Embed Size (px)
DESCRIPTION
international guidelines onvenous thromboembolism prenetion in critical care patients
Citation preview

Guidelines for Prevention of Venous Thromboembolism in Critical Care Patients
D. Sandesc“Victor Babes” University of Medicine and Pharmacy, Timisoara

Guidelines for Prevention of Venous Thromboembolism in Critical Care Patients
Main sources. General recommendations
VTE prevention in the ICU VTE prevention guidelines in severe
sepsis VTE prevention in politrauma VTE prevention in burn patients

Evidence-Based Clinical Practice Guidelines of the American College of Chest Physicians
(8th Edition)
*William H. Geerts, David Bergqvist, Graham F. Pineo, John A. Heit,Charles M. Samama, Michael R. Lassen and Clifford W. Colwell
Chest 2008;133;381-453 DOI 10.1378/chest.08-0656http://chestjournal.org/cgi/content/abstract/133/6_suppl/381S
Downloaded from chestjournal.org on June 25, 2008
Prevention of Venous Thromboembolism

Prevention and treatment of Venous Thromboembolism
International Consensus Statement (Guidelines according to scientific evidence)
Int.Angiol 2006, 25:101-161
Nicolaides AN, Fareed J, Kakkav AK, et. al.



1Cohen AT. Presented at the 5th Annual Congress of the European Federation of Internal Medicine; 2005.2Eurostat statistics on health and safety 2001. Available from: http://epp.eurostat.cec.eu.int.
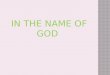
Annual mortality due to VTE in Europe (25 countries)
Mortality due to VTE1 in hospital 261,477 ambulatory 108,535
Combined mortality due to : AIDS 5,8602
Breast cancer 86,8312
Prostate cancer 63,6362
Traffic accidents 53,5992
209,926

The majority of the postoperative episodes of VTE
are undetectable
10–20%symptomatic
80–90% asymptomatic

Nu
mb
er o
f p
atie
nts
wit
h f
atal
P
Ep < 0.005
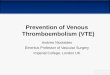
Postoperative prophylaxis of the fatal PE using low dose unfractioned Heparin (Kakkar , Lancet ,
1975)
16
2
00
22
44
66
88
1010
1212
1414
1616
1818
ControlControl NFH
Kakkar VV, et al. Lancet. 1975;2:45Low doses of UFH save 7 lives each 1,000 patients who have undergone surgery.
PE = Pulmonary Embolism; UFH = Unfractioned Heparin
(N = 2,076) (N = 2,045)

Risk Factors for VTE (1)
Surgery Trauma (major trauma or lower extremity injury) Cancer (active or occult) Cancer therapy (hormonal, chemotherapy, angiogenesis inhibitors,
radiotherapy) Previous VTE Venous compression (tumor, haematoma, arterial abnormality) Increasing age Pregnancy and the postpartum period Estrogen-containing oral contraceptives or hormone replacement
therapy

Risk Factors for VTE (2)
Selective estrogen receptor modulators Erythropoiesis-stimulating agents Acute medical illness Inflammatory bowel disease Inherited or acquired thrombophilia Nephrotic syndrome Myeloproliferative disorders Paroxysmal nocturnal hemoglobinuria Obesity

Specific risk factors for VTE in the ICU
Central vascular access Mechanical ventilation Muscular paralysis Extrarenal epuration techniques Prolonged immobilisation

Approximate Risks of DVT in Hospitalized Patients*
Patient Group DVT Prevalence, %
Medical patients 10-20
General surgery 15-40
Major gynecologic surgery 15-40
Major urologic surgery 15-40
Neurosurgery 15-40
Stroke 20-50
Hip or knee arthroplasty, HFS 40-60
Major trauma 40-80
SCI 60-80
Critical care patients 10-80
* Rates based on objective diagnostic screening for asymptomatic DVT in patients not receiving thromboprophylaxis

Levels of Thromboembolic Risk and Recommended Thromboprophylaxis in Hospitalized Patients *

Hospital ThromboprophylaxisPolicy
For every general hospital, active strategy that addresses the prevention of VTE is to be developed (Grade 1A).
Local strategy, in form of a written, institution-wide thromboprophylaxis policy (Grade 1C).
The use of strategies shown to increase thromboprophylaxis adherence, including the use of computer decision support systems (Grade 1A), preprinted orders (Grade 1B), and periodic audit and feedback (Grade 1C). Passive methods such as distribution of educational materials or educational meetings are not recommended as sole strategies to increase adherence to thromboprophylaxis (Grade 1B).

Mechanical Methods ofThromboprophylaxis
Recommended primarily in patients at high risk of bleeding (Grade 1A), or possibly as an adjunct to anticoagulant-based thromboprophylaxis (Grade 2A).
Careful attention to be directed towards ensuring the proper use of, and optimal adherence with, these methods (Grade 1A).
GCS : Gradual Compression Stockings IPC : Intermitent Pneumatic Compression

Aspirin as Thromboprophylaxis
We recommend against the use of aspirin alone as prophylaxis against VTE for any patient group (Grade 1A)

Anticoagulant dosing
We recommend that clinicians follow the manufacturer suggested dosing guidelines (Grade 1C)
We recommend renal function to be considered when making decisions about the use and/or dose of LMWH, fondaparinux and other antithrombotic drugs (Grade 1A)
*LMWH= Low Molecular Weight Heparin*LDUH= Low Dose Unfractioned Heparin

Use of Antithrombotic Drugs for Prophylaxis in Patients with Renal Impairment
Moderate (ClCr 30–50 mL/min) and mild renal impairment (ClCr 50–80 mL/min)
Severe renal impairment(ClCr < 30 mL/min)
Enoxaparin1 No adjustment needed “dose to be adjusted”Dose is being specified.
Dalteparin2 No information available “To be used with precaution”Dose is not being specified.
Tinzaparin3 No information available “To be used with precaution”Dose is not being specified.
Fondaparinux Used with precaution in moderate renal impairment
“Contraindicated”
1Clexane®-Lovenox® prescribing information. sanofi-aventis.2Fragmin® prescribing information. Pfizer.
3Innohep® prescribing information. Pharmion. 4Arixtra® prescribing information. GlaxoSmithKline.

Thromboprophylaxis and body weight
Men < 57 kg and Women < 45 kg)
Obese(IMC 30–48 kg/m2)
Enoxaparin1 No adjustment needed
No adjustment needed
Dalteparin2 No information available
No information available
Tinzaparin3 No information available
No information available
Fondaparinux
“Not if < 50 kg No information available
1Clexane®-Lovenox® prescribing information. Sanofi-aventis.2Fragmin® prescribing information. Pfizer.
3Innohep® prescribing information. Pharmion. 4Arixtra® prescribing information. GlaxoSmithKline.

Guidelines for Prevention of Venous Thromboembolism in Critical Care Patients
Main sources. General recommendations
VTE prevention in the ICU VTE prevention in severe sepsis VTE prevention in politrauma VTE prevention in burn patients

Critical Care (1)
Patients admitted to a critical care unit:- recommended routine assessment for VTE risk and routine thromboprophylaxis (Grade 1A).
For critical care patients who are at moderate risk for VTE (eg, medically ill or postoperative general surgery patients):
- LMWH or LDUH thromboprophylaxis (Grade 1A).

Critical Care (2)
Critical care patients who are at higher risk (eg, following major trauma or orthopedic surgery):- LMWH thromboprophylaxis (Grade 1A).
Critical care patients who are at high risk for bleeding:- recommended the optimal use of mechanical thromboprophylaxis at least until the bleeding risk decreases (Grade 1A). When the high bleeding risk decreases, pharmacologic thromboprophylaxis is recommended to be substituted for or added to the mechanical thromboprophylaxis (Grade 1C).

Guidelines for Prevention of Venous Thromboembolism in Critical Care Patients
Main sources. General recommendations
VTE prevention in the ICU VTE prevention guidelines in severe
sepsis VTE prevention in politrauma VTE prevention in burn patients

VTE prevention in severe sepsis (Surviving Sepsis Campaign 2008 )
“…a) Low-dose unfractionated heparin (UFH) administered twice or three times per day; or b) Daily low-molecular weight heparin (LMWH) unless there are contraindications (i.e., thrombocytopenia,
If contraindication for heparin use : mechanical prophylactic device, unless contraindicated (grade 1A).
Very high-risk patients (history of DVT, trauma, or orthopedic surgery) : a combination of pharmacologic and mechanical therapy to be used unless contraindicated or not practical (grade 2C).
Patients at very high risk : LMWH to be used rather than UFH as LMWH is proven superior in other high-risk patients (grade 2C).

Guidelines for Prevention of Venous Thromboembolism in Critical Care Patients
Main sources. General recommendations
VTE prevention in the ICU VTE prevention guidelines in severe
sepsis VTE prevention in trauma VTE prevention in burn patients

Trauma(1) For all major trauma patients:
- recommended: routine thromboprophylaxis if possible (Grade 1A). For major trauma patients in the absence of a major contraindication:
- LMWH thromboprophylaxis starting as soon as it is considered safe to do so (Grade 1A)
- An acceptable alternative is the combination of LMWH and the optimal use of a mechanical method of thromboprophylaxis (Grade 1B).
If LMWH thromboprophylaxis is contraindicated due to active bleeding or high risk for clinically important bleeding:- Mechanical thromboprophylaxis with IPC or GCS alone (Grade 1B). When the high bleeding risk decreases, we recommend pharmacologic thromboprophylaxis to be substituted for or added to the mechanical thromboprophylaxis (Grade 1C).

Trauma(2)
Trauma patients :- not recommended: the use of an IVC filter as thromboprophylaxis (Grade 1C).
For major trauma patients:- recommended: the continuation of thromboprophylaxis until hospital discharge (Grade 1C). For trauma patients with impaired mobility who undergo inpatient rehabilitation, we suggest continuing thromboprophylaxis with LMWH or a VKA (target INR, 2.5; range, 2.0 to 3.0) (Grade 2C).

Acute Spinal Cord Injury(1)
For all patients with acute SCI: - routine thromboprophylaxis recommended (Grade 1A).
- thromboprophylaxis with LMWH, commenced once primary hemostasis is evident (Grade 1B). Alternatives include the combined use of IPC and either LDUH (Grade 1B) or LWMH (Grade 1C).
SCI with high bleeding risk :- recommended: the optimal use of IPC and/or GCS (Grade 1A). When the high bleeding risk decreases, we recommend pharmacologic thromboprophylaxis to be substituted for or added to the mechanical thromboprophylaxis (Grade 1C).

Acute Spinal Cord Injury(2)
For patients with an incomplete SCI associated with evidence of a spinal hematoma on CT or MRI:- mechanical thromboprophylaxis instead of anticoagulant thromboprophylaxis at least for the first few days after injury (Grade 1C).
Following acute SCI:- recommended against: the use of LDUH alone (Grade 1A).
For patients with SCI:- recommended against: the use of an IVC filter as thromboprophylaxis (Grade 1C).
For patients undergoing rehabilitation following acute SCI:- recommended: the continuation of LMWH thromboprophylaxis or conversion to an oral VKA (INR target, 2.5; range, 2.0 to 3.0) (Grade 1C).

Guidelines for Prevention of Venous Thromboembolism in Critical Care Patients
Main sources. General recommendations
VTE prevention in the ICU VTE prevention guidelines in severe
sepsis VTE prevention in politrauma VTE prevention in burn patients

Burns
Burn patients who have additional risk factors for VTE, including one or more of the following: advanced age, morbid obesity, extensive or lower-extremity burns, concomitant lower-extremity trauma, use of a femoral venous catheter, and/or prolonged immobility:- recommended: routine thromboprophylaxis if possible (Grade 1A).- recommended: the use of either LMWH or LDUH, starting as soon as it is considered safe to do so (Grade 1C).
Burn patients who have a high bleeding risk:- recommended: mechanical thromboprophylaxis with GCS and/or IPC until the bleeding risk decreases (Grade 1A).

VTE prevention in critical patients-conclusions
VTE - major public health problem VTE - avoidable disease ! VTE in ICU – special category , needs
individual , dynamic evaluation VTE prevention in special populations
(renal failure ,extreme weights, etc): use the products with adapted doses
Institutional and national strategy necessary