Embed Size (px)
Citation preview

J Clin Pathol 1992;45:295-298
Desmoplastic malignant mesothelioma: a reviewof 17 cases
G E Wilson, P S Hasleton, A K Chatterjee
AbstractAims: To identify the histological
features of desmoplastic mesothelioma,and to determine its incidence and prog-nosis.Methods: Two hundred and fifty five
cases of malignant mesothelioma wereexamined over seven years (1982-9) toidentify the desmoplastic variant. Sec-tions were cut at 5 um and stained withhaemotoxylin and eosin and withCAM 5 2(Dakopatts). Asbestos fibre counts werecarried out by light microscopy in 14cases using the potash digestion method.Results: Seventeen cases were iden-
tified as desmoplastic mesothelioma giv-ing an incidence of 6-6%. In 11 cases thecell type in more cellular areas wassarcomatous and in six others it wasbiphasic. The mean survival time fromonset of symptoms to death was 5-8months for the sarcomatous variant and6-8 months for the biphasic variant.Twelve of 16 patients had had previousoccupational exposure to asbestos, rang-ing from five months to 43 years. Thediagnosis of desmoplastic mesotheliomawas only accepted if acellular connectivetissue comprised 50% or more of thetumour bulk. Also seen was collagennecrosis, anastomosing bands of oftenhyalinised collagen with a prominentstoriform pattern, and where cellulardetail was present there were hyper-chromatic nuclei.Conclusions: Desmoplastic meso-
thelioma is a rare variant of malignantmesothelioma with a storiform collagenpattern, collagen necrosis, blandacellular collagen and focal cytologicalfeatures ofmalignancy. Though rare, it isimportant to recognise this variant anddistinguish it from a pleural plaque, non-specific reactive pleural fibrosis, pleurisy,rheumatoid disease, or, rarely, spindlecell sarcomas.
Although rare, malignant mesotheliomas haveassumed great importance during the past twodecades because of their increased incidence,especially among persons with previousexposure to asbestos.'2 Up to 90% of meso-theliomas are associated with asbestos withinoccupationally exposed groups" and becauseof the long latency period ofbetween 25 and 45years for the effects of exposure to asbestos todevelop into mesothelioma, it is expected thatthe number of cases will continue to increaseuntil 2000 and beyond.' 2 4
There is a subgroup of malignant meso-thelioma, termed desmoplastic malignantmesothelioma (DMM), in which 50% or moreof the tumour is fibrous and has a low cellcontent.67 The hypocellular, bland appearan-ces of such desmoplastic areas can be extremelydifficult to interpretate and the correct diag-nosis ofmalignancy may not be suspected. Thisis particularly the case when needle biopsy isperformed, and many cases of DMM are stillonly diagnosed at necropsy.
MethodsTwo hundred and fifty five cases of malignantmesothelioma were seen at or referred to theregional cardiothoracic centre between 1982and 1989.
Seventeen (6-6%) of these cases were con-sidered to be DMM-that is, more than 50%of the tumour was composed of dense hypo-cellular fibrous tissue. In seven patients thediagnosis was made during life by thoracotomyand biopsy. Post mortem examinations werecarried out in 16 of the 17 cases. Clinical andoccupational histories were taken from hospitalrecords or from the Medical Boarding Panel(Respiratory Diseases) notes. Relevant blocksof tissue were fixed in formalin and embeddedin paraffin wax. Sections (5 gm) were stainedwith haematoxylin and eosin for light micro-scopical examination. An average of sevenblocks of tumour per case were available forstudy (range two to 19). Immunohistochemicalstaining was done on formalin fixed tissue usingthe standard peroxidase method8 followed byapplication of the low molecular weight cyto-keratin antibody CAM 5-2 (Dakopatts).Counts of asbestos fibres were carried out bylight microscopy in 14 cases using the potashdigestion method.9The ages of 16 ofthe 17 patients were known
and ranged from 41-79 years (mean 60-1 years)at the time of diagnosis. Fifteen patients weremale and two female. In 11 the presentingcomplaints included pleural effusion in five,shortness of breath in three, and anaemia,pleuritic chest pain, and weight loss, respec-tively in three. The length of survival fromonset of symptoms was known in 12 cases, themean survival being 5-8 months in eightpatients with sarcomatous tumours and 6-8months in four patients with mixed tumours.Twelve of 16 patients had had previous
occupational exposure to asbestos. The dura-tion of exposure ranged from five months to 43years where it was known. Specific treatmentwas given in five cases and included pleuraldecortication in three, radiation in one, andchemotherapy in one.
Department ofPathology, RegionalCardiothoracicCentre, WythenshaweHospital, ManchesterM23 9LTG E WilsonP S HasletonMedical BoardingCentre (RespiratoryDiseases), ManchesterA K ChatterjeeCorrespondence to:Dr P S Hasleton.Accepted for publication23 September 1991
295
Wilson, Hasleton, Chatterjee
'f~~~~~~~~.......::
oo;~~~~~~~~~~~~~~~~~~~~~...
g~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.
0X .; S ' }~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.
4
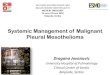
Figure 1 Stonform pattern in a desmoplastic mesothelioma: note lack of nuche(haematoxylin and eosin).
ResultsGROSS PATHOLOGYIn 13 (72-2%) cases tumour was in tpleural cavity. In two cases pleuralwere bilateral, the other case being leThe site of one tumour was unknown.invariably encompassed the pleural ca~extension along the interlobar fissuretrating the underlying lung parench3affecting the mediastinal structures irthe pericardium. Spread to thechest.
I
...
v '';
4\ -:e'f
¾o t &
I
E
*.f 1t
...
.0. ~
.4
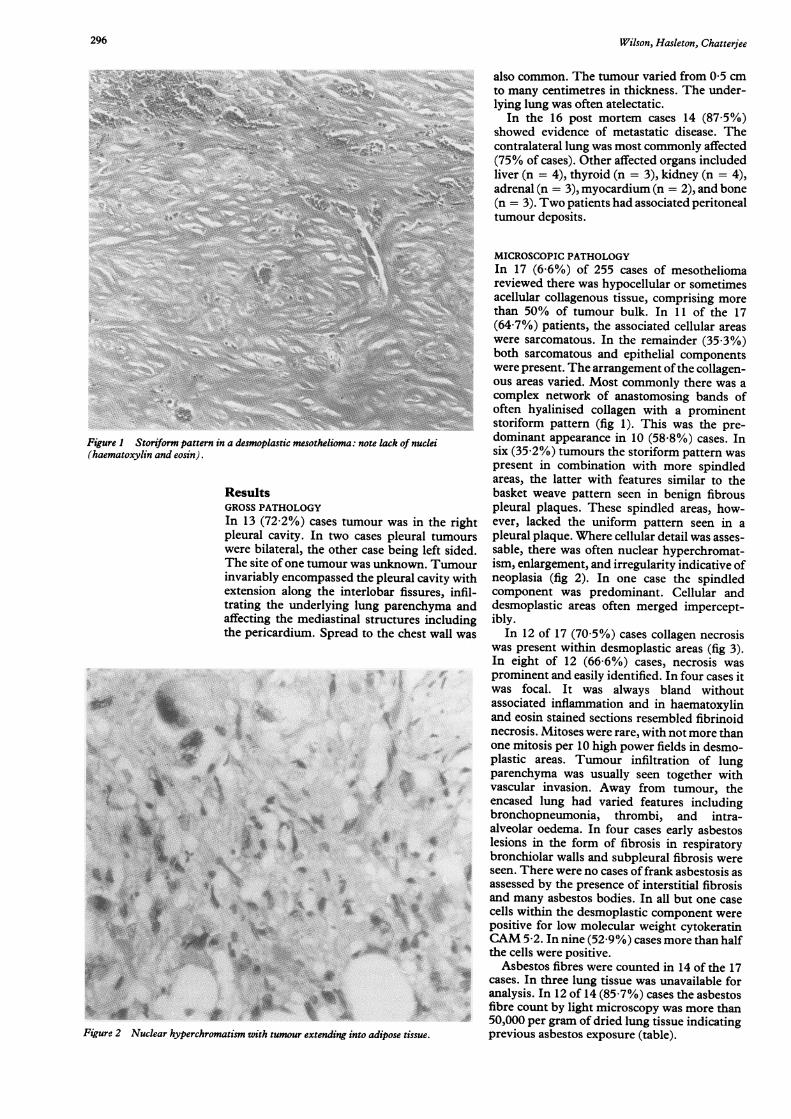
Figure 2 Nuclear hyperchromatism with tumour extending into adipose tissue.
also common. The tumour varied from 05 cmto many centimetres in thickness. The under-lying lung was often atelectatic.
In the 16 post mortem cases 14 (87-5%)showed evidence of metastatic disease. Thecontralateral lung was most commonly affected(75% of cases). Other affected organs includedliver (n = 4), thyroid (n = 3), kidney (n = 4),adrenal (n = 3), myocardium (n = 2), and bone(n = 3). Two patients had associated peritonealtumour deposits.
MICROSCOPIC PATHOLOGYIn 17 (6-6%) of 255 cases of mesotheliomareviewed there was hypocellular or sometimes
° acellular collagenous tissue, comprising morethan 50% of tumour bulk. In 11 of the 17(64-7%) patients, the associated cellular areaswere sarcomatous. In the remainder (35-3%)both sarcomatous and epithelial componentswere present. The arrangement ofthe collagen-ous areas varied. Most commonly there was acomplex network of anastomosing bands ofoften hyalinised collagen with a prominentstoriform pattern (fig 1). This was the pre-
ei dominant appearance in 10 (58-8%) cases. Insix (35-2%) tumours the storiform pattern waspresent in combination with more spindledareas, the latter with features similar to thebasket weave pattern seen in benign fibrouspleural plaques. These spindled areas, how-
the right ever, lacked the uniform pattern seen in atumours pleural plaque. Where cellular detail was asses-ft sided. sable, there was often nuclear hyperchromat-Tumour ism, enlargement, and irregularity indicative ofvity with neoplasia (fig 2). In one case the spindledes, infil- component was predominant. Cellular andyma and desmoplastic areas often merged impercept-ncluding ibly.wall was In 12 of 17 (705%) cases collagen necrosis
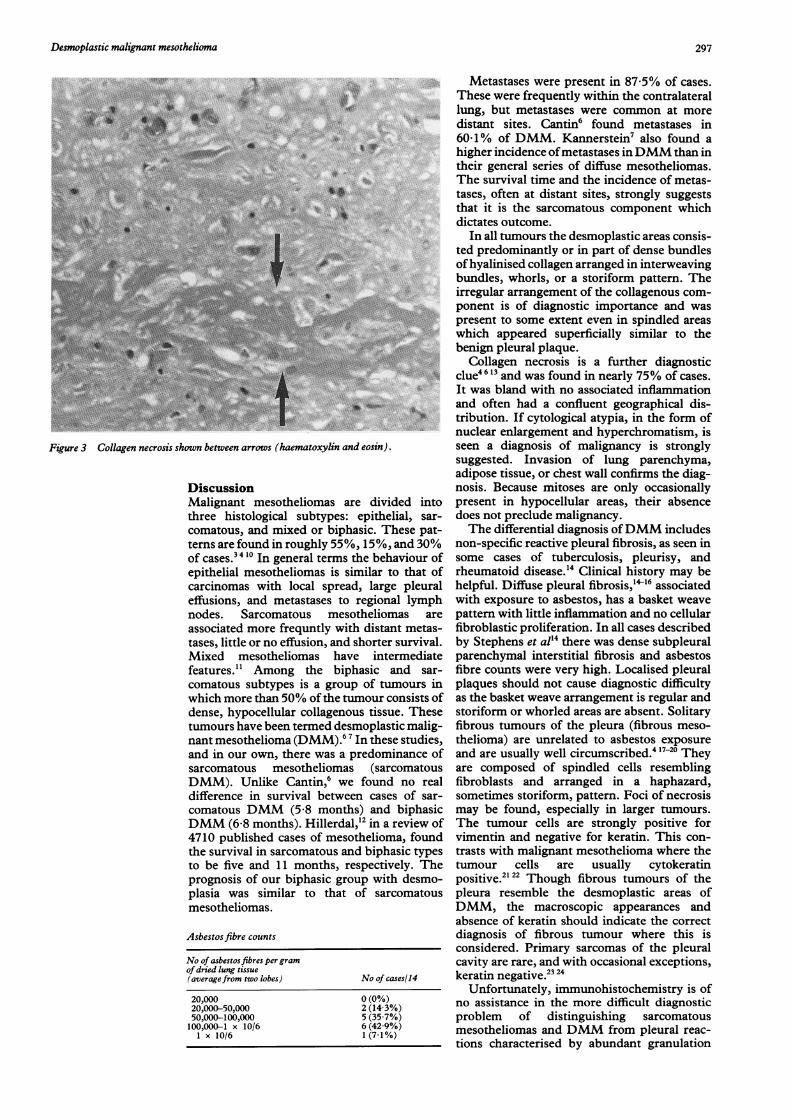
was present within desmoplastic areas (fig 3).In eight of 12 (66-6%) cases, necrosis wasprominent and easily identified. In four cases itwas focal. It was always bland withoutassociated inflammation and in haematoxylinand eosin stained sections resembled fibrinoidnecrosis. Mitoses were rare, with not more thanone mitosis per 10 high power fields in desmo-plastic areas. Tumour infiltration of lungparenchyma was usually seen together withvascular invasion. Away from tumour, theencased lung had varied features includingbronchopneumonia, thrombi, and intra-alveolar oedema. In four cases early asbestoslesions in the form of fibrosis in respiratorybronchiolar walls and subpleural fibrosis wereseen. There were no cases offrank asbestosis asassessed by the presence of interstitial fibrosisand many asbestos bodies. In all but one casecells within the desmoplastic component werepositive for low molecular weight cytokeratinCAM 5-2. In nine (52-9%) cases more than half
* r- the cells were positive.Asbestos fibres were counted in 14 of the 17
cases. In three lung tissue was unavailable foranalysis. In 12 of 14 (85-7%) cases the asbestosfibre count by light microscopy was more than50,000 per gram of dried lung tissue indicatingprevious asbestos exposure (table).
296
..
AN."-S
c..w.... .1 1'.
W-I%%'.%lw.....0 A.:.... 416
IIIF?.
.#-N.
Desmoplastic malignant mesothelioma
I
::~~~~~~~~~~~ ~~~~~~~~~~~~~~~.... ...
...c .c .....
Figure 3 Collagen necrosis shown between arrows (haematoxylin and eosin).
DiscussionMalignant mesotheliomas are divided intothree histological subtypes: epithelial, sar-comatous, and mixed or biphasic. These pat-terns are found in roughly 55%, 15%, and 30%of cases.34 10 In general terms the behaviour ofepithelial mesotheliomas is similar to that ofcarcinomas with local spread, large pleuraleffusions, and metastases to regional lymphnodes. Sarcomatous mesotheliomas areassociated more frequntly with distant metas-tases, little or no effusion, and shorter survival.Mixed mesotheliomas have intermediatefeatures.'" Among the biphasic and sar-comatous subtypes is a group of tumours inwhich more than 50% of the tumour consists ofdense, hypocellular collagenous tissue. Thesetumours have been termed desmoplastic malig-nant mesothelioma (DMM).67 In these studies,and in our own, there was a predominance ofsarcomatous mesotheliomas (sarcomatousDMM). Unlike Cantin,6 we found no realdifference in survival between cases of sar-comatous DMM (5-8 months) and biphasicDMM (6-8 months). Hillerdal,'2 in a review of4710 published cases of mesothelioma, foundthe survival in sarcomatous and biphasic typesto be five and 11 months, respectively. Theprognosis of our biphasic group with desmo-plasia was similar to that of sarcomatousmesotheliomas.
Asbestosfibre counts
No of asbestos fibres per gramof dried lung tissue(averagefrom two lobes) No of cases/14
20,000 0 (0%)20,000-50,000 2 (14-3%)50,000-100,000 5 (35-7%)100,000-1 x 10/6 6 (42-9%)
1 x 10/6 1 (7-1%)
Metastases were present in 87-5% of cases.These were frequently within the contralaterallung, but metastases were common at moredistant sites. Cantin6 found metastases in60 1% of DMM. Kannerstein7 also found ahigher incidence ofmetastases inDMMthan intheir general series of diffuse mesotheliomas.The survival time and the incidence of metas-tases, often at distant sites, strongly suggeststhat it is the sarcomatous component whichdictates outcome.
In all tumours the desmoplastic areas consis-ted predominantly or in part of dense bundlesofhyalinised collagen arranged in interweavingbundles, whorls, or a storiform pattern. Theirregular arrangement of the collagenous com-ponent is of diagnostic importance and waspresent to some extent even in spindled areaswhich appeared superficially similar to thebenign pleural plaque.
Collagen necrosis is a further diagnosticclue46 13 and was found in nearly 75% of cases.It was bland with no associated inflammationand often had a confluent geographical dis-tribution. If cytological atypia, in the form ofnuclear enlargement and hyperchromatism, isseen a diagnosis of malignancy is stronglysuggested. Invasion of lung parenchyma,adipose tissue, or chest wall confirms the diag-nosis. Because mitoses are only occasionallypresent in hypocellular areas, their absencedoes not preclude malignancy.The differential diagnosis ofDMM includes
non-specific reactive pleural fibrosis, as seen insome cases of tuberculosis, pleurisy, and
F rheumatoid disease.'4 Clinical history may behelpful. Diffuse pleural fibrosis,'14-6 associatedwith exposure to asbestos, has a basket weavepattern with little inflammation and no cellularfibroblastic proliferation. In all cases describedby Stephens et al'4 there was dense subpleuralparenchymal interstitial fibrosis and asbestosfibre counts were very high. Localised pleuralplaques should not cause diagnostic difficulty
f as the basket weave arrangement is regular andstoriform or whorled areas are absent. Solitaryfibrous tumours of the pleura (fibrous meso-thelioma) are unrelated to asbestos exposure
f and are usually well circumscribed.4 1720 Theyare composed of spindled cells resemblingfibroblasts and arranged in a haphazard,sometimes storiform, pattern. Foci of necrosismay be found, especially in larger tumours.
F The tumour cells are strongly positive forvimentin and negative for keratin. This con-trasts with malignant mesothelioma where thetumour cells are usually cytokeratinpositive.122 Though fibrous tumours of thepleura resemble the desmoplastic areas ofDMM, the macroscopic appearances andabsence of keratin should indicate the correctdiagnosis of fibrous tumour where this isconsidered. Primary sarcomas of the pleuralcavity are rare, and with occasional exceptions,22keratin negative.
Unfortunately, immunohistochemistry is ofno assistance in the more difficult diagnosticproblem of distinguishing sarcomatousmesotheliomas and DMM from pleural reac-
. tions characterised by abundant granulation
297
.. .....
....
.....

Wilson, Hasleton, Chatterjee
tissue and fibrosis.25 This is because in reactivestates submesothelial spindle cells acquirecytokeratin intermediate filaments, usually oflow molecular weight, while retaining theirconnective tissue markers and so stain for bothcytokeratin and vimentin.132526 The same pat-tern of staining is seen in most sarcomatoidmesotheliomas.
In inflammatory pleural lesions there isusually active granulation tissue formationwith an acute and chronic inflammatory infil-trate and fibrosis. The fibrosis does not have astoriform or basket weave appearance andnuclear hyperchromatism is not a feature.Apart from malignant mesothelioma, other
epithelial and mesenchymal tumours may con-tain desmoplastic areas and, in these, there isgood evidence to indicate that this is theconsequence of stimulation of stromalmyofibroblasts.27 28 Many cells within the des-moplastic areas ofDMM are, however, positivefor cytokeratin, findings which are in accor-dance with those of Cantin.' Malignantmesothelial cells, in certain cases, seem toassume the functional capacity of fibroblastsand at least one study has shown that mesoth-elial cells can produce collagen in tissue cul-ture.29
I Spirtas R, Beebe GW, Connelly RR, et al. Recent trends inmesothelioma incidence in the United States. Am J IndMed 1986;9:397-407.
2 Craighead JE. Current pathogenic concepts ofdiffuse malig-nant mesothelioma. Hum Pathol 1987;18:544-57.
3 Whitwell F, Rawcliffe RM. Diffuse malignant pleuralmesothelioma and asbestos exposure. Thorax 1971;26:6-22.
4 Roggli VL, Kolbeck J, Sanfilippo F, Shelbume JD. Path-ology of human mesothelioma. Aetiologic and diagnosticconsiderations. Pathol Annu 1987;2:91-131.
5 Jones JSP. Asbestos fibres and their biological effects on themesothelium. In: Jones JSP, ed. Pathology of the meso-thelium. London: Sringer-Verlag, 1987:237-43.
6 Cantin R, Al-Jabi M, McCaughey WTE. Desmoplasticdiffuse mesothelioma. Am J Surg Pathol 1982;6:215-22.
7 Kannerstein M, Churg J. Desmoplastic diffuse malignantmesothelioma. In: Fenoglio CM, WolffM, eds. Progress insurgicalpathology. Vol II. New York: Masson Publishing,1980:19-29.
8 Hasleton PS, Kelehan P, Whittaker JS, Burslem RW,Turner L. Benign and malignant struma ovarii. ArchPathol Lab Med 1978;102:180-4.
9 Ashcroft T, Heppleston AG. The optical and electron
microscopic determination of pulmonary asbestos fibreconcentration and its relation to the human pathologicalreaction. J Clin Pathol 1973;26:224-34.
10 Chailleux E, Dabouis G, Pioche D, et al. Prognostic factorsin diffuse malignant pleural mesothelioma. A study of 167patients. Chest 1988;93:159-62.
11 Law MR, Hodson ME, Heard BE. Malignant mesotheliomaof the pleura: relation between histological type andclinical behaviour. Thorax 1982;37:810-5.
12 Hillerdal G. Malignant mesothelioma 1982: Review of 4710published cases. Br J Dis Chest 1983;77:321-43.
13 Bolen JW, Hammar SP, McNuttMA. Reactive and neoplas-tic serosal tissue. A light microscopic, ultrastructural andimmunocytochemical study. Am J Surg Pathol 1986;10:34-47.
14 Stephens M, Gibbs AR, Pooley FD, Wagner JC. Asbestosinduced diffuse pleural fibrosis: pathology and min-eralogy. Thorax 1987;42:583-8.
15 Albelda SM, Epstein DM, Gefter WB, Miller WT. Pleuralthickening: its significance and relationship to asbestosdust exposure. Am Rev Respir Dis 1982;126:621-4.
16 McLoud TC, Woods BO, Carrington CB, Eplet GR,Gaensler EA. Diffuse pleural thickening in an asbestos-exposed population. Am JRadiol 1985;144:9-18.
17 Carter D, Otis CN. Three types of spindle cell tumours ofthe pleura. Fibroma, sarcoma and sarcomatoid mesoth-elioma. Am J Surg Pathol 1988;12:747-53.
18 Dervan PA, Tobin B, O'Connor M. Solitary (localised)fibrous mesothelioma: evidence against mesothelial cellorigin. Histopathology 1986;10:867-75.
19 Said JW, Nash G, Banks-Schlegel S, Sassoon AF, ShintakuPI. Localised fibrous mesothelioma. An immunohisto-chemical and electron microscopic study. Hum Pathol1984;15:440-3.
20 Briselli M, Mark EJ, Dickersin R. Solitary fibrous tumoursof the pleura: Eight new cases and review of 360 cases inthe literature. Cancer 1981;47:2678-89.
21 Corson JM, Pinkus GS. Mesothelioma: Profile of keratinproteins and carcinoembryonic antigen. An immuno-peroxidase study of 20 cases and comparison with pul-monary adenocarcinomas. Am J Pathol 1982;108:80-7.
22 Montag AG, Pinkus GS, Corson JM. Keratin proteinimmunoreactivity of sarcomatoid and mixed types ofdiffuse malignant mesothelioma. An immunoperoxidasestudy of 30 cases. Hum Pathol 1988;19:336-42.
23 Corson JM, Weiss LM, Banks-Schlegel SP, Pinkus G.Keratin proteins in synovial sarcoma. Am J Surg Pathol1983;7:107-9.
24 Chase DR, Weiss SW, Enzinger FM, Langloss JM. Keratinin epithelioid sarcoma. An immunohistochemical study.Am J Surg Pathol 1984;8:435-41.
25 Al-Izzi M, Thurlow NP, Corrin B. Pleural mesothelioma ofconnective tissue type, localised fibrous tumour of pleuraand reactive submesothelial hyperplasia. An immunohis-tochemical comparison. J Pathol 1989;158:41-4.
26 Epstein JI, Budin RE. Keratin and epithelial membraneantigen immunoreactivity in non-neoplastic fibrouspleural lesions. Implications for the diagnosis of desmo-plastic mesothelioma. Hum Pathol 1986;17:514-9.
27 Seemayer TA, Lagace R, Schurch W, Tremblay G.Myofibroblasts in the stroma of invasive and metastaticcarcinoma. Am J Surg Pathol 1979;3:525-33.
28 Lagace R, Schurch W, Seemnayer TA. Myofibroblasts in softtissue sarcomas. Virchows Arch (Pathol Anat)1980;389:1-1 1.
29 Raftery AT. Regeneration of parietal and visceral periton-eum: an electron microscopical study. J Anat 1973;115:375-92.
298