Embed Size (px)
DESCRIPTION
..
Citation preview
7/17/2019 nuevos anticoagulantes
http://slidepdf.com/reader/full/nuevos-anticoagulantes-56909d54767c6 1/11NATURE REVIEWS | CARDIOLOGY ADVANCE ONLINE PUBLICATION | 1
Icahn School ofMedicine at MountSinai, One GustaveL. Levy Place,PO Box 1030, NewYork, NY 10029, USA(U.B., I.M., R.M.).
Correspondence to:R.M.roxana.mehranmssm.edu
Balancing ischaemia and bleeding risks
with novel oral anticoagulantsUsman Baber, Ioannis Mastoris and Roxana Mehran
Abstract | Vitamin K antagonists (VKAs) have long been the standard of care for treatment of venous
thromboembolism (VTE), and thromboprophylaxis in atrial fibrillation (AF). Despite their efficacy, their use
requires frequent monitoring and is complicated by drug–drug interactions and the need to maintain a narrow
therapeutic window. Since 2009, novel oral anticoagulants (NOACs), including the direct thrombin inhibitor
dabigatran and the direct factor Xa inhibitors apixaban, edoxaban, and rivaroxaban, have become alternative
options to VKAs owing to their predictable and safe pharmacological profiles. The overall clinical effect
of these drugs, which is a balance between ischaemic benefit and bleeding harm, varies according to the
clinical scenario. As adjunctive therapy to dual antiplatelet therapy in patients with acute coronary syndrome,
NOACs are associated with incremental bleeding risks and modest benefits. For treatment of VTE, NOACshave a safer profile than VKAs and a similar efficacy. In thromboprophylaxis in AF, NOACs are associated
with the greatest benefits by reducing both ischaemic events and haemorrhagic complications and might
reduce mortality compared with VKAs. The role of NOACs continues to evolve as these drugs are evaluated in
different patient populations, including those with renal impairment or with AF and undergoing percutaneous
coronary intervention.
Baber, U. et al. Nat. Rev. Cardiol. advance online publication 4 November 2014; doi:10.1038/nrcardio.2014.170
Introduction
The treatment and prevention of thrombotic disordersinvolving either the venous or arterial circulations man-dates the use of antiplatelet or anticoagulant therapies, orboth. However, an important tenet to the use of potent
antithrombotic pharmacotherapy is that beneficial reduc-tions in ischaemic events are realized only at the cost ofexcess bleeding. Historically, quantifying this balancehas been difficult, because bleeding end points wereusually considered secondary to ischaemic events instudy designs, and the lack of standardized approachesto measure bleeding rendered comparisons betweentrials difficult. In addition, treatment algorithms forpatients with atrial fibrillation (AF; such as CHADS
2 and
CHA2DS
2-VASc) or chest pain (TIMI risk score) were
derived and validated for purposes of reducing ischaemicevents, such as myocardial infarction or stroke.1–3
Over the past 10 years, bleeding has emerged as a
marked and independent risk for adverse events, themagnitude of which is similar to recurrent ischaemicevents.4 The increased recognition of the prognostic
relevance of bleeding has led to standardized approachesto define this adverse effect, and the inclusion of bleed-ing along with ischaemic events in composite primaryend points of clinical trials, such as ‘net adverse clini-
cal events’.5 Risk scores to estimate bleeding complica-tions have been developed and are now incorporated intreatment guidelines to refine the optimal choice andintensity of antithrombotic therapy.3,6–8 Concordant withthese developments has been the introduction of severalnovel oral anticoagulant (NOAC) drugs that mighteither replace or serve a complementary role to exist-ing antithrombotic therapy. In this Review, we provide acomprehensive and contemporary summary of the risksand benefits of NOACs in several distinct clinical set-tings, including stroke prevention in AF, treatment for venous thromboembolism (VTE), and therapy for acutecoronary syndromes (ACS), with a focus on the balance
between ischaemic benefit and bleeding harm withineach clinical condition.
NOAC pharmacology
Vitamin K antagonists (VKAs) were discovered >80 yearsago after the development of fatal bleeding in cattle. 9 Warfarin is the primary VKA used in the USA, whereasacenocoumarol and phenprocoumon are mostly usedin Europe. These drugs share a common mechanismof action in inhibiting the vitamin K epoxide reductasecomplex subunit 1, which is essential in the recyclingof vitamin K in the liver.10 Despite the proven efficacy ofVKAs in the treatment of various clinical conditions
Competing interests
R.M. declares that she is or has been a consultant for AbbottVascular, AstraZeneca, Boston Scientific, Covidien, CSL Behring,Janssen Pharmaceuticals, Maya Medical, Merck, RegadoBiosciences, and Sanofi-Aventis; a member of the AdvisoryBoard for Covidien, Janssen Pharmaceuticals, and Sanofi-Aventis; and has received institutional research grant supportfrom Bristol–Myers Squibb, CardioKinetix, Daiichi Sankyo, Lilly,Sanofi-Aventis, and The Medicines Company. The other authorsdeclare no competing interests.
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved

7/17/2019 nuevos anticoagulantes
http://slidepdf.com/reader/full/nuevos-anticoagulantes-56909d54767c6 2/11

7/17/2019 nuevos anticoagulantes
http://slidepdf.com/reader/full/nuevos-anticoagulantes-56909d54767c6 3/11NATURE REVIEWS | CARDIOLOGY ADVANCE ONLINE PUBLICATION | 3
yielded a 34% relative reduction in the risk of stroke orsystemic embolism compared with warfarin (HR 0.66,95% CI 0.53–0.82) whereas the difference with a dose of110 mg twice daily was nonsignificant (HR 0.91, 95% CI0.74–1.11).21 In terms of safety, investigators in eachtrial reported numerical reductions in fatal or intra-cranial bleeding, whereas reductions in composite orless severe bleeding were variable. Reductions in gastro-intestinal bleeding, for example, were observed only withapixaban, whereas the other NOACs were associatedwith increased gastrointestinal bleeding.
A pooled analysis by Ruff and colleagues of study-level data from each of the principal phase III trialswas undertaken to provide more precise risk estimatesfor selected subgroups and important secondary endpoints.35 Not surprisingly, the pooled risk ratio for theprimary efficacy end points favoured NOACs (relativerisk [RR] 0.81, 95% CI 0.73–0.91) without evidence ofheterogeneity between studies (P =0.13).35 In an analy-sis of components of the efficacy end points, the benefitin stroke reduction was primarily attributable to reduc-
tions in haemorrhagic (RR 0.49, 95% CI 0.38–0.64),rather than ischaemic (RR 0.92, 95% CI 0.83–1.02)stroke.35 Another important finding from this analysiswas that all-cause mortality was significantly reducedwith NOACs (RR 0.90, 95% CI 0.85–0.95).35 Withrespect to bleeding end points, the rate of intracranialhaemorrhage was significantly reduced with NOACscompared with warfarin (RR 0.48, 95% CI 0.29–0.59),whereas gastrointestinal bleeding was significantly morecommon with NOACs than with warfarin (RR 1.25,95% CI 1.01–1.55).35 The pooled risk ratio for bleedingfavoured NOACs compared with warfarin (RR 0.86,95% CI 0.83–1.00), but heterogeneity for this effect was
significant (I 2 = 83%, P = 0.001).35
In important selected clinical subgroups, the point esti-mates for both ischaemic and bleeding end points wereuniform with the exception of anticoagulation control,quantified using the time in therapeutic range (TTR).The relevance of TTR as a valid correlate of outcomesin patients treated with warfarin was highlighted in theresults of the SPORTIF III and SPORTIF V trials,36,37 inwhich higher rates of major bleeding (3.85% vs 1.96% vs 1.58%) and annual mortal ity (4.20% vs 1.84% vs1.69%) were observed in the group with poor controlof international normalized ratio (INR; TTR <60%)than in the groups with moderate (TTR 60–75%) or
good (TTR >75%) control, respectively. In the analysisby Ruff and colleagues, NOACs provided no significantreductions in bleeding compared with VKAs in centreswith a TTR >66% (RR 0.93, 95% CI 0.76–1.13), whereasan increase in bleeding was observed in centres withpoorly managed TTR (<66%; HR 0.69, 95% CI 0.59–0.81,P = 0.02 for interaction).35 By contrast, the magnitudeof benefit with NOACs in reducing ischaemic eventsremained uniform across TTR strata (P = 0.60 for inter-action).35 The reductions in stroke or systemic embolismnotwithstanding, the accentuated reductions in bleedingobserved with poorly managed anticoagulation controlin these clinical trials will translate to an overall greater
net clinical benefit in real-world settings, which are gen-erally characterized by suboptimal INR control.38 Indeed,even in the rigorous context of a randomized trial, themean TTR in the RE-LY trials was 77% for Swedishparticipants, whereas mean TTR in the USA was only66%.39 A number of environmental factors complicateINR control, such as drugs, herbal remedies, dietarychanges, and disease states in addition to genetic muta-tions that modulate warfarin metabolism and affect itspharmacokinetics, precluding any fixed-dose response.Accordingly, NOACs might be an attractive alternative towarfarin owing to a wider therapeutic window, predict-able dose response, fewer drug–drug interactions, andestablished safety compared with VKA use.
