Embed Size (px)
Citation preview
Mipoat
0
d
J Oral Maxillofac Surg69:747-753, 2011
Orthodontic Microsurgery for RapidDental Repositioning in
Dental MalpositionsDario Bertossi, MD,* Tomaso Vercellotti, MD,†
Andrea Podesta, MD,‡ and Pier Francesco Nocini, MD, DDS§
Purpose: Malposition of dental elements can be easily corrected when the patient is young; however,the opposite is true for adults. Middle-age patients normally request a rapid solution, but they usually alsohave associated pathologic features, such as advanced periodontal disease, dental migration, and anky-losis. Shortening the orthodontic treatment time is possible but not easy to achieve. We appliedpiezosurgical bone cuts to 10 patients affected by different dental malformations to determine the effectsof a shorter treatment time.
Materials and Methods: A total of 10 patients (8 women and 2 men) were treated using themonocortical tooth dislocation and ligament distraction technique. We included 5 patients with dentalankylosis (group A, with a range of 4 to 5 mm of dental intrusion into the bone), who presented withat least 4 elements included in the mandible, and 5 preoperative patients affected by maxillary hypoplasiaand transverse maxillary diameter reduction (group B, with a range of 6 to 8 mm measured at the firstmolar palatal cusp).
Results: Dental repositioning was achieved within 18 to 25 days for the dental intrusion group (groupA) and within 68 to 150 days for the preoperative group (group B). The average period was 20 days forgroup A and 100 days for both dental arches in group B. The decrease in orthodontic treatment time was70% for the ankylotic teeth and 65% for the preoperative group. We observed no periodontal or gingivaldamage, although all 10 patients experienced moderate edema and pain.
Conclusions: This method of shortening the orthodontic treatment time is simple, and performingosteotomic lines laterally and apically to the tooth radix on the bone has proved useful in reducing thetreatment time. In addition, the technique is very easy to use and has a low incidence of side effects.© 2011 American Association of Oral and Maxillofacial Surgeons
J Oral Maxillofac Surg 69:747-753, 2011otqhvtsbtwsrfwps
po
alposition of single dental elements plays a key rolen affecting occlusion. Multiple dental and skeletalroblems can severely influence facial esthetics. Therthodontic treatment of these defects can be easilyccomplished when the patient is young; however,he opposite is true for adults, for whom combined
*Associate Professor, Department of Maxillofacial Surgery, Uni-
versity of Verona, Verona, Italy.
†Assistant Professor, University of Chieti, Chieti, Scalo, Italy, and
Periodontist, Genova, Italy.
‡Private Practice, Genova, Italy.
§Head, Dental Clinic and Department of Maxillofacial Surgery,
University of Verona, Verona, Italy.
Address correspondence and reprint requests to Dr Bertossi:
Department of Maxillofacial Surgery, University of Verona, Piazzale
La Scuro 10, Verona 37134 Italy; e-mail: [email protected]
© 2011 American Association of Oral and Maxillofacial Surgeons
278-2391/11/6903-0019$36.00/0
aoi:10.1016/j.joms.2009.07.112
747
rthodontic surgical treatment is often necessary. Fur-hermore, patients 30 to 60 years of age usually re-uest a rapid solution to their problem but also oftenave associated pathologic features, such an ad-anced periodontal disease, dental migration in defec-ive areas, post-traumatic occlusal problems, ankylo-is, and/or the presence of fixed dental elementsecause of implant insertion. A certain number ofhese potential patients forgo orthodontic treatment,ith their decision influenced by the period neces-
ary for the appliance to be worn. In addition, theyequest rapid achievement of a good occlusion andacial esthetics using safe procedures and, possibly,ith reduced costs. This is even more important inlaces in which few people can afford medical orurgical treatment.
Therefore, the key for successful treatment of theseatients is to shorten the period required for orth-dontic treatment by way of a less invasive technique
nd at affordable costs. Many attempts to achieve a
aaob
evdalomtamnVtcam
eoft
748 RAPID DENTAL REPOSITIONING
decrease in the treatment time have been reported.1,2
However, the only effective technique to date hasbeen Wilkodontics—selective alveolar decorticationassociated with alveolar augmentation.3 The remark-ble accelerated orthodontic treatment they havechieved passes through surgery and takes advantagef the regional acceleratory phenomenon describedy Frost4 in 1989. The Wilkodontics technique also
uses bone grafting. Because orthodontics is a peri-odontal phenomenon that takes advantage of the dy-namics of resorption and apposition related to accel-erated bone turnover and the decrease in regionalbone densities, in the present study, we sought toapply a technique that could be an alternative to theWilkodontics technique and, at the same time, takeadvantage of the cell-mediated process in the peri-odontal ligament. Vercellotti5 introduced a device (Pi-zosurgery; Mectron Medical Technology, Sestri Le-ante GE, Italy) that, using microvibrations andedicated surgical tips, can produce very thin cuts insafe and selective way. In 2007, Vercellotti6 pub-
ished a report showing precisely how shortening therthodontic treatment time can be achieved usingonocortical tooth dislocation and ligament distrac-
ion. We selected 5 patients with dental malocclusionnd 5 with dental ankylosis of multiple dental ele-ents and used the microsurgical orthodontics tech-
ique with a prototype of an insert that we call aeronatip. We recorded the degree of inflammation,
iming, and the healing process to evaluate the de-rease in the orthodontic time, pain, and costs, andny possible side effects of this new surgical treat-ent.
Materials and Methods
A total of 10 patients (8 women and 2 men) weretreated using the monocortical tooth dislocationand ligament distraction technique and the Verona-tip. Of the 10 patients, 5 had dental ankylosis(group A, with a range of 4 to 5 mm of dentalintrusion into the bone), who presented with atleast 4 elements included in the mandible. Theremaining 5 were preoperative patients affected bymaxillary hypoplasia and transverse maxillary diam-eter reduction (group B, with a range of 6 to 8 mmmeasured at the first molar palatal cusp). The pre-treatment screening was performed by us, togetherwith 2 residents. We recorded the medical historyand used clinical analysis to exclude any majormetabolic pathologic findings. We studied the oc-clusion with the aid of casts, in which we designedand measured the osteotomy sites and analyzed theteeth position and desired post-treatment position.We used panoramic radiographs, cone-beam computed
tomography (Newtom, QR Verona, Italy), frontal andlateral conventional radiographs, and periapical ra-diographs with the O-ring technique to determinethe correct position of the osteotomy, monitor thepatient postoperatively for periodontal examina-tion, and to provide oral hygiene instructions.Cephalometric studies were performed accordingto the methods of Arnett and Bergman7 and Rick-tts8 and were normally combined to double checkur surgical planning. All patients provided in-ormed consent for the microsurgical orthodonticsechnique.
SURGICAL TECHNIQUE
Surgery was performed with the patient under localanesthesia (bupivacaine 1:100,000, 4 mL, plus ropiva-caine 7.5 mg, 4 mL) combined with intravenous se-dation (5 mg of midazolam in 100 mL of saline for 60minutes) after waiting 20 minutes for vasoconstric-tion to take effect. Dexamethasone 8 mg was given 1hour before surgery and 1 hour after surgery to avoidedema, and omeprazole 20 mg was prescribed oncedaily for 12 days. The gingival incision must be bev-eled above the papilla, with the scalpel positioned at45° with respect to the vestibular gingiva on thealveolar area, close to the teeth, and following eachteeth enamel margin to avoid retraction and boneresorption. Osteotomies were performed using thenew insert (horizontal and vertical osteotomies) andOT8 left and right tips (horizontal mandibular osteot-omies; Piezosurgery, Mectron Medical Technology).We performed only 1 full-thickness flap on the ves-tibular side. The selected cutting power for bonemust be set at 1 and the irrigation solution pump levelat 4. A vertical inverted Y corticotomy (the osteotomyalong the lateral margin of the ideal tooth radix posi-tion should be the longer part of the Y, with the apicalpart of the Y above the papilla) was performed topreserve the interproximal bone. The number andsite of the osteotomies varied with tooth form andposition. If intrusive movements had occurred, a cer-tain amount of apical bone was removed. If bone wasneeded for grafting, we harvested it using the OP3Piezosurgery insert from the apical area, over thetooth root. If the torque on some teeth needed to bechanged, we also performed osteotomies on the lin-gual side. We used 4 back-and-forth 4-0 Vicryl sutureson the vestibular side toward the palatal gingiva,deeper to the papilla to avoid retraction and thenused 5-0 nylon sutures to fix the papilla. Edema wasevaluated clinically by measuring the soft tissue thick-ness using a plicometer and photographs evaluated bythe surgeon and 2 residents at the postoperative fol-low-up visits. Edema was scored as light (�2 mm),moderate (2 to 4 mm), or severe (�4 mm). A buccalstraight wire technique was applied, and the ligament
distraction was obtained using palatal appliances of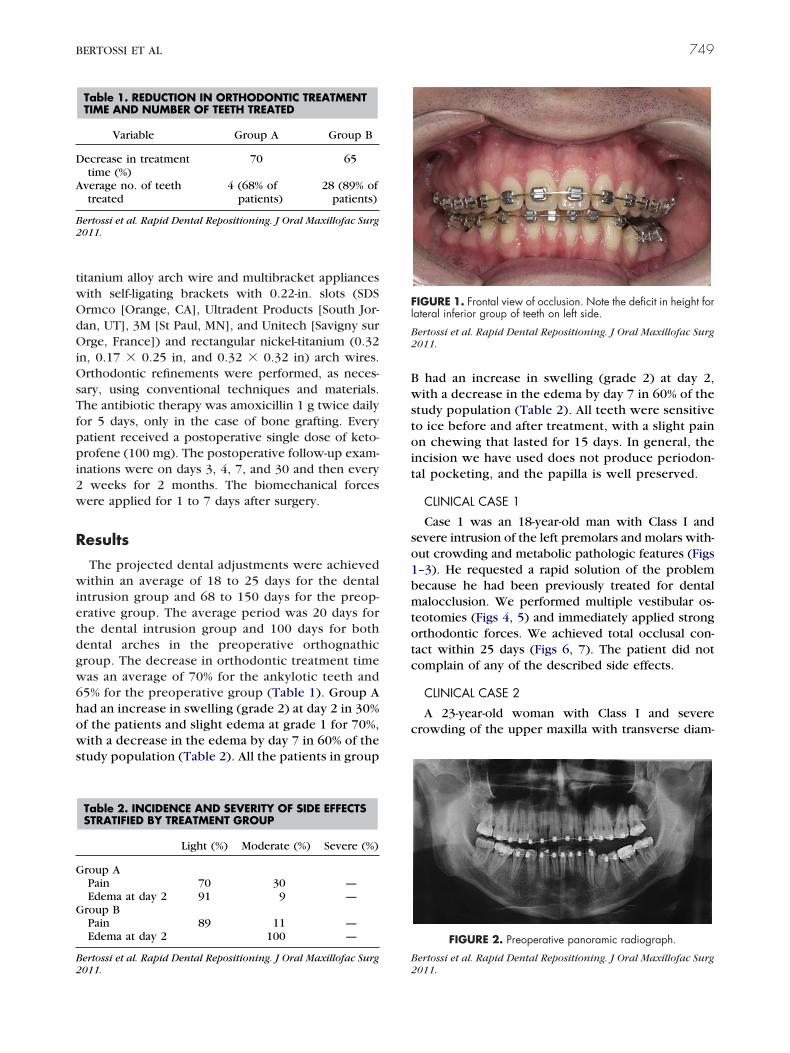
OsTfppi2w
1bmtotc
G
G
A
B
BERTOSSI ET AL 749
titanium alloy arch wire and multibracket applianceswith self-ligating brackets with 0.22-in. slots (SDSOrmco [Orange, CA], Ultradent Products [South Jor-dan, UT], 3M [St Paul, MN], and Unitech [Savigny surOrge, France]) and rectangular nickel-titanium (0.32in, 0.17 � 0.25 in, and 0.32 � 0.32 in) arch wires.
rthodontic refinements were performed, as neces-ary, using conventional techniques and materials.he antibiotic therapy was amoxicillin 1 g twice daily
or 5 days, only in the case of bone grafting. Everyatient received a postoperative single dose of keto-rofene (100 mg). The postoperative follow-up exam-
nations were on days 3, 4, 7, and 30 and then everyweeks for 2 months. The biomechanical forces
ere applied for 1 to 7 days after surgery.
Results
The projected dental adjustments were achievedwithin an average of 18 to 25 days for the dentalintrusion group and 68 to 150 days for the preop-erative group. The average period was 20 days forthe dental intrusion group and 100 days for bothdental arches in the preoperative orthognathicgroup. The decrease in orthodontic treatment timewas an average of 70% for the ankylotic teeth and65% for the preoperative group (Table 1). Group Ahad an increase in swelling (grade 2) at day 2 in 30%of the patients and slight edema at grade 1 for 70%,with a decrease in the edema by day 7 in 60% of thestudy population (Table 2). All the patients in group
Table 2. INCIDENCE AND SEVERITY OF SIDE EFFECTSSTRATIFIED BY TREATMENT GROUP
Light (%) Moderate (%) Severe (%)
roup APain 70 30 —Edema at day 2 91 9 —
roup BPain 89 11 —Edema at day 2 100 —
Bertossi et al. Rapid Dental Repositioning. J Oral Maxillofac Surg
Table 1. REDUCTION IN ORTHODONTIC TREATMENTTIME AND NUMBER OF TEETH TREATED
Variable Group A Group B
Decrease in treatmenttime (%)
70 65
verage no. of teethtreated
4 (68% ofpatients)
28 (89% ofpatients)
Bertossi et al. Rapid Dental Repositioning. J Oral Maxillofac Surg2011.
2011. 2
B had an increase in swelling (grade 2) at day 2,with a decrease in the edema by day 7 in 60% of thestudy population (Table 2). All teeth were sensitiveto ice before and after treatment, with a slight painon chewing that lasted for 15 days. In general, theincision we have used does not produce periodon-tal pocketing, and the papilla is well preserved.
CLINICAL CASE 1
Case 1 was an 18-year-old man with Class I andsevere intrusion of the left premolars and molars with-out crowding and metabolic pathologic features (Figs–3). He requested a rapid solution of the problemecause he had been previously treated for dentalalocclusion. We performed multiple vestibular os-
eotomies (Figs 4, 5) and immediately applied strongrthodontic forces. We achieved total occlusal con-act within 25 days (Figs 6, 7). The patient did notomplain of any of the described side effects.
CLINICAL CASE 2
A 23-year-old woman with Class I and severecrowding of the upper maxilla with transverse diam-
FIGURE 1. Frontal view of occlusion. Note the deficit in height forlateral inferior group of teeth on left side.
Bertossi et al. Rapid Dental Repositioning. J Oral Maxillofac Surg2011.
FIGURE 2. Preoperative panoramic radiograph.
ertossi et al. Rapid Dental Repositioning. J Oral Maxillofac Surg
011.
B
750 RAPID DENTAL REPOSITIONING
eter contraction (Figs 8, 9). She requested a rapidsolution of the problem because her wedding cere-mony was occurring soon. We performed multiplevestibular osteotomies and immediately appliedstrong orthodontic forces with the aid of internal andexternal orthodontic arches (Figs 10, 11). We alignedthe upper maxilla teeth within 105 days (Fig 12). The
FIGURE 3. Preoperative dental casts. Note the reduced contactbetween 2 dental arches.
Bertossi et al. Rapid Dental Repositioning. J Oral Maxillofac Surg2011.
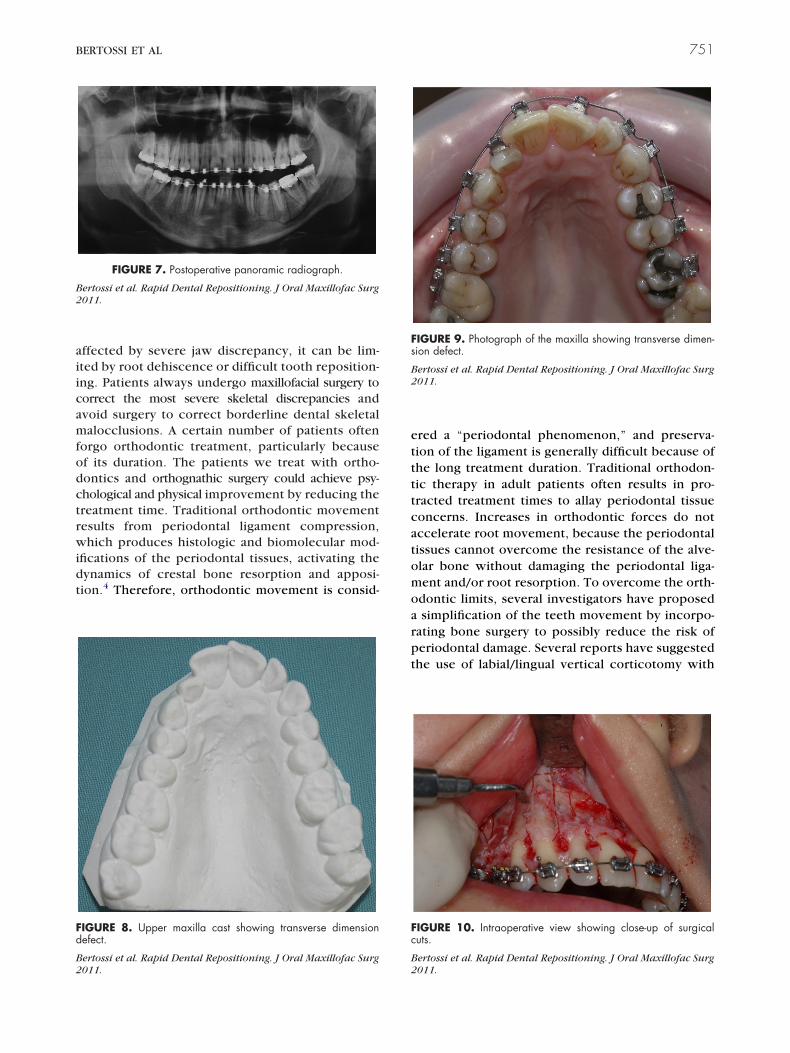
FIGURE 4. Intraoperative view showing close-up of surgical cutsclose to mentalis foramen.
Bertossi et al. Rapid Dental Repositioning. J Oral Maxillofac Surg
22011.patient did not complain of any of the described sideeffects.
Discussion
When we think of maxillomandibular surgery, wethink of patients requiring surgery because of vary-ing degrees of malocclusion that can be caused byseveral factors, including the spread of advancedperiodontal disease, dental migration toward areasof tooth loss, and tooth movement produced bytraumatic occlusal problems, as well as associatedcongenital skeletal disease. However, although manypatients come to us for functional reasons, they alsonaturally express concerns about what how theywill look postoperatively and how long the treat-ment will last before undergoing surgery. Althoughtraditional orthodontic therapy is the standard fortreating many adult dental malpositions, when ap-plied to patients with a thin skeletal biotype or
FIGURE 6. Frontal view of occlusion: final solution.
ertossi et al. Rapid Dental Repositioning. J Oral Maxillofac Surg
FIGURE 5. Intraoperative view showing close-up of surgicalcuts.
Bertossi et al. Rapid Dental Repositioning. J Oral Maxillofac Surg2011.
011.
BERTOSSI ET AL 751
affected by severe jaw discrepancy, it can be lim-ited by root dehiscence or difficult tooth reposition-ing. Patients always undergo maxillofacial surgery tocorrect the most severe skeletal discrepancies andavoid surgery to correct borderline dental skeletalmalocclusions. A certain number of patients oftenforgo orthodontic treatment, particularly becauseof its duration. The patients we treat with ortho-dontics and orthognathic surgery could achieve psy-chological and physical improvement by reducing thetreatment time. Traditional orthodontic movementresults from periodontal ligament compression,which produces histologic and biomolecular mod-ifications of the periodontal tissues, activating thedynamics of crestal bone resorption and apposi-tion.4 Therefore, orthodontic movement is consid-
FIGURE 7. Postoperative panoramic radiograph.
Bertossi et al. Rapid Dental Repositioning. J Oral Maxillofac Surg2011.
FIGURE 8. Upper maxilla cast showing transverse dimensiondefect.
Bertossi et al. Rapid Dental Repositioning. J Oral Maxillofac Surg
2011.ered a “periodontal phenomenon,” and preserva-tion of the ligament is generally difficult because ofthe long treatment duration. Traditional orthodon-tic therapy in adult patients often results in pro-tracted treatment times to allay periodontal tissueconcerns. Increases in orthodontic forces do notaccelerate root movement, because the periodontaltissues cannot overcome the resistance of the alve-olar bone without damaging the periodontal liga-ment and/or root resorption. To overcome the orth-odontic limits, several investigators have proposeda simplification of the teeth movement by incorpo-rating bone surgery to possibly reduce the risk ofperiodontal damage. Several reports have suggestedthe use of labial/lingual vertical corticotomy with
FIGURE 9. Photograph of the maxilla showing transverse dimen-sion defect.
Bertossi et al. Rapid Dental Repositioning. J Oral Maxillofac Surg2011.
FIGURE 10. Intraoperative view showing close-up of surgicalcuts.
Bertossi et al. Rapid Dental Repositioning. J Oral Maxillofac Surg
2011.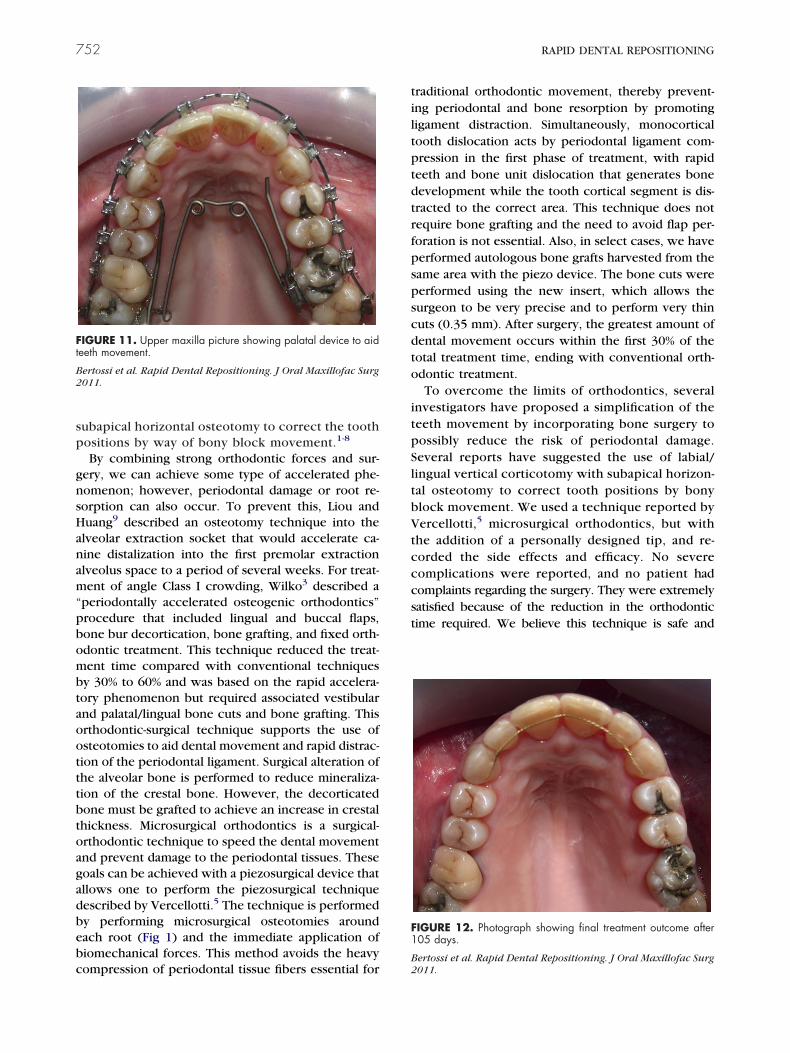
bebc
tiltptdtrfpspscdto
itpSltbV
752 RAPID DENTAL REPOSITIONING
subapical horizontal osteotomy to correct the toothpositions by way of bony block movement.1-8
By combining strong orthodontic forces and sur-gery, we can achieve some type of accelerated phe-nomenon; however, periodontal damage or root re-sorption can also occur. To prevent this, Liou andHuang9 described an osteotomy technique into thealveolar extraction socket that would accelerate ca-nine distalization into the first premolar extractionalveolus space to a period of several weeks. For treat-ment of angle Class I crowding, Wilko3 described a“periodontally accelerated osteogenic orthodontics”procedure that included lingual and buccal flaps,bone bur decortication, bone grafting, and fixed orth-odontic treatment. This technique reduced the treat-ment time compared with conventional techniquesby 30% to 60% and was based on the rapid accelera-tory phenomenon but required associated vestibularand palatal/lingual bone cuts and bone grafting. Thisorthodontic-surgical technique supports the use ofosteotomies to aid dental movement and rapid distrac-tion of the periodontal ligament. Surgical alteration ofthe alveolar bone is performed to reduce mineraliza-tion of the crestal bone. However, the decorticatedbone must be grafted to achieve an increase in crestalthickness. Microsurgical orthodontics is a surgical-orthodontic technique to speed the dental movementand prevent damage to the periodontal tissues. Thesegoals can be achieved with a piezosurgical device thatallows one to perform the piezosurgical techniquedescribed by Vercellotti.5 The technique is performed
y performing microsurgical osteotomies aroundach root (Fig 1) and the immediate application ofiomechanical forces. This method avoids the heavy
FIGURE 11. Upper maxilla picture showing palatal device to aidteeth movement.
Bertossi et al. Rapid Dental Repositioning. J Oral Maxillofac Surg2011.
ompression of periodontal tissue fibers essential for
raditional orthodontic movement, thereby prevent-ng periodontal and bone resorption by promotingigament distraction. Simultaneously, monocorticalooth dislocation acts by periodontal ligament com-ression in the first phase of treatment, with rapideeth and bone unit dislocation that generates boneevelopment while the tooth cortical segment is dis-racted to the correct area. This technique does notequire bone grafting and the need to avoid flap per-oration is not essential. Also, in select cases, we haveerformed autologous bone grafts harvested from theame area with the piezo device. The bone cuts wereerformed using the new insert, which allows theurgeon to be very precise and to perform very thinuts (0.35 mm). After surgery, the greatest amount ofental movement occurs within the first 30% of theotal treatment time, ending with conventional orth-dontic treatment.To overcome the limits of orthodontics, several
nvestigators have proposed a simplification of theeeth movement by incorporating bone surgery toossibly reduce the risk of periodontal damage.everal reports have suggested the use of labial/ingual vertical corticotomy with subapical horizon-al osteotomy to correct tooth positions by bonylock movement. We used a technique reported byercellotti,5 microsurgical orthodontics, but with
the addition of a personally designed tip, and re-corded the side effects and efficacy. No severecomplications were reported, and no patient hadcomplaints regarding the surgery. They were extremelysatisfied because of the reduction in the orthodontictime required. We believe this technique is safe and
FIGURE 12. Photograph showing final treatment outcome after105 days.
Bertossi et al. Rapid Dental Repositioning. J Oral Maxillofac Surg
2011.
BERTOSSI ET AL 753
allows a reduction in treatment time for adult patients,with a low biologic cost.
References1. Kole H: Surgical operation on the alveolar ridge to correct
occlusal abnormalities. Oral Surg Oral Med Oral Pathos 12:515,1959
2. Anholm JM, Crites DA, Hoff R, et al: Corticotomy-facili-tated orthodontics: Case reports. J Periodontol 61:34,1990
3. Wilko WM, Wilko MT, Ferguson DJ, et al: Accelerated orthodon-
tics with alveolar reshaping: Two case reports. J Orthop Pract11:63, 20004. Frost HM: The biology of fracture healing: An overview forclinicians. Part II. Clin Orthop Relat Res 248:294, 1989
5. Vercellotti T: Technological characteristics and clinical indica-tions of piezoeletric bone surgery. Minerva Stomatol 53:207,2004
6. Vercellotti T: Orthodontic microsurgery: A new surgicallyguided technique for dental movement. Int J Periodont RestoratDent 27:325, 2007
7. Arnett GW, Bergman RT: Facial keys to orthodontic diagnosisand treatment planning: Part I. Am J Orthod Dentofac Orthop103:299, 1993
8. Ricketts RM: New perspectives on orientation and their benefitsto clinical orthodontics—Part I. Angle Orthod 45:238, 1975
9. Liou EJ, Huang C: Rapid canine retraction through distraction of
the periodontal ligament. Am J Orthod Dentofac Orthoped 114:372, 1998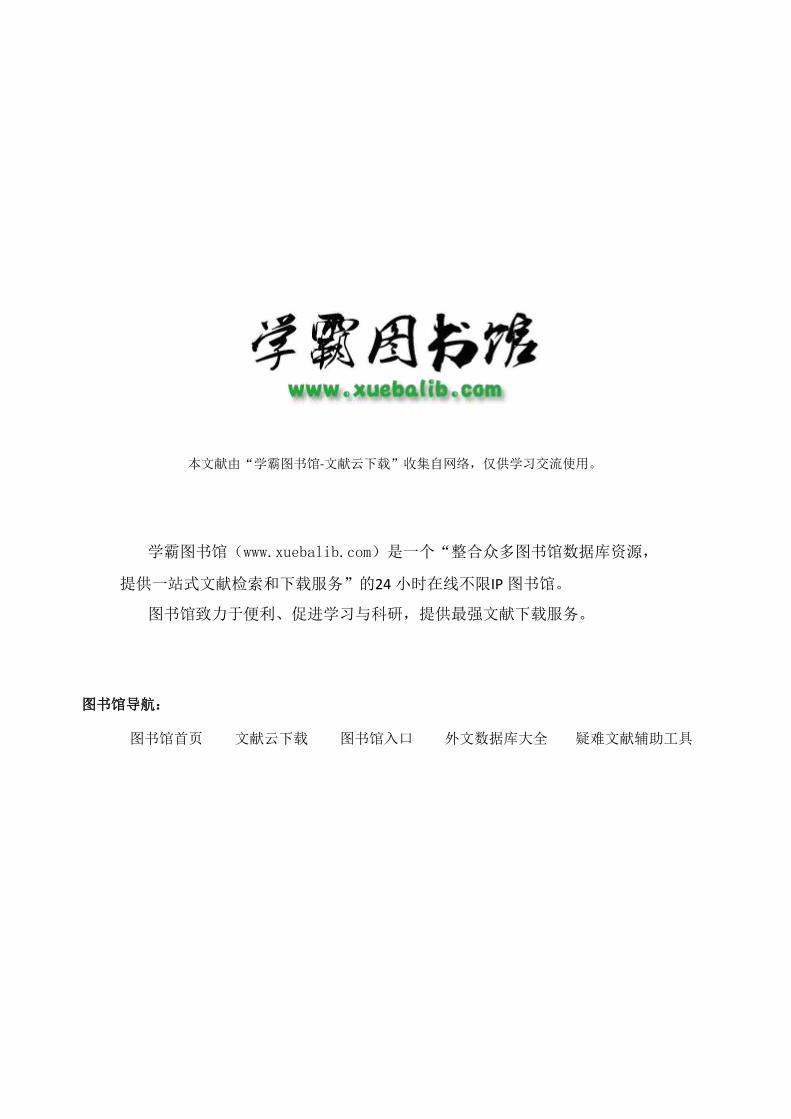
本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具