Embed Size (px)
Citation preview

Adrian Hill
The Jenner Institute, Oxford University
New Vaccines for Global Health
Edward Jenner DM (Oxon)
1796: Jenner Invents Vaccination

• Same or related diseases in two species– e.g. tuberculosis, influenza
• Rapid efficacy testing in large animal species– allowing biomarker identification
• Large animals better predictors of immunogenicity • Common novel technology platforms• Similar cost constraints for low income markets
But until now largely independent development
Synergies in Human and Livestock Vaccine Development


Malaria Mortality and Morbidity
• Currently about 900,000 deaths each year from Plasmodium falciparum– Mostly in young children– Mostly in Africa
• About 250,000,000 clinical cases a year
• Malaria control now costing $2 billion annually– Tools such as spraying, drugs and impregnated bed nets
have a finite period of utility– Current economic cost of malaria to Africa : ~$12bn

A Complex Parasite Life-CycleMany Target Antigens

Transmission Blocking Vaccines Parasite Candidate Antigens
a: Expressed in host b: Expressed in vector
Pfs48/45Pfs230
Pfs25PfsHAP2Pfs48/45Pfs230

Transmission Blocking Vaccines Mosquito Vector Candidate Antigens
Alanyl Aminopeptidase N1: a mosquito midgut receptor
• mosquito midgut antigen
• transmission blocking activity against multiple parasite species
• most Anopheles vectors appear susceptible

Blood-Stage Malaria Vaccines

• Most natural immunity targets blood-stage
• Multiple target antigens are available
• A major target, PfEMP1, shows antigen variation
• Many show substantial polymorphism
Leading Blood-Stage Malaria Antigens

Phase Vaccine name Blood-stage Antigen(s)
Allele(s) Adjuvant Lead Author
Year GIA Efficacy Population
Ia AMA1-C1 AMA1 3D7 + FVO M ISA 720 Pierce 2010 Yes (up to 65%) Not assessed Australian adultsIa AMA1-C1 AMA1 3D7 + FVO Alhydrogel Malkin 2005 Yes (up to 54%) Not assessed US adultsIa AMA1-C1 AMA1 3D7 + FVO Alhydrogel + CpG7909 Ellis 2009 Yes (up to 97%) Not assessed US adultsIa AMA1-C1 AMA1 3D7 + FVO Alhydrogel + CpG7909 Mullen 2008 Y (up to 96%) Not assessed US adultsIa Pf(3D7)AMA1 AMA1 3D7 M ISA 720 Saul 2005 Not assessed Not assessed Australian adultsIa AMA1 FVO AMA1 FVO Alhydrogel/ M ISA720
/AS02Roestenberg 2008 Yes Not assessed Dutch adults
Ia FMP2.1 AMA1 3D7 AS02A Polhemus 2007 Yes (median up to 17%) Not assessed US adultsIa MSP1-C1 MSP1 3D7 + FVO Alhydrogel plus CpG7909 Ellis 2010 Y (up to 32%) Not assessed US adultsIa FMP1 MSP142 3D7/FVO Alhydrogel Malkin 2007 Y (< 20%) Not assessed US adultsIa FMP1 MSP142 3D7 AS02A Ockenhouse 2006 Y (<25%) Not assessed US adultsIa FMP1 MSP142 3D7 AS01B Start 2008Ia Combination B MSP1/MSP2/SERA 3D7 M ISA 720 Saul 1999 Not assessed Not assessed Australian adultsIa P30P2 MSP-119 MSP119 3D7 or FVO Alum Keitel 1999 Not assessed Not assessed US adultsIa MSP3-LSP MSP3 Conserved Alum/ M ISA 720 Audran 2005 Not assessed Not assessed Swiss adultsIa GMZ2 GLURP/MSP3 Conserved Alum Esen 2009 Not assessed Not assessed German adultsIa PfCP2.9 AMA1/MSP119 3D7 + FVO M ISA 720 Hu 2008 No Not assessed Chinese adultsIa PfCP2.9 AMA1/MSP119 3D7 + FVO M ISA 720 Malkin 2008 Yes (up to 13%) Not assessed Chinese adultsIa PfCA AMA1 3D7 AdHu5 NIAID Unpublished Not known Not assessed US adultsIb AMA1-C1 AMA1 3D7 + FVO Alhydrogel + CpG7909 Sagara 2009 FVO only (<10%
increase)Not assessed Malian adults
Ib AMA1-C1 AMA1 3D7 + FVO Alhydrogel Dicko 2008 Not assessed Not assessed Malian childrenIb AMA1-C1 AMA1 3D7 + FVO Alhydrogel Dicko 2007 No Not assessed Malian adultsIb FMP2.1 AMA1 3D7 AS02A Thera 2008 Yes (median < 40%) Not assessed Malian adultsIb FMP1 MSP142 3D7 AS02A Thera 2006 Not assessed Not assessed Malian adultsIb FMP1 MSP142 3D7 AS02A Stoute 2007 Not assessed Not assessed Kenyan adultsIb Combination B MSP1/MSP2/SERA 3D7 M ISA 720 Genton 2000 Not assessed Not assessed PNG adultsIb Combination B MSP1/MSP2/SERA 3D7 M ISA 720 Genton 2003 Not assessed None PNG childrenIb MSP3-LSP MSP3 Conserved Alum Lusingu 2009 Not assessed Not assessed Tanzanian childrenIb MSP3-LSP MSP3 Conserved Alum Sirima 2007 Not assessed Not assessed Burkina Faso
adultsIb MSP3-LSP MSP3 Conserved Alum Nebie 2009 Not assessed Not assessed Burkina Faso
adultsI/IIa FMP2.1 AMA1 3D7 AS02A vs AS01B Spring 2009 Yes (mean 3D7 up to
30%)Some US adults
I/IIa PEV3A AMA1 Conserved Virosome Thompson 2008 No Some UK adultsI/IIa NYVAC-Pf7 MSP1, AMA1, SERA 3D7 NYVAC Ockenhouse 1998 Not assessed Some US adultsIIa Combination B MSP1/MSP2/SERA 3D7 M ISA 720 Lawrence 2000 Not assessed None Australian adultsI/IIb SPf66 83, 55, 35 kDa
peptidesAlum Cochrane
Review1990-1998 Not assessed Some (South
America)South America, Africa, Asia
IIb AMA1-C1 AMA1 3D7 + FVO Alhydrogel Sagara 2009 Not assessed None Malian childrenIIb FMP1 MSP142 3D7 AS02 Ogutu 2009 Not assessed None Kenyan childrenIIb Combination B MSP1/MSP2/SERA 3D7 M ISA 720 Genton 2002 Not assessed Some PNG children
Blood-Stage Vaccine Trials

• Mosquito bites protect!– Irradiated parasites– >1000 bites required
• Effective in mice, fowl, monkeys, humans– Known since 1970s
• Irradiation can now be replaced– by genetic alteration of parasites
Pre-Erythrocytic Malaria VaccinesSporozoite and Liver-stages

SANARIAThe quest for a whole sporozoite vaccine

Difficulties for the Whole Irradiated Sporozoite Vaccine Approach
• Manufacturing– One batch per day
• Storage– Liquid nitrogen required
• Lack of efficacy– with 137,000 parasites x 6

Parasites
P
Cytoplasm
HLA = HumanLeucocyteAntigen
Receptor
Liver Cell Killer T Cell
Killer T-Cell Attack on an Infected Liver Cell
KILLING

The MeTRAP Vaccine InsertTargets the Liver-Stage of Plasmodium falciparum
ME: Multiple malaria Epitopes
TRAP: Thrombospondin-Related Adhesion Protein
TRAP strain is T9/96in this vaccine
A Polyepitope-Protein Vaccine Construct

Why Use Viral Vectors in Prime-Boost Regimes?
• Best means of safely inducing T cells in humans
• Only 5 vaccines have induced >1000 SFU/ml– in malaria (x 3), tuberculosis and influenza– all used viral vector boosting
• Adenovirus – MVA is the most potent approach– better than DNA – Adenovirus– better than Adenovirus - Heterologous Ad
Adenovirus Prime MVA Boost8 weeks

Viral Vector Vaccines to Maximise Cellular Immunogenicity
Adenovirus Prime MVA Boost
8 weeks
Malaria, HCV, HIV, influenza, TB...


Vectored Liver-Stage Vaccines for Malaria
• Efficacy correlated with CD8 T cell numbers in phase II trials– First example for any vaccine
• Excellent safety data for both adenovirus and MVA vectored vaccines
• Phase I trials of AdCh63-MVA completed successfully in Kenya and The Gambia
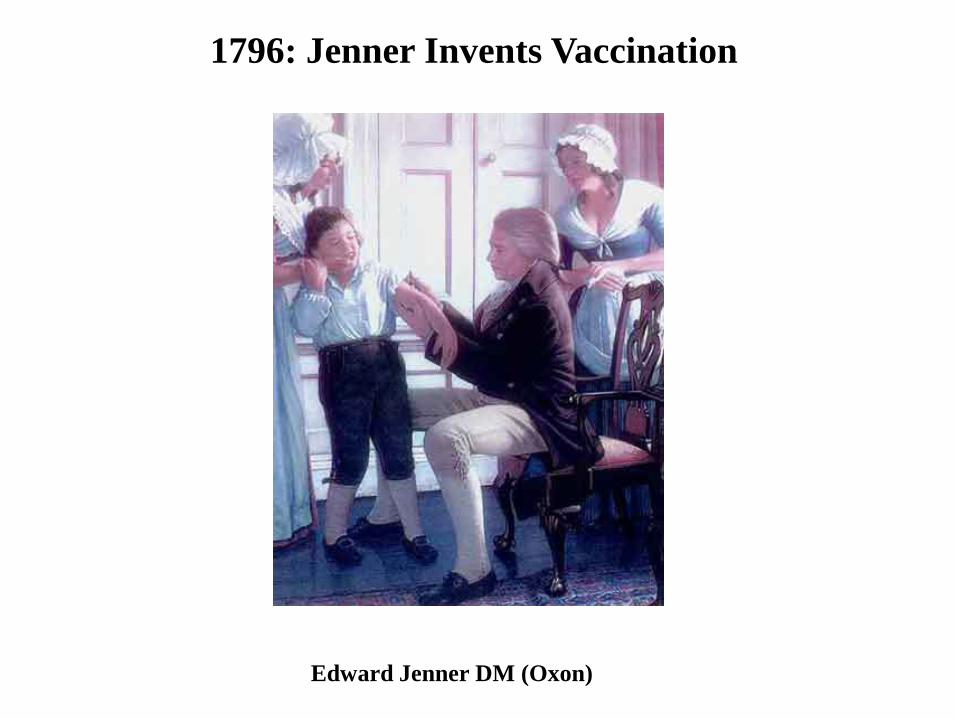
The RTS,S Malaria Vaccine Candidate

RT
RTS,S Sporozoite Challenge Typically Shows 60% Sterile or Partial Protection


A Sporozoite and Liver-Stage Vaccinea combination two-hit approach
RBC
schizonts Liver Stage:T Cells clear the
remaining liver cells
Sporozoite Stage: Antibodies clear most sporozoites

RTS,S + Vectored TRAPan infant immunisation regime
A Simple Regime for Deployment in Developing Countries through the Expanded Programme on Immunisation
0 1 2 3 4 5 6 7 8 9 months
R+A R+A R+M
R = RTS,S/AS01 A = AdCh63 MeTRAP M = MVA MeTRAP

Sukuta Vaccine ClinicThe Gambia

Conclusions
• Pre-erythrocytic malaria vaccines have shown most efficacy in humans clinical trials– Blood-stage vaccines have been more difficult– Sexual and mosquito stage vaccines just starting in the clinic
• Both RTS,S and vectored vaccines now show efficacy in most people on sporozoite challenge– Through antibodies and CD8 T cells, respectively
• RTS,S shows efficacy of ~40% in field trials– Now in a large phase III licensure trial– A combination approach with vectors + RTS,S would
probably show much higher efficacy

Jenner Institute Laboratories
OLD ROAD CAMPUS RESEARCH BUILDING

Centre for Clinical Vaccinology and Tropical Medicine
Churchill Hospital Facilities
Clinical Biomanufacturing Facility

Vaccine Trial Partners in Africa
• Wellcome-KEMRI, Kilifi, Kenya • University of Cape Town, South Africa• MRC Laboratories, The Gambia• University of Nairobi, Kenya• Université Cheikh Anta Diop, Senegal• CNRFP, Ouagadougou, Burkina Faso
Three Priorities for the Jenner Institute
• Global Health– vaccines that make a difference
• HIV, TB, malaria, dengue, pandemic influenza
• Translational Research– rapid early clinical testing
• 28 vaccines made for clinical trials
• One Health– vaccines for humans and other animals

Estimated tuberculosis incidence rates 2008

Epidemiology of TB in the21st Century
• 8.8 million new cases per annum• 1.7 million deaths per annum• Resistance
– MDR-TB– XDR-TB
• Overlap with HIV epidemic• Burden of latent infection

Global Plan to Stop TB: 2006 - 2015
• Targets (from Millenium Development Goals)– > 70% with infectious TB will be diagnosed– > 85% of those will be cured– By 2015, global prevalence of TB will be
reduced to 50% of 1990 levels– By 2050, global incidence will be
< 1/ million population
• How?– Use of current tools
• DOTS; DOTS-plus; DOTS expansion– New tools
• New drugs• New diagnostics• New vaccines
Total cost of plan: $56 billion – so a $31 billion funding gap

Bacille Calmette-Guerin
• Live attenuated Mycobacterium bovis
• First used in 1921 (orally)
• 2 big trials in 1950s:– UK (Copenhagen strain, highly effective)– US (Tice strain, no effect)

Efficacy of BCG
• Good– Disseminated TB and TB meningitis – Leprosy
• Bad– Lung disease – at any age – Boosting (Rodrigues et al, Lancet 2005)

New TB Vaccines in the ClinicVaccine Developer What Clinical
StageType
rBCG30 UCLA Recombinant BCG overexpressing Ag85B I - ended Mycobacterial
rBCGΔUreA::Hly VPM Recombinant BCG expressing Lysteriolysin
I Mycobacterial
M72 inAS01
GSKBio Subunit fusion protein of Rv1196 and Rv0125 in ASO1 adjuvant
I Protein inadjuvant
85B-ESAT6in IC31 (Hyb1)
SSI Subunit fusion protein of Ag85B and ESAT6 in IC31 adjuvant
I Protein inadjuvant
85B-TB10.4 in IC31 (HyVAC4)
SSI Subunit fusion protein of Ag85B and TB10.4 in IC31 adjuvant
I Protein inadjuvant
rAd35-Ag85A, 85B,TB10.4
Crucell Recombinant adenovirus35 expressing Ag 85A, 85B, 10.4
Ib Viral vector
MVA85A Oxford University / OETC
Recombinant vaccinia expressing Ag85A IIb Viral vector

MVA85A
• Expresses a major gene from Mycobacterium tuberculosis
• Made in Oxford in 1999– Replication-impaired
• First clinical trial in Oxford in 2002• Now 14 completed clinical trials
• In the UK, The Gambia, Senegal, South Africa• Remarkable CD4 T cell potency
• The most advanced new TB vaccine in clinical development
Helen McShane

Dunn’s: *, p < 0.05; **, p < 0.01
BCG / MVA85A:Enhanced Protection In The Lungs
of M. Bovis Infected Calves
Vordermeier et al. 2009

Summary of Clinical Trials with MVA85A since 2002

BCG – MVA85A induces High and Sustained Antigen 85A-Specific Immune Responses in UK
Vaccinees
0
500
1000
1500
2000
2500
3000
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Time (weeks)
SFC
/ 10
^6 P
BM
C BCG
MVA85A
BCG-MVA85A
McShane et al, Nature Medicine 2004
* p<0.05** p<0.01*
**
** *

MVA85A Induced Antigen Specific CD4+ T Cells Are Highly Polyfunctional
2+
1+
4+
3+
Number of functions:Pre-MVA85A Wk 1 Wk 2 Wk 8 Wk 24
Pre-MVA85A Wk 1 Wk 2 Wk 8 Wk 24
Beveridge N et al, EJI 2007

MVA85A Target Indications
• Booster vaccine administered in infancy (4-6 months)• Booster vaccine administered to HIV+ at diagnosis• Booster vaccine administered in adolescence
– i.e. 3 possible efficacy trials
• If effective, MVA85A would be indicated anywhere in the world where BCG is used
– But you need a high incidence area to test efficacy


Infant Phase IIb Efficacy Trial• Objectives:
– Safety– Immunogenicity– Efficacy (against disease & infection)– Immune correlates
• Design: – BCG vaccinated infants in Worcester, South Africa– Randomised at 18-22 weeks to receive either:
• MVA85A (1 x 108pfu)• placebo (Candin)
– Sample size = 2784 (1392/arm)• Cumulative TB incidence of 3%• 90% power to detect 60% improvement over BCG alone
Oxford + Emergent BioSolutions: Oxford Emergent Tuberculosis Consortium- with Wellcome Trust and Aeras Global TB Vaccine Foundation funding - collaboration with University of Cape Town

Phase IIb Efficacy Trial of MVA85A in HIV-Infected Adults
• Proof of concept study in HIV+ adults– protection against TB disease– protection against M. tb infection– safety & immunogenicity
• Two sites– South Africa: Cape Town with R Wilkinson– Senegal: Dakar with S Mboup
• Sponsored by Aeras Global TB Vaccine Foundation
• Funded by EDCTP, MRC and Aeras
• Due to start in May 2011

AE
C
C
C
B
BB
32 million people are living with HIV infection, mainly in Africa
Global Distribution of HIV Strains

Gag Pol Vif Env
mAb epitope PkMamu-A*01 epitope H-2Dd & Ld epitope
C C C CD D D DA A AB B B
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Humanized codons
AdCh63attenuated
adenoviruses
MVAattenuated poxvirus
Synthetic HIVCONSV Vaccine
Tom Hanke, Lucy Dorrell, Andrew McMichael

A New Cross-Strain Influenza Vaccine
• targets the internal antigens of flu• these are conserved between human and avian viruses• excellent phase I safety and immunogenicity

The Influenza A Virus Virion
Two surface glycoproteins
- haemagglutinin (HA)
- neuraminidase (NA)
Embedded M2 protein
The ribonucleoprotein complex
- nucleoprotein (NP)
- three polymerase proteins
- matrix (M1) protein .

FLU002- a Phase IIa Efficacy Trial
• Collaboration with Retroscreen Virology Ltd.
• Screen healthy volunteers for low anti-flu antibodies
• Challenge all intranasally 4 weeks after vaccination date, in a contained facility– Monitor viral shedding and symptoms for 10 days– All given oseltamivir prior to leaving containment
51

Enhancing the Immunogenicity and Efficacy of Vectored Vaccines
Grand Challenge 5: Solve how to design antigens for effective, protective immunity

The HydRIS SystemGlass stabilisation of vaccines on a membrane

Bioengineering Technologiesfor Vaccine Delivery
Stratum corneum (10-20µm)
Epidermis
Nerve
Sweat gland
Dermis
Hair follicle
Subcutaneous layer
Microneedle array

JENNER VACCINE
FOUNDATION
Funders
Key Contributors
• Helen McShane Tuberculosis• Sarah Gilbert Influenza• Simon Draper Malaria• Andrew McMichael HIV
Babatunde Imoukhuede, Souleyman Mboup, Greg Hussey, Kevin Marsh, Tumani Corrah





![Types of vaccines 1 - First generation vaccines are whole-organism vaccines - either live and weakened, or killed forms. [1] Live, attenuated vaccines,](https://img.pdfslide.us/doc/110x75/56649e155503460f94afff0b/types-of-vaccines-1-first-generation-vaccines-are-whole-organism-vaccines.jpg)