Embed Size (px)
Citation preview

Thrombosis Research 130 (2012) 343–349
Contents lists available at SciVerse ScienceDirect
Thrombosis Research
j ourna l homepage: www.e lsev ie r .com/ locate / thromres
Regular Article
Monitoring hypercoagulability and hypofibrinolysis following acute venousThromboembolism in Children: Application of the CloFAL assay in a prospectiveinception cohort study
Christopher Bombardier a,c, Elizabeth Villalobos-Menuey a,c, Katherine Ruegg a,c, William E. Hathaway a,c,Marilyn J. Manco-Johnson a,c, Neil A. Goldenberg a,b,c,⁎a Department of Pediatrics, University of Colorado School of Medicine and Children's Hospital Colorado, Aurora, CO, USAb Department of Medicine, University of Colorado School of Medicine and Children's Hospital Colorado, Aurora, CO, USAc Divisions of Hematology/Oncology/, Bone Marrow Transplantation and the Mountain States Regional Hemophilia and Thrombosis Center, University of Colorado School of Medicine andChildren's Hospital Colorado, Aurora, CO, USA
⁎ Corresponding author at: Hemophilia and ThroColorado School of Medicine, 13199 E. Montview Blvd.Tel.: +1 303 724 7028; fax: +1 303 724 0947.
E-mail address: [email protected] (N.A
0049-3848/$ – see front matter © 2012 Elsevier Ltd. Alldoi:10.1016/j.thromres.2012.03.030
a b s t r a c t
a r t i c l e i n f oArticle history:Received 26 November 2011Received in revised form 2 March 2012Accepted 20 March 2012Available online 30 April 2012
Keywords:CoagulationFibrinolysisThromboembolismPediatricGlobal assay
Although individual thrombophilia tests are frequently performed in children with venous thromboembo-lism (VTE), global assays provide the opportunity to fill the gap in knowledge regarding their net impact onoverall coagulative (and in some cases fibrinolytic) function. We first evaluated analytic sensitivity of the ClotFormation and Lysis (CloFAL) global assay to hypercoagulability and alterations in fibrinolysis, and thencharacterized changes in plasma coagulative and fibrinolytic capacities over time in children with acute VTE.In plasma ex vivo and in vitro experiments, the CloFAL assay area-under-the-curve (AUC) was analyticallysensitive to hypercoagulable states, and its modified fibrinolytic index (FI2) was sensitive to both hyper- andhypofibrinolytic conditions. Clinical data and plasma samples for assay were collected during follow-up of 50children enrolled in a prospective inception cohort study of VTE from May 2006 to June 2010. Follow-upperiods were designated as follows: acute (b1 month post-event), sub-acute (1–3 months), early chronic(3–12 months), and late chronic (>12 months). Since most children were sampled at fewer than three pre-defined follow-up periods, study population findings were grouped by timepoint. AUC was significantlyincreased, and FI2 significantly decreased, in the acute period of VTE when compared to healthy controls,indicating hypercoagulability and hypofibrinolysis, respectively. One-third of patients were hypercoagulable,and 23% were hypofibrinolytic, in the late chronic phase. AUC and FI2 were strongly correlated withfunctional fibrinogen levels. These findings indicate the utility of the CloFAL assay in monitoring plasmacoagulative and fibrinolytic capacities in children with VTE. Studies of its potential role in outcome predictionare ongoing.
© 2012 Elsevier Ltd. All rights reserved.
Introduction
Venous thromboembolism (VTE) is a rare condition in childrenthat nevertheless is rising in frequency as a cause or complication ofpediatric hospitalizations [1]. Conventional treatment is with antic-oagulation, and optimal duration of anticoagulant therapy is predi-cated in large part upon the duration of clinically significantunderlying prothrombotic risk factors [2]. However, while clinicalrisk factors contributing to venous stasis and endothelial damage(e.g., post-operative state following major orthopedic surgery) in thetriad of Virchow are readily assessed in children, the hypercoagulablestate (much as in adults) is difficult to measure [3].
mbosis Center, University of, Suite 200, Aurora, CO 80045.
. Goldenberg).
rights reserved.
In children with acute VTE, both acquired thrombophilia factors(e.g., antiphospholipid antibodies, elevated factor VIII activity) andmild genetic thrombophilia traits (e.g., the factor V Leiden polymor-phism) are highly prevalent [4]. However, the net impact of suchabnormalities on overall coagulative function remains in question,and the presence of persistent hypercoagulability is likely to beimportant for patient outcomes. Although high-quality direct evi-dence is lacking, it has been speculated that the duration of thehypercoagulable state influences the time-dependent risk of recur-rent VTE following acute VTE in children [5]. This hypothesis issupported by the observation that, in idiopathic VTE in adults, apersistently elevated plasma level ofD-dimer (a surrogate marker ofhypercoagulability) following a 6 month course of therapeutic antic-oagulation significantly increases the risk of recurrent VTE [6]. Bycomparison to thrombophilia testing, the potential contribution ofdeficiencies of fibrinolysis to the pathogenesis of VTE and itsrecurrence in children has received little attention, and remains

344 C. Bombardier et al. / Thrombosis Research 130 (2012) 343–349
unknown. The objectives of this work were to (1) investigate theanalytical sensitivity of the Clot Formation and Lysis (CloFAL) assayarea-under-the-curve (AUC) to known hypercoagulable states and itsmodified fibrinolytic index (FI2) to both hyper- and hypofibrinolysis,and (2) employ the CloFAL assay to characterize changes in plasmacoagulative and fibrinolytic capacities over time in an inceptioncohort of children with acute VTE.
The CloFAL assay has been used for several years on a researchbasis as a turbidimetric assay to serially monitor changes in opticaldensity of plasma to which activators of coagulation (tissue factor[TF], phospholipid) and fibrinolysis (tissue plasminogen activator[tPA]) have been added [7]. A clot formation and lysis waveform isgenerated, whose measured and calculated parameters have beenapplied to the investigation various physiologically and pathophysio-logically altered states of coagulation and fibrinolysis [8–10]. Unlikethe thromboelastogram, which requires a unique device to measureviscoelasticity of fresh whole blood in which coagulation has beenactivated, the CloFAL assay can be performed on fresh or frozenplasma samples using conventional clinical laboratory spectropho-tometry equipment, affording pragmatic evaluation of serial samplesover time in a single assay.
Methods
Subjects
Following written informed consent/assent, children with acuteVTE were enrolled in a prospective inception cohort study forpediatric and adult VTE between April 1, 2006 and June 1, 2010.Inclusion criteria consisted of age birth to 18 years (inclusive) andradiologically-confirmed VTE within 14 days of symptom onset.Children with arterial events (including arterial ischemic stroke)and those without symptomatic presentation were excluded. Inaddition, patients with prior VTE in whom severe thrombophiliatraits had been established were further excluded from the analysis ofthe study's secondary objective (characterization of changes inplasma coagulative and fibrinolytic capacities over time in pediatricVTE), but included in the analysis of the first objective (determinationof analytical sensitivity of the CloFAL assay to known hypercoagulablestates and altered fibrinolysis. Healthy children (n=44) who werewithout acute illness or chronic medical condition, were taking nomedication, and had no personal or family history of thromboticevents or abnormal bleeding, were enrolled from a well-childambulatory setting as a comparator group for laboratory normativevalues. (Control children underwent a single venipuncture for studypurposes; however, reproducibility of the assay findings wasinvestigated in a subgroup of the control population (n=10), andfound to be excellent for AUC (intra-class correlation coefficient [ICC]of 0.94) and very good for FI2 (ICC of 0.70), using the Bland-Altmanmethod for measuring agreement) [11].
Data were systematically collected on patient and thrombuscharacteristics, clinical prothrombotic risk factors, results of compre-hensive thrombophilia testing, antithrombotic therapy, follow-upduration, and development of symptomatic recurrent VTE. Follow-upvisits occurred at 4–6 weeks post-VTE diagnosis, 3 months,12 months, and annually in long-term follow-up. Additional visits at6 months and 9 months were frequently performed.
Blood samples for research evaluation of coagulative and fibrino-lytic capacities were routinely obtained during follow-up visits whenvenipuncture was being performed for clinical purposes, andoccasionally procured for research purposes alone (when consentwas provided for same). Follow-up periods were designated asfollows: acute (b1 month post-event), sub-acute (1–3 months), earlychronic (3–12 months), and late chronic (>12 months). In the case ofmore than one sampling during a given follow-up period, the firstsample within the period was uniformly utilized for assessment.
Blood Collection, Plasma Processing, and Sample Preparation
Whole blood was collected by atraumatic peripheral venipuncturetechnique using minimal applied stasis into BD Vacutainer 3.2%buffered sodium citrate siliconized blood collection tubes (Becton-Dickinson, Franklin Lakes, NJ, USA) with participant at rest and alertin a seated position. The initial 1 mL of whole blood was collected intoa discard tube. Whole blood was centrifuged at 2500 g for 15 min at4 °C. The supernatant was isolated and subjected to repeat centrifu-gation for 15 minutes at the aforementioned settings. The resultingplatelet-poor plasma supernatant was pooled, aliquoted into poly-propylene tubes, and subsequently frozen at −70 °C for long-termstorage.
CloFAL Assay Procedure
Samples obtained while a patients was being anticoagulated withheparin (including unfractionated or low-molecular-weight heparin)were analyzed after the addition of heparinase (Hepzyme®, SiemensHealthcare Diagnostics, Deerfield, IL, USA), as previously described[12]. Samples obtained while a patient was being treated withwarfarin were excluded from the analysis, given that the purpose ofthe study was not to monitor efficacy of pharmacological vitamin Kantagonism, but to assess native plasma coagulative and fibrinolyticfunction.
The CloFAL assay method was performed according to thepreviously summarized modification [9] to the original method [7].In brief summary, plasma samples were loaded in quadruplicate wellsof a 96-well round-bottom Nunc microassay plate (Fisher Scientific,Santa Clara, CA, USA). A buffered (Tris-buffered saline [TBS], pH 7.0)reagent providing citrate reversal with CaCl, coagulation activationwith TF and phospholipid, and fibrinolytic enhancement with tPA,was added to three of the four wells for a given sample; TBS alone wasadded to the remaining well, to serve as a blank. Final plasmaconcentrations were as follow: CaCl2, 17 mM; human recombinantnon-lipidated tissue factor (TF; American Diagnostica, Stamford, CT)and human recombinant lipidated TF (American Diagnostica), ratio1.4:1, total5 pM; human recombinant double-chain tissue plasmin-ogen activator (American Diagnostica), 450 ng/mL. Kinetic blankeddual-wavelength (405 and 605 nm) absorbance measurements wereimmediately obtained at 45-s intervals in a PowerWave HT™microplate scanning spectrophotometer (BIO-TEK, Winooski, VT,USA) for 3 h, generating a clot formation and lysis waveform.Absorbance data and waveforms were stored via KC4™ data analysissoftware, and exported to Microsoft Excel for further analysis. Theassay standard was pooled normal adult plasma (George King Inc.,Overland Park, KS). Assay controls consisted of a separate poolednormal plasma (George King Inc.) and severe factor VIII-deficiencyplasma (derived from a well characterized patient at untreatedbaseline, and maintained as a local laboratory standard).
In addition to previously-established measurements (time tomaximum amplitude, T1; maximum amplitude, MA; coagulationindex, CI , defined as area-under-the curve [AUC] through 30 minutesfor the sample as a percent of the standard]), cumulative AUC for theentire assay (as a percent of the standard) was used to modelhypercoagulability. (This was made feasible by the observation thatthe CloFAL waveform in all healthy controls and pediatric VTEpatients–unlikely those previously reported with hemophilia A or B)[8,9]–peaked and returned to baseline prior to completion of theassay run-time.) A modified fibrinolytic index (FI2) was alsodeveloped to enhance sensitivity to altered states of fibrinolysis,while maintaining suitable precision. In utilizing the area-over-the-curve (AOC), FI2 is similar to the with-versus-without-tPA subtractionmethod employed by Blömback and co-workers for modeling OverallFibrinolytic Potential in the OHP assay [13]. However, unlike the lattercalculation, FI2 adjusts fibrinolytic capacity for magnitude of clot, by

345C. Bombardier et al. / Thrombosis Research 130 (2012) 343–349
indexing to MA. In addition, by restricting the AOC measurement tothe first 20 minutes following T1, FI2 maximizes sensitivity to changein slope of absorbance measurements following peak amplitude.Calculation of FI2 is given below.
FI2 ¼ AOC T1− T1þ20minð Þ½ � sampleð ÞMA sampleð Þ
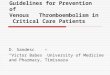
The additions of AUC and FI2 to the CloFAL assay calculatedparameters are represented in Fig. 1. Inter-assay coefficients ofvariation as evaluated in 30 consecutive runs of normal controls(pooled normal plasma) were 15.0% for AUC and 16.3% for FI2.
Additional Laboratory Assay Procedures
Functional fibrinogen was determined by clotting assay using theClauss method, as previously described [7]. Thrombin and plasmingeneration were serially measured in selected clinical case examplesusing the Simultaneous Thrombin and Plasmin generation (STP)assay [14], and euglobulin lysis time (ELT) was evaluated byautomated euglobulin clot lysis assay [15], in accordance withpublished methods.
In Vitro Experiments
For determination of the CloFAL assay's analytical sensitivity toknown thrombophilia states, plasma samples were obtained fromselect pediatric and adult VTE subjects in the cohort study, in whomsevere inherited states had been previously established (see alsoSubjects, above). To evaluate analytical sensitivity of the CloFAL assayto alterations in fibrinolysis, immunodepleted plasminogen-deficientand alpha-2-antiplasmin-deficient plasmas were obtained commer-cially (Affinity Biologicals, Inc., Lancaster, ON, Canada) and used inplasma mixing studies. These deficient plasmas were serially dilutedwith standard pooled normal plasma to achieve activity levels ofapproximately 50, 30, and10 U/dL. Aminocaproic acid treatment ofplasma was performed using a final plasma concentration of 2.5 mg/mL. The influence of tissue plasminogen activator (tPA) was assessedby altering the concentration of tPA in the assay reagent, achievingconcentrations of 0.5x and 1.5x.
Statistical Analyses
Descriptive statistics involved non-parametric measures; data arepresented as medians and observed ranges. Given challenges of serialblood sampling in children, and the exclusion of sampling time pointswhile on warfarin (due to inability to “correct” in the assay forinfluence of this anticoagulant on factor activities), the principalanalysis relied upon aggregative comparisons grouped by time point,
Fig. 1. CloFAL assay waveform in pooled normal adult plasma, demonstrating AUC andFI2 calculated parameters.
rather than averaged per-patient changes over time. Distributions ofdata were compared between subject groups (patients versuscontrols; dichotomous patient subgroups) using the Mann–WhitneyU test. Proportions were compared between groups by chi-squaredtest or Fisher's exact test, as appropriate. A P-value of b0.05considered as statistically significant. All statistics were performedusing SAS 9.3 statistical software (SAS Institute, Cary, NC, USA).
Results
Analytical Sensitivity of the CloFAL Assay for known HypercoagulableStates and Alterations in Fibrinolysis
CloFAL assay waveforms and parameters in excess thrombinstates, as evaluated ex vivo in plasma in adults, including heterozy-gous antithrombin deficiency, homozygosity for the prothrombinG20210A polymorphism, and pregnancy at term, are shown in Fig. 2Ain comparison to pooled normal adult plasma. Fig. 2B similarlydisplays waveforms for protein C pathway defects, including protein Sdeficiency and homozygosity for the factor V Leiden polymorphism inchildren, relative to a representative healthy pediatric control. In
Fig. 2. CloFAL assay waveforms in hypercoagulable states in which thrombingeneration is increased (panel A, including heterozygous antithrombin deficiencyand homozygous prothrombin G20210A polymorphism) or the protein C pathway isimpaired (panel B, including moderately severe protein S deficiency, homozygousfactor V Leiden polymorphism, pregnant female at term). With regard to the strikingdifference in CloFAL waveforms between the two examples of protein S deficiency, thetwo patients were unrelated, and it is possible that these waveforms represent distinctgenetic defects that confer different severities in global coagulative function.Investigation of other contributors to global coagulative function (including fibrinogen[Clauss assay], factor VIII activity and dilute Russell viper venom time results) revealedthat only fibrinogen differed between the two patients, with hyperfibrinogenemiapresent in the patient with the hypercoagulable CloFAL waveform.

Fig. 3. CloFAL assay waveforms in altered fibrinolytic states: hypofibrinolysis (panel A,including plasminogen deficiency, decreased tPA reagent in pooled normal plasma,elevated PAI-1 , and treatment of pooled normal plasma with aminocaproic acid); andhyperfibrinolysis (panel B, including alpha-2 anti-plasmin deficiency and increasedtPA reagent in pooled normal plasma). In each panel, the pooled adult plasma standardis shown for reference.
346 C. Bombardier et al. / Thrombosis Research 130 (2012) 343–349
most cases, CloFAL waveforms show an increased AUC, suggestinganalytic sensitivity of this assay measurement in particular tohypercoagulable states. At the same time, given some examples ofnormal waveforms in protein C pathway defects (i.e.: homozygousfactor V Leiden example; one of two protein S deficiency examples),
Table 1Summary findings of CloFAL AUC, FI2, and fibrinogen clotting activity in healthy pediatric s
Lab measure Healthy PediatricControls (n=44)
AcutePost-VTE(b1 mo)
CloFAL AUC (% of adultpooled normal plasma)
87(55-150)
148(59-405)
% (freq) of subjectshypercoagulable⁎
– 47%(8/17)
Fibrinogen (mg/dL) 301(231-362)
312(244-647)
% (freq) of subjectshyperfibrinogenemic⁎
– 57%(8/14)
CloFAL FI2 (A.U.) 31(13-48)
19(8-49)
% (freq) of subjectshypofibrinolytic⁎⁎
– 33%(5/15)
⁎ Defined as >90th percentile of normative values established in healthy pediatric contr⁎⁎ Defined as b10th percentile of normative values established in healthy pediatric contro
the assay may have only moderate sensitivity to alternations in thispathway in the absence of a reagent (such as Protac®) that enhancesprotein C activation.
With regard to fibrinolytic aberrations, CloFAL waveforms andparameters are given in Fig. 3A for hypofibrinolytic states ofplasminogen deficiency (30%), decreased tPA reagent (0.5x) inpooled normal plasma, elevated PAI-1 (41 ng/mL), and treatment ofpooled normal plasma with aminocaproic acid (final concentration,2.5 mg/mL). Hyperfibrinolytic states are shown in Fig. 3B, includingalpha-2 anti-plasmin deficiency (30%) and increased tPA reagent (2x)in pooled normal plasma. FI2 was markedly decreased in hypofibri-nolytic states and increased in hyperfibrinolytic states.
Prospective Inception Cohort Findings: Changes in Coagulative andFibrinolytic Capacities Over Time Following Acute VTE in Children
Clinical data (including baseline patient and thrombus character-istics, thrombophilia findings, follow-up duration, and cumulativeincidence of symptomatic recurrent VTE at 2 years, are summarizedin Table 1 for the cohort of 50 consecutive children with acute VTE.Median age was 14 years (range: birth to 19 years), and genderdistribution was balanced. Two-thirds of VTE cases consisted of deepvenous thrombosis of the limbs and/or pulmonary embolism, andnearly 20% were cerebral sinovenous thromboses. The most com-monly identified clinical risk factors for VTE were central venouscatheterization (29%) and systemic/serious infection (27%, includingbacteremia/viremia, bacterial pneumonia, and osteomyelitis). Eightpercent of children (16% of females) were receiving estrogen-containing birth control pills. Inherited thrombophilia was disclosedin 21% of the cohort, and 38% met criteria for antiphospholipidantibody syndrome.
Table 2 provides distributions of CloFAL AUC and FI2 values andfibrinogen levels, along with proportion of samples abnormal, seriallyover time post-VTE event. Testing from sampling obtained at ≥1 ofthe 4 pre-specified follow-up periods (acute, sub-acute, early chronic,and late chronic) was performed in 100% of the cohort, from ≥2periods in 36%, and from ≥3 periods in 10%. As noted in the Methods,these sampling rates are in part reflective of the fact that no sampleswere obtained during warfarin therapy, so as to validly measurecoagulative function in the absence of anticoagulant effects. (For thisreason, all samples obtained on heparin therapy were pre-treatedwith heparinase; see also Methods).
Relative to healthy pediatric controls (n=44; see Methods), VTEpatients at each time point had significantly increased AUC anddecreased FI2 (Pb0.05 for each). While a progressive decrease inmedian AUC was observed over time, a slight and transient increasewas noted in the proportion of patients who were hypercoagulable
ubjects and pediatric acute VTE cohort patients over time post-event.
Sub-acutePost-VTE(1-b3 mo)
Early chronicPost-VTE(3-b12 mo)
Late chronicPost-VTE(≥12 mo)
136(79-262)
115(77-300)
122(66-235)
37%(7/19)
47%(7/15)
36%(8/22)
344(245-568)
312(244-647)
301(222-513)
40%(6/15)
27%(3/11)
30%(6/20)
24(7-51)
21(9-55)
24(9-46)
26%(5/19)
13%(2/15)
23%(5/22)
ol subjects.l subjects.

347C. Bombardier et al. / Thrombosis Research 130 (2012) 343–349
during the early chronic period, when anticoagulation was typicallydiscontinued. Notably, one-third of patients were hypercoagulableand 23% were hypofibrinolytic by CloFAL assay in the late chronicphase. Group-wise time trends in functional fibrinogen (and theproportion of patients with elevated fibrinogen levels) were
Fig. 4. Serial CloFAL assay waveforms over time post-event in 4 children with acute VTE, repand the plasma waveform in a representative healthy pediatric subject are shown for refetherapy (with heparinase treatment of samples immediately prior to assay). Panel A: 17 y.o.plasma samples obtained during the acute and subacute periods post-event. Functional fihypercoagulability, were both elevated acutely but normalized by the time of sub-acute sampnormal pediatric values) at both time points, suggesting insensitivity of this measure to the iactivity, plasmin generation was at the upper limit (95th percentile) of normal pediatric valutPA-mediated cleavage of plasminogen). However, an acutely decreased CloFAL FI2 (indicawas insufficient in overcoming the impact of hyperfibrinogenemia on global fibrinolytic funacross both time points, suggesting its insensitivity to the influence of fibrinogen on fibrinolunderlying systemic lupus erythematosus, with plasma samples obtained during the subacufibrinogen levels were normal across all time points, as were global coagulability and fibrinopoints. By contrast, thrombin and plasmin generation were both elevated at the subacute anassay AUC and FI2. Panel C: 17 y.o. male with acute lymphoblastic leukemia in first remissiothe acute, early chronic, and late chronic (off anticoagulation) phases post-event. L-asparaacutely. Accordingly, the CloFAL assay AUC, as a measure of global hypercoagulability, was elacutely but borderline-elevated at the early chronic time points, suggesting that the CloFstrongly influenced by fibrinogen. With regard to fibrinolytic activity, the CloFAL assay FI2 wplasmin generation and ELT were normal across all time points. Panel D: 16 y.o. female withsubacute, early chronic, and late-chronic periods post-event (all during therapy with low-syndrome was disclosed; however, fibrinogen and factor VIII are both markedly elevatedThrombin and plasmin generation were normal throughout, with the exception of elevated phypofibrinolysis) suggested that the borderline-increased plasmin generation in the late chrfibrinolytic function.
concordant with the findings for AUC in monitoring hypercoagul-ability, and appeared inversely related to FI2 as a measure ofhypofibrinolysis. Correlation testing revealed a strong associationbetween AUC and fibrinogen (r=0.70, Pb0.001), and an inversecorrelation of FI2 with fibrinogen (r=−0.64, Pb0.001); this
resenting common pediatric scenarios. In each panel, the pooled adult plasma standardrence. All plasma samples were either obtained off-therapy or during heparin-basedmale with bilateral upper limb DVT associated with acute trauma and immobility, withbrinogen level (i.e., clotting activity) and CloFAL assay AUC, as a measure of globalling. Thrombin generation was decreased (Vmax [thrombin] b5th percentile of healthy
nfluence of fibrinogen on coagulative function in this patient. With regard to fibrinolytices acutely (as anticipated in the context of elevated levels of the fibrinogen scaffold forting net hypofibrinolysis) suggested that the borderline-increased plasmin generationction. ELT was normal (b459 min, the upper limit of healthy normal pediatric values)ysis in this patient. Panel B: 18 y.o. female with VTE presenting during an acute flare ofte, early chronic, and late chronic (off anticoagulation) periods post-event. Functionallysis as measured by CloFAL AUC and FI2, respectively. ELT was also normal across timed early chronic time points, suggesting that these are distinct measures from the CloFALn and L-asparaginase-associated lower limb DVT, with plasma samples obtained duringginase-induced antithrombin deficiency and hyperfibrinogenemia were demonstratedevated acutely but normal at subsequent time points. Thrombin generation was normalAL assay AUC and thrombin generation are distinct measures, with the former moreas decreased (indicated net hypofibrinolysis) in the early chronic period, whereas bothpost-partum cerebral sinovenous thrombosis, with plasma samples obtained during themolecular weight heparin). No inherited thrombophilia or antiphospholipid antibodyin long-term follow-up, as reflected in the persistently elevated CloFAL assay AUC.lasmin generation at the late chronic time point. A decreased CloFAL FI2 (indicating netonic period was insufficient in overcoming the impact of hyperfibrinogenemia on global

348 C. Bombardier et al. / Thrombosis Research 130 (2012) 343–349
indicated that as fibrinogen levels increased, coagulability wasenhanced and fibrinolytic capacity impaired.
No associations were found between CloFAL values and presence/absence of inherited thrombophilia; however, no patients in thecohort had severe inherited thrombophilias. Interestingly, patientswith spontaneous VTE tended to have a higher AUC than those withclinically-triggered VTE (median 201 [range 69–430] vs. median 148[range 58–291], respectively), although this difference was notstatistically significant (P=0.09). Examples of serial CloFAL assaywaveforms in individual patients during longitudinal follow-up areshown in Fig. 4.
With a median duration of follow-up of 2 years (range: 0.3 –
5 years) in the cohort, recurrent VTE occurred in 6 children (12%),including 3 with APS and an additional two who were re-exposed to aclinical trigger (i.e.: insertion of a central venous catheter; adminis-tration of L-asparaginase) associated with the initial event. Therewere no discernible clinical risk factors or thrombophilia panelprofiles that distinguished these patients from those withoutrecurrent VTE. Additionally, the small number of children withrecurrence did not permit formal analysis of associations with AUCand FI2.
Discussion
The present work provides data in support of the analyticsensitivity of the CloFAL assay AUC to hypercoagulable states andthe assay's FI2 to both hyper- and hypofibrinolytic conditions.Furthermore, by means of a prospective inception cohort of pediatricacute VTE, we have shown that AUC is significantly increased(denoting hypercoagulablility) in the acute phase post-event, andthat FI2 is significantly decreased (indicating hypofibrinolysis). Atendency was observed toward decrement in hypercoagulablity andhypofibrinolysis during longitudinal follow-up post-event. However,a slight, transient increase was noted in the proportion of patientswho were hypercoagulable during the early chronic period (3–-12 months following VTE, during which anticoagulation is commonlydiscontinued), and a considerable minority of children exhibitedpersistent hypercoagulability (33%) or hypofibrinolysis (21%) in long-term follow-up, one year or more post-VTE.
These findings are important in their novel demonstration of theutility of a global assay that is (1) suitable for fresh or frozen(including banked/batched) plasma and (2) technologically based onwidely-available spectrophotometry, for the monitoring of overallcoagulative and fibrinolytic capacities in VTE patients. Early work inthis area (which continues presently in some research laboratories)utilized thromboelastography [16–21]; however, with the exceptionof a plasma-based modification currently under development/validation, this assay requires a fresh whole blood sample, and itsinter-assay coefficient of variation may not permit reliable compar-isons across serial samples obtained in a patient in long-term follow-up. Recent work has emphasized thrombin generation assays[22–32]. Yet, measurement of thrombin generation has importantpotential limitations regarding lack of analytical sensitivity tochanges in fibrinogen concentration and activity [21,33], which arelikely to strongly contribute to the hypercoagulable state–particularlyin the young, wherein underlying conditions predisposing to VTEfrequently induce alterations in fibrinogen. By contrast, as shown inthis work, the CloFAL assay AUC and FI2 were both strongly correlatedwith fibrinogen.
Our observation of a statistically significant reduction in fibrino-lytic activity in pediatric VTE patients relative to healthy controls,particularly early in the course post-VTE, is also novel. Thishypofibrinolysis is likely contributed to by a relative increase infibrinogen levels, as observed here. Given the findings of acutelyincreased fibrinogen and AUC, the hypofibrinolytic state may also beinfluenced by thrombin-activatable fibrinolytic inhibitor (TAFI,
whose impact on the CloFAL assay has been indirectly shown inprior work [8]), or by plasminogen activator inhibitor-1 (PAI-1,whose influence on the assay is illustrated in Fig. 2B). Prior work bythe group of Lisman and co-workers using a similar turbidimetricplasma assay methodology to the CloFAL assay, but a distincttechnique for calculating fibrinolytic capacity, has shown thathypofibrinolysis was associated with increased risk of both incident[34] and recurrent [35] VTE in adults. In the latter study, hypofi-brinolysis (using a clot lysis time cutoff of the 90th percentile amonghealthy controls) was observed in 16% of patients with VTE who wereassessed at least 3 months from the time of event (including somewho were undergoing continued oral vitamin K antagonist therapy).Recently, this group has shown that this hypofibrinolytic state in VTEpatients is attributable, in part, to both TAFI and PAI-1 [36]. In otherwork, using an assay methodology similar to that of the CloFAL assaybut a distinct calculation of fibrinolytic capacity, Rooth and colleagueshave also recently observed hypofibrinolysis in both the acute andconvalescent phases of ischemic stroke in a prospective series ofelderly adults [37].
Limitations of the present study include the sample size which,although relatively small, is nevertheless among the largest prospec-tive inception cohort studies of pediatric VTE to employ serialevaluation of coagulative and fibrinolytic testing. In addition, giventhat children were not urged to have research samples obtainedduring standardized follow-up visits wherein venipuncture was notalready being performed for clinical purposes, our findings are limitedby an emphasis on aggregative comparisons grouped by time point,rather than averaged per-patient changes over time; further studiesare justified in which research sampling is performed at all timepoints. Notwithstanding these limitations, our findings indicate theutility of the CloFAL assay in monitoring plasma coagulative andfibrinolytic capacities in children with VTE, and in appreciating thepathophysiological contribution of changes in fibrinogen thereto.Studies of the potential role of the CloFAL assay in outcome predictionare ongoing, including a sub-study of the Kids-DOTT trial (www.kids-dott.net). If shown prognostic for pediatric recurrent VTE, it is hopedthat the determination of persistent hypercoagulability by CloFALassay following VTE in children (as has been the case for D-dimer inspontaneous DVT in adults) can play an important role in further risk-stratifying duration of anticoagulant therapy in future randomizedcontrolled clinical trials.
Conflict of Interest Statement
None of the authors have conflicts of interest with the referencedmanuscript.
References
[1] Raffini L, Huang YS, Witmer C, Feudtner C. Dramatic increase in venousthromboembolism in children's hospitals in the United States from 2001 to2007. Pediatrics 2009;124:1001–8.
[2] Monagle P, Chalmers E, Chan A, DeVeber G, Kirkham F, Massicotte P, et al.Antithrombotic therapy in neonates and children: American College of ChestPhysicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest2008;133(6 Suppl.):887S–968S.
[3] Pipe S, Goldenberg NA. Acquired disorders of hemostasis. In: Orkin SH, GinsburgD, Nathan DG, Look AT, Fisher DE, Lux SE, editors. Nathan and Oski's Hematologyof Infancy and Childhood. 7th edition. Cambridge, MA: Elsevier; 2008.
[4] Goldenberg NA, Knapp-Clevenger R, Manco-Johnson MJ. Elevated plasma factorVIII and D-dimer levels and poor outcomes of thrombosis in children. N Engl JMed 2004;351:1081–8.
[5] Goldenberg NA. Thrombophilia states andmarkers of coagulation activation in theprediction of outcomes of venous thromboembolism in children: a comparativeanalysis with respect to adult evidence. Hematology Am Soc Hematol EducProgram 2008:236–44.
[6] Palareti G, Cosmi B, Legnani C, Tosetto A, Brusi C, Iorio A, et al. D-dimer testing todetermine the duration of anticoagulation therapy. N Engl J Med 2006;355:1780–9.
[7] Goldenberg NA, HathawayWE, Jacobson L, Manco-JohnsonMJ. A new global assayof coagulation and fibrinolysis. Thromb Res 2005;116:345–56.

349C. Bombardier et al. / Thrombosis Research 130 (2012) 343–349
[8] Goldenberg NA, Bombardier C, Hathaway WE, McFarland K, Jacobson L,Manco-Johnson MJ. Influence of factor IX on overall plasma coagulability andfibrinolytic potential as measured by global assay: monitoring in haemophilia B.Haemophilia 2008;14:68–77.
[9] Goldenberg NA, Hathaway WE, Jacobson L, McFarland K, Manco-Johnson MJ.Influence of factor VIII on overall coagulability and fibrinolytic potential ofhaemophilic plasma as measured by global assay: monitoring in haemophilia A.Haemophilia 2006;12:605–14.
[10] Santoro C, Simpson ML, Goldenberg NA, Jacobson L, Villalobos-Menuey L,Manco-Johnson MJ. Enhanced understanding of pathophysiology and phenotypein congenital afibrinogenemia using multiple global assays of coagulation. JThromb Haemost 2011;9(Suppl. 2):945.
[11] Bland JM, Altman DG. Statistical methods for assessing agreement between twomethods of clinical measurement. Lancet 1986;1:307–10.
[12] Manco-Johnson MJ, Nuss R, Jacobson LJ. Heparin neutralization is essential foraccurate measurement of factor VIII activity and inhibitor assays in blood samplesdrawn from implanted venous access devices. J Lab Clin Med 2000;136:74–9.
[13] He S, Zhu K, Skeppholm M, Vedin J, Svensson J, Egberg N, et al. A global assay ofhaemostasis which uses recombinant tissue factor and tissue-type plasminogenactivator to measure the rate of fibrin formation and fibrin degradation in plasma.Thromb Haemost 2007;98:871–82.
[14] Simpson ML, Goldenberg NA, Jacobson LJ, Bombardier CG, Hathaway WE,Manco-Johnson MJ. Simultaneous thrombin and plasmin generation capacitiesin normal and abnormal states of coagulation and fibrinolysis in children andadults. Thromb Res 2011;127:317–23.
[15] Smith AA, Jacobson LJ, Miller BI, Hathaway WE, Manco-Johnson MJ. A neweuglobulin clot lysis assay for global fibrinolysis. Thromb Res 2003;112:329–37.
[16] Kapoor S, Pal S, Sahni P, Chattopadhyay TK. Thromboelastographic evaluation ofcoagulation in patients with extrahepatic portal vein thrombosis andnon-cirrhotic portal fibrosis: a pilot study. J Gastroenterol Hepatol 2009;24:992–7.
[17] Koopman K, Uyttenboogaart M, Hendriks HG, Luijckx GJ, Cramwinckel IR,Vroomen PC, et al. Thromboelastography in patients with cerebral venousthrombosis. Thromb Res 2009;124:185–8.
[18] Spiezia L, Marchioro P, Radu C, Rossetto V, Tognin G, Monica C, et al. Whole bloodcoagulation assessment using rotation thrombelastogram thromboelastometry inpatients with acute deep vein thrombosis. Blood Coagul Fibrinolysis 2008;19:355–60.
[19] Wen YR, Ho WY, Sun WZ, Or CH, Yeh M, Yao WC, et al. Thrombo-elastographicstudy of thrombosis in the implantable central venous access device. ActaAnaesthesiol Sin 1997;35:223–8.
[20] Kupesiz OA, Chitlur MB, Hollon W, Tosun O, Thomas R, Warrier I, et al. Fibrinolyticparameters in children with noncatheter thrombosis: a pilot study. Blood CoagulFibrinolysis 2010;21:313–9.
[21] Santoro C, Simpson ML, Goldenberg NA, Jacobson L, Villalobos-Menuey L,Manco-Johnson MJ. Enhanced understanding of pathophysiology and phenotypein congenital afibrinogenemia using multiple global assays of coagulation. JThromb Haemost 2011;9(Suppl. 2):943 [Abstract].
[22] Eichinger S, Heinze G, Jandeck LM, Kyrle PA. Risk assessment of recurrence inpatients with unprovoked deep vein thrombosis or pulmonary embolism: theVienna prediction model. Circulation 2010;121:1630–6.
[23] Chaireti R, Jennersjö C, Lindahl TL. Thrombin generation and D-dimer concentra-tions in a patient cohort investigated for venous thromboembolism. Relations tovenous thrombosis, factor V Leiden and prothrombin G20210A. The LIST study.Thromb Res 2009;124:178–84.
[24] ten Cate-Hoek AJ, Dielis AW, Spronk HM, van Oerle R, Hamulyák K, Prins MH, et al.Thrombin generation in patients after acute deep-vein thrombosis. ThrombHaemost 2008;100:240–5.
[25] Besser M, Baglin C, Luddington R, van Hylckama Vlieg A, Baglin T. High rate ofunprovoked recurrent venous thrombosis is associated with highthrombin-generating potential in a prospective cohort study. J Thromb Haemost2008;6:1720–5.
[26] Tripodi A, Legnani C, Chantarangkul V, Cosmi B, Palareti G, Mannucci PM. Highthrombin generation measured in the presence of thrombomodulin is associatedwith an increased risk of recurrent venous thromboembolism. J Thromb Haemost2008;6:1327–33.
[27] van Hylckama Vlieg A, Christiansen SC, Luddington R, Cannegieter SC, RosendaalFR, Baglin TP. Elevated endogenous thrombin potential is associated with anincreased risk of a first deep venous thrombosis but not with the risk ofrecurrence. Br J Haematol 2007;138:769–74.
[28] Lincz LF, Lonergan A, Scorgie FE, Rowlings P, Gibson R, Lawrie A, et al. Endogenousthrombin potential for predicting risk of venous thromboembolism in carriers offactor V Leiden. Pathophysiol Haemost Thromb 2006;35:435–9.
[29] Tripodi A, Martinelli I, Chantarangkul V, Battaglioli T, Clerici M, Mannucci PM. Theendogenous thrombin potential and the risk of venous thromboembolism.Thromb Res 2007;121:353–9.
[30] Dargaud Y, Trzeciak MC, Bordet JC, Ninet J, Negrier C. Use of calibrated automatedthrombinography +/− thrombomodulin to recognise the prothrombotic pheno-type. Thromb Haemost 2006;96:562–7.
[31] Hron G, Kollars M, Binder BR, Eichinger S, Kyrle PA. Identification of patients atlow risk for recurrent venous thromboembolism by measuring thrombingeneration. JAMA 2006;296:397–402.
[32] Brummel-Ziedins KE, Vossen CY, Butenas S, Mann KG, Rosendaal FR. Thrombingeneration profiles in deep venous thrombosis. J Thromb Haemost 2005;3:2497–505.
[33] Simpson ML, Goldenberg NA, Jacobson LJ, Bombardier CG, Hathaway WE,Manco-Johnson MJ. Simultaneous thrombin and plasmin generation capacitiesin normal and abnormal states of coagulation and fibrinolysis in children andadults. Thromb Res 2011;127:317–23.
[34] Lisman T, de Groot PG, Meijers JC, Rosendaal FR. Reduced plasma fibrinolyticpotential is a risk factor for venous thrombosis. Blood 2005;105:1102–5.
[35] Meltzer ME, Bol L, Rosendaal FR, Lisman T, Cannegieter SC. Hypofibrinolysis as arisk factor for recurrent venous thrombosis; results of the LETS follow-up study. JThromb Haemost 2010;8:605–7.
[36] Meltzer ME, Lisman T, de Groot PG, Meijers JC, le Cessie S, Doggen CJ, et al. Venousthrombosis risk associated with plasma hypofibrinolysis is explained by elevatedplasma levels of TAFI and PAI-1. Blood 2010;116:113–21.
[37] Rooth E, Wallen NH, Blombäck M, He S. Decreased fibrin network permeabilityand impaired fibrinolysis in the acute and convalescent phase of ischemic stroke.Thromb Res 2011;127:51–6.