-
The PDF of the article you requested follows this cover
page.
This is an enhanced PDF from The Journal of Bone and Joint
Surgery
1976;58:195-201. J Bone Joint Surg Am.NK Poppen and PS
Walker
Normal and abnormal motion of the shoulder
This information is current as of January 26, 2010
Reprints and Permissions
Permissions] link. and click on the [Reprints
andjbjs.orgarticle, or locate the article citation on
to use material from thisorder reprints or request
permissionClick here to
Publisher Information
www.jbjs.org20 Pickering Street, Needham, MA 02492-3157The
Journal of Bone and Joint Surgery
http://www2.ejbjs.org/misc/reprints_perms.dtlhttp://www.jbjs.orghttp://www.jbjs.org
-
Or,
(4)
References
CORTICAL BONE ATROPHY SECONDARY TO FIXATION 195
VOL. 58-A, NO. 2, MARCH 1976
(2) showed one-to-one correspondence between o . and
P. Hence, the stress calculated when P = maz the ulti-
mate bending strength (or stress crc).
The flexural modulus of elasticity (E) of the bonespecimen can
also be calculated using the following
formula :
(3) Yq(4 (L.)() (a +--)
where Y(,( .4 5 the vertical deformation at point A (Fig.
2).
E= Pa 6IY, . \ 2
= 8.64 (-i-- (L\Y(,( A! \bh3
wherea = L = 1.2 cm.
Now atA the Instron cross-head displacement, andthe initial
slope ofthe load-deformation diagram (Fig. 2) is
at A- Therefore, E can be calculated from equation (4).
I . AKESON, W. H., Woo. S. L-Y; COUTTS, R. D.; MATTHEWS, J. V. ;
GON5ALVES, M.; and AMIEL, D.: Quantitative Histological Evaluation
ofEarly Fracture Healing of Cortical Bones Immobilized by Stainless
Steel and Composite Plates. CaIc. Tissue Res. , 19: 27-37,
1975.
2. BARDOS, D. L.: An Evaluation ofTi-6Al-4V Alloy forOrthopedic
Applications. In Proceedings ofthe Orthopaedic Research Society. J.
Boneand Joint Surg. ,56-A: 847, June 1974.
3. BAUMF.ISTER, T.: Marks Standard Handbook for Mechanical
Engineers. Ed. 7, chapters 5-31. New York, McGraw-Hill, 1967.4.
BYNUM. D. . JR.: ALLEN, G. F.; RAY, D. R.; and LEDBETTER, W. B.: In
Vitro Performance of Installed Internal Fixation Plates in
Compression.
J. Biomed. Mat. Res., 5: 389-405, 1971.5. CURREY, J. D.: The
Mechanical Properties of Bone. Clin. Orthop., 73: 210-231, 1970.6.
GODFREY. J. L.: Looking at Bone Plates and Screws. Eng. in Med., 1:
17-18, 1971.7. HICKS, J. H.: The Fixation of Fracture Using Plates.
Eng. in Med., 2: 60-63, 1973.8. LINDAHI., OLov: The Rigidity of
Fracture Immobilization with Plates. Acta Orthop. Scandinavica, 38:
101-114, 1967.9. ROMANUS, B.: Physical Properties and Chemical
Content of Canine Femoral Cortical Bone in Nutritional Osteopenia.
Acta Orthop. Scan-
dinavica, Supplementum 155, 1974.
10. UHTHOFF, H. K., and DUBUC, F. L.: Bone Structure Changes in
the Dog Under Rigid Internal Fixation. Clin. Orthop., 81: 165-170,
1971.1 1 . Woo, S. L-Y; SIMoN, B. R.; and AKESON, W. H.: Evaluation
of Rigidity of Internal Fixation Plate on Long Bone Remodeling.
Abstract
published in Proceedings of the Twenty-eighth meeting of ACEMB,
p. 150, New Orleans, Louisiana, September 1975.12. Woo, S. L-Y:
AKESON. W. H.; LEVENETZ, B.; COUTTS, R. D.; MATTHEWS, J. V.; and
AMIEL, D.: Potential Application ofGraphite Fiber and
Methyl Methacrylate Resin Composites as Internal Fixation
Plates. J. Biomed. Mat. Res., 8: 321-338, 1974.