Pooled analyses have provided clinically relevantinsights into the aggregate effects of NOACs comparedwith warfarin, but direct comparisons between NOACsremain lacking. Given the substantial costs and time toconduct large phase III clinical trials, randomized com-parisons of these agents are unlikely. Therefore, compar-ative inferences between the NOACs will necessitate the
use of indirect comparisons or new analytical techniquesfor the foreseeable future. In one such report, indirectcomparisons were made between apixaban, dabigatran,and rivaroxaban using data from each respective clini-cal trial.40 Using techniques developed by Bucher andcolleagues,41 the researchers generated hazard ratioscomparing each NOAC to the others for both ischae-mic and haemorrhagic end points. To provide a validcomparison with the higher-risk patients enrolled in theROCKET-AF trial33 than in the other studies, the analy-sis was restricted to patients with a CHADS
2 score ≥3.
Each NOAC yielded statistically similar rates of stroke orsystemic embolism, whereas the rate of major haemor-
rhage was lowest with apixaban, and similarly higherwith dabigatran or rivaroxaban.40
Management of ACS
The management of patients with ACS has advancedsubstantially with the use of invasive approaches,potent inhibitors of the platelet P2Y purinoceptor 12(P2Y
12 receptor) and adjunctive pharmacotherapy
including angiotensin-converting-enzyme inhibitorsand statins.42 These advances notwithstanding, residualatherothrombotic risk remains substantial, with rates ofadverse events approaching 10% in randomized-trialparticipants treated with contemporary, evidence-based
medicine.43 Initial studies suggested that anticoagulationwith oral VKAs might reduce adverse events in patientswith ACS,44 but this practice was largely abandonedowing to bleeding concerns coupled with the improvedefficacy of dual antiplatelet therapy in reducing stentthrombosis.45,46 However, the introduction of NOACshas spurred renewed interest in the potential role ofadjunctive oral anticoagulation in the treatment of ACS.
In the RE-DEEM trial,47 the effect of various dosesof dabigatran (50 mg, 75 mg, 110 mg, or 150 mg twicedaily) was compared with placebo in the prevention ofmajor or clinically relevant minor bleeding among 1,861patients with recent ACS (within the past 14 days). Over
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved

7/17/2019 nuevos anticoagulantes
http://slidepdf.com/reader/full/nuevos-anticoagulantes-56909d54767c6 4/114 | ADVANCE ONLINE PUBLICATION www.nature.com/nrcardio
the 6-month study period, dabigatran was associatedwith a dose-dependent increase in bleeding without anyappreciable reduction in ischaemic events. Analogously,both apixaban and rivaroxaban, also yielded incre-mental risks of bleeding with increasing dose of eitherdrug in similar phase II studies involving patients
with ACS.48,49 However, in contrast to the findings withdabigatran,47 both factor Xa inhibitors demonstratedmodest, albeit nonsignificant, reductions in ischaemicadverse events.48,49 Results from each of these studiesalso showed that bleeding risk and efficacy might varyaccording to antiplatelet therapy status (monotherapy versus dual antiplatelet therapy [DAPT]). For example,in the APPRAISE trial,48 the absolute increase in bleed-ing observed with apixaban (10 mg daily) comparedwith placebo was 6% and 1% among those receivingbaseline DAPT or aspirin monotherapy, respectively.Analogously, the absolute reduction in ischaemic eventswith this dose of apixaban was 2% and 6%, respec-
tively. Similar findings were observed for rivaroxaban.49 Although hypothesis-generating, these results suggestthat the net clinical benefit of either factor Xa inhibi-tor might be optimal in patients with ACS treated withantiplatelet monotherapy rather than DAPT. These find-ings led to pivotal large-scale, phase III trials for bothapixaban and rivaroxaban in patients with ACS (Table 2).
In the APPRAISE-2 trial,50 apixaban administered ata twice-daily dose of 5 mg was compared with placeboin 7,392 patients with a recent ACS (within the past7 days). The study was powered to detect a 20% reduc-tion in relative risk with apixaban versus placebo, assum-ing a total of 938 patients would reach a primary efficacy
outcome of cardiovascular death, myocardial infarction,or ischaemic stroke. The trial was stopped prematurelyafter accruing only 572 events (60% of estimated), owingto an excess risk of bleeding without a concomitantreduction in ischaemic events. The rate of the primaryefficacy outcome in the apixaban and placebo groups was7.9% and 7.5%, respectively (HR 0.95, 95% CI 0.80–1.11,P = 0.51), and the rates of TIMI major bleeding were1.3% and 0.5% (HR 2.59, 95% CI 1.50–4.46, P = 0.001).50 In contrast to the findings from the phase II study, theincremental bleeding risks and ischaemic benefits asso-ciated with apixaban were uniform in the APPRAISE-2trial,50 irrespective of background antiplatelet therapy.
In the ATLAS ACS 2-TIMI 51 trial,51 rivaroxaban atdoses of 2.5 mg or 5.0 mg twice daily was compared withplacebo in 15,526 patients with a recent ACS (withinthe past 7 days). The overall risk–benefit ratio slightlyfavoured the lower dose of rivaroxaban owing to numeri-cally fewer bleeding events in this group compared with
the 5.0 mg dose.Given that apixaban and rivaroxaban are both
factor Xa inhibitors, the divergent results from thephase III studies of each drug might seem counter-intuitive. However, differences in the study design andpatient populations might account for the discordantresults. For example, the APPRAISE-2 trial50 was spe-cifically designed to enrol patients with high-risk fea-tures resulting in a cohort who were older, with a greaterburden of diabetes mellitus and impaired renal func-tion, than the patients in the ATLAS ACS 2-TIMI 51trial.51 In addition, the dose of apixaban used in theAPPRAISE-2 trial50 (5.0 mg twice daily) is identical to
the dose with the greatest efficacy for stroke preventionin AF. By contrast, the doses of rivaroxaban used in theATLAS ACS 2-TIMI 51 trial51 were only 25–50% of thosetested in patients with AF. These findings suggest thatthe optimal degree of factor Xa inhibition that yields thegreatest net clinical benefit might be lower in patientswith ACS than in those with AF. Irrespective of theunderlying reasons for the lack of consistency betweentrials, the conflicting results of these phase III studieshas led to some degree of uncertainty about the role ofNOACs in patients with ACS, with regulatory agencieshesitant to provide approval for this indication.52,53
Treatment of VTEVTE, including deep vein thrombosis and pulmonaryembolism, is a common condition and associated withsubstantial morbidity and mortality. Classic approachesto treating VTE involve initiating treatment with aparenteral anticoagulant, usually unfractionated orlow-molecular-weight heparin, followed by chronic oralVKA therapy.54 Although efficacious in reducing recur-rent VTE, the inherent limitations of long-term VKAtherapy render this strategy suboptimal and highlight theneed for alternative approaches. Therefore, NOACs havebeen studied in the prophylaxis, treatment, and second-ary prevention of VTE in a variety of studies. The role
Table 2 | Main results of selected phase III trials of NOACs in patients with ACS
Trial NOAC (n) Control
(n)
Primary efficacy end point Primary safety end point
NOAC
(%)
Control
(%)
HR
(95% CI)
NOAC
(%)
Control
(%)
HR
(95% CI)
APPRAISE-250 Apixaban 5 mg twice daily(3,705)
Placebo(3,687)
7.5 7.9 0.95(0.80–1.11)
1.3 0.5 2.59(1.50–4.46)
ATLAS ACS
2-TIMI 5151
Rivaroxaban 2.5 mg
twice daily (5,174)
Placebo
(5,176)
9.1 10.7 0.84
(0.72–0.97)
1.8 0.6 3.46
(2.08–5.77)
ATLAS ACS2-TIMI 5151
Rivaroxaban 5.0 mgtwice daily (5,176)
Placebo(5,176)
8.8 10.7 0.85(0.73–0.98)
2.4 0.6 4.47(2.71–7.36)
ATLAS ACS2-TIMI 5151
Rivaroxaban combined withantiplatelet therapy (10,350)
Placebo(5,176)
8.9 10.7 0.84(0.74–0.96)
2.1 0.6 3.96(2.46–6.38)
Abbreviations: ACS, acute coronary syndrome; n, number of patients; NOAC, novel oral anticoagulant.
