Embed Size (px)
Citation preview

Guidelines for the Management of Diabetic Foot and Leg Ulcers Ratified by: Drugs & Therapeutics Committee
Date of ratification: October 2013 Review Date: October 2016
Page 1 of 12
Guidelines for the Management of Diabetic Foot and Leg Ulcers
ID Number 2013 129
Author’s name Chantal Kong
Author’s job title Consultant Physician
Division Acute Medical Care
Department Diabetes & Endocrinology
Version number 2
Ratifying Committee Drugs & Therapeutics Committee
Ratified date October 2013
Review date October 2016
Upload date November 2013
Name of manager responsible for review Prema Singh
Job title of manager responsible for review Microbiologist Consultant
Email address for this manager [email protected]
Referenced (Yes/No) Yes
Key words (to aid searching) Diabetic, Foot, Leg Ulcers, Guidelines
User Group Clinical staff
The Trust is committed to promoting an environment that values diversity. All staff are responsible for ensuring that all patients and their carers are treated equally and fairly and not discriminated against on the grounds of race, sex, disability, religion, age, sexual orientation or any other unjustifiable reason in the application of this policy, and recognising the need to work in partnership with and seek guidance from other agencies and services to ensure that special needs are met.

Guidelines for the Management of Diabetic Foot and Leg Ulcers Ratified by: Drugs & Therapeutics Committee
Date of ratification: October 2013 Review Date: October 2016
Page 2 of 12
1. Change History 3
2. Introduction 3
3. Management of acute diabetic foot ulcers 3
4. Discharge and out-patient follow-up arrangements 3
5. Monitoring and Compliance 5
6. Management of the Acute Charcot Foot 6
Appendices
1 Antibiotic guidelines for the treatment of diabetic foot ulcers 7
2 Referral pathway for the acute diabetic foot to secondary care 8
3 Clinical Management Protocol for the Acute Diabetic Foot 9
4 Referral pathway for management of Acute Diabetic Charcot Foot 10
5 Diabetic Foot Inpatient Assessment Proforma 11

Guidelines for the Management of Diabetic Foot and Leg Ulcers Ratified by: Drugs & Therapeutics Committee
Date of ratification: October 2013 Review Date: October 2016
Page 3 of 12
1. Change History
Version Date Authors Reason Ratification Required
1 July 2013 Dr Chantal Kong New guideline Yes
2 October 2013 Dr Chantal Kong Revision Yes
2. Introduction
Diabetic foot ulcers are a major cause of morbidity and mortality and lead to the most common cause of non-traumatic lower extremity amputation in patients. As many as one in four diabetics will develop a foot problem at some point in their lives. Patients undergoing amputation exhibit a mortality rate of 50 – 75% within five years. Timely detection, early treatment and education of both patients and healthcare professionals in recognising clinical foot emergency is therefore essential in order to prevent foot complications /amputations and ultimately preserve life. This involves a partnership between professionals working together on a multi-disciplinary level across the health community in order to achieve maximum effectiveness. In the event that a clinical foot emergency is detected (identification of a foot ulcer/open wound/tissue breakdown or potential Charcot’s arthropathy), NICE guidelines recommend that the patient should receive a rapid assessment (within 24 hours where possible) and be referred to the Multidisciplinary Foot Care Team consisting of the Diabetes medical team, diabetes specialist nurses, podiatrists, vascular team, specialist orthopaedic team, tissue viability nurses and orthotists. Patients with active infected diabetes foot ulcers associated with moderate to severe cellulitis, faiIing to respond to oral antibiotics or with critical/near critical ischaemic limb should be admitted as an emergency for parenteral antibiotics and further urgent vascular assessment. In principle, these patients are best cared for by the Diabetes Medical team with prompt review by the vascular/specialist orthopaedic team (if osteomyelitis) unless if they have an acutely ischaemic toe(s)/ limb in which case they should be referred directly to the vascular team as well as with input by the Diabetes team. The attached flowcharts set out the recommended care pathway for these high risk patients.
3. Management
There are 8 factors which need to be managed:
Underlying loss of bone density suggesting osteomyelitis any foreign body gas in the deep tissues indicating severe infection Charcot’s joint

Guidelines for the Management of Diabetic Foot and Leg Ulcers Ratified by: Drugs & Therapeutics Committee
Date of ratification: October 2013 Review Date: October 2016
Page 4 of 12
2) Metabolic control Wound healing and neutrophil function is impaired by hyperglycaemia, therefore
tight glycaemic control (aim for CBG 4 - <10 mmol/l) is paramount along with optimal blood pressure control (NICE). Ensure no other systemic, metabolic or nutritional disturbance to retard healing.
Baseline blood tests required: FBC, CRP, U&Es, LFTs, recent HbA1c (within last 2 months), blood cultures if patient pyrexial or systemically unwell.
3) Vascular assessment
All patients with acutely ischaemic or neuroischaemic foot ulcers should be referred promptly to the vascular team for further assessment and early appropriate vascular investigations and intervention.
4) Wound management
All wounds should be debrided with removal of dead tissue and foreign bodies and cleaned up. Ulcers need to be dressed with sterile non-adherent dressings unless specified otherwise by the tissue viability nurses and podiatrists. Some cases may require surgical debridement.
5) Pain control
Ischaemic and neuroischaemic ulcers can be quite painful especially if infected. Please refer to West Hertfordshire Pain control guidelines. Initiate with simple analgesics. Many patients will require stronger narcotic analgesics. Consider the use of Entonox for acute pain relief, such as local non-surgical wound debridement. Refer to the pain control team for further specialist advice if unsure. Neuropathic pain may respond to Amitriptyline +/- Pregabalin +/- Duloxetine or other atypical agents and often needs specialist hospital referral.
6) Pressure relief
Bed rest facilitates wound healing. Avoidance of pressure can also be attained by e.g. crutches, wheelchairs, orthotic assessment (need to offload neuropathic ulcers by casting once open wound has healed).
7) Educational
Patients should be given full explanation of their foot problems with reinforcement of foot health care education with the intended management plan.
8) Antibiotics and Antimicrobial guidelines
All clinically infected wounds should have swabs taken and sent for microbiology, culture and sensitivity without delay. Deep swabs or deep tissue or bone sequestra should be sent after debridement. Blood cultures should also be taken if there is evidence of systemic infection clinically. There should be close consultation with the microbiology department and patients with positive results should be treated with appropriate antibiotics until there is evidence of clinical and microbiological cure.
Always take an allergy history before prescribing any drug and check on contraindications, cautions, drug interactions and adverse effects (refer to the British National Formulary www.bnf.org)
The following are guidelines for empirical treatment prior to positive culture results which should allow specific antibiotic treatment according to sensitivities. However, be aware that infections are usually more extensive than the initial appearance. Careful clinical assessment of the patient’s clinical status including severity of the infected diabetic ulcer/wound is vital to help decide on the most appropriate antibiotics along with any swab results. Advise consult with Microbiology if unsure.
Patients presenting with mildly infected foot ulcers (please see definition on next page) do not need hospital admission unless there is evidence of acute ischaemia and can be

Guidelines for the Management of Diabetic Foot and Leg Ulcers Ratified by: Drugs & Therapeutics Committee
Date of ratification: October 2013 Review Date: October 2016
Page 5 of 12
managed in the community. However, these patients should be promptly referred to the appropriate Diabetes Multidisciplinary Specialist Foot clinic following discharge from the acute trust.
Patients with moderate to severe infected diabetic foot ulcers especially with signs of near to critical limb ischaemia need acute hospital admission for further appropriate treatment and management including intravenous antibiotics initially.
All patients admitted with an active diabetic foot ulcer need to be followed up and should be promptly referred to the diabetes multidisciplinary foot clinic after hospital discharge.
Please fax copy of discharge summary with covering referral letter to the following:
Watford residents Maria Whitlock (Secretary) Dr Pusalkar (Consultant)
Tel Ext Fax
01923 217696 7696 01923 217952
Hemel & St Albans residents
Judith Conlon Drs Chantal Kong/ Thomas Galliford (Consultants)
Tel Ext Fax
01442 287083 2083 01442 287381
St Albans residents AS WELL AS TO:
Nancy Kemp (Temp secretary) Dr Chantal Kong (Consultant) Community Podiatry Service
Tel Ext Fax Tel Fax
01727 897858 4858 01727 897518 01582 711544 01582 760329
Patients may also be followed up in the vascular or orthopaedic clinics as requested by the appropriate surgical clinical teams.
It is crucial that all members of the multidisciplinary footcare team should communicate closely with each other on the best management care plan for each individual patient as well as on the agreed follow-up arrangements.
5. Monitoring and Compliance
In order to ensure effective continuing healing of infected diabetic foot ulcer wounds and improve patient compliance, it is important that patients are informed of their follow-up management and diabetes care plans including prescription of any antibiotics and/or other changes made to their other diabetes treatment, especially on discharge. A copy of the patient’s TTA should be sent to their GP as well as to the specialist foot team +/_ vascular/orthopaedic team as appropriate, including instructions to the GP regarding appropriate continuation of antibiotics if needed based on clinical review of the patient.
There should also be clear arrangements made for regular change of wound dressings, for eg, via the district nurses with appropriate clinical monitoring prior to being reviewed in the diabetes foot clinic.
Adherence to these guidelines will be monitored via regular audits carried out by the medical diabetes team.

Guidelines for the Management of Diabetic Foot and Leg Ulcers Ratified by: Drugs & Therapeutics Committee
Date of ratification: October 2013 Review Date: October 2016
Page 6 of 12
6. Management of Acute Charcot Joint
This is a serious condition which, if unrecognised and untreated, causes collapse and deformity with considerable long term morbidity and high risk for foot ulceration. Early diagnosis and treatment is essential. Charcot usually involves midfoot, but may involve any part of foot or ankle. It may be difficult to differentiate from osteomyelitis. Osteomyelitis is usually preceded by an ulcer and often affects the metatarsals and calcaneum, whereas Charcot Joint more often affects the midfoot or ankle. The differential diagnosis includes cellulitis, osteomyelitis or gout. History:
Suspect if acute onset unilateral erythema, oedema and warmth.
Pain may or may not be present.
History of mild trauma. Examination: Document the following:
Site and description of cellulitis/ulcer/deformity
Reflexes, light touch, vibration, position sense, pain and temperature, 10g monofilament
Pulses femoral, popliteal, DP and PT
Document lying and standing BP Investigations:
Us & Es, bone profile, CRP, urate, HbA1c, FBC, ESR, glucose
Foot x-ray (to include weight bearing view)
Isotope bone scan
MRI or white cell scan may be needed – Consultant decision only in consultation with radiologist.
Management:
Urgent referral to diabetes medical team.
Podiatry review same day if possible.
Urgent antibiotics if osteomyelitis is possible continue till excluded.
Optimise glycaemic control.
Radiology review. MRI scan may be required.
Review by orthopaedic foot surgeon with special interest.
Immobilisation non weight bearing cast for 1 month then total contact cast or aircast with very gradual mobilisation.
Regular measurements of CRP and Alk phosphatase at diagnosis and follow-up. Pharmacological: There is a limited evidence base for management of acute Charcot Joint and local protocols may vary.
Please seek urgent advice from Diabetes consultant. Pamidronate infusion under specialist supervision ONLY may be appropriate (up to 6 infusions at 2 to 4 weekly intervals may be necessary). This is an unlicensed indication. Follow-up:
Regular clinical assessment by foot health services, usually in consultation with diabetes physician.
Footwear assessment moulded inserts etc.
Regular podiatry 2 to 4 weeks when discharged
Orthopaedic follow-up may be indicated
Repeat isotope bone scan at 3 months and 6 months
The affected joint must be relieved of all pressure from weight bearing by an offloading orthotic appliance.

Guidelines for the Management of Diabetic Foot and Leg Ulcers
Page 7 of 12
Indication First line (Antibiotic naive) Alternative therapy, e.g. peniciliin allergy or non-
antibiotic naive
Duration/comment
Mild Infection:
Pus or 2 or more of: erythema, warmth, pain, tenderness, induration
Any cellulitis,2cm around the wound confined to skin or subcutaneous tissue, and
No evidence of systemic infection
Flucloxacillin 500 mgs qds PO Doxycycline 100mgs bd PO or Clindamycin 300 – 450 mg qds
7-14 days and review No hospital admission
required. Refer to the Diabetes MDT Specialist Foot
clinic.
Moderate infection:
Lymphatic streaking, deep tissue infection involving subcutaneous tissue, tendon, fascia, bone or abscess, or
Cellulitis >2cm, and
No evidence of systemic infection
Flucloxacillin1g qds IV(for MSSA or beta-haemolytic streptococci)
Alternatives: Co-Amoxiclav 625 mgs tds IV
Add Metronidazole 400 mg tds PO if anaerobes suspected
If pseudomonas isolated: Add Ciprofloxacin 500 mg bd PO
(PLSE CONSULT WITH MICROBIOLOGY)
If MRSA:
IV Teicoplanin Oral switch:
Rifampicin 300mg bd (with either trimethoprim 200mgs bd, doxycycline
100mg bd, or fusidic acid 500 mg tds) or Linezolid 600 mg bd
(see full Abx guidelines)
Osteomyelitis
Clindamycin 300-450mgs qds for 4-6 weeks minimum prior to review
If MRSA infection of bone, add Rifampicin 600mg bd or
Sodium Fusidate 500mg tds
Clindamycin 300 – 450 mg qds PO
If pseudomonas isolated: Add Ciprofloxacin 500 mg
bd PO
(PLEASE DISCUSS WITH MICROBIOLOGY FIRST DUE
TO RISK OF C. DIFFICILE)
14-21 days course and review
IV antibiotics may be switched to oral after
an appropriate interval
Rifampicin: Monitor patient’s LFTS weekly
Linezolid – monitor FBC weekly
Sodium Fusidate – monitor LFT’s
Severe Infection:
Any infection accompanied by severe toxicity (fever, chills, shock, vomiting, confusion, metabolic instability).
The presence of critical ischaemia of the involved limb may make the infection severe
Piperacillin/tazobactam 4.5 mgs tds IV Add gentamicin 5 mg/kg once daily if
required (Note: Initial oral therapy inappropriate)
If MRSA:
IV Teicoplanin Oral switch:
Rifampicin 300mg bd (with either trimethoprim 200mgs bd, doxycycline
100mg bd, or fusidic acid 500 mg tds) or Linezolid 600 mg bd
Osteomyelitis
Clindamycin 300-450mg qds for 4-6 weeks minimum prior to review
If MRSA infection of bone, add Rifampicin 600mg bd or
Sodium Fusidate 500mg tds
If penicillin-allergic or concerned about renal function
IV ciprofloxacin 400mg bd and metronidazole 500mg tds
Add IV Teicoplanin if MRSA suspected
If non-antibiotic naïve/not
penicillin allergic: IV piperacillin/tazobactam
4.5g tds, Add IV Teicoplanin if MRSA
suspected
Oral switch
Ciprofloxacin 500-750mg bd and metronidazole 400mg tds
14-28 days initially, then review
IV antibiotics may be switched to oral at an
appropriate interval
Rifampicin: Monitor patient’s LFT’s weekly
Linezolid – monitor
FBC weekly
Sodium Fusidate – monitor LFT’s
Limb/life threatening infected gangrene
Admit for Intravenous antibiotics and urgent surgical review
Piperacillin/tazobactam 4.5 mg tds IV and Metronidazole 500mg tds IV
Convert to oral therapy once clinically appropriate
Admit for Intravenous antibiotics and urgent surgical review
IV Teicoplanin 400 mg OD plus IV Ciprofloxacin 400mg bd plus Metronidazole 500mg tds
IV
14-28 day course and review
References:
Managing the Diabetic Foot. Edmonds M.E. and Foster A.V.M. Blackwell Sciences 2002 Diabetic Foot ulcer classification system for research purposes. Diabetes Metab Res Rev 20(Suppl 1):S90-5, Schaper (2004) A review of the revised Infectious Disease Society of America diabetic foot infection guidelines. The Diabetic Foot Journal
Vol 16 No2 2013; p56-62

Guidelines for the Management of Diabetic Foot and Leg Ulcers Ratified by: Drugs & Therapeutics Committee
Date of ratification: October 2013 Review Date: October 2016
Page 8 of 12
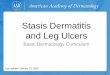
aaaaaabcabscess?/Ne
Refer urgently to Surgical Registrar on-call within 4 hrs
and to Medical SpR on-call for review
Refer to Medical Registrar
on-call (AAU L1)
Bloods (FBC, CRP, U&Es, glucose, HbAlc, blood cultures)
Plain Foot X-ray Deep wound swab If evidence of infection, start antibiotics
Refer urgently to Vascular Consultant on call for review within 24 hours
Admit under Vascular
team
Refer to Diabetes SpR (Bleep 1027) on the next
working day Admit Heronsgate Ward
(CAT1 Endo)
Bloods (FBC, CRP, U&Es, glucose, HbAlc, blood cultures)
Plain Foot X-ray Deep wound swab If evidence of infection, start antibiotics

Guidelines for the Management of Diabetic Foot and Leg Ulcers Ratified by: Drugs & Therapeutics Committee
Date of ratification: October 2013 Review Date: October 2016
Page 9 of 12
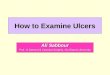
Clinical Management Protocol for the Acute Diabetic Foot
Examine patient’s feet and lower legs to detect risk factors:
Neuropathy (test foot sensation using 10g monofilament
or tuning fork for vibration)
Ischaemia (palpation of foot pulses)
Foot deformity
Inspection of footwear
DOCUMENT ON DIABETIC FOOT PROFORMA
Is the foot critically
ischaemic?
(Necrosis /gangrene)
Yes No
Refer urgently to Vascular
Surgical Team on call
Active foot ulceration
with moderate cellulitis
+ patient septic
Suspected acute Charcot’s
foot if hot foot +/- ulcer
Refer to:
Diabetes Medical Team
Vascular Team
TVN
Chiropodist
Baseline Assessment
Bloods (FBC, CRP, U&Es, glucose,
HbAlc, blood cultures)
Plain Foot X-ray
Deep wound swab
Start antibiotics (refer to WHHT
Diabetes Guidelines)
Offload the affected foot
Offload the affected foot
Refer to the Medical
Diabetes Team for further
assessment &
management
Once clinically stable and no
longer requiring in-patient
management, discharge to
the Diabetes MDT Foot clinic
+/- Vascular +/- Orthopaedic
clinics for follow-up

Guidelines for the Management of Diabetic Foot and Leg Ulcers Ratified by: Drugs & Therapeutics Committee
Date of ratification: October 2013 Review Date: October 2016
Page 10 of 12
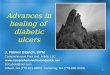
Appendix 4
CHARCOT REFERRAL PATHWAY
Definition: This diagnosis is always difficult and often mimics cellulitis/ foot infection initially. Think
Charcot if there is no break in the skin, the erythema is not very clearly demarcated, there is a lot of
foot or ankle swelling, any new deformity, or the patient has systemic symptoms. It is also worth noting
that Charcot occurs in the neuropath if previously diagnosed. If there is ANY doubt REFER!
Yes No
Yes No
No
Yes
Diabetes and Hot foot/feet +/- swelling
and/or deformity, pain or not
Is an ulcer present?
Follow the Acute Diabetic Foot ulcer
Pathway
Is there sign of cellulitis/infection?
Is the patient systemically
unwell, and/or are there signs
of toxicity?
Advise patient to non weight-bear
Refer to the MDT Foot clinic within
24 hrs
Follow the Acute Diabetic Foot ulcer
Pathway Start on oral Flucloxacillin 500 mgs qds or Doxycycline 100 mgs bd if
penicillin-allergic. Refer to MDT Foot clinic within 24
hrs. Risk stratify

Guidelines for the Management of Diabetic Foot and Leg Ulcers Ratified by: Drugs & Therapeutics Committee
Date of ratification: October 2013 Review Date: October 2016
Page 11 of 12
: Document ulcer size, ulcer depth, deformity (e.g. Charcot), cellulitis, gangrene.
Right Foot Left Foot
Posterior Tibial Present Absent
Present Absent
Dorsalis Pedis Present Absent
Present Absent
Sensation Normal Impaired - see next step Level:______________________
Normal Impaired – see next step Level:________________________
DATE _ _ / _ _ / _ _ _ _ Growth: ______________________________________________________ DATE _ _ / _ _ / _ _ _ _ Growth: ______________________________________________________ DATE _ _ / _ _ / _ _ _ _ Growth: ______________________________________________________
Q: Has the patient been on antibiotics for a diabetic foot problem pre-admission? Y / N Q: If yes, please state type of antibiotic(s) and duration: ____________________________
(place patient label OR complete the following:
Name:…………………………………………………….. D.O.B:…………………………………………………….. Hospital no:………………………………………………..

Guidelines for the Management of Diabetic Foot and Leg Ulcers Ratified by: Drugs & Therapeutics Committee
Date of ratification: October 2013 Review Date: October 2016
Page 12 of 12