Embed Size (px)
Citation preview






Morning Report
Anne LachiewiczSeptember 22, 2009

Broncholitis obliterans organizing pneumonia
(BOOP) Cryptogenic organizing pneumonia Inflammatory lung disease Intraluminal organizing fibrosis in distal
airspaces (bronchioles, alveolar ducts, and alveoli)
Reversible fibrosis Dx by lung bx. VAT preferred to
transbronchial bx to obtain sufficient tissue to exclude other diagnoses with overlapping features

Classification of BOOP Idiopathic (most common) Rapidly progressive Focal nodular Postinfection Drug-related (case reports) Rheumatologic or connective tissue related Immunologic disorder Organ transplantation (lung, bone marrow) Radiotherapy (breast cancer) Environmental exposures Miscellaneous

Intra-alveolar stages Fibrinoid inflammatory cell clusters, fibrin
bands with cells (esp. lymphocytes) Fibroinflammatory buds, fibroblasts migrate,
proliferate & develop Mature fibrotic buds: concentric rings of
fibroblasts alternating with layers of connective tissue (mainly collagen bundles, few inflammatory cells (usually in the center of the buds)
Mild interstitial chronic inflammation in alveolar walls with reactive type II cells
Increased foamy macrophages in the alveoli without buds
Histologic features

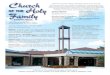
Copyright restrictions may apply.
Epler, G. R. Arch Intern Med 2001;161:158-164.
A, Intraluminal organization and polypoid granulation tissue within a small bronchiole

Preservation of lung architecture Patchy distribution, rarely unilateral Uniform temporal appearance Absence of
interstitial fibrosis granulomas neutrophils or abscesses necrosis hyaline membranes eosinophilic infiltration vasculitis
Features

Males = Females Mean age 50-60 years 2x more in non-smokers/ex-smokers Flu-like illness, malaise, fever Persistent nonproductive cough Progressive mild dyspnea Weight loss of greater than 10 pounds
(57%) Inspiratory rales or focal sparse crackles 25% normal pulmonary exam No clubbing
Clinical presentation

Studies
Labs: 50% leukocytosis, elevated ESR, CRP, no eosinophilia
PFTs: mild-mod restrictive defect, only 20% obstructive (all former smokers)
BAL: Mixed pattern (mild increase in lymphocytes, neutrophils, eosinophils)

Imaging: 3 main patterns of COP
1) Typical – multiple alveolar opacities, usually bilateral, peripheral, and often migratory, may see an air bronchogram
2) Focal – solitary opacity, often upper lobes and may be cavitary, not a characteristic pattern, may have false + FDG-PET uptake
3) Infiltrative – infiltrative opacities associated with interstitial & superimposed small alveolar opacities, may be a polygonal , perilobular pattern

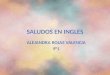
Copyright restrictions may apply.
Epler, G. R. Arch Intern Med 2001;161:158-164.
A, Chest radiograph of a 54-year-old man with a flulike illness, bilateral crackles, decreased vital capacity, and a decreased diffusing capacity that shows bilateral patchy infiltrates in the lower
lungs

Treatment & Prognosis Treatment: corticosteriods, no precise dose or tx duration
established Prednisolone IV bolus, then prednisone 0.75-1.5mg/kg/day then
taper, tx for 24 wks to 1 yr Reports of spontaneous improvement or response to abx,
especially macrolides
Prognosis: excellent without sequelae (65-80% cured with steriods)
Relapse is common (13-58%) but not associated with increased mortality or long-term functional morbidity
Pts may risk relapse rather than taking high-dose steriods for a year
Solitary pattern usually does not relapse after surgical excision

References
Cordier, J-F. Cryptogenic organizing pneumonia. Eur Respir J. 2006;26:422-446.
Epler, GR. Bronchiolitis obliterans organizing pneumonia. Arch Inten Med. 2001;161:158-164.
King, TE. Cryptogenic organizing pneumonia. In: UpToDate, Basow, DS (Ed), UpToDate, Waltham, MA, 2009.