Embed Size (px)
Citation preview
TESTICULAR TUMORSNILOY SHARMA SHUVO
Faridpur medical college, Bangladesh
Topics
Introduction Etiology Classification Pathophysiology Clinical Feature Investigation Differential Diagnosis Treatment
Introduction
Although rare, is the most common malignancy in men in 15-35 yr age group
Delayed diagnosis Has become one of the most curable
solid tumour Associated with accurate tumour markers Origin in germ cells Capacity to differentiate into histologically
more benign forms Predictable, systematic pattern of spread Occurrence in young individuals
What is Testicular Tumour
Cancer of the testicles, also known as testicular cancer, is one of the less common cancers. It usually affects younger men between the ages of 15 and 49. The most common symptom is a painless lump or swelling in the testicles.
Etiology
The exact cause of most cases of testicular tumour is not known.
Congenital Causes: Cryptorchidism Klinefelter’s syndrome
Age: 20-35 years highest risk group Hormones
Maternal hormone ingestion during pregnancy History of mumps orchitis, inguinal hernia, hydrocele
in childhood - Atrophy High socioeconomic status Testicular cancer contralateral testis HIV positive.
Classification
I. Primary Neoplasma of Testis A.Germ Cell Tumour (90-95%) B.Non-Germ Cell Tumour (5-10%) II. Secondary Neoplasms.
III. Paratesticular Tumours.
PRIMARY NEOPLASMS OF TESTIS
Germinal Neoplasms : (90 - 95 %)
Seminomas - 40% (a) Classic Typical Seminoma (b) Anaplastic Seminoma (c) Spermatocytic Seminoma Teratoma - 25 - 35% (a) Mature (b) Immature Embryonal Carcinoma - 20 - 25% Choriocarcinoma - 1% Yolk Sac Tumour
Nongerminal Neoplasms : ( 5 to 10% )
Specialized gonadal stromal tumor (a) Leydig cell tumor (b) Sertoli’s cell tumour (c) Granulosa cell tumour (b) Other gonadal stromal tumor Gonadoblastoma Miscellaneous Neoplasms (a) Adenocarcinoma of the rete
testis (b) Mesenchymal neoplasms (c) Carcinoid
SEMINOMA Typical : 82-85%
ThirtiesSlow growth
Anaplastic: 5-10%More aggressive, potentially more lethalGreater metastatic potential
Spermatocytic Seminoma: 2-12 %Cells closely resemble different phases of maturing spermatogoniaB/L tumours have been reportedExtremely low metastatic potentialFavourable prognosis
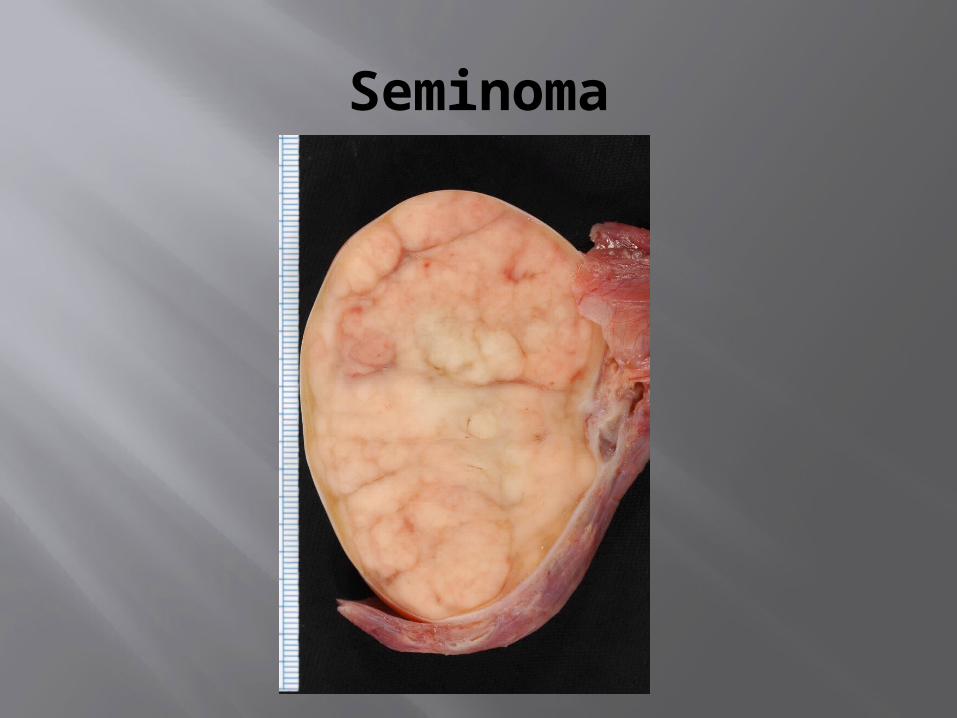
Seminoma
Teratoma
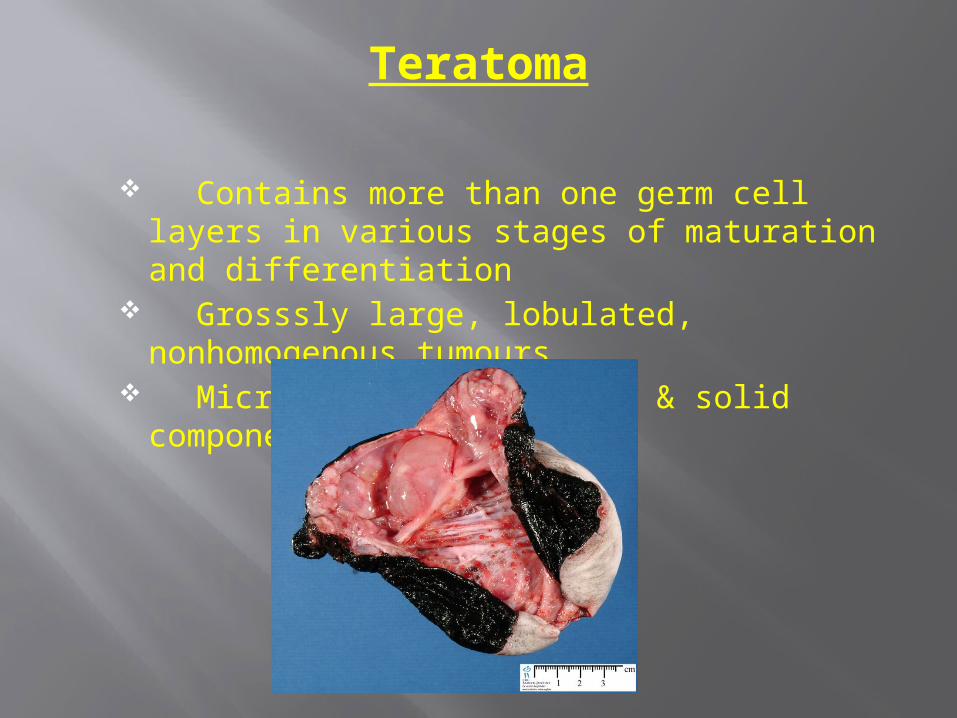
Contains more than one germ cell layers in various stages of maturation and differentiation
Grosssly large, lobulated, nonhomogenous tumours
Microscopically, cystic & solid componenets
Pathophysiology
The malignant transformation of carcinoma in situ is characterised by growth beyond the basement membrane, eventually replacing most of the testicular parenchyma. Spontaneous regression is rare; therefore, any growth of the testis should be regarded as malignant and managed accordingly. The tunica albugenia is a natural barrier to local metastasis so it should not be compromised by direct diagnostic scrotal needle biopsy.
Pathophysiology
Lymphatic spread is the most common cause of metastasis and commonly occurs through spermatic cord lymphatics to the retroperitoneal lymph node chain. One exception is pure choriocarcinoma, which may disseminate more frequently through vascular invasion. On rare occasions a direct communication exists between testicular lymphatics and the thoracic duct, causing a thoracic (sternal) metastasis without retroperitoneal involvement. Scrotal invasion may present with inguinal metastasis. Germ cell cancers may also present with extranodal distant metastasis following direct vascular invasion or tumour embolisation through lymphatico-venous communications. This accounts for most regional treatment failures despite radical orchiectomy and retroperitoneal surgical clearance.
Pathophysiology
Non-seminoma doubling time ranges from 10 to 30 days. This is reflected by alterations in the serum tumour markers. Most treatment failure cases followed by mortality occur within the first 2 to 3 years of diagnosis. Seminoma usually has a much slower doubling time and may recur 2 to 10 years after initial treatment because of its indolent course. Based on the natural history of the disease, curability after multimodality treatment regimens is often declared after 5 years. However, relapse has been reported 10 years after treatment.
CLINICAL FEATURES
Nodule/Painless Swelling of One Gonad Dull Ache or Heaviness in Lower
Abdomen 10% - Acute Scrotal Pain 10% - Present with Metatstasis
- Neck Mass / Cough / Anorexia / Back Ache
5% - Gynecomastia Infertility
Investigation
Ultrasound - Hypoechoic area Chest X-Ray - PA and lateral views CT Scan MRI 4. Tumour Markers - AFP - HCG - LDH - PLAP(placental alkaline
phosphatase)
Staging of testicular tumour
Stage 1-Testis lesion-No spread Stage 2-Nodes below the Diaphragm only Stage 3-Nodes above the diaphragm Stage 4-Pulmonary or Hepatic metastases
Differential Diagnosis
Torsion Epididymitis Epididimo-orchitis Hydrocele Hernia Haematoma Spermatocele Syphilitic gumma
Treatment
Staging is an essential step in planning treatment Blood is collected to enable the levels of tumours
markers (HCG,Alpha fetoprotein and LDH) to be measured. Tumour marker level can be used to monitor the response to treatment.
A chest radiograph shows whether there are pulmonary deposit.
Orchidectomy is essential to remove the primary tumour and to obtain histology
Computerised tomography (CT) and MRI are the most useful means of detecting secondary and for monitoring the response to therapy
Any Question???
Thank yo
u All





![Perinatal Testicular · PDF filePerinatal Testicular TorsionTorsion Audrey C. Durrant, ... departments with acute scrotum. ... Neonatal Testicular Torsion.ppt [Compatibility Mode]](https://img.pdfslide.us/doc/110x75/5a9f7f227f8b9a62178cccbd/perinatal-testicular-testicular-torsiontorsion-audrey-c-durrant-departments.jpg)



![Testicular tumours in children: an approach to diagnosis and … · 2020. 5. 27. · benign tumours are not included [2]. However, our per-sonal experience is that prepubertal-type](https://img.pdfslide.us/doc/110x75/60a9e5eec943202ac316820f/testicular-tumours-in-children-an-approach-to-diagnosis-and-2020-5-27-benign.jpg)







![Isolated Testicular Tuberculosis Mimicking Testicular ... involvement, but testicular involvement is an unusual clinical condition [3]. In this report, a case with isolated testicular](https://img.pdfslide.us/doc/110x75/5f3d57bf74280d66ef795ba2/isolated-testicular-tuberculosis-mimicking-testicular-involvement-but-testicular.jpg)