Embed Size (px)
Citation preview

Obesity – Implications for the Anaesthetist
Dr Martina BiekerConsultant Anaesthetist
1

2

O iOverview
BackgroundSurgerySurgeryPreoperative AssessmentP ti l t f th iPractical aspects of anaesthesia
3

4

Why surgery?y g yEconomical and Personal benefitC t f b it t NHS £3 5 billi /Cost of obesity to NHS = £3.5 billion/yr30 000 deaths, 18 million days off work/yrB i t i d t £ 7000 € 12000Bariatric procedure – cost £ 7000 or € 12000Takes about 4 years to recoup costs of medicationmedicationBariatric surgery reduces all cause mortalityDiabetes remission rate – 73%Diabetes remission rate 73%Remission of obstructive sleep apnoea, hypertension, cardiac failure
5

H tl d iHeartlands experience
April 2003 – December 20071335 patients – gastric bands1335 patients gastric bandsMean age – 42.5 years (18 – 72)M i ht 121 5 k (73 268)Mean preop weight 121.5 kg (73 –268)Mean preop BMI – 44.1 (35- 99)No hospital mortalityAverage stay – 1 02 days
6
Average stay 1.02 days
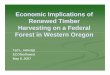
Comparisonp30d mortality Side effects Weight loss Patient
(Average excess)
compliancerequired
Gastric band 0.05% 11.3% 41-54% High
Sleeve ? ? 30-50% MediumgastrectomyRoux-en-Y 0.5% 23.6% 57-67% Medium
Duodenal switch
1.1% 15% 66-74% High
7

Ad tAdverse events
Operative (10%)Thrombo-embolic
Long term (20-30%)Iron deficiency
BleedingPneumonia
yCalciumVitamin B12
UlcersInfection/ peritonitis
Vitamin B1Protein deficiencyInfection/ peritonitis Protein deficiencyGall stonesWeight gain
8
Weight gain

9

P tPreassessment
Cardiovascular systemRespiratory systemRespiratory systemAirwayM t b li di dMetabolic disorders
10

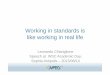
Apples and ppPears
11Sattar and Lean ABC of Obesity – 2007 Blackwell Publishing

Android fat distribution
W i t t hi tiAndroid fat distribution
Waist-to-hip ratio: For men >1
Greater significanceCentral obesity and
For women >0.8cardiovascular diseaseF t i k dFat in neck and around airwaysDiffi ltDifficult surgery
12Bellamy and Struys: OUP (2007) Anaesthesia for the Obese Patient
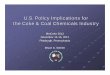
G id f t di t ib tiGynaecoid fat distribution
Arms, legs and buttocksLess severeLess severe
N t l l tNot always clear cut
13

A tAssessment
May be difficult to assess fitnessTechnical difficulties withTechnical difficulties with EchocardiogramsMay not be able to exerciseMay not be able to exerciseNumber of “Fat years” significantVague symptoms may have serious underlying pathology
14

Cardiovascular Pathology
15Adams et al 2000 Br. J. Anaesth. 85:91-108

Cardiomyopathy of Obesity
? Separate entity30 asymptomatic patients (BMI 49 2)30 asymptomatic patients (BMI 49.2) Mean age 37.8 years83% h t i83% hypertensive
Left ventricular hypertrophy 82%
16Rocha et al (2007) Arquivos Brasileiros de Cardiologia (88)

C di thCardiomyopathy
Diagnosis: weight gain, dyspnoea, orthopnoea, oedema, ascitesp , ,LV hypertrophy with increased wall thickness and LV cavity sizethickness and LV cavity size
E h di f ll?Echocardiograms for all?
17Owan and Litwin (2007) Current Heart Failure Reports 4: 221-8

ECG b litiECG abnormalities
Low voltage due to chest wall LV hypertrophy or strainLV hypertrophy or strainProlonged QT intervalI f l t l T b litInferolateral T wave abnormalityRight axis deviation or RBBB – showing right heart strain
18
Respiratory Respiratory pathophysiology
Excess metabolic activity of adipose tissueTherefore increased oxygen demand and CO2 productionExcess work of breathing due to reduced compliance and increased resistanceFRC <1 litre if BMI >40
19

