Embed Size (px)
DESCRIPTION
Citation preview

NEURO-ONCOLOGYPROGRAM ACCREDITATION APPLICATION
PROGRAM INFORMATION FORM (PIF)
FOR NEW APPLICATIONS ONLY
Revised: 08-20-08
A. INTRODUCTION
The mission of the United Council for Neurologic Subspecialties (UCNS) is to provide an accreditation and certification process for fellowship training programs with the goals of enhancing quality training in Neurologic subspecialties and quality patient care. The Accreditation Council (AC) strives to develop evaluation methods and processes that are valid, effective, fair, open and ethical. The AC is a voluntary accreditation organization and functions as a council of the UCNS. To be an accredited program by the UCNS, compliance with the program requirements is monitored through completion of the Program Information Form (PIF). In creating this form, the AC has referenced the model used by the Accreditation Council for Graduate Medical Education (ACGME).
B. INSTRUCTIONS
APPLICATION FOR NEW PROGRAM: This form is for use by programs making initial application only.
All programs, new and existing, must complete the entire Program Information Form.
For new training programs where statistical data are not available, e.g., number of graduates, you should mark that section as “NA” (not applicable).
The PIF template and Appendix A-G template should be downloaded and completed off-line. The PIF template question fields should not be altered. The space in text and tables for responses will expand to accommodate your program’s needs. The page numbers will automatically reformat. Once it is completed, submit the PIF form and Appendices A-G document electronically via e-mail to the UCNS at [email protected]. The UCNS will send a confirmation acknowledging receipt of the application. Should you require additional space in specific fields, please e-mail the UCNS. The Program Director is responsible for the content of the completed form, and the information will not be considered complete without the Program Director’s signature. All sections of the form applicable to the program must be completed in order to be accepted for review. If any requested information is not available, an explanation should be given in the appropriate place on the form.
Many items require a composed response to a specific question. Please respond briefly and concisely.
The form also includes requests for the following additional data. Please use the Appendix A-G template to provide this information.
Appendix A: participating institution letter from Department Chair(s) of the participating institution (not the full affiliation agreement; not Program Letter of Agreement)
Appendix B: one page curriculum vitae (Program Director and faculty)Appendix C: written goals and objectives by year and rotationUCNS Program Accreditation Application Page 1 of 21Neuro-Oncology 2008
Appendix D: list of clinical conferences at each institution; list of clinical lectures, conferences, courses in other areas; list of other lectures
Appendix E: list of neuro-oncology meetings attended by fellowsAppendix F: list of research projects by fellowsAppendix G: list of publications by fellows
Please do not attach any unnecessary materials such as reprints, brochures, annual reports, schedules, minutes of meetings and conferences, etc. The UCNS considers only the information requested on the PIF form and provided in the appendices. Any extra material not requested will be discarded. C. APPLICATION FEE
The UCNS has two program application categories: New Applicant and Continuing Applicant. You are applying for program accreditation as a New Applicant.
New Applicant $3150 Application Fee ($1150 first-year accreditation fee + $2000 non-refundable application fee)
The accreditation year is the academic year, July 1 through June 30. An annual accreditation fee will be assessed at $1150. Fees are subject to change.
D. PAYMENT
The UCNS accepts checks (or money orders) only at this time. Please submit payment in US funds (payable to United Council for Neurologic Subspecialties) to the UCNS Executive Office, 1080 Montreal Avenue, Saint Paul, MN 55116.
E. APPLICATION DEADLINE
The UCNS accepts applications throughout the year and reviews applications twice per year, in the spring and fall. Your application must be submitted and payment received by July 1, 2008, for fall 2008 review and accreditation for the 2009 academic year (beginning July 1, 2009). The next deadline is December 31, 2008, for spring 2009 review and accreditation for the 2009 academic year.
F. PROGRAM SITE REVIEW
A site review of the program will not normally be required for the first application of programs. Should the UCNS determine that a site visit is necessary; you will be notified and provided the additional necessary information.
G. ADMINISTRATIVE STAFF CONTACTS FOR QUESTIONS
Contact the UCNS Executive Office with questions: UCNS Executive Office, 1080 Montreal Ave., St. Paul, MN 55116 Tel: 651-695-2816 Fax: 651-361-4916 E-mail: [email protected].
H. GLOSSARY OF TERMS
A glossary of terms used in the Program Requirements and PIF can be found on the UCNS website at www.ucns.org.
UCNS Program Accreditation Application Page 2 of 21Neuro-Oncology 2008
I. TABLE OF CONTENTS
Section
1 Program Information
1.A Program Identification
1.B Program Director Information
2 Institutional Affiliates
3 Fellow Information
3.A Number of Positions
3.B Actively Enrolled Fellows
3.C Aggregate Data on Fellows Completing or Leaving the Program for the Last Three (3) Years
3.D Fellows Completing the Program in the Last Three Years
3.E Fellows Leaving the Program in the Last Three Years
4 Faculty & Personnel
4.A Program Director
4.B Program Teaching Faculty—Neuro-Oncology
4.C Other Teaching Faculty
5 Facilities and Resources
5.A Facilities
5.B Library Facilities
6 Educational Program
6.A Curriculum
6.B Seminars and Conferences
6.C Educational Program
6.D Educational Policies
7 Research and Scholarly Activity
7.A Fellow Meeting Attendance
7.B List of Research Projects by Fellows
7.C List of Publications by Fellows
7.D Scholarly Activity Summary
8 Evaluation
8.A Fellow Evaluation
8.B Program Evaluation
8.C Curriculum Development
8.D Curriculum Evaluation
9 Signatures
AppendicesAppendix A: participating institution letter(s) from department chair(s) of participating
institution(s) (not the full affiliation agreement; not Program Letter of Agreement)Appendix B: one page curricula vitae (Program Director and faculty)
Appendix C: written goals and objectives by year and rotationAppendix D: list of clinical conferences at each institution; list of clinical lectures, conferences,
courses in other areas; list of other lecturesAppendix E: list of neuro-oncology meetings attended by fellowsAppendix F: list of research projects by fellowsAppendix G: list of publications by fellows
UCNS Program Accreditation Application Page 3 of 21Neuro-Oncology 2008
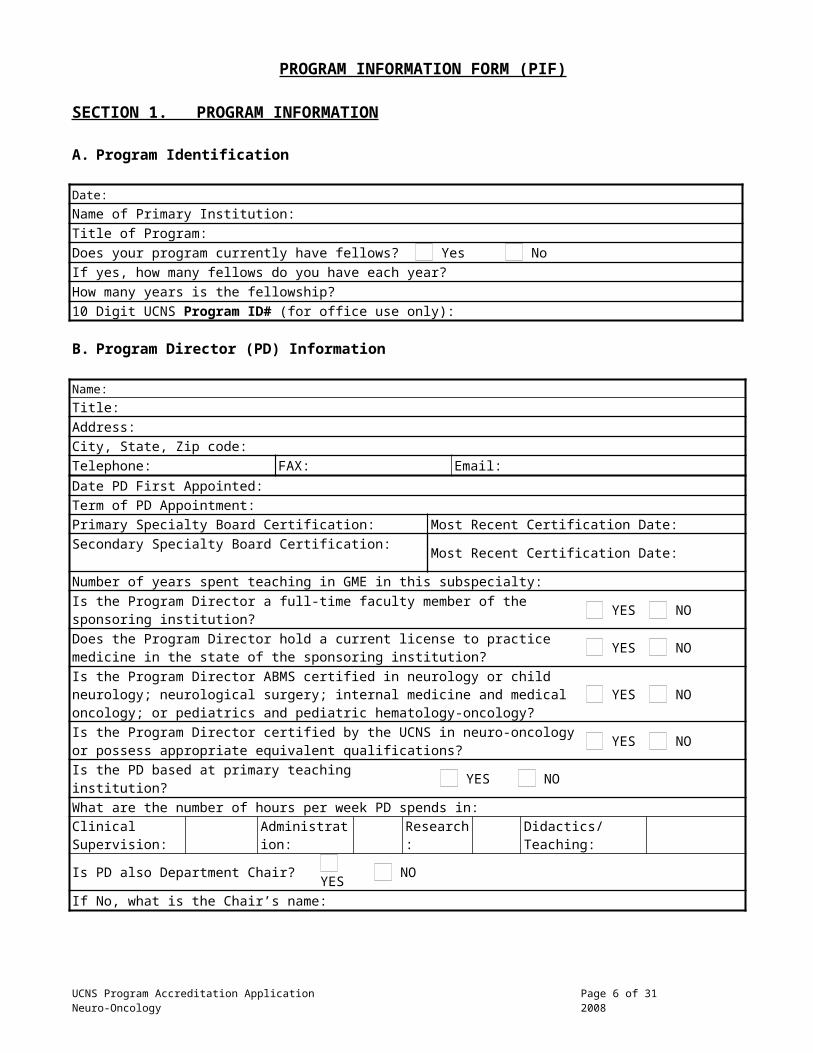
PROGRAM INFORMATION FORM (PIF)
SECTION 1. PROGRAM INFORMATION
A. Program Identification
Date:
Name of Primary Institution:
Title of Program:
Does your program currently have fellows? Yes No
If yes, how many fellows do you have each year?
How many years is the fellowship?
10 Digit UCNS Program ID# (for office use only):
B. Program Director (PD) Information
Name:
Title:
Address:
City, State, Zip code:
Telephone: FAX: Email:
Date PD First Appointed:
Term of PD Appointment:
Primary Specialty Board Certification: Most Recent Certification Date:
Secondary Specialty Board Certification: Most Recent Certification Date:
Number of years spent teaching in GME in this subspecialty:
Is the Program Director a full-time faculty member of the sponsoring institution? YES NODoes the Program Director hold a current license to practice medicine in the state of the sponsoring institution?
YES NO
Is the Program Director ABMS certified in neurology or child neurology; neurological surgery; internal medicine and medical oncology; or pediatrics and pediatric hematology-oncology?
YES NO
Is the Program Director certified by the UCNS in neuro-oncology or possess appropriate equivalent qualifications?
YES NO
Is the PD based at primary teaching institution? YES NO
What are the number of hours per week PD spends in:Clinical Supervision:
Administration: Research: Didactics/Teaching:
Is PD also Department Chair? YES NO
If No, what is the Chair’s name:
UCNS Program Accreditation Application Page 4 of 21Neuro-Oncology 2008

SECTION 2. INSTITUTIONIONAL AFFILIATES (Program Requirements II, A, B)
SPONSORING INSTITUTION: (Institution #1) (The university, hospital, or foundation that has ultimate responsibility for this program.)Name of Sponsor: Address: Sponsoring Core Residency Program?
YES NOCity, State, Zip code:
Type of Institution: (e.g., Teaching Hospital, General Hospital, Medical School):
Ownership Type: (e.g., State, Corporation, Church):
Is Institution ACGME Accredited YES NO Length of Accreditation: Next review date:
Name of DIO (Designated Institutional Official) Responsible for Oversight of Training at this Institution:
Does SPONSOR have an affiliation with a medical school (could be the sponsoring institution)?
YES NO
If yes, name the medical school below.
Name of Medical School #1:
Name of Medical School #2:
PRIMARY INSTITUTION (Institution #2) If different than the sponsoring institution.
Name:
Address:
City, State, Zip Code: Name of Individual Responsible for Oversight of Training at This Institution: (Site Coordinator):
Type of Institution: (e.g., Teaching Hospital, General Hospital, Medical School):
PARTICIPATING INSTITUTION (Institution #3) If more than one participating institution, please e-mail [email protected].
Name:
Address:
City, State, Zip Code: Distance between Institutions 1 & 2:
Miles: Minutes:
Type of Rotation (select one)
Elective Required Both
Length of Fellows Rotation (in months) Year 1: Year 2:
Name of Individual Responsible for Oversight of Training at This Institution (Site Coordinator):
Type of Institution: (e.g., Teaching Hospital, General Hospital, Medical School):
Brief Educational Rationale for Use of This Institution:
UCNS Program Accreditation Application Page 5 of 21Neuro-Oncology 2008
RELATED CORE PROGRAM IN NEUROLOGY OR CHILD NEUROLOGY
Name of Institution or Hospital:
Address:
City, State, Zip Code: Website Address:
Date Program Approved for Accreditation:
Next Review Date:
Name of Program Director:
Total Number of Faculty:
RELATED CORE PROGRAM IN NEUROLOGICAL SURGERY
Name of Institution or Hospital:
Address:
City, State, Zip Code: Website Address:
Date Program Approved for Accreditation:
Next Review Date:
Name of Program Director:
Total Number of Faculty:
RELATED CORE PROGRAM IN INTERNAL MEDICINE AND MEDICAL ONCOLOGY
Name of Institution or Hospital:
Address:
City, State, Zip Code: Website Address:
Date Program Approved for Accreditation:
Next Review Date:
Name of Program Director:
Total Number of Faculty:
RELATED CORE PROGRAM IN PEDIATRICS AND PEDIATRIC HEMATOLOGY-ONCOLOGY
Name of Institution or Hospital:
Address:
City, State, Zip Code: Website Address:
Date Program Approved for Accreditation:
Next Review Date:
Name of Program Director:
Total Number of Faculty:
SECTION 3. FELLOW INFORMATION
A. Number of Positions (For the current academic year)
UCNS Program Accreditation Application Page 6 of 21Neuro-Oncology 2008

Positions Year 1 Year 2 Total
Number of Requested Positions
Number of Filled Positions*
*For established programs without currently active fellows, complete table with 0 and indicate here when last fellow finished: For programs that have never had fellows, complete table with “NA”.
Note: The total number of fellows in years 1 and 2 should not exceed the 2:1 faculty to fellow ratio for the fellowship program. Faculty included in determining the ratio are those listed in section 4.B. See Program Requirements III.A.4.
B. Actively Enrolled Fellows (if applicable) (Program Requirements III)
1. List all fellows actively enrolled in this program as of August 31 of current academic year (see Section 3.A). List names alphabetically. Indicate fellows accepted as transfer with an asterisk (*).
YEAR ONE
Name Medical SchoolPrior GME training
programABPN/RCPSC eligible or
Certified?
YES NO YES NO YES NO YES NO YES NO YES NO
YEAR TWO
Name Medical SchoolPrior GME training
programABPN/RCPSC eligible or
Certified?
YES NO YES NO YES NO YES NO YES NO YES NO
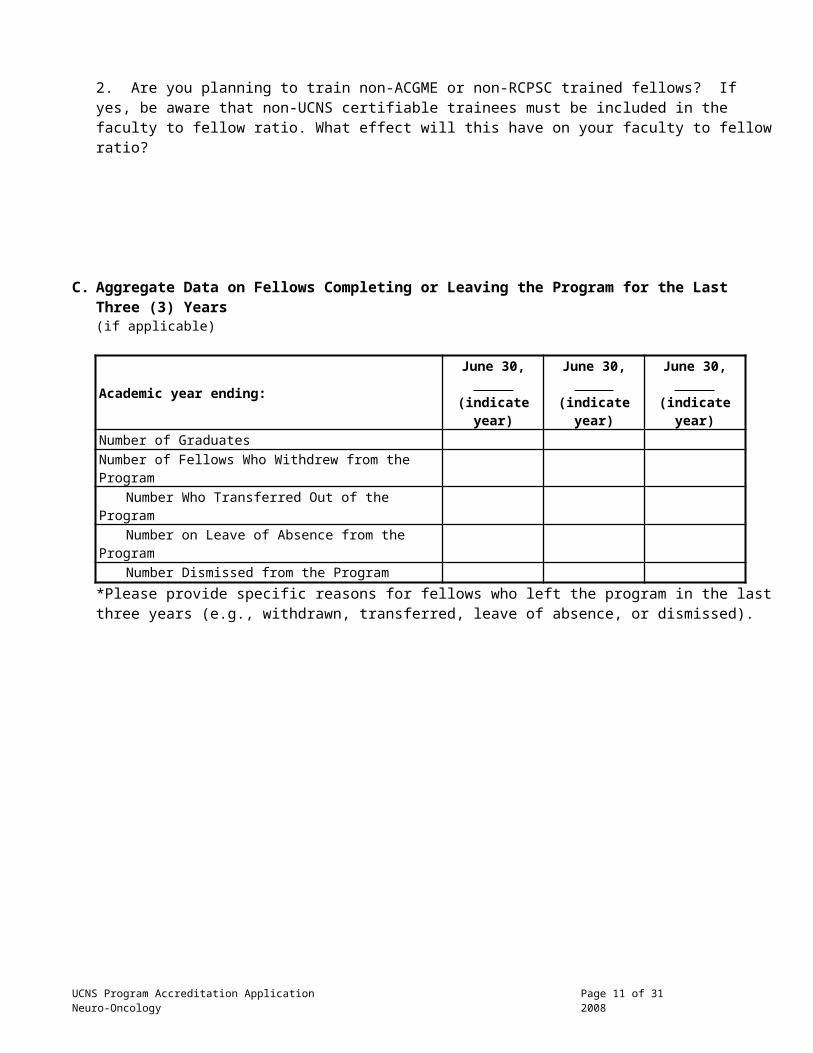
2. Are you planning to train non-ACGME or non-RCPSC trained fellows? If yes, be aware that non-UCNS certifiable trainees must be included in the faculty to fellow ratio. What effect will this have on your faculty to fellow ratio?
C. Aggregate Data on Fellows Completing or Leaving the Program for the Last Three (3) Years (if applicable)
UCNS Program Accreditation Application Page 7 of 21Neuro-Oncology 2008
Academic year ending:June 30, (indicate year)
June 30, (indicate year)
June 30, (indicate year)
Number of Graduates
Number of Fellows Who Withdrew from the Program
Number Who Transferred Out of the Program
Number on Leave of Absence from the Program
Number Dismissed from the Program
*Please provide specific reasons for fellows who left the program in the last three years (e.g., withdrawn, transferred, leave of absence, or dismissed).
D. Fellows Completing Program in the Last Three Years (if applicable). List of fellows who completed all training for this subspecialty based on the last full academic year ending June 30, .
Name Start DateActual Date of Completion
Practice Position
ABPN/RCPSC Certified?
UCNS Certified?
YES NO YES NO
YES NO YES NO
YES NO YES NO
List of fellows who completed all training for this subspecialty based on the last academic year ending June 30, .
Name Start DateActual Date of Completion
Practice Position
ABPN/RCPSC Certified?
UCNS Certified?
YES NO YES NO
YES NO YES NO
YES NO YES NO
List of fellows who completed all training for this subspecialty based on the last academic year ending June 30, .
Name Start DateActual Date of Completion
Practice Position
ABPN/RCPSC Certified?
UCNS Certified?
YES NO YES NO
YES NO YES NO
YES NO YES NO
UCNS Program Accreditation Application Page 8 of 21Neuro-Oncology 2008
SECTION 4. FACULTY AND PERSONNEL
A. Program Director (Program Requirements IV, A, B)
1. Describe the Program Director’s qualifications in neuro-oncology. Indicate appropriate qualifications, including subspecialty expertise in neuro-oncology and at least five years in post graduate practice, as well as documented clinical, educational and administrative abilities, and experience in his/her field.
2. Describe the Program Director’s prior experience in the training of medical students or post-doctoral medical or surgical trainees.
3. Describe how the Program Director is able to foster and optimize multidisciplinary interactions and teaching in neuro-oncology within the institution(s).
4. Give a brief description of the Program Director’s responsibilities and activities. Attach one page curriculum vitae (Appendix B) for the Program Director (use Appendix B form). CVs using the NIH Biographical Sketch format will be accepted as long as it provides current hospital staff privileges.
B. Required Faculty - Neuro-Oncology (Program Requirements IV, D)
1. Neuro-Oncologista) Is a board certified neurologist or child neurologist a member of the program faculty?
YES NO If yes, is this neurologist also board certified in medical or pediatric oncology?
YES NO If no, is neurologist supported by a faculty member who is board certified in either medical or pediatric oncology?
YES NO
b) Is a board certified medical or pediatric oncologist a member of the program faculty? YES NO
If yes, is this oncologist board also certified in neurology or child neurology? YES NO
If no, is oncologist supported by a faculty member who is board certified in either neurology or child neurology?
YES NO
c) Is a board certified (in neurological surgery) neurosurgeon a member of the program faculty? YES NO Is the neurosurgeon supported by a faculty member who is board certified in medical or pediatric
oncology? YES NO
2. Is a neurosurgeon with reasonable experience in surgical treatment of neuro-oncology patients and management of patients with central nervous system tumors a member of the program faculty?
YES NO
3. Is a radiation oncologist a member of the program faculty? YES NO
UCNS Program Accreditation Application Page 9 of 21Neuro-Oncology 2008

4. Is a neuro-radiologist a member of the program faculty? YES NO
5. Is a neuro-pathologist or general pathologist a member of the program faculty? YES NO
6. Is a medical oncologist a member of the program faculty? YES NO
7. Does your program offer pediatric neuro-oncology fellowships? YES NO
If yes, is a pediatric neuro-oncologist a member of the program faculty? YES NO
UCNS Program Accreditation Application Page 10 of 21Neuro-Oncology 2008
List all members of the program responsible for training. For those with dual appointments, identify primary appointment (neurology or other department) in parentheses.
Note: These faculty members count toward the program’s faculty to fellow ratio.
See Section 2 for institution numbers.
Name, Degree, Title and Position
Role in Curriculum
Privileges at
Institution #1,2,3,4
Full-Time
If Part-time, State Current
Certification* Wks/Yr
Hrs/Wk
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
Attach a one page curriculum vitae (Appendix B) for each of the faculty listed above (use Appendix B form). CVs using the NIH format Biographical Sketch format will be accepted as long as they provide current hospital staff privileges.
If additional rows are needed to list more than 18 faculty, please e-mail [email protected].
*Indicate certification by ABMS or RCPSC and the specialties in which certified. Indicate certification by UCNS and the subspecialty in which certified.
UCNS Program Accreditation Application Page 11 of 21Neuro-Oncology 2008

C. Other Teaching Faculty
List other teaching faculty regularly involved in teaching fellows, including consultants and basic science faculty. Note their department, title and certifying credentials, and supervisory responsibilities to the program.
See Section 2 for institution numbers.
Name, Degree, Title and Position
Role in Curriculum
Privileges at
Institution #1,2,3,4
Full-Time
If Part-time, State Current
Certification* Wks/Yr
Hrs/Wk
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
Attach one page curriculum vitae (Appendix B) for members with major teaching responsibilities (use Appendix B form). CVs using the NIH Biographical Sketch format will be accepted.
If additional rows are needed to list more than 18 faculty, please e-mail [email protected].
*Indicate certification by ABMS or RCPSC and the specialties in which certified. Indicate certification by UCNS and the subspecialty in which certified.
UCNS Program Accreditation Application Page 12 of 21Neuro-Oncology 2008
SECTION 5. PROGRAM RESOURCES AND FACILITIES (Program Requirements V, F)
A. Facilities
1. Facilities and resources for training
See Section 2 for institution numbers.
Are the following office space and resources available?
Faculty and ResourcesInst
1Inst
2Inst
3Inst
4
a. Neuro-Oncology Faculty Offices and Facilities YES
NO YES
NO YES
NO YES
NOIs there administrative support for the Fellowship & Program Director?
YES NO
YES NO
YES NO
YES NO
Is a clinical and/or research nurse a member of the program faculty?
YES NO
YES NO
YES NO
YES NO
b. Fellow Offices and Resources
Does each fellow have his/her own office? YES
NO YES
NO YES
NO YES
NO
Are the offices for groups of fellows? YES
NO YES
NO YES
NO YES
NO
Is there dedicated administrative support for fellows? YES
NO YES
NO YES
NO YES
NODoes the fellow have access to other office equipment such as copiers, slide projectors, PowerPoint, video projection equipment or services for slides presentations, illustration services?
YES NO
YES NO
YES NO
YES NO
c. Laboratory Facilities YES
NO YES
NO YES
NO YES
NO
d. Imaging Facilities YES
NO YES
NO YES
NO YES
NO
e. Psychiatric Consultation YES
NO YES
NO YES
NO YES
NO
f. Psychological Services YES
NO YES
NO YES
NO YES
NO
g. Pain Services YES
NO YES
NO YES
NO YES
NO
h. Chemotherapy YES
NO YES
NO YES
NO YES
NO
i. Radiation Oncology YES
NO YES
NO YES
NO YES
NO
j. Neuropathology YES
NO YES
NO YES
NO YES
NOk. Social Work and Case Management Including Palliative Care and
Hospice YES
NO YES
NO YES
NO YES
NO
2. Briefly describe conference facilities at each institution that will be used for neuro-oncology conferences.
3. Briefly describe the space provided for neuro-oncology program faculty and fellow research at each institution. (Program Requirements V, F)
UCNS Program Accreditation Application Page 13 of 21Neuro-Oncology 2008

B. Library Facilities
Use the table below to describe the institutional and departmental library holdings and other reference resources at each institution.
See Section 2 for institution numbers.
Are the following facilities and resources available?
Library FacilitiesInst
1Inst
2Inst
3Inst
4a. Journals
Access to Medline YES NO
YES NO
YES NO
YES NO
b. Computer databases available YES NO
YES NO
YES NO
YES NO
Access in hospital YES NO
YES NO
YES NO
YES NO
Access in library YES NO
YES NO
YES NO
YES NO
24 hour access YES NO
YES NO
YES NO
YES NO
Access to major texts and full text journals YES NO
YES NO
YES NO
YES NO
Internet search capabilities YES NO
YES NO
YES NO
YES NO
c. Library available on site YES NO
YES NO
YES NO
YES NO
Library with major texts in all areas of medicine on site or nearby YES NO
YES NO
YES NO
YES NO
Interlibrary loan capability YES NO
YES NO
YES NO
YES NO
Textbook availability YES NO
YES NO
YES NO
YES NO
Major Neuro-oncology texts on wards YES NO
YES NO
YES NO
YES NO
Major Neuro-oncology texts in clinic YES NO
YES NO
YES NO
YES NO
Teleconference capability YES NO
YES NO
YES NO
YES NO
UCNS Program Accreditation Application Page 14 of 21Neuro-Oncology 2008

SECTION 6. EDUCATIONAL PROGRAM
A. Curriculum
Describe in block form the typical curriculum for fellows by months (or four-week stints), not weeks, including the institution (#1, 2, 3, 4) as listed in Section 2. If you require an extended table, please email a request to [email protected].
Please refer to Program Requirements V.D. for a required triad of clinical experiences in neuro-oncology. Curricular components may be offered in blocks or longitudinally. An example of the latter is a regularly scheduled clinic attended over a period of time while assigned to other rotations. Those components offered in block assignments each year should be recorded in the block template. Those clinical experiences offered longitudinally should be recorded separately in the longitudinal templates by year. You should not include conferences, lectures or other didactic experiences in the longitudinal template.
Include the goals and objectives for each of these curricular assignments and the programs overall goals and objectives as Appendix C.
1. Have these goals and objectives been provided to the fellows? YES NO
BLOCK ROTATIONS –YEAR 1
July August September October November December January February March April May June
LONGITUDINAL EXPERIENCES - YEAR 1
Type Of ExperienceTime Commitment/Weekly Structured
Number Of Weeks/YearAmount Of Time in Months (e.g. 40 Half Days=1 Month)
UCNS Program Accreditation Application Page 15 of 21Neuro-Oncology 2008

Include the goals and objectives for each of these curricular assignments and the program’s overall goals and objectives as Appendix C.
2. Have these goals and objectives been provided to the fellows? YES NO
BLOCK ROTATIONS - YEAR 2
July August September October November December January February March April May June
LONGITUDINAL EXPERIENCES – YEAR 2
Type Of Experience Weekly Structured Number Of WeeksAmount Of Time in Months (e.g. 40 Half Days=1 Month)
UCNS Program Accreditation Application Page 16 of 21Neuro-Oncology 2008

B. Seminars and Conferences (Program Requirements V, C)
1. Attach a schedule of clinical conferences for fellows in each institution (Appendix D). Name the faculty member assigned to each conference. Indicate which conferences are mandatory for fellows.
2. Attach a list of required lectures (>50 in total) comprising the formal didactic component of the fellowship (see Program Requirements V.C.1). (Appendix D)
3. Attach a list of the courses, conferences and/or lectures given in each of the other areas required in the program (Appendix D).
4. Attach a list of lectures not already supplied, such as lectures by visiting neuroscientists (Appendix D).
5. Is there a journal club? YES NO
Specify attendance by fellow and faculty, the frequency of meeting, and the organization of the club. If there is no journal club, what substitutes for it?
C. Educational Program
1. What teaching responsibilities do fellows have?
2. Describe how the program has integrated the six Accreditation Council for Graduate Medical Education (ACGME) core competencies (www.acgme.org) listed below into the didactic and clinical curriculum. Describe the method(s) used to evaluate fellow performance in each area (e.g. fellow, director, and faculty evaluation also known as 360 degree evaluation; patient surveys; portfolios; record review; simulations; standardized oral exams; standardized patients; written examinations; etc.)
a. Patient care
b. Medical knowledge
c. Practice-based learning and improvement
d. Interpersonal and communication skills
e. Professionalism
f. Systems-based practice
UCNS Program Accreditation Application Page 17 of 21Neuro-Oncology 2008
3. Required Clinical Components (Program Requirements V, D). Provide the amount of time in months spent in each setting. Also, please indicate whether the curriculum includes at least four months experience in each of the three required areas: neuro-oncologic issues in systemic cancers; neuro-oncologic issues in primary nervous system cancer, ancillary and palliative care issues.
TYPE OF EXPERIENCE TIMING IN PROGRAM
FORMAT (block vs. longitudinal)
TOTAL AMOUNT OF TIME
Outpatient, including both consultation and continuity clinics
Inpatient (ward-service) experiences Inpatient consultation Emergency room experiences neuro-oncology consultation in patients with systemic cancer
Care of patients with primary nervous system neoplasms
Experience with supportive and ancillary care
4. Document how fellows are provided with direct experience in progressive responsibility for patient management.
5. Core Content
Document how the program will teach the following areas of study.
a. Adult Primary Nervous System Tumors
b. Pediatric Nervous System Tumors
c. Treatment of Metastatic Cancer to the Nervous System
d. Systemic Cancer-Related Neurological Disorders
e. Interdisciplinary Management of neuro-oncology Patients
D. Educational Policies (Program Requirements V, F)
1. Describe the Program Director’s supervision of fellows in each clinical setting.
2. Describe how compliance with ACGME duty hours is maintained (www.acgme.org). Please submit a copy of the policy on duty hours and a call schedule.
UCNS Program Accreditation Application Page 18 of 21Neuro-Oncology 2008
SECTION 7. RESEARCH AND SCHOLARLY ACTIVITY
A. Fellow Meeting AttendanceComment on how many and how often fellows attend local, regional, and national neuro-oncology meetings. You should provide a list of meetings that fellows have attended over the past three years, showing the fellows by name, as Appendix E.
B. List of Research Projects by FellowsList the research projects by fellows from the section/division during the past 3 years as Appendix F.
C. List of Publications by FellowsList the publications by fellows from the section/division during the past 3 years as Appendix G(not manuscripts submitted or in preparation)
D. Scholarly Activity Summary
Academic Year Ending June 30, June 30, June 30 Number of Nationally Peer-Reviewed Published Articles Authored or Co-Authored by Fellows in the Past Year
Number of Fellow Presentations at Regional or National Meetings in the Past Year
SECTION 8. EVALUATION (Program Requirements VI, A)
A. Fellow Evaluation
1. Describe the methods & frequency for fellow evaluation used in the program.
2. Fellow Feedback and RecordsDescribe how and by whom feedback to fellows is provided and what remedial actions are taken in cases of deficiency. What kind of records of fellow evaluations does the program maintain?
3. Final EvaluationPlease provide a copy of a final evaluation used for fellows who complete the program.
4. Impaired FellowsWhat policies are in place for dealing with impaired fellows?
5. Fellow StressHow does the program monitor fellow stress, provide counseling and support services to fellows?
B. Faculty Evaluation (Program Requirements VI, B)Describe the system by which the faculty is evaluated. Are written evaluations by fellows used in this process? If not, please explain. YES NO
UCNS Program Accreditation Application Page 19 of 21Neuro-Oncology 2008

C. Program Evaluation (Program Requirements VI, C)Describe the system by which the program is evaluated.
D. Curriculum Development
1. Describe how written evaluations by fellows are used in the curriculum development process.
2. Describe the participation by fellows in the curriculum development and evaluation process.
3. Describe who participated in the development of written goals and objectives for the required experiences and state the time of most recent revision.
E. Curriculum Evaluation
1. Describe the criteria used in assessing the extent to which goals and objectives (Appendix C) are met.
2. Explain how often the goals and objectives are reviewed and how they are evaluated.
3. Describe how the performance by graduates on the certifying examinations is used to evaluate the effectiveness of the program and to modify the goals and objectives.
UCNS Program Accreditation Application Page 20 of 21Neuro-Oncology 2008

SECTION 9. SIGNATURES
If this form was completed by the Program Coordinator, please provide the following information:
Program Coordinator Name:
Telephone Number: E-mail:
The signatures below attest to the completeness and accuracy of the information provided. Please insert an electronic signature, or sign and fax this page to the UCNS Executive Office at 651-361-4916.Insertion of an electronic signature:
By typing your name in the space provided, you are submitting the electronic equivalent of a legal signature. You are also asserting that you completed the application. To verify the contents of the application, the signatory must enter his/her name in the space provided. Acceptable “signatures” should be preceded and followed by the forward slash (/) symbol. Acceptable “signature” should be as follows: /John Doe/.
Neuro-Oncology Program Director
Name:
Signature: Date:
Department Chair
Name:
Signature: Date:
Please use the Appendices A-G template for submitting Appendices A-G.
UCNS Program Accreditation Application Page 21 of 21Neuro-Oncology 2008





