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved
7/17/2019 nuevos anticoagulantes
http://slidepdf.com/reader/full/nuevos-anticoagulantes-56909d54767c6 5/11NATURE REVIEWS | CARDIOLOGY ADVANCE ONLINE PUBLICATION | 5
of NOACs in the primary prevention of postoperativeVTE55–57 has been reviewed elsewhere and will not be
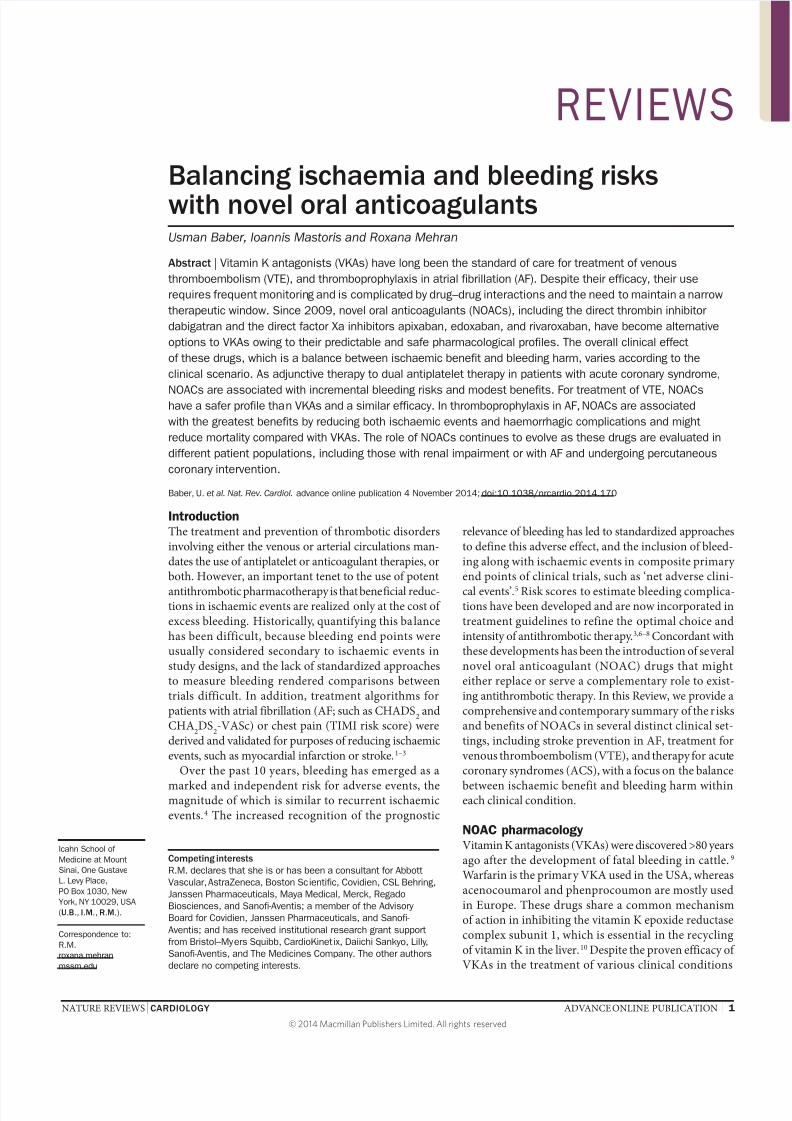
discussed further. The main phase III clinical trials toexamine different NOACs in the treatment of VTE areshown in Table 3.58–63 Each of the phase III trials was sim-ilarly designed as a noninferiority comparison between aNOAC and warfarin with follow-up ranging between3 months and 1 year. Moreover, in all trials the primaryefficacy and safety end points were defined usingcommon methods. Efficacy was usually defined astime to recurrent nonfatal VTE or VTE-related death.The primary safety outcome was consistently definedusing the criteria set out by the International Society ofThrombosis and Haemostasis.64
Findings from these trials, in terms of both safety and
efficacy, were also consistent. Specifically, each trial metthe primary efficacy end point of noninferiority withuse of a NOAC compared with warfarin in the preven-tion of VTE or VTE-related death (Table 3). Althoughthe magnitude of this effect varied between studies, notrial showed superiority with NOAC use associated withthe primary efficacy outcome. These efficacy resultswarrant consideration within the context of the inten-sity and quality of anticoagulation achieved with thewarfarin comparator. In general, the TTR with warfarinwas higher (55–60%) than that achieved in real-worldpatients.58–63 Accordingly, these findings suggest thateither a NOAC or well-managed warfarin yield similar
benefits in treating patients with VTE. However, the‘real-world’ efficacy of NOACs in treatment of VTEmight be greater than that observed in the randomizedstudies given the less-effective INR control seen outsideof controlled trial settings.
The aggregated evidence to date shows similaritybetween the NOACs and warfarin in the acute treatmentof VTE, along with a strong trend towards improvedsafety. However, the ideal balance between bleedingharm and ischaemic benefit for the use of NOACs inthis clinical scenario needs to be considered within thedesign constraints and risk profile of patients enrolled ineach trial. First, patients with haemodynamic instability
or those requiring initial treatment with fibrinolytics or vena cava filters, which might result from a large pulmo-
nary embolism, were excluded from all studies, therebylimiting generalizability to these high-risk individuals.Second, antecedent parenteral anticoagulation before ini-tiation of NOAC therapy or warfarin was not uniformacross trials. In the RE-COVER I trial,59 for example,patients received parenteral anticoagulation for a medianof 9 days before dabigatran or matching placebo was ini-tiated. This design reflected previous experience showinga high risk of recurrent VTE when direct thrombininhibitors were used without overlapping anticoagula-tion. By contrast, in the EINSTEIN-PE61 and EINSTEIN62 trials, a higher dose of rivaroxaban (15 mg twice daily)was administered for the first 3 weeks, and then a lower
dose (20 mg daily) was recommended thereafter.
Application to clinical practice
Estimating ischaemic and bleeding risks in AF
Outside the controlled environment of clinical trials,the decision of how to manage patients with AF requirescareful evaluation of the relative risks of ischaemic andbleeding complications. Ultimately, balancing thesecompeting influences will determine the need for, andurgency of, treatment. Accomplishing this task man-dates evaluating a patient’s risk of ischaemic stroke inthe absence of therapy, and the risk of haemorrhagewith treatment. Several ischaemic and bleeding risk
scores have been developed, including the CHADS2,CHA
2DS
2-VASc, and HAS-BLED schemes.3,6,65 In
general, guidelines are concordant in recommendingthe use of oral anticoagulants in patients at intermedi-ate risk of stroke (CHADS
2 ≥2).66–68 Despite this consist-
ency, the extent to which risk-stratification algorithmsinfluence and reflect real-world clinical decision-makingwarrants examination, because particular scores wereoriginally derived in clinical-trial cohorts with carefulpatient selection and close monitoring. For example,in many of the landmark trials in which the efficacy oforal anticoagulation for stroke prevention in patientswith nonvalvular AF was established, fewer than 10% of
Table 3 | Main results of selected phase III trials of NOACs in patients with VTE
Trial NOAC (n) Control
(n)
Primary efficacy end point Primary safety end point
NOAC
(%)
Control
(%)
HR
(95% CI)
NOAC
(%)
Control
(%)
HR
(95% CI)
AMPLIFY58 Apixaban 5 mg or 10 mgtwice daily (2,691)
Warfarin(2,704)
2.3 2.7 0.84(0.60–1.18)
0.6 1.8 0.31(0.17–0.55)
RE-COVER I59 Dabigatran 150 mg
twice daily (1,273)
Warfarin
(1,266)
2.4 2.1 1.10
(0.65–1.84)
1.6 1.9 0.82
(0.45–1.48)
RE-COVER II60 Dabigatran 150 mgtwice daily (1,280)
Warfarin(1,288)
2.3 2.2 1.08(0.64–1.80)
1.2 1.7 0.69(0.36–1.32)
EINSTEIN-PE61 Rivaroxaban 15 mg twice dailyor 20 mg once daily (2,419)
VKA(2,413)
2.1 1.8 1.12(0.75–1.68)
10.3 11.4 0.90(0.76–1.07)
EINSTEIN62 Rivaroxaban 15 mg twice dailyor 20 mg once daily (1,731)
VKA(1,718)
2.1 3.0 0.68(0.44–1.04)
8.1 8.1 0.97(0.76–1.22)
HOKUSAI-VTE63 Edoxaban 60 mgonce daily (4,118)
Warfarin(4,122)
3.2 3.5 0.89(0.70–1.13)
8.5 10.3 0.81(0.71–0.94)
Abbreviations: n, number of patients; NOAC, novel oral anticoagulant; VTE, venous thromboembolism.
