Embed Size (px)
Citation preview

Science of the Total Environment 408 (2010) 3102–3112
Contents lists available at ScienceDirect
Science of the Total Environment
j ourna l homepage: www.e lsev ie r.com/ locate /sc i totenv
Mortality due to tumours of the digestive system in towns lying in the vicinity ofmetal production and processing installations
Javier García-Pérez a,b,⁎, María Felicitas López-Cima a,b,c, Beatriz Pérez-Gómez a,b, Nuria Aragonés a,b,Marina Pollán a,b, Enrique Vidal a,b, Gonzalo López-Abente a,b
a Cancer and Environmental Epidemiology Unit, National Centre for Epidemiology, Carlos III Institute of Health, Avda. Monforte de Lemos, 5, 28029 Madrid, Spainb CIBER en Epidemiología y Salud Pública (CIBERESP), Spainc Molecular Epidemiology of Cancer Unit, University Institute of Oncology, University of Oviedo, C/Fernando Bongera, s/n, 33006 Oviedo, Spain
⁎ Corresponding author. Área de Epidemiología Ambiede Epidemiología, Instituto de Salud Carlos III, Avda.Madrid, Spain. Tel.: +34 918222640; fax: +34 913877
E-mail address: [email protected] (J. García-Pérez).
0048-9697/$ – see front matter © 2010 Elsevier B.V. Adoi:10.1016/j.scitotenv.2010.03.051
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 6 October 2009Received in revised form 15 March 2010Accepted 30 March 2010Available online 27 April 2010Keywords:Digestive tumoursMetallurgical installationsMetalworking fluidsIndustrial pollutionMortalityFocused clustering
Background: Releases to the environment of pollutants from industrial metal production and processinginstallations can pose a health problem to humans, owing to the toxic substances that such emissionscontain.Objectives: To investigate whether there might be excess mortality due to tumours of the digestive systemamong the population residing near Spanish metal production and processing installations included in theEuropean Pollutant Emission Register.Methods: Ecological study designed to examine mortality due to malignant tumours of the digestive system(oral cavity and pharynx, oesophagus, stomach, pancreas, liver, gallbladder, and colon–rectum) at themunicipal level, over the period 1994–2003. Population exposure to pollution was estimated on the basis ofdistance from town of residence to the pollution source. Using mixed Poisson regression models, weanalysed: risk of dying from cancer in a 5-kilometre zone around installations by year of commencement ofoperations; effect of pollution discharge route (air or water) and type of industrial activity; and risk gradient
within a 50-kilometre radius of such installations.Results: Excess mortality (relative risk, 95% confidence interval) was detected in the vicinity of pre-1990installations for colorectal cancer (1.05, 1.02–1.08 in men; 1.04, 1.00–1.07 in women) and liver cancer (1.06,1.00–1.12 in men), with this risk being concentrated in installations that released pollution to air. Onstratifying by type of industrial activity, statistically significant associations were also observed between theremaining tumours and certain metal production and processing activities. There was also a gradient effectin the proximity to a number of installations.Conclusions: The results support the existence of an association between risk of dying due to some tumoursof the digestive system and residential proximity to the Spanish metal production and processinginstallations studied.© 2010 Elsevier B.V. All rights reserved.
1. Introduction
Residential proximity to industrial point sources of air and waterpollution is a potential source of exposure to known or suspectedcarcinogens. Metal production and processing installations constitutean industrial sector that warrants special attention by reason of itspollutant emissions. Human exposure to metals is common, due totheir wide use in industry and long-term environmental persistence.Historically, the heaviest metal exposures occurred in the workplaceor in environmental settings situated close to industrial sources(Hayes, 1997). These types of industries, which include non-ferrous
ntal y Cáncer, Centro NacionalMonforte de Lemos, 5, 28029815.
ll rights reserved.
and ferrous metal smelters, emit inorganic arsenic and other metals,such as chromium, cadmium, lead and nickel, regarded as known orpossible carcinogens. Furthermore, fumes in the iron and steelfoundry industry are known to emit other carcinogenic substances,such as polycyclic aromatic hydrocarbons (PAHs) (Humfrey et al.,1996), while chemical exposures in the primary aluminium industryare known to include numerous toxic substances (Benke et al., 1998).In addition, metalworking fluids (MWFs) –a group of chemicalsubstances which epidemiological evidence has shown to becarcinogenic in humans (Savitz, 2003)– are used in installations forsurface treatment of metals and plastic materials, as well as to cooland lubricate metalworking processes. It would thus seem altogetherappropriate to assess the possible relationship between suchinstallations and the frequency of cancer in their environs. Amongthe tumours that have been associated with carcinogens emitted bythese industries are those of the digestive system (oral cavity and

3103J. García-Pérez et al. / Science of the Total Environment 408 (2010) 3102–3112
pharynx, oesophagus, stomach, pancreas, liver, gallbladder andcolon–rectum) (Clapp et al., 2005; Siemiatycki et al., 2004).
In Spain, tumours of the digestive system represented one third ofcancer-related deaths in 2007, with colorectal cancer being thesecond most frequent site with 13,516 deaths. This same year therewere 5747 deaths due to stomach cancer, 4976 due to pancreaticcancer, 4544 due to liver cancer, 2204 due to oral and pharyngealcancer, 1777 due to oesophageal cancer and 1305 due to gallbladdercancer, in both sexes (Instituto Nacional de Estadística, 2010). Thesetumour sites share common risk factors, such as tobacco, alcohol(colon–rectum, oral cavity and pharynx, oesophagus, liver andpancreas), ionising radiation (colon–rectum, oesophagus, stomach,liver and pancreas) and type of diet (colon–rectum, oral cavity andpharynx, stomach and pancreas) (Blot et al., 2006; Clapp et al., 2005;Crew and Neugut, 2006; Giovannucci and Wu, 2006; Hsing et al.,2006; London and McGlynn, 2006; Lowenfels and Maisonneuve,2006; Mucci and Adami, 2002). Insofar as occupational exposure isconcerned, some studies have detected an increased risk of tumoursof oesophagus, colon–rectum, stomach and pancreas among workersexposed to MWFs and mineral oils, and particularly among workersinvolved in grinding operations (Calvert et al., 1998; Mirer, 2003;Tolbert, 1997). There are also studies that have associated: exposureto heavy metals with tumours of stomach, pancreas and liver;exposure to organic solvents with tumours of rectum, oesophagus,stomach, liver and pancreas; and exposure to reactive chemicals withtumours of oral cavity and pharynx, liver and pancreas (Blair andKazerouni, 1997; Clapp et al., 2005; Landrigan et al., 2000; Lynge et al.,1997; Siemiatycki et al., 2004).
Table 1Relative risk of death due to tumours of the digestive system in towns lying at a distancePoisson mixed regression models.
Metal (all) installations Pre-1990 installations
Obsa RR 95%CI Obsa RR 95%CI
Oral and pharyngeal cancerTotal 4823 0.96 0.92–1.01 4551 0.98 0.94–1.Men 4061 0.96 0.91–1.01 3833 0.99 0.94–1.Women 762 1.02 0.92–1.12 718 1.01 0.92–1.
Oesophageal cancerTotal 3868 0.95 0.90–1.00 3655 0.97 0.92–1.Men 3403 0.93 0.88–0.98 3210 0.96 0.91–1.Women 465 1.05 0.91–1.21 445 1.08 0.94–1.
Stomach cancerTotal 12,397 1.00 0.97–1.03 11,672 1.00 0.97–1.Men 7602 0.99 0.96–1.03 7191 1.00 0.96–1.Women 4795 1.02 0.97–1.06 4481 1.00 0.95–1.
Pancreatic cancerTotal 7719 0.98 0.94–1.01 7284 0.99 0.95–1.Men 4122 1.00 0.95–1.05 3899 1.01 0.96–1.Women 3597 0.96 0.91–1.01 3385 0.96 0.91–1.
Liver cancerTotal 5154 1.05 1.00–1.10 4875 1.06 1.01–1.Men 3768 1.05 1.00–1.11 3551 1.06 1.00–1.Women 1386 1.05 0.96–1.14 1324 1.05 0.96–1.
Gallbladder cancerTotal 2652 1.00 0.94–1.06 2514 0.99 0.93–1.Men 895 1.02 0.93–1.12 852 1.03 0.93–1.Women 1757 1.01 0.94–1.09 1662 0.99 0.92–1.
Colorectal cancerTotal 23,217 1.04 1.02–1.07 21,883 1.04 1.02–1.Men 13,057 1.05 1.03–1.08 12,256 1.05 1.02–1.Women 10,160 1.03 1.00–1.06 9627 1.04 1.00–1.
a Observed.
The European Pollutant Emission Register (EPER) (EPER, 2009), apublic inventory of industries set up by the European Commissionunder the terms of Directive 96/61/EC, is a valuable resource formonitoring industrial pollution, and enables the possible associationbetween residential proximity to these pollutant installations and riskof cancer mortality to be studied (Garcia-Perez et al., 2009; Monge-Corella et al., 2008; Ramis et al., 2009). One of the EPER's industrialgroups encompasses metal production and processing installations,with data on the pollutants released and the geographical coordinatesof each installation.
This paper sought to ascertain whether there was excess mortalitydue to tumours of the digestive system among the population residingin the vicinity of Spanish metal production and processing installa-tions which report their emissions to the EPER.
2. Materials and methods
An ecological study was designed to examine mortality due totumours of the digestive system at a municipal level (8073 Spanishtowns), over the period 1994–2003. Separate analyses wereperformed for the overall population and for each sex.
Observed municipal mortality data were drawn from the recordsof the National Statistics Institute for the study period, andcorresponded to deaths coded as: malignant neoplasm of lip, oralcavity, and pharynx— codes 140–149 (International Classification ofDiseases/ICD-9) and C00–C14 (ICD-10); malignant neoplasm ofoesophagus — codes 150 (ICD-9) and C15 (ICD-10); malignantneoplasm of stomach — codes 151 (ICD-9) and C16 (ICD-10);
of less than 5km from metal production and processing installations, estimated using
Pre-1990 installations
Air Only water
Obsa RR 95%CI Obsa RR 95%CI
03 2781 0.97 0.92–1.03 1770 0.99 0.93–1.0504 2360 0.98 0.92–1.04 1473 0.99 0.92–1.0612 421 1.05 0.93–1.18 297 0.98 0.86–1.11
02 2251 0.98 0.92–1.05 1404 0.96 0.89–1.0301 1978 0.97 0.90–1.04 1232 0.94 0.88–1.0224 273 1.11 0.94–1.32 172 1.03 0.85–1.26
03 6893 1.00 0.97–1.04 4779 0.99 0.95–1.0304 4252 0.99 0.95–1.04 2939 1.01 0.96–1.0605 2641 1.03 0.97–1.09 1840 0.97 0.91–1.03
02 4203 1.00 0.96–1.05 3081 0.97 0.92–1.0206 2238 1.02 0.96–1.08 1661 1.00 0.94–1.0701 1965 0.99 0.92–1.05 1420 0.93 0.87–1.00
11 2676 1.11 1.04–1.18 2199 1.01 0.95–1.0712 1963 1.10 1.02–1.17 1588 1.02 0.96–1.1014 713 1.14 1.01–1.27 611 0.98 0.87–1.09
05 1390 0.96 0.89–1.04 1124 1.01 0.94–1.1013 461 0.96 0.85–1.09 391 1.10 0.97–1.2506 929 1.00 0.91–1.09 733 0.98 0.89–1.08
07 12,514 1.06 1.03–1.09 9369 1.02 1.00–1.0508 7088 1.06 1.02–1.09 5168 1.04 1.00–1.0807 5426 1.06 1.02–1.11 4201 1.01 0.96–1.05

3104 J. García-Pérez et al. / Science of the Total Environment 408 (2010) 3102–3112
malignantneoplasmof pancreas— codes 157 (ICD-9) andC25 (ICD-10);malignant neoplasm of liver and intrahepatic bile ducts — codes 155(ICD-9) and C22 (ICD-10); malignant neoplasm of gallbladder andextrahepatic bile ducts— codes 156 (ICD-9) and C23–C24 (ICD-10); andmalignant neoplasm of colon, rectum, and anus— codes 153–154,159.0(ICD-9) and C18–C21, C26.0 (ICD-10). Expected cases were calculatedby multiplying the specific rates for Spain as a whole, broken down byage group (18 groups), sex, and five-year period (1994–1998, 1999–2003), by the person-years for each town, broken down for the samestrata. For calculation of person-years, the two five-year periods wereconsidered, with data corresponding to the 1996 municipal roll and2001 census being taken as the estimator of the population.
Table 2Relative risk of death due to tumours of the digestive system in towns lying at a distance of lepollution to air, estimated using Poisson mixed regression models, by type of industrial act
Total Men
Obsa RR 95%CI Obs
Oral and pharyngeal cancerMultiple pollution sources 1610 1.04 0.97–1.13 136Steel 335 0.81 0.72–0.92 28Galvanizing 44 1.08 0.80–1.46 4Ferrous metals 122 0.85 0.71–1.03 10Non-ferrous metals 475 0.98 0.87–1.10 40Surface treatment 195 1.07 0.91–1.27 16
Oesophageal cancerMultiple pollution sources 1238 1.02 0.93–1.11 109Steel 333 0.99 0.87–1.13 29Galvanizing 35 1.07 0.76–1.51 3Ferrous metals 125 1.03 0.85–1.24 10Non-ferrous metals 360 0.90 0.79–1.03 31Surface treatment 160 0.97 0.81–1.17 14
Stomach cancerMultiple pollution sources 3276 0.99 0.94–1.04 206Steel 1141 1.02 0.95–1.10 70Galvanizing 114 1.16 0.96–1.41 7Ferrous metals 305 1.03 0.92–1.16 19Non-ferrous metals 1322 0.93 0.87–1.00 76Surface treatment 735 1.08 0.98–1.18 45
Pancreatic cancerMultiple pollution sources 2175 0.95 0.90–1.02 116Steel 626 0.97 0.89–1.07 35Galvanizing 68 1.05 0.82–1.33 3Ferrous metals 196 1.04 0.90–1.21 9Non-ferrous metals 822 1.06 0.97–1.15 42Surface treatment 317 1.14 1.00–1.30 17
Liver cancerMultiple pollution sources 1330 1.06 0.82–1.37 98Steel 459 1.00 0.89–1.11 33Galvanizing 65 1.47 1.14–1.90 4Ferrous metals 83 0.81 0.65–1.01 6Non-ferrous metals 582 1.38 1.23–1.54 40Surface treatment 157 1.01 0.83–1.23 12
Gallbladder cancerMultiple pollution sources 727 0.87 0.78–0.96 23Steel 214 0.99 0.85–1.16 6Galvanizing 5 0.30 0.12–0.73Ferrous metals 61 0.85 0.66–1.11 1Non-ferrous metals 249 1.15 0.98–1.35 9Surface treatment 134 1.26 1.03–1.54 4
Colorectal cancerMultiple pollution sources 6665 1.04 1.00–1.08 379Steel 1859 1.05 1.00–1.11 105Galvanizing 217 1.20 1.05–1.38 13Ferrous metals 508 0.96 0.88–1.05 29Non-ferrous metals 2323 1.09 1.03–1.15 128Surface treatment 943 1.14 1.06–1.23 53
a Observed.
Population exposure to industrial pollution was estimated byreference to the distance from the centroid of town of residence to theindustrial facility. Data on industries were obtained from the EPER-Spain (Ministerio de Medio Ambiente y Medio Rural y Marino, 2007).We selected the 118 Integrated Pollution Prevention and Control(IPPC) category-2 metal production and processing installations thatreported their releases to air and water in 2001, along with thepreviously validated geographic coordinates of their respectivelocations. These installations included: production of pig iron or steel(17 installations) — category 2.2; hot-rolling mills (steel) (5 installa-tions) — category 2.3.a; galvanizing (3 installations) — category 2.3.c;ferrous metal foundries (18 installations) — category 2.4; production
ss than 5km from pre-1990 metal production and processing installations that releasedivity.
Women
a RR 95%CI Obsa RR 95%CI
4 1.06 0.97–1.15 246 1.15 1.00–1.323 0.81 0.71–0.93 52 0.87 0.66–1.151 1.16 0.85–1.59 3 0.53 0.17–1.655 0.86 0.70–1.05 17 0.95 0.58–1.531 0.96 0.85–1.09 74 1.05 0.83–1.336 1.09 0.91–1.31 29 1.08 0.75–1.57
1 1.00 0.91–1.10 147 1.14 0.90–1.454 0.96 0.84–1.10 39 1.19 0.84–1.681 1.06 0.74–1.52 4 1.24 0.45–3.393 0.94 0.77–1.16 22 1.81 1.16–2.844 0.94 0.82–1.09 46 0.91 0.64–1.275 0.97 0.80–1.19 15 0.92 0.52–1.62
4 0.99 0.93–1.06 1212 0.98 0.90–1.077 0.99 0.91–1.09 434 1.09 0.97–1.221 1.23 0.97–1.57 43 1.07 0.79–1.462 0.99 0.86–1.15 113 1.11 0.91–1.341 0.88 0.80–0.96 561 1.02 0.91–1.147 1.12 1.00–1.26 278 1.04 0.90–1.21
6 1.00 0.92–1.09 1009 0.91 0.83–1.004 1.01 0.90–1.14 272 0.95 0.83–1.081 0.93 0.65–1.33 37 1.18 0.84–1.645 0.95 0.77–1.17 101 1.16 0.95–1.420 1.04 0.93–1.18 402 1.08 0.95–1.223 1.15 0.96–1.36 144 1.11 0.92–1.33
4 1.06 0.95–1.17 346 1.06 0.89–1.260 0.99 0.87–1.12 129 1.06 0.87–1.319 1.40 1.05–1.88 16 1.75 1.04–2.947 0.87 0.68–1.12 16 0.60 0.36–1.007 1.33 1.17–1.52 175 1.48 1.21–1.816 1.06 0.85–1.32 31 0.83 0.55–1.25
7 0.88 0.74–1.04 490 0.90 0.79–1.025 0.89 0.69–1.16 149 1.08 0.90–1.313 0.46 0.15–1.44 2 0.19 0.05–0.788 0.79 0.49–1.26 43 0.92 0.68–1.261 1.16 0.91–1.48 158 1.15 0.94–1.397 1.38 1.00–1.89 87 1.26 0.98–1.61
2 1.04 0.99–1.10 2873 1.04 0.98–1.096 1.02 0.95–1.09 803 1.09 1.01–1.183 1.27 1.06–1.51 84 1.10 0.88–1.370 0.95 0.84–1.07 218 0.97 0.85–1.125 1.09 1.01–1.17 1038 1.08 1.00–1.172 1.13 1.02–1.24 411 1.16 1.03–1.30

Table 3Relative risk of death due to tumours of the digestive system in towns situated at a distance of less than 5km from “individual” pre-1990 metal production and processinginstallations, with statistically significant results in “near vs. far” and/or RR gradient analyses.
EPER code Near vs. far RR gradient
[0–5 km) [5–10 km) [10–20 km) [20–30 km) [30–50 km)a p trend
RR 95%CI Observed RR Observed RR Observed RR Observed RR Observed
Oral and pharyngeal cancer385 Total 0.71 0.31–1.64 9 6.56 6 1.57 20 1.48 25 1.39 42 0.24
Men 0.58 0.22–1.54 6 0.54 4 1.14 17 1.37 18 1.23 35 0.70Women 1.29 0.22–7.63 3 1.02 2 6.00 3 2.12 7 2.20 7 0.05
771 Total 1.15 0.72–1.85 20 1.46 10 1.37 141 1.46 138 1.28 182 0.01Men 1.20 0.72–1.97 18 1.52 9 1.47 129 1.51 118 1.18 161 0.00Women 0.90 0.21–3.94 2 1.14 1 0.91 12 1.10 20 2.26 21 0.70
3462 Total 1.00 0.34–2.96 4 1.25 0 – 57 1.42 74 1.23 180 0.10Men 0.89 0.26–3.08 3 1.06 0 – 48 1.25 60 1.11 164 0.39Women 1.63 0.16–16.29 1 2.97 0 – 9 3.02 14 2.53 16 0.03
3684 Total 0.92 0.58–1.45 49 1.58 0 – 2 0.51 31 1.64 24 0.57Men 0.74 0.44–1.25 35 1.12 0 – 1 0.34 24 1.49 20 0.62Women 2.06 0.81–5.26 14 4.85 0 – 1 1.17 7 2.15 4 0.05
Oesophageal cancer774 Total – – 0 – 29 1.23 102 1.15 102 0.94 224 0.27
Men – – 0 – 21 1.01 87 1.10 87 0.92 199 0.72Women – – 0 – 8 2.75 15 1.58 15 1.17 25 0.04
3100 Total 1.69 1.07–2.66 22 1.53 3 0.54 102 1.28 34 1.24 110 0.16Men 1.79 1.12–2.86 21 1.47 3 0.54 88 1.13 27 1.07 100 0.33Women 0.78 0.10–5.93 1 1.24 0 0.00 14 3.50 7 3.01 10 0.15
3680 Total 1.51 0.95–2.39 44 2.84 3 1.26 15 1.77 20 1.70 41 0.04Men 1.42 0.86–2.36 36 2.31 3 1.37 12 1.61 14 1.19 35 0.07Women 2.34 0.77–7.13 8 7.62 0 0.00 3 3.02 6 8.00 6 0.21
Stomach cancer385 Total 1.62 0.97–2.69 27 2.36 11 1.54 33 1.07 41 1.03 106 0.09
Men 1.86 0.99–3.48 19 3.46 7 2.02 24 1.48 29 1.40 57 0.01Women 1.26 0.52–3.04 8 1.34 4 1.10 9 0.64 12 0.64 49 0.58
1478 Total 1.15 0.98–1.35 404 0.89 82 0.84 144 0.85 235 0.74 304 0.40Men 1.03 0.84–1.27 220 0.71 50 0.76 93 0.84 137 0.61 174 0.91Women 1.33 1.04–1.70 184 1.16 32 0.94 51 0.85 98 0.96 130 0.24
1544 Total 1.18 0.90–1.53 145 1.27 17 0.96 85 1.39 30 0.85 191 0.07Men 1.11 0.80–1.54 93 1.15 9 0.78 47 1.21 12 0.57 124 0.46Women 1.31 0.84–2.06 52 1.53 8 1.27 38 1.76 18 1.26 67 0.04
1997 Total 1.45 0.68–3.11 10 1.32 21 0.60 64 0.88 49 1.07 214 0.55Men 0.45 0.10–2.02 2 0.38 14 0.54 38 0.79 24 0.93 121 0.08Women 3.37 1.26–9.02 8 3.50 7 0.67 26 1.00 25 1.27 93 0.30
2649 Total 1.40 1.12–1.77 100 1.33 30 1.13 53 0.91 380 1.05 289 0.13Men 1.34 1.00–1.80 60 1.39 19 1.28 35 1.05 244 1.15 167 0.08Women 1.51 1.05–2.16 40 1.24 11 0.92 18 0.72 136 0.93 122 0.80
3177 Total 1.29 1.06–1.55 153 1.18 35 1.11 61 0.87 396 0.93 342 0.14Men 1.31 1.03–1.67 92 1.11 19 0.87 38 0.79 228 0.81 229 0.56Women 1.25 0.92–1.70 61 1.33 16 1.62 23 1.03 168 1.16 113 0.10
3680 Total 1.42 1.02–1.97 74 1.49 8 2.20 28 1.06 38 1.48 105 0.07Men 1.18 0.79–1.78 46 1.02 5 1.76 20 1.00 19 0.79 76 0.54Women 2.02 1.16–3.50 28 3.45 3 4.19 8 1.21 19 5.33 29 0.02
3684 Total 1.35 1.01–1.81 136 1.19 0 – 15 1.04 44 0.96 76 0.34Men 1.41 0.98–2.02 94 1.35 0 – 9 0.88 28 1.02 48 0.27Women 1.22 0.75–2.00 42 0.97 0 – 6 1.35 16 0.87 28 0.85
Pancreatic cancer76 Total 1.56 1.06–2.30 55 1.59 3 1.42 15 1.50 31 1.05 109 0.01
Men 2.12 1.25–3.58 32 2.24 1 0.82 13 2.07 20 1.22 57 0.00Women 1.04 0.59–1.85 23 1.05 2 2.44 2 0.60 11 0.87 52 0.89
1478 Total 1.23 1.02–1.49 323 1.38 53 1.10 87 0.96 189 1.22 149 0.14Men 1.11 0.86–1.44 165 0.91 34 0.88 52 0.83 90 0.83 83 0.79Women 1.37 1.04–1.82 158 2.48 19 1.51 35 1.23 99 2.07 66 0.06
1786 Total 1.30 0.84–2.00 26 1.27 11 0.87 58 1.09 35 0.75 96 0.32Men 1.72 0.98–3.01 16 1.93 6 1.08 33 1.27 15 0.74 54 0.05Women 0.93 0.47–1.83 10 0.81 5 0.76 25 1.00 20 0.74 42 0.67
3183 Total 1.00 0.74–1.37 47 1.05 38 1.40 31 1.10 57 1.15 259 0.31Men 1.16 0.78–1.72 29 1.36 23 1.75 14 0.94 38 1.23 135 0.04Women 0.83 0.51–1.35 18 0.75 15 0.93 17 1.33 19 1.10 124 0.45
3628 Total 2.23 1.11–4.46 9 2.03 1 0.30 5 0.91 19 1.16 245 0.35Men 2.10 0.83–5.29 5 1.87 0 0.00 3 0.90 11 1.08 127 0.73Women 2.44 0.85–7.00 4 2.24 1 0.72 2 0.92 8 1.25 118 0.32
Liver cancer1489 Total 1.29 0.32–5.19 3 2.62 0 – 8 2.69 12 4.32 13 0.03
Men 1.57 0.37–6.69 3 3.88 0 – 7 3.56 10 4.47 10 0.02Women 0.00 0–Inf 0 0.00 0 – 1 0.83 2 4.52 3 1.00
(continued on next page)
3105J. García-Pérez et al. / Science of the Total Environment 408 (2010) 3102–3112

Table 3 (continued)
EPER code Near vs. far RR gradient
[0–5 km) [5–10 km) [10–20 km) [20–30 km) [30–50 km)a p trend
RR 95%CI Observed RR Observed RR Observed RR Observed RR Observed
1544 Total 1.56 0.93–2.62 46 1.59 9 1.68 18 1.13 11 1.17 40 0.05Men 1.68 0.94–2.99 40 1.64 7 1.87 12 1.00 9 1.35 33 0.06Women 1.01 0.30–3.43 6 1.16 2 1.36 6 1.30 2 0.50 7 0.68
3337 Total 1.45 1.01–2.06 34 1.50 15 1.38 14 1.46 3142 1.07 357 0.01Men 1.35 0.88–2.07 23 1.38 14 1.71 10 1.37 2163 1.05 267 0.04Women 1.71 0.91–3.22 11 1.83 1 0.38 4 1.82 979 1.13 90 0.14
3421 Total 2.48 1.07–5.80 93 4.33 4 2.07 17 1.48 10 1.91 45 0.01Men 2.20 0.85–5.69 70 3.85 3 1.50 14 1.62 4 0.84 35 0.03Women 4.53 0.67–30.57 23 18.39 1 13.31 3 1.39 6 9.56 10 0.06
3628 Total 2.06 0.72–5.83 4 1.67 1 0.98 3 2.01 5 0.81 140 0.34Men 1.35 0.32–5.79 2 1.23 0 0.00 2 1.83 2 0.38 107 0.80Women 4.47 0.97–20.58 2 3.07 1 5.35 1 2.55 3 2.87 33 0.04
Gallbladder cancer3397 Total 1.20 0.78–1.87 23 1.24 2 0.62 1106 1.07 58 1.00 134 0.48
Men 1.49 0.73–3.04 9 2.10 1 1.38 371 1.86 19 1.43 33 0.03Women 1.09 0.62–1.90 14 0.98 1 0.40 735 0.83 39 0.86 101 0.50
3628 Total 2.18 0.76–6.24 4 1.95 3 2.26 1 0.34 8 1.17 105 0.25Men 0.00 0–Inf 0 0.00 0 0.00 0 0.00 1 0.30 37 0.13Women 3.34 1.14–9.75 4 3.28 3 4.97 1 0.68 7 1.78 68 0.01
3705 Total 1.79 0.91–3.53 12 2.72 2 1.02 28 1.85 11 1.84 11 0.06Men 1.15 0.33–4.08 3 2.19 1 0.57 10 1.54 5 1.80 6 0.65Women 2.08 0.91–4.73 9 3.85 1 6.15 18 4.08 6 4.07 5 0.03
Colorectal cancer30 Total 1.37 0.97–1.93 69 1.33 12 1.26 37 1.07 86 1.13 212 0.21
Men 1.64 1.07–2.51 45 1.87 8 1.35 23 1.18 44 0.98 126 0.05Women 0.98 0.55–1.74 24 0.41 4 1.12 14 0.94 42 1.34 86 0.61
774 Total – – 0 – 99 1.12 394 1.04 452 1.11 850 0.30Men – – 0 – 56 1.31 207 1.15 227 1.11 431 0.05Women – – 0 – 43 0.94 187 0.93 225 1.11 419 0.61
1478 Total 1.09 0.98–1.23 848 1.20 157 1.16 264 1.06 496 1.06 403 0.08Men 1.23 1.05–1.44 452 1.30 85 1.19 129 0.91 251 1.02 230 0.03Women 0.97 0.82–1.14 396 1.15 72 1.16 135 1.27 245 1.14 173 0.81
1544 Total 1.19 0.96–1.47 217 1.20 28 0.79 123 1.02 64 0.94 304 0.28Men 1.04 0.78–1.39 114 1.07 16 0.88 74 1.11 36 1.04 172 0.74Women 1.41 1.02–1.94 103 1.39 12 0.68 49 0.90 28 0.82 132 0.21
1606 Total 1.17 0.82–1.67 46 1.62 0 – 3 0.53 75 1.56 266 0.04Men 1.41 0.89–2.24 27 1.93 0 – 2 0.55 43 1.82 143 0.02Women 0.85 0.48–1.52 19 1.30 0 – 1 0.66 32 1.39 123 0.62
3076 Total 1.09 0.99–1.20 850 1.00 17 0.85 529 0.88 114 0.96 870 0.81Men 1.14 1.01–1.29 476 1.06 11 1.11 289 0.91 65 1.05 463 0.34Women 1.03 0.90–1.18 374 0.93 6 0.59 240 0.84 49 0.85 407 0.46
3183 Total 1.26 1.07–1.49 172 1.29 116 1.33 71 0.80 158 1.04 791 0.00Men 1.11 0.88–1.41 83 1.14 67 1.38 36 0.75 93 1.12 424 0.16Women 1.44 1.14–1.81 89 1.46 49 1.27 35 0.85 65 0.94 367 0.01
3486 Total 1.24 0.89–1.72 50 1.20 43 1.12 1037 1.10 998 0.95 469 0.16Men 1.57 1.05–2.33 37 1.52 23 0.87 603 1.10 578 0.93 286 0.35Women 0.77 0.42–1.42 13 0.75 20 1.60 434 1.09 420 1.00 183 0.29
3684 Total 1.01 0.81–1.26 203 1.18 0 – 34 1.33 92 1.15 109 0.41Men 0.85 0.64–1.13 119 0.92 0 – 17 0.99 68 1.24 67 0.30Women 1.30 0.91–1.88 84 1.77 0 – 17 2.04 24 0.93 42 0.01
3703 Total 1.46 0.99–2.17 34 1.50 16 1.03 28 0.79 85 1.01 347 0.06Men 1.20 0.70–2.07 17 1.29 10 0.76 16 0.76 47 0.92 202 0.44Women 1.88 1.06–3.33 17 1.87 6 1.60 12 0.80 38 1.15 145 0.05
a Reference group in RR gradient analysis.
Liver cancer
3106 J. García-Pérez et al. / Science of the Total Environment 408 (2010) 3102–3112
of non-ferrous crude metals (7 installations) — category 2.5.a;smelting of non-ferrous metals (19 installations) — category 2.5.b;and surface treatment of metals and plastic materials using anelectrolytic or chemical process (49 installations) — category 2.6.Data on date of commencement of industrial activity were obtainedfrom official websites of the metal industries.
In a first phase, we conducted an initial exploratory “near vs. far”analysis to estimate the relative risks (RRs) of towns situated at a distanceof less than 5km frommetal production and processing installations. Theexposurevariablewascodedasa “dummy”with the following three levels:
1) exposedgroup(“near”), i.e., townshaving theirmunicipal centroidat adistance ≤5 km from a metal production and processing installation;
2) intermediate group, i.e., townsat adistance≤5 kmfromany industrialinstallation other than production and processing of metals; and,
3) unexposed group (“far”), i.e., towns having no EPER-registeredindustry within 5 km of their municipal centroid (reference level).
RRs and their 95% confidence intervals (95%CIs) were estimated onthe basis of a Poisson regression model (Breslow and Day, 1987),using expected cases as offset for the total population, men, andwomen, and the Spanish rates as reference. Estimationswere adjustedfor the following standardised socio-demographic indicators, chosenfor their availability at a municipal level: population size; percentageof illiteracy, farmers and unemployed; average persons per householdaccording to the 1991 census; and, mean income as a measure of

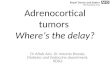
Fig. 1. Geographical location of “individual” metal production and processing installations which commenced operations prior to 1990 and displayed statistically significant excessmortality in the “near vs. far” analysis and/or significant test for trend in the risk gradient analysis, for two or more tumours specified in the headline of each map.
3107J. García-Pérez et al. / Science of the Total Environment 408 (2010) 3102–3112
income level (Ayuso Orejana et al., 1993). In addition, mixed modelswere fitted (Gelman and Hill, 2007), including province as a randomeffects term, to enable geographic variability to be taken into accountand unexposed towns belonging to the same geographic setting to beconsidered as the reference level, something that is justified by thegeographic differences observed in mortality attributable to thesetumours (Lopez-Abente et al., 2006).
In order to take theminimum tumour latency periods into account,the analysis was replicated, by confining the above model to the 105industries that entered into operation prior to 1990. Furthermore,separate analyses were performed for industries that had releasedsome type of pollutant to air (61 installations) and for those that hadreleased pollutants solely to water (44 installations). Similarly, inorder to stratify the risk by type of industrial activity, we created avariable of interest coded as a “dummy” with various levels:
1) group 1, i.e., towns lying at ≤5 km from more than one IPPCcategory-2 metal installation (multiple pollution sources);
2) group 2, i.e., towns lying at ≤5 km from a single IPPC category-2.2or -2.3.ametal installation (steel production and hot-rollingmills);
3) group 3, i.e., towns lying at≤5 km from a single IPPC category-2.3.c metal installation (galvanizing);
4) group 4, i.e., towns lying at ≤5 km from a single IPPC category-2.4metal installation (ferrous metal smelters);
5) group 5, i.e., towns lying at≤5 km froma single IPPC category-2.5.a or-2.5.b metal installation (non-ferrous metal smelters and producers);
6) group 6, i.e., towns lying at ≤5 km from a single IPPC category-2.6metal installation (surface treatment using an electrolytic orchemical process);
7) intermediate group, i.e., towns lying at ≤5 km from any industryother than metal production and processing; and,
8) unexposed group, i.e., towns having no EPER-registered industrywithin a radius of 5 km from the centroid (reference level).
Finally, in view of that fact that the characteristics of the respectivemetal installations vary (years of operation, type and amount of

3108 J. García-Pérez et al. / Science of the Total Environment 408 (2010) 3102–3112

3109J. García-Pérez et al. / Science of the Total Environment 408 (2010) 3102–3112
emissions), a “near vs. far” analysiswas performed in the case of townsbelonging to groups 2–6 (“individual” metal pollution sources) witheach installation that commenced operations prior to 1990 beinganalysed individually (38 installations). Moreover, the analysis wasconfined to an area of 50 km surrounding each complex, so as to have alocal comparison group. To take into account the problem of multiplecomparisons, p-values were also suitably adjusted by controlling forthe expected proportion of false positives (False Discovery Rate), usingthe method proposed by Benjamini (Benjamini and Hochberg, 1995;Benjamini and Yekutieli, 2001). The risk gradient in the vicinity of eachfacilitywas likewise studied,with distance from town to installation asan explanatory variable, categorised in concentric rings (0–5, 5–10,10–20 and 20–30 km; and 30–50 km as reference). This was includedin all models as both a categorical and a continuous variable, therebymaking it possible for: the effect of the respective distances to beestimated by the former; the existence of radial effects to beascertained by the latter (rise in RR with increasing proximity to aninstallation); and, by applying the likelihood ratio test, the statisticalsignificance of such distance-related effects to be computed. RRestimates were adjusted for the above-mentioned socio-demographicvariables, and towns that had some EPER-registered industry otherthanproduction andprocessing ofmetalswithin a radius of 5 kmof themunicipal centroid were excluded.
3. Results
From 1994 to 2003 there were 113,512 deaths in Spain due tocolorectal cancer, 62,185 due to stomach cancer, 38,227 due topancreatic cancer, 23,251 due to liver cancer, 21,875 due to oral andpharyngeal cancer, 17,823 due to oesophageal cancer and 13,865 dueto gallbladder cancer, in both sexes.
Table 1 shows the RRs and their 95%CIs for towns with metalproduction and processing installations at a distance of less than 5 km,estimated by Poisson mixed regression models for the seven tumoursunder study. As can be seen, the “near vs. far” analysis covering allmetal installations and those that commenced operations prior to1990 showed a slight statistically significant excess risk of dying dueto liver and colorectal cancer in towns in the vicinity of theseinstallations, both overall and for males (in the case of colorectalcancer there was also a significant excess risk for women). When thisrisk was stratified by pollution discharge route (air or only water), inliver cancer the significant excess risk was concentrated exclusively ininstallations that released some type of pollutant to air, whereas incolorectal cancer the statistically significant excess risk appeared inboth types of installations, for the overall population and males alike,but was nevertheless greater in installations with releases to air. Itshould also be noted that, in the case of women, there was asignificant excess risk of both tumours associated with this latter typeof installation.
Table 2 shows the RRs of towns lying at less than 5 km from pre-1990 metal production and processing installations that releasedpollution to air, by type of industrial activity, for the seven tumoursunder study. In cancer of oral cavity and pharynx, a statisticallysignificant excess risk was observed for women in towns exposed tomultiple pollution sources. In oesophageal cancer, the highest RR(1.81) was found among women in towns lying close to ferrous metalfoundries. Insofar as tumours of stomach and pancreas wereconcerned, the significant excess risk was concentrated in thesurroundings of installations for surface treatment using an electro-lytic or chemical process, among males and the overall populationrespectively. For liver cancer, which already registered a statistically
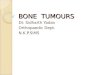
ig. 2. Geographical location of “individual” metal production and processing installations which commenced operations prior to 1990 and displayed statistically significant excessortality in the “near vs. far” analysis and/or significant test for trend in the risk gradient analysis, for a single tumour.
Fm
significant excess risk in the analysis shown in Table 1, the risk wasconcentrated in the environs of galvanizing installations and non-ferrous metal producers and smelters, among men and women alike.Gallbladder cancer displayed a significant excess risk for males intowns lying in the vicinity of installations for surface treatment. Lastly,for colorectal cancer therewas a significant excess risk in both sexes inthe vicinity of almost all types of industrial activities studied, with thesingle exception of the ferrous metal group. The sex-specific analysisshowed that, among men, the excess was concentrated in thesurroundings of galvanizing, non-ferrous metals and surface treat-ment installations, whilst among women this was found in thevicinity of steel, non-ferrous metal and surface treatmentinstallations.
With regard to metal production and processing installations thatreleased pollution solely to water (data not shown), there was anelevated, statistically significant excess risk (3.81) for cancer of oralcavity and pharynx among women in towns lying in the vicinity offerrous metal installations, though with only 3 cases observed.Attention should be drawn to the fact that among males, liver cancerdisplayed an RR of 1.59 in towns neighbouring galvanizing complexes,and gallbladder cancer displayed an RR of 2.10 for non-ferrous metalinstallations. In the case of colorectal cancer, a significant excess riskwas observed in the environs of multiple pollution sources (1.09) formen, and in the environs of ferrous metal (1.80) and non-ferrousmetal installations (1.35) for women.
Table 3 shows the RRs for the environs of “individual” metalpollution sources that commenced industrial activity prior to 1990,and for ever-decreasing radiuses within a 50-kilometre areasurrounding each complex. The data are shown for complexeswhich yielded statistically significant results in the “near vs. far”and/or risk gradient analyses, for one or more of the tumours studied.Of the 26 installations shown in the table, a total of 8 (thegeographical locations of which are depicted in Fig. 1) registeredsignificant results for two or more tumours. In general, excess risksand significant test for trend appeared in both men and women.
The analyses in the above table were performed separately foreach of the pre-1990 installations (both “individual” and multiplepollution sources), as were the corrections using multiple compar-isons (see Supplementary material).
Fig. 2 depicts the geographical location of those metal productionand processing installations in Table 3 which registered significantresults for a single tumour.
4. Discussion
Our results indicate a slight excess risk of dying from liver canceramong men, and from colorectal cancer in both sexes, in the vicinity ofSpanish metal production and processing installations, regardless ofwhether these are studied jointly or after eliminating the most recentinstallations, the possible influence ofwhich is arguable bearing inmindthe minimal latency periods of solid tumours. Moreover, on stratifyingthe risk by pollution discharge route and type of industrial activity,associations were observed between the remaining tumours studiedand residential proximity to certain types of installations, namely:
a) between “installations for surface treatment using an electrolyticor chemical process”which release pollution to air, and tumours ofstomach (men), pancreas (total population), gallbladder (men)and colon–rectum (both sexes);
b) between “non-ferrous metal production and smelting installa-tions” that release pollution to air and tumours of liver and colon–

3110 J. García-Pérez et al. / Science of the Total Environment 408 (2010) 3102–3112
rectum (both sexes), and between those that release pollution towater only and tumours of gallbladder (men) and colon–rectum(women);
c) between “galvanizing installations” that release pollution to air andtumours of liver (both sexes)andcolon–rectum(men), andbetweenthose that release pollution to water only and liver cancer (men);
d) between “ferrous metal smelting installations” that releasepollution to air and oesophageal cancer (women), and betweenthose that release pollution to water only and colorectal cancer(women); and,
e) between “hot-rolling steel mills” that release pollution to air andcolorectal cancer (women).
It is important to mention here that, in the individualised analysis,there were quite a few industries that registered statisticallysignificant results in both sexes, in the “near vs. far” and risk gradientanalyses, for one or more of the seven tumours studied, and for thoseof the colon–rectum, stomach and liver in particular.
A further noteworthy aspect of the results is the fact that, intumours of liver and colon–rectum, significant excess risks affectedboth sexes, which might be indicative of a pathway of environmentalexposure. In tumours of stomach and gallbladder, however, thesignificant results solely affected men, thus being indicative of apossible occupational-exposure pathway. Owing to a lack of data, wewere unable to control for occupational exposures that might accountfor this difference between men and women. Lastly, it should also benoted that, for oesophageal cancer, the highest excess risks wereexclusively in evidence for women.
Despite suffering from some limitations, the hypothesis that someexcess cancer mortality may, in part, be due to pollutant emissions ofindustrial origin has gathered strength in recent years. Specifically, aseries of studies has been published reinforcing the idea of a possibleassociation between residential proximity to industrial complexesand an increased risk of various tumours, such as those of lung, larynx,bladder, non-Hodgkin's lymphoma, prostate and colon–rectum (Case-lla et al., 2005; Garcia-Perez et al., 2009; Parodi et al., 2005; Ramiset al., 2009; Tsai et al., 2009; Viel et al., 2008). Although occupationalstudies serve to formulate hypotheses and guide research into manycarcinogenic risk factors (Firth et al., 1999; Rotimi et al., 1993; Simet al., 2009), the association between industrial emissions anddigestive tumours in the population can be studied via other typesof designs, such as the one described in this study. One advantage ofthe design chosen is its high power, owing to the inclusion of a greaternumber of subjects. Another advantage lies in the fact that theanalysis can be repeated in future for the purpose of monitoring andcontrolling for the effects of environmental pollution on health.
This study likewise has some limitations.Workingwith small areasmeans that the data display great random variability, an aspect thatcould affect women in the results obtained for some tumour sites,though the small study area reduces any possible ecological biasassociated with the nature of the study per se.
In an attempt to reduce possible biases deriving from confoundingvariables not included in the study, mixed models were fitted with“province” as the random effects term, something that constitutes amore conservative option. Another point to be borne in mind is thatsome installations for which significant excess risks were observed,are situated in areas with numerous industries releasing pollutioninto the environment. This is why risk was stratified by type ofindustrial activity and a distinction drawn between “multiple andindividual metal pollution sources”, with in-depth analysis of theinstallations belonging to this latter group, in which towns areexposed to a single metal-sector pollution source.
This study uses distance to the pollution source as a proxy ofexposure, assuming an isotropic model, something that couldintroduce a problem of misclassification, since real exposure iscritically dependent on prevailing winds, geographical landforms
and releases into aquifers. A further possible bias in the allocation ofexposure is the use of centroids as coordinates to pinpoint the entirepopulation of a town, when, in reality, the population may be fairlywidely dispersed. Nevertheless, these problems would be posed in allcases, limiting the capacity to find positive results but not invalidatingthe associations found.
Another critical decision when analysing the risk of towns situated“near” pollution sources is the choice of radius. The choice of 5 kmaround metal production and processing installations is in line withthe characteristics of such plants, many of which extend over largesurface areas and release discharges to the local water, with thepollution so emitted achieving a wide radius of spread.
Although the industries analysed in this study reported pollutiondata in 2001, the date of commencement of their industrial activitywas nevertheless taken into account for analytical purposes: the greatmajority began operations prior to the 1960s, so that the surroundingpopulations could have been exposed to their emissions for longperiods of time, a fact that is coherent with the latency periodsdescribed for solid tumours.
Of all the industrial groups registered in the EPER-Spain, metalproduction and processing installations are the principal emitters toair of cadmium, hydrogen cyanide, CO, chromium, copper, lead,perfluorocarbons, tetrachloroethylene and zinc, and the principalemitters to water of benzene, toluene, ethylbenzene, xylenes,cyanides, dichloromethane, phenols, fluorides, PAHs and nickel.
The presence of metal production and processing installations,which encompass several types of industrial activities, arouses socialalarm due to the health problems that may be generated in theirworkers and environs, and the financial consequences stemming froma possible administrative intervention. According to the InternationalAgency for Research on Cancer (IARC), exposure circumstances suchas aluminium production and iron and steel founding are recognisedas carcinogenic to humans, as are a number of substances released bysuch installations, including arsenic, benzene, cadmium, chromium,dioxins, asbestos, formaldehyde, radon, silica, crystalline, soots, coal-tar pitches and some PAHs. Other substances are either: probablecarcinogens, such as tetrachloroethylene, trichloroethylene, acrylam-ide and nitrosamines; or possible carcinogens, such as lead, nickel,furans, ethylbenzene, hexachloroethane and welding fumes (IARC,2009; Tossavainen, 1990). Additionally, chemical exposures entailedin the alumina and primary aluminium industry include many toxicsubstances, such as diesel fumes, solvents, oils, sulphur dioxide,copper dust and silica dust (Benke et al., 1998). Moreover, installa-tions for surface treatment of metals and plastic materials (many ofwhich belong to the automobile sector) use MWFs, a range of oils andother chemical substances, which are used to cool and/or lubricatemetal workpieces when they are being machined, ground, milled, etc.,and are known to be carcinogens in humans (Savitz, 2003). There issubstantial evidence to show that some MWFs have been associatedwith increased risk of certain cancers, including tumours of thedigestive system. Although measures have been taken in recentdecades to reduce these exposures in the occupational sphere, e.g.,removal of PAHs from MWFs began in the 1950s, and U.S.Environmental Protection Agency (US-EPA) regulations in the 1980swere directed at reducing nitrosamine exposures, there is nonethelessinsufficient data to conclude that these changes will have eliminatedall carcinogenic risks (DHHS (NIOSH), 1998). Lastly, it should bestressed that effluents from the metals industries are genotoxic: theyinduce cytogenetic damage, mutations, and DNA damage in repairprocesses (Houk, 1992).
A number of studies have associated residential proximity to metalproduction and processing installations with lung cancer (Brownet al., 1984; Pershagen, 1985; Smith et al., 1987). In the case oftumours of the digestive system, Casella observed an associationbetween municipal proximity to a steel production plant and excessrisk of colorectal and bowel cancer in women (Casella et al., 2005).

3111J. García-Pérez et al. / Science of the Total Environment 408 (2010) 3102–3112
Furthermore, some studies have reported statistically significantexcess risks in metal industry workers, due to tumours of stomach(Rockette and Arena, 1983; Rotimi et al., 1993; Sim et al., 2009),pancreas (Rockette and Arena, 1983; Rotimi et al., 1993), liver(Adzersen et al., 2003) and oesophagus (Firth et al., 1999). Firth alsodetected a significant excess mortality when he studied all thetumours of the digestive system as a whole (Firth et al., 1999). Insofaras occupational exposure to MWFs is concerned, a number of studieshave linked this to tumours of the digestive system, particularly thoseof pancreas, rectum and stomach (Bardin et al., 1997; Calvert et al.,1998; Malloy et al., 2007; Mirer, 2003).
One of the most interesting results of our study is the excessmortality due to tumours of liver and colon–rectum in the vicinity ofgalvanizing installations. The galvanizing sector is one of theindustrial activities that releases dioxins to air (ATEG-Grupo Interlab,2005) and is included in the Spanish National Dioxin and FuraneInventory (Martinez et al., 2008). Dioxins are recognised by the IARCas carcinogens in humans (IARC, 2009) and there are studies that haveobserved increased risks for all cancers combined, and for digestivesystem cancers in particular (IARC, 1997). Furthermore, humanexposure to dioxins due to industrial or accidental exposure hasbeen associated with alterations in liver enzyme levels in children andadults (IARC, 1997).
Another of themost noteworthy results is the excess mortality dueto tumours of liver, gallbladder and colon–rectum found in thevicinity of non-ferrous metal production and smelting installations.One of the principal environmental challenges facing these types ofinstallations, especially facilities producing copper, aluminium, lead,zinc, cadmium and alkalinemetals, is the treatment and elimination ofdioxins which are generated by the presence of small amounts ofchlorine in secondary raw materials (Integrated Pollution PreventionControl (IPPC) (2001)). As mentioned above, these substances arecarcinogens linked to tumours of the digestive system and could berelated to the excess risk observed in our study. Finally, the point mustbemade that non-ferrousmetals smelting installations release arsenicto air, a known carcinogen for liver cancer (Clapp et al., 2005).
In brief, it can be said that industrial emissions from metalproduction and processing installations comprise a complex mix ofcarcinogens and toxic substances released to air and water. It is highlylikely that chemical substances released to water pass into the soil andwater catchment areas, and thence into the human food chain, wherethey cause damage to the digestive organs. With regard to substancesreleased to air, on the one hand the population would be directlyexposed to the polluted air, and on the other, the heavy metals wouldbe deposited in plants, soil and water, and would then pass into thetrophic chain affecting the population.
The fact that EPER data are available to the public means thatemissions from these types of installations can be ascertained.Unfortunately, there are no data on the amounts of hazardous waste(such as MWFs and mineral oils) discharged by these industrialcomplexes, though the updating of the EPER in the form of the newEuropean Pollutant Release and Transfer Register (E-PRTR) at the endof 2009 will provide a valuable tool for gathering information on thistype of toxic waste.
5. Conclusion
The results of this study show: an association between residentialproximity to metal production and processing installations as a wholeand excess risk of mortality due to tumours of liver and colon–rectum;and an excess risk in the remaining tumours of the digestive systemassociatedwith certain types of industrial activity. Furthermore, in theenvirons of a number of “individual” pollution sources, excess riskswere observed in the “near vs. far” analysis, along with statisticallysignificant risk gradients. The ecological nature of the study may
hinder interpretation of the results of association in terms of causeand effect.
At present, the study of cancer mortality in areas surroundingindustrial pollution sources is beginning to assume growing impor-tance, and industrial pollutant emission registers such as the EPER andE-PRTR afford a very useful tool for the surveillance andmonitoring ofthe possible effects of industrial pollution on the health of thepopulation.
Acknowledgements
This study was funded by a grant from Spain's Health ResearchFund (Fondo de Investigación Sanitaria — FIS 040041) and formed partof the MEDEA project (Mortalidad en áreas pequeñas Españolas yDesigualdades socio-Económicas y Ambientales — Mortality in smallSpanish areas and socio-economic and environmental inequalities).
Appendix A. Supplementary data
Supplementary data associated with this article can be found, inthe online version, at doi:10.1016/j.scitotenv.2010.03.051.
References
Adzersen KH, Becker N, Steindorf K, Frentzel-Beyme R. Cancer mortality in a cohort ofmale German iron foundry workers. Am J Ind Med 2003;43:295–305.
ATEG-Grupo Interlab. Documento de orientación sectorial para la medición, cálculo yestimación de emisiones de sustancias EPER; 2005. Available: http://www.prtr-es.es/fondo-documental/metodos-de-medicion-y-calculo,15500,10,2007.html[accessed 15 March 2010].
Ayuso Orejana J, Fernández Cuesta JA, Plaza Ibeas JL. Anuario del Mercado Español.Madrid: Banco Español de Crédito; 1993.
Bardin JA, Eisen EA, Tolbert PE, Hallock MF, Hammond SK, Woskie SR, et al. Mortalitystudies of machining fluid exposure in the automobile industry. V: a case–controlstudy of pancreatic cancer. Am J Ind Med 1997;32:240–7.
Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerfulapproach to multiple testing. J R Stat Soc Ser B (Methodol) 1995;27:289–300.
Benjamini Y, Yekutieli D. The control of the false discovery rate in multiple testingunder dependency. Ann Stat 2001;29:1165–88.
Benke G, Abramson M, Sim M. Exposures in the alumina and primary aluminiumindustry: an historical review. Ann Occup Hyg 1998;42:173–89.
Blair A, Kazerouni N. Reactive chemicals and cancer. Cancer Causes Control 1997;8:473–90.
Blot WJ, McLaughlin JK, Fraumeni Jr JF. Esophageal cancer. In: Schottenfeld D, FraumeniJr JF, editors. Cancer Epidemiology and Prevention. Third Edition. New York: OxfordUniversity Press; 2006. p. 697–706.
Breslow NE, Day NE. Statistical methods in cancer research. Volume II—the design andanalysis of cohort studies. IARC Sci Publ; 1987. p. 1-406.
Brown LM, Pottern LM, Blot WJ. Lung cancer in relation to environmental pollutantsemitted from industrial sources. Environ Res 1984;34:250–61.
Calvert GM, Ward E, Schnorr TM, Fine LJ. Cancer risks among workers exposed tometalworking fluids: a systematic review. Am J Ind Med 1998;33:282–92.
Casella C, Garrone E, Gennaro V, Orengo MA, Puppo A, Stagnaro E, et al. Healthconditions of the general population living near a steel plant. Epidemiol Prev2005;29:77–86.
Clapp RW, Howe GK, Jacobs MM. Environmental and occupational causes of cancer. AReview of Recent Scientific Literature. Lowell Center for Sustainable Production;2005.
Crew KD, Neugut AI. Epidemiology of gastric cancer. World J Gastroenterol 2006;12:354–62.
DHHS (NIOSH). Criteria for a recommended standard: occupational exposure tometalworking fluids. No. 98–102. National Institute for Occupational Safety andHealth; 1998.
EPER. European Pollutant Emission Register; 2009. Available: http://eper.ec.europa.eu/eper/ [accessed 15 March 2010].
Firth HM, Elwood JM, Cox B, Herbison GP. Historical cohort study of a New Zealandfoundry and heavy engineering plant. Occup Environ Med 1999;56:134–8.
Garcia-Perez J, Pollan M, Boldo E, Perez-Gomez B, Aragones N, Lope V, et al. Mortalitydue to lung, laryngeal and bladder cancer in towns lying in the vicinity ofcombustion installations. Sci Total Environ 2009;407:2593–602.
Gelman A, Hill J. Data analysis using regression and multilevel/hierarchical models.New York: Cambridge University Press; 2007.
Giovannucci E, Wu K. Cancer of the colon and rectum. In: Schottenfeld D, Fraumeni Jr JF,editors. Cancer Epidemiology and Prevention. Third Edition. New York: OxfordUniversity Press; 2006. p. 809–29.
Hayes RB. The carcinogenicity of metals in humans. Cancer Causes Control 1997;8:371–85.
Houk VS. The genotoxicity of industrial wastes and effluents. Mutat Res 1992;277:91-138.

3112 J. García-Pérez et al. / Science of the Total Environment 408 (2010) 3102–3112
Hsing AW, Rashid A, Devesa SS, Fraumeni Jr JF. Biliary tract cancer. In: Schottenfeld D,Fraumeni Jr JF, editors. Cancer Epidemiology and Prevention. Third Edition. NewYork: Oxford University Press; 2006. p. 787–800.
Humfrey CD, Levy LS, Faux SP. Potential carcinogenicity of foundry fumes: acomparative in vivo–in vitro study. Food Chem Toxicol 1996;34:1103–11.
IARC. Monographs on the evaluation of carcinogenic risks to humans. PolychlorinatedDibenzo-para-dioxins and Polychlorinated Dibenzofurans; 1997. Available: http://monographs.iarc.fr/ENG/Monographs/vol69/index.php [accessed 15 March 2010].
IARC. Monographs on the evaluation of carcinogenic risks to humans; 2009. Available:http://monographs.iarc.fr/ENG/Classification/crthall.php [accessed 15 March 2010].
Instituto Nacional de Estadística. Defunciones según la Causa de Muerte 2007; 2010.Available: http://www.ine.es/jaxi/tabla.do?path=/t15/p417/a2007/l0/&file=01001.px&type=pcaxis&L=0 [accessed 15 March 2010].
Integrated Pollution Prevention Control (IPPC). Reference document on best availabletechniques in the non ferrousmetals industries; 2001. Available: http://www.prtr-es.es/data/images/BREF%20Metalurgia%20no%20f%C3%A9rrea%20I-4CDE805E16D2361F.pdf[accessed 15 March 2010].
Landrigan PJ, Boffetta P, Apostoli P. The reproductive toxicity and carcinogenicity oflead: a critical review. Am J Ind Med 2000;38:231–43.
London WT, McGlynn KA. Liver cancer. In: Schottenfeld D, Fraumeni Jr JF, editors.Cancer Epidemiology and Prevention. Third Edition. New York: Oxford UniversityPress; 2006. p. 763–86.
Lopez-Abente G, Ramis R, PollanM, Perez-Gomez B, Gomez-Barroso D, Carrasco JM, et al.Atlas municipal de mortalidad por cáncer en España, 1989–1998. Instituto de SaludCarlos III; 2006.
Lowenfels AB, Maisonneuve P. Epidemiology and risk factors for pancreatic cancer. BestPract Res Clin Gastroenterol 2006;20:197–209.
Lynge E, Anttila A, Hemminki K. Organic solvents and cancer. Cancer Causes Control1997;8:406–19.
Malloy EJ, Miller KL, Eisen EA. Rectal cancer and exposure to metalworking fluids in theautomobile manufacturing industry. Occup Environ Med 2007;64:244–9.
Martinez MA, Sanz P, Ruiz ML, Fabrellas B, Abad E, Rivera J. Evaluation of the Spanishhot dip galvanising sector as a source of polychlorinated dibenzo-p-dioxins andpolychlorinated dibenzofurans. Chemosphere 2008;71:1127–34.
Ministerio de Medio Ambiente y Medio Rural y Marino. Registro Estatal de Emisiones yFuentes Contaminantes; 2007. Available: http://www.prtr-es.es/ [accessed 15March 2010].
Mirer F. Updated epidemiology of workers exposed to metalworking fluids providessufficient evidence for carcinogenicity. Appl Occup Environ Hyg 2003;18:902–12.
Monge-Corella S, Garcia-Perez J, Aragones N, PollanM, Perez-Gomez B, Lopez-Abente G.Lung cancer mortality in towns near paper, pulp and board industries in Spain: apoint source pollution study. BMC Public Health 2008;8:288.
Mucci L, Adami HO. Oral and pharyngeal cancer. In: Adami HO, Hunter D, TrichopoulosD, editors. Textbook of cancer epidemiology. New York: Oxford University Press;2002.
Parodi S, Stagnaro E, Casella C, Puppo A, Daminelli E, Fontana V, et al. Lung cancer in anurban area in Northern Italy near a coke oven plant. Lung Cancer 2005;47:155–64.
Pershagen G. Lung cancer mortality among men living near an arsenic-emittingsmelter. Am J Epidemiol 1985;122:684–94.
Ramis R, Vidal E, Garcia-Perez J, Lope V, Aragones N, Perez-Gomez B, et al. Study of non-Hodgkin's lymphoma mortality associated with industrial pollution in Spain, usingPoisson models. BMC Public Health 2009;9:26.
Rockette HE, Arena VC. Mortality studies of aluminum reduction plant workers:potroom and carbon department. J Occup Med 1983;25:549–57.
Rotimi C, Austin H, Delzell E, Day C, Macaluso M, Honda Y. Retrospective follow-upstudy of foundry and engine plant workers. Am J Ind Med 1993;24:485–98.
Savitz DA. Epidemiologic evidence on the carcinogenicity of metalworking fluids. ApplOccup Environ Hyg 2003;18:913–20.
Siemiatycki J, Richardson L, Straif K, Latreille B, Lakhani R, Campbell S, et al. Listingoccupational carcinogens. Environ Health Perspect 2004;112:1447–59.
Sim MR, Del Monaco A, Hoving JL, Macfarlane E, McKenzie D, Benke G, et al. Mortalityand cancer incidence in workers in two Australian prebake aluminium smelters.Occup Environ Med 2009;66:464–70.
Smith GH, Williams FL, Lloyd OL. Respiratory cancer and air pollution from ironfoundries in a Scottish town: an epidemiological and environmental study. Br J IndMed 1987;44:795–802.
Tolbert PE. Oils and cancer. Cancer Causes Control 1997;8:386–405.Tossavainen A. Estimated risk of cancer attributable to occupational exposures in iron
and steel foundries. In: Vainio H, Sorsa M, McMichael AJ, editors. Complex mixturesand cancer risk. Lyon: IARC Scientific Publications; 1990. p. 363–7.
Tsai SS, Tiao MM, Kuo HW, Wu TN, Yang CY. Association of bladder cancer withresidential exposure to petrochemical air pollutant emissions in Taiwan. J ToxicolEnviron Health A 2009;72:53–9.
Viel JF, Daniau C, Goria S, Fabre P, Crouy-Chanel P, Sauleau EA, et al. Risk for nonHodgkin's lymphoma in the vicinity of French municipal solid waste incinerators.Environ Health 2008;7:51.