-
NEURO ONCOLOGY AND METABOLIC COMPLICATIONDr.Teguh A.S Ranakusuma
SpS(K)*; Dr.Tiara A Wicaksono SpS**Guru Besar Tetap Neurologi FKUI
& Kepala Divisi Neuro-onkologi*Staf Pengajar Neuro-Onkologi
Neurologi**Divisi Neuro-OncologiDepartemen Neurologi
FKUI-RSCMJakarta Neuro-onkologi di Rumah Sakit PGI Cikini Jakarta
2008
-
Global Concept on Health1980 1990Decade of the Gastrointestinal
(Enteric Brain)???1990 2000Decade of the Brain2000 2010 Bone &
Joint Decade2010 2020Decade of the Proteomic ????
-
HUMAN EVOLUTION: SOCIO-HEALTH-PHARMACO ECONOMICNATIONAL HEALTH
SYSTEMEarly detection for Oncologic Prone Person with/ without
Clinical EventsEarly diagnostic is the bestGood QoL
-
Neuro-oncologyRecently in Indonesia :An increased incidence of
primary & secondary brain tumor.General symptoms are due to
mass effect (increased intracranial pressure).Destruction of
adjacent brain tissue.The focal symptoms depends on the location
tumor.
Diagnosis procedure are better (Radiology, Neuroimaging,
CT-Scan, MRI, MRA, EEG)MRI nobel prize 2003
-
Neuro-oncologyA lesion in the brain should not be assumed to be
a metastases just because a patient had a previous cancer; such
assumption could result in overlooking appropriate treatment of
curable tumorPrimary brain tumors rarely spread to other areas of
the body, but they can spread to other parts of the brain and to
the spinal axisThe suggested guideline for work-up, management, and
follow-up in order how to solve neuro-oncologic problems in
Indonesia are showed in following tables with consideration of the
special socio-economic, health system and cultural of
Indonesia.
-
Brain TumorPrimarySecondary
-
Neuro-oncologyPRIMARY BRAIN TUMOR (BT I)Prognosis of patient
with primary brain tumor are determinated by : Histological
typeGradePost-operative sizeExtend of the tumorPatient
agePerformance status of patientDuration of symptoms
-
Neuro-oncologySECONDARY BRAIN TUMOR (BT II)Secondary brain tumor
> primary brain tumorMetastases to brain :Lung cancer, breast
cancer, melanoma and kidneySecondary brain tumor :Usually multiple,
solitary metastases may also occur Brain involvement can occur with
cancer on the nasopharyngeal region by direct extension along the
cranial nerves or through the foramina at the base of
skull.Metastases meningeal involvement can also occur especially
with leukemia, lymphoma, small cell lung cancer, breast cancer and
primary CNS tumors such as medulloblastoma & ependymal
gliomas.
-
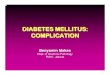
New Case of Brain Tumor
GP; Neurologist; Non Neurologist
- Ro, CT Scan, MRI, MRA, MRS, PET- SPECT Laboratory ECG,
Doppler, Evoked Potensial
Positive Brain Tumor: VP Shunt BiopsyStereo
tacticOpenResectionResidual tumor
Primary Brain Tumor IICP PA Total Removal To Reduce Tumor
Size
Secondary Brain Tumor IICP Soliter
Histologic Finding (PA)
Radiosurgery
Radiotherapy
Chemotherapy
Out come
Quality of life & life expectancy
3 cm
Definitive Radio Tx
3 Modalities Treatment
?
Palliative
Depend on Primary Cancer
Clinical-Neurologic Examination
Medical anticipation
Non Brain Tumor
Stop ???
No Budget
Neuro Emergency
-
Effects of brain tumorDirect:Suppression of neural
tissueSuppression of vascular tissue
Indirect:
ICP Immunity changesHematologic abnormalityHormonal
imbalanceElectrolyte imbalanceNeurologic deficits
Seizure
Systemic changesBrain edema
-
Monro-Kellie-Burrow doctrinePhysiologic state with normal
intracranial pressure (ICP)Major intracranial components:Brain
(80%)Arterial & venous blood (10%)CSF (10%)Cranium: a rigid
container, intracranial volume: constantIntracranial volume: are
shown with ICP (N 10 - 15 mmHg) ICP = Pressure sagital venous +
CSF
-
Physiologic state w/ normal ICPModerate Intracranial mass w/
compensation (normal ICP) intracranial content (egress of venous
blood into the jugular veins & egress of CSF through the for.
magnum spinal canal)Large Intracranial mass w/ decompensation
(ICP), beyond the pressure-buffering capacity of venous blood &
CSF
-
Pressure-volume curveInitial phase: no ICP (compensatory venous
blood & CSF)The compliance is high (elastance low)Further
expansion: compliance is low (elastance high)Terminal stage:
Compensatory: exhaustedSteep rise in pressure (no compliance,
highest elastance)
-
Seizures 30 -90% of intracranial tumor ptsHigh incidence:Low
gradeLocation: supratentorial, cortical, frontal lobeAge: 45 - 64
y.o.Originate not from the mass itself, but from the brain adjacent
to the tumor nidus
-
Effects of seizuresHypoxia & hypercapniaRespiratory acidoses
HypoglycemiaHypocalcemiaMetabolic changesVascular
changesNeurotransmitter alteration: GABA &
somatostatinDeafferentiation & trans synaptic degenerationLocal
neuronal injuryElectrolyte imbalanceSeizures
- Immunity changesDiminished immune responseStructure of
BBBinactivate lymphocytesuppression of Ag-presenting cellsMost of
the CNS is immunologically privilaged.Lymphocytic
infiltration:
-
Hematologic AbnormalityCancer: thrombosis, bleeding,
susceptibility to infectionThromboembolic complication:Risk of any
intracranial procedure: length of operative procedure or duration
of pt immobilityType: DVTs in 72% of meningioma, 60% of
gliblastoma, 20% of brain metastasesSolid tumor: thromboembolism,
metastatic: DIC Location: pt w/ suprasellar tumor suffer PE 5x than
tumor situated elsewhereGrading: platelet adhesiveness more
prominent among malignant tumors than benign ones
-
Hematologic AbnormalityHematologic abNs: >90% of oncologic
ptsPolycythemiaCytopeniaCoagulopathyThrombosisDIC (spec. brain
metastases)Autopsy from brain tumor pts:Pulmonary embolism (PE)
3%DVT 27,5%
-
Tumor cellsMultiple procoagulant substances:tissue factorCancer
procoagulantFactor V receptorMajor protein on the surface that
regulate the fibrinolytic pathway:tissue-type plasminogen
activatorplasminogen activator inh 1 & 2Released
proinflammatory cytokines that impair normal anticoagulant activity
of vasc endothel: TNF & IL-1Attached to vessel walls localised
clotting activation & thrombus formationActivate platelets by:-
Platelet adhesion to tumor cell surfaceMalignant cell relaseof
proaggregatory molActivate the monocyte macrophage syst, &
induce their expression of tissue factor-coagulation factors: V,
VIII, IX, & XI-markers of coagulation activation: D-dimer, FDP,
thrombin-antithrombin complex
-
Nutritional changesNormal physiological conditions: Brain energy
from aerobic oxidation of glucoseA gradually circulating glucose
ketone utilization for energy >>Cancer cells: Unable to
transition from glucose ketone Energy from glucose &
lactate
-
Hormonal ChangesEspecially: sellar region tumors, pituitary
adenoma hypo/hyper: cortisol, GH, prolactin, TSH, FSH, LHSteroid
hormone receptors: meningiomas & astrocytomasMeningiomas:
progesterone receptorsgrowths: menstrual cycle & pregnancy
-
Electrolyte changesHyper/hyponatremia Hyper/hypocalcemia
Hyper/hypophosphatemia Hyper/hypokalemia Hyper/hypouricemia
Hyper/hypoglicemiaADHDrugs: carbamazepineHyperosmolar state
(mannitol th/)SIADH secondary to intracranial hypertension,
hypoxia, stress, pain, morphine, BarbiturateshyponatremiaSecondary
to diabetes insipidus or iatrogenic
causeshypernatremiacorticosteroidsBrain edema
-
Neuro-oncologyTreatment :Some brain tumor are curable by surgery
alone, and some are curable by surgery & radiation therapyThe
reminder require surgery, radiation therapy and chemotherapy.Tumor
that requires all modalities are infrequently curable.
-
Neuro-oncologyClinical Symptom & Sign of Brain
TumorHeadacheSeizureHemiparise etc
Neurological Examination :GeneralNeurologyNeuro-optamology
Radiology & Neuro-imagingSkull X-RayBasisSelatursicaCT-Scan
axial & coronerMRI, MRA, DWINuclear MachineLaboratoriesBlood
analysisLever FunctionKidney FunctionCoagulation systemetcNew Cases
Brain Tumor
-
Neuro-oncology & Systemic ComplicationDirect complications
of neuro oncology
Indirect complications of neuro oncology
Neurologic complications of chemotherapy and Biologic
Therapies.
Neurlogic complications of Radiotion Therapy
-
Direct effects of cancerSide effects of
chemotherapySurgeryRadiationInfectionCoagulopathiesCachexia
-
Neurologic ComplicationsThe most complicated of the Indirect
Neuro- Complication of Cancer in
neuro-oncology.................
-
Neurologic complications Two pathological processes: 1.
Paraneoplastic syndrome: a response paraneoplastic antineureal
autoantibodies
2. As the complications of cancer therapy: caused by
neurotoxicities prosses of radiation and chemotherapy or
combination L Bataller, J Dalmau.,2003.; W.T Cornblath, 2004
-
Paraneoplastic syndrome(PNS) Can affect virtually any part of
the nervous system : from muscle, neuromuscular junction,
peripheral nerve, dorsal root ganglion, spinal cord, brainstem,
brain cortex to the optic nerve and retina
-
PathogenesisOnconeuronal immunity Antibodies ( onconeuronal
antibodies) against the cancer-expressed neuronal- proteins
(onconeuronal antigen).
Other immunologic mechanisms Abnormal production of
immunoglobulin /immunoglobulin fragments by neoplastic cells.
-
Diagnosis of PNSUsually established by : Clinical phenomena:
specific-clinical neurologic history presence of accompanying
symptoms. Clinical electro-physiologic phenomena: peripheral
neurpathies ( motoric, sensoric and autonomic) Neuro-imaging
Phenomena :Ctscan, MRI, PET, SPECT etc Cerebrospinal Fluid
studies
-
PNS of the brain & cerebellumInitial symptoms , Focal to
multifocal or multifocal from the onset. Cortical encephalitis :
epilepsia partialis continua Limbic encephalitis : short-term
memory problems, confuseion, irritability, depression & seizure
Brainstem encephalitis : cranioneuropathies, dysarthria, dysphagia,
autonomic centers disorder, oculor movement disorder : nystagmus,
supranuclear/nuclear pareses
-
PNS of the brain.. cont Cerebellitis resulting in cerebellar
ataxia and do not associate with encephalomyelitis in several cases
of paraneoplastic cerebellar degeneration(PNCD). Myelitis causing
motor weakness as a result of upper/lower motor neuron dysfunction,
segmental rigidity, myoclonus & muscle spasms.
-
PNS of the brain..cont Paraneoplastic cerebellar degeneration :
Initial symptoms dizziness, nausea & vomiting, patients develop
gait and limb ataxia, blurry vision, or diplopia, dysarthria, and
dysphagia. Paraneoplastic opsoclonus-myoclonus syndrome: ocular
motility characterized by involuntary chaotic saccades that occur
in all direction of gaze and frequently assoiciates with myoclonus
& ataxia. ( Lung&Breast Ca in adult; neuroblastoma in
children) (L.Battaller, J.Dalmau., 2003)
-
PNS of the spinal cord The most common PNS of the spinal cord :
Stiff-man syndrome; myelitis and ence- phalomyelitis; subacute
motor neuropathies ( Hodgkins lymphoma ); acute/subacute
necrotizing myelopathy ( viral infection ); progressive multifocal
leukoencephalopathy (papavavirus infection); primary lateral
sclerosis-like syndrome (breast cancer ).
-
PNS of the dorsal root ganglia & nerveParaneoplastic sensory
neuronopathy : associated with symmetric or asymmetric deficits of
all modalities of sensation, painful dysesthesias, radicular pain
and decreased or absent reflexes,due to process of inflamatory
infiltrates, neuronal degeneration, proliferation of satellite
cells, and secondary Wallerian degeneration of the spinal cord
& often associated with paraneoplastic encephalomyelitis.
-
PNS of the dorsal..cont Paraneoplastic peripheral neuropathies 5
groups :subacute axonal/demyelinating peripheral
neuropathies.Vasculitis of the nerve and musclePeripheral
neuropathies associated with monoclonal gammopathies(multiple
myeloma, osteosclerotic myeloma, POEMS syndrome/ polyneuropathy,
organomegaly, endocrinopathy, M component and skin changes,
Waldenstrms macroglobulinemia and Castlemans
disease/angiofollicular lymph node hyperplasia).Gullian-Barre and
plexitis.Neuromyotonia ( Isaacs syndrome )
-
PNS of the neuromuscular junctionLambert-Eaton myasthenic
syndrome(LEMS) : proximal muscle weakness in lower& upper
extremities (fatique, leg weakness, muscle ache & vague
parasthesias), autonomic dysfunction ( dry mouth, erectile
dysfunction, constipation, altered sweating & orthostatic
hypotension), mild cranio-neuropathies ( transient ptosis and
diplopia). LEMS is associated with Ca 50% to 70%(SCLC, LM and other
Ca)
-
PNS of the neuromuscular..contMyathenia gravis (MG) : fatigue,
diplopia, ptosis, dysarthria, neuromuscular respiratory failure and
weakness of the extremities.
Paraneoplastic clinical manifestation of thymoma or thymic
hyperplasia, total thymectomi can develop MG up 6 years after
surgery, breast Ca is the most common cause of extrathymic
malignancies.
-
PNS of the muscle The muscle : Polymyositis/dermatomyositis
Acute necrotizing myopathy Cachectic myopathy Carcinoid myopathy
Myotonia
-
PNS of the muscle..cont...Polymyositis & dermatomyositis are
different immune-mediated inflammatory disorders of the muscle,
with similar neurologic symptoms : myalgias, muscle tenderness
& proximal muscle weakness frequently accompanied by dyphagia
and involvement of neck flexor-extensor muscles, respiratory
muscles failure. Inflammatory infiltrates predominantly of
CD8+T-cells are main cause of muscle injury & fiber necrosis in
polymyositis.
-
PNS of the muscle..contDermatomyositis is associated with skin
changes characterized by purplish discoloration of the eyelids(
heliotrope rash) with edema and erythematous, scaly lesions over
the knuckles. Associated with an immune-mediated intramuscular
angiopathy thought to be antibody-mediated, which leads muscle
ischemic, necrosis and charateristic perifascicular atrophy ( CD4+T
cells, B-cells and macrophages/inflam.infil.; and C3, C9 &
membrane attack complex/ImmunoGl&compl.)
-
PNS of the muscle..cont.. Acute necrotizing myopathy: this
syndrome develop subacute myalgias & rapidly progressive
weakness of the extremities, with frequent involvement of
pharyngeal & respiratory muscles. Ca most frequently involved
are SCLC, Ca of GIT, Breast, kidney & prostate, deposits of
C5-C9 in intramuscular vessels & muscle fibers. DD/
rhabdomyolysis induced by CTh & cytokines (IL-2, interferon-
).
-
Treatment There is extensive evidence that many PNS are mediated
by immunologic responses against onco-neuronal antigens. A
practical implication is that these immunologic disorders
frequently are associated with antibodies that are excellent
diagnostic markers of PNS & Ca, and the second implication is
that prompt detection & treatment of the tumor is the most
efficacious therapeutic approach, at times leading to stabilization
of the PNS. S. Shamsili, P.S Smitt, 2005
-
Treatment and PrognosisPNCD : tumor excision, plasma-exchange,
steroids, IVIg or cyclophosphamide, the outcome is generally poor
& no recommended treatment exists.Limbic encephalitis : treat
the DIC, antitumor th/, spontaneous complete recopvery has been
described.Encephalomyelitis : tumor treatment offers the best
chance of stabilizing the patients neurologic status. S Shamsili,
P.S Smitt 2005
-
Treatment & prog..contParaneoplastic
Opsoclonus-Myoclonus(POM) may remit either spontaneously, following
treatment of the tumor, or in associatein with clonazepam or
thiamine treatment.Stiff-man syndrome, response to treatment with
baclofen, diazepam, valproate, vigabatrin, and carbamazepin,
steroid, PE and IVIg.
-
Treatment and prog..contPeripheral nervous system : subacute
sensory neuropathy, sensorimotor neuropathy, sensorimotor
neuropathy associated with M-proteins,etc.Neuromuscular Junction
and muscle : LEMs, treatment(tailored) of the tumor + PE,IVIg,
immonosuppressive+ cholinesterase inhibitors MG relies on
cholinesterase inhibitor +immuno- therapy comprises thymectomy,
immuno- suppressive, PE and IVIg.
S.Shamsili, P.S Smitt, 2005
-
C o n c l u s i o n Although PNSNS are not common, their
recognition is important.In Indonesia the medical facilities is
insufficient.However, the diagnosis of a PNSNS can lead to the
diagnosis of an underlying tumor or avoid the continued search for
metastasis in a patient who has known cancer. An appropriate
diagnosis leads to providing appropriate treatment and prognostic
information with unfortunate consequence of high cost.
-
T H A N KY O U Neuro-oncology : HUT 110 Rumah Sakit Universitas
Kristen Indonesia,Jkt 26.01.08