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved

7/17/2019 nuevos anticoagulantes
http://slidepdf.com/reader/full/nuevos-anticoagulantes-56909d54767c6 6/116 | ADVANCE ONLINE PUBLICATION www.nature.com/nrcardio
the screened patients were randomly assigned to eitherstudy group. In addition, many patients at high risk ofbleeding were excluded from these studies, highlight-ing the lack of generalizability of trial participants toreal-world patients.
To examine this issue, Steinberg and colleagues evalu-ated the concordance between empirical risk estimatesand physicians’ subjective assessment in a large cohort ofpatients with AF (n = 10,094).69 Although 72% of patientswere in the high-risk category using the CHADS
2 algo-
rithm, physicians considered only 16% to be at highrisk.69 Analogously, physicians rated 7% of patients as
being at high risk of bleeding, compared with 17% usingan objective scale.69 The poor correlation observed inthis study might be attributable to several factors. First,physicians might consider some risk factors in theirassessment that are not captured by established riskscores, such as frailty or cognitive decline, when assessingbleeding and ischaemic risk in patients with AF. Second,physicians might value and weight particular risk factorsfor stroke or bleeding differently from the empiricalmodels. Third, lack of familiarity with established riskalgorithms might lead to poor calibration by clinicians.The underestimation of ischaemic risk by physicianscompared with objective estimates might contribute to
undertreatment and increased rates of stroke or systemicembolism in real-world patients with AF compared withthose participating in clinical trials. Further investiga-tion to understand these discrepancies is warranted,because subjective evaluation by physicians is a strongerdeterminant of decision-making than objective estimates.
Another crucial consideration in the balance betweenischaemic and bleeding risk is the objective effect andsubjective perception of these events on subsequentmorbidity and mortality in patients with AF. Ischaemicrisk scores were primarily developed to predict exclu-sively ischaemic stroke or systemic embolism, whereasbleeding algorithms have generally involved broader
outcomes. In the derivation of the HAS-BLED score,for example, risk factors were identified that correlatedwith a composite bleeding outcome that comprisedintracranial or extracranial haemorrhages, transfusion,and haemoglobin decrease >2 g/l.6 Accordingly, weigh-ing all haemorrhagic events equivalently to that of anischaemic stroke might be an oversimplification of theirtrue effect when conducting risk–benefit calculations fororal anticoagulation therapy in patients with AF.
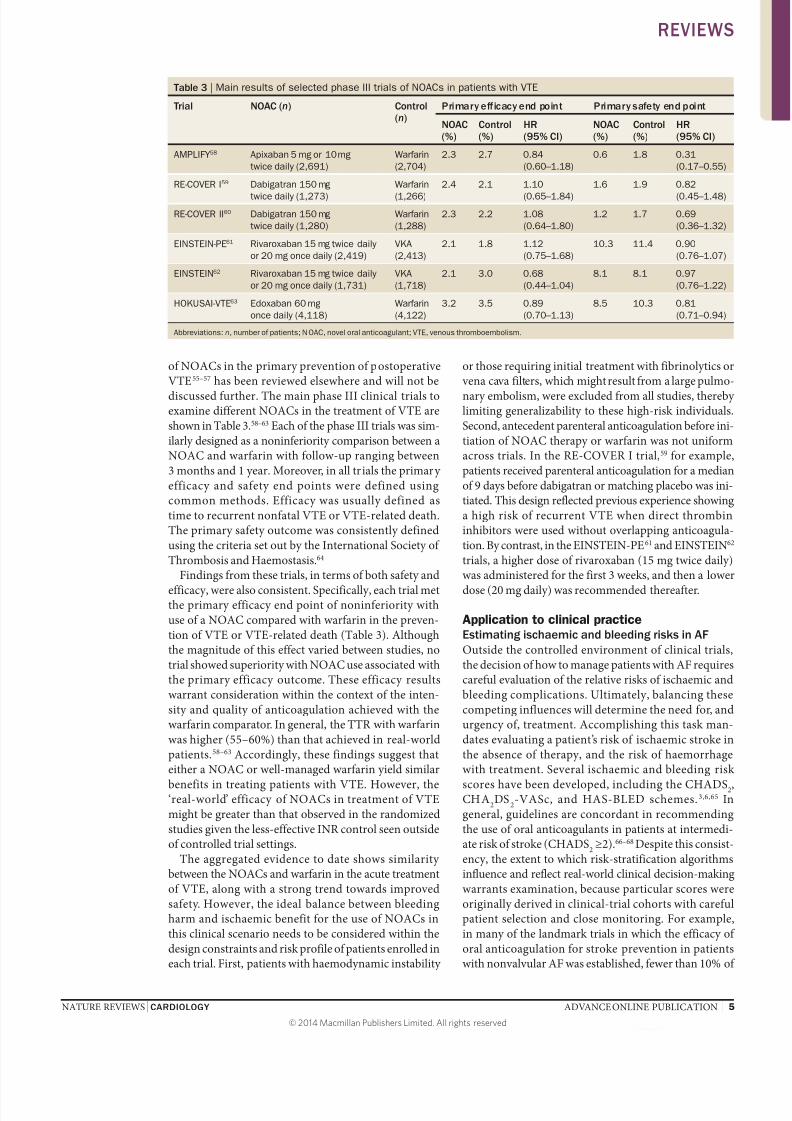
To illustrate this point, Fang and colleagues evaluatedthe incidence of intracranial and extracranial bleed-ing and the effect on 30-day mortality in patients withnonvalvular AF treated with oral anticoagulation.70 The overall rate of intracranial haemorrhage was 0.47%(n = 72), whereas the corresponding rate of extracranialbleeding was 0.64% (n = 98), the majority (89%) of whichwas gastrointestinal.70 The effect on mortality of thedifferent types of bleeding varied substantially, with a30-day mortality of 48.6% and 5.1% among those withintracranial and extracranial bleeding, respectively(Figure 1).70 The respective rates of major disability
were 34% and 1%.70 In a separate study, Hylek and col-leagues found that 30-day mortality after an ischaemicstroke in patients with AF treated with oral anticoagu-lants was 22%, less than half the mortality estimatedby Fang and colleagues for intracranial haemorrhage(Figure 1).71 Taken together, these studies highlight thesubstantial heterogeneity in both morbidity and mortal-ity after ischaemic and haemorrhagic events in patientswith AF. Particularly relevant is the observation thatintracranial haemorrhage is a much stronger determi-nant of poor outcomes than gastrointestinal bleedingin patients treated with warfarin, and that extracranialbleeding might warrant a smaller influence on decision-
making about oral anticoagulant therapy. This stanceis supported by findings from investigators who foundthat patients are more willing than physicians to acceptan increased risk of gastrointestinal bleeding for acorresponding reduction in the risk of stroke.72
The variable effect on mortality from intracranial versusextracranial bleeding also provides an important contextto appreciate bleeding risks when considering the use ofNOACs. Specifically, whereas dabigatran, edoxaban, andrivaroxaban were all associated in randomized trials witha significantly increased risk of gastrointestinal haemor-rhage, apixaban did not increase the rate of gastrointestinalbleeding compared with VKAs in the ARISTOTLE
study.32 Perhaps more importantly, all the NOACs haveshown substantial reductions in the risk of intracranialhaemorrhage compared with VKAs.21,32–34 Indeed, in apooled analysis, Ruff and colleagues found that intra-cranial haemorrhage was reduced by 50% compared withVKAs, without evidence of heterogeneity between trials.35 Although gastrointestinal bleeding is more common thanintracranial haemorrhage in patients treated with oralanticoagulants, the risk of death associated with intra-cranial haemorrhage is markedly higher than that withgastrointestinal bleeding. Therefore, protection fromintracranial haemorrhage might outweigh the potentialgastrointestinal adverse effects in many patients with AF.
Ischaemicstroke
Intracranialbleeding
Clinical event
3 0 - d a y m o r t a l i t y ( % )
Extracranialbleeding
0
60
40
20
30
10
50
Figure 1 | Effect of clinical adverse events (ischaemicstroke, and intracranial and extracranial bleeding) on30-day mortality.70,71 Patients receiving warfarin therapyand who experience an ischaemic stroke have asubsequent 30-day mortality of 22%. Patients treated withwarfarin and who sustain an intracranial bleed have asignificantly higher 30-day mortality (48.6%) than thosewith an extracranial bleeding complication (5.1%).
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved

7/17/2019 nuevos anticoagulantes
http://slidepdf.com/reader/full/nuevos-anticoagulantes-56909d54767c6 7/11NATURE REVIEWS | CARDIOLOGY ADVANCE ONLINE PUBLICATION | 7
However, in patients with definite risk factors, or who areat very high risk of gastrointestinal bleeding, an individu-
alized approach might be needed, either to treat with theNOAC with the lowest risk of gastrointestinal bleeding(apixaban) or even to consider a VKA.73
Alternative metrics to balance risks
Treatment effects are usually expressed as relative orabsolute risks on the basis of findings from randomizedtrials, but the complexities and nuances of clinicaldecision-making often require more comprehensivemetrics to evaluate the potential benefits of novel thera-pies. For example, Singer and colleagues quantified thenet clinical benefit of warfarin anticoagulation usingthe following equation:
(event rateoff warfarin
– event rateon warfarin
)– weight × (ICH rate
on warfarin – ICH rate
off warfarin)
where ICH is intracranial haemorrhage. Importantly, thiscalculation assigns a larger weighting to bleeding thanto ischaemic events, consistent with the higher risk ofdeath observed after a haemorrhagic than an ischaemicstroke.71 Using this method, Banerjee and colleagues cal-culated the net clinical benefit of NOACs in a real-worldsetting.74 Using data from the Danish National Registryof patients with nonvalvular AF (n = 132,372) between1997 and 2008, the researchers calculated rates of ischae-
mic stroke and intracranial haemorrhage for patientsreceiving NOAC or warfarin therapy. Treatment effectsderived from the clinical trials of each drug were thenapplied to derive the theoretical rates of ischaemic strokeand intracranial haemorrhage across different strata ofstroke and bleeding risk. Their results demonstrate thatamong patients at the lowest risk of stroke (CHADS
2 = 0),
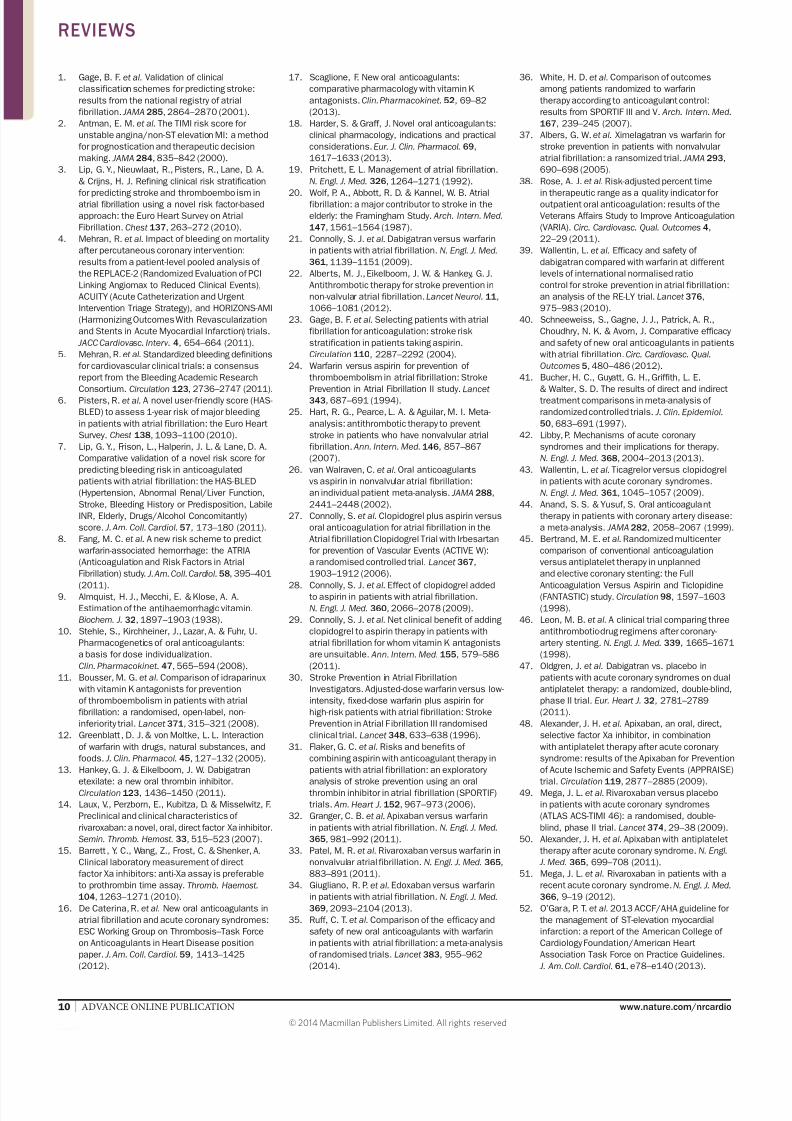
the net clinical benefits of the NOACs exceed those ofwarfarin, although the magnitude of benefit is modest(Figure 2).74 Coupled with the fairly low rate of adverseischaemic and bleeding events among such patients,widespread use of the NOACs in these individuals mightnot be cost-effective. By contrast, net clinical benefits
were larger among those with a CHADS2 score ≥1, irre-
spective of bleeding risk.74 Moreover, in these patients, the
magnitude of benefit with each NOAC remained largerthan that with warfarin. In addition, among patients at thehighest risk of stroke (CHADS
2 score ≥2), the net clinical
benefit with any anticoagulant was greater among thoseat higher bleeding risk than those at lower bleeding risk,as assessed using the HAS-BLED score.74 These findingshighlight the complementary roles of using both ischae-mic and bleeding risk stratification to identify the patientswho might receive the greatest benefit from NOACs.
Alternatively, calculating the ‘number needed to treat’or ‘number needed to harm’ provides a complementarymetric to relative risk estimates or the net clinical benefitwhen assessing the benefits or harms of novel therapies.
The number needed to treat quantifies the number ofpatients requiring treatment with a therapy to preventone adverse event. By contrast, the number needed toharm quantifies the number of patients who would needto be exposed to a therapy to cause one adverse event.The number needed to treat to prevent one ischaemicstroke with NOACs compared with warfarin is 78–500patients (Figure 3; Table 4).21,32–34 Treating 1,000 patientswith apixaban prevents one gastrointestinal haemor-rhage, whereas treatment of 101, 204, and 357 patientswith rivaroxaban, dabigatran, or edoxaban, respectively,will result in one gastrointestinal bleed. All the NOACsreduce intracranial haemorrhage compared with war-
farin, with an approximately similar number of patientswho would require treatment to realize this benefit.
Cost-effectiveness
The use and cost-effectiveness of NOACs should be inter-preted within the context of the overall health-care system.Two groups of researchers have addressed this issue byapplying a Markov decision analysis.75,76 Harrington andcolleagues modelled the cost-effectiveness of variousNOACs compared with warfarin in a hypothetical cohortof patients aged 70 years with nonvalvular AF, a CHADS
2
score ≥1, and a creatinine clearance ≥50 ml/min.75 Theinvestigators found that the incremental cost-effectiveness
Apixaban Dabigatran
Anticoagulant
N e t c l i n i c a l b e n e fi t
Rivaroxaban Warfarin
0
3
2
1
CHADS2
2–6
1
0
4
Apixaban Dabigatran
Anticoagulant
Rivaroxaban Warfarin
HAS-BLED ≤2a b HAS-BLED ≥3
Figure 2 | Net clinical benefit of apixaban, dabigatran, rivaroxaban, and warfarin in prevention of ischaemic stroke andintracranial haemorrhage stratified by risk of ischaemic stroke (CHADS
2 score) and bleeding (HAS-BLED score).74 Results
for patients at a | low (HAS-BLED ≤2) and b | high (HAS-BLED ≥3) bleeding risk. Using warfarin therapy as a reference, allnovel oral anticoagulants show incremental net clinical benefit with increasing ischaemic risk, irrespective of bleeding risk.
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved

7/17/2019 nuevos anticoagulantes
http://slidepdf.com/reader/full/nuevos-anticoagulantes-56909d54767c6 8/118 | ADVANCE ONLINE PUBLICATION www.nature.com/nrcardio
ratio was highest with apixaban 5 mg, intermediate withdabigatran, and lowest with rivaroxaban.75 In a similarstudy, You concluded that cost-effectiveness was largelyinfluenced by TTR of INR in patients taking warfarin.76 Specifically, NOACs exhibited a trend towards decreasingcost-effectiveness as anticoagulation control with warfarinimproved.76 This trend persisted even after accounting forthe incremental service costs to improve anticoagulationcontrol, highlighting the dynamic cost savings that mightbe accrued with NOACs with better INR monitoring.However, the results of these studies should be interpretedcautiously because the estimations reflect assumptions ofstable anticoagulation efficacy, sufficient patient adher-ence, predefined patient profiles, long-term adverse out-comes based on clinical trials, and prespecified thresholdsfor cost-effectiveness.
