Embed Size (px)
Citation preview

NEW CLINICAL GUIDELINES TO OFF-LOAD & HELP HEAL DIABETIC FOOT ULCERS: ACTIONABLE EVIDENCE TO IMPROVE OUTCOMES
This educational event is supported by Derma Sciences Inc.
David G. Armstrong, DPM, MD, PhDProfessor of Surgery and DirectorSouthern Arizona Limb Salvage Alliance (SALSA)University of Arizona College of Medicine
Robert Snyder, DPM, MScProfessor and Director, Clinical ResearchBarry University School of Podiatric MedicinePast President, Association for the Advancement of Wound Care
Andrew J. Applewhite, MDMedical Director, Comprehensive Wound Center of Baylor University Medical Center

AGENDA
1. David Armstrong, DPM, MD, PhD
• Are DFUs worse and more costly than cancer?
• Stairway to amputation
2. Rob Snyder, DPM, MSc
• New consensus guidelines: DFU management through optimal off-loading
• Evidence-based off-loading selection
3. Andrew J. Applewhite, MD
• Off-loading in practice
• Practical Implementation in a clinic

NEW CLINICAL GUIDELINES TO OFF-LOAD & HELP HEAL DIABETIC FOOT ULCERS: ACTIONABLE EVIDENCE TO IMPROVE OUTCOMES
1. David Armstrong, DPM, MD, PhD• Are DFUs worse and more costly than
cancer?• Stairway to amputation

DIABETES, A GROWING THREAT
In 2011, 26 millionAmericans had diabetes (8.3% of the US population)1
15% of patients with diabetes are at risk of developing a foot ulcer (DFU)2
45% 5-year mortality rate post-LEA among diabetic patients4
85% of lower extremity amputations (LEAs) in diabetic patients are preceded by a foot ulcer3
1. Centers for Disease Control. http://www.cdc.gov/diabetes/pubs/pdf/ndfs_2011.pdf. 2. National Diabetes Data Group: Diabetes in America, Vol. 2. Bethesda, MD, National Institutes of Health 1995 (NIH publ. no. 95-1468) 3. Incidence of diabetic foot ulcer and lower extremity amputation among Medicare beneficiaries, 2006 to 2008, www.ahrq.gov. 4. Centers for Disease Control http://www.cdc.gov/diabetes/pubs/pdf/ndfs_2011.pdf.

8
18 18
45 47 4855
64
86
97
0
20
40
60
80
100
Percent
Armstrong DG, Wrobel J, Robbins JM. Are diabetes-related wounds and amputations worse than cancer? Int Wound J. 2007;4(4):286–7.
5-YEAR MORTALITY VS. CANCER

COST VS. CANCER

HEALTH CARE COSTS
• Nearly 80,000 LEAs are performed on diabetics each year1
• Two-year costs associated with initial hospitalization, rehospitalizations, post-acute care and prosthesis-related costs were $91,1062
• The projected lifetime health care cost for the patients who had undergone amputation $509,2752
1. Incidence of diabetic foot ulcer and lower extremity amputation among Medicare beneficiaries, 2006 to 2008, www.ahrq.gov. 2. MacKenzie EJ1, et al. Health-care costs associated with amputation or reconstruction of a limb-threatening injury. J Bone Joint Surg Am. 2007
Aug;89(8):1685-92.

STAIRWAY TO AMPUTATION
THREE QUESTIONS
1. What am I going to take off this wound that might help it heal?
2. What can I put on this wound that might help it heal faster, easier and better?
3. How can I prevent (severe) recurrence?

OFF-LOADING EVIDENCE-BASED SOLUTIONS
Sackett DL, Straus SE, Richardson WS, et al. Evidence-based medicine: how to practice and teach EBM. 2nd ed. Edinburgh: Churchill Livingstone, 2000.

NEW CLINICAL GUIDELINES TO OFF-LOAD & HELP HEAL DIABETIC FOOT ULCERS: ACTIONABLE EVIDENCE TO IMPROVE OUTCOMES
2. Rob Snyder, DPM, MSc• New consensus guidelines: DFU
management through optimal off-loading
• Evidence-based off-loading section
THE MANAGEMENT OF DIABETIC FOOT ULCERS THROUGH OPTIMAL OFF-LOADINGBuilding Consensus Guidelines and Practical Recommendations to Improve Outcomes
Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014
PANEL MEMBERS
Robert SnyderDPM, MScProfessor and Director of Clinical Research at Barry University SPM and President of the Association for the Advancement of Wound Care
Robert G. FrykbergDPM, MPHChief of the Podiatry section and Podiatric Residency Director at the Carl T. Hayden Veterans Affairs Medical Center in Phoenix, Arizona and Adjunct Professor, Midwestern University Program in Podiatric Medicine
Lee C. RogersDPMCo-director of the Amputation Prevention Center at Valley Presbyterian Hospital and the medical director of Paradigm Medical Management
Andrew J. ApplewhiteMDMedical Director at the Comprehensive Wound Center of Baylor University Medical Center
Gregory BohnMDDirector of the Trinity Center for Wound Care and Hyperbaric Medicine at Trinity Bettendorf and Moline Clinics at Trinity Regional Medical Center
Caroline FifeMDChief Medical Officer of "Intellicure," and Executive Director of the U.S. Wound Registry
Jeffrey JensenDPMDirector of research at the Barry University School of Podiatric Medicine and developer of the first commercially viable standardized Total Contact Casting kit
Desmond BellDPMCo-founder and Executive Director of the “Save A Leg, Save A Life” Foundation
James WilcoxRNDirector of Research & Quality for MedicalAffairs for Healogics, Inc.
Snyder RJ, et al. The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes. Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014

WHY DEVELOP A NEW CONSENSUS?
The group met to develop a comprehensive, evidence-based consensus on the optimal use of off-loading in DFU treatment because:
1DFUs are a major and costly complication that can:• Reduce quality of life (QOL)• Result in amputations and death
2There is a gap between evidence and practice with regards to the use of off-loading in the treatment of DFUs
Snyder RJ, et al. The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes. Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014

GOOD DFU MANAGEMENT
Begins with a comprehensive history and physical
Thorough wound assessment and treatment including:• Management of peripheral arterial disease (PAD)• Infection control and management• Debridement• Off-loading• Maintaining a moist wound environment
Timely wound healing is less likely without comprehensive management, including off-loading.
Snyder RJ, et al. The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes. Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014

WHY OFF-LOADING?
Off-loading reduces both pressure on the foot and
strain rate.
A diverse variety of off-loading devices and techniques exists, including:
• Removable or non-removable devices• Surgical techniques• Other assistive devices, which lets the
clinician employ off-loading based on the patient’s individual situation and needs
Snyder RJ, et al. The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes. Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014

METHOD
The panel performed a literature search of PubMed articles for evidence on off-loading.
Inclusion criteria were based upon the support of the consensus statement.
From approximately 90 selected studies, 64 studies were included in the evidence tables, along with 3 additional publications known by the authors but not found in the literature searches.
Snyder RJ, et al. The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes. Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014

METHOD
The panel used the GRADE1 approach to develop strength of recommendation: The recommendation
levels are:
✔✔✔✔
High:further research is very unlikely to change confidence in the estimate of the effect
Moderate: further research is likely to have an important impact on confidence and may change the estimate
Low: further research is very likely to have an important effect on the confidence in the estimate and is likely to change the estimate
Very Low: any estimate of the effect is very uncertain
Strong: patients should receive the
recommended action
Weak: clinicians should evaluate the recommendation within the
context of a particular patient’s situation
?
1. Atkins D, et al. Grading quality of evidence and strength of recommendations. BMJ. 2004 Jun 19;328(7454):1490.2. Snyder RJ, et al The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes.
Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014
GRADE = Grades of Recommendation, Assessment, Development, and Evaluation

ResultsEight evidence-based consensus guidelines and core recommendations resulted from the collaborative work of the panel.
Each statement references the level of the evidence and the strength of the recommendation - e.g., Moderate/Strong.
Snyder RJ, et al. The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes. Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014

CONSENSUS STATEMENTS

CONSENSUS STATEMENTS
1
The VIPs (vascular management, infection management and prevention, and pressure relief) are essential to DFU healing
2Adequate off-loading increases the likelihood of DFU healing
Grade Recommendation
✔✔✔✔
✔✔✔✔
Snyder RJ, et al. The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes. Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014

CONSENSUS STATEMENTS
3The panel endorses the Charcot foot in diabetes consensus report1
The Charcot Foot in Diabetes
ADA & APMA GuidelinesDiabetes Care, 2011
4Total contact casting (TCC) is the preferred method for off-loading diabetic plantar foot ulcers, as it has most consistently demonstrated the best healing outcomes and is a cost-effective treatment
Grade Recommendation
1. Rogers LC, Frykberg RG, Armstrong DG, et al. The Charcot foot in diabetes. J Am Podiatr Med Assoc. 2011;101(5):437–46. Review.2. Snyder RJ, et al The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes.
Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014
✔✔✔✔
✔✔✔✔

CONSENSUS STATEMENTS
5There currently exists a “gap” between the evidence supporting the efficacy of DFU off-loading and what is performed in clinical practice
6The likelihood of DFU healing is increased with off-loading adherence
Grade Recommendation
✔✔✔✔
✔✔✔✔
Snyder RJ, et al. The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes. Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014

CONSENSUS STATEMENTS
7Advanced therapeutics are unlikely to succeed in improving wound-healing outcomes unless effective off-loading is achieved
8
The panel supports the development of a per-visit off-loading quality measure to address the gap between evidence of off-loading and its current use in clinical practice
Grade Recommendation
✔✔✔✔
✔✔✔✔
Snyder RJ, et al. The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes. Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014

KEY OUTCOMES
• Likelihood of healing is increased with off-loading adherence
• The panel recommends TCC as the preferred method for effective pressure relief
• Evidence consistently shows that when off-loading is integrated into the patient encounter process and provided at each visit, the likelihood of DFU healing increases and the chance of complications decreases
Snyder RJ, et al. The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes. Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014

OFF-LOADING DEVICE AND EVIDENCE REVIEW

EVIDENCE FOR OFF-LOADING DEVICES AND TECHNIQUES
Removable Devices Evidence – Yes or No Level of Evidence
Walker cast (Stabil-D®) Yes46 Moderate
Shoe modification/custom-made temporary footwear Yes41,44,57 Moderate
Combinations of methods/techniques Yes19,31,32 Moderate
Fixed Ankle Walker (CAM/Bledsoe) Yes35,43 Low
Custom “CROW” (Charcot Restraint Orthotic Walker) Yes35 Low
DH Walker®, CAM boot shoe Yes20,35,43 Low
Air cast/pneumatic ankle/walking brace/splint Yes35,44,45 Low
Half Wedge shoe/Integrated Prosthetic and Orthotic System Yes19,35 Low
Diabetic shoe Yes45 Low
Felt and foam Yes35,44 Low
Custom Ankle Orthotic No -
Custom Hinged Device No -
Removable Cast Walker (tall/short) No -
Heel relief shoe No -
Surgical shoe No -
Snyder RJ, et al. The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes. Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014
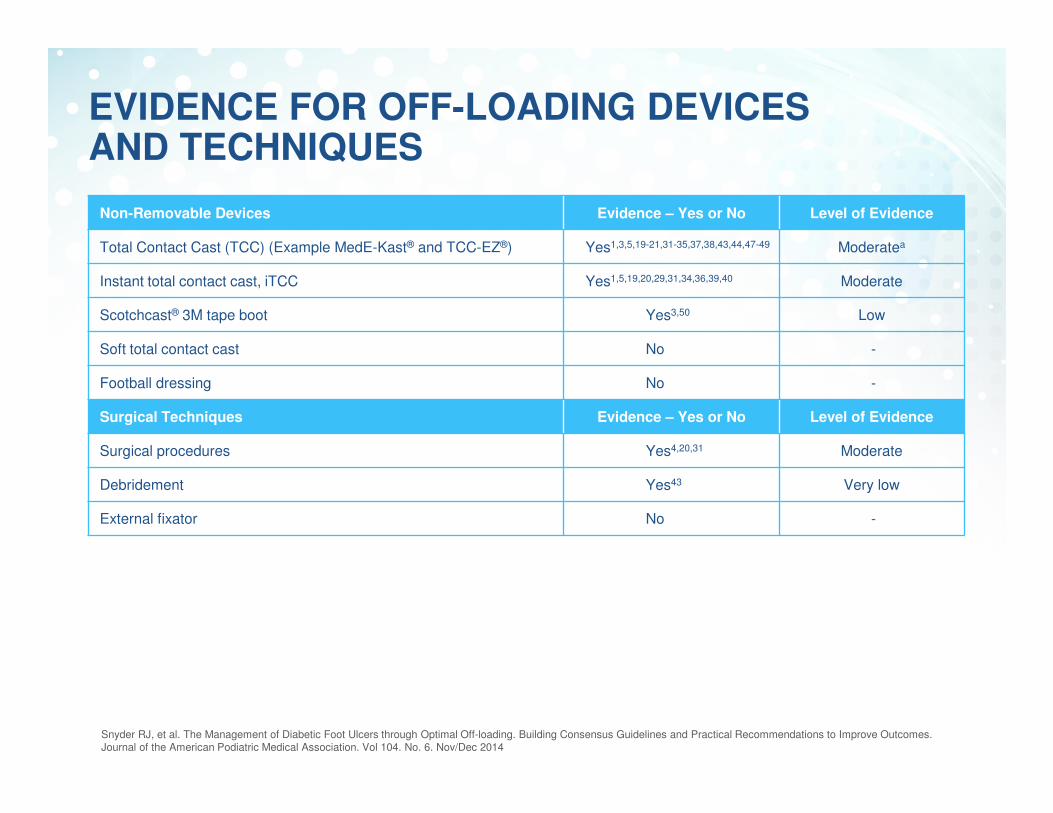
EVIDENCE FOR OFF-LOADING DEVICES AND TECHNIQUES
Non-Removable Devices Evidence – Yes or No Level of Evidence
Total Contact Cast (TCC) (Example MedE-Kast® and TCC-EZ®) Yes1,3,5,19-21,31-35,37,38,43,44,47-49 Moderatea
Instant total contact cast, iTCC Yes1,5,19,20,29,31,34,36,39,40 Moderate
Scotchcast® 3M tape boot Yes3,50 Low
Soft total contact cast No -
Football dressing No -
Surgical Techniques Evidence – Yes or No Level of Evidence
Surgical procedures Yes4,20,31 Moderate
Debridement Yes43 Very low
External fixator No -
Snyder RJ, et al. The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes. Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014

EXAMPLES OF REMOVABLE OFF-LOADING DEVICES
CAM Walker
CROW walker
DH WalkerAir Cast Pneumatic walker
Half Wedge shoe
Snyder RJ, et al. The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes. Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014
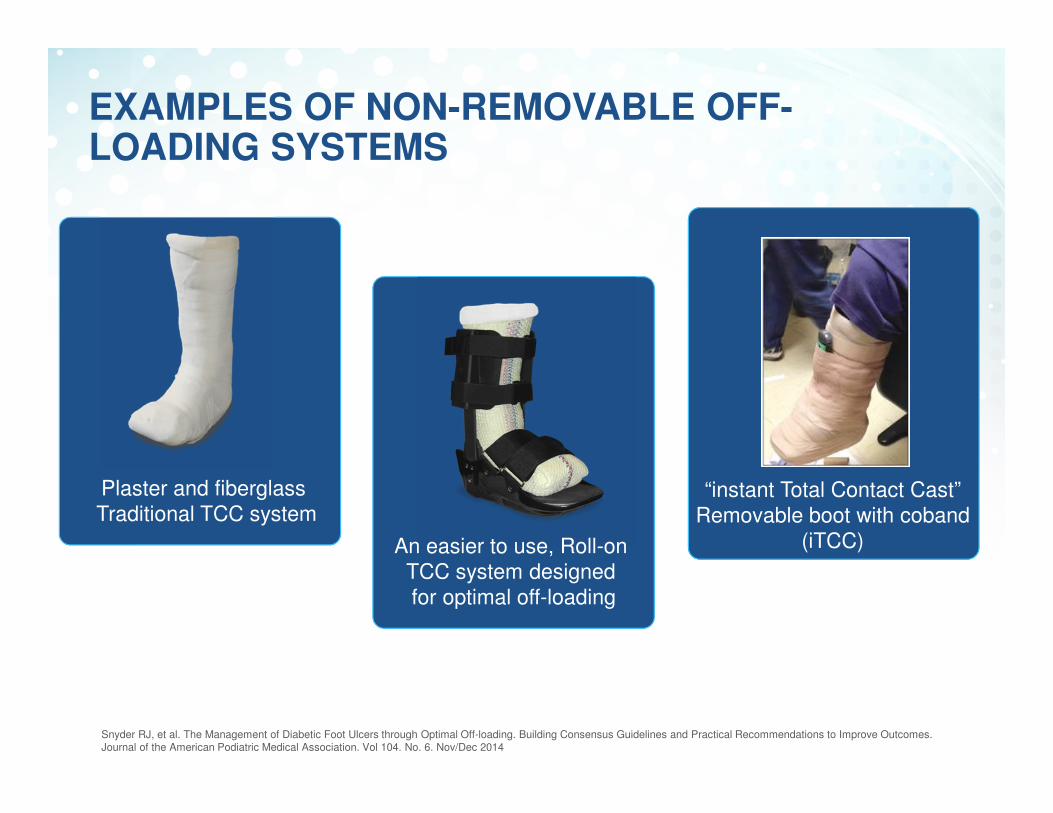
EXAMPLES OF NON-REMOVABLE OFF-LOADING SYSTEMS
An easier to use, Roll-on TCC system designed for optimal off-loading
“instant Total Contact Cast”Removable boot with coband
(iTCC)
Plaster and fiberglass Traditional TCC system
Snyder RJ, et al. The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes. Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014

Heel relief shoe
EXAMPLES OF REMOVABLE OFF-LOADING DEVICES – WITH NO EVIDENCE
Surgical / Post-op shoe
Snyder RJ, et al. The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes. Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014
Custom ankle orthotic

OFF-LOADING DEVICES AND TECHNIQUES WITH NO EVIDENCE
Other Assisted Devices Evidence – Yes or No Level of Evidence
Crutches No -
Canes No -
Walkers No -
Rolling walkers No -
Bed rest No -
Crutches WheelchairSnyder RJ, et al. The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes. Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014
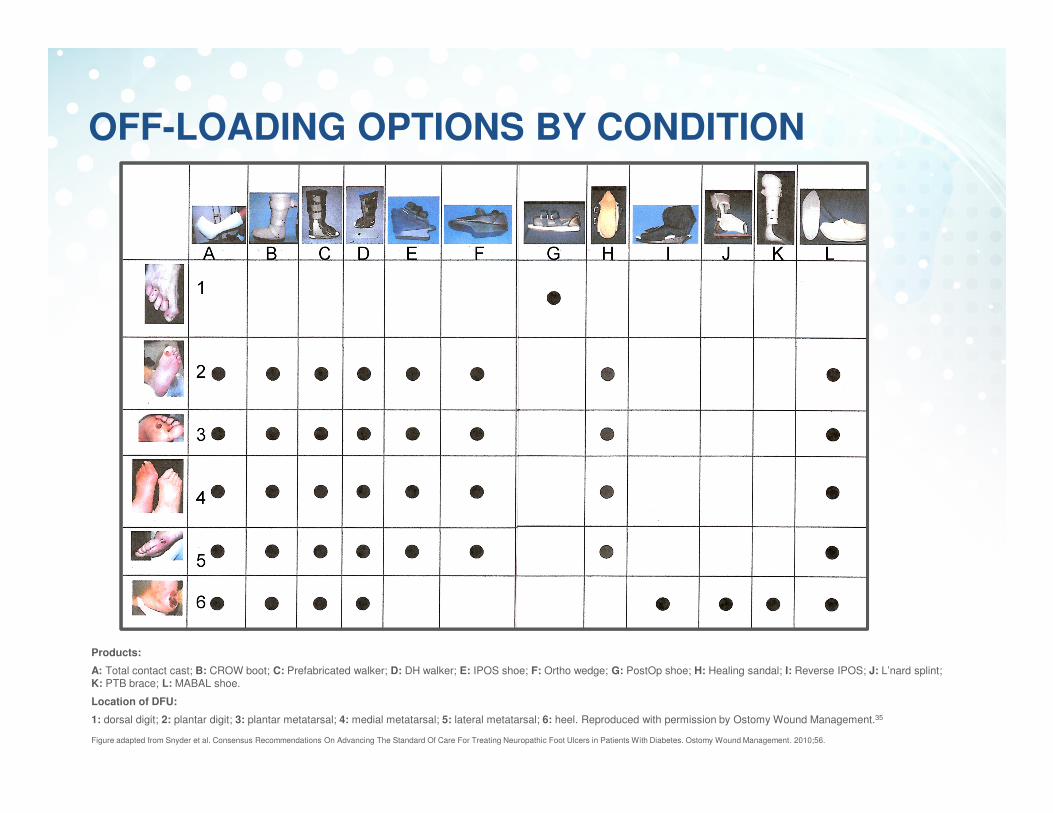
OFF-LOADING OPTIONS BY CONDITION
Products:
A: Total contact cast; B: CROW boot; C: Prefabricated walker; D: DH walker; E: IPOS shoe; F: Ortho wedge; G: PostOp shoe; H: Healing sandal; I: Reverse IPOS; J: L’nard splint; K: PTB brace; L: MABAL shoe.
Location of DFU:
1: dorsal digit; 2: plantar digit; 3: plantar metatarsal; 4: medial metatarsal; 5: lateral metatarsal; 6: heel. Reproduced with permission by Ostomy Wound Management.35
Figure adapted from Snyder et al. Consensus Recommendations On Advancing The Standard Of Care For Treating Neuropathic Foot Ulcers in Patients With Diabetes. Ostomy Wound Management. 2010;56.

OFF-LOADING OPTIONS BY AMOUNT OF EVIDENCE
Products:
A: Total contact cast; B: CROW boot; C: Prefabricated walker; D: DH walker; E: IPOS shoe; F: Ortho wedge; G: PostOp shoe; H: Healing sandal; I: Reverse IPOS; J: L’nard splint; K: PTB brace; L: MABAL shoe.
A. B. C. D. E. F. L.G. H. I. J. K.
Snyder RJ, et al. The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes. Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014

RECENT RCTs, META-ANALYSIS AND RECOMMENDATIONS REGARDING TOTAL CONTACT CASTING

PROVEN CLINICAL EFFICACY FOR TCC –COCHRANE SYSTEMATIC REVIEW 2013
Lewis J, et al. Pressure-relieving interventions for treating diabetic foot ulcers. Cochrane Database Syst Rev. 2013;1:CD002302
In 5/7 studies, non-removable casts were associated with a statistically significant increase in healed ulcers compared with removable devices
7 studies (366 participants) comparing non-removable casts with removable pressure-relieving devices

ADDITIONAL CLINICAL EFFICACY FOR TCC
Primary endpoint*: Patients achieving wound closure with full epithelialization (N=73)
• 90% of patients with TCC• 50% of patients with a healing sandal• 40% of patients with a shear-reducing
walking boot
Secondary endpoint*: Average time to healing
5.4 weeks for patients with TCC 8.9 weeks for patients with a healing sandal6.7 weeks for patients in a walking boot
%
Patient satisfaction was equal across devices.
Lavery AL, et al. Randomised clinical trial to compare total contact casts, healing sandals and a shear-reducing removable boot to heal diabetic foot ulcers. Int Wound J 2014.
Lavery AL, et al. Randomised clinical trial to compare total contact casts, healing sandals and a shear-reducing removable boot to heal diabetic foot ulcers. International Wound Journal 2014
N=73*‘Per-protocol analysis’ = only subjects who completed the study were included in the analysis.
TCC has a healing rate of about
90% within 6–8 weeks*
PROVEN CLINICAL EFFICACY FOR TCC –7 RCTs (N=371)
*ReferencesArmstrong DG, et al. Off-loading the diabetic foot wound. Diabetes Care 24:1019-1022, 2001.Mueller NJ, et al. Effect of Achilles tendon lengthening on neuropathic plantar ulcers. Journal of Bone and Joint Surgery 85-A:8; 1436-1445, 2003. Katz IA, et al. A randomized trial of two irremovable off-loading devices in the management of plantar neuropathic diabetic foot ulcers. Diabetes Care 28:555-559, 2005. Piaggesi A, et al. An off-the-shelf instant contact casting device for the management of diabetic foot ulcers. Diabetes Care 30:586-590, 2007. Mueller NJ, et al. Total contact casting in treatment of diabetic plantar ulcers; Controlled clinical trial. Diabetes Care 12:384-388, 1989. Armstrong DG, et al. Evaluation of removable and irremovable cast walkers in the healing of diabetic foot wounds. Diabetes Care 28:551-554, 2005. Lavery AL, et al. Randomised clinical trial to compare total contact casts, healing sandals and a shear-reducing removable boot to heal diabetic foot ulcers. Int Wound J 2014.
%

CAROLINE E. FIFE ET AL. DIABETIC FOOT ULCER OFF-LOADING: THE GAP BETWEEN EVIDENCE AND PRACTICEData from the US Wound Registry 2007 - 2013
C. E. Fife, MD, et al, Diabetic foot ulcer off-loading: The Gap Between Evidence and Practice: Data from the U.S. Wound Registry. Advances in Skin and Wound Care, 27(7) p. 310-316, 2014

USWR DFU “OFF-LOADING IN PRACTICE” PROJECT
Off-loading devices (2.2%)
(N = 4896)
TCC (16%)(N = 781)
Postoperative shoes (36.8%)
(N = 1803)
Others (47.2%)(N = 2312)
Roll on cast -TCC-EZ® (36%)
Traditional casting (64%)
C. E. Fife, MD, et al, Diabetic foot ulcer off-loading: The Gap Between Evidence and Practice: Data from the U.S. Wound Registry. Advances in Skin and Wound Care, 27(7) p. 310-316, 2014

USWR DFU ‘OFF-LOADING IN PRACTICE’ PROJECT
Patient outcomes
* Data was not stratified
0
1
2
3
4
5
6
TCC Non-TCC
DF
U p
ati
en
ts w
ho
ne
ed
ed
am
pu
tati
on
s (
%)
Amputations
0
0.5
1
1.5
2
2.5
3
TCC Non-TCC
Infe
cti
on
s (
pe
r ye
ar)
Infections (per year)
P = 0.001* P = 0.0000000021 *
C. E. Fife, MD, et al, Diabetic foot ulcer off-loading: The Gap Between Evidence and Practice: Data from the U.S. Wound Registry. Advances in Skin and Wound Care, 27(7) p. 310-316, 2014
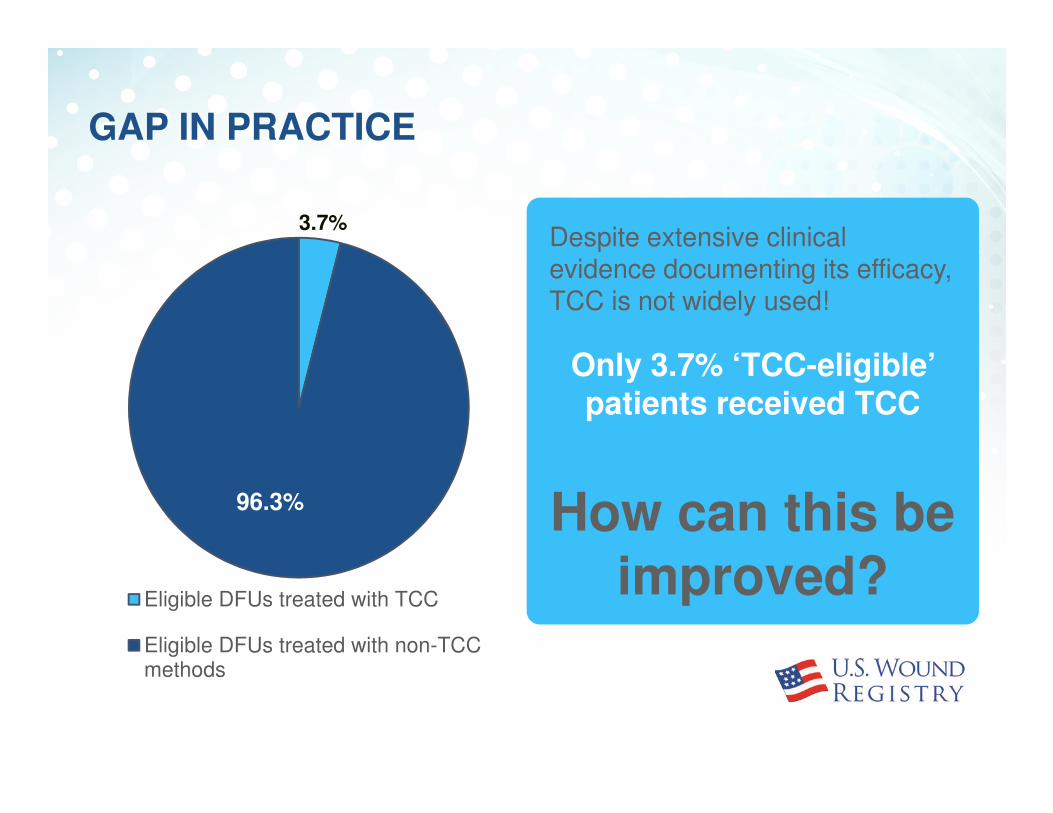
Despite extensive clinical evidence documenting its efficacy, TCC is not widely used!
Only 3.7% ‘TCC-eligible’ patients received TCC
How can this be improved?
GAP IN PRACTICE
3.7%
96.3%
Eligible DFUs treated with TCC
Eligible DFUs treated with non-TCCmethods

BARRIERS TO TCC
Clinician-related
• Lack of skill• Misperception that
TCC delays healing• Staff training barriers• Cost and time vs.
reimbursement
Patient-related
• Reluctance• Transportation
issues (driving)• Heavy patients• Fear of falling
Organizational
• Cost• Hard to integrate
into patient flow• Storage of supplies

CHANGE THE PARADIGM TO OVERCOME BARRIERS
Based on Registry Data:
Four times more patients were casted in clinics using
TCC-EZ® compared to traditional casts2
Traditional TCC TCC-EZ®
Novel “Roll-on” cast system
VS.
2. C. E. Fife, MD, et al, Diabetic foot ulcer off-loading: The Gap Between Evidence and Practice: Data from the U.S. Wound Registry. Advances in Skin and Wound Care, 27(7) p. 310-316, 2014
Consensus Statement: “Newer techniques that approximate the effect of traditional TCC, and which are easier to use and faster to apply, may increase the use of adequate off-loading in clinical practice.”1
1. Snyder RJ, et al. The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes. Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014
Education of Patients and Clinicians

IMPLICATIONS FOR PRACTICE
1Non-removable casts provide the most effective pressure-relieving intervention for the healing of DFUs.
3Use of this intervention has to be balanced against restrictions in movement, although patients may still be able to work and carry out daily activities.
4Where non-removable casts are not indicated (i.e. fall risks) or have not been successful, other interventions — such as removable devices, adhesive felt, or “off-loading” surgery — should be considered.
2TCC is a cost-effective method for DFU treatment.

GENERAL RECOMMENDATIONS
1Off-loading with casts as well as aggressive off-loading with other studied methods need to be more widely adopted in clinical practice
2Due to the increased likelihood of healing, TCC is recommended as the preferred method for effective pressure relief. Newer, easier to apply cast should be considered to overcome barriers to use
3More education is needed for the clinician and the patients to increase off-loading use and compliance
Snyder RJ, et al. The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes. Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014

NEW CLINICAL GUIDELINES TO OFF-LOAD & HELP HEAL DIABETIC FOOT ULCERS: ACTIONABLE EVIDENCE TO IMPROVE OUTCOMES
3. Andrew J. Applewhite, MD• Off-loading in practice• Practical Implementation in a clinic

USING TCC AS FIRST LINE TREATMENT
• Fear: Fear is probably one of biggest hurdles to TCC being used as first line treatment for off-loading DFUs
• With TCC-EZ®, we overcame those fears. TCC is standard of care at Baylor. Close to 90% of our DFU patients get a cast
Clinician-related Patient-related Organizational
OVERCOMING BARRIERS TO TCC

TCC-EZ® MAKES TCC EASIER
Jensen J, et al. TCC-EZ – Total Contact Casting System Overcoming the
Barriers to Utilizing a Proven Gold Standard Treatment. DF Con. 2008
TCC-EZ® offers the GOLD Standard of care
3 easy steps: prep, roll & apply
Completed in under 10 minutes
Ease & consistency of application helps to decrease potential for causing tissue damage
Requires minimal training time
Light-weight woven design offers a more comfortable fit
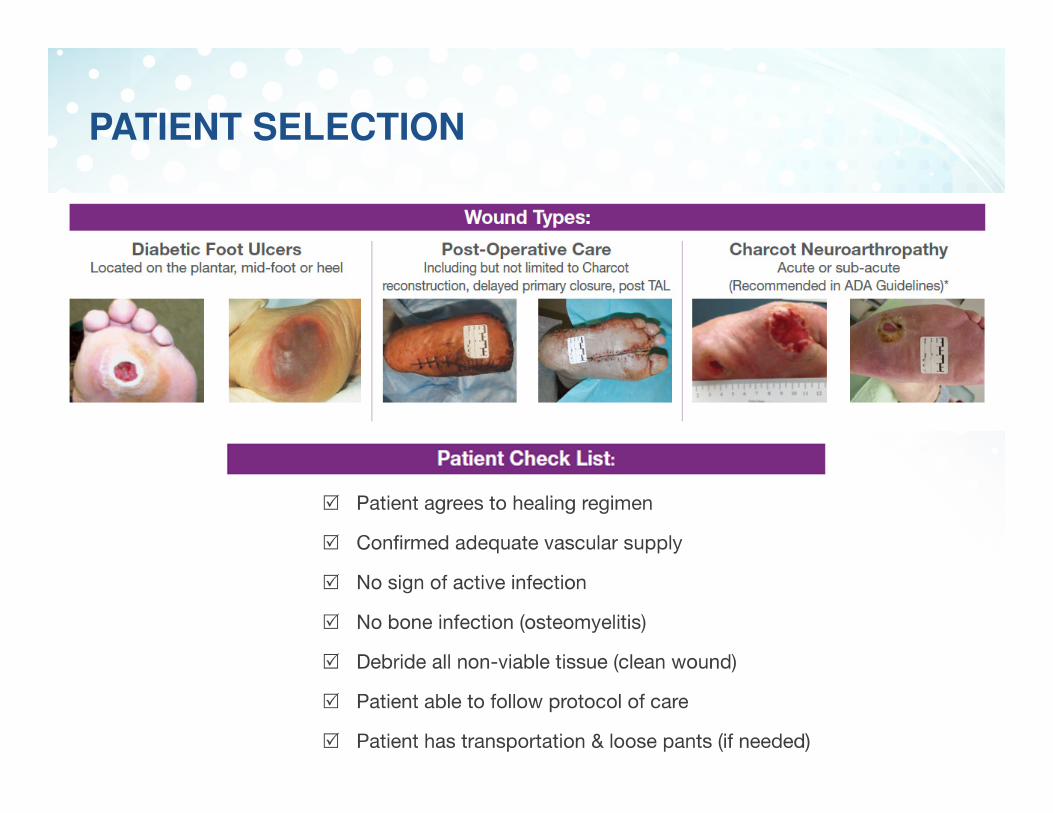
PATIENT SELECTION

HOW IT WORKS
• Casting in practice• Cast 5-10 patients per day
• 60% of patients have DFUs• Eventually 85-90% of patients will wear a TCC-EZ®
• TCC is the first line treatment for off-loading
• Patient Push Back• Talk with confidence to patient and family - explain that TCC is the
treatment of choice• Mortality is much higher for a DFU than a broken leg and with a
broken leg you would expect to be casted
• Consider use of other advanced technologies in conjunction with off-loading
• TCC in conjunction with CTP (Cellular- and/or Tissue-based Products)• TCC in conjunction with HBO

PATIENT FLOW
A BUSY METROPOLITAN WOUND CARE CENTER HAS SUCCESSFULLY INCORPORATED A ROLL-ON TOTAL CONTACT
CAST SYSTEM TO HEAL CHALLENGING FOOT WOUNDS
1. This case series will describe 14 patients that were treated with Total Contact Casting (TCC) to heal their challenging foot ulcers.
2. This case series will illustrate how integrating a scientifically proven modality such as TCC can lead to positive outcomes in healing diabetic foot ulcers in an outpatient wound care setting.
Methods:This series describes 14 patients with diabetic foot wounds. The wounds range in chronicity from 4 weeks to 1 1/2 years prior to being treated with TCC. The clinic staff were educated on the useof the Roll-on TCC Cast System. Wound assessment, debridement and topical wound therapy were used based on moist wound healing principles.1 Foot wounds and Charcot foot arthropathy2 were successfully off-loaded with the Roll-on TCC System to produce optimal patient outcomes.
References: 1. Bryant RA, Nix DP. Acute and Chronic Wounds: Current Management Concepts. 4th Edition. St. Louis, MO: Mosby Elsevier, 2012. 2. Rogers LC, et al: The Charcot Foot in Diabetes. Diabetes Care 34:2123-2129, 2011.
Clinical Poster Presented SAWC Fall, 2014

This 58-year-old female was admitted for osteomyelitis of first metatarsal head. She refused a toe amputation. After 6 weeks of IV antibiotics she agreed to proper off-loading and her wound healed in 8 weeks.
CASE 1
1.29.14 3.12.14 – 1st TCC application 5.07.14

This 49-year-old female was diagnosed with osteomyelitis and peripheral artery disease. After stent placement and IV antibiotics she was still reluctant to wear a cast. Once she agreed, she experienced healing in 8 weeks with Roll-on TCC.
CASE 2
3.26.14 4.24.14 5.28.14

14 PATIENT CASE SERIES
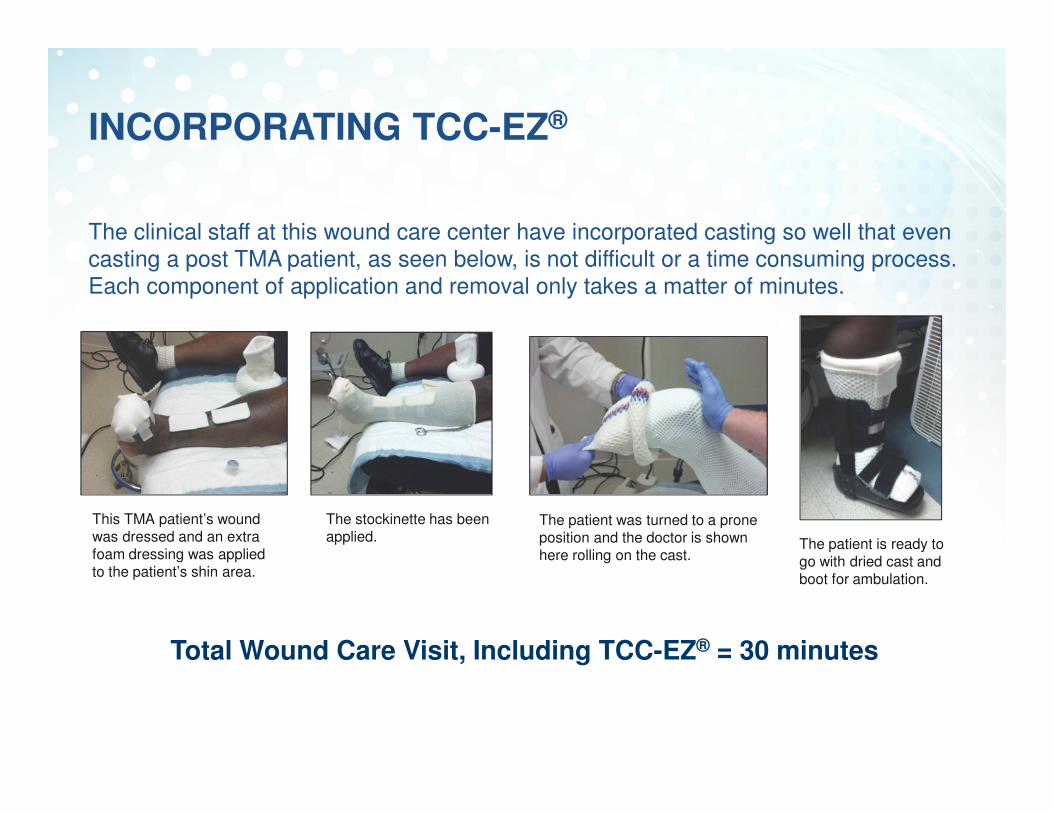
INCORPORATING TCC-EZ®
The clinical staff at this wound care center have incorporated casting so well that even casting a post TMA patient, as seen below, is not difficult or a time consuming process. Each component of application and removal only takes a matter of minutes.
This TMA patient’s wound was dressed and an extra foam dressing was applied to the patient’s shin area.
The stockinette has been applied.
The patient was turned to a prone position and the doctor is shown here rolling on the cast.
The patient is ready togo with dried cast andboot for ambulation.
Total Wound Care Visit, Including TCC-EZ® = 30 minutes

FINAL RESULTS & CONCLUSION
• All 14 patients achieved complete wound closure after implementation of TCC. Several wounds were healed in 4–6 weeks
• More complicated wounds took longer to heal as would be expected
• This case series demonstrates successful treatment regimens involving neuropathic and other complicated foot wounds treated with the Roll-on TCC System

CONCLUSION
• Even in clinics that use TCC, it is often only seen as last resort option when faced with an amputation, instead of being a first line treatment when indicated.
• The cost associated with DFUs are too high for us not to stop patients climbing the amputation staircase. As clinicians we need to lead the way.
Snyder RJ, et al. The Management of Diabetic Foot Ulcers through Optimal Off-loading. Building Consensus Guidelines and Practical Recommendations to Improve Outcomes. Journal of the American Podiatric Medical Association. Vol 104. No. 6. Nov/Dec 2014
What is holding you back? It’s a new year - will you make TCC first line therapy in your clinic?
QUESTIONS?
Find out more at about the leading casting system:
TCCEZ.com,patient website TCCpatient.com
David G. Armstrong, DPM, MD, PhDProfessor of Surgery and DirectorSouthern Arizona Limb Salvage Alliance (SALSA)University of Arizona College of Medicine
Robert Snyder, DPM, MScProfessor and Director, Clinical ResearchBarry University School of Podiatric MedicinePast President, Association for the Advancement of Wound Care
Andrew J. Applewhite, MDMedical Director, Comprehensive Wound Center of Baylor University Medical Center

SUMMARY OF EVIDENCE SUPPORTING THE CONSENSUS

REFERENCES
1. Snyder RJ, Kirsner RS, Warriner RA, 3rd, et al. Consensus recommendations on advancing the standard of care for treating neuropathic foot ulcers in patients with diabetes. Ostomy Wound Manage. 2010;56:S1.
2. Frykberg RG, Zgonis T, Armstrong DG, et al. Diabetic foot disorders. A clinical practice guideline (2006 revision). J
Foot Ankle Surg. 2006;45:S1.
3. Boulton AJ. Pressure and the diabetic foot: clinical science and offloading techniques. Am J Surg. 2004;187:17S.
4. Steed DL, Attinger C, Brem H, et al. Guidelines for the prevention of diabetic ulcers. Wound Repair Regen. 2008;16:169.
5. Cavanagh PR, Bus SA. Off-loading the diabetic foot for ulcer prevention and healing. J Vasc Surg. 2010;52:37S.
6. Bus SA. Priorities in offloading the diabetic foot. Diabetes Metab Res Rev. 2012;28:54.
7. Nabuurs-Franssen MH, Sleegers R, Huijberts MS, et al. Total contact casting of the diabetic foot in daily practice: a prospective follow-up study. Diabetes Care. 2005;28:243.
8. Castronuovo JJ, Jr., Adera HM, Smiell JM, et al. Skin perfusion pressure measurement is valuable in the diagnosis of critical limb ischemia. J Vasc Surg. 1997;26:629.
9. Gibbons GW, Shaw PM. Diabetic vascular disease: characteristics of vascular disease unique to the diabetic patient. Semin Vasc Surg. 2012;25:89.
10. Sumpio BE, Aruny J, Blume PA. The multidisciplinary approach to limb salvage. Acta Chir Belg. 2004;104:647.

REFERENCES
11. Sumpio BE, Lee T, Blume PA. Vascular evaluation and arterial reconstruction of the diabetic foot. Clin Podiatr
Med Surg. 2003;20:689.
12. Schaper NC, Andros G, Apelqvist J, et al. Diagnosis and treatment of peripheral arterial disease in diabetic patients with a foot ulcer. A progress report of the International Working Group on the Diabetic Foot. Diabetes
Metab Res Rev. 2012;28:218.
13. Bakker K, Apelqvist J, Schaper NC. Practical guidelines on the management and prevention of the diabetic foot 2011. Diabetes Metab Res Rev. 2012;28:225.
14. Frykberg RG, Wittmayer B, Zgonis T. Surgical management of diabetic foot infections and osteomyelitis. Clin
Podiatr Med Surg. 2007;24:469.
15. Lipsky BA, Berendt AR, Cornia PB, et al. 2012 Infectious Diseases Society of America clinical practice guideline for the diagnosis and treatment of diabetic foot infections. Clin Infect Dis. 2012;54:e132.
16. Lipsky BA, Peters EJ, Berendt AR, et al. Specific guidelines for the treatment of diabetic foot infections 2011. Diabetes Metab Res Rev. 2012;28:234.
17. Eneroth M, Apelqvist J, Stenstrom A. Clinical characteristics and outcomes in 223 diabetic patients with deep foot infections. Foot Ankle Int. 1997;18:716.
18. Edelson GW, Armstrong DG, Lavery LA, et al. The acutely infected diabetic foot is not adequately evaluated in an inpatient setting. J Am Podiatr Med Assoc. 1997;87:260.
19. Bus SA, Valk GD, van Deursen RW, et al. Specific guidelines on footwear and offloading. Diabetes Metab Res
Rev. 2008;24:S192.

REFERENCES
20. Lewis J, Lipp A. Pressure-relieving interventions for treating diabetic foot ulcers. Cochrane Database Syst Rev 1: CD002302, 2013.
21. Kirsner RS, Bell D, Gibbons G, et al. Expert recommendations for optimizing outcomes utilizing Apligraf® for diabetic foot ulcers. 2012; www.woundresearch.com/pdfs/wounds_orgo.pdf. Accessed May 30, 2013.
22. Rathur HM, Boulton AJ. Pathogenesis of foot ulcers and the need for offloading. Horm Metab Res. 2005;37:61.
23. Armstrong DG, Holtz-Neiderer K, Wendel C, et al. Skin temperature monitoring reduces the risk for diabetic foot ulceration in high-risk patients. Am J Med. 2007;120:1042.
24. Lavery LA, Armstrong DG. Temperature monitoring to assess, predict, and prevent diabetic foot complications. Curr Diab Rep. 2007;7:416.
25. Lavery LA, Higgins KR, Lanctot DR, et al. Preventing diabetic foot ulcer recurrence in high-risk patients: use of temperature monitoring as a self-assessment tool. Diabetes Care. 2007;30:14.
26. Zou D, Mueller MJ, Lott DJ. Effect of peak pressure and pressure gradient on subsurface shear stresses in the neuropathic foot. J Biomech. 2007;40:883.
27. Landsman AS, Meaney DF, Cargill RS, 2nd et al. 1995 William J. Stickel Gold Award. High strain rate tissue deformation. A theory on the mechanical etiology of diabetic foot ulcerations. J Am Podiatr Med Assoc.
1995;85:519.

REFERENCES
28. Bus SA, Waaijman R, Arts M, et al. Effect of custom-made footwear on foot ulcer recurrence in diabetes: a multicenter randomized controlled trial. Diabetes Care. 2013;36:4109.
29. Katz IA, Harlan A, Miranda-Palma B, et al. A randomized trial of two irremovable offloading devices in the management of neuropathic diabetic foot ulcers. Diabetes Care. 2005;28:555.
30. Steed DL, Attinger C, Colaizzi T, et al. Guidelines for the treatment of diabetic ulcers. Wound Repair Regen. 2006;14:680.
31. Rogers LC, Frykberg RG, Armstrong DG, et al. The Charcot foot in diabetes. Diabetes Care. 2011;34:2123.
32. Armstrong DG, Nguyen HC, Lavery LA, et al. Off-loading the diabetic foot wound: a randomized clinical trial. Diabetes Care. 2001;24:1019.
33. Gutekunst DJ, Hastings MK, Bohnert KL, et al. Removable cast walker boots yield greater forefoot off-loading than total contact casts. Clin Biomech (Bristol, Avon). 2011;26:649.
34. Bus SA, Valk GD, van Deursen RW, et al. The effectiveness of footwear and offloading interventions to prevent and heal foot ulcers and reduce plantar pressure in diabetes: a systematic review. Diabetes Metab Res Rev. 2008;24:S162.
35. Snyder RJ, Lanier KK. Offloading difficult wounds and conditions in diabetic patient. Ostomy Wound Manage. 2002;48:32.
REFERENCES
36. Armstrong DG, Lavery LA, Wu S, et al. Evaluation of removable and irremovable cast walkers in the healing of diabetic foot wounds: a randomized controlled trial. Diabetes Care. 2005;28:551.
37. Jimenez A. “Total contact casting,” in Update 2003, p 282, The Podiatry Institute; 2003.
38. Wertsch JJ, Frank LW, Zhu H, et al. Plantar pressures with total contact casting. J Rehabil Res Dev. 1995;32:205.
39. Armstrong DG, Short B, Espensen EH, et al. Technique for fabrication of an "instant total-contact cast" for treatment of neuropathic diabetic foot ulcers. J Am Podiatr Med Assoc. 2002;92:405.
40. Piaggesi A, Macchiarini S, Rizzo L, et al. An off-the-shelf instant contact casting device for the management of diabetic foot ulcers: a randomized prospective trial versus traditional fiberglass cast. Diabetes Care. 2007;30:586.
41. Van De Weg FB, Van Der Windt DA, Vahl AC. Wound healing: total contact cast vs. custom-made temporary footwear for patients with diabetic foot ulceration. Prosthet Orthot Int. 2008;32:3.
42. Owings TM, Apelqvist J, Senstro M, et al. Plantar pressures in diabetic foot ulcer patients who have remained healed. Diabet Med. 26:1141.
43. Foley F. Pressure point offloading in the diabetic foot. Primary Intention August. 1999;102-105.

REFERENCES
44. Birke JA, Pavich MA, Patout Jr CA, et al. Comparison of forefoot ulcer healing using alternative offloading methods in patients with diabetes mellitus. Adv Skin Wound Care. 2002;15:210.
45. Beuker BJ, Van Deursen RW, Price P, et al. Plantar pressure in offloading devices used in diabetic ulcer treatment. Wound Rep Regen. 2005;13:537.
46. Faglia E, Caravaggi C, Clerici G, et al. Effectiveness of removable walker cast versus nonremovable fiberglass off-bearing cast in the healing of diabetic plantar foot ulcer. A randomized controlled trial. Diabetes Care. 2010;33:1419.
47. de Souza LJ. Charcot arthropathy and immobilization in a weight-bearing total contact cast. J Bone Joint Surg
Am. 2008;90:754.
48. Pinzur MS, Lio T, Posner M. Treatment of Eichenholtz stage I Charcot foot arthropathy with a weightbearing total contact cast. Foot Ankle Int. 2006;27:324.
49. Trepman E, Pinzur MS, Shields NN. Application of the total contact cast. Foot Ankle Int. 2005;26:108.
50. Ha Van G, Siney H, Hartmann-Heurtier A, et al. Nonremovable, windowed, fiberglass cast boot in the treatment of diabetic plantar ulcers: efficacy, safety, and compliance. Diabetes Care. 2003;26:2848.
51. Fife CE, Carter MJ, Walker D. Why is it so hard to do the right thing in wound care? Wound Repair Regen. 2010;18:154.
52. Sinacore DR. Total contact casting for diabetic neuropathic ulcers. Phys Ther. 1996;76:296.

REFERENCES
53. Schuster MA, McGlynn EA, Brook RH. How good is the quality of health care in the United States? The Milbank
Quarterly. 1998;76:517.
54. Wu SC, Jensen JL, Weber AK, et al. Use of pressure offloading devices in diabetic foot ulcers: do we practice what we preach? Diabetes Care. 2008;31:2118.
55. Prompers L, Huijberts M, Apelqvist J, et al. Delivery of care to diabetic patients with foot ulcers in daily practice: results of the Eurodiale Study, a prospective cohort study. Diabet Med. 2008;25:700.
56. Reiber GE, Smith DG, Wallace C, et al. Effect of therapeutic footwear on foot reulceration in patients with diabetes: a randomized controlled trial. JAMA. 2002;287:2552.
57. Lavery LA, Vela SA, Fleischli JG, et al. Reducing plantar pressure in the neuropathic foot: a comparison of footwear. Diabetes Care. 1997;20:1706.
58. Armstrong DG, Lavery LA, Kimbriel HR, et al. Activity patterns of patients with diabetic foot ulceration: patients with active ulceration may not adhere to a standard pressure off-loading regimen. Diabetes Care. 2003;26:2595.
59. Maciejewski ML, Reiber GE, Smith DG, et al. Effectiveness of diabetic therapeutic footwear in preventing reulceration. Diabetes Care. 2004;27:1774.
60. Sheehan P, Jones P, Caselli A, et al. Percent change in wound area of diabetic foot ulcers over a 4-week period is a robust predictor of complete healing in a 12-week prospective trial. Diabetes Care. 2003;26:1879.

REFERENCES
61. Marston WA, Hanft J, Norwood P, et al. The efficacy and safety of Dermagraft in improving the healing of chronic diabetic foot ulcers: results of a prospective randomized trial. Diabetes Care. 2003;26:1701.
62. Veves A, Falanga V, Armstrong DG, et al. Apligraf Diabetic Foot Ulcer S. Graftskin, a human skin equivalent, is effective in the management of noninfected neuropathic diabetic foot ulcers: a prospective randomized multicenter clinical trial. Diabetes Care. 2001;24:290.
63. Edmonds M. European and Australian Apligraf Diabetic Foot Ulcer Study Group: Apligraf in the treatment of neuropathic diabetic foot ulcers. Int J Low Extrem Wounds. 2009;8:11.
64. Kashefsky H, Marston W. Total contact casting combined with human fibroblast-derived dermal tissue in 15 DFU patients. J Wound Care. 2012;21:236.





