Normal and Abnormal Motion of the Shoulder
BY NORMAN K. POPPEN, M.D.*, AND PETER S. WALKER, PH.D.t, NEW
YORK, N.Y.
From The Hospitalfor Special Surgery, Affiliated with The New
York Hospital-
Cornell Unisersitv Medical College. New York Cit
ABSTRACT: The roentgenographic parameters ofmotion in normal and
abnormal shoulders, including
the movement of the scapula, arm angle, glenohumeral
angle, scapulothoracic angle, excursion of the humeralhead, and
instant center of motion for abduction in theplane of the scapula,
were determined in twelve normalsubjects and fifteen patients. The
scapula rotated ex-
ternally with abduction. The ratio of glenohumeral
toscapulothoracic movement was 5:4 after about 30 de-
grees of abduction. The center of rotation of the
glenohumeral joint for abduction in the plane of the
scapula was located within six millimeters of thegeometric
center of the humeral ball. The average ex-
cursion of the humeral ball on the face of the glenoid inthe
superoinferior plane between each 30-degree arc of
motion was less than 1 .5 millimeters in normal sub-
jects. Significant previous injury resulting in
abnormalmechanics of the shoulder joint was associated withabnormal
values for excursion of the instant center and
* 535 East 70th Street, New York, N.Y. 10021.t Reprint requests
to Dr. Walker, Codman and Shurtleff, Inc.,
Randolph, Massachusetts 02368.
of the humeral head. An abnormal glenohumeral-to-scapulothoracic
ratio was associated with significantpain in the shoulder. The fact
that these variousparameters were sensitive indicators of normal
and
abnormal motion raises the possibility of diagnostic
clinical application.
Many authors 2,3.4.5.6.7,8,1O.II.I2,13 have pointed out the
complexity of the shoulder and nearly a century ago 2.3 the
interplay of the sternoclavicular, acromioclavicular,
scapulothoracic, and glenohumeral joints was described. It
has been suggested 11.12 that true abduction of the arm
should not be in the coronal plane, but rather in the plane
of the scapula which is angled 30 to 45 degrees anteriorto the
coronal plane, because in the scapular plane the in-
ferior part of the capsule is not twisted and the deltoid
andsupraspinatus are optimally aligned for elevation of the
arm. Inman and co-workers showed that all of the joints in
the shoulder girdle move simultaneously, and that in the
motion of abduction the glenohumeral joint moves twice
as much as the scapulothoracic joint. Saha described a
zero position of the humeral head on the glenoid basedon how
much rolling and sliding takes place at the
-
I 96 N. K. POPPEN AND P. 5. WALKER
THE JOURNAL OF BONE AND JOINT SURGERY
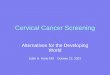
FIG. I
Reference axes are taken in the humerus: x.y, scapula x,y, and
bodyx,Y. The line x is a perpendicular to the true )Fthe axis ofThe
humerus)through O. the center of the humeral head. The line v
passes through thesuperior and inferior edges of the glenoid and .v
is the mid-line of thescapular spine. O is chosen at the center of
the glenoid fossa and hence
the x-axis passes through this point perpendicular to the
y-axis.
glenohumeral joint. Dernpster applied the concept of treat-
ing the upper extremity as a series of rigid links to
measure
the contributions made by each joint of the upper extremity
to bring the hand to a position where it can perform a re-
quired task. Freedman and Munro and Doody and as-
sociates analyzed abduction in the scapular plane and
found a ratio of 3:2 between glenohumeral and
scapulothoracic motion. This ratio was not substantially
affected when there was resistance to movement.
In this study we attempted to measure two other pa-
rameters of motion, as well as the angular movements of
the humerus and scapula when the arm is abducted in the
scapular plane: namely, the centers of rotation of the hu-
meral ball in relation to the scapula, and the excursion of
the
ball on the face of the scapula. Using the various mea-
surernents we were able to compare the motion of the nor-
mal and the abnormal shoulder.
Subjects Studied
Materials and Methods
The main motion we studied was abduction ofthe arm
in the plane of the scapula. We had twenty-seven subjects,
of whom twelve were asymptomatic, normal volunteers
twenty-two to sixty-three years old, and fifteen were pa-
FIG. 2
Three sets of x-y axes are taken to define the joints positions.