Emerging therapeutic areas
Chronic kidney disease
Patients with chronic kidney disease (CKD) presentunique challenges for antithrombotic pharmacotherapybecause these individuals are at increased risk of bothischaemic and haemorrhagic complications comparedwith those with preserved renal function.77,78 CKD is alsoa common finding in patients with AF,79 highlighting thesubstantial overlap in risk factors common to both con-ditions. Moreover, CKD is an independent risk factorfor both thromboembolic and bleeding in the setting ofAF, rendering the use of oral anticoagulation in thesepatients controversial.80 Despite the excess risk of adversecardiovascular events in patients with CKD, anticoagu-lation with VKAs is underused owing to concomitantbleeding-related concerns.81,82 The use of VKAs in thishigh-risk group of patients has been called into ques-tion on the basis of the uncertain risk–benefit profile forthe routine use of warfarin. Shah and colleagues dem-onstrated that VKA use in patients with AF undergoingdialysis was associated with a similar risk of cardio-
vascular accident (stroke or transient ischaemic attack),but increased bleeding risk compared with patientswho did not receive a VKA.83 However, in a prospectiveSwedish registry of patients with myocardial infarctionand concomitant AF and CKD, patients treated with aVKA had a reduced 1-year risk of ischaemic events, withno increase in bleeding, irrespective of CKD severity.84 Notably, patients had a high percentage of TTR for goalINR, which might render these results less reproduciblein a real-world setting with less-optimal INR control. Inlight of these results, tailored therapy for this high-riskgroup of patients is warranted.
Post-hoc analyses of several NOAC trials have been
performed to examine the safety and eff icacy of theseagents compared with warfarin in the high-risk popu-lation of patients with CKD.85,86 Both apixaban andrivaroxaban undergo primarily hepatic elimination, butapproximately 25–30% of each drug is excreted by thekidneys. Therefore, these drugs were administered atreduced doses in the ARISTOTLE32 and ROCKET-AF33 trials, respectively. The substantial number of patientswith CKD enrolled in each study allowed valid com-parisons between the different NOACs and warfarin inthis important subgroup. Results from these analysesshowed that rates of both ischaemic and bleeding eventsincreased in a graded fashion with worsening renal func-
tion, irrespective of randomized assignment, consist-ent with previous reports.85,86 Rivaroxaban was associatedwith similar reductions in stroke and systemic embolismamong those with or without renal impairment, withoutevidence of interaction.85 Similar findings were observedwith apixaban.86 However, compared with warfarin,rivaroxaban was not associated with a significant reduc-tion in bleeding in patients with or without CKD.85 Bycontrast, apixaban was associated with an accentuatedreduction in bleeding with more severe levels of renalimpairment than with warfarin.86 Specifically, apixabanwas associated with a reduced risk of major bleedingamong patients with a creatinine clearance ≥80 ml/min
Apixaban Dabigatran
Anticoagulant
N u m b e r o f p a t i e n t s
Edoxaban Rivaroxaban
– 1,500
1,000
500
0
–500
–1,000
1,500NNT (stroke)
NNH (intracranial haemorrhage)
NNH (gastrointestinal bleeding)
Figure 3 | NNT and NNH calculated for the novel oralanticoagulants. A positive value for NNH quantifies thenumber of patients who would need to be treated toresult in a bleed from the new therapy, whereas a negativevalue indicates the number of patients who would needto be treated to prevent a bleed. Values for NNT andNNH derived from principal results of the phase IIIrandomized trials for each novel oral anticoagulant.21,32–34 NNT and NNH calculated from annual event rate forapixiban, dabigatran, and edoxaban, and total event ratefor rivaroxaban. Abbreviations: NNH, number needed toharm; NNT, number needed to treat.
Table 4 | Events prevented or caused per 1,000 patients treated with NOACs
Drug Strokes
prevented
ICHs
prevented
GI bleeding
induced
GI bleeding
prevented
Apixaban 3 5 0 1
Dabigatran 6 4 5 0
Edoxaban 2 5 3 0
Rivaroxaban 5 4 10 0
Calculations of the number needed to treat or harm based on data from phase III randomized trials inwhich each NOAC was compared with warfarin.21,32–34 Data for dabigatran and edoxaban calculated fromhigh-dose regimens. Number needed to treat or harm calculated from annual event rate for apixaban,dabigatran, and edoxaban, and total event rate for rivaroxaban. Abbreviations: GI, gastrointestinal; ICH,intracranial haemorrhage; NOAC, novel oral anticoagulant.
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved

7/17/2019 nuevos anticoagulantes
http://slidepdf.com/reader/full/nuevos-anticoagulantes-56909d54767c6 9/11
7/17/2019 nuevos anticoagulantes
http://slidepdf.com/reader/full/nuevos-anticoagulantes-56909d54767c6 10/1110 | ADVANCE ONLINE PUBLICATION www.nature.com/nrcardio
1. Gage, B. F. et al. Validation of clinicalclassification schemes for predicting stroke:results from the national registry of atrialfibrillation. JAMA 285, 2864–2870 (2001).
2. Antman, E. M. et al. The TIMI risk score forunstable angina/non-ST elevation MI: a methodfor prognostication and therapeutic decisionmaking. JAMA 284, 835–842 (2000).
3. Lip, G. Y., Nieuwlaat, R., Pisters, R., Lane, D. A.& Crijns, H. J. Refining clinical risk stratification
for predicting stroke and thromboembolism inatrial fibrillation using a novel risk factor-basedapproach: the Euro Heart Survey on AtrialFibrillation. Chest 137, 263–272 (2010).
4. Mehran, R. et al. Impact of bleeding on mortalityafter percutaneous coronary intervention:results from a patient-level pooled analysis ofthe REPLACE-2 (Randomized Evaluation of PCILinking Angiomax to Reduced Clinical Events),ACUITY (Acute Catheterization and UrgentIntervention Triage Strategy), and HORIZONS-AMI(Harmonizing Outcomes With Revascularizationand Stents in Acute Myocardial Infarction) trials.
JACC Cardiovasc. Interv. 4, 654–664 (2011).5. Mehran, R. et al. Standardized bleeding definitions
for cardiovascular clinical trials: a consensusreport from the Bleeding Academic Research
Consortium. Circulation 123, 2736–2747 (2011).6. Pisters, R. et al. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleedingin patients with atrial fibrillation: the Euro HeartSurvey. Chest 138, 1093–1100 (2010).
7. Lip, G. Y., Frison, L., Halperin, J. L. & Lane, D. A.Comparative validation of a novel risk score forpredicting bleeding risk in anticoagulatedpatients with atrial fibrillation: the HAS-BLED(Hypertension, Abnormal Renal/Liver Function,Stroke, Bleeding History or Predisposition, LabileINR, Elderly, Drugs/Alcohol Concomitantly)score. J. Am. Coll. Cardiol. 57, 173–180 (2011).
8. Fang, M. C. et al. A new risk scheme to predictwarfarin-associated hemorrhage: the ATRIA(Anticoagulation and Risk Factors in AtrialFibrillation) study. J. Am. Coll. Cardiol. 58, 395–401
(2011).9. Almquist, H. J., Mecchi, E. & Klose, A. A.Estimation of the antihaemorrhagic vitamin.Biochem. J. 32, 1897–1903 (1938).
10. Stehle, S., Kirchheiner, J., Lazar, A. & Fuhr, U.Pharmacogenetics of oral anticoagulants:a basis for dose individualization.Clin. Pharmacokinet. 47, 565–594 (2008).
11. Bousser, M. G. et al. Comparison of idraparinuxwith vitamin K antagonists for preventionof thromboembolism in patients with atrialfibrillation: a randomised, open-label, non-inferiority trial. Lancet 371, 315–321 (2008).
12. Greenblatt, D. J. & von Moltke, L. L. Interactionof warfarin with drugs, natural substances, andfoods. J. Clin. Pharmacol. 45, 127–132 (2005).
13. Hankey, G. J. & Eikelboom, J. W. Dabigatran
etexilate: a new oral thrombin inhibitor.Circulation 123, 1436–1450 (2011).14. Laux, V., Perzborn, E., Kubitza, D. & Misselwitz, F.
Preclinical and clinical characteristics ofrivaroxaban: a novel, oral, direct factor Xa inhibitor.Semin. Thromb. Hemost. 33, 515–523 (2007).
15. Barrett, Y. C., Wang, Z., Frost, C. & Shenker, A.Clinical laboratory measurement of directfactor Xa inhibitors: anti-Xa assay is preferableto prothrombin time assay. Thromb. Haemost. 104, 1263–1271 (2010).
16. De Caterina, R. et al. New oral anticoagulants inatrial fibrillation and acute coronary syndromes:ESC Working Group on Thrombosis–Task Forceon Anticoagulants in Heart Disease positionpaper. J. Am. Coll. Cardiol. 59, 1413–1425(2012).
17. Scaglione, F. New oral anticoagulants:comparative pharmacology with vitamin Kantagonists. Clin. Pharmacokinet. 52, 69–82(2013).
18. Harder, S. & Graff, J. Novel oral anticoagulants:clinical pharmacology, indications and practicalconsiderations.Eur. J. Clin. Pharmacol. 69,1617–1633 (2013).
19. Pritchett, E. L. Management of atrial fibrillation.N. Engl. J. Med. 326, 1264–1271 (1992).
20. Wolf, P. A., Abbott, R. D. & Kannel, W. B. Atrialfibrillation: a major contributor to stroke in theelderly: the Framingham Study. Arch. Intern. Med. 147, 1561–1564 (1987).
21. Connolly, S. J. et al. Dabigatran versus warfarinin patients with atrial fibrillation. N. Engl. J. Med. 361, 1139–1151 (2009).
22. Alberts, M. J., Eikelboom, J. W. & Hankey, G. J.Antithrombotic therapy for stroke prevention innon-valvular atrial fibrillation. Lancet Neurol. 11,1066–1081 (2012).
23. Gage, B. F. et al. Selecting patients with atrialfibrillation for anticoagulation: stroke riskstratification in patients taking aspirin.Circulation 110, 2287–2292 (2004).
24. Warfarin versus aspirin for prevention ofthromboembolism in atrial fibrillation: Stroke
Prevention in Atrial Fibrillation II study. Lancet 343, 687–691 (1994).25. Hart, R. G., Pearce, L. A. & Aguilar, M. I. Meta-
analysis: antithrombotic therapy to preventstroke in patients who have nonvalvular atrialfibrillation. Ann. Intern. Med. 146, 857–867(2007).
26. van Walraven, C. et al. Oral anticoagulantsvs aspirin in nonvalvular atrial fibrillation:an individual patient meta-analysis. JAMA 288,2441–2448 (2002).
27. Connolly, S. et al. Clopidogrel plus aspirin versusoral anticoagulation for atrial fibrillation in theAtrial fibrillation Clopidogrel Trial with Irbesartanfor prevention of Vascular Events (ACTIVE W):a randomised controlled trial. Lancet 367,1903–1912 (2006).
28. Connolly, S. J. et al. Effect of clopidogrel addedto aspirin in patients with atrial fibrillation.N. Engl. J. Med. 360, 2066–2078 (2009).
29. Connolly, S. J. et al. Net clinical benefit of addingclopidogrel to aspirin therapy in patients withatrial fibrillation for whom vitamin K antagonistsare unsuitable. Ann. Intern. Med. 155, 579–586(2011).
30. Stroke Prevention in Atrial FibrillationInvestigators. Adjusted-dose warfarin versus low-intensity, fixed-dose warfarin plus aspirin forhigh-risk patients with atrial fibrillation: StrokePrevention in Atrial F ibrillation III randomisedclinical trial. Lancet 348, 633–638 (1996).
31. Flaker, G. C. et al. Risks and benefits ofcombining aspirin with anticoagulant therapy inpatients with atrial fibrillation: an exploratory
analysis of stroke prevention using an oralthrombin inhibitor in atrial fibrillation (SPORTIF)trials. Am. Heart J. 152, 967–973 (2006).
32. Granger, C. B. et al. Apixaban versus warfarinin patients with atrial fibrillation. N. Engl. J. Med. 365, 981–992 (2011).
33. Patel, M. R. et al. Rivaroxaban versus warfarin innonvalvular atrial fibrillation. N. Engl. J. Med. 365,883–891 (2011).
34. Giugliano, R. P. et al. Edoxaban versus warfarinin patients with atrial fibrillation. N. Engl. J. Med. 369, 2093–2104 (2013).
35. Ruff, C. T. et al. Comparison of the efficacy andsafety of new oral anticoagulants with warfarinin patients with atrial fibrillation: a meta-analysisof randomised trials. Lancet 383, 955–962(2014).
36. White, H. D. et al. Comparison of outcomesamong patients randomized to warfarintherapy according to anticoagulant control:results from SPORTIF III and V. Arch. Intern. Med. 167, 239–245 (2007).
37. Albers, G. W. et al. Ximelagatran vs warfarin forstroke prevention in patients with nonvalvularatrial fibrillation: a ransomized trial. JAMA 293,690–698 (2005).
38. Rose, A. J. et al. Risk-adjusted percent time
in therapeutic range as a quality indicator foroutpatient oral anticoagulation: results of theVeterans Affairs Study to Improve Anticoagulation(VARIA). Circ. Cardiovasc. Qual. Outcomes 4,22–29 (2011).
39. Wallentin, L. et al. Efficacy and safety ofdabigatran compared with warfarin at differentlevels of international normalised ratiocontrol for stroke prevention in atrial fibrillation:an analysis of the RE-LY trial. Lancet 376,975–983 (2010).
40. Schneeweiss, S., Gagne, J. J., Patrick, A. R.,Choudhry, N. K. & Avorn, J. Comparative efficacyand safety of new oral anticoagulants in patientswith atrial fibrillation.Circ. Cardiovasc. Qual.
Outcomes 5, 480–486 (2012).41. Bucher, H. C., Guyatt, G. H., Griffith, L. E.
& Walter, S. D. The results of direct and indirecttreatment comparisons in meta-analysis ofrandomized controlled trials. J. Clin. Epidemiol. 50, 683–691 (1997).
42. Libby, P. Mechanisms of acute coronarysyndromes and their implications for therapy.N. Engl. J. Med. 368, 2004–2013 (2013).
43. Wallentin, L. et al. Ticagrelor versus clopidogrelin patients with acute coronary syndromes.N. Engl. J. Med. 361, 1045–1057 (2009).
44. Anand, S. S. & Yusuf, S. Oral anticoagulanttherapy in patients with coronary artery disease:a meta-analysis. JAMA 282, 2058–2067 (1999).
45. Bertrand, M. E. et al. Randomized multicentercomparison of conventional anticoagulationversus antiplatelet therapy in unplannedand elective coronary stenting: the Full
Anticoagulation Versus Aspirin and Ticlopidine(FANTASTIC) study. Circulation 98, 1597–1603(1998).
46. Leon, M. B. et al. A clinical trial comparing threeantithrombotic-drug regimens after coronary-artery stenting. N. Engl. J. Med. 339, 1665–1671(1998).
47. Oldgren, J. et al. Dabigatran vs. placebo inpatients with acute coronary syndromes on dualantiplatelet therapy: a randomized, double-blind,phase II trial. Eur. Heart J. 32, 2781–2789(2011).
48. Alexander, J. H. et al. Apixaban, an oral, direct,selective factor Xa inhibitor, in combinationwith antiplatelet therapy after acute coronarysyndrome: results of the Apixaban for Preventionof Acute Ischemic and Safety Events (APPRAISE)
trial. Circulation 119, 2877–2885 (2009).49. Mega, J. L. et al. Rivaroxaban versus placeboin patients with acute coronary syndromes(ATLAS ACS-TIMI 46): a randomised, double-blind, phase II trial. Lancet 374, 29–38 (2009).
50. Alexander, J. H. et al. Apixaban with antiplatelettherapy after acute coronary syndrome. N. Engl.
J. Med. 365, 699–708 (2011).51. Mega, J. L. et al. Rivaroxaban in patients with a
recent acute coronary syndrome. N. Engl. J. Med. 366, 9–19 (2012).
52. O’Gara, P. T. et al. 2013 ACCF/AHA guideline forthe management of ST-elevation myocardialinfarction: a report of the American College ofCardiology Foundation/American HeartAssociation Task Force on Practice Guidelines.
J. Am. Coll. Cardiol. 61, e78–e140 (2013).
REVIEWS
© 2014 Macmillan Publishers Limited. All rights reserved

7/17/2019 nuevos anticoagulantes
http://slidepdf.com/reader/full/nuevos-anticoagulantes-56909d54767c6 11/11| |
53. Jneid, H. et al. 2012 ACCF/AHA focused updateof the guideline for the management of patientswith unstable angina/non-ST-elevation myocardialinfarction (updating the 2007 guideline andreplacing the 2011 focused update): a report ofthe American College of Cardiology Foundation/American Heart Association Task Forceon Practice Guidelines. J. Am. Coll. Cardiol. 60,645–681 (2012).
54. Ageno, W. et al. Oral anticoagulant therapy:
antithrombotic therapy and prevention ofthrombosis, 9th ed: American College of ChestPhysicians evidence-based clinical practiceguidelines.Chest 141 (Suppl.), e44S–e88S(2012).
55. Lassen, M. R. et al. Apixaban or enoxaparinfor thromboprophylaxis after knee replacement.N. Engl. J. Med. 361, 594–604 (2009).
56. Lassen, M. R. et al. Rivaroxaban versusenoxaparin for thromboprophylaxis after total kneearthroplasty. N. Engl. J. Med. 358, 2776–2786(2008).
57. Turpie, A. G. et al. Rivaroxaban versusenoxaparin for thromboprophylaxis after totalknee arthroplasty (RECORD4): a randomisedtrial. Lancet 373, 1673–1680 (2009).
58. Agnelli, G. et al. Oral apixaban for the treatment
of acute venous thromboembolism. N. Engl. J.Med. 369, 799–808 (2013).
59. Schulman, S. et al. Dabigatran versuswarfarin in the treatment of acute venousthromboembolism.N. Engl. J. Med. 361,2342–2352 (2009).
60. Schulman, S. et al. Treatment of acute venousthromboembolism with dabigatran or warfarin andpooled analysis. Circulation 129, 764–772 (2014).
61. Büller, H. R. et al. Oral rivaroxaban for thetreatment of symptomatic pulmonary embolism.N. Engl. J. Med. 366, 1287–1297 (2012).
62. Bauersachs, R. et al. Oral rivaroxaban forsymptomatic venous thromboembolism. N. Engl.
J. Med. 363, 2499–2510 (2010).63. Büller, H. R. et al. Edoxaban versus warfarin
for the treatment of symptomatic venous
thromboembolism.N. Engl. J. Med. 369,1406–1415 (2013).64. Schulman, S. & Kearon, C. Definition of
major bleeding in clinical investigationsof antihemostatic medicinal products innon-surgical patients. J. Thromb. Haemost. 3,692–694 (2005).
65. Gage, B. F. et al. Validation of clinicalclassification schemes for predicting stroke:results from the National Registry of AtrialFibrillation. JAMA 285, 2864–2870 (2001).
66. January, C. T. et al. 2014 AHA/ACC/HRSguideline for the management of patients withatrial fibrillation: a report of the American Collegeof Cardiology/American Heart Association TaskForce on Practice Guidelines and the HeartRhythm Society. J. Am. Coll. Cardiol. http://
dx.doi.org/10.1016/j.jacc.2014.03.022.67. Camm, A. J. et al. Guidelines for themanagement of atrial fibrillation: the Task
Force for the Management of Atrial Fibrillationof the European Society of Cardiology (ESC).Eur. Heart J. 31, 2369–2429 (2010).
68. Camm, A. J. et al. 2012 focused update of theESC guidelines for the management of atrialfibrillation: an update of the 2010 ESCguidelines for the management of atrialfibrillation: developed with the specialcontribution of the European Heart RhythmAssociation.Eur. Heart J. 33, 2719–2747
(2012).69. Steinberg, B. A. et al. Lack of concordancebetween empirical scores and physicianassessments of stroke and bleeding risk inatrial fibrillation: results from the OutcomesRegistry for Better Informed Treatment of AtrialFibrillation (ORBIT-AF) registry. Circulation 129,2005–2012 (2014).
70. Fang, M. C. et al. Death and disability fromwarfarin-associated intracranial and extracranialhemorrhages. Am. J. Med. 120, 700–705(2007).
71. Hylek, E. M. et al. Effect of intensity of oralanticoagulation on stroke severity andmortality in atrial fibrillation. N. Engl. J. Med. 349,1019–1026 (2003).
72. Devereaux, P. J.et al. Differences between
perspectives of physicians and patients onanticoagulation in patients with atrial fibrillation:observational study. BMJ 323, 1218–1222(2001).
73. Lane, D. A. & Lip, G. Y. Use of theCHA
2DS
2-VASc and HAS-BLED scores to aid
decision making for thromboprophylaxis innonvalvular atrial fibrillation. Circulation 126,860–865 (2012).
74. Banerjee, A., Lane, D. A., Torp-Pedersen, C.& Lip, G. Y. Net clinical benefit of new oralanticoagulants (dabigatran, rivaroxaban,apixaban) versus no treatment in a ‘real world’atrial fibrillation population: a modellinganalysis based on a nationwide cohort study.Thromb. Haemost. 107, 584–589 (2012).
75. Harrington, A. R., Armstrong, E. P., Nolan, P. E. Jr
& Malone, D. C. Cost-effectiveness of apixaban,dabigatran, rivaroxaban, and warfarin forstroke prevention in atrial fibrillation. Stroke 44,1676–1681 (2013).
76. You, J. H. Novel oral anticoagulants versuswarfarin therapy at various levels ofanticoagulation control in atrial fibrillation—a cost-effectiveness analysis. J. Gen. Intern.
Med. 29, 438–446 (2014).77. Latif, F. et al. In-hospital and 1-year outcomes
among percutaneous coronary interventionpatients with chronic kidney disease in the eraof drug-eluting stents: a report from the EVENT(Evaluation of Drug Eluting Stents and IschemicEvents) registry. JACC Cardiovasc. Interv . 2,37–45 (2009).
78. Tonelli, M. et al. Risk of coronary events in
people with chronic kidney disease comparedwith those with diabetes: a population-levelcohort study. Lancet 380, 807–814 (2012).
79. Soliman, E. Z. et al. Chronic kidney disease andprevalent atrial fibrillation: the Chronic RenalInsufficiency Cohort (CRIC). Am. Heart J. 159,1102–1107 (2010).
80. Olesen, J. B. et al. Stroke and bleeding in atrialfibrillation with chronic kidney disease. N. Engl. J.
Med. 367, 625–635 (2012).81. Johnston, J. A. et al. Predictors of warfarin use
among Ohio Medicaid patients with new-onsetnonvalvular atrial fibrillation. Arch. Intern. Med.
163, 1705–1710 (2003).82. Marinigh, R., Lane, D. A. & Lip, G. Y. Severerenal impairment and stroke prevention in atrialfibrillation: implications for thromboprophylaxisand bleeding risk. J. Am. Coll. Cardiol. 57,1339–1348 (2011).
83. Shah, M. et al. Warfarin use and the risk forstroke and bleeding in patients with atrialfibrillation undergoing dialysis. Circulation 129,1196–1203 (2014).
84. Carrero, J. J. et al. Warfarin, kidney dysfunction,and outcomes following acute myocardialinfarction in patients with atrial fibrillation. JAMA 311, 919–928 (2014).
85. Fox, K. A. et al. Prevention of stroke andsystemic embolism with rivaroxaban comparedwith warfarin in patients with non-valvular atrial
fibrillation and moderate renal impairment.Eur. Heart J. 32, 2387–2394 (2011).86. Hohnloser, S. H. et al. Efficacy of apixaban when
compared with warfarin in relation to renalfunction in patients with atrial fibrillation:insights from the ARISTOTLE trial. Eur. Heart J. 33, 2821–2830 (2012).
87. Dewilde, W. J. M. et al. Use of clopidogrelwith or without aspirin in patients taking oralanticoagulant therapy and undergoingpercutaneous coronary intervention: an open-label, randomised, controlled trial. Lancet 381,1107–1115 (2013).
88. Gibson, C. M. et al. Reduction of stentthrombosis in patients with acute coronarysyndromes treated with rivaroxaban in ATLAS-ACS 2 TIMI 51. J. Am. Coll. Cardiol. 62, 286–290
(2013).89. US National Library of Medicine. ClinicalTrials.gov [online], http://clinicaltrials.gov/ct2/show/NCT02024230 (2014).
90. Oldgren, J. et al. New oral anticoagulants inaddition to single or dual antiplatelet therapyafter an acute coronary syndrome: a systematicreview and meta-analysis. Eur. Heart J. 34,1670–1680 (2013).
91. van der Hulle, T. et al. Effectiveness and safetyof novel oral anticoagulants as compared withvitamin K antagonists in the treatment of acutesymptomatic venous thromboembolism: asystematic review and meta-analysis. J. Thromb.
Haemost. 12, 320–328 (2014).
Author contributions
All the authors researched data for the article,discussed its content, and wrote, reviewed, andedited the manuscript before submission.
REVIEWS