Embed Size (px)
Citation preview

Opportuni)es and Challenges in Drug Discovery for Au)sm Spectrum Disorders
Lawrence W Fitzgerald, PhD, MBA 03/03/15
1
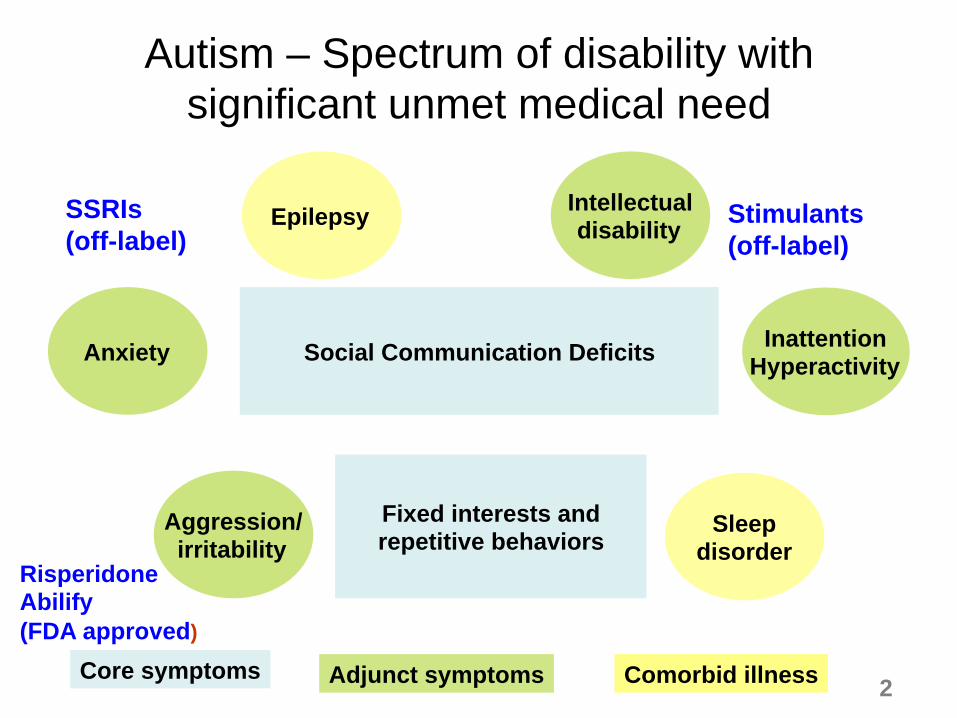
Autism – Spectrum of disability with significant unmet medical need
Social Communication Deficits
Fixed interests and repetitive behaviors
Aggression/ irritability
Anxiety
Intellectual disability
Inattention Hyperactivity
Epilepsy
Sleep disorder
Core symptoms Adjunct symptoms Comorbid illness
Risperidone Abilify (FDA approved)
SSRIs (off-label)
Stimulants (off-label)
2
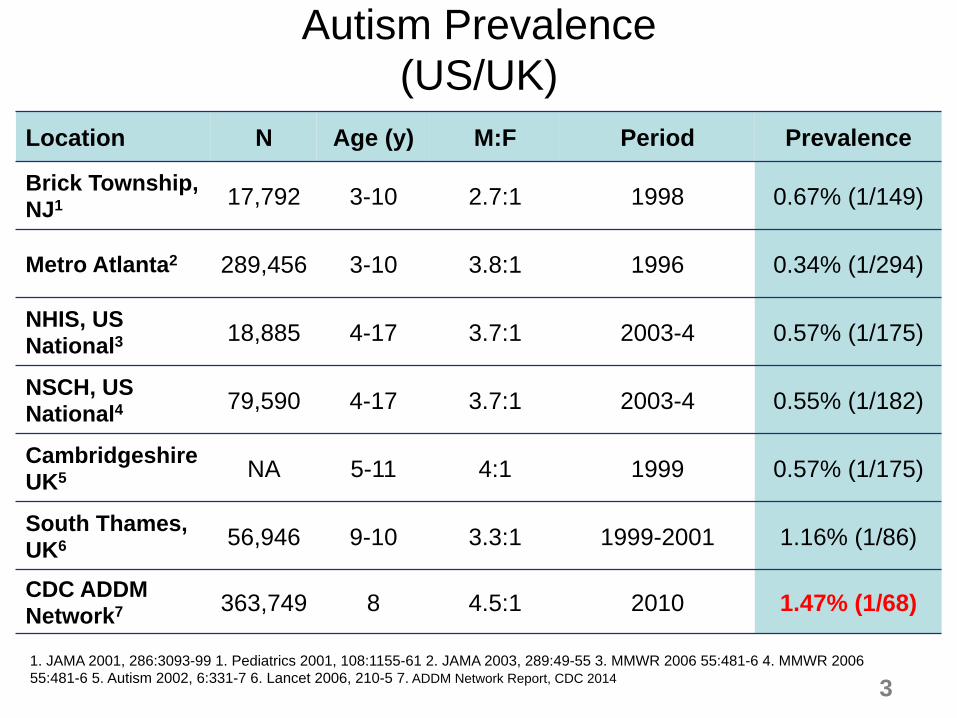
Location N Age (y) M:F Period Prevalence
Brick Township, NJ1 17,792 3-10 2.7:1 1998 0.67% (1/149)
Metro Atlanta2 289,456 3-10 3.8:1 1996 0.34% (1/294)
NHIS, US National3 18,885 4-17 3.7:1 2003-4 0.57% (1/175)
NSCH, US National4 79,590 4-17 3.7:1 2003-4 0.55% (1/182)
CambridgeshireUK5 NA 5-11 4:1 1999 0.57% (1/175)
South Thames, UK6 56,946 9-10 3.3:1 1999-2001 1.16% (1/86)
CDC ADDM Network7 363,749 8 4.5:1 2010 1.47% (1/68)
1. JAMA 2001, 286:3093-99 1. Pediatrics 2001, 108:1155-61 2. JAMA 2003, 289:49-55 3. MMWR 2006 55:481-6 4. MMWR 2006 55:481-6 5. Autism 2002, 6:331-7 6. Lancet 2006, 210-5 7. ADDM Network Report, CDC 2014
Autism Prevalence (US/UK)
3
Autism prevalence – why the trending?
§ Estimates regarding the prevalence of autism (and later ASD) have increased exponentially – For decades, the prevalence was thought to be 4 to 5 cases per
10,000 children in the US
– In a 2014 report, CDC network study (covering 2010) resulted in a revised estimate of approximately 1 child in every 68 in the US will have an ASD
– Approximately 50% will have significant to borderline intellectual disability where as 50% will have average to above average IQ
§ Increased prevalence is likely driven by publicity, reduction in stigma, broadening/defining diagnosis (e.g., ID→ASD), public services
4
ASD Genetics
§ Autism is among the most heritable of all neuropsychiatric disorders…some of genetic changes are spontaneous!
§ Concordance rates – 82-92% for monozygotic twins; 1-10% for dizygotic twins
§ Multiple underlying genes – complex disorder, phenotypic variability
– chromosomal abnormalities
– CNVs - copy number changes (duplication/deletions; e.g., 15q11, 22q13),
– rare single gene mutations - Monogenic syndromic ASDs (FXS, Rett, Angelmans, TSC) and others (Shank3, Pten)
5
Life time costs of autism
6
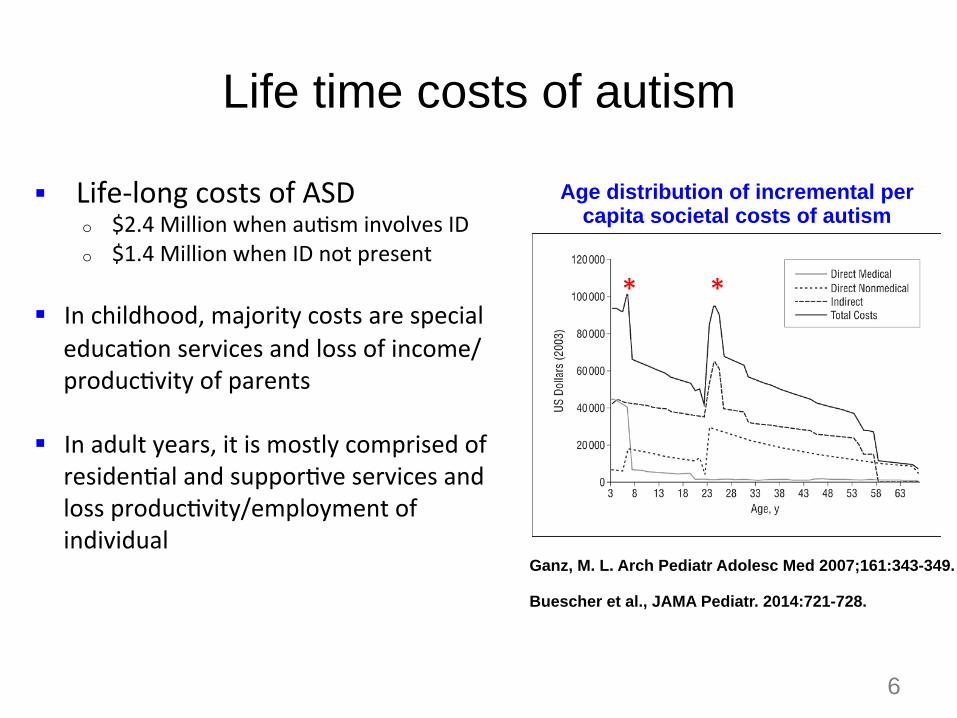
Ganz, M. L. Arch Pediatr Adolesc Med 2007;161:343-349. Buescher et al., JAMA Pediatr. 2014:721-728.
Age distribution of incremental per capita societal costs of autism
* *
§ Life-‐long costs of ASD o $2.4 Million when au)sm involves ID o $1.4 Million when ID not present
§ In childhood, majority costs are special educa)on services and loss of income/produc)vity of parents
§ In adult years, it is mostly comprised of residen)al and suppor)ve services and loss produc)vity/employment of individual
7
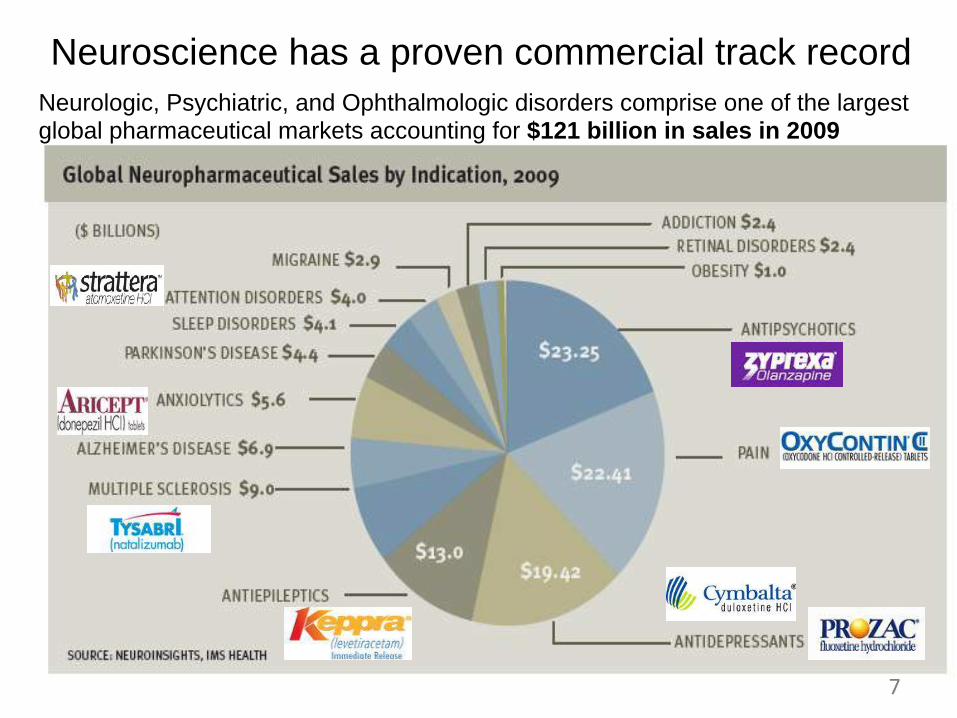
Neurologic, Psychiatric, and Ophthalmologic disorders comprise one of the largest global pharmaceutical markets accounting for $121 billion in sales in 2009
7
Neuroscience has a proven commercial track record
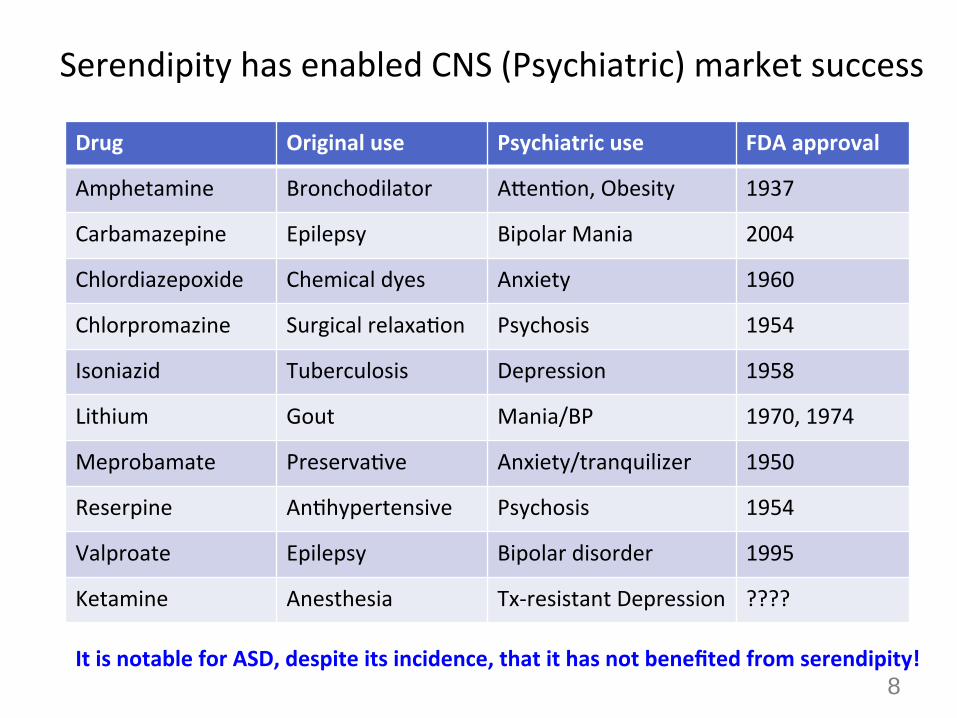
Serendipity has enabled CNS (Psychiatric) market success
Drug Original use Psychiatric use FDA approval
Amphetamine Bronchodilator AQen)on, Obesity 1937
Carbamazepine Epilepsy Bipolar Mania 2004
Chlordiazepoxide Chemical dyes Anxiety 1960
Chlorpromazine Surgical relaxa)on Psychosis 1954
Isoniazid Tuberculosis Depression 1958
Lithium Gout Mania/BP 1970, 1974
Meprobamate Preserva)ve Anxiety/tranquilizer 1950
Reserpine An)hypertensive Psychosis 1954
Valproate Epilepsy Bipolar disorder 1995
Ketamine Anesthesia Tx-‐resistant Depression ????
It is notable for ASD, despite its incidence, that it has not benefited from serendipity! 8
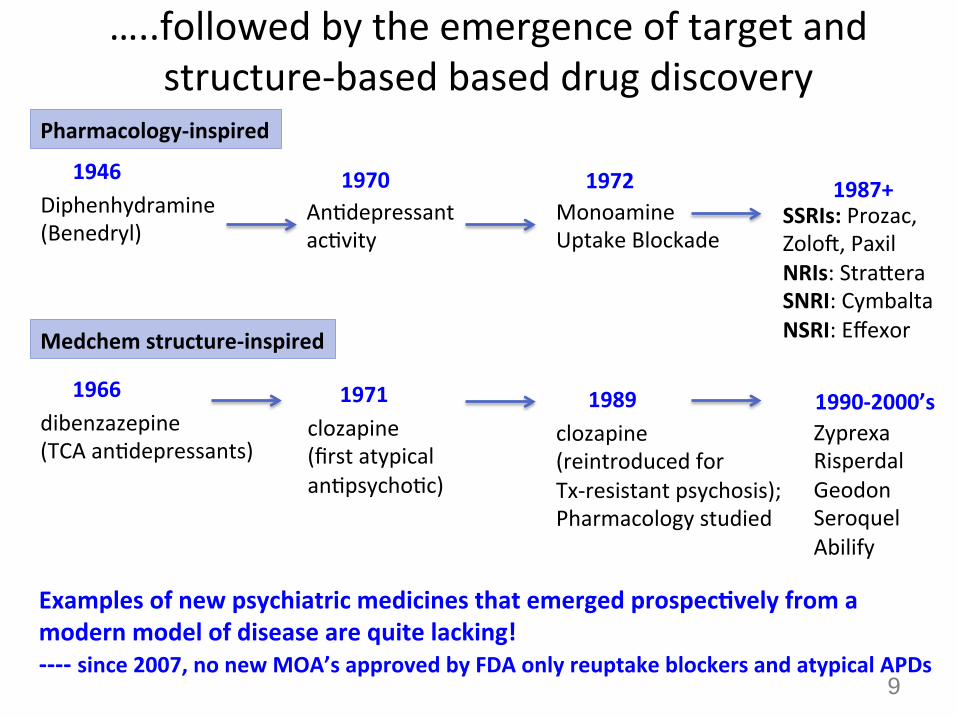
…..followed by the emergence of target and structure-‐based based drug discovery
Diphenhydramine (Benedryl)
An)depressant ac)vity
Monoamine Uptake Blockade
SSRIs: Prozac, Zoloe, Paxil NRIs: StraQera SNRI: Cymbalta NSRI: Effexor
1946 1970 1972 1987+
dibenzazepine (TCA an)depressants)
1966
clozapine (first atypical an)psycho)c)
1971
clozapine (reintroduced for Tx-‐resistant psychosis); Pharmacology studied
1989 Zyprexa Risperdal Geodon Seroquel Abilify
1990-‐2000’s
Pharmacology-‐inspired
Examples of new psychiatric medicines that emerged prospecQvely from a modern model of disease are quite lacking! -‐-‐-‐-‐ since 2007, no new MOA’s approved by FDA only reuptake blockers and atypical APDs
9
Medchem structure-‐inspired
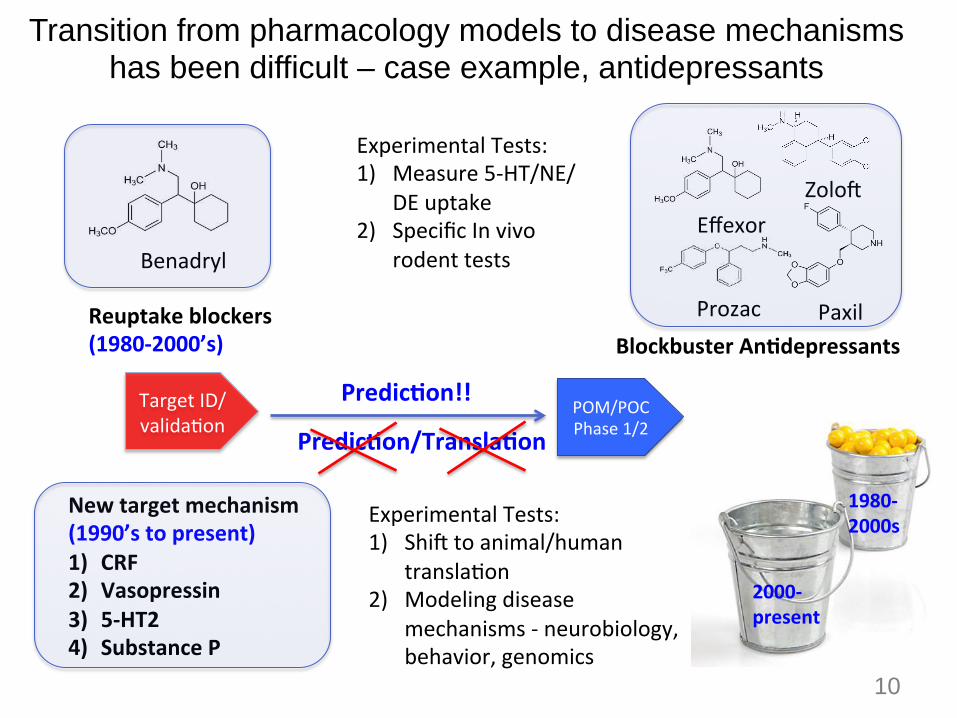
Transition from pharmacology models to disease mechanisms has been difficult – case example, antidepressants
10
Target ID/valida)on
POM/POC Phase 1/2
PredicQon!!
Benadryl
Prozac
Effexor Zoloe
Paxil
Experimental Tests: 1) Measure 5-‐HT/NE/
DE uptake 2) Specific In vivo
rodent tests
Reuptake blockers (1980-‐2000’s) Blockbuster AnQdepressants
PredicQon/TranslaQon
New target mechanism (1990’s to present) 1) CRF 2) Vasopressin 3) 5-‐HT2 4) Substance P
Experimental Tests: 1) Shie to animal/human
transla)on 2) Modeling disease
mechanisms -‐ neurobiology, behavior, genomics
1980-‐2000s
2000-‐present
10
11
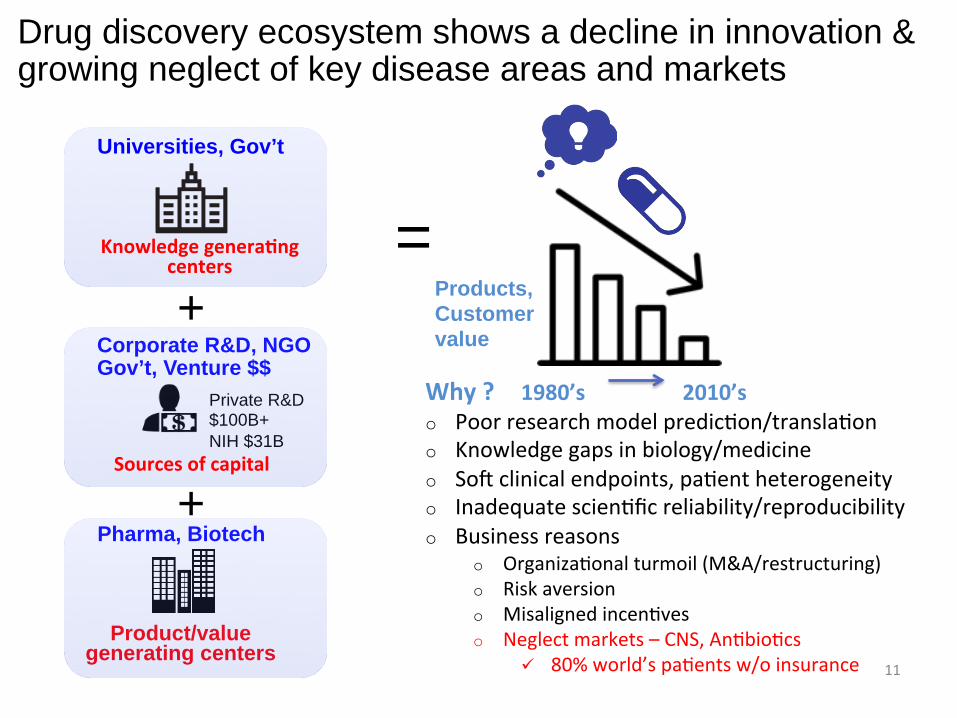
Universities, Gov’t
Knowledge generaQng centers
Private R&D $100B+ NIH $31B
Corporate R&D, NGO Gov’t, Venture $$
Sources of capital
Product/value generating centers
Pharma, Biotech
+
+
=
Drug discovery ecosystem shows a decline in innovation & growing neglect of key disease areas and markets
Why ? 1980’s 2010’s o Poor research model predic)on/transla)on o Knowledge gaps in biology/medicine o Soe clinical endpoints, pa)ent heterogeneity o Inadequate scien)fic reliability/reproducibility o Business reasons
o Organiza)onal turmoil (M&A/restructuring) o Risk aversion o Misaligned incen)ves o Neglect markets – CNS, An)bio)cs
ü 80% world’s pa)ents w/o insurance
Products, Customer value
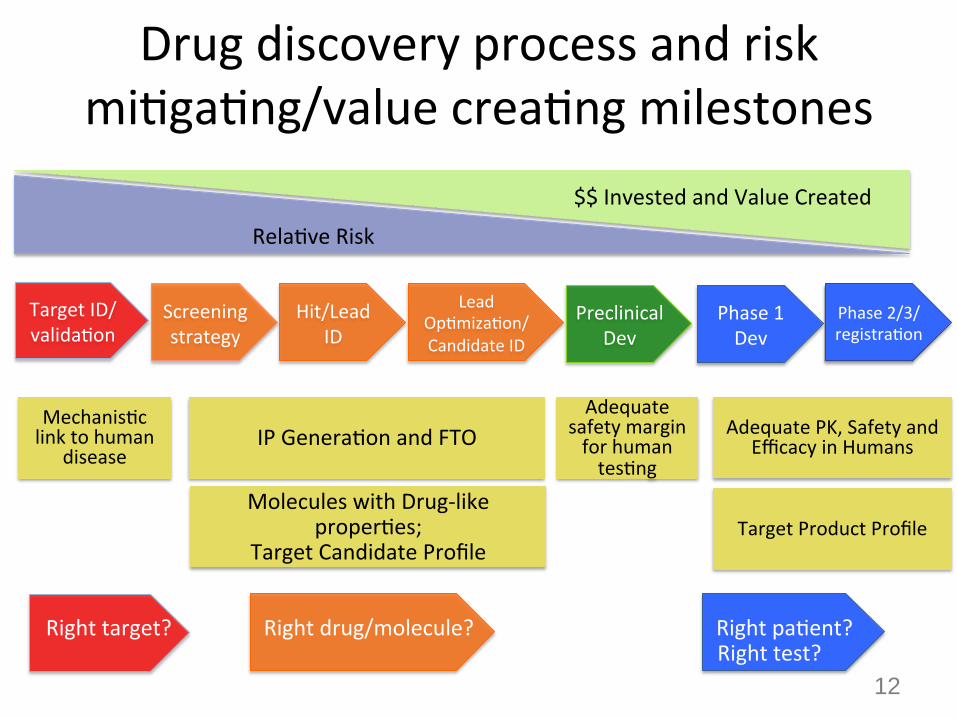
Drug discovery process and risk mi)ga)ng/value crea)ng milestones
Screening strategy
Hit/Lead ID
Lead Op)miza)on/Candidate ID
Target ID/valida)on
Preclinical Dev
Phase 1 Dev
Rela)ve Risk
$$ Invested and Value Created
Phase 2/3/registra)on
Mechanis)c link to human
disease IP Genera)on and FTO
Molecules with Drug-‐like proper)es;
Target Candidate Profile
Adequate safety margin for human tes)ng
Adequate PK, Safety and Efficacy in Humans
Target Product Profile
12
Right target? Right drug/molecule? Right pa)ent? Right test?
Bridging the knowledge gap – is it Au)sm’s )me?
13
R&D strategic opportunities • Tx of adjunct/comorbid illness (e.g., irritability, ID, ADHD, sleep, mood)
– Ideal candidates do not exacerbate core symptoms – Consider combining w behavioral interven)ons to show benefits – Upside: “winning with low hanging fruit”, Downside: low commercial appeal/no
differenQated benefit
• Anchor to rare molecular variant, sequenQally expand to other mechanisQcally convergent (similar) disease segments – U)lize genomics, systems and mechanis)c biology, translatable biomarkers, pa)ents
stra)fica)on strategies. Examples, prolifera)ve pathways, I/E balance, protein synthesis – Upside: “Targeted medicine, strong mechanisQc link to eQology of disease; Downside:
Efficacy limited to rare and narrow segment, potenQally expensive drugs
• UQlized systems biology/neurochemical/behavioral approach to tx symptoms – Modulators of specific neural circuits that underlie symptoms domains (e.g., OT) – U)lize gene)c models and natural rodent strains with symptoms that pass face validity – Upside: “broader appeal”, tx diverse forms of ASD” Downside: there is no magic bullet
14
Confiden)al | Copyright 2011 SAGE Therapeu)cs 15
Pfizer Internal Use
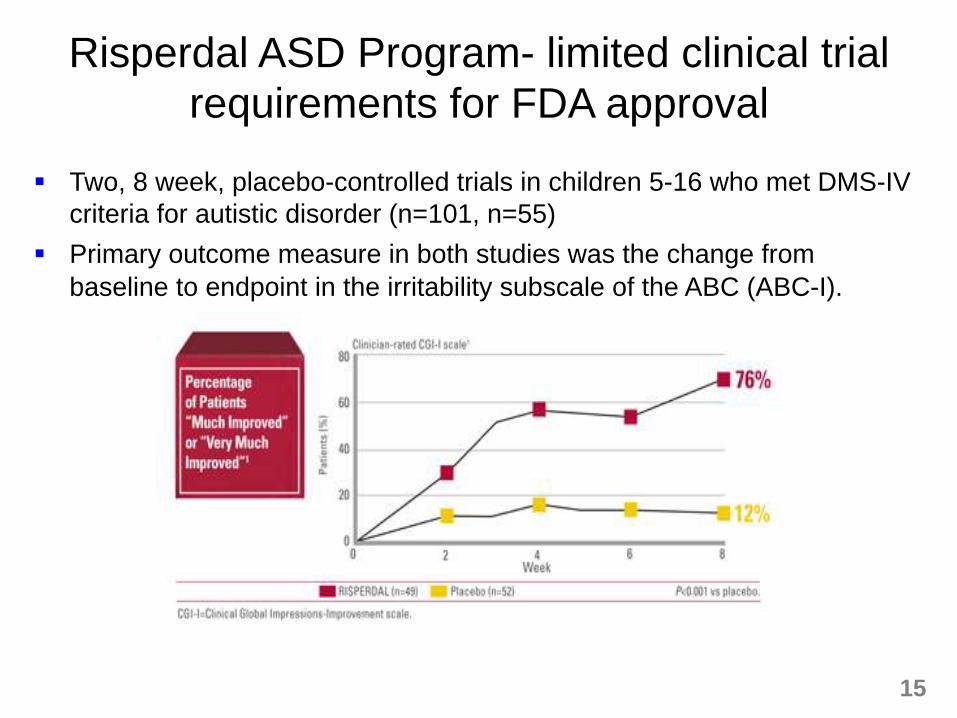
Risperdal ASD Program- limited clinical trial requirements for FDA approval
§ Two, 8 week, placebo-controlled trials in children 5-16 who met DMS-IV criteria for autistic disorder (n=101, n=55)
§ Primary outcome measure in both studies was the change from baseline to endpoint in the irritability subscale of the ABC (ABC-I).
15
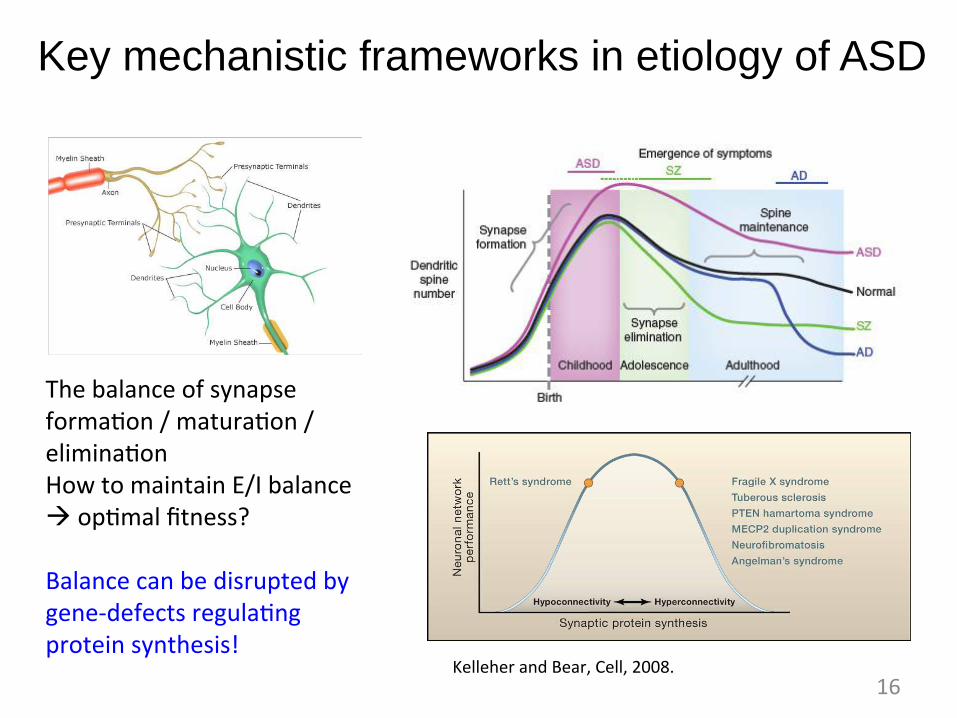
Key mechanistic frameworks in etiology of ASD
16
The balance of synapse forma)on / matura)on / elimina)on How to maintain E/I balance à op)mal fitness? Balance can be disrupted by gene-‐defects regula)ng protein synthesis!
Kelleher and Bear, Cell, 2008.
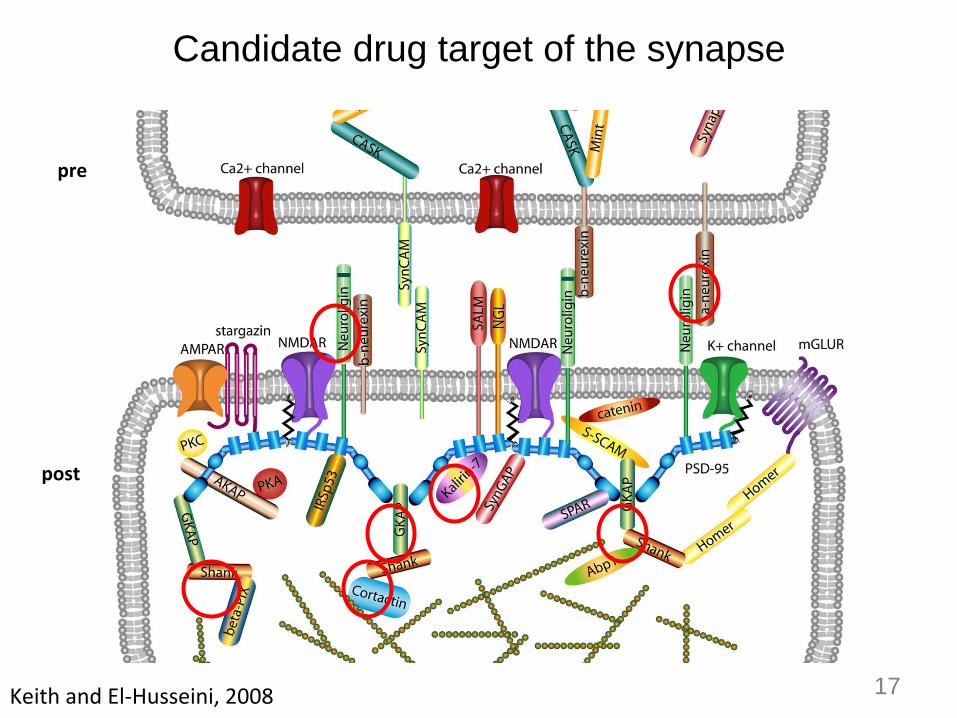
Candidate drug target of the synapse
pre
post
Keith and El-‐Husseini, 2008 17
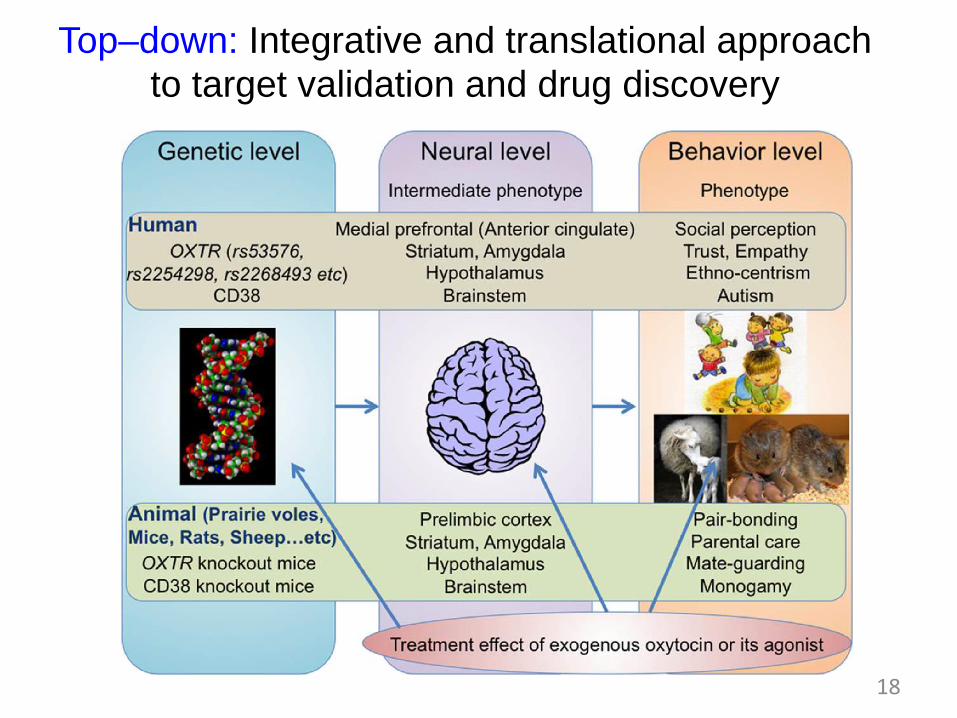
Top–down: Integrative and translational approach to target validation and drug discovery
18
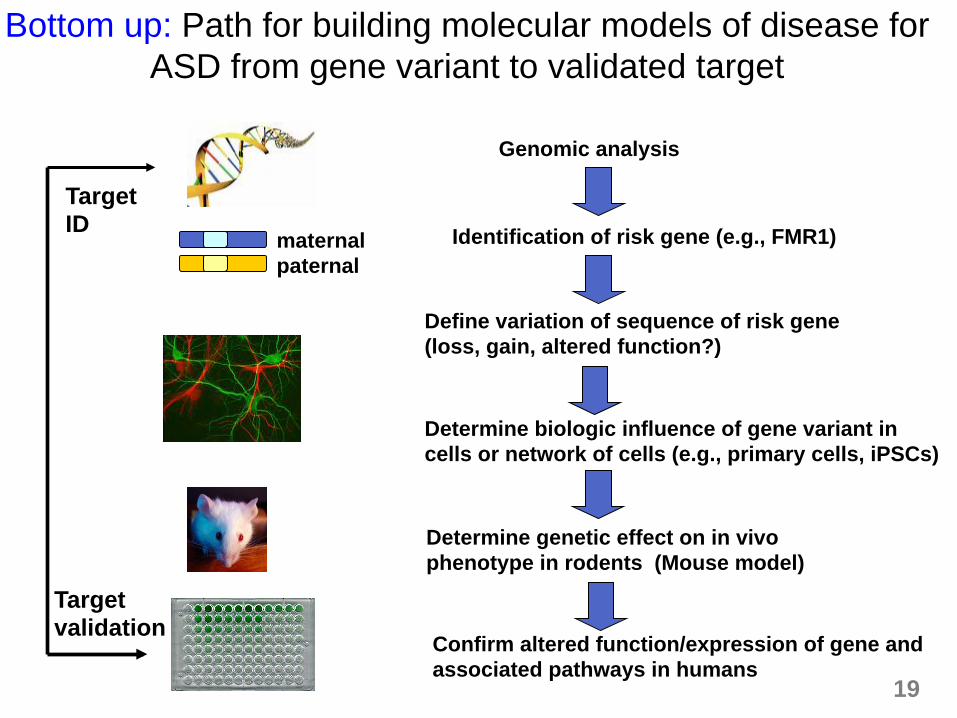
Genomic analysis
Identification of risk gene (e.g., FMR1)
Define variation of sequence of risk gene (loss, gain, altered function?)
Determine biologic influence of gene variant in cells or network of cells (e.g., primary cells, iPSCs)
Determine genetic effect on in vivo phenotype in rodents (Mouse model)
Confirm altered function/expression of gene and associated pathways in humans
maternal paternal
Target ID
Target validation
Bottom up: Path for building molecular models of disease for ASD from gene variant to validated target
19
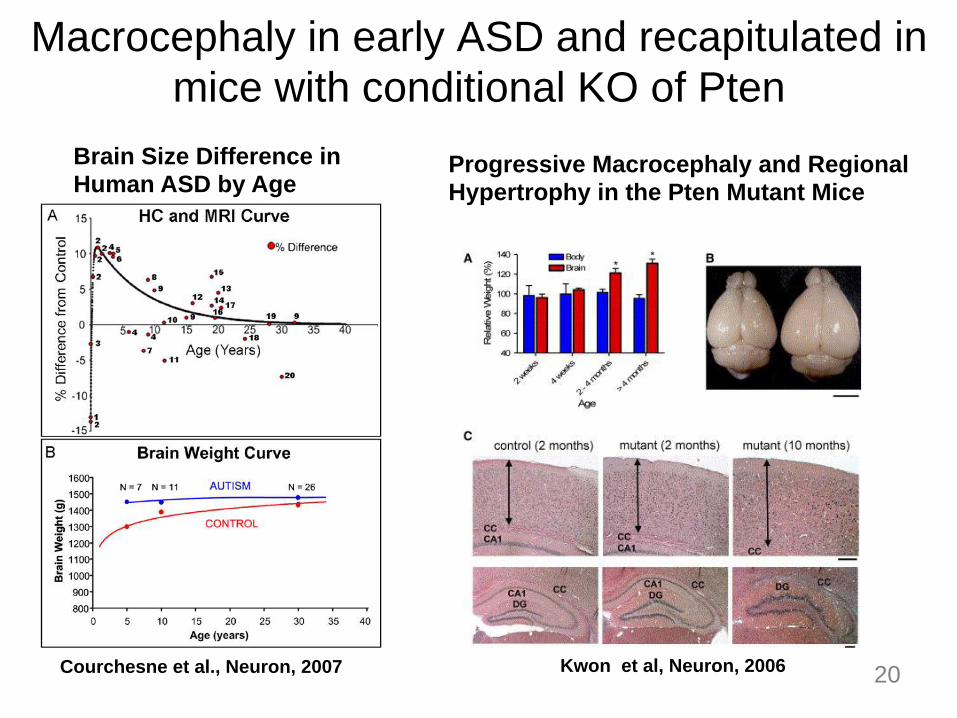
Macrocephaly in early ASD and recapitulated in mice with conditional KO of Pten
Brain Size Difference in Human ASD by Age
Progressive Macrocephaly and Regional Hypertrophy in the Pten Mutant Mice
Courchesne et al., Neuron, 2007 Kwon et al, Neuron, 2006 20
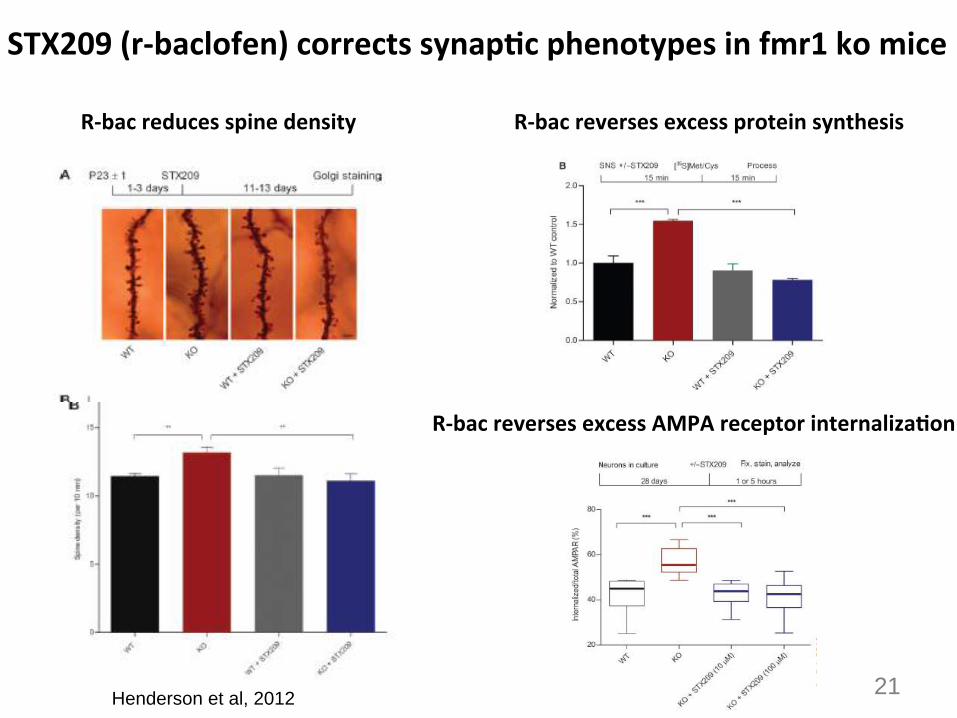
STX209 (r-‐baclofen) corrects synapQc phenotypes in fmr1 ko mice
21 Henderson et al, 2012
R-‐bac reduces spine density R-‐bac reverses excess protein synthesis
R-‐bac reverses excess AMPA receptor internalizaQon
22
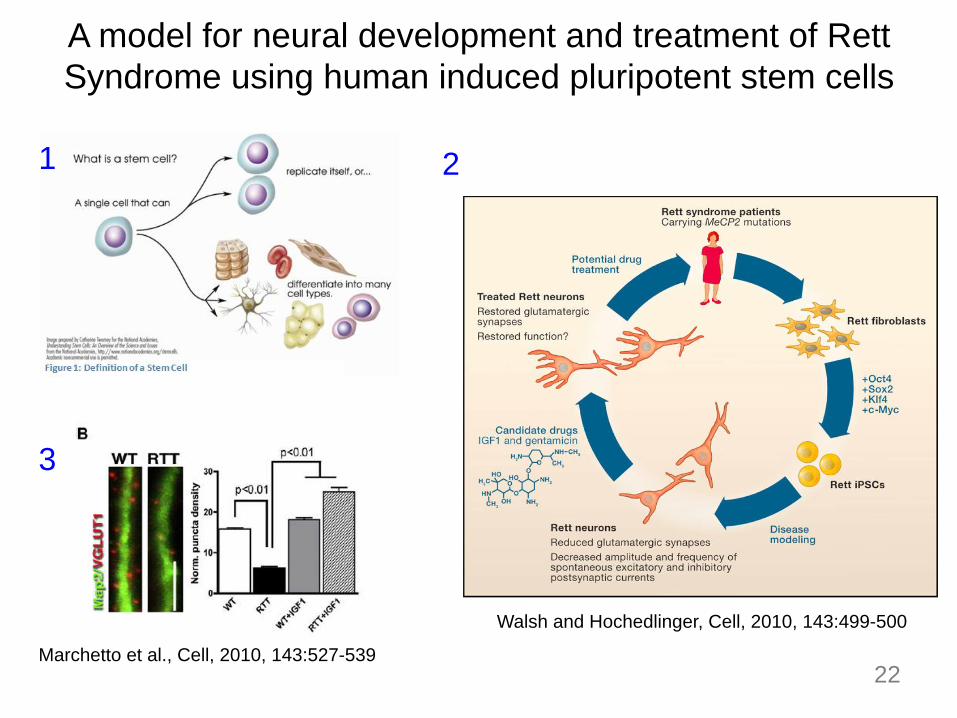
Walsh and Hochedlinger, Cell, 2010, 143:499-500
Marchetto et al., Cell, 2010, 143:527-539
A model for neural development and treatment of Rett Syndrome using human induced pluripotent stem cells
1 2
3
FMR1
pten
Shank3
TSC1/2
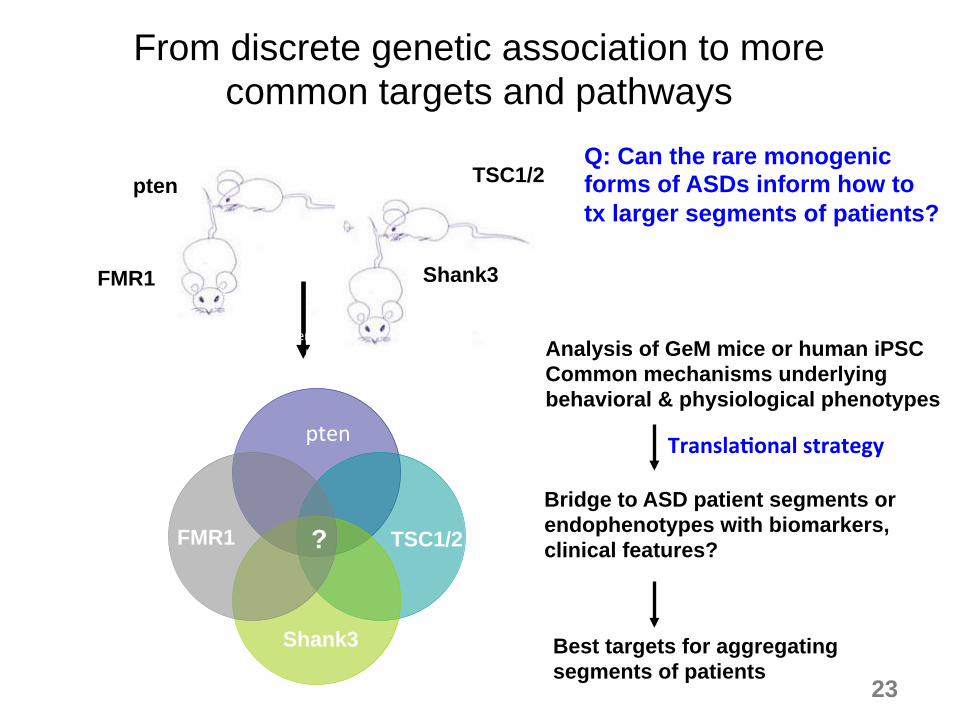
Analysis of GeM mice or human iPSC Common mechanisms underlying behavioral & physiological phenotypes
Bridge to ASD patient segments or endophenotypes with biomarkers, clinical features?
Best targets for aggregating segments of patients
From discrete genetic association to more common targets and pathways
Q: Can the rare monogenic forms of ASDs inform how to tx larger segments of patients?
23
pen pen
NRL4 FMR1 TSC1/2 FMR1 ?
pten
Shank3
TranslaQonal strategy
Category and utility of biomarkers Biomarker is a laboratory measurement or physiological sign in association with a physiological process of therapeutic or diagnostic value
§ Target biomarker – measures physical or biological interaction with the molecular target (PET ligand demonstration of receptor occupancy, measurement of enzyme inhibition); o benefits: PK/PD (dose selection), demonstrate target engagement o PET ligand, e.g., mGlur5 NAM; CSF levels of drug
§ Mechanistic biomarker – measures a biological effect presumed to be downstream of molecular target
o benefits: like target + target-mediated activity,
o may be change in physiological (blood flow), biochemical (substrate turnover), behavioural (reaction time), genetic (gene expression) or proteomic (composition of protein in tissues/biofluids).
o qEEG, CSF/plasma markers § Outcome/surrogate marker – impact on pathophysiology that links to clinical
efficacy. Opportunity for patient segmentation, predict long-term efficacy o protein synthesis (11C-leucine PET), ERP –EEG, fMRI/DTI, eye gazing etc.
24
25
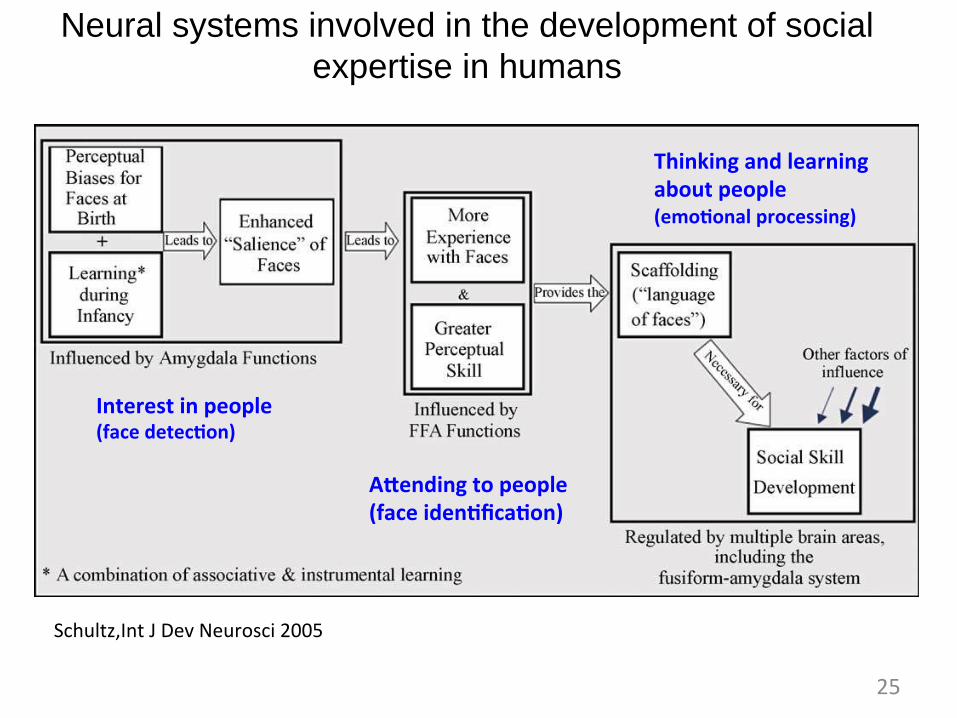
Schultz,Int J Dev Neurosci 2005
Interest in people (face detecQon)
Alending to people (face idenQficaQon)
Thinking and learning about people (emoQonal processing)
Neural systems involved in the development of social expertise in humans
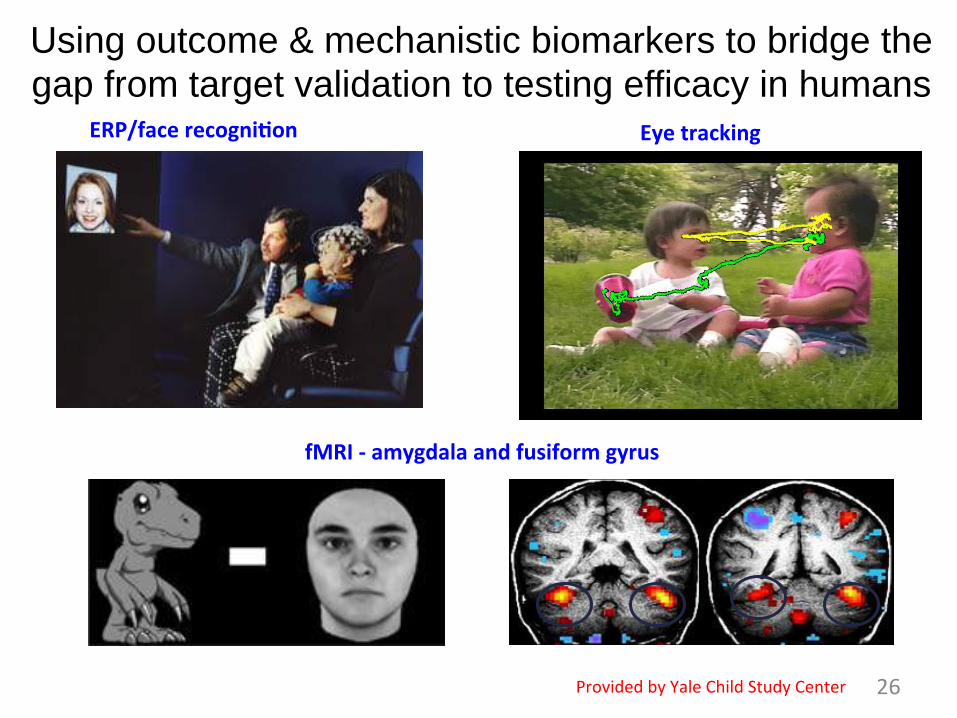
26
ERP/face recogniQon Eye tracking
fMRI -‐ amygdala and fusiform gyrus
Provided by Yale Child Study Center
Using outcome & mechanistic biomarkers to bridge the gap from target validation to testing efficacy in humans
27
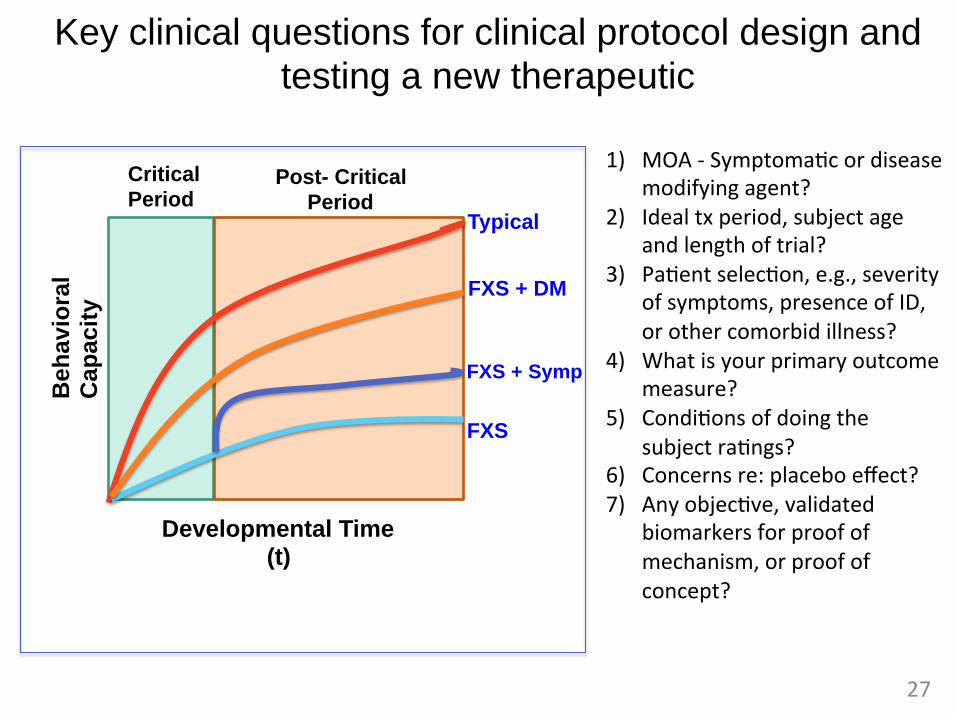
Key clinical questions for clinical protocol design and testing a new therapeutic
March 5, 2015 Confiden)al | Copyright 2011 SAGE Therapeu)cs 27
Developmental Time (t)
Beh
avio
ral
Cap
acit
y
Typical
FXS
FXS + DM
FXS + Symp
Critical Period
Post- Critical Period
1) MOA -‐ Symptoma)c or disease modifying agent?
2) Ideal tx period, subject age and length of trial?
3) Pa)ent selec)on, e.g., severity of symptoms, presence of ID, or other comorbid illness?
4) What is your primary outcome measure?
5) Condi)ons of doing the subject ra)ngs?
6) Concerns re: placebo effect? 7) Any objec)ve, validated
biomarkers for proof of mechanism, or proof of concept?
28
Validation of ABC-C for Fragile X
ORIGINAL PAPER
Psychometric Study of the Aberrant Behavior Checklist in FragileX Syndrome and Implications for Targeted Treatment
Stephanie M. Sansone • Keith F. Widaman • Scott S. Hall • Allan L. Reiss •
Amy Lightbody • Walter E. Kaufmann • Elizabeth Berry-Kravis •
Ave Lachiewicz • Elaine C. Brown • David Hessl
Published online: 5 October 2011! Springer Science+Business Media, LLC 2011
Abstract Animal studies elucidating the neurobiology offragile X syndrome (FXS) have led to multiple controlled
trials in humans, with the Aberrant Behavior Checklist-
Community (ABC-C) commonly adopted as a primaryoutcome measure. A multi-site collaboration examined the
psychometric properties of the ABC-C in 630 individuals
(ages 3–25) with FXS using exploratory and confirmatoryfactor analysis. Results support a six-factor structure, with
one factor unchanged (Inappropriate Speech), four modi-
fied (Irritability, Hyperactivity, Lethargy/Withdrawal, andStereotypy), and a new Social Avoidance factor. A com-
parison with ABC-C data from individuals with general
intellectual disability and a list of commonly endorseditems are also reported. Reformulated ABC-C scores based
on this FXS-specific factor structure may provide added
outcome measure specificity and sensitivity in FXS clinicaltrials.
Keywords FMR1 gene ! Fragile X syndrome ! Autism !Factor analysis ! Rating scale ! Social avoidance
Fragile X syndrome (FXS) is the leading known cause of
both inherited intellectual disability (ID) and autism, andrecent estimates of the frequency of the full-mutation are as
high as one in every 2,500 births (Hagerman 2008). FXS is
caused by the expansion of a trinucleotide repeat sequence,cytosine-guanine-guanine (CGG), in the promoter region
of the Fragile X Mental Retardation 1 gene (FMR1) on the
long arm of the X chromosome at Xq27.3. Expansions
A portion of the data was presented at the 44th Annual GatlinburgConference, San Antonio, TX, in March 2010.
Electronic supplementary material The online version of thisarticle (doi:10.1007/s10803-011-1370-2) contains supplementarymaterial, which is available to authorized users.
S. M. Sansone ! D. Hessl (&)Medical Investigation of Neurodevelopmental Disorders(MIND) Institute, University of California Davis MedicalCenter, 2825 50th Street, Sacramento, CA 95817, USAe-mail: [email protected]
K. F. WidamanDepartment of Psychology, University of California, Davis,One Shields Avenue, Davis, CA, USA
S. S. Hall ! A. L. Reiss ! A. LightbodyDepartment of Psychiatry and Behavioral Sciences, Center forInterdisciplinary Brain Sciences Research, Stanford University,401 Quarry Road, Stanford, CA, USA
W. E. KaufmannCenter for Genetic Disorders of Cognition and Behavior,Kennedy Krieger Institute, Johns Hopkins University Schoolof Medicine, Baltimore, MD, USA
E. Berry-KravisDepartments of Pediatrics, Neurological Sciences, Biochemistry,Rush University Medical Center, Chicago, IL, USA
A. LachiewiczDepartments of Pediatrics and Psychiatry and BehavioralSciences, Duke University Medical Center, Durham, NC, USA
A. Lachiewicz ! E. C. BrownPrivate Practice, Reno, NV, USA
D. HesslDepartment of Psychiatry and Behavioral Sciences,University of California, Davis, School of Medicine,Sacramento, CA, USA
123
J Autism Dev Disord (2012) 42:1377–1392
DOI 10.1007/s10803-011-1370-2
• ABC-C scale originally validated in the MR/ID population • Multi-site collaboration examined the psychometric properties for ABC in 630 individuals with FXS, ages 3-25 yrs • Results supported a 6 factor scale structure with one unchanged (inappropriate speech), 4 modified scales (Irritability, Hyperactivity, Lethargy/withdrawal, Stereotypy), and the additional of one new factor, Social Avoidance • The new reformulated ABC-C scores based on FXS-specific factor structure may provide outcome measure specificity and sensitivity for FXS clinical trials
Confiden)al | Copyright 2011 SAGE Therapeu)cs 29
tant physiological role (23), is the main structure of reward expectationand placebo response (24).
Here, methylation of the FMR1 promoter in whole blood was as-sessed with an MSP assay of bisulfite-treated DNA and sequencing ofbisulfite-treated DNA clones. The sensitivity of these techniques is highcompared with the standard methylation-specific Southern blot. Thisdifference in techniquesmay explain the relatively high observed occur-rence of partial FMR1 promoter methylation in a population in whichall of the patients carry the fullmutation. In addition, we cannot excludeascertainment bias toward higher-functioning patients, and thus alsotoward individuals with partial FMR1 promoter methylation, giventhe rigorous study schedule and the procedures involved. The detectionof partial methylation at the FMR1 promoter may suggest the presenceof a mosaic of premutation (between 55 and 200 CGG repeats withoutmethylation at the FMR1 promoter and usually few to no symptoms ofFXS) and full-mutation (more than 200 CGG repeats) alleles. Becauselarge premutations (100 to 200 CGG repeats) have been associated withabove-normal levels ofFMR1mRNA,but reducedFMRP(21), thenormallevels of FMR1 mRNA detected in two patients could be explained by amosaic of premutation and full-mutation alleles. Partial FMR1 promotermethylation could also be explained by distinct FMR1 promoter meth-ylation status in different tissues after somatic expansion of the CGGrepeats in the early stages of embryonic development. Investigation intothe tissue-specific pattern ofFMR1 promotermethylation and expressionmay shedmore light on the functional consequences of FMR1 dysregula-tion on disease phenotypes and drug response and may offer additionalopportunities for discovering other indicators of treatment response.
AFQ056 was reasonably well tolerated in this population, with allpatients completing the up-titration, reaching the target dosage, andcompleting the AFQ056 period of treatment. Adverse events were re-ported by 80%of the patients in the study,with these eventsmainlymildor moderate in severity, andmost commonly fatigue and headache. Fa-tigue was reported in both AFQ056 and placebo treatment groups,whereas headachewas only reported dur-ing AFQ056 treatment. Only one patientexperienced a serious adverse event, andbecause this occurred while he was in theplacebo treatment period, the event wasnot suspected to be related to the studydrug.
This study was designed to investigatethe effects of AFQ056 treatment on aber-rant behaviors in patients with FXS andthe safety and tolerability of this drug inthis population. A two-treatment, two-period, crossover design was used to al-low intraindividual comparisons andhencereduce the number of patients required toachieve satisfactory statistical power. To re-duce interpatient variability, we recruitedonly men with the full FXS mutation tothe study. These men were aged between18 and 35 years, because AFQ056 pharma-cokinetic data are only available for adultsand because there are few available data onFXS patients older than 35 years. The treat-ment regimen in this study used AFQ056doses shown to have an acceptable safety
and tolerability profile in healthy subjects. Because this was the firstexperience of AFQ056 in patients with FXS, a slow titration dosingregimen was used. Because AFQ056 plasma concentrations were ex-pected to reach a steady state within 3 to 4 days, 4-day intervals betweendose escalations were considered sufficient to assess the safety and tol-erability of each dose. The 28-day treatment periods were chosen on thebasis of the available AFQ056 toxicology data, and the 1-week washoutperiod was considered sufficient to avoid carryover effects becausecomplete elimination of AFQ056 was expected after ~3.5 days.
This study is limited by the small sample size of 30 patients, thecrossover design, and the short time scale. This is particularly relevantfor the exploratory analysis comparing patients with full and partialFMR1 promoter methylation, where only a small number of patientswith full FMR1 promoter methylation were shown to respond signifi-cantly to AFQ056 treatment. The levels of FMR1mRNAwere assessed,but assessment of the levels of FMRP in each patient may have aidedanalysis of the results. It seems likely that patientswith fullmethylation atthe FMR1 promoter and no detectable FMR1 mRNA do not expressFMRP, but knowing the levels of FMRP expression in patientswith partialFMR1 promoter methylation may have helped explain the variable treat-ment response in these patients. Larger, longer-term, prospective trials arerequired to confirm the findings of this study, to test the long-termefficacyof AFQ056 on behavior, and to study any effects on the cognitive deficitsassociated with FXS. If these results are positive, then future studies will beneeded to test safety and efficacy in childrenwithFXS, because the greatestbenefits from mGluR5 inhibition may be derived during development.
We have shown that the selective inhibition of mGluR5 by AFQ056can provide a significant effect on behavioral problems in a subpop-ulation of patients with FXS. If confirmed in future studies, these resultssuggest that AFQ056 may provide valuable improvement in behavioralsymptoms of FXS and that this improvement is predicted by full meth-ylation at the FMR1 promoter. Why subjects lacking FMR1 expressionare better responders to the AFQ056 treatment remains an open ques-
60
A
40
20
0
Chan
ge fr
om b
asel
ine
to d
ay 1
9/20
on
ABC
–C
–20
–40
–60
60
B
40
20
0
–20
–40
–60Placebo AFQ056 Placebo AFQ056
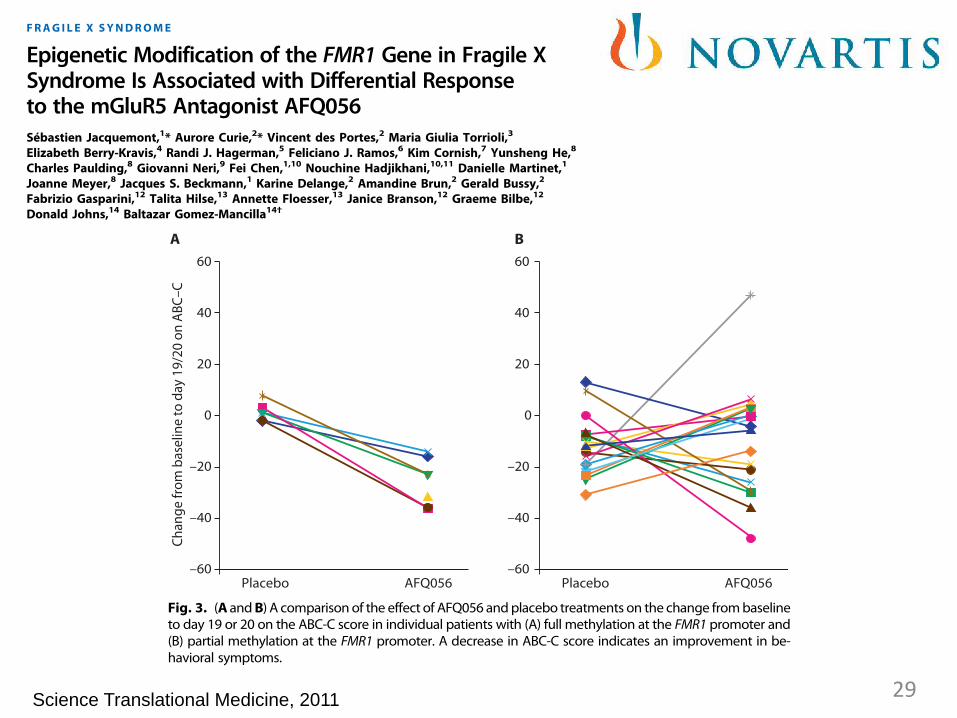
Fig. 3. (A andB) A comparison of the effect of AFQ056 andplacebo treatments on the change frombaselineto day 19 or 20 on the ABC-C score in individual patients with (A) full methylation at the FMR1 promoter and(B) partial methylation at the FMR1 promoter. A decrease in ABC-C score indicates an improvement in be-havioral symptoms.
R E S EARCH ART I C L E
www.ScienceTranslationalMedicine.org 5 January 2011 Vol 3 Issue 64 64ra1 6
on
Sep
tem
ber
14, 2
012
stm
.sci
ence
mag
.org
Dow
nloa
ded
from
FRAG I L E X SYNDROME
Epigenetic Modification of the FMR1 Gene in Fragile XSyndrome Is Associated with Differential Responseto the mGluR5 Antagonist AFQ056Sébastien Jacquemont,1* Aurore Curie,2* Vincent des Portes,2 Maria Giulia Torrioli,3
Elizabeth Berry-Kravis,4 Randi J. Hagerman,5 Feliciano J. Ramos,6 Kim Cornish,7 Yunsheng He,8
Charles Paulding,8 Giovanni Neri,9 Fei Chen,1,10 Nouchine Hadjikhani,10,11 Danielle Martinet,1
Joanne Meyer,8 Jacques S. Beckmann,1 Karine Delange,2 Amandine Brun,2 Gerald Bussy,2
Fabrizio Gasparini,12 Talita Hilse,13 Annette Floesser,13 Janice Branson,12 Graeme Bilbe,12
Donald Johns,14 Baltazar Gomez-Mancilla14†
Fragile X syndrome (FXS) is an X-linked condition associated with intellectual disability and behavioral problems. It iscaused by expansion of a CGG repeat in the 5! untranslated region of the fragile X mental retardation 1 (FMR1) gene.Thismutation is associatedwith hypermethylation at the FMR1promoter and resultant transcriptional silencing. FMR1silencinghasmany consequences, includingup-regulation ofmetabotropic glutamate receptor 5 (mGluR5)–mediatedsignaling. mGluR5 receptor antagonists have shown promise in preclinical FXS models and in one small open-labelstudy of FXS. We examined whether a receptor subtype–selective inhibitor of mGluR5, AFQ056, improves thebehavioral symptoms of FXS in a randomized, double-blind, two-treatment, two-period, crossover study of 30 maleFXS patients aged 18 to 35 years. We detected no significant effects of treatment on the primary outcome measure,the Aberrant Behavior Checklist–Community Edition (ABC-C) score, at day 19 or 20 of treatment. In an exploratoryanalysis, however, seven patients with full FMR1 promoter methylation and no detectable FMR1 messenger RNAimproved, as measured with the ABC-C, significantly more after AFQ056 treatment than with placebo (P < 0.001). Wedetected no response in 18 patients with partial promotermethylation. Twenty-four patients experienced an adverseevent, which was mostly mild to moderately severe fatigue or headache. If confirmed in larger and longer-termstudies, these results suggest that blockade of the mGluR5 receptor in patients with full methylation at the FMR1promoter may show improvement in the behavioral attributes of FXS.
INTRODUCTION
Fragile X syndrome (FXS) is an X-linked genetic condition associatedwith intellectual disability and behavioral problems including anxiety,aggression, hyperactivity, impulsivity, shyness, attention deficit dis-order, and autism (1). It is caused by expansion of a CGG trinucleotiderepeat in the 5! untranslated region of the fragile X mental retardation
1 (FMR1) gene. This mutation is associated with hypermethylation atthe FMR1 promoter and consequent transcriptional silencing (2–5).The FMR1 protein (FMRP) is a cytoplasmic RNA binding proteinknown to repress the translation of messenger RNAs (mRNAs) atsynapses (6). It has been suggested that in the absence of FMRP, lossof repression ofmetabotropic glutamate receptor 5 (mGluR5)–mediatedpathways results in the behavioral and cognitive impairments associatedwith FXS (7).
Recent studies in animal models of FXS have suggested that manyaspects of the FXS phenotype, including behavioral abnormalities, cog-nitive deficits, and altered dendritic spines, may be attributable to exces-sive signaling by mGluR5, a group I mGluR. Genetic down-regulationof mGluR5 expression by crossing Fmr1 knockout mice with heterozy-gous Grm5 knockout mice rescues many of the FXS phenotypes, withthe exception of macroorchidism (8). Consequently, selective mGluR5antagonists may offer effective treatment for the symptoms of FXS.These compounds have been available as research tools for nearly adecade, and the prototype of the class, 2-methyl-6-(phenylethynyl)-pyridine (MPEP), has been tested extensively in animal models ofFXS.MPEP rescues themost robust central nervous system phenotypesin Fmr1 knockout mice, namely, hyperactivity and audiogenic seizuresusceptibility (9). Cognitive and neuroanatomical phenotypes were res-cued in a fruit fly model (10), neurite branching and craniofacial ab-normalities were rescued in a zebrafish model (11).
1Service de Génétique Médicale, Centre Hospitalier Universitaire Vaudois, CH-1011Lausanne, Switzerland. 2National Reference Center for Fragile X and Other XLMR, HospicesCivils de Lyon, Université de Lyon and CNRS UMR 5230 (L2C2), F-69675 Bron, France.3Università Cattolica del Sacro Cuore, Cattedra di Neuropsichiatria Infantile, 00168 Rome,Italy. 4Departments of Pediatrics, Neurological Sciences, and Biochemistry, Rush UniversityMedical Center, Chicago, IL 60612, USA. 5Department of Pediatrics and MedicalInvestigation of Neurodevelopmental Disorders (M.I.N.D.) Institute, University of California,Davis, School of Medicine, Sacramento, CA 95817, USA. 6Department of Pediatrics, Universityof Zaragoza Medical School, 50009 Zaragoza, Spain. 7Centre for Developmental Psychiatryand Psychology, School of Psychology and Psychiatry, Monash University, Melbourne,Victoria 3800, Australia. 8Biomarker Development, Novartis Institutes for BiomedicalResearch, Cambridge, MA 02139, USA. 9Università Cattolica del Sacro Cuore, Istituto diGeneticaMedica, 00191 Rome, Italy. 10BrainMind Institute, École Polytechnique Fédérale deLausanne, CH-1015 Lausanne, Switzerland. 11Martinos Center for Biomedical Imaging,Harvard Medical School, Boston, MA 02129, USA. 12Neuroscience Discovery, NovartisPharma AG, CH-4056 Basel, Switzerland. 13Neuroscience Clinical Sciences and Innovation,Novartis Institutes for Biomedical Research, Novartis PharmaAG, CH-4056 Basel, Switzerland.14Neuroscience Translational Medicine, Novartis Institutes for Biomedical Research, NovartisPharma AG, CH-4056 Basel, Switzerland.*These authors contributed equally to this work.†To whom correspondence should be addressed. E-mail: [email protected]
R E S EARCH ART I C L E
www.ScienceTranslationalMedicine.org 5 January 2011 Vol 3 Issue 64 64ra1 1
on
Sep
tem
ber
14, 2
012
stm
.sci
ence
mag
.org
Dow
nloa
ded
from
Science Translational Medicine, 2011 29
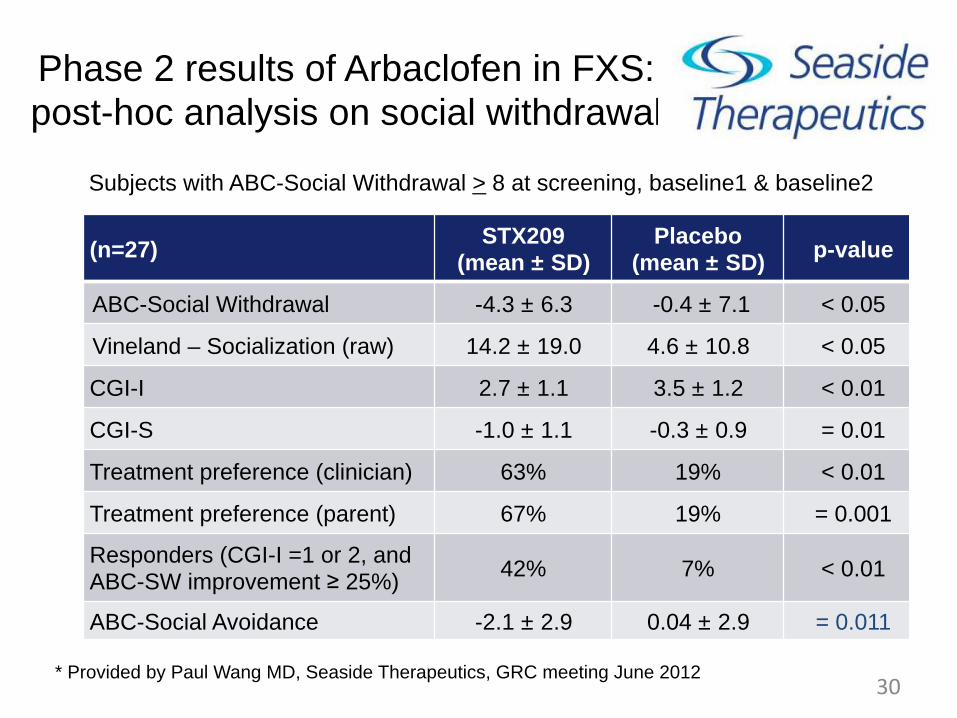
Phase 2 results of Arbaclofen in FXS: post-hoc analysis on social withdrawal
30
FXS Study 22001: Post-hoc analyses
(n=27) STX209
(mean ± SD)!Placebo
(mean ± SD)! p-value!
ABC-Social Withdrawal -4.3 ± 6.3 -0.4 ± 7.1 < 0.05
Vineland – Socialization (raw) 14.2 ± 19.0 4.6 ± 10.8 < 0.05
CGI-I 2.7 ± 1.1 3.5 ± 1.2 < 0.01
CGI-S -1.0 ± 1.1 -0.3 ± 0.9 = 0.01
Treatment preference (clinician) 63% 19% < 0.01
Treatment preference (parent) 67% 19% = 0.001
Responders (CGI-I =1 or 2, and ABC-SW improvement ≥ 25%) 42% 7% < 0.01
ABC-Social Avoidance -2.1 ± 2.9 0.04 ± 2.9 = 0.011
10
Subjects with ABC-Social Withdrawal > 8 at screening, baseline1 & baseline2
* Provided by Paul Wang MD, Seaside Therapeutics, GRC meeting June 2012
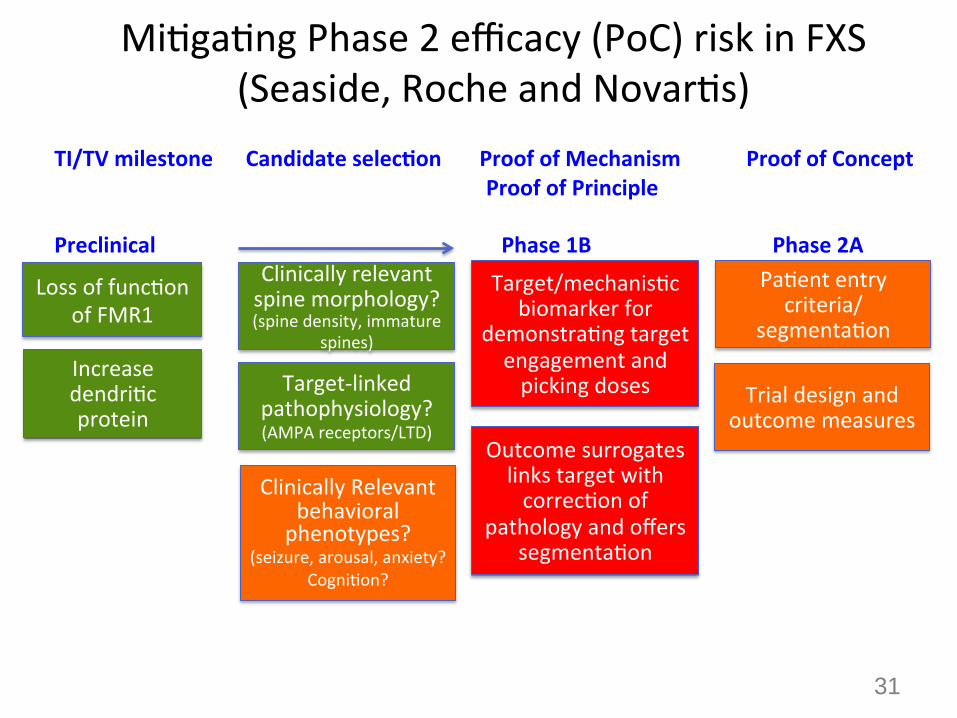
Mi)ga)ng Phase 2 efficacy (PoC) risk in FXS (Seaside, Roche and Novar)s)
Loss of func)on of FMR1
Increase dendri)c protein
Clinically relevant spine morphology? (spine density, immature
spines)
Target-‐linked pathophysiology? (AMPA receptors/LTD)
Clinically Relevant
behavioral phenotypes?
(seizure, arousal, anxiety? Cogni)on?
Pa)ent entry criteria/
segmenta)on
Trial design and outcome measures
Outcome surrogates links target with correc)on of
pathology and offers segmenta)on
Target/mechanis)c biomarker for
demonstra)ng target engagement and picking doses
TI/TV milestone Candidate selecQon Proof of Mechanism Proof of Concept
Proof of Principle Preclinical Phase 1B Phase 2A
31
32
*ABC-‐C showed no sta)s)cally meaningful effect…only their ReQ-‐specific clinical scale
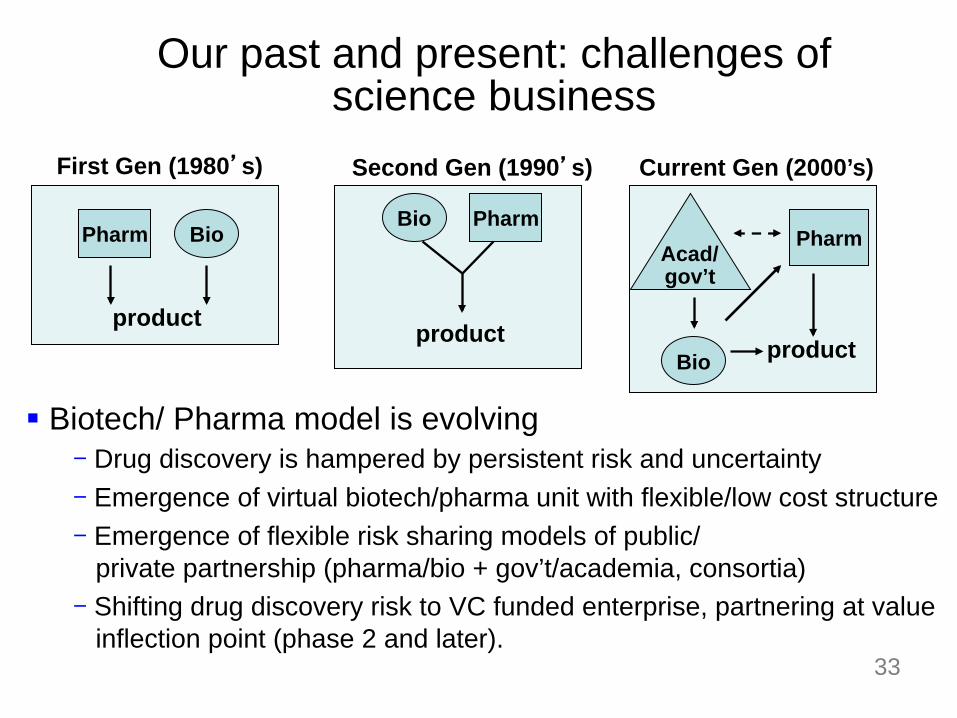
Our past and present: challenges of science business
§ Biotech/ Pharma model is evolving
- Drug discovery is hampered by persistent risk and uncertainty
- Emergence of virtual biotech/pharma unit with flexible/low cost structure
- Emergence of flexible risk sharing models of public/ private partnership (pharma/bio + gov’t/academia, consortia) - Shifting drug discovery risk to VC funded enterprise, partnering at value inflection point (phase 2 and later).
Pharm Bio Pharm
Acad/ gov’t
Pharm Bio
product product
Bio product
First Gen (1980’s) Second Gen (1990’s) Current Gen (2000’s)
33
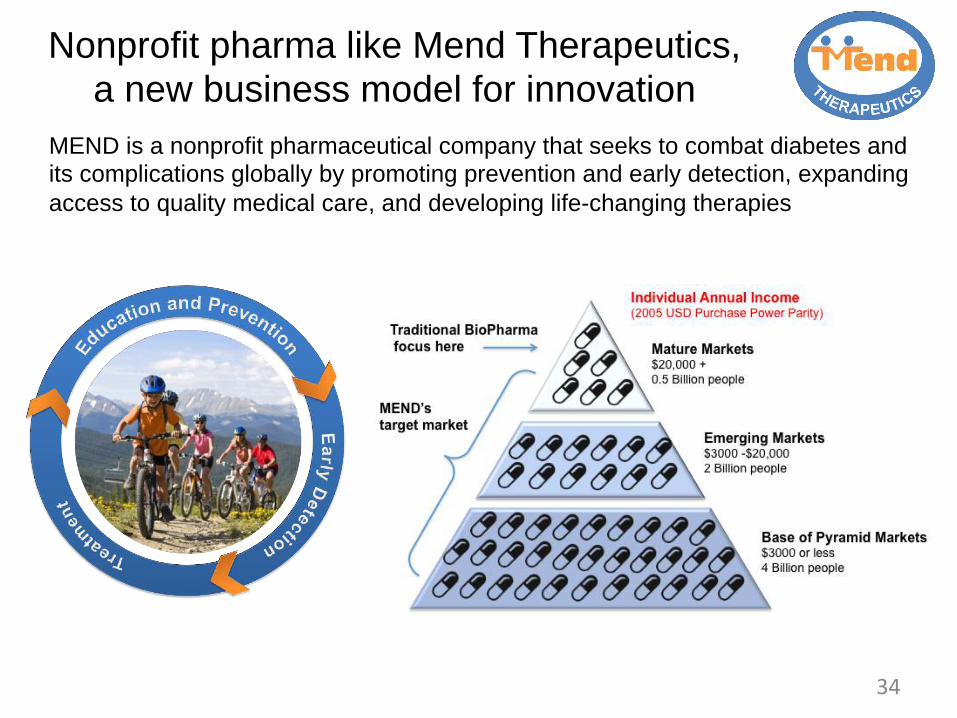
Nonprofit pharma like Mend Therapeutics, a new business model for innovation
34
MEND is a nonprofit pharmaceutical company that seeks to combat diabetes and its complications globally by promoting prevention and early detection, expanding access to quality medical care, and developing life-changing therapies
35
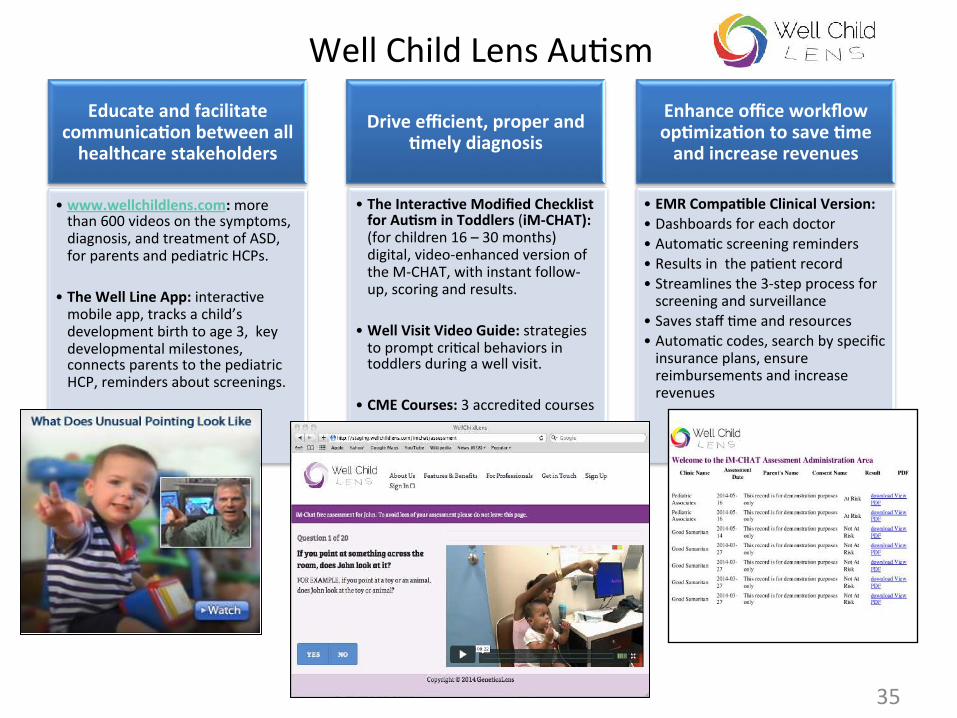
Well Child Lens Au)sm Educate and facilitate
communicaQon between all healthcare stakeholders
• www.wellchildlens.com: more than 600 videos on the symptoms, diagnosis, and treatment of ASD, for parents and pediatric HCPs.
• The Well Line App: interac)ve mobile app, tracks a child’s development birth to age 3, key developmental milestones, connects parents to the pediatric HCP, reminders about screenings.
Drive efficient, proper and Qmely diagnosis
• The InteracQve Modified Checklist for AuQsm in Toddlers (iM-‐CHAT): (for children 16 – 30 months) digital, video-‐enhanced version of the M-‐CHAT, with instant follow-‐up, scoring and results.
• Well Visit Video Guide: strategies to prompt cri)cal behaviors in toddlers during a well visit.
• CME Courses: 3 accredited courses
Enhance office workflow opQmizaQon to save Qme and increase revenues
• EMR CompaQble Clinical Version: • Dashboards for each doctor • Automa)c screening reminders • Results in the pa)ent record • Streamlines the 3-‐step process for screening and surveillance
• Saves staff )me and resources • Automa)c codes, search by specific insurance plans, ensure reimbursements and increase revenues
Summary
36
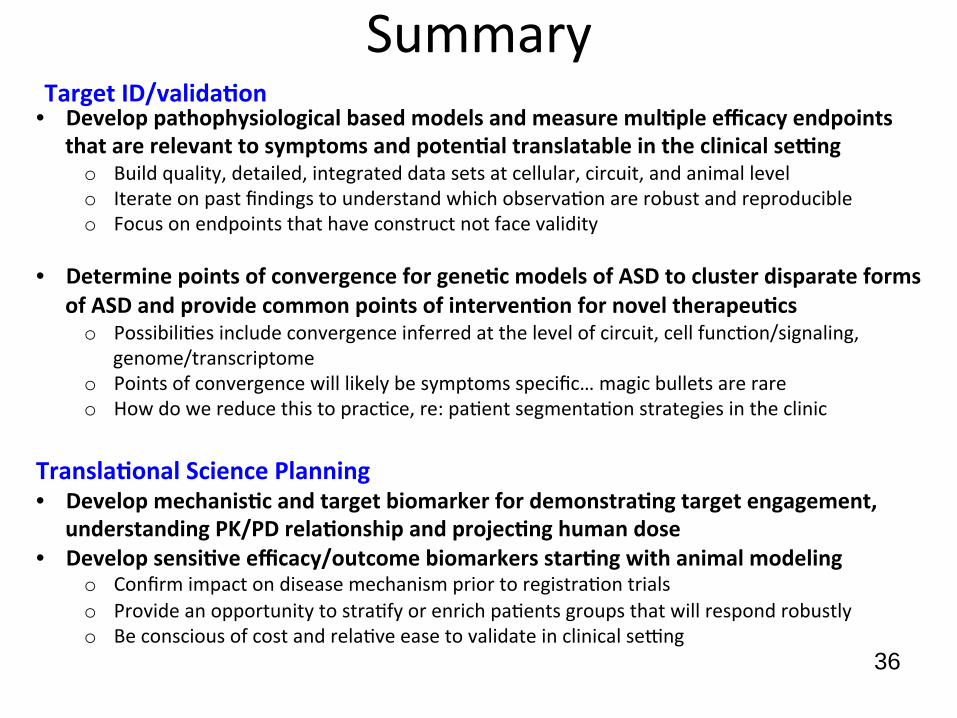
• Develop pathophysiological based models and measure mulQple efficacy endpoints that are relevant to symptoms and potenQal translatable in the clinical sepng o Build quality, detailed, integrated data sets at cellular, circuit, and animal level o Iterate on past findings to understand which observa)on are robust and reproducible o Focus on endpoints that have construct not face validity
• Determine points of convergence for geneQc models of ASD to cluster disparate forms of ASD and provide common points of intervenQon for novel therapeuQcs o Possibili)es include convergence inferred at the level of circuit, cell func)on/signaling,
genome/transcriptome o Points of convergence will likely be symptoms specific… magic bullets are rare o How do we reduce this to prac)ce, re: pa)ent segmenta)on strategies in the clinic
TranslaQonal Science Planning • Develop mechanisQc and target biomarker for demonstraQng target engagement,
understanding PK/PD relaQonship and projecQng human dose • Develop sensiQve efficacy/outcome biomarkers starQng with animal modeling
o Confirm impact on disease mechanism prior to registra)on trials o Provide an opportunity to stra)fy or enrich pa)ents groups that will respond robustly o Be conscious of cost and rela)ve ease to validate in clinical sexng
Target ID/validaQon
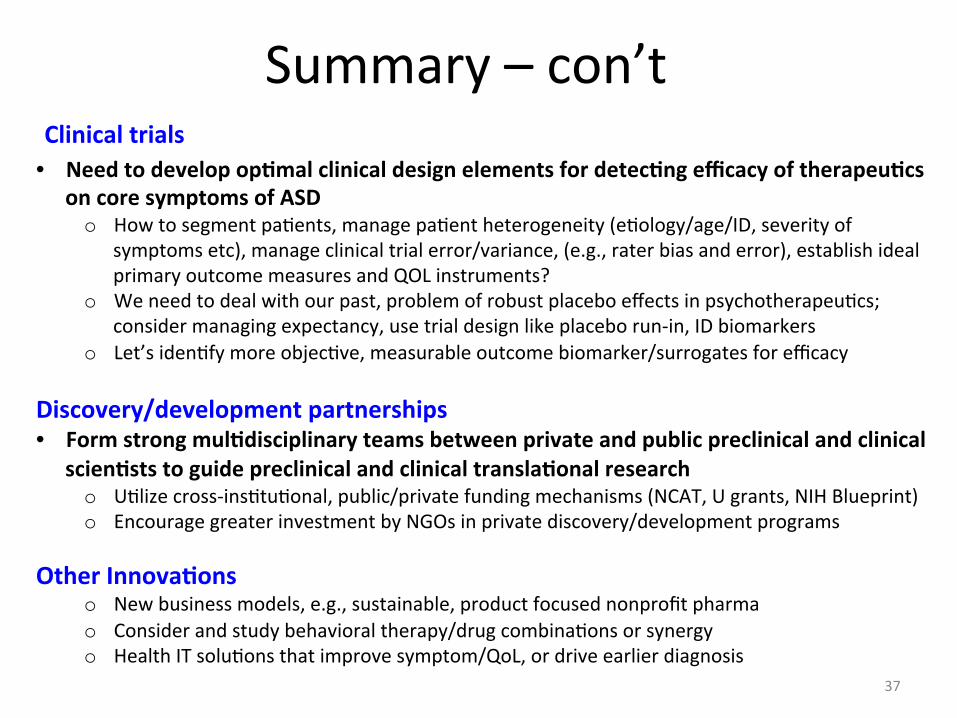
Summary – con’t
37
• Need to develop opQmal clinical design elements for detecQng efficacy of therapeuQcs on core symptoms of ASD o How to segment pa)ents, manage pa)ent heterogeneity (e)ology/age/ID, severity of
symptoms etc), manage clinical trial error/variance, (e.g., rater bias and error), establish ideal primary outcome measures and QOL instruments?
o We need to deal with our past, problem of robust placebo effects in psychotherapeu)cs; consider managing expectancy, use trial design like placebo run-‐in, ID biomarkers
o Let’s iden)fy more objec)ve, measurable outcome biomarker/surrogates for efficacy Discovery/development partnerships • Form strong mulQdisciplinary teams between private and public preclinical and clinical
scienQsts to guide preclinical and clinical translaQonal research o U)lize cross-‐ins)tu)onal, public/private funding mechanisms (NCAT, U grants, NIH Blueprint) o Encourage greater investment by NGOs in private discovery/development programs
Other InnovaQons o New business models, e.g., sustainable, product focused nonprofit pharma o Consider and study behavioral therapy/drug combina)ons or synergy o Health IT solu)ons that improve symptom/QoL, or drive earlier diagnosis
Clinical trials
Acknowledgements
38
Pfizer AuQsm Unit (co-‐founders/partners/advisors) Diane Stephenson (Cri)cal Path) Howard Mayer (Shire HGT) Mahesh Lachyankar (MEND Therapeu)cs) Mat Pletcher (Pfizer Rare Diseases) Mark Bear (MIT, Seaside Tx) Michael Ehlers (Pfizer) Rob Malenka (Stanford) Nonprofits Rob Ring (Au)sm Speaks) Dan Smith (Au)sm Speaks) Steve Roberds (Tuberous Sclerosis Alliance) Mike Tranfaglia (FRAXA) Gerry Fischbach (Simons Founda)on)
Sage TherapeuQcs Gabi Belfort Carlos Loya Jim Doherty Rebecca Hammond
Seaside TherapeuQcs Paul Wang Randy Carpenter
GeneQcaLens/Well Child Lens Louise Tiranoff Barbara Floyd









![Engineering'a'Market:'Concepts' &'Research'on'the'HAT · 2015-08-23 · The'H.A.T' • Pla\orm'for'Mul+]sided'Market'powered'by'Internet]of]Things:' Opportuni+es'for'New'Economic'&'Business'Models](https://img.pdfslide.us/doc/110x75/5faaa05d630d6653ba7d419f/engineeringamarketconcepts-researchonthe-2015-08-23-thehat-a.jpg)

