XY isfixed in the thorax, xy is fixed in the scapula, and ,y is
fixed in thehumerus. 0A #{176}GH #{176}ST#{149}The arm angle (eA)
is the angle formed bythe y-axis of the humerus and a line parallel
to the Y-axis of the body.The glenohumeral angle (O(;H) 15 defined
as the angle formed by they-axis of the humerus and the y-axis of
the scapula. The scapulothoracicangle (O) is the angle formed by
the y-axis of the scapula and a lineparallel to the Y-axis of the
body.
tients seventeen to seventy-two years old who had lesions
of the shoulder and were about to have arthrography. We
adopted a technique similar to that of Freedman and
Munro to obtain roentgenograms in the plane of the
scapula with the arm in neutral rotation. An anteropos-
tenor roentgenograrn was made of each shoulder with the
patient standing with the torso at a 30-degree angle to the
plane of the roentgenogram. When the arm was abducted
to each of the required positions, the plane of abduction
was parallel to the plane of the roentgenogram and the
amount of abduction was gauged with reference to the axis
of the body.
Selection of Reference Axes
A study of the motion of the shoulder must start with
a definition of the axes in each of the two moving parts
(humerus and scapula) relative to the stationary part, the
torso (Fig. 1). The geometric center of the humeral head
(Oh) is chosen as one reference point because the curvatureis
sufficiently close to uniform for this purpose, and the
center can be found by a simple geometric construction.
The reference point for the scapula (Os) was chosen to be
the center of a line joining the limits of the glenoid
fossa.
On each roentgenogram the three sets of axes were drawn;
the axes of the torso were designated X,Y, the axes of the
scapula, x,y, and the axes of the humerus, x,y (Fig. 2).
Because Figure 2 was drawn from a roentgenograrn made
with the subject facing the x-ray source at a 30-degree
angle, in other words in the plane of the scapula, the XY
axes are in this plane and not in the coronal plane of thebody.
The arm angle, glenohurneral angle, and
scapulothoracic angle are defined in Figure 2.
Several roentgenograms were made for each subject,
at 30-degree intervals from the dependent arm position up
-
A2
NORMAL AND ABNORMAL MOTION OF THE SHOULDER I 97
VOL. 58-A. NO. 2. MARCH 976
to maximum abduction in the plane of the scapula. Be-cause of
the inevitable minor variations in a sequential set
of roentgenograms, a method was needed to obtain satis-
factory superposition of the sets of roentgenograms. A
master tracing was made of the scapula and humerus at 60
degrees of abduction (mid-range) and the axes were
marked. Each of the other roentgenograms (made at 0, 30,
90, 120, and I 50 degrees and at maximum abduction) was
superimposed over the master tracing as closely as possi-
ble and the individual axes then were drawn. In this way,
sequential patterns of movement were obtained.
Definitions of Parameters
Still referring to Figure 2, various parameters of in-
terest can now be defined. The tnosement ofthe scapula onthe
thorax can be defined by following one point and one
angle, that is, O and the scapulothoracic angle (OST). In-
formation on the rotation ofthe scapula can be obtained by
determining the center of rotation of the scapula for each
30-degree interval considered. The directions of measure-
ment must be defined relative to the several axes. Also,
changes in and #{176}ST can be related to the arm angle
(OA) and the ratio OGH:OST can be determined.The excursion or
sliding of the hurneral head on the
face of the glenoid (the rise and fall of the geometric
center
of the ball, Oh) can be expressed as the parameter e, the
distance on the y-axis that #{176}h lies above or below the
center of the glenoid (Os).
The motion of the humerus on the glenoid can be de-
scribed in terms of the center of rotation. The method for
determining it is shown in Figure 3. For each 30-degree
interval of the arm angle between two sequential
A1
FIG. 3
Two roentgenograms of the same individual with different angles
ofabduction can be used to determine the center of rotation for the
anglemoved. This is done as follows: Draw the set of axes based on
thehumerus for the tWo roentgenograms; select a single arbitrary
interval
(OA) which is measured on the four lines of the two axes (A,01,
B1,01, BI)4; bisect the lines A,.A and B,B: erect perpendiculars
tothose lines: and C (center of rotation) is the intersection of
those perpen-
diculars.
roentgenograrns of the same subject, the center of rotation
for that arc of motion is the pivot point about which thehumerus
appears to rotate. The center of rotation of the
scapula on the thorax was determined by a similar tech-
nique.