R i t h i lRespiratory physiology
20

Obstructive Sleep ApnoeaObstructive Sleep ApnoeaIncidence of 3%%History of snoring, daytime sleepiness, mood swings, poor concentrationAssociation with hypertension and obesityMay not be able to lie flat –may sleep upright or
d t t b t t iprone – may desaturate or obstruct airwayDiagnosed with polysomnography (sleep laboratory)laboratory)Treatment: CPAP at nightMay need awake intubation in sitting position
21
May need awake intubation in sitting position
Ward NEJM (2002) 347: 498-503

Hypoventilation of obesityHypoventilation of obesityPickwickian syndromeSustained hypoventilation during sleepSustained hypoventilation during sleepExcessive hypersomnolance, morning headachesheadachesMaybe breathless at rest, unable to speak in full sentences snore when awakein full sentences, snore when awakeDaytime hypoxia, raised Pa CO2 (> 5.9 kPa) and polycythemiakPa) and polycythemia In up to 31% of hospitalised morbidly obese – increases with increased BMI
22
– increases with increased BMI
Olson et al Am J Med (2005) 118: 948-956

Leads to right heart failure and mortalityPerioperatively at risk of respiratory depressionDiagnosis: Absence of other causesBMI>30Raised Pa CO2 OSA in 85%OSA in 85%
Treat with elective CPAP or NIVTreat with elective CPAP or NIVOnly cure is weight loss
23

Epworth scorepScore of sleepinessM th 10
1. Sitting and reading __W t hi TVMore than 10 –
sleepyMore than 18 very
2. Watching TV __3. Sitting inactive in public place __4 Passenger in vehicle for hour orMore than 18 – very
sleepy – seek advice4. Passenger in vehicle for hour or
more __5. Lying down in afternoon __
0 – never doze/sleep1 – slight chance
6. Sitting and talking to someone __7. Sitting quietly after lunch (no
l h l)g
2 – moderate chance3 – high chance
alcohol) __8. Stopped in traffic for few minutes
while driving
24
while driving __

AirwayDifficulty predicted by male sexand neck circumference (>17.5 inches)( )Associated with history of OSADifficult intubation is 6.4-9% in non obese population vs. 13-24% in obeseDue to fat pad behind neck and increased fat in soft tissues of soft palate and pharynxsoft tissues of soft palate and pharynxPositioning importantDesaturate extremely quickly after inductionDesaturate extremely quickly after induction even with prolonged preoxygenationNeed for awake fibreoptic intubation?
25
p
Ezri et al Anaesthesia: (2003) 58:1101-8

M t b li tMetabolic etcDiabetes 67% of type II are overweight andDiabetes –67% of type II are overweight and 50% obese MetforminMetforminHigh doses of insulinHypothyroidHypothyroid Up to 90% of patients still have gastric volume of > 25 ml with pH <2 5 after fasting –volume of > 25 ml with pH <2.5 after fasting risk of aspirationHiatus hernia with reflux
26
Hiatus hernia with reflux

Risk scoringgObesity Mortality Score
1 point each for:Male
Score:0-1 = lowest risk =
Age above 45Hypertension
mortality 0.2%2-3 = intermediate =
BMI equal or greater than 50Increased risk for
mortality 1.1%4-5 = high risk =
Increased risk for thrombo-embolic disease
mortality 2.4%
27De Maria et al (2007) Ann Surg 246(4) 578-584

TestsFBC, u+e, LFT and blood glucoseECG mandatory – rhythm abnormality and cor pulmonale – guide for further testsBlood gas if suspect OSA or hypoventilation – useful guide to weaning from ventilationEcho and CXR – asses cardiac function/ cardiac failureExercise – formal or walk/ stair climb
28

National Obesity Surveyy yProf Bellamy (Leeds) – presented at y ( ) pmeeting of Society of Bariatric Anaesthetist (Chichester: September 2008)Carried out end of 2007 in UKNot published yet, but:Routine tests: FBC, u+e, ECG: 100%, ,LFTs: 84%TFTs:45%
29
TFTs:45%

Glucose: 90%Pulmonary function tests: 24%Pulmonary function tests: 24%Routine specific tests - Blood gas: 10%E th 45%Epworth score: 45%Echocardiogram: 10%Cardiopulmonary exercise test: none
30

31

Practical considerationsTEAM WORKTransportSpecial equipment (including large gowns)Special equipment (including large gowns)PositioningMonitoringMonitoringVenous accessI t b tiIntubationThrombo-prophylaxis (size of TEDs)
32

Equipmentq p
33

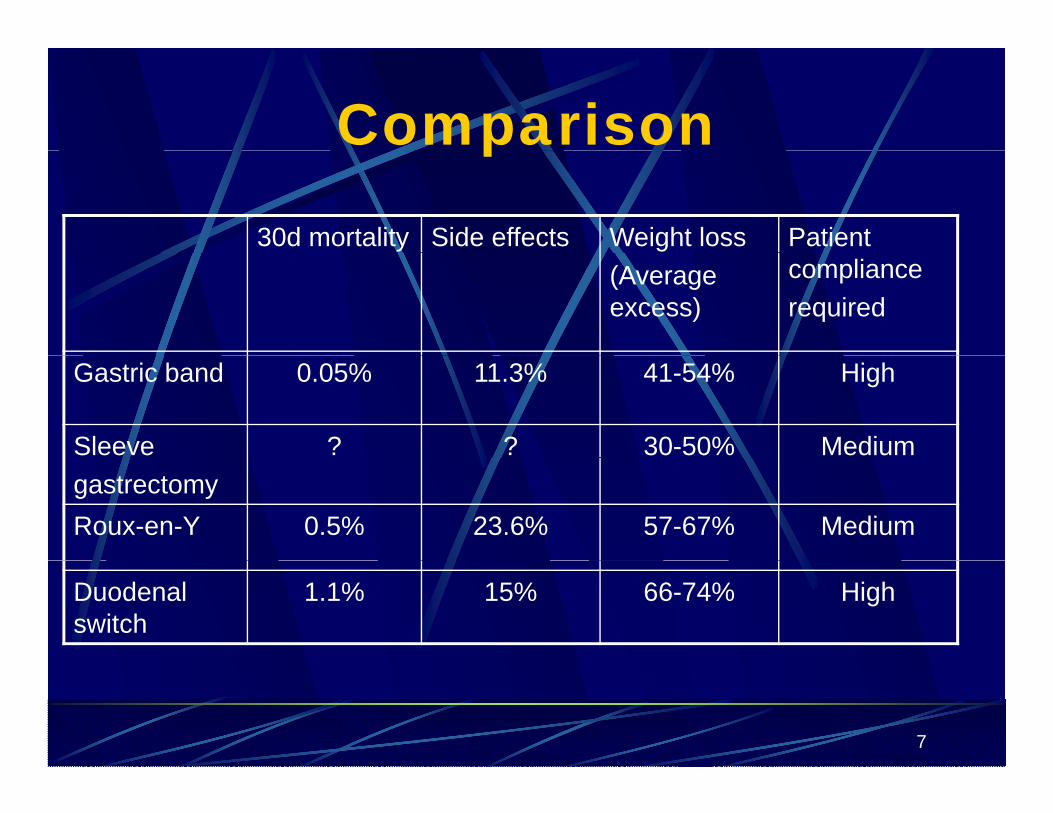
Positioning
X 34
“Ramping”

35
Practical considerationsTEAM WORKTransportSpecial equipmentPositioningg
MonitoringVenous accessVenous accessIntubationThrombo-prophylaxis
36

W ki Waking up
37
38

Key Recommendationsy1. All trained anaesthetists should be competent in
management of MOmanagement of MO2. All patients should have their height and weight
recorded3. BMI is not ideal measure of risk - is most useful4. Named anaesthetist and theatre staff member4. Named anaesthetist and theatre staff member5. Protocols and availability of specialist equipment6 Manual handling courses6. Manual handling courses7. Preoperative assessment is mandatory8 Communication!
39
8. Communication!
Wh t?Where next?
Revision surgeryDay surgery: ASA 1 and 2 and BMI< 50Day surgery: ASA 1 and 2 and BMI< 50Bariatric patients in other surgical disciplines notably obstetrics anddisciplines notably obstetrics and orthopaedic surgeryEEmergency surgeryPaediatric- BMJ 25th of October
40

A k l d tAcknowledgment
Thank you to Dr B. Prasad for the use of some of the photosp
41

The future?The future?
42