Embed Size (px)
Citation preview

361www.i-mri.org
MRI Finding of Retroperitoneal Desmoplastic Small Round Cell Tumor with Hepatic Metastasis and Portal Vein Thrombosis: a Case Report
INTRODUCTION
Desmoplastic small round cell tumor (DSRCT) is a rare malignant mesenchymal neoplasm that shows an aggressive nature and poor prognosis (1-3). DSRCT commonly affects adolescent and young male (2, 4). Patients with DSRCT show minor symptoms such as abdominal discomfort and vague abdominal pain. Occasionally, they have a physical symptoms with palpable abdominal mass (2). Since DSRCT develops from mesenchymal cells of serosal surface, multiple solid masses without primary organ of origin in abdominopelvic cavity present the common imaging findings of DSRCT. They accompany metastasis at the time of diagnosis (1). This study reports a rare manifestation of DSRCT showing atypical features both clinically and radiologically.
CASE REPORTS
A 70-year-old female patient visited our clinic with symptoms such as weight loss and general weakness. Physical examination yielded no findings. Hematological examination only revealed that alkaline phosphatase (ALP) level was high (at 1023 IU/L, normal range: 44 to 147 IU/L). Others parameters that were normal included bilirubin of 0.71 mg/DL, aspartate aminotransferase (AST) of 45 IU/L, and alanine aminotransferase (ALT) of 37 IU/L. Abdominal computed tomography revealed a large heterogeneous
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: April 12, 2019Revised: June 12, 2019Accepted: July 2, 2019
Correspondence to: Young Hwan Lee, M.D., Ph.D.Department of Radiology, Wonkwang University College of Medicine and Hospital, 895 Muwang-ro, Iksan, Jeonlabuk-do 54538, Korea.Tel. +82-63-859-1920Fax. +82-63-851-4749E-mail: [email protected]
Copyright © 2019 Korean Society of Magnetic Resonance in Medicine (KSMRM)
iMRI 2019;23:361-366 https://doi.org/10.13104/imri.2019.23.4.361
Case ReportDesmoplastic small round cell tumor (DSRCT) is a rare and aggressive malignancy common in young male patient. Typical imaging features of DSRCT include multiple soft tissue masses in the peritoneal cavity, omentum, or mesentery without an organ of origin. This report presents a rare manifestation of DSRCT revealing a solitary large retroperitoneal mass with hepatic metastasis and malignant portal vein thrombosis in 70-year-old women together with the review of literature. The tumor showed a hemorrhagic and necrotic mass with peripheral portion of T2 hypo-intensity and delayed enhancement that indicated desmoplastic stroma with dense cellularity.
Keywords: Desmoplastic small round cell tumor; Retroperitoneum; Metastasis
pISSN 2384-1095eISSN 2384-1109
Youe Ree Kim1, Young Hwan Lee1, Keum-Ha Choi21Department of Radiology, Wonkwang University College of Medicine and Hospital, Iksan, Korea2Department of Pathology, Wonkwang University College of Medicine and Hospital, Iksan, Korea
Magnetic resonance imaging

www.i-mri.org362
MRI Findings of Retroperitoneal DSRCT | Youe Ree Kim, et al.
enhancing mass of about 12 cm in the left abdominal cavity. However, its location and origin were not immediately identified. During the venous phase images of this mass, the peripheral part showed mild enhancement whereas the central portion did not show any enhancement. Additionally, there were multiple variable sized homogeneous enhancing masses in the liver. Both the intrahepatic portal veins and
the main portal vein showed mild enhancement. Moreover, malignant portal vein thrombosis which causes widening of vein was observed (Fig. 1a).
Abdominal MRI (Ingenia CX, 3T, Philips Healthcare, Best, the Netherlands) was performed using gadolinium ethoxybenzyl diethylenetriamine pentaacetic acid (Primovist®, Gd-EOB-DTPA). On MR T2 and T2 fat
a b
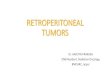
Fig. 1. A 70-year-old woman with retroperitoneal desmoplastic small round cell tumor (DSRCT), liver metastasis, and malignant portal vein thrombosis. (a) Axial CT venous image showing a large solitary retroperitoneal mass demonstrating mild peripheral enhancing portion and central enhancing part. Multiple mild enhancing hepatic masses and malignant portal vein thrombosis at the umbilical section of left portal vein (arrow) were indicated. (b, c) Coronal T2 weighted image and axial T2 fat suppressed image showing mild hyperintense peripheral portion and more hyperintense central part in the retroperitoneal mass. The left adrenal gland was displaced and externally compressed by the mass (arrow). (d) Axial pre-contrast T1 fat suppressed gradient echo image showing ill-defined hyperintensity in central part suggesting hemorrhagic necrosis.
c d

363www.i-mri.org
https://doi.org/10.13104/imri.2019.23.4.361
suppression images, the following was observed: the stomach in the front, the spleen in the back, the pancreas at the lower front, the kidney at the lower back and the left adrenal gland was pushed to the medial side. As a result of these findings, a retroperitoneal origin mass was considered (Fig. 1b, c). The peripheral part of a large retroperitoneal mass displayed intermediate or mild high signal intensity more than the liver while the central part showed bright high signal intensity on T2-weighted images. Multifocal lesions with T1 high signal intensity on pre-contrast T1-weighted image were considered as intra-tumoral hemorrhage (Fig. 1d). The peripheral portion of the mass exhibited delayed enhancement on dynamic enhanced MR and the central portion of the mass showing high signal intensity on T2 weighted image showed no enhancement, necrosis was considered (Fig. 1e-g). The peripheral part that
showed enhancement also exhibited diffusion restriction (Fig. 1h, i). Metastatic masses in the liver also revealed mild delayed enhancement. Additionally, malignant portal vein thrombosis exhibited mild delayed enhancement. Metastatic lymphadenopathy was not detected. Peritoneal or mesenteric masses (except a large retroperitoneal mass) were not observed. Based on these imaging findings and tumor position (suspected retroperitoneal space), the differential diagnoses included gastric or retroperitoneal origin gastrointestinal stromal tumor, adrenal cortical adenocarcinoma, retroperitoneal neuroendocrine tumor, and retroperitoneal sarcoma.
Ultrasonographic imaging revealed a large mass with heterogeneous echogenicity. The liver mass was observed to be hypoechoic. Percutaneous biopsy was performed on both the primary mass and liver mass including the peripheral
e f
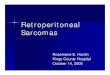
Fig. 1. (e-g) Dynamic enhanced T1 fat suppressed images showing arterial nodular enhancement and delayed enhancement of peripheral part. Liver masses and portal vein thrombosis presented mild delayed enhancement.
g

www.i-mri.org364
MRI Findings of Retroperitoneal DSRCT | Youe Ree Kim, et al.
and central part of the primary mass. Hematoxylin and Eosin (H&E) staining images revealed a small clustered round cell enclosed by desmoplastic stroma. The immunochemical staining test results showed positive responses on Vimentin, pan-CK, EMA, and NSE, and weakly positive responses to C-kit and TTF-1, and negative responses to LCA, CD099, bcl-2, desmin, SMA, CD34, S-100 protein, and CD 68. In conclusion, a desmoplastic small round cell tumor was diagnosed (Fig. 1j, k). The patient snubbed chemotherapy and chose to be discharged.
DISCUSSION
DSRCT was discovered recently. In 1989, two cases were reported. It was classified and analyzed as a pathologic entity in 1991 (5, 6). DSRCT is a series of blue round cell tumors including: neuroblastoma, malignant lymphoma, rhabdomyosarcoma, Ewing sarcoma, Wilms tumor, primitive neuroectodermal tumor, and anaplastic synovial sarcoma. DSRCT is reportedly common in young white males (1). However, new cases have recently been reported in East Asia (2). In this case, a 70-year-old female patient was diagnosed with DSRCT and its metastasis based on the biopsy results
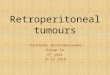
Fig. 1. (h, i) Diffusion weighted images (b factor = 800) showing diffusion restriction at peripheral solid part, high and low ADC at central part that resulted from hemorrhagic necrosis. (j, k) Photomicrograph (× 40, Hematoxylin and Eosin) showing desmoplastic stroma and dense speckled cells made up of small round cell and immunohistochemistry (× 400) showing positive results of WT-1, Vimentin, pan-CK, and NSE.
j k
h i

365www.i-mri.org
https://doi.org/10.13104/imri.2019.23.4.361
of both the retroperitoneal and liver mass. Diagnosis was challenging due to inconsistencies with previously identified clinical characteristics. According to the distinctive pathologic findings, it was possible to diagnose it with DSRCT. DSRCT is pathologically observed to reveal abundant desmoplastic stroma and poorly differentiated small round cells as observed in this case. In immunohistochemistry, it is characterized by the presentation of epithelial, neural, myogenic, and mesenchymal markers.
DSRCT, a sarcoma originating from the mesenchymal cell on the serosal surface, is identified at the time of diagnosis as multiple or bulky masses and metastases in the abdominopelvic cavity. It is difficult to locate the primary organ at the time of diagnosis (1, 2, 7). This is because diagnosis could be delayed as a result of ambiguous clinical symptoms of DSRCT or due to the aggressive nature of the tumor itself. Based on previous studies, the 3-year survival rate of DSRCT was 30% and the 5-year survival was 15% (1). In this case, a large mass and multiple liver metastases were detected. Since the patient declined treatment, she died within one year.
The number of DSRCT cases is small. There have been less than 300 cases of radiological reports, most of which are done using CT (2, 4). CT is helpful for initial staging and follow up of DSRCT. DSRCT presents itself as a form of multiple heterogeneous enhancing masses in the abdominopelvic cavity (1, 7). Therefore, the differential diagnosis of DSRCT includes: rhabdomyosarcoma, peritoneal sarcomatosis, lymphoma, mesothelioma, etc. (4). Report of a single large retroperitoneal mass on CT image like in this case is very rare (8). In such cases, large retroperitoneal mass and liver metastasis might be diagnosed as retroperitoneal GIST, retroperitoneal neuroendocrine tumor, retroperitoneal sarcoma, adrenal malignancy, etc. Additionally, there was an area on CT that did not show enhancement. This area is as a result of necrosis and hemorrhage as well as high fibrotic content (1).
Few studies have reported on MR features of DSRCT, including one case of mixed iso- and hyperintensity and the other, a case of mixed hypo-/iso-/hyperintensity on MR T2. Another study reported an area with low signal intensity on T2- weighted images (7, 9). The area of low T2 signal was observed because of densely packed cells and desmoplastic response. In each biopsy of this case, necrosis was observed in the central T2 hyperintense area, while dense desmoplastic stroma and cells were observed in peripheral T2 mild hyperintense area, which are in line with the findings of previous studies.
In previous reports of DSRCT cases, there was no mention of dynamic enhancement, and only mild heterogeneous enhancements were observed (7, 9). Compared to previous studies which only reported on small masses, this case presented a large mass, which made it easier to analyze the enhancement patterns. In this case, delayed enhancement was observed in the peripheral part of the mass which showed mild hyperintensity area in T2. This was considered as a delayed enhancement of the desmoplastic stroma. Based on the biopsy specimen from the peripheral portion of the retroperitoneal mass, we assume that dense stroma in DSRCT could be mild delayed contrast enhancement. Although previous studies failed to report on the relationship between dense stroma and enhancement pattern in DSRCT, delayed enhancement might be revealed in other stromal tumors with dense stroma. As the central portion of the mass showed T2 hyperintensity coupled with T1 hyperintensity area, necrosis and hemorrhage were observed in this case, as in the previous studies.
This case presented liver metastasis, the most common visceral metastasis. Other types of metastases included lung, bone, spleen, and pleura (1, 10). The involvement of ascites and lymphadenopathy has been reported (4). However, no previous cases have revealed malignant portal vein thrombosis as observed in this case. It showed mild delayed enhancement in MR dynamic in addition to the primary mass.
According to literature review, it appears that DSRCT usually occurs in young men and presents itself as multiple peritoneal masses, the most common being liver metastasis which has poor prognosis. It is a rare case of DSRCT for a 70-year-old woman who had a large solitary retroperitoneal mass with liver metastasis and malignant portal vein thrombosis. Necrosis and hemorrhage may be observed based on MR T1- and T2-weighted images. Particularly, delayed enhancement of T2 mild hyperintense area indicating desmoplastic stroma, which might be of assistance in differential diagnosis.
REFERENCES
1. Bellah R, Suzuki-Bordalo L, Brecher E, Ginsberg JP, Maris J, Pawel BR. Desmoplastic small round cell tumor in the abdomen and pelvis: report of CT findings in 11 affected children and young adults. AJR Am J Roentgenol 2005;184:1910-1914
2. Shen XZ, Zhao JG, Wu JJ, Liu F. Clinical and computed

www.i-mri.org366
MRI Findings of Retroperitoneal DSRCT | Youe Ree Kim, et al.
tomography features of adult abdominopelvic desmo-plastic small round cell tumor. World J Gastroenterol 2014;20:5157-5164
3. Chouli M, Viala J, Dromain C, Fizazi K, Duvillard P, Vanel D. Intra-abdominal desmoplastic small round cell tumors: CT findings and clinicopathological correlations in 13 cases. Eur J Radiol 2005;54:438-442
4. Morani AC, Bathala TK, Surabhi VR, et al. Desmoplastic small round cell tumor: imaging pattern of disease at presentation. AJR Am J Roentgenol 2019;212:W45-W54
5. Gerald WL, Rosai J. Case 2. Desmoplastic small cell tumor with divergent differentiation. Pediatr Pathol 1989;9:177-183
6. Gerald WL, Miller HK, Battifora H, Miettinen M, Silva EG, Rosai J. Intra-abdominal desmoplastic small round-cell tumor. Report of 19 cases of a distinctive type of
high-grade polyphenotypic malignancy affecting young individuals. Am J Surg Pathol 1991;15:499-513
7. Zhang WD, Li CX, Liu QY, Hu YY, Cao Y, Huang JH. CT, MRI, and FDG-PET/CT imaging findings of abdominopelvic desmoplastic small round cell tumors: correlation with histopathologic findings. Eur J Radiol 2011;80:269-273
8. Shen CJ, Loeb DM, Terezakis SA. Desmoplastic small round cell tumor: postoperative retroperitoneal mass. Radiol Case Rep 2016;11:248-250
9. Gorospe L, Gomez T, Gonzalez LM, Lopez A. Desmoplastic small round cell tumor of the pelvis: MRI findings with histopathologic correlation. Eur Radiol 2007;17:287-288
10. Kis B, O'Regan KN, Agoston A, Javery O, Jagannathan J, Ramaiya NH. Imaging of desmoplastic small round cell tumour in adults. Br J Radiol 2012;85:187-192