Embed Size (px)
Citation preview

Venous Thromboembolism in Intensive Venous Thromboembolism in Intensive Care MedicineCare Medicine
Kenneth E. Wood, DOKenneth E. Wood, DOProfessor of Medicine and AnesthesiologyProfessor of Medicine and Anesthesiology
Director of Critical Care Medicine and Respiratory Director of Critical Care Medicine and Respiratory CareCare
The Trauma and Life Support CenterThe Trauma and Life Support CenterUniversity of Wisconsin Hospital and ClinicsUniversity of Wisconsin Hospital and Clinics

Venous Thromboembolism in ICUVenous Thromboembolism in ICU
Pathophysiology of ThrombosisPathophysiology of ThrombosisProphylaxis and DVTProphylaxis and DVTPathophysiology of Pulmonary EmbolismPathophysiology of Pulmonary EmbolismPulmonary Embolism DiagnosticsPulmonary Embolism DiagnosticsPulmonary Embolism TherapeuticsPulmonary Embolism Therapeutics

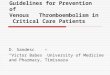
ICU Venous Thromboembolism OverviewICU Venous Thromboembolism Overview
Diagnostics
Therapeutics
Secondary Development
Virchows Triad
Risk Factors Prophylaxis
Cardiac Echo Spiral CTDoppler US D-dimerAngiogram
Warfarin
UF Heparin
LMWH LepirudinArgatroban
Thrombolytics
• Hypercoaguable (25%)• Stasis• Vessel Damage
Primary Presentation
Respiratory Failure
Hemodynamic Instability

Venous Thromboembolism in ICUVenous Thromboembolism in ICU
Pathophysiology of Thrombosis

Venous ThromboembolismVenous Thromboembolism
“ “ The detachment of larger or smaller fragments from the The detachment of larger or smaller fragments from the end of the softening thrombus are carried along by the end of the softening thrombus are carried along by the current of blood and driven in remote vessels. This gives current of blood and driven in remote vessels. This gives rise to the very frequent process upon which I have rise to the very frequent process upon which I have bestowed the name EMBOLIA.”bestowed the name EMBOLIA.”
Vessel Injury Stasis Hyper-coagulability
Virchow 1846
Acquired Inherited

Virchows TriadVirchows Triad
HypercoagulableHypercoagulable
StasisStasis
Vessel DamageVessel Damage

Intensivists General ParadigmIntensivists General Paradigm
Pipes
Stuff Flow

Hematology 101 for IntensivistsHematology 101 for Intensivists
= Biologically Active Conduit
Clot Bleed
Stuff
Pipe
Flow
Stuff
Coagulation fibrinolysis

Hematology 101 for IntensivistsHematology 101 for Intensivists
= Biologically Active Conduit
Bleed
Stuff
Pipe
Flow (stasis)
Stuff
Coagulation fibrinolysis
Clot

Pathogenesis of Venous Pathogenesis of Venous Thromboembolism Thrombogenic StimuliThromboembolism Thrombogenic StimuliEndothelial DamageEndothelial Damage Exposure of tissue factor/subendothelial matrixExposure of tissue factor/subendothelial matrix Hypoxia Hypoxia receptors for leukocytes receptors for leukocytes Activation by inflammatory cytokines (IL-1, TNF)Activation by inflammatory cytokines (IL-1, TNF) Express tissue factorExpress tissue factor Internalize thrombomodulinInternalize thrombomodulin Release PAI-1Release PAI-1
Activation of CoagulationActivation of Coagulation Inflammation (IL-1, TNF)Inflammation (IL-1, TNF)
♦ Monocytes Monocytes tissue factor and tethered leukocytes tissue factor and tethered leukocytes♦ Internalize thrombomodulin (Internalize thrombomodulin ( Protein C activation) Protein C activation)♦ Shedding endothelial protein C receptorShedding endothelial protein C receptor
Coagulation cascade activationCoagulation cascade activation
Clot
Bleed
Adapted from Wertz Adapted from Wertz Lung Biology Health DiseaseLung Biology Health Disease 2003 2003

Pathogenesis of Venous Pathogenesis of Venous Thromboembolism Thrombogenic StimuliThromboembolism Thrombogenic Stimuli
Blood Flow (Stasis)Blood Flow (Stasis) SystemicSystemic
♦ Immobilization pools blood in calve venous sinusesImmobilization pools blood in calve venous sinuses♦ Increased blood viscosityIncreased blood viscosity
LocalLocal♦ Hypoxia of valve cusps produces tissue factor and Hypoxia of valve cusps produces tissue factor and
activates coagulationactivates coagulation♦ Accumulation of clotting factors in venous sinuses Accumulation of clotting factors in venous sinuses
of calf or valve cusp pockets of calf or valve cusp pockets
Adapted from Wertz Lung Biology Health Disease 2003
Clot
Bleed

ICU Venous ThromboembolismICU Venous Thromboembolism
Adopted from Dalen Adopted from Dalen CHESTCHEST 2002; 122:1440-56 2002; 122:1440-56
ICU Risk FactorsICU Risk Factors HypercoagHypercoag StasisStasis VesselVessel
Major SurgeryMajor Surgery XX XX XX
TraumaTrauma XX XX XX
MI/CHFMI/CHF XX
StrokeStroke XX
BurnsBurns XX
SepsisSepsis XX XX
CatheterCatheter XX XX XX

Venous Thromboembolism in ICUVenous Thromboembolism in ICU
Prophylaxis and DVT

Importance of DVT ProphylaxisImportance of DVT Prophylaxis
Acute DVT/PE preventionAcute DVT/PE prevention
Valvular DamageValvular Damage
Symptomatic proximal DVT can be an extension of Symptomatic proximal DVT can be an extension of distal DVT that was previously asymptomaticdistal DVT that was previously asymptomatic
Significant number of fatal PE’s Significant number of fatal PE’s NOTNOT preceded by preceded by symptomatic DVTsymptomatic DVT
Most preventable cause of hospital associated death Most preventable cause of hospital associated death in medical patientsin medical patientsPEPE
Recurrence
Post-phlebitic syndrome
DVT
PE

Asymptomatic DVT ICU AdmitAsymptomatic DVT ICU Admit
Patient PopulationPatient Population % DVT% DVT
Surgical ICUSurgical ICU 7.5%7.5%Harris Harris J Vas SurgJ Vas Surg 1997; 26:734-9 1997; 26:734-9
Respiratory ICURespiratory ICU 10.7%10.7%Schonhster Schonhster RespirationRespiration 1998; 65:173-7 1998; 65:173-7
MICU-Resp fail/ventMICU-Resp fail/vent 19%19%Goldberg Goldberg Am J Resp CCMAm J Resp CCM 1996; 153:A94 1996; 153:A94
MICU-Resp fail/ventMICU-Resp fail/vent 6.3%6.3%Fraisse Fraisse Am J Resp CCMAm J Resp CCM 2000; 161:1109-14 2000; 161:1109-14

Prospective Eval DVT Critically Ill Prospective Eval DVT Critically Ill Non-ProphylaxedNon-Prophylaxed
StudyStudy ControlControl ScreenScreen ## % DVT% DVTMoser 1981Moser 1981 RespiratoryRespiratory Fib LSFib LS 2323 13%13%
Cade 1982Cade 1982 GeneralGeneral Fib LSFib LS 6060 29%29%
Hirsch 1995Hirsch 1995 MedicalMedical USUS 104104 32%32%
Kapoor 1999Kapoor 1999 MedicalMedical USUS 390390 31%31%
Fraisse 2000Fraisse 2000 Vent COPDVent COPD VenogramVenogram 8585 28%28%

Natural History of DVTNatural History of DVT
132 Surgical patients no prophylaxis
56%
No PE (5)
44%
PE (4)
42% Calf only (17)
23% propagation Popliteal/femoral (9)
35% Calf with spontaneous
lysis (14)
30%
DVT (40)
70%
No DVT (92)
Kakkar Kakkar LancetLancet 1969; 6:230-32 1969; 6:230-32

Incidence of VTEIncidence of VTEMajor Trauma Major Trauma WithoutWithout Prophylaxis Prophylaxis
• 50% face chest abdomen50% face chest abdomen• 54% major head injury54% major head injury• 62% spinal injury62% spinal injury
69% lower extremity ortho69% lower extremity ortho
61% pelvic fractures61% pelvic fractures
80% femoral fractures80% femoral fractures
77% tibial fractures77% tibial fractures
Incidence
Geerts Geerts NEJM NEJM 1994; 331:1601-16061994; 331:1601-1606
Lower leg DVT 58%, proximal DVT 18%Lower leg DVT 58%, proximal DVT 18%
Vast majority clinically Vast majority clinically notnot apparent apparent

DVT Prophylaxis Trials in Critically IllDVT Prophylaxis Trials in Critically Ill
Geerts Geerts JJ Crit CareCrit Care 2002; 17:95-104 2002; 17:95-104
StudyStudy ControlControl % DVT% DVT TreatmentTreatment % DVT% DVT
Cade 82Cade 82 PlaceboPlacebo 29%29% UF HeparinUF Heparin 13%13%
Kapoor 99Kapoor 99 PlaceboPlacebo 31%31% UF HeparinUF Heparin 11%11%
Fraisse 00Fraisse 00 Placebo Placebo 28%28% NadroparinNadroparin 15%15%

Femoral Catheter Associated DVTFemoral Catheter Associated DVT
StudyStudy PopulationPopulation ScreenScreen % DVT% DVT
Meredith 93Meredith 93 Trauma 8.5 FrTrauma 8.5 Fr USUS 14%14%
Trottier 95Trottier 95 Med/SurgMed/Surg USUS 25%25%
Durbec 97Durbec 97 Med/SurgMed/Surg VenogramVenogram 7% Femoral7% Femoral
17% Tibial17% Tibial
Durbec 97Durbec 97 Med/SurgMed/Surg VenogramVenogram 9% Femoral9% Femoral
26% Tibial26% Tibial
Jogut 00Jogut 00 Med/SurgMed/Surg USUS 11%11%

Pulmonary Embolism in Patients Pulmonary Embolism in Patients with Upper Extremity Catheter DVTwith Upper Extremity Catheter DVT
86 consecutive patients catheter DVT86 consecutive patients catheter DVT
15% high probability (PE) V/Q scan 15% high probability (PE) V/Q scan (13/86)(13/86)
31% PE patients symptomatic (4/13)31% PE patients symptomatic (4/13)
15% PE patient mortality (2/13) despite full 15% PE patient mortality (2/13) despite full anticoagulationanticoagulation
DVT polyvinyl chloride or polyethyleneDVT polyvinyl chloride or polyethyleneMonreal Monreal Throm HaemostThrom Haemost 1994; 72:548-50 1994; 72:548-50

Autopsy Studies PE Critically IllAutopsy Studies PE Critically Ill
PE AutopsyPE Autopsy
StudyStudy ICU SettingICU Setting PresentPresent FatalFatal
Neuhaus 1978Neuhaus 1978 Med/SurgMed/Surg 27%27% 12%12%
Moser 1981Moser 1981 RespiratoryRespiratory 20%20% 0%0%
Pingleton 1981Pingleton 1981 MedicalMedical 23%23% ----
Cullin 1986Cullin 1986 SurgicalSurgical 10%10% 1%1%
Blosser 1998Blosser 1998 MedicalMedical 7%7% 2%2%
Willemsen 2000Willemsen 2000 SurgicalSurgical 8%8% 3%3%
Geerts J Geerts J Crit CareCrit Care 2002; 17:95-104 2002; 17:95-104

VTE ProphylaxisVTE Prophylaxis
Pharmacologic
Unfractionated heparin
Low molecular weight heparin
Vit K Antagonists
Mechanical
Graduated Compression Stockings
Intermittent Pneumatic Compression Devices
IVC filters

Thromboembolism RiskThromboembolism RiskSurgical Patients Surgical Patients Prophylaxis Prophylaxis
DVT, %DVT, % PE, %PE, %
CalfCalf ProximalProximal ClinicalClinical FatalFatal
Low RiskLow Risk 2%2% 0.4%0.4% 0.2%0.2% <0.01%<0.01%
Minor Surgery < 40 no risk factorsMinor Surgery < 40 no risk factors
Moderate RiskModerate Risk 10-20 %10-20 % 2-4%2-4% 1-2%1-2% 0.1-0.4%0.1-0.4%
Minor surgery risk factorsMinor surgery risk factors
Surgery 40-60 no risk factorsSurgery 40-60 no risk factors
High RiskHigh Risk 20-40%20-40% 4-8%4-8% 2-4%2-4% 0.4-1.0%0.4-1.0%
Surgery >60, 94 40-60 with additional risk factors (prior VTE, cancer, hypercoagulability)Surgery >60, 94 40-60 with additional risk factors (prior VTE, cancer, hypercoagulability)
Highest RiskHighest Risk 40-80%40-80% 10-20%10-20% 4-10%4-10% 0.2-5%0.2-5%
Surgery with multiple risk factors (age > 40 yr, cancer, prior VTE)Surgery with multiple risk factors (age > 40 yr, cancer, prior VTE)
Hip or knee arthroplasty, HFSHip or knee arthroplasty, HFS
Major trauma, SCIMajor trauma, SCI
Geerts Geerts CHESTCHEST 2004;126(3)Supplement: 338S-400S 2004;126(3)Supplement: 338S-400S

0
30
40
50
60
70
20
10
Control Heparin
Screening DVT Fatal PE
Pe
rce
nta
ge
60.5
20.3
1.9 0.6
Relative risk reduction 67%
Relative risk reduction 68%
Collins Collins NEJMNEJM 1988; 318:1162-73 1988; 318:1162-73

Trauma and Venous ThromboembolismTrauma and Venous Thromboembolism
Patients recovering from major trauma have Patients recovering from major trauma have highest risk for developing VTE amongst all highest risk for developing VTE amongst all hospitalized patients hospitalized patients (Geerts (Geerts NEJMNEJM 1994; 331:1601-06) 1994; 331:1601-06)
Without prophylaxis, multisystem or major trauma Without prophylaxis, multisystem or major trauma have a DVT risk exceeding 50% have a DVT risk exceeding 50% (Kudsk (Kudsk Am J SurgAm J Surg 1989; 1989; 158:515-19)158:515-19)
PE is the third leading cause of death in trauma PE is the third leading cause of death in trauma patients that survive beyond the first day patients that survive beyond the first day (Acosta (Acosta J Am J Am Coll SurgColl Surg 1998; 186:528-33) 1998; 186:528-33)

Significant Risk Factors and Odds Ratios for Significant Risk Factors and Odds Ratios for Venous Thromboembolism Developed From Venous Thromboembolism Developed From
the National Trauma Data Bankthe National Trauma Data BankRisk Factor (Number at Risk)Risk Factor (Number at Risk) Odds Ratio (95% CI)Odds Ratio (95% CI)
*Age *Age 40y (n=178,851) 40y (n=178,851) 2.29 (2.07 – 2.55)2.29 (2.07 – 2.55)
Pelvic fracture (n=2707)Pelvic fracture (n=2707) 2.93 (2.01 – 4.27)2.93 (2.01 – 4.27)
*Lower extremity fracture (n=63,508)*Lower extremity fracture (n=63,508) 3.16 (2.85 – 3.51)3.16 (2.85 – 3.51)
Spinal cord injury with paralysis (n=2852)Spinal cord injury with paralysis (n=2852) 3.39 (2.41 – 4.77)3.39 (2.41 – 4.77)
*Head injury (AIS score *Head injury (AIS score 3) (n=52,197) 3) (n=52,197) 2.59 (2.31 – 2.90)2.59 (2.31 – 2.90)
*Ventilator days > 3 (n=13,037)*Ventilator days > 3 (n=13,037) 10.62 (9.32 – 12.11)10.62 (9.32 – 12.11)
*Venous injury (n=1450)*Venous injury (n=1450) 7.93 (5.83 – 10.78)7.93 (5.83 – 10.78)
Shock on admission (BP<90 mm Hg) (n=18,510)Shock on admission (BP<90 mm Hg) (n=18,510) 1.95 (1.62 – 2.34)1.95 (1.62 – 2.34)
*Major surgical procedure (n=73,974)*Major surgical procedure (n=73,974) 4.32 (3.91 – 4.77)4.32 (3.91 – 4.77)
Knudson Knudson Ann SurgAnn Surg 2004; 240:490-98 2004; 240:490-98

Knudson Knudson Ann SurgAnn Surg 2004; 240:490-498 2004; 240:490-498
INJURED PATIENT
High Risk Factors(Odds ratio for VTE = 2 – 3)
• Age 40• Pelvic fx• Lower extremity fx• Shock• Spinal cord injury• Head Injury (AIS 3)
Very High Risk Factors(Odds ratio for VTE = 4 - 10)
• Major operative procedure• Venous injury• Ventilator days > 3 • 2 or more high risk factors
Does the patient have contraindication for Heparin?
Does the patient have contraindication for Heparin?
Yes No
YesNo
Mechanical Compression
LMWH*
* Prophylactic dose
LMWH* and Mechanical
Compression
Mechanical Compression and
serial CFDI OR
Temporary IVC filter

Critical Care PatientCritical Care Patient
Mechanical ProphylaxisMechanical Prophylaxis Graduated compression Graduated compression
stockings (GCS)stockings (GCS) Intermittent pneumatic Intermittent pneumatic
compression devices (IPC)compression devices (IPC)
Delayed prophylaxis until high risk Delayed prophylaxis until high risk bleeding abatesbleeding abates
Screen for proximal DVT with Screen for proximal DVT with Doppler US in high risk patientsDoppler US in high risk patients
Low dose unfractionated Low dose unfractionated heparin (LDUH)heparin (LDUH)Low molecular weight Low molecular weight heparin (LMWH)heparin (LMWH)Combination of LMWH and Combination of LMWH and mechanical prophylaxis for mechanical prophylaxis for high risk patients high risk patients
Assess Bleeding Risk
High Low
Adapted from Geerts Adapted from Geerts CHEST CHEST 2003; 124(6)S:357S-363S2003; 124(6)S:357S-363S

Critical Care PatientCritical Care PatientBleedingBleeding
RiskRisk
ThrombosisThrombosis
RiskRisk
Prophylaxis Prophylaxis
RecommendationRecommendation
LowLow ModerateModerate LDH 5000 units SC bidLDH 5000 units SC bid
LowLow HighHigh LMWHLMWH• DalteparinDalteparin• Enoxaparin Enoxaparin
HighHigh ModerateModerate GCS or IPC GCS or IPC LDUH when LDUH when bleeding risk subsidesbleeding risk subsides
HighHigh High High GCS or IPC GCS or IPC LMWH when LMWH when bleeding risk subsidesbleeding risk subsides
Adapted from Geerts Adapted from Geerts CHEST CHEST 2003; 124(6)S:357S-363S2003; 124(6)S:357S-363S

Anti-Xa Activity After Enoxaparin Anti-Xa Activity After Enoxaparin 40 mg SQ40 mg SQ
1.0
Time (hours)
An
ti X
a a
ctiv
ity
(U/m
l)
0 3 6 9 120
0.2
0.4
0.6
0.8Ward (Group 2), n=13
ICU patients (Group 1), n=16
Priglinger Priglinger CCMCCM 2003; 31:1405-09 2003; 31:1405-09

Vena Caval FiltersVena Caval Filters
5 filter types-all equal efficacy5 filter types-all equal efficacy
Pulmonary embolism 2.6%-3.8%Pulmonary embolism 2.6%-3.8%
Deep Venous Thrombosis 6%-32%Deep Venous Thrombosis 6%-32%
Insertion site thrombosis 23%-36%Insertion site thrombosis 23%-36%
Inferior caval thrombosis 3.6%-11.2%Inferior caval thrombosis 3.6%-11.2%
Postphlebitic syndrome 14%-41%Postphlebitic syndrome 14%-41%
Streiff Streiff BloodBlood 2000; 95:3669- 2000; 95:3669-7777

Venous Thromboembolism in ICUVenous Thromboembolism in ICU
Pathophysiology ofPulmonary Embolism


mPAP - LVEDPPVR = CO
Pulmonary Artery Pressure
Q = Flow = Cardiac Output
Incremental Resistance
Mean Closing Pressure
P2 - P1
Q = R
mPAP - LVEDPCO = PVR
Major Pulmonary Embolism

Pulmonary Artery Pressure
Q = Flow = Cardiac Output
Effect of Pulmonary Embolism
Mean Closing
Pressure
Incremental Resistance
Major Pulmonary Embolism


Venous Thromboembolism in ICUVenous Thromboembolism in ICU
Pulmonary Embolism Diagnostics

Massive Pulmonary EmbolismDiagnostics
•History•Physical•CXR•ABG•EKG
Angio
Helical CT
MRI Angio
Echo

Risk Stratification In Risk Stratification In Pulmonary EmbolismPulmonary Embolism
MortalityMortality Clinical StateClinical State
65%65% Cardiac ArrestCardiac Arrest
25%25% ShockShock
15%15% Hypotension without Hypotension without hypoperfusionhypoperfusion
8.1%8.1% Normal BP RV Normal BP RV dysfunctiondysfunction
0-1%0-1% Normal BP and RVNormal BP and RV
Data from MAPPET – Kasper Data from MAPPET – Kasper JACCJACC 1997; 30:1165-1171 1997; 30:1165-1171
High Risk
Low Risk
Predictions
History/Physical
Diagnostic Studies
• EKG
• CXR
• ABG
• Troponin
• BNP
• Echo
Confirmatory Studies
• V/Q
• CT Angio
• Angio


EKG ManifestationsEKG Manifestations
Normal EKGNormal EKG UPET 14% (6% massive and 23% submassive)UPET 14% (6% massive and 23% submassive) PIOPED 30%PIOPED 30%
Rhythm disturbances rareRhythm disturbances rare Atrial fibrillation/flutter 0-5%Atrial fibrillation/flutter 0-5% Blocks or ventricular dysrhythmias non existentBlocks or ventricular dysrhythmias non existent PEA cardiac arrestPEA cardiac arrest
Electrocardiographic Cor PulmonaleElectrocardiographic Cor Pulmonale Right axis, RBBB, SRight axis, RBBB, SIIQQIIIIIITTIIIIII Related to embolism sizeRelated to embolism size
Non-specific ST-T segment changesNon-specific ST-T segment changes UPET 42%UPET 42% PIOPED 49%PIOPED 49%


Chest X-Ray (CXR)Chest X-Ray (CXR)
UPETUPET Normal CXR 34%Normal CXR 34% Parenchymal abnormalities 67%Parenchymal abnormalities 67%
♦ Elevated hemidiaphragm 46%Elevated hemidiaphragm 46%♦ Consolidation 39%Consolidation 39%♦ Pleural effusion 30%Pleural effusion 30%♦ Atelectasis 28%Atelectasis 28%
Vascular abnormalities 37%Vascular abnormalities 37%♦ Diminished vascularity 22%Diminished vascularity 22%♦ Prominent central PA 86%Prominent central PA 86%
PIOPEDPIOPED Normal 16%Normal 16% Atelectasis/parenchymal abnormality 68%Atelectasis/parenchymal abnormality 68% Pleural effusion 48%-blunting 86%Pleural effusion 48%-blunting 86%

Arterial Blood Gas (ABG)Arterial Blood Gas (ABG)
Hypoxia not uniformHypoxia not uniform
PaOPaO22 80 80
♦ 12% UPET12% UPET
♦ 19% PIOPED19% PIOPED
Normal A-a gradient does Normal A-a gradient does NOTNOT exclude PE exclude PE
PIOPED (PaOPIOPED (PaO22>80,PaCO>80,PaCO22>35)>35)
♦ 38% without cardiopulmonary disease38% without cardiopulmonary disease
♦ 14% with cardiopulmonary disease14% with cardiopulmonary disease

D-DimerD-Dimer
Elevated in clinical conditions where fibrin cross Elevated in clinical conditions where fibrin cross links are cleaved by plasminlinks are cleaved by plasminHigh sensitivity and negative predictive valueHigh sensitivity and negative predictive valueLow specificityLow specificityELISAELISA
Accurate quantitative measurementAccurate quantitative measurement Expensive and labor intensive Expensive and labor intensive
Semi-quantitative latex assaySemi-quantitative latex assay Faster and less expensiveFaster and less expensive Unacceptably low sensitivityUnacceptably low sensitivity

Estimating Pre-test Estimating Pre-test Probability of PEProbability of PE
Implicit (empiric)Implicit (empiric) Uses clinician knowledge and experienceUses clinician knowledge and experience Frequent disagreementFrequent disagreement Experience level influences assessmentExperience level influences assessment Estimates trend towards middle few low or high Estimates trend towards middle few low or high
probability groupsprobability groups Inaccurate low risk assessmentInaccurate low risk assessment
Explicit CriteriaExplicit Criteria Scoring systemsScoring systems Prediction rulesPrediction rules Clinical decision rulesClinical decision rules

Canadian Score for Pre-test ProbabilityCanadian Score for Pre-test ProbabilityCreating the ScoreCreating the Score
CriteriaCriteria PointsPoints
Suspected DVTSuspected DVT 3.03.0
An alternative diagnosis is less likely than PEAn alternative diagnosis is less likely than PE 3.03.0
Heart rate >100 beats/minHeart rate >100 beats/min 1.51.5
Immobilization or surgery in the previous 4 wkImmobilization or surgery in the previous 4 wk 1.51.5
Previous DVT/PEPrevious DVT/PE 1.51.5
HemoptysisHemoptysis 1.01.0
Malignancy (on treatment, treated in thep past 6 mo, or palliativeMalignancy (on treatment, treated in thep past 6 mo, or palliative 1.01.0
Interpretation of the ScoreInterpretation of the Score
Score RangeScore Range Mean Probability Mean Probability
of PE, %of PE, %
Patients with this Patients with this Score, %Score, %
Interpretation of Interpretation of RiskRisk
0-2 points0-2 points 3.63.6 4040 LowLow
3-6 points3-6 points 20.520.5 5353 ModerateModerate
>6 points>6 points 66.766.7 77 HighHigh
WellsWells ThromThrom HaemostHaemost 2000; 2000; 83:416-420.83:416-420.

Geneva Score for Assessment of Pretest Geneva Score for Assessment of Pretest Probability for Pulmonary EmbolismProbability for Pulmonary Embolism
Age 60-79 yearsAge 60-79 yearsAge > 79 yearsAge > 79 yearsPrior DVT/PEPrior DVT/PERecent surgeryRecent surgeryHeart rate > 100 beats/minHeart rate > 100 beats/minPaCOPaCO22, mmHg, mmHg
<36<3636-3936-39
PaOPaO22, mmHg, mmHg<49<4949-6049-60>60-71>60-71>71-82>71-82
Chest radiographChest radiographPlatelike atelectasisPlatelike atelectasisElevation of hemidiaphragmElevation of hemidiaphragm
Creating the score Points
Interpretation of the score
Criteria
0-4 points0-4 points5-8 points5-8 points9-12 points9-12 points
101038388181
4949444466
LowLowModerate Moderate
HighHigh
Score range Mean probability of PE, % Patients with this score, %
Interpretation of risk
1122223311
2211
44332211
1111
Wicki Wicki Arch IntArch Int MedMed 2001; 2001; 161:92-97161:92-97

Clinical Gestalt vs Prediction RulesClinical Gestalt vs Prediction Rules
Clinical GestaltClinical Gestalt Prediction RulesPrediction Rules
Pretest Pretest
ProbProb
Rate Pulmonary Rate Pulmonary EmbolismEmbolism
Rate Pulmonary Rate Pulmonary EmbolismEmbolism
LowLow 8% - 19%8% - 19% 3% - 28%3% - 28%
ModerateModerate 26% - 47%26% - 47% 16% - 46%16% - 46%
HighHigh 46% - 91%46% - 91% 38% - 98%38% - 98%
“Clinical gestalt of experienced clinicians and prediction rules used by physicians of varying experience have shown similar accuracy in discriminating among patients who have a low, moderate or high pretest probability of PE”
Chandilal Chandilal JAMA JAMA 2003; 290:2849-28582003; 290:2849-2858

Diagnostic Approach to Pulmonary EmbolismDiagnostic Approach to Pulmonary EmbolismHigh Clinical Probability
CT Angio
Positive CT
Diagnosis confirmed
Negative CT
Duplex Ultrasound
PositiveNegative
Diagnosis ConfirmedPulmonary Angiography
PositiveNegative
Diagnosis Excluded Diagnosis Confirmed
Fedullo Fedullo NEJM NEJM 2003; 349:1247-562003; 349:1247-56

Diagnostic Strategies for Excluding Pulmonary Diagnostic Strategies for Excluding Pulmonary Embolism with Upper 95% ConfidenceEmbolism with Upper 95% Confidence
Limit of 3% or less and 3 month riskLimit of 3% or less and 3 month risk
Initial EvaluationInitial Evaluation
Diagnostic StrategyDiagnostic Strategy 3-month Risk for VTE 3-month Risk for VTE complications (upper 95% CL)complications (upper 95% CL)
Normal pulmonary angiogramNormal pulmonary angiogram 0.8 (2.1)0.8 (2.1)
Normal lung scanNormal lung scan 0.9 (2.3)0.9 (2.3)
Normal lung scan, normal legsNormal lung scan, normal legs 0.6 (1.2)0.6 (1.2)
Normal D-dimerNormal D-dimer 0.0 (1.8)0.0 (1.8)
Normal D-dimer low clinical Normal D-dimer low clinical probabilityprobability
0.2 (0.8)0.2 (0.8)
Marieke Marieke Ann Int MedAnn Int Med 2003; 138:941-951 2003; 138:941-951

Clinical Validity of a Negative CT Scan in Clinical Validity of a Negative CT Scan in Suspected Pulmonary EmbolismSuspected Pulmonary Embolism
Overall negative likelihood ratio of VTE after negative chest CT Scan Overall negative likelihood ratio of VTE after negative chest CT Scan → → 0.07 (CI 0.05 – 0.11)0.07 (CI 0.05 – 0.11)Overall negative predictive value → 99.1% (CI 98.7% - 99.5%)Overall negative predictive value → 99.1% (CI 98.7% - 99.5%)Negative likelihood ratio of VTE after a negative single slice spiral CT Negative likelihood ratio of VTE after a negative single slice spiral CT scan → 0.08 (CI 0.05 – 0.13)scan → 0.08 (CI 0.05 – 0.13)Negative likelihood ratio of VTE after negative multidetector-row CT Negative likelihood ratio of VTE after negative multidetector-row CT scan → 0.15 (CI 0.05 – 0.43)scan → 0.15 (CI 0.05 – 0.43)Overall negative likelihood ratio of mortality attributable to PE → 0.01 Overall negative likelihood ratio of mortality attributable to PE → 0.01 (CI 0.01 – 0.02)(CI 0.01 – 0.02)Overall negative predictive value 99.4% (CI 98.7% - 99.9%)Overall negative predictive value 99.4% (CI 98.7% - 99.9%)
“Clinical validity of using a CT Scan to rule out PE is similar to that reported for angiography”
Quiroz Quiroz JAMA JAMA 2005; 293:2012-20172005; 293:2012-2017

BNP and TroponinsBNP and Troponins
Complementary Biomarkers for Risk Stratification Future Directions?
Hemodynamically Stable PE
And Stretch Ischemia RV Dysfxn RV damage BNP < 50 TnT > 0.01 detects
detects low risk high risk
BNP Troponin
Both ElevatedBoth Normal
Low risk
Heparin
Floor Outpatient
High risk
Echocardiogram
Heparin Medical or Surgical Embolectomy
vs

Major Pulmonary EmbolismMajor Pulmonary EmbolismEcho FindingsEcho Findings
• Right sided thrombiRight sided thrombi• Correlation with obstructionCorrelation with obstruction• RV dilatation/hypokinesisRV dilatation/hypokinesis• Pul Art DilatationPul Art Dilatation• LV size; LV size; RV/LV ratio RV/LV ratio• Tricuspid regurgitationTricuspid regurgitation• Abnormal/paradoxical septumAbnormal/paradoxical septum• Loss of inspiratory collapse Loss of inspiratory collapse
IVCIVC
• AM IAM I• TamponadeTamponade• Aortic dissectionAortic dissection• Valvular diseaseValvular disease
Pulmonary Embolism Alternative Diagnosis

Major Pulmonary EmbolismMajor Pulmonary Embolism
Transthoracic Echo
Transesophageal Echo
RV Dilatation
PE bilateral
PE 50%-90% central/proximal
• TEE sensitivity 80-97% specificity 84%-100%
• Comparable sensitivity to spiral CT attributed to TEE ability to visualize proximal extending mobile portions of distally impacted emboli
• Low sensitivity beyond proximal
Pruszczyk Pruszczyk Chest Chest 1997; 112:722-281997; 112:722-28
Wittlich Wittlich J Am Soc EchoJ Am Soc Echo 1992; 5:515-24 1992; 5:515-24

Venous Thromboembolism in ICUVenous Thromboembolism in ICU
Pulmonary Embolism Therapeutics

Massive Pulmonary EmbolismTherapeutics
Heparin
Thrombolytics Embolectomy
Vena Caval filters
Standard Bolus Catheter Surgical


ACCP Therapeutic ACCP Therapeutic RecommendationsRecommendations
High suspicion PE- anticoagulate eval period High suspicion PE- anticoagulate eval period Non-massive PE- LMWH over UFHNon-massive PE- LMWH over UFHNon-massive PE- initial LMWH/UFH for at least 5 daysNon-massive PE- initial LMWH/UFH for at least 5 daysRenal failure- IV UFH over LMWHRenal failure- IV UFH over LMWHUFH- aPTT prolongation plasma heparin level 0.3 to 0.7UFH- aPTT prolongation plasma heparin level 0.3 to 0.7Inability to achieve therapeutic aPTT-measure anti-XaInability to achieve therapeutic aPTT-measure anti-XaInitiate VKA on day 1 and discontinue heparin when INR Initiate VKA on day 1 and discontinue heparin when INR is stable and greater than 2.0is stable and greater than 2.0
CHESTCHEST 2004; 126(3):401S-428S 2004; 126(3):401S-428S

ACCP Recommendations Long TermACCP Recommendations Long Term
Transient reversible risk- VKA 3 monthsTransient reversible risk- VKA 3 monthsFirst idiopathic PE- VKA 3-6 months (consider indefinite First idiopathic PE- VKA 3-6 months (consider indefinite treatment)treatment)PE and Cancer- LMWH 3 to 6 monthsPE and Cancer- LMWH 3 to 6 monthsAntiphosopholipid antibodies or two or more thrombophilic Antiphosopholipid antibodies or two or more thrombophilic conditions- 12 monthsconditions- 12 monthsFirst episode with deficiency of protein C, protein S, First episode with deficiency of protein C, protein S, prothrombin 20210 gene mutation, homocysteinemia or prothrombin 20210 gene mutation, homocysteinemia or high factor VIII levels- 6-12 monthshigh factor VIII levels- 6-12 monthsTwo or more episodes-indefinite treatmentTwo or more episodes-indefinite treatmentINR target 2.5 (range 2.0 to 3.0)INR target 2.5 (range 2.0 to 3.0)
PE and cancer-LMWH for 3-6 monthsPE and cancer-LMWH for 3-6 months CHESTCHEST 2004; 126(3):401S-428S 2004; 126(3):401S-428S

Major Pulmonary EmbolismMajor Pulmonary EmbolismPotential Benefits of Thrombolytic TherapyPotential Benefits of Thrombolytic Therapy
• Eliminate venous thrombi Eliminate venous thrombi decrease recurrent PE decrease recurrent PE• Prevent chronic vascular obstruction and pulmonary HPTPrevent chronic vascular obstruction and pulmonary HPT• Reduction of morbidity and mortalityReduction of morbidity and mortality
Rapid Clot Lysis
Enhance pulmonary perfusion
Early hemodynamic improvement
Improve gas exchange

Thrombolytic Therapy-Randomized TrialsThrombolytic Therapy-Randomized Trials
StudyStudy ## MortalityMortality RecurrentRecurrent MortalityMortality RecurrentRecurrent
UPET 1970UPET 1970 160160 7%7% 19%19% 9%9% 15%15%
Tibbutt 1974Tibbutt 1974 3030 8%8% ---- 0%0% ----
Ly 1978Ly 1978 2020 9%9% ---- 0%0% ----
Marini 1988Marini 1988 3030 0%0% 0%0% 0%0% 0%0%
PIOPED 1990PIOPED 1990 1313 0%0% ---- 11%11% ----
Levine 1990Levine 1990 5858 0%0% 0%0% 3%3% 0%0%
Goldhaber 1993Goldhaber 1993 101101 4%4% 9%9% 0%0% 0%0%
Sanchez 1995Sanchez 1995 88 100%100% ---- 0%0% 0%0%
Konstantinides 2002Konstantinides 2002 256256 2.2%2.2% 2.9%2.9% 3.4%3.4% 3.4%3.4%
HeparinHeparin LysisLysis

Major Pulmonary EmbolismMajor Pulmonary EmbolismThrombolytic Therapy “Facts”Thrombolytic Therapy “Facts”
Heparin better than placeboHeparin better than placeboBarritt Barritt LancetLancet 1961; 1:729 1961; 1:729
12 hr Urokinase=24 hr Urokinase 12 hr Urokinase=24 hr Urokinase 24 Streptokinase24 StreptokinaseheparinheparinUPET II UPET II JAMAJAMA 1974; 229:1606-13 1974; 229:1606-13
2 hr TPA>12/24 hr Urokinase2 hr TPA>12/24 hr UrokinaseGoldhaber Goldhaber Lancet Lancet 1988; 2:293-98; Meyer 1988; 2:293-98; Meyer J Am Coll CardiolJ Am Coll Cardiol 1992; 19:239-45 1992; 19:239-45
2 hr TPA=2 hr short infusion Urokinase2 hr TPA=2 hr short infusion UrokinaseGoldhaber Goldhaber J Am Coll CardiolJ Am Coll Cardiol 1992; 20:24-30 1992; 20:24-30
IV= Intrapulmonary TPAIV= Intrapulmonary TPAVerstraete Verstraete Cir Cir 1988; 77:353-601988; 77:353-60
Bolus TPA=2 hr TPABolus TPA=2 hr TPALevine Levine CHESTCHEST 1990; 98:1473-79; Goldhaber 1990; 98:1473-79; Goldhaber CHESTCHEST 1994; 106:718-24; 1994; 106:718-24; Sors Sors CHESTCHEST 1994; 106:712-17 1994; 106:712-17
2 hr TPA>12 hr Streptokinase2 hr TPA>12 hr StreptokinaseMeneveau Meneveau Eur Heart JEur Heart J 1997;18:1141-48 1997;18:1141-48
2 hr TPA=2 hr Streptokinase2 hr TPA=2 hr StreptokinaseMeneveau Meneveau J Am CollJ Am Coll Cardiol 1998; 31:1057-63 Cardiol 1998; 31:1057-63

Major Pulmonary EmbolismMajor Pulmonary EmbolismComplications of Thrombolytic TherapyComplications of Thrombolytic Therapy
Major hemorrhage (12%)Major hemorrhage (12%) TPA 13.7%TPA 13.7% UK 10.2%UK 10.2% SK 8.8%SK 8.8%
Intra-cranial hemorrhage Intra-cranial hemorrhage (1.2%)(1.2%) Fatal in 50%Fatal in 50% SK-none reportedSK-none reported UK 1.3%UK 1.3% TPA 1.6%TPA 1.6% Elevated diastolic BP as riskElevated diastolic BP as risk
FatalFatalIntra-cranialIntra-cranialRequiring Requiring transfusion/surgerytransfusion/surgery
Arcasoy Arcasoy CHEST CHEST 1999; 115:1695-17071999; 115:1695-1707

Major Pulmonary EmbolismMajor Pulmonary Embolism
Diagnostic confirmatory studies can delay Diagnostic confirmatory studies can delay definitive treatment and contribute to mortality; definitive treatment and contribute to mortality; angio 14%-67%angio 14%-67%
Cardiopulmonary bypass > venous inflow Cardiopulmonary bypass > venous inflow occlusionocclusion
Mortality decreasing but variable (16% - 46%)Mortality decreasing but variable (16% - 46%) 1960’s 57%1960’s 57% 1990’s 26%1990’s 26% Highest mortality with cardiac arrest (60%)Highest mortality with cardiac arrest (60%)
Catheter fragmentation an option if no arrestCatheter fragmentation an option if no arrest
Surgical or Catheter Embolectomy

Heparin Induced Thrombocytopenia Heparin Induced Thrombocytopenia Hypercoagulable ParadoxHypercoagulable Paradox
Thrombosis risk Thrombosis risk degree of thrombocytopenia degree of thrombocytopenia Mild thrombocytopenia 50%Mild thrombocytopenia 50% Severe thrombocytopenia 90%Severe thrombocytopenia 90%
Isolated “HIT” Isolated “HIT” 50% thrombosis post dx/stop heparin 50% thrombosis post dx/stop heparin
Warkentin Heparin Induced Thrombocytopenia 2001
VenousVenous
Aortic or iliofemoral thrombosis Aortic or iliofemoral thrombosis acute limb ischemia infarct (5-10%)acute limb ischemia infarct (5-10%)
Acute thrombotic stroke (3-5%)Acute thrombotic stroke (3-5%)
Myocardial infarction (3-5%)Myocardial infarction (3-5%)
ArterialArterial
DVT 50%DVT 50%
PE (25%)PE (25%)
Cerebral vein thrombosisCerebral vein thrombosis
Adrenal hemorrhagic Adrenal hemorrhagic infarctinfarct

Venous Thromboprophylaxis in the Venous Thromboprophylaxis in the Critically IllCritically Ill
Venous thromboembolism is common in Venous thromboembolism is common in critically ill patientscritically ill patientsModifiable risk factors are limited in ICUModifiable risk factors are limited in ICUDVT prophylaxis is essentialDVT prophylaxis is essentialPE risk stratification is crucial to define optimal PE risk stratification is crucial to define optimal TxTx
Summary