Results
A typical set of sequential roentgenograms from a
normal subject (Fig. 4) illustrates the information ob-
tamed. In the relaxed position of the extremity with the
subject standing, the average arm angle (OA) for the fifteen
normal subjects was 2.5 degrees, with a range of from -3
to +9 degrees. The average scapulothoracic angle (OsT)was -4.7
degrees, with a range of from - I I to + 10 de-
grees. Freedman and Munro obtained a mean value of
-5.3 degrees, although Basmajian and Bazant stated that
itinvariably faced somewhat upward.
In moving the extremity, in normal subjects the rela-
tionships among 0A #{176}GH and #{176}STwere different (Fig.
5)
in the arc of motion between 0 and 30 degrees of abduction,as
compared with the arc of motion between 30 and 120
degrees. In all of our twenty-seven subjects as well as in
those of Inman and associates, Freedman and Munro, and
Saha results are in reasonable agreement. The averagearm angle
measured from our roentgenograms with thearm in approximately 30
degrees of abduction was in fact
24 degrees. For the arm angle range of 2.5 to 24 degrees,
the ratio of the glenohumeral angle to the scapulothoracic
angle was 4.3: 1 . In other words, the scapula moved only
slightly compared with the humerus. The mean regression
lines were drawn for the range 24 degrees to maximum ab-
duction. For the twelve normal subjects, as well as for
three patients who were found to be normal in all respects,
the equations of the regression lines were: #{176}(;H
+ 12.6 and #{176}ST #{176}-40A 12.4. These indicate that in
that range (24 degrees to maximum arm angle) the ratio of
glenohumeral to scapulothoracic motion was actually 5:4
or 1 .25: 1 , meaning that there was not a great deal of
dif-ference in the amounts by which they rotated. Freedmanand
Munros ratio was 1.35:1 for the range 0 to 135 de-
grees, which is not very different from ours. Saha how-ever,
found an average ratio of 2.34: 1 for the range 30 to
135 degrees for abduction in the plane of the scapula. Our
data are in contrast to the findings of Inman and associates
for abduction in the coronal plane; they stated that at the
glenohumeral and scapulothoracic articulations, the ratio,from
almost the beginning to the termination of the arc, isrespectively
two to one
Typically, as abduction progressed the glenoid face
moved medially, then tilted upward, and finally moved
upward somewhat as the arm was brought to maximum
elevation (Fig. 6). These motions can be expressed in
terms of the center of rotation of the scapula with respect
to the fixed axes in the body. From 0 to 30 degrees, the
scapula rotated about its lower mid-portion, and then from
60 degrees onward the center of rotation shifted towards
the glenoid, so that it was rotating about that area,
result-
-
Sequential roentgenograms made in abduction in the plane of the
scapula.
Y
GLtNO-HUStFRA A\C11 OGHSCAPUO-THORACI( A.GF Si
Tfus stud
- - - Inman Sarclers H. Abbott 1H44-.- SaGa 11
U Doodv freedar) Valerland IH7O00 .Freedman \lunro 1%6 7
V/
V
0
60 -
30
800
Fi;. 5
The relationships between the glenohumeral angle (();j) and the
armangle (OA) and between the scapulothoracic angle (O) and the
armangle. Each letter 0 denotes the O value for a representative
individualpatient for the corresponding #{176}A#{149}
x
ARM ANGLE 9
198 N. K. POPPEN AND P. S. WALKER
THE JOURNAL OF BONE AND JOINT SURGERY
ing in a large lateral displacement of the inferior tip of
the
scapula.
By plotting the positions of the tips of the acromion
and the coracoid it was clear that the scapula twisted about
its x-axis. Figure 7 shows how this was detected on a plain
roentgenogram. Assume that there is rotation about O in a
counter-clockwise direction. The coracoid tip will move
predominantly upward, while the acromion tip will move
backwards in the same transverse plane in relation to the
face of the glenoid. Hence, by measuring the upward
movement of the coracoid with respect to the face of the
glenoid, the angle of rotation can be calculated. The rota-
tion could, of course, be about the same axis parallel to x.
For all subjects, patients as well as normal individuals,
the
acrornion remained stationary with respect to the face of
the glenoid except at high abduction angles when it tended
120
to rotate slightly downwards, as would be predicted (Figs.
6 and 7). This is consistent with a counter-clockwise rota-
tion (twisting) of the scapula on abduction of the arm that
occurs in the plane of the scapula. For the fifteen normal
subjects, the regression line for the twisting was: 0xs =
#{176}590ST with a correlation coefficient of 0.83.This means
that the twisting angle was 0.59 times the
FIG. 6
The motion of the scapula in its own plane is defined by the
position ofthe glenoid and the centers of rotation relative to
fixed XY axes in thebody. The center of rotation of the scapula
begins low in the body of thescapula and progresses upwards toward
the glenoid. (Asterisk denotes
center of rotation for the specific intervals, 0 to 30 degrees
and so on.)The outlines of the scapula corresponding to the 0 and I
50-degree ab-duction positions are shown.
-
Acromion
30600
150 150..120.90
60.
0-Coracoid
x
up
FIG. 7
30#{176}to Max.Glenohumeral to
Scapulothoracic RatioInstantCenter
(nun)
Excursion of
Ball on Glenoid(in,i)
Clinical Findings
VARIOUS PARAMETERS AND CLINICAL DETAILS OF THE PATIENTS AND Two
NORMAL VOLUNTEERS (SUBJECTS K AND N)
MaximumSubject Arm Angle
Average of Normals
(Degrees)
Normal volunteersISO .25 0.25 6.0 1.85 1.09 0.475
K I 56 1.00 8.7 A* 1.2 Old GH dislocation (normal volunteer)
N 150 1.87 4.4 1.2 Normal volunteer
CL 112 1.00 7.1 4.OA Rotator-cuff tear
E 150 0.99 A 4.8 1.0 Shoulder pain; normal arthrogram
H 137 1.14 6.5 0.8 Rotator-cuff tear
J 147 1.36 6.6 1 .0 Painful shoulder; previous injury
M 155 1.15 10.7 A 2.OA Shoulder pain; normal arthrogram
0 156 1.38 1 1.2 A 1.45 Rotator-cuff tear
Q 137 0.99 A 4.2 0.8 Rotator-cuff tearR 152 2.24 A 8.2 1.1
Shoulder pain; normal arthrogram:
arthritis in cervical spine
T 128 0.68 A 4.0 0.6 Rotator-cuff tear
U 99 0.72 A 4.9 1.0 Shoulder pain; normal
arthrogram:degenerative arthritis GH joint
V 123 0.83 A 12.1 A 2.7 A GH dislocation
W 164 0.93 A 10.8 A 2.2 A Rotator-cuff tear
x 129 1.41 14.2 A 4.OA Rotator-cuff tearY 99 0.236 A 13.25 A 2.2
A GH dislocations
z_ 148 0.826 A 12.7 A 2.2 A Painful shoulder; previous
injury_______
* Designates a value outside of one standard deviation of the
normal.
NORMAL AND ABNORMAL MOTION OF THE SHOULDER 199
VOL. 58-A, NO. 2. MARCH 1976
Rotation or twisting of the scapula about the x-axis is shown by
theupward movement of the coracoid and little shift in the acromion
relativeto the face of the glenoid (left). If the scapula is viewed
in the lateralprojection (right), the coracoid would be seen to
move upward with theacromion remaining on the same horizontal plane
relative to the glenoid.
scapulothoracic angle. The mean amount of twisting at
maximum abduction was 40 degrees ( 9 degrees standard
deviation).
This twisting can be described as the superior angle of
the scapula moving away from the body wall and the in-
ferior angle moving into the body wall, that is, external
ro-
tation of the scapula. This is of significance when con-
sidered with the external rotation of the humerus which
often occurs after 90 degrees of abduction. It now is evi-
dent that the humerus and the scapula move synchronously
to some extent, so that the relative amount of rotation may
be small, depending on how much the humerus rotates.
instant centers of rotation and ball excursion: In all
of the normal subjects, although there was some variation,
the instant centers lay quite close to each other and to the
center of the hurneral ball. In contrast to this, many of
the
patients displayed centers of rotation which deviated con-
siderably from the center of the ball (Table I, Subjects K,
0, V, W, X, Y, and Z).
In order to assign a value which was descriptive of the
instant center patterns, the center of the humeral head was
located and the distance from it to each instant center was
measured. The distances were then averaged and scaled up
or down to correspond to an average humeral-head diame-
ter of forty-four millimeters. The average instant centervalue
for the normal subjects was 6.0 1 .8 millimeters.
An abnormal value for instant center was one that was lo-
cated ten millimeters or more from the center of the ball.
The ball excursions showed an interesting feature.
From 0 to 30 degrees, and often from 30 to 60 degrees, the
humeral ball moved upwards on the glenoid face by about
three millimeters. Thereafter it remained constant, moving
only one millimeter or at most two millimeters upward or
downward between each successive position. For the
normal individuals the average movement from position to
TABLE I
-
200 N. K. POPPEN AND P. S. WALKER
THE JOURNAL OF BONE AND JOINT SURGERY
position was only 1 .09 0.47 millimeters. It was ex-
pected that there would be a correlation between the in-
stant center and the ball excursion, and this was borne out
when the abnormal values were compared (Table I).
Only seven shoulders from our series of twenty-seven
subjects showed distinctly greater instant centers and ex-
cursions than the remainder. Analysis of the seven abnor-
mal and one borderline abnormal shoulder was revealing
(Table I). All had either a previous glenohumeral disloca-
tion (Subjects V and Y), a rotator-cuff tear (Subjects CL,
W, and X), or significant shoulder pain associated with a
previous history of injury (Subjects M and Z).
Three (Subjects H, Q, and T) of the seven patients
with rotator-cuff tears documented by arthrogram did not
have abnormal values for ball excursion and instant center,
and one of these (Subject Q) was also noted to have a sig-
nificant tear of the rotator cuff at the time of surgery.
All of the three patients with a previous glenohumeral
dislocation (Subjects K, V. and Y) had abnormal values
for the instant center and only one had a normal value for
ball excursion. This sixty-one-year-old patient had been
asymptomatic for thirty-six years following a glenohum-
eral dislocation.
In the analysis of the ratios of glenohumeral to
scapulothoracic angle in the ten individuals with abnormal
ratios, none were patients. Two had had previous
glenohumeral dislocations (Subjects V and Y), three had
rotator-cuff tears (Subjects Q, T, and W), and one had
roentgenographic changes compatible with degenerative
arthritis of the glenohumeral joint (Subject U), one had
cervical osteoarthritis (Subject R), and two had significant
shoulder pain associated with a history of injury to the
shoulderjoint (Subjects Z and E). One individual with an
abnormal value was an asymptomatic volunteer (Subject
N). All but one of these ten subjects had significant shoul-
der pain or neck and shoulder pain. The five subjects with
abnormal glenoh umeral-to- scapulothorac ic ratios , butnormal
values for instant center and ball excursion, in-
cluded one with degenerative osteoarthritis of the
glenohumeral joint (Subject U), two with rotator-cuff
tears, and one with no known shoulder symptoms (Subject
N).
A normal value for the glenohumeral-to-scapulo-
thoracic ratio was not significant because four subjects
with rotator-cuff tears (Subjects CL, 0, W, and X), one
subject with previous glenohumeral dislocation (Subject
K), and one with normal motion values and a painful
shoulder (Subject M) had normal glenohumeral-to-
scapulothoracic ratios.
It may be concluded that if a patient has an abnormal
instant center value (more than ten centimeters) and in ad-
dition an abnormal ball excursion (more than I .5 millime-
ters), a significant previous injury has occurred resulting
in
abnormal mechanics of the shoulder joint.
An abnormal glenohumeral-to-scapulothoracic ratio
was associated with significant disease, but a normal ratio
of this kind did not rule out significant disease of the
shoulder joint.
Discussion
The measurements which have been described de-
pended primarily on the selection of reference axes drawn
in the thorax, scapula, and humerus. With careful
roentgenographic and graphic techniques these axes could
be drawn accurately and reproducibly. The glenohumeral-
to-scapulothoracic ratio in abduction motion was found to
be 5:4 after 30 degrees of abduction was reached. It is
emphasized that for a given arc of motion, this means that
the humerus moves 5 degrees on the glenoid, while the
scapula moves 4 degrees on the thorax. In contrast, a study
of Figure 5 reveals that the absolute angles O; to
#{176}STare
in about a two-to-one ratio. The reason for this difference
is that from 0 to 30 degrees most of the movement is
glenohumeral, elevating that line, while there is lowering
of the scapulothoracic line for the motion from 30 degrees
upwards. This may explain the discrepancy mentioned at
the outset.
There is a surprising degree of conformity between
the humeral head and the glenoid in the frontal scapular
plane. Therefore, as long as there is a compressive force
acting, the glenohumeral articulation would be expected to
be stable, and the humeral head will rotate on a more or
less fixed center with little, if any, excursion. For the
nor-
mal shoulder this was found to be the case. The upward
excursion occurring in the early range of motion would
probably be due to an initial sag of the ball in the depen-
dent position. Excessive excursion. along varying centers
of rotation, would occur if the conformity of the joint were
lost or if the component of shear force acting upward or
downward were excessive. The latter situation could arise
due to an imbalance of forces caused by muscle tears or if
pain disturbed the muscle coordination.
The fact that these various parameters seem to be sen-
sitive indicators of motion means that they can be of diag-
nostic use. For instance, as an adjunct to arthrography, a
motion study may indicate whether or not there is a
rotator-cuff tear producing abnormality of motion.
NoTF: Wt. ire gratelul fir a grant mm Sir. and Mrs. Skcn C.
Clarke. Jr .. in support ofthus ork. and 0 Dr. Rohc L. Paucrson.
Jr. . for hi guidance. S5.. faflk Sir. Ray Scafea andDr. Bernard
Ghcfman for carrysng out the radiography . Mrs. Margaret Erkrnan
greatfy a%sisted% oh the Organl/att()n and analysis of the
materiaf
References
I . BASMAJIAN, J. V., and BAZANT, F. J.: Factors Preventing
Downward Dislocation ofthe ShoulderJoint. An Electromyographic and
Morphologi-cal Study. J. Bone and Joint Surg.. 41-A: I 82-I 86.
Oct. 1959.
2. CATHCART, C. W.: Movements of the Shoulder Girdle Involved in
Those of the Arm and Trunk. J. Anat. and Physiol.. 18: 21 1-218,
1884.3. CLELAND, JOHN: Shoulder-Girdle and Its Movements. Lancet,
I: 283-284, 1881.4. CODMAN, E. A.: The Shoulder. Boston, Thomas
Todd Co. . 1934.5. DEMPSTER, W. T.: Mechanisms of Shoulder
Movement. Arch. Phys. Med. and Rehab. , 46: 49-70, 1965.
-
NORMAL AND ABNORMAL MOTION OF THE SHOULDER 201
VOL. 58-A, NO. 2, MARCH 1976
6. DOODY, S. 0.; FREEDMAN, LEONARD; and WATERLAND, J. C.:
Shoulder Movements During Abduction in the Scapular Plane. Arch.
Phys. Med.and Rehab. , 51: 595-604, 1970.
7. FISK, G. H.: Some Observations of Motion at the Shoulder
Joint. Canadian Med. Assn. J. , 50: 213-216, 1944.8. FREEDMAN,
LEONARD, and MUNRO, R. R.: Abduction ofthe Arm in the Scapular
Plane: Scapular Glenohumeral Movements. J. Bone and Joint
Surg., 48-A: 1503-1510, Dec. 1966.9. GRAVES, W. W.: The Types of
Scapulae. A Comparative Study of Some Correlated Characteristics in
Human Scapulae. Am. J. Phys. An-
thropol., 4: 111-128, 1921.10. INMAN, V. T.; SAUNDERS, J. B.
DEC. M.; and ABBOTT, L. C.: Observations on the Function ofthe
ShoulderJoint. J. Bone and Joint Surg.. 26:
1-30, Jan. 1944.1 1 . JOHNSTON, T. B.: The Movements of the
Shoulder Joint. A Plea for the Use of the Plane of the Scapula as
the Plane of Reference for Move-
ments Occurring at the Humero-scapular Joint. British J. Surg. ,
25: 252-260, 1937.12. SAHA, A. K.: Mechanism of Shoulder Movements
and a Plea for the Recognition of Zero Position of Glenohumeral
Joint. Indian J. Surg. , 12:
153-165, 1950.13. SAHA, A. K.: Theory of the Shoulder Mechanism:
Descriptive and Applied. Springfield, Illinois, Charles C Thomas,
1961.
Electromyography before and after Surgery for Hip Deformity
in Children with Cerebral Palsy
A COMPARISON OF CLINICAL AND ELECTROMYOGRAPHIC FINDINGS
BY JACQUELIN PERRY, M.D.*, M. MARK HOFFER, M.D.*, DANIEL
ANTONELLI, M.5.*,
JOHN PLUT, M.D.*, GORDON LEWIS, M.D.*, AND RON GREENBERG,
R.P.T.*, DOWNEY, CALIFORNIA
ABSTRACT: Twenty-three ambulatory children with
spastic diplegic cerebral palsy were evaluated clinically
and by electromyography before and after hip-muscle
surgery. The stretch tests originally designed to distin-
guish specific muscle tightness and spasticity werefound to be
non-specific when tested by electromyo-graphy. Ambulatory
electromyograms using needle
electrodes and telemetry generally showed decreasedactivity in
the released muscles and, on occasion,
changes in activity in muscles not operated on. These
unanticipated changes after release may explain some
of the unpredictability of results of such procedures incerebral
palsy.
Currently children with cerebral palsy and a spastic
gait are evaluated by observation of their gait and by a
series of stretch tests 15,8 Unfortunately, surgical treat-
ment based on these criteria may produce unpredictable re-
sults. We hoped that electromyography during the stretch
tests and and during gait might clear up some of the confu-
sion and aid in planning operative procedures that would
give predictable results. Initial work in this area was done
by Sutherland and associates.
Methods and Clinical Material
From January 1971 to August 1974, twenty-three
ambulatory children (Cases 1 to 23) with spastic diplegic
cerebral palsy, five to eighteen years old, were evaluated
and treated for their crouched walking posture (walking
with flexed hips and knees and internally rotated thighs).
Their functional class of gait 6 and use of apparatus as
well
* The Professional Staff Association, Rancho Los Amigos
Hospital,
7413 Golondrinas Street, Downey, California 90242.
as the findings by clinical stretch tests, gait examination,
and gait films were recorded (Table I and Chart VI).
In each patient, electrodes of fifty-micrometer
nylon-shielded copper wire were inserted in the rectus
femoris, gluteus maximus, gluteus medius, lateral ham-
strings, medial hamstrings, gracilis, adductor longus, and
iliacus , assuming iliacus activity to be similar to that ofthe
psoas and hence representative of the activity of the
iliopsoas. Our testing system permitted only eight muscle
tests per run. We therefore selected the eight muscles that
we considered to be the most significant hip or knee mus-
des affecting gait. Prior to the selection, we tested four
children with cerebral palsy and found that the activity of
the tensor fasciae femoris roughly paralleled that of the
gluteus medius during gait and that of the hip flexors dur-
ing stretch tests. Furthermore, this preselection study
showed that the activity of the vastus muscles roughly
paralleled that of the rectus femoris during gait. Precise
definition of the contribution of these and other muscles
should, of course, await testing systems with twelve or
more testing channels.
The following stretch tests were carried out while re-
cordings were made: straight-leg-raising, hip flexion with
knees flexed, adductor stretch with hips and knees flexed,
Thomas test , external rotation of the extended hip, ex-ternal
rotation of the flexed hip, Phelps-Baker gracilis
test 18 (extension of the knee with the hip flexed in exten-
sion and abduction), and prone flexion of the knee with the
hip extended (prone rectus test of Duncan or Ely) . These
tests were carried out in a standardized fashion for both
the
clinical and the electromyographic evaluations. Each pa-
tient was first positioned in the testing posture and then
slow stretch was applied for four seconds as indicated by a