Embed Size (px)
Citation preview
Pregnancy & Newborn Screening Developments
Newborn Screening for Sickle Cell Disorders
What are the haemoglobinopathies?
• The Haemoglobinopathies are common inherited blood conditions, they mainly affect people who have originated from Africa, the Caribbean, the Middle East, Asia and the Mediterranean, but are also found in the northern European population
• The most commonly recognised are the sickle disorders and the thalassaemias
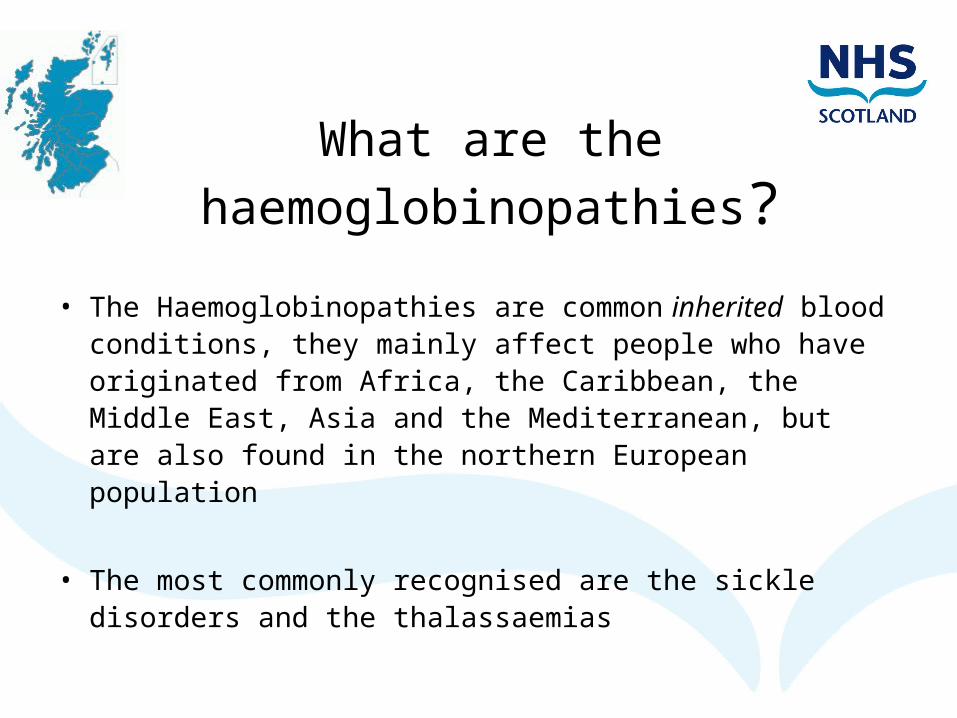
Sickle Cell Disorders
What are they?Blood disorders which affect the structure of haemoglobin
Normal blood cellImage reference: http://www.biocrossroads.com
Sickle blood cellImage reference: http://www.utdallas.edu/research/ibmst/focusgroups/
Sickle Cell Disorders
• Who do they affect?– Can affect anyone from any population– More common in people of African, Caribbean, Middle Eastern, and Asian
ancestry• How are individuals affected?
– Red blood cells "sickle" when they are short of oxygen, causing anaemia, risk of life-threatening infections, unpredictable attacks of severe pain (crises), morbidity, mortality
• How is the condition managed?– Information for family on risk factors – dehydration, heat, cold, infection,
stress– Prophylactic antibiotics from early age– Regular clinic attendance– Specialist clinical care– Rapid access to medical help in emergency
Conditions Screened for:
Antenatal (Carrier)• Hb-AS• Hb-AC• Hb-ADPunjab
• Hb-AE• Hb-AOArab
• Hb-A Lepore• thalassaemia trait • δ-thalassaemia trait• αo thalassaemia trait• HPFH
Newborn (Conditions)• HbSS • HbSC • HbSD• Hb-SDPunjab • HbS/ß thalassaemia• HbS OArab • HbS/HPFH• HbSE
How are Sickle Cell Disorders inherited
• Inherited by both parents passing on an altered gene• When a mother and a father both carry an altered gene for
sickle cell, every time they have a baby there is:
• 25% (one in four) chance that their baby will not be a carrier or have sickle cell disorder
• 50% (two in four) chance that their baby will be a carrier• 25% (one in four) chance that their baby will have a sickle cell disorder
Why screen for Sickle Cell Disorders
• Early detection in newborn babies and appropriate management improves quality of life
• Parents can be taught to avoid risk factors that trigger painful ‘crisis’ attacks in baby/child
• Babies should be commenced on penicillin and pneumococcal vaccine by 3 months of age
• Children with a sickle cell disorder are 600 times more likely to get a pneumococcal infection than other children
• It is strongly recommended that penicillin is given throughout childhood and carried on into adulthood
• Thalassaemia disorders not screened for at birth • Limited expression of ß-globin genes at birth• Limitations of the analytical procedures available
Linked Pregnancy & Newborn Programme
• Vital for Scottish Newborn Screening Laboratory to know parents carrier status – therefore must be recorded on bloodspot card
• Testing babies born to at-risk couples• Important to know parents’ carrier status when dealing with
newborn results• Important to remember that Beta Thalassaemia may not be
detected from newborn bloodspot
Transfused Babies
Babies who receive a blood transfusion prior to Sickle Cell screening will require a repeat test at 4 months post transfusion. This also includes intrauterine transfusions.
Therefore it is strongly recommended that a pre-transfusion blood spot specimen is obtained from all babies in SCBU or NNU for SCD screening.
Obtain one spot on admission to unit and mark as pre-transfusion. Then send to lab with the 5 day sample if baby receives a transfusion
Sickle Cell Carriers
• Babies who are sickle cell carrier will be detected through the screening programme (approx 170 cases per year)
• Carriers inherit one altered gene that makes sickle haemoglobin S and one gene that makes usual haemoglobin A – HbAS
• Carriers will never have a sickle cell disorder. They will always be a healthy carrier
• However parents need to know to:• Inform health care professionals before child undergoes surgery/anaesthetic
• Take extra care if their child might be in a situation involving a lack of oxygen i.e. high-altitude mountaineering
• It is important that parents tell their child about being a carrier so that if they want to plan a family of their own they can suggest a blood test for their partner. If their partner is also a carrier there is a chance that their baby could inherit a sickle cell disorder
• GP will be informed of babies who are carriers so they can offer referral to genetic counselling
Useful Links
• www.pnsd.scot.nhs.uk• Sickle Cell Disease – A parent’s guide
http://sct.screening.nhs.uk/cms.php?folder=2503• NHS Sickle cell & thalassaemia screening programme
http://sct.screening.nhs.uk/• Results of newborn blood spot screening leaflets:
http://newbornbloodspot.screening.nhs.uk/cms.php?folder=2545