Embed Size (px)
Citation preview

Newborn Screening: Sickle Cell Disease
Peter Lane, MD
At the completion of this session, the participant will be able to:
Review the genetics, pathophysiology, and clinical manifestations of SCD
Understand the organization of and access to newborn screening follow-
up services
Understand the incidence, demographics and mortality of SCD in Georgia
Appreciate challenges of transition to adult care for individuals with SCD
Dr. Lane has no significant financial relationships to disclose. He will not be discussing products which he had a
role in developing. He will include a discussion of Hydroxyurea which is not yet FDA approved for use in
children. His presentation will include patient care recommendations.
This CME activity is supported by an educational grant from the GA Department of Public Health

Peter A Lane, MD
Professor of PediatricsEmory University School of Medicine
Director, Sickle Cell Disease Program
Children’s Healthcare of Atlanta
SICKLE CELL DISEASE IN GEORGIA
From Newborn Screening to Transition
Dr. Lane has no significant financial relationships to disclose. He
will not be discussing products which he had a role in
developing.
He will include a discussion of Hydroxyurea which is not yet FDA
approved for use in children. His presentation will include
patient care recommendations.
Disclosure Information
SICKLE CELL DISEASE (SCD) IN GEORGIAObjectives
• Review the genetics, pathophysiology, and clinical manifestations of SCD
• Understand the organization of and access to newborn screening follow-up services
• Understand the incidence, demographics and mortality of SCD in Georgia
• Appreciate challenges of transition to adult care for individuals with SCD
Aflac Cancer and Blood Disorders Center
SICKLE CELL DISEASE IN GEORGIA
• Brief Overview of SCD
Pathophysiology
Clinical manifestations
Genetics and inheritance
• GA Newborn Screening and Follow-up Program
• Results of SCD surveillance in Georgia
• SCD mortality in Georgia
• Transition to adult care
• Management Guidelines and Resources for Providers
Aflac Cancer and Blood Disorders Center
Aflac Cancer and Blood Disorders Center
Point mutation in β-globin: β6 (Glu Val)
Most common hemoglobin variant worldwide
Sickle cell trait (AS)
• 7-8% Africans Americans• Hispanic, Mediterranean, Middle East, Caribbean, India,
Central & South America
≥ 100,000 persons with SCD in US
Deoxy-Hb S polymerizes
• Damages RBC hemolysis• Vaso-occlusion and tissue injury
Sickle Hemoglobin (Hb S)
Aflac Cancer and Blood Disorders Center

SICKLE CELL DISEASE
Clinical Manifestations of Hemolysis
• Chronic anemia
• Jaundice
• Cholelithiasis
• Aplastic crisis
• Decreased energy / exercise intolerance
• Growth and pubertal delay
Aflac Cancer and Blood Disorders Center
Sickling and Vaso-occlusion
Hemolysis Vasoocclusion
SICKLE CELL DISEASE
Acute Events• Pain• Splenic sequestration• Infection• Acute chest syndrome• Stroke• Priapism
Chronic Organ Damage• Splenic dysfunction• Chronic pain • Lung disease• Neuro-cognitive • Pulm hypertension• Nephropathy
Treatment Complications• Medication toxicity • Iron overload• RBC alloimmunization• Other iatrogenic
Psychosocial Complications• Absence from school & work• ↓ Academic achievement • ↓ Readiness for transition • Stress, depression, ↓ self esteem
AAC
Complex Progressive Chronic
Vasculopathy
↓Quality of LifeMorbidityEarly DeathHigh Cost
Sickle Cell Anemia: Autosomal Recessive Inheritance
SICKLE CELL DISEASE
Vasoocclusion
++++
++ / ++++
-
+ / ++0
Genotype *
Hb SS
Hb SC
S β thalassemia
S β thalassemia
Approx % of
U.S. Patients
65
25
7
2 ++++
Hemolysis
++++
+
+
+++
*Each genotype characterized by largely
unpredictable and widely variable phenotype
SD, SO, SE, SLepore 1 Varies Varies
SICKLE CELL DISEASE
Family testing for Carriers *
Individuals at risk• Sickle cell trait (AS)
• Hemoglobin C trait (AC)
• β thalassemia
• Other hemoglobin variants
Laboratory testing • Hemoglobin electrophoresis, HPLC
• CBC / MCV
• Quantitation of A2 & F if MCV low or
low normal
*Provided by Sickle Cell Foundation of
Georgia at reduced or no cost Aflac Cancer and Blood Disorders Center
S
Sickledex(Hemoglobin
solubility
test)

NEWBORN SCREENING (NBS) FOR SCD IN GEORGIA
• 1980: Targeted screening of cord blood
• 1998: Universal screening of NBS dried blood spot specimens
• ~130,000 births per year
• ~130 infants with SCD born annually (SS, SC, Sβ+thal, Sβᴼthal, other SCD genotypes)
• SCD most prevalent disorder identified by NBS in GA (1:1,000)
Aflac Cancer and Blood Disorders Center
Genotype Approx %
of U.S.
Patients
Newborn
Screening
Results
Hb SS 65 FS
SC 25 FSC
S β+-
Thalassemia8 FSA or FS
S βo-
Thalassemia2 FS
Newborn Screening for SCD in GA
HPLC and isoelectric focusing
Aflac Cancer and Blood Disorders Center
Genotype % of
U.S.
Patien
ts
Newbo
rn
Screeni
ng
Results
SS 65 FS
SC 25 FSC
S β+-
Thalasse
mia
8FSA or
FS
S βo-
Newborn Screening for SCD in GA
HPLC and isoelectric focusing
Aflac Cancer and Blood Disorders Center
NEWBORN SCREENING (NBS) in GAHemoglobinopathy Follow-up Program
• Clinically significant disease (FS, FSC, FSA FC, FE)
NBS lab faxes results to NBS F/U coordinators (CHOA/GRU)
Confirmatory testing (Hgb electrophoresis/HPLC)
Parental education
Penicillin prophylaxis (SCD)
Referral for comprehensive specialty care
Complete follow-up activities within 2 months of age
• Heterozygous carriers (FAS, FAC, FAE, etc)
Results sent to Sickle Cell Foundation of Georgia
Family testing, education, and counseling
Aflac Cancer and Blood Disorders Center
Aflac Cancer and Blood Disorders Center | Emory University
Newborn Screening (NBS) in Georgia:~130 infants with SCD /yr
•
17
AugustaAugustaAugustaAugustaAugustaAugustaAugustaAugustaAugusta
MaconMaconMaconMaconMaconMaconMaconMaconMaconColumbusColumbusColumbusColumbusColumbusColumbusColumbusColumbusColumbus
SavannahSavannahSavannahSavannahSavannahSavannahSavannahSavannahSavannah
NBS lab faxes results to F/U Programs• CHOA for metro Atlanta (~85/yr)• GRU for non-metro Atlanta (~65/yr)
F/U Coordinators at CHOA and GRU• Contact PCP within 24-72 hr (~60%)• Contacts families directly (~40%)• Coordinates F/U activities with PCP• Confirmatory testing • Initiation of PCN prophylaxis• Referral to Comprehensive SCD
clinics• Referral for family testing• Documentation in SENDSS
Sickle Cell Disease ProgramChildren’s Healthcare of Atlanta
• Largest in US (1,800 active patients annually)
• Comprehensive clinics, ED and inpatient services
Egleston
Scottish Rite
Hughes Spalding
• Multidisciplinary SCD teams on all 3 campuses
Hematologists, nurse practitioners, nurses, social workers, psychologists, child life specialists, chaplains
• NBS Follow-up Program
Confirmatory testing in CHOA lab
Initial outpatient consultation
Subsequent coordination of care with PCPAflac Cancer and Blood Disorders Center

NEWBORN SCREENING FOR SCDScreening System Failures
• Blood transfusion prior to screening
• Extreme prematurity
• Sample never drawn or lost in transit to lab
• Inadequate sample
• Mislabeled specimen
• Laboratory or clinical error
• Inability to locate infant
• Inappropriate confirmatory testing or interpretation
• Parental denial
Aflac Cancer and Blood Disorders Center Aflac Cancer and Blood Disorders Center
NEONATAL SCREENING RESULTS
“No news is no news!”
Aflac Cancer and Blood Disorders Center Aflac Cancer and Blood Disorders Center | Emory University
Public Health Surveillance for SCD in Georgia
NIH/CDC RuSH Grant: (2010-2012)
• One of 7 states funded to conduct surveillance for SCD and thalassemia
CDC PHRESH Grant: (2012-2014)
• Only state (of 7) funded for continued SCD surveillance
Georgia CDC Transfusion Complications Grant: (2014-2019)
• Only state funded to characterize and reduce complications of blood transfusions in SCD & thalassemia
CDC Foundation Grant (2016)
• Extend SCD surveillance to include 2004-2014
Aflac Cancer and Blood Disorders Center | Emory University
Surveillance for SCD in Georgia 2004-2008
Results of CDC-funded RuSH Project
24
Surveillance for SCD in Georgia 2004-2008Cases by County and SCD Clinics
Comprehensive SCD centers (CHOA, Grady, GRU)Public Health Outreach sickle cell clinics
Number of residents with sickle cell disease* by county, 04-08
Dublin – Pediatric Athens – Pediatric Macon – AdultSavannah – Adult
Waycross – Pediatric and adultValdosta – Pediatric and adult Albany – Pediatric and adult
SCD residents per 100,000
*thalassemia excluded
SCD births 2004-2008
0
1 - 10
11 - 20
21 - 100
101 +

Hospital Encounters by Age for SCD*
* For individuals who had at least one ER or in-patient encounter in 2004-2008Aflac Cancer and Blood Disorders Center
Data from Georgia Registry and Surveillance for Hemoglobinopathies (RuSH)
Care Providers for SCD Patients in GA
Provider SpecialtyOutpatient
VisitsPercentage of
Visits
Internal Medicine 52,890 19%
Family Practice/General Practice 48,161 17%
Pediatrics 40,554 14%
Hematology 31,512 11%
Emergency Medicine 16,976 6%
Population: Medicaid all-cause outpatient visits 2004-2008 for confirmed and probable cases of SCD
Aflac Cancer and Blood Disorders CenterData from Georgia Registry and Surveillance for Hemoglobinopathies (RuSH)
Age at Date of Death in SCD
RuSH Dx Level Observations N Mean Median Mode
Confirmed 268 136 37.55 38 50
Probable 280 208 44.99 44 55
Total 548 344 42.05 41 50
Aflac Cancer and Blood Disorders CenterData from Georgia Registry and Surveillance for Hemoglobinopathies (RuSH)
SCD not listed on death certificate in 55% of cases!
SCD Mortality in GeorgiaCDC-RuSH Surveillance Project (7,299 patients)*
SCD not listed on death certificate in 55% of cases!
BARRIERS AND CHALLENGES TO TRANSITION TO ADULT CARE
• Parents enablement and fostering of dependency
• Pediatric providers enablement and fostering dependency
• Over dependence on pediatric providers
• Adolescents lack of SCD specific knowledge
• Neurocognitive and/or developmental delays
• Low self-esteem and self reliance
• Inadequate academic and vocational skills
• Lack of health insurance
• Lack of adult providers with interest and expertise in SCD
• Ineffective pediatric / adult provider communication
Aflac Cancer and Blood Disorders Center
Clinical Report on Health Care Transition AAP/AAFP/ACP 2011*
Targets all youth, beginning at age 12
Algorithmic structure with
• Branching for youth with special health care needs
• Application to primary and specialty practices
• Extends through transfer of care to adult medical home
* Pediatr 2011: 128; 182
DeBaun, Telfair: Transition and Sickle Cell Disease. Pediatr 2012: 130; 1
www. gottransition.org
Age 12 – Youth and family aware of transition policy
Age 14 – Health care transition planning initiated
Age 16 – Preparation of youth and parents for adult approach to care and discussion of preferences and timing for transfer to adult health care
Age 18 – Transition to adult approach to care
Age 18-22 – Transfer of care to adult medical home and specialists with transfer package
Aflac Cancer and Blood Disorders Center
NIH: Evidence-Based Management of
Sickle Cell Disease 2014
Objective:
• To expand the number of health
professionals able and willing to provide
care for persons with SCD
Target audience:
• PCPs, other health care professionals
Contents:
• Health Maintenance
• Management of Acute Complications
• Management of Chronic Complications
• Hydroxyurea Therapy
• Blood Transfusions
Yawn, et al, JAMA 2014: 321(10): 1033-1048
http://www.nhlbi.nih.gov/health-
pro/guidelines/sickle-cell-disease-guidelines
Aflac Cancer and Blood Disorders Center
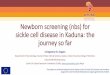
Red Blood Cells
HYDROXYUREA
Before Hydroxyurea On Hydroxyurea
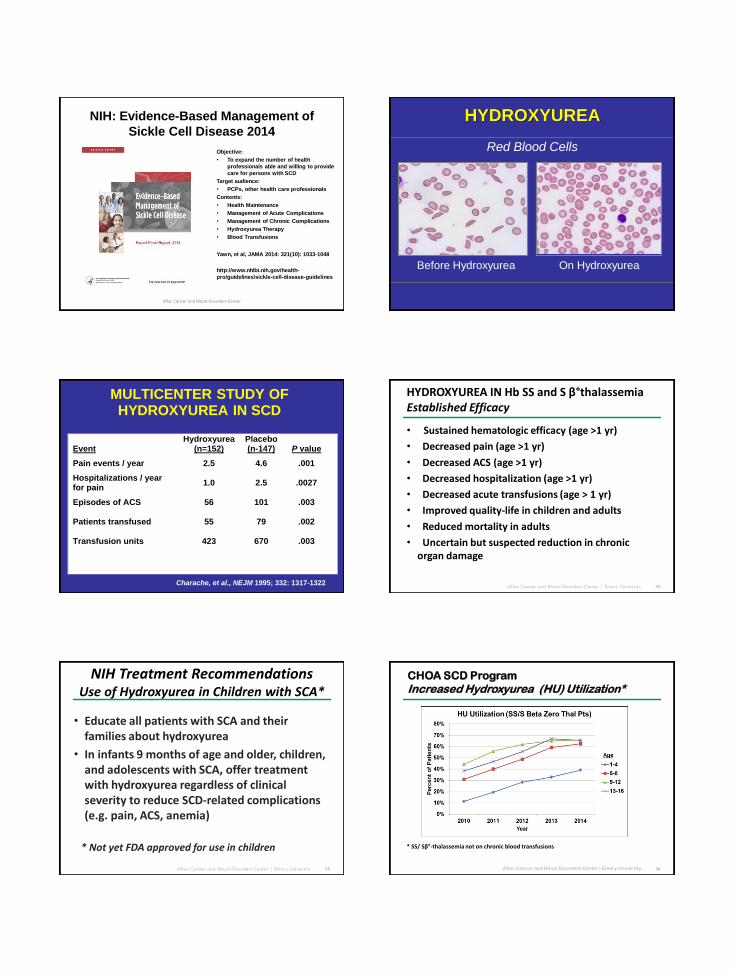
MULTICENTER STUDY OF HYDROXYUREA IN SCD
Charache, et al., NEJM 1995; 332: 1317-1322
Event Hydroxyurea
(n=152) Placebo (n-147) P value
Pain events / year 2.5 4.6 .001
Hospitalizations / year for pain
1.0 2.5 .0027
Episodes of ACS 56 101 .003
Patients transfused 55 79 .002
Transfusion units 423 670 .003
Aflac Cancer and Blood Disorders Center | Emory University
HYDROXYUREA IN Hb SS and S β°thalassemia Established Efficacy
• Sustained hematologic efficacy (age >1 yr)
• Decreased pain (age >1 yr)
• Decreased ACS (age >1 yr)
• Decreased hospitalization (age >1 yr)
• Decreased acute transfusions (age > 1 yr)
• Improved quality-life in children and adults
• Reduced mortality in adults
• Uncertain but suspected reduction in chronic organ damage
34
Aflac Cancer and Blood Disorders Center | Emory University
NIH Treatment Recommendations Use of Hydroxyurea in Children with SCA*
• Educate all patients with SCA and their families about hydroxyurea
• In infants 9 months of age and older, children, and adolescents with SCA, offer treatment with hydroxyurea regardless of clinical severity to reduce SCD-related complications (e.g. pain, ACS, anemia)
35
* Not yet FDA approved for use in children
Aflac Cancer and Blood Disorders Center | Emory University
CHOA SCD Program
Increased Hydroxyurea (HU) Utilization*
36
* SS/ Sβ°-thalassemia not on chronic blood transfusions

Reduced utilization 2 years after vs. 2 years before
initiation of HU
Pain Encounters 36%
Acute Chest Syndrome 43%
ED Visits 43%
Hospitalizations 47%
Inpatient Days 50%
Blood transfusions 57%
* Quarmyne, et al: Am J Hematol 2016
HU may be more effective when started in patients <10 years of age
Effectiveness of Hydroxyurea (HU)*Reduced Utilization after Initiation of HU
37
SICKLE CELL DISEASE IN GEORGIASummary
Major health issue in children and adults across GA
• Multiple SCD genotypes with variable manifestations and severity
• Complex progressive chronic vasculopathy
• Life-threatening acute and chronic complications
• Significant morbidity and early mortality
Newborn F/U programs housed at CHOA and GRU (Augusta University)
• Prompt confirmatory testing, family education, specialty care, ongoing
partnership between SCD clinic and PCP
Major challenges with transition to adult care
• Inadequate number of adult providers with expertise in SCD
• Marked increase in ED and inpatient utilization and mortality after age 18
NIH Evidence-based Management Recommendations, including use of HU
Aflac Cancer and Blood Disorders Center
SICKLE CELL DISEASE IN GEORGIAOther Resources for Providers
On-line:http://ghpc.gsu.edu/project/hemoglobin-disorders-data-coordinating-center/www.scifo.org
Phone Contacts:
Newborn Screening Follow-up Coordinators
• Greater Metro Atlanta 404 785-1087
• Outside Metro ATL 706 721-6251
Sickle Cell Foundation of Georgia 404 755-1461
Pediatric SCD Clinics
• CHOA at Hughes Spalding 404 785-7893
• CHOA at Egleston 404 785-1319
• CHOA at Scottish Rite 404 785-3519
• Augusta University 706 721-4929
Adult SCD Clinics
• Grady Hospital 404 616-5984
• Augusta University 706 721-2171Aflac Cancer and Blood Disorders Center