Embed Size (px)
Citation preview
D-dimer for Exclusion of VenousThromboembolism
D-dimer for Exclusion of VenousThromboembolism
CONTENT
What is venousthromboembolism (VTE)?........................ p.5
How is VTE diagnosed?.............................p.7
What is D-dimer?.........................................p.8
Why consider D-dimerin the diagnosis of VTE?.......................... p.9
Choosing a D-dimer assayfor VTE exclusion....................................... p.10
Not all D-dimer assaysare equal......................................................... p.12
D-dimer in non-invasivestrategies to diagnose VTE................... p.13
Frequently asked questions................. p.18
References..................................................... p.22
● The vast majority (80% or more) of outpatients* attending ahospital emergency department with clinical signs of venousthromboembolism (VTE; deep vein thrombosis and/orpulmonary embolism) will not have the disease. • This illustrates the need for rapid, non-invasive and
cost-effective diagnostic strategies for VTE exclusion.
● The combination of risk stratification by clinicalpre-test probability (PTP) assessment and D-dimer testing is recommended as the first step in the diagnostic pathwaybecause it safely excludes VTE in about 1/3rd of suspectedoutpatients**.
• This has advantages for the health care system because it willgreatly reduce the need for time-consuming and expensiveimaging procedures and avoid unnecessary treatment withanticoagulants.
• D-dimer testing is not standardized and available assays varywidely in analytical, operational and clinical performancecharacteristics. Clinicians and laboratory managers should beaware of these aspects before selecting a D-dimer assay aspart of a VTE diagnostic algorithm. Preference should begiven to rapid, quantitative assays with the lowest coefficientof variation at the cut-off point and to those tests that haveundergone proper clinical validation.
*Bounameaux H, Perrier A. Diagnostic approaches to suspected deep veinthrombosis and pulmonary embolism. Hematol J 2003; 4: 97-103.
**ten Cate-Hoek AJ, Prins MH. Management studies using a combination ofD-dimer test result and clinical probability to rule out venousthromboembolism. J Thromb Haemost 2005; 3: 2465-70.
Summary Points
Preface
Introduction
Experience with using D-dimer as a diagnostic help in suspected deep veinthrombosis (DVT) or pulmonary embolism (PE) has a history of almosttwenty years (1,2). Its widespread use has been made possible withthe development of rapid assays that allow result delivery within one hour orless after blood sampling. However, the heterogeneity of the assays has raiseduncertainty among clinicians and called for rigorous evaluation of the varioustests. Uncertainty further increased because the usefulness of the test was alsofound to be dependent upon the populations to which it was applied, due tovariations in test specificity.
Depending on the particular assay used, D-dimer measurement is a moderateto highly sensitive diagnostic tool for the presence of DVT or PE (3). Particleagglutination assays such as classical plasma-based latex slide tests and directwhole blood tests, give quick answers but are generally less sensitive than ELISAmethods. Rapid quantitative assays based on the ELISA technique or automatedturbidimetric methods have been developed with an excellent sensitivity.Such tests are increasingly being incorporated in diagnostic algorithms forvenous thromboembolism. Evidence has accumulated that DVT and PE can besafely ruled out in outpatients in the emergency room based on a negativeD-dimer test alone. For safety reasons, however, this policy is restricted tonon-high clinical probability patients. This implies that the D-dimer test must beused in conjunction with clinical probability assessment.
D-dimer testing for DVT/PE exclusion is particularly useful consideringthe prevalence of the disease among clinically suspected outpatients. This hasbeen decreasing steadily over the past fifteen years with reported contemporaryprevalence below 20% or even below 10% in some diagnostic centers inCanada and the US. Thus, the question is no longer to confirm but to excludethe disease, and to restrict further imaging modalities to those patients witha D-dimer level above the diagnostic cut-off. Other patient populations such asinpatients, postoperative patients, pregnant women, and elderly subjects havehigher baseline D-dimer levels, thereby reducing the specificity for VTE.This limits the practical usefulness of the test in these populations in case ofsuspected venous thromboembolism.
The saga of D-dimer measurement has been exemplary. Diagnosticperformance has been accurately determined with appropriate comparators (3).Usefulness has been assessed in large outcome studies (4).Finally, cost-effectiveness has also been established (5). However, the proportionof patients with positive D-dimer but without DVT or PE increases dramaticallyin daily clinical practice, probably in part because it is easier to order D-dimertesting than to question the pertinence of looking for DVT or PE in a givenpatient. Even a good test can be misused, and even a good test does notdispense from clinical reasoning.
Henri Bounameaux, MDProfessor of Medicine and ChairmanDepartment of Medicine - University Hospital of Geneva, Geneva, Switzerland
What is venous thromboembolism (VTE)?
Venous thromboembolism (VTE) is a common medical condition withan annual incidence in the general population of about 0.2 percent (6).Clinical manifestations are deep vein thrombosis (DVT) and its majorcomplication, pulmonary embolism (PE).
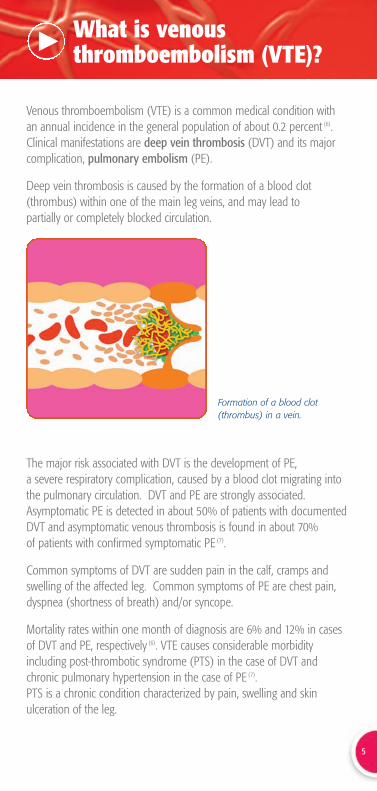
Deep vein thrombosis is caused by the formation of a blood clot(thrombus) within one of the main leg veins, and may lead to partially or completely blocked circulation.
The major risk associated with DVT is the development of PE, a severe respiratory complication, caused by a blood clot migrating intothe pulmonary circulation. DVT and PE are strongly associated.Asymptomatic PE is detected in about 50% of patients with documentedDVT and asymptomatic venous thrombosis is found in about 70% of patients with confirmed symptomatic PE (7).
Common symptoms of DVT are sudden pain in the calf, cramps andswelling of the affected leg. Common symptoms of PE are chest pain,dyspnea (shortness of breath) and/or syncope.
Mortality rates within one month of diagnosis are 6% and 12% in casesof DVT and PE, respectively (6). VTE causes considerable morbidity including post-thrombotic syndrome (PTS) in the case of DVT andchronic pulmonary hypertension in the case of PE (7). PTS is a chronic condition characterized by pain, swelling and skin ulceration of the leg.
5
Formation of a blood clot(thrombus) in a vein.
6
Table 1. Risk factors for VTE (8).
VTE is a multi-factorial disease and often results from a combination of risk factors, including environmental and genetic sources (Table 1).
Prophylactic treatment with anticoagulant drugs is indicated in thepresence of certain moderate or high risk factors. Patients with a first VTEevent are at risk of having a second event. The annual recurrence rate is3-10% (7).
Once VTE is diagnosed, current practice is to provide an initial shorttreatment with intravenous unfractionated heparin or subcutaneous low-molecular-weight heparin, followed by an oral anticoagulant drug(e.g. warfarin) for several months to prevent embolization and recurrence (9).The optimum dosage and duration of oral anticoagulant therapy after a first event, however, is largely dictated by underlying risk factors (8,9).
Strong Risk Factors
• Fracture (hip or leg)
• Hip or knee replacement
• Major general surgery
• Major trauma
• Spinal cord injury
Moderate Risk Factors
• Arthroscopic knee surgery
• Catheterisation (central venous lines)
• Chemotherapy
• Congestive heart or respiratory failure
• Hormone replacement therapy
• Cancer
• Oral contraceptives
• Paralytic stroke
• Pregnancy/post-partum
• Previous VTE
• Thrombophilia
Weak Risk Factors
• Bed rest > 3 days
• Minimal immobility (e.g. prolonged travel in car or plane)
• Increasing age (> 40 years)
• Laparoscopic surgery
• Obesity
• Pregnancy / ante-partum
• Varicose veins
How is VTE diagnosed?
VTE may or may not be associated with clinical symptoms such as painand swelling of the affected leg (DVT) or dyspnea, chest pain and/orsyncope (PE). This means that diagnosis of VTE is difficult and notreliable when based on clinical symptoms alone. Clinical suspicion ofVTE must therefore be confirmed with objective tests (10).
Venography (phlebography) and pulmonary angiography are thegold standard methods to diagnose DVT and PE respectively – but theyare invasive, costly and not universally available.
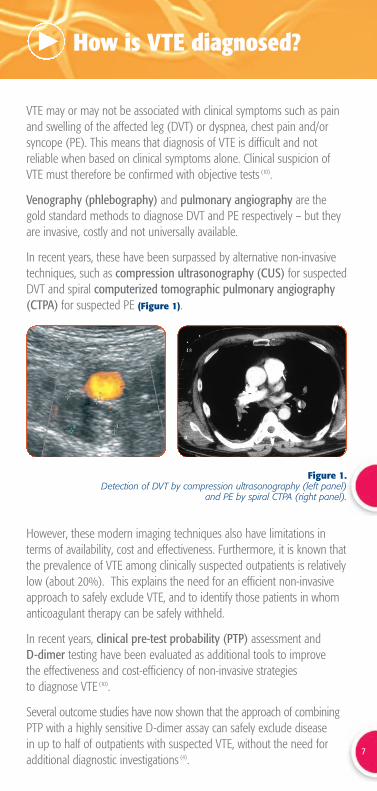
In recent years, these have been surpassed by alternative non-invasivetechniques, such as compression ultrasonography (CUS) for suspectedDVT and spiral computerized tomographic pulmonary angiography(CTPA) for suspected PE (Figure 1).
However, these modern imaging techniques also have limitations interms of availability, cost and effectiveness. Furthermore, it is known thatthe prevalence of VTE among clinically suspected outpatients is relativelylow (about 20%). This explains the need for an efficient non-invasiveapproach to safely exclude VTE, and to identify those patients in whomanticoagulant therapy can be safely withheld.
In recent years, clinical pre-test probability (PTP) assessment and D-dimer testing have been evaluated as additional tools to improve the effectiveness and cost-efficiency of non-invasive strategies to diagnose VTE (10).
Several outcome studies have now shown that the approach of combiningPTP with a highly sensitive D-dimer assay can safely exclude diseasein up to half of outpatients with suspected VTE, without the need foradditional diagnostic investigations (4).
Figure 1.Detection of DVT by compression ultrasonography (left panel)
and PE by spiral CTPA (right panel).
7
What is D-dimer?
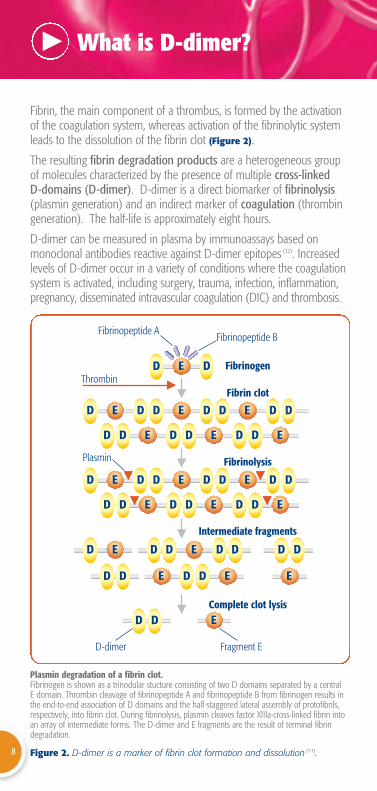
Fibrin, the main component of a thrombus, is formed by the activationof the coagulation system, whereas activation of the fibrinolytic systemleads to the dissolution of the fibrin clot (Figure 2).
The resulting fibrin degradation products are a heterogeneous group of molecules characterized by the presence of multiple cross-linked D-domains (D-dimer). D-dimer is a direct biomarker of fibrinolysis(plasmin generation) and an indirect marker of coagulation (thrombingeneration). The half-life is approximately eight hours.
D-dimer can be measured in plasma by immunoassays based on monoclonal antibodies reactive against D-dimer epitopes (12). Increasedlevels of D-dimer occur in a variety of conditions where the coagulationsystem is activated, including surgery, trauma, infection, inflammation,pregnancy, disseminated intravascular coagulation (DIC) and thrombosis.
Figure 2. D-dimer is a marker of fibrin clot formation and dissolution (11).8
ED D
ED D ED D DED D
ED D EDED DD
ED D ED D DED D
ED D EDED DD
ED EED DD
EDD
ED D D D DED D
D-dimer Fragment E
Fibrinopeptide BFibrinopeptide A
Complete clot lysis
Intermediate fragments
Fibrinolysis
Fibrin clot
Fibrinogen
Plasmin
Thrombin
Plasmin degradation of a fibrin clot.Fibrinogen is shown as a trinodular stucture consisting of two D domains separated by a central E domain. Thrombin cleavage of fibrinopeptide A and fibrinopeptide B from fibrinogen results inthe end-to-end association of D domains and the half-staggered lateral assembly of protofibrils,respectively, into fibrin clot. During fibrinolysis, plasmin cleaves factor XIIIa-cross-linked fibrin intoan array of intermediate forms. The D-dimer and E fragments are the result of terminal fibrindegradation.

Why consider D-dimer in the diagnosis of VTE?
9
Due to the simultaneous activation of fibrinolysis, D-dimer levels areraised in the presence of large blood clots that obstruct the circulation insymptomatic patients with VTE. However, activation of coagulation andsubsequent fibrinolysis also occurs in a variety of other disorders withoutgiving rise to an occluding clot. Consequently, D-dimer is not a specificmarker for VTE, since its level can also be increased due to co-morbidconditions such as cancer or recent surgery. D-dimer is also significantlyelevated in the elderly and during pregnancy.
Therefore, a positive D-dimer assay alone will not confirm VTE.However, D-dimer levels are raised in almost all patients with acute VTEwhen assayed with a highly sensitive test. Consequently, a patient witha normal D-dimer plasma level (i.e. below a predefined cut-off value) is very unlikely to have DVT or PE.
The usefulness of this test, therefore lies in its ability to safely excludethe presence of VTE due to its high negative predictive value (NPV).
Prospective management studies have shown that D-dimer testing, combined with clinical probability assessment, allows rapid and safeexclusion of VTE in 30% to 50% of suspected outpatients (4).
D-dimer and clinical assessment are now highlyrecommended as the first step in the investigationof patients with suspected VTE (13-17).
This has two important advantages for the healthcare system:
● Cost-savings for the hospital• Avoids unnecessary imaging procedures and treatment.• Reduces length of hospital stay or need for transfer.
● Improved patient comfort• Avoids risk associated with invasive procedures.• Avoids bleeding complications associated with unnecessary
anticoagulant treatment.
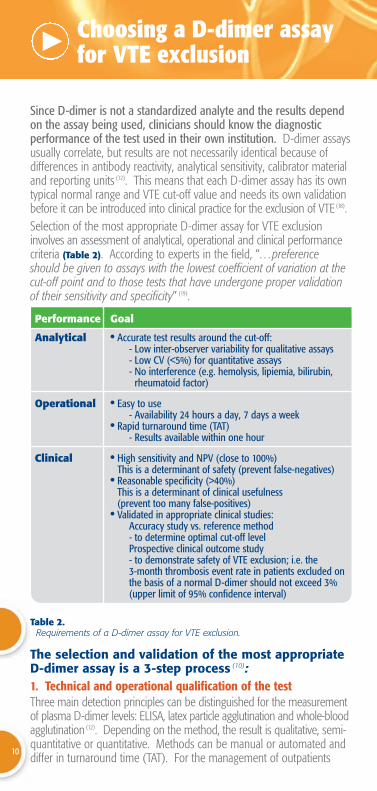
Table 2.Requirements of a D-dimer assay for VTE exclusion.
Choosing a D-dimer assay for VTE exclusion
Since D-dimer is not a standardized analyte and the results dependon the assay being used, clinicians should know the diagnostic performance of the test used in their own institution. D-dimer assaysusually correlate, but results are not necessarily identical because of differences in antibody reactivity, analytical sensitivity, calibrator materialand reporting units (12). This means that each D-dimer assay has its owntypical normal range and VTE cut-off value and needs its own validationbefore it can be introduced into clinical practice for the exclusion of VTE (18). Selection of the most appropriate D-dimer assay for VTE exclusioninvolves an assessment of analytical, operational and clinical performancecriteria (Table 2). According to experts in the field, “…preferenceshould be given to assays with the lowest coefficient of variation at thecut-off point and to those tests that have undergone proper validation of their sensitivity and specificity” (19).
The selection and validation of the most appropriateD-dimer assay is a 3-step process (10):1. Technical and operational qualification of the testThree main detection principles can be distinguished for the measurementof plasma D-dimer levels: ELISA, latex particle agglutination and whole-bloodagglutination (12). Depending on the method, the result is qualitative, semi-quantitative or quantitative. Methods can be manual or automated anddiffer in turnaround time (TAT). For the management of outpatients
10
Performance Goal
Analytical • Accurate test results around the cut-off: - Low inter-observer variability for qualitative assays- Low CV (<5%) for quantitative assays- No interference (e.g. hemolysis, lipiemia, bilirubin,
rheumatoid factor)
Operational • Easy to use- Availability 24 hours a day, 7 days a week
• Rapid turnaround time (TAT)- Results available within one hour
Clinical • High sensitivity and NPV (close to 100%)This is a determinant of safety (prevent false-negatives)
• Reