Embed Size (px)
Citation preview
Newborn Sickle Cell Screening
Charles Kiyaga MSc, MPhil
National EID/NBS Coordinator
Central Public Health Laboratories
Ministry of Health – Uganda
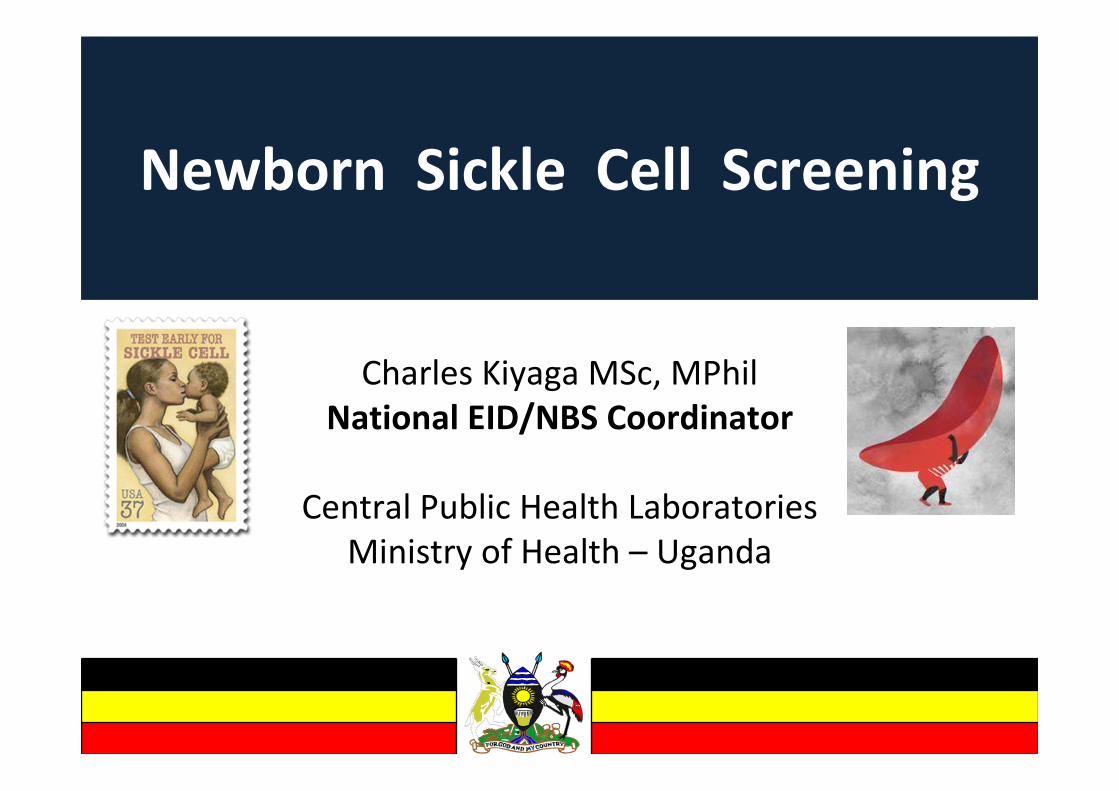
Early Infant HIV Diagnosis (EID) Program
served as a Precursor for Sickle Cell NBS
• The national EID program targeting HIV exposed infants started in 2006 working
with 8 partner run laboratories with molecular capacity.
• To make the program more efficient and cost effective, the Ministry of Health
decided to consolidate the labs into one managed under the public system in 2011.
• To make the centralized EID lab accessible a sample transport network was
formed.
• This improved efficiency and reduced TAT from 2 months to 2 weeks, reduced the
unit cost per test from $40 to $18, and improved MOH oversight and coordination
of the program
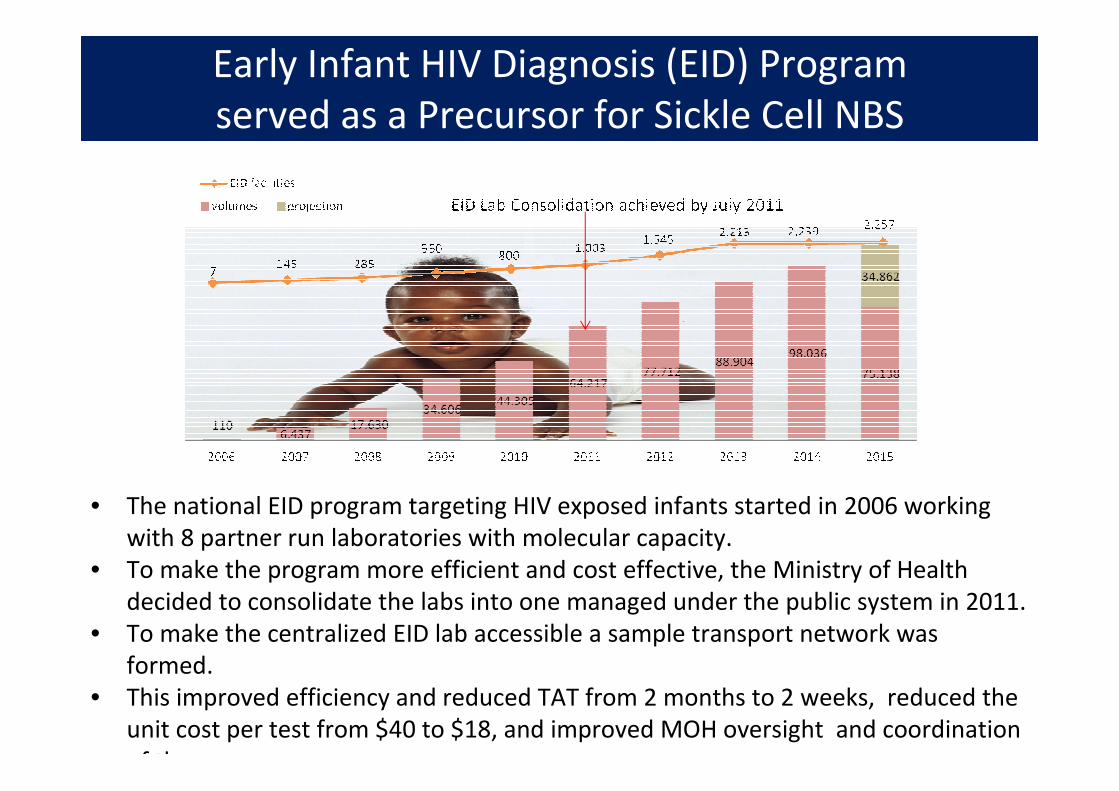
The National Sample Transport System
3
In order to increase access to the central EID laboratory, and quality lab services in general,
MoH decided to invest in a sample transport system. This system involves setting up local area
networks centered around major hospitals, and health centers which we called hubs.
xx
xx Monday
Route
x
x
x
x
xTuesday
Routex
DNA PCR
Laboratory
HUB
• Each hub operated with in 30 to 40km radius reaching 25 to 35 health facilities
• Each hub is given a motorbike and a rider who through scheduled routes visits 5 to 8 health
facilities a day picking sample and dropping results of the previous visit.
• The hub will run those tests they have capacity for, and refer highly specialized ones to CPHL
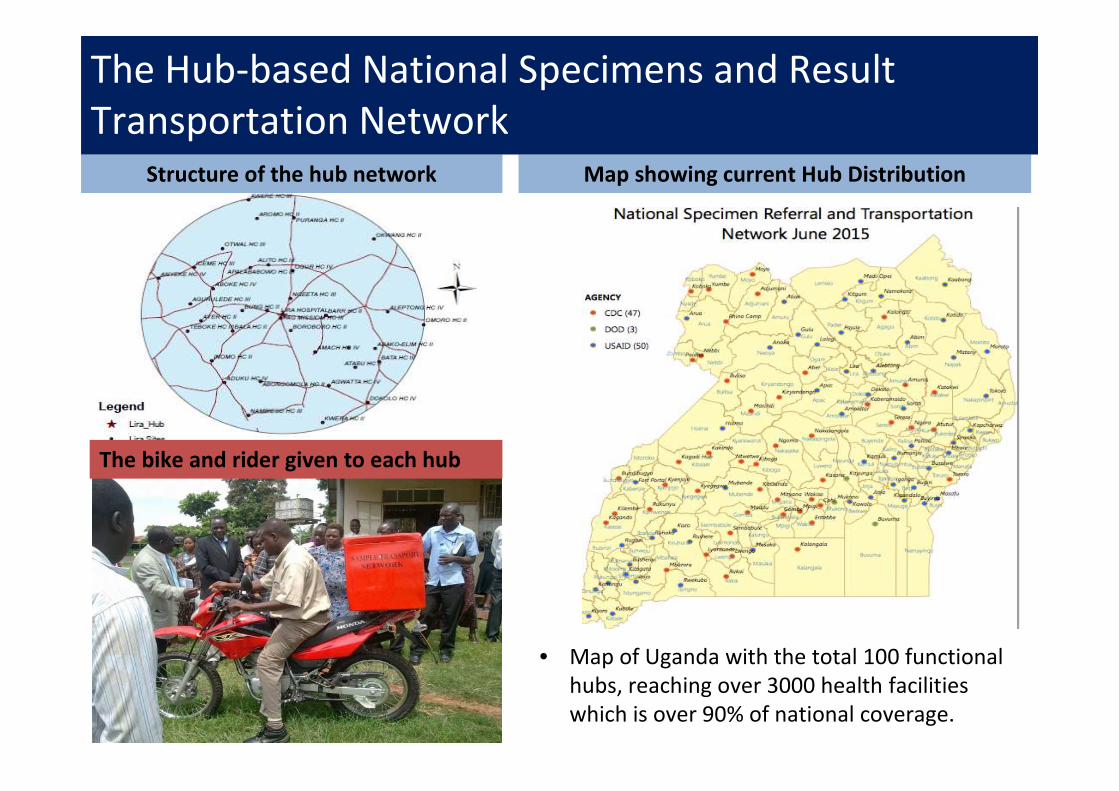
• Map of Uganda with the total 100 functional
hubs, reaching over 3000 health facilities
which is over 90% of national coverage.
Structure of the hub network Map showing current Hub Distribution
The bike and rider given to each hub
The Hub-based National Specimens and Result
Transportation Network
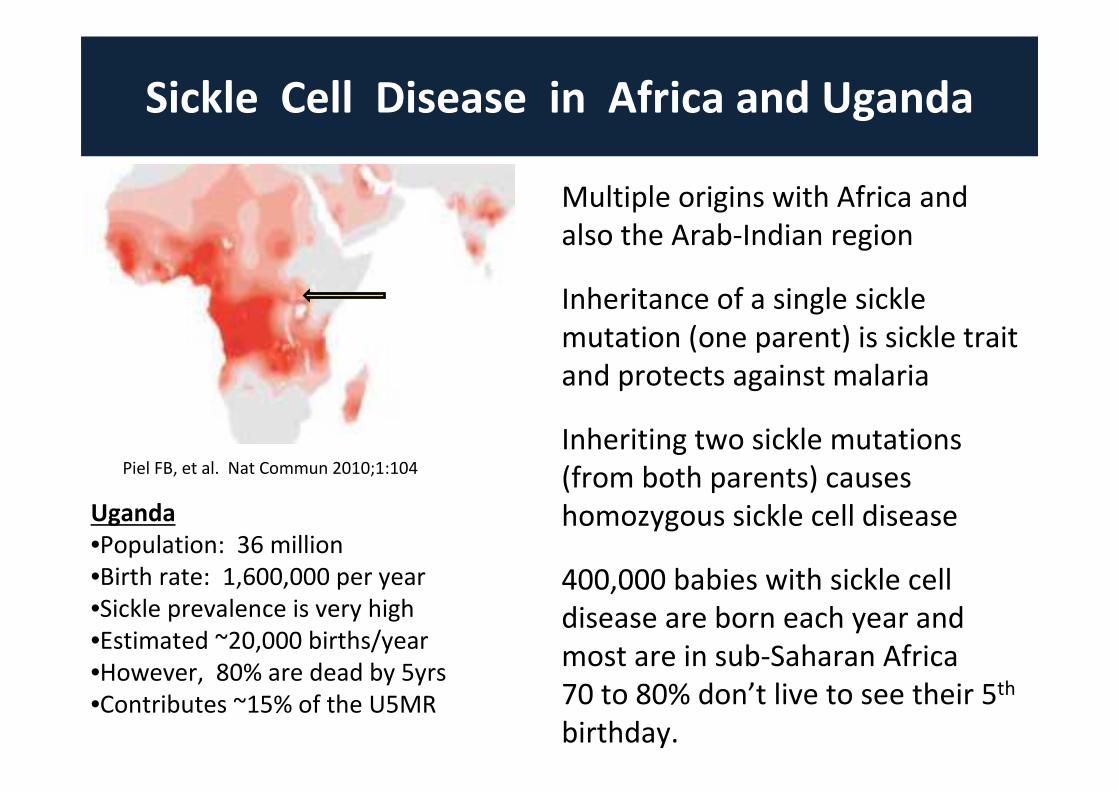
Sickle Cell Disease in Africa and Uganda
Uganda
•Population: 36 million
•Birth rate: 1,600,000 per year
•Sickle prevalence is very high
•Estimated ~20,000 births/year
•However, 80% are dead by 5yrs
•Contributes ~15% of the U5MR
Piel FB, et al. Nat Commun 2010;1:104
Multiple origins with Africa and
also the Arab-Indian region
Inheritance of a single sickle
mutation (one parent) is sickle trait
and protects against malaria
Inheriting two sickle mutations
(from both parents) causes
homozygous sickle cell disease
400,000 babies with sickle cell
disease are born each year and
most are in sub-Saharan Africa
70 to 80% don’t live to see their 5th
birthday.
Sickle Cell Challenges in Uganda
• Limited data regarding the sickle cell burden
• Lack of knowledge among healthcare workers and
public, not recognized or accurately diagnosed
• Not on non-communicable disease agenda
• No national policy and strategy
• No newborn screening, lack of access to care
Sickle Cell Survey Proposal
• Establish Partnerships
MOH/CPHL, Makerere University
Cincinnati Children’s Hospital
• Country-wide surveillance study
Map the burden of SCT and SCD
Build local capacity, raise awareness
Ride on the already existing EID infrastructure
• Surveillance Study � sickle cell newborn screening
Sickle Cell Laboratory
Space at the CPHL was renovated and fully equipped
Laboratory set-up and training of CPHL personnel by
Cincinnati team, plan for ongoing training and monitoring
Short-term goals to build local capacity and determine
feasibility for high-volume testing
In February 2014, the Sickle Cell Laboratory was opened
Uganda Sickle Surveillance Study
Primary objective was to describe the current prevalence
and distribution of SCD in Uganda
We hypothesized that there is a large sickle cell burden
across Uganda, but with substantial geographic variability
Design and Methods:
•One year cross-sectional study
•Use dried blood spots collected in EID program
•Perform hemoglobin electrophoresis using isoelectric
(IEF) technique on 75,000-100,000 samples
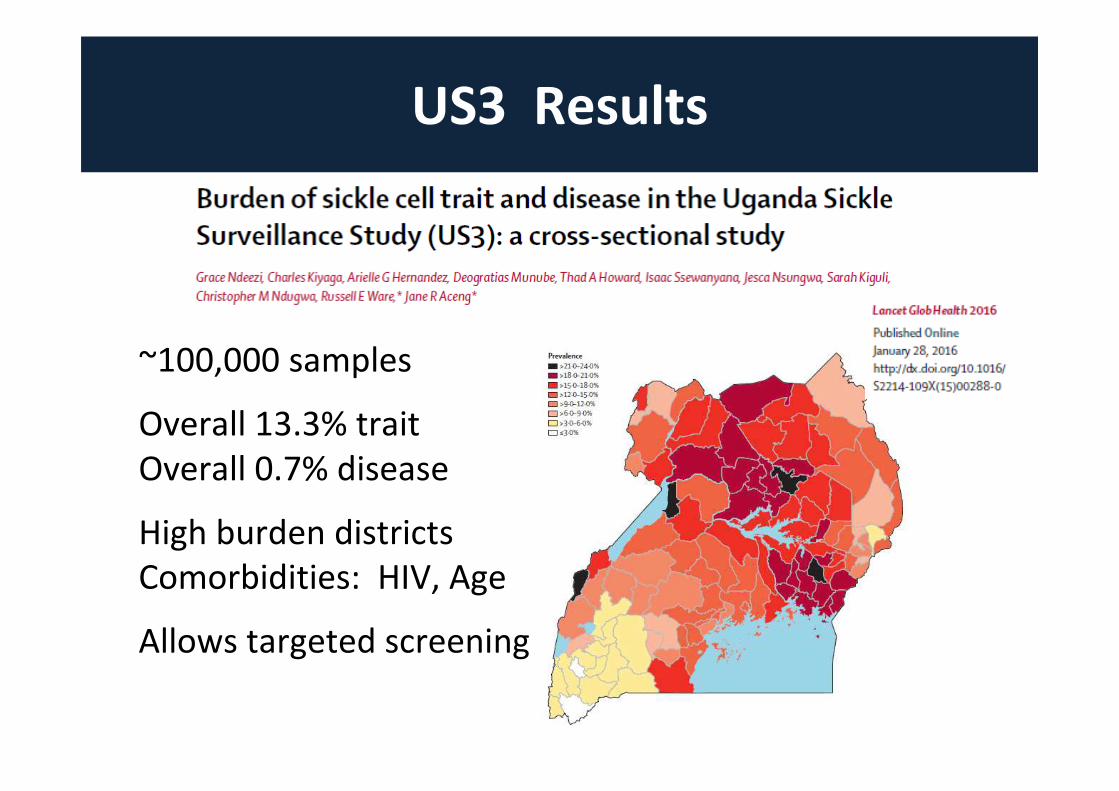
US3 Results
~100,000 samples
Overall 13.3% trait
Overall 0.7% disease
High burden districts
Comorbidities: HIV, Age
Allows targeted screening
Highest Prevalence Districts
• 49 of the 112 districts have sickle cell trait >15.0%
• 8 districts have sickle cell trait >20.0%
• 14 districts contain 47% of the sickle cell disease
• Screening should focus on highest burden regions
Sickle Cell Newborn Screening
Where to begin screening?
•12-14 highest burden districts
•Mid Northern and Central regions
•Maternity wards for in-hospital births
•Healthcare facilities, immunization clinics
Whom to screen?
•All newborns within the hub
•Include children under 2 years in
high burden districts
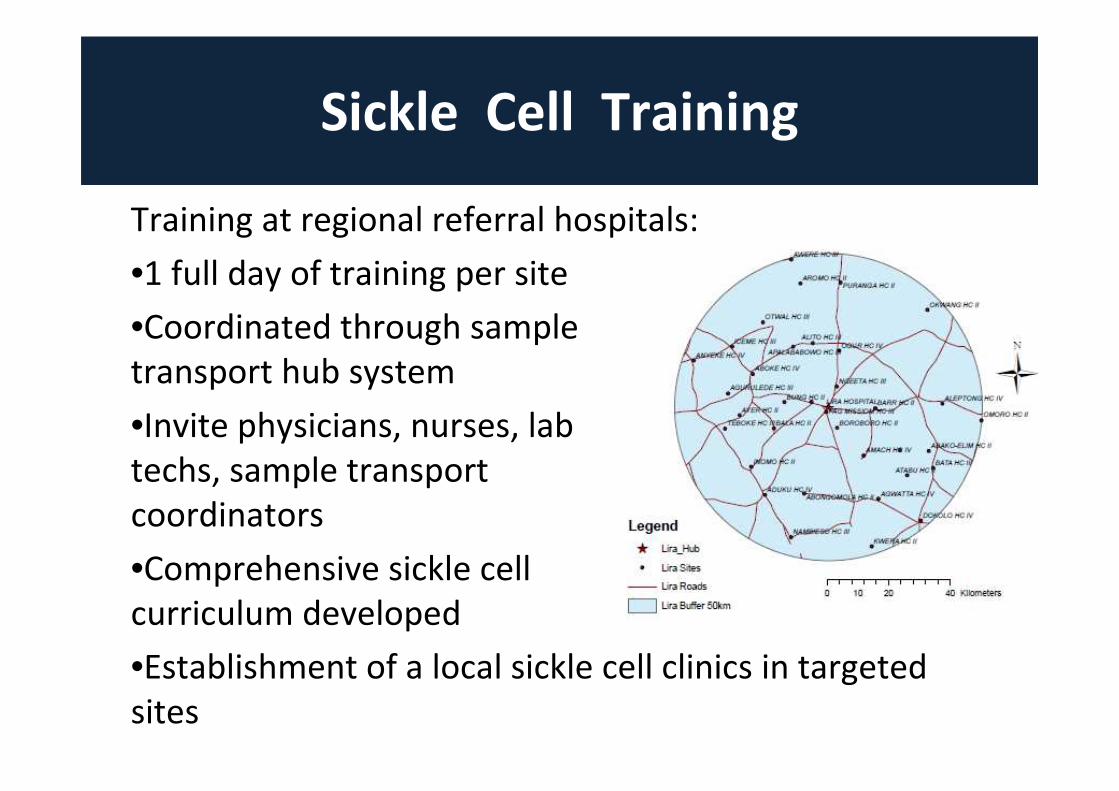
Sickle Cell Training
West Nile
SCT 13.8%Mid Northern
SCT 19.2%North East
SCT 15.8%
Training at regional referral hospitals:
•1 full day of training per site
•Coordinated through sample
transport hub system
•Invite physicians, nurses, lab
techs, sample transport
coordinators
•Comprehensive sickle cell
curriculum developed
•Establishment of a local sickle cell clinics in targeted
sites
Targeted Screening Results
West Nile
SCT 13.8%Mid Northern
SCT 19.2%North East
SCT 15.8%
• Since the completion of the US3 study, 12 hub sites have now received sickle cell training and have begun targeted sickle cell screening
• Over 35,000 samples have been collected on children <2 years of age, from high-burden districts using the EID sample transport system
• ~20% sickle cell trait is confirmed in the East Central and Mid Northern regions of Uganda, with >1% disease
• Co-morbidity with HIV is supported by our new data
• Site training and follow-up training occurs with support of PerkinElmer and Cincinnati Children’s Hospital
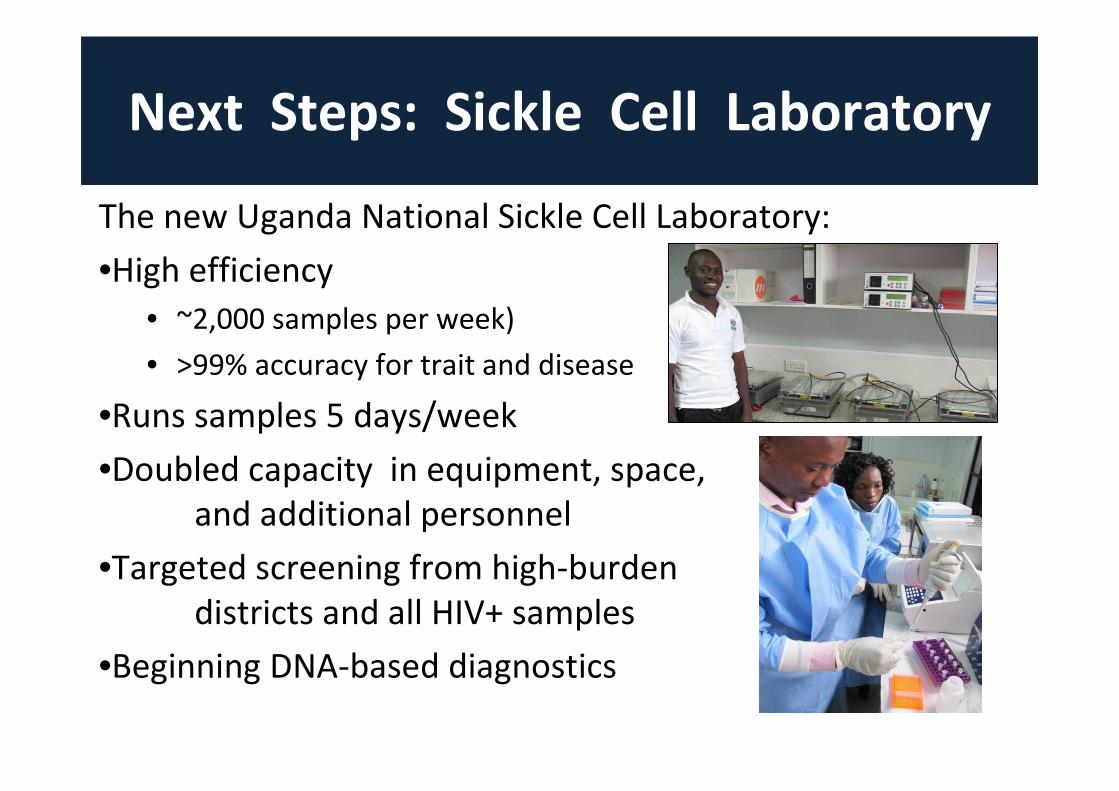
Next Steps: Sickle Cell Laboratory
The new Uganda National Sickle Cell Laboratory:
•High efficiency
• ~2,000 samples per week)
• >99% accuracy for trait and disease
•Runs samples 5 days/week
•Doubled capacity in equipment, space,
and additional personnel
•Targeted screening from high-burden
districts and all HIV+ samples
•Beginning DNA-based diagnostics
Long-Term Goals in Uganda
West Nile
SCT 13.8%Mid Northern
SCT 19.2%North East
SCT 15.8%
• Continue scaling up targeted screening in high-burden
districts
• Improve clinical care with district hospital clinics but
also incorporate sickle cell into primary health care
• Increase public awareness by media and ad campaigns
• Establish national guidelines and encourage MOH to
write formal national sickle cell strategy
• Universal sickle cell screening with appropriate
intervention, education, and treatment
• Use sickle cell screening as a precursor for other NBS
interventions
End
Acknowledgements
•Thanks to our collaborating partners Cincinnati
Children’s Hospital based in the US for the
technical and logistical support
•Thanks to Perkin Elmer for the logistical
support.
•To Makerere University for supporting the
study