter or Sengstaken–Blakemore tube (aspiration channel for drainage of lochia) 2. If the cervical tear extends into the uterus, laparotomy and hysterectomy may be required 3. Angiographic embolization of bleeding vessels 4. Bilateral internal iliac artery ligation
Table 2 Management of major postpartum hemorrhage (blood loss > 1000 ml or clinical shock) (seereference 13)
220Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:01
Color profile: Generic CMYK printer profileComposite Default screen

principle is the same for vaginal packing) toallow for easy removal16. Generally, packs areleft in place for 24–36 h before removal17. Aurinary Foley catheter and broad-spectrumantibiotic cover should be given where packsare used. Balloon tamponade using Rüschcatheters18 or Blakemore-Sengstaken19 tubes,as described for treatment of uterine bleeding(see Chapters 28 and 29), can also be used.
Pinborg and colleagues20 described thesuccessful use of the blood pressure cuff intwo patients to control intractable vaginalbleeding following evacuation of vaginalhematoma that developed after spontaneousvaginal delivery. A blood pressure cuff wasinserted into a sterile glove, which in turn wasinserted into the vagina and the pressure thengradually increased to 120 mmHg, 10 mmHgabove the systolic pressure, to stop the bleeding.Eight hours later, the pressure of the cuffwas reduced by 10 mmHg/h and the cuff thentaken out after 32 h. Both patients made anuneventful recovery.
Cervical tear
Any cervical tear extending above the internalos warrants laparotomy. Small, non-bleedinglacerations of the cervix do not need to besutured. Any bleeding cervical tear, andcertainly any tear longer than 2 cm, however,should be sutured by using an absorbable sutureon a tapered (rather than a cutting) needle.A suitable method for suturing is shown inFigure 2.
Both edges of the most caudal part of thelaceration are grasped with a ring forceps andthen sutured with an interrupted or figure-of-eight stitch. This is then held with a hemostat tobring down into view the next part of the tear,which is sutured in the same way, and so onuntil the apex is secured. The laceration shouldbe observed for a few minutes after suturing, toensure adequate hemostasis. The ring forcepscan be replaced and left on for some time ifoozing persists.
Cervical and vaginal vault lacerations thatcontinue to ooze despite treatment as detailedabove or those that are associated with hema-tomas may be amenable to selective arterialembolization (see below).
199
Bleeding from the lower genital tract
Figure 2 (a)–(c) Suturing cervical tear
(b)
(c)
(a)
221Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp04 September 2006 17:20:15
Color profile: Generic CMYK printer profileComposite Default screen

Hematoma management
The literature on the management of para-genital hematomas is limited and no random-ized studies of the efficacy of various treatmentsexist21.
Infralevator hematomas
As always, initial management consists of resus-citation measures and analgesia followed by aperiod of observation. For hematomas that areless than 5 cm and not expanding, conservativetreatment with ice packs, pressure dressing andanalgesia is recommended22. The visible skinmargin of the hematomas should be markedto help establish whether it is expanding. Forhematomas that are expanding or more than5 cm in size, surgical intervention is recom-mended. Where possible, the surgical incisionshould be made via the vagina to minimizevisible scarring. Distinct bleeding points shouldbe under-run with figure-of-eight dissolvablesutures. The presence of any residual bleedingor a hematoma cavity is an indication forinsertion of a drain, a vaginal pack and a Foleycatheter, all of which should be left in placefor at least 24 h. Usually, however, no distinctbleeding point can be seen, in which case adrain and pack should be inserted10.
Supralevator hematomas
Approximately 50% of broad ligament hema-tomas present early with symptoms of lowerabdominal pain, hemorrhage and in severe cases,shock. The other 50% present after 24 h. Broadligament and retroperitoneal hematomas are ini-tially managed expectantly if the patient is stableand the lesions are not expanding23. Ultrasound,CT scanning and MRI may all be used to assessthe size and progress of these hematomas. Closeobservation, intravenous fluid resuscitation,blood transfusion, vaginal packing or balloon/blood pressure cuff tamponade and antibioticsare commenced as appropriate, but, if it is notpossible to maintain a stable hemodynamic state,then active intervention is indicated, with optionsincluding the following:
(1) Laparotomy ± total abdominal hysterectomyThis is indicated where there is any
possibility that a supralevator/broad liga-ment hematoma is due to a ruptured uterusor where a cervical tear appears to haveextended up into the uterus. At laparotomy,if there is continuing bleeding from theupper vagina, then the anterior division ofthe internal iliac artery should be ligated incontinuity, which will reduce the pulsepressure to the distal internal iliac arterybranches (that supply the uterus andvagina) by 85% and the blood flow byabout 50%24 (see Chapters 32 and 34). Afurther vaginal pack should be inserted.
(2) Selective arterial embolization Where thereis continuing expansion of a supralevatorhematoma without extension into the cervixor uterus, selective arterial embolization isseen as the treatment of choice25 over inter-nal iliac artery ligation, which in itself has anuncertain chance of success26 and involvesimposing a laparotomy on an already unsta-ble patient. The blood supply to the uppervagina is from a rich anastomotic networkof vessels, arising mainly from branches ofthe anterior trunk of the internal iliac artery(vaginal, uterine, middle rectal arteries) andthe internal pudendal artery, which is themost inferior branch of the posterior trunkof the internal iliac artery. The technique ofselective arterial embolization investigatesthese vessels by preliminary transfemoralarteriography, followed by embolizationusing Gelfoam (gelatin) pledglets. Pelageand colleagues25 reported a series of 35patients who underwent this procedurefor unanticipated postpartum hemorrhage.Bleeding was controlled in all but one,who required hysterectomy 5 days later forre-bleeding. All women who had successfulembolization resumed menstruation. Theprocedure, however, is not without risk anddeaths have been reported due to sepsis andmultiple organ failure27 (see Chapter 44).
SUMMARY
In summary, bleeding from the lower genitaltract should always be considered as a possiblecause of primary postpartum hemorrhagewhere there is continuing bleeding despite a
200
POSTPARTUM HEMORRHAGE
222Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:06
Color profile: Generic CMYK printer profileComposite Default screen

well-contracted uterus. Primary repair of vagi-nal or cervical tears with full-thickness suturesusing a dissolving suture on a taper-cut needle,followed by insertion of a vaginal pack andcatheter for at least 24 h will stem most bleed-ing. Urgent resort to laparotomy is necessary ifthere is a cervical tear extending beyond theinternal cervical os up into the uterus, or ifbleeding fails to settle despite an attempt atvaginal tamponade. Internal iliac artery ligationor selective arterial embolization should beconsidered where there is continuing expansionof a supralevator hematoma or upper vaginalbleeding despite the above measures. As always,regular assessments, clear documentation, aproactive approach and early intervention arevital to obtain a good outcome.
References
1. Smellie W. A Treatise on the Theory and Practice ofMidwifery, 1792
2. Millward-Sadler H. Why Mothers Die 2000–2002.The Confidential Enquiries into Maternal Deaths inthe United Kingdom. London: Royal College ofObstetricians and Gynaecologists, 2004:227
3. Etuk S, Asuqo E. Effects of community andhealth facility interventions on postpartumhaemorrhage. Int J Gynaecol Obstet 2000;70:381–3
4. Stones R, Paxton C, Saunders N. Risk factorsfor major obstetric haemorrhage. Eur J ObstetGynecol Reprod Biol 1993;48:15–18
5. Drife J. Management of primary postpartumhaemorrhage. Br J Obstet Gynaecol 1997;104:275–7
6. Hankins G, Zahn C. Puerperal haematomas andlower genital tract lacerations. In Hankins G,et al., eds. Operative Obstetrics. Connecticut:Appleton & Lange, 1995:57–72
7. Cheung TH, Chang A. Puerperal haematomas.Asia-Oceania J Obstet Gynaecol 1991;17:119–23
8. Combs C, Murphy E, Laros R. Factors associ-ated with postpartum hemorrhage with vaginalbirth. Obstet Gynecol 1991;77:69–76
9. Stones R, Paterson C, Saunders N. Risk factorsfor major obstetric haemorrhage. Eur J ObstetGynecol Reprod Biol 1993;48:15–18
10. James D, Steer P, Weiner C, et al. High-riskPregnancy Management Options, 2nd edn.London: WB Saunders, 1999:1187–204
11. Healy D, Quinn M, Pepperell R. Rotationaldelivery of the fetus: Kielland’s forceps and two
other methods compared. Br J Obstet Gynaecol1982;89:501–6
12. Management of Postpartum haemorrhage – AClinical Practice Guideline for Professionalsinvolved in Maternity Care in Scotland. Aberdeen:Scottish Programme for Clinical Effectiveness inReproductive Health, 1998
13. Bonnar J. Massive obstetric hemorrhage.Baillieres Best Pract Res Clin Obstet Gynaecol2000;14:1–18
14. Johanson R. Continuous vs. interrupted suturesfor perineal repair. In Keirse M, Renfrew M,Neilson J, Crowther C, eds. Pregnancy andChildbirth Module. The Cochrane Pregnancy andChildbirth Database. London: BMJ PublishingGroup, 1994
15. Bobrowski R, Jones T. A thrombogenic uterinepack for postpartum hemorrhage. Obstet Gynecol1995;85:836–7
16. Wax J, Channell J, Vandersloot J. Packing of thelower uterine segment: new approach to an oldtechnique? Int J Gynaecol Obstet 1993;43:197–8
17. Maier R. Control of postpartum haemorrhagewith uterine packing. Am J Obstet Gynecol 1993;169:317
18. Johanson R, Kumar M, Obhrai M, et al. Man-agement of massive postpartum haemorrhage:use of a hydrostatic balloon catheter to avoidlaparotomy. Br J Obstet Gynaecol 2001;108:420–2
19. Katesmark M, Brown R, Raju K. Successfuluse of a Sengstaken-Blakemore tube to controlmassive postpartum haemorrhage. Br J ObstetGynaecol 1994;101:259–60
20. Pinborg A, Bodker B, Hogdall C. Postpartumhaematoma and vaginal packing with a bloodpressure cuff. Acta Obstet Gynecol Scand 2000;79:887–9
21. Ridgway LE. Puerperal emergency. Vaginal andvulvar haematomas. Obstet Gynecol Clin NorthAm 1995;22:275–83
22. Zahn C, Yeomans E. Postpartum haemorrhage:placenta accrete, uterine inversion and puerperalhaematomas. Clin Obstet Gynaecol 1990;33:422
23. Lingam K, Hood V, Carty M. Angiographicembolisation in the management of pelvic haem-orrhage. Br J Obstet Gynaecol 2000;107:1176–8
24. Burchell R. Physiology of internal iliac arteryligation. J Obstet Gynaecol Br Commonwealth1968;75:642–51
25. Pelage J, Le Dref O, Jacob D, et al. Selectivearterial embolisation of the uterine arteries inthe management of intractable postpartumhaemorrhage. Acta Obstet Gynecol Scand 1999;78:698–703
201
Bleeding from the lower genital tract
223Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:06
Color profile: Generic CMYK printer profileComposite Default screen

26. Evans S, McShane P. The efficacy of internaliliac artery ligation in obstetric haemorrhage.Surg Gynecol Obstet 1985;160:250–3
27. Ledee N, Ville Y, Musset D, et al. Managementin intractable obstetric haemorrhage: an auditstudy on 61 cases. Eur J Obstet Gynecol ReprodBiol 2001;94:189–96
202
POSTPARTUM HEMORRHAGE
224Z:\Sapiens Publishing\A5211 - Postpartum Hemorrhage\Make-up\Postpartum Hemorrhage - Voucher Proofs #T.vp30 August 2006 14:21:06
Color profile: Generic CMYK printer profileComposite Default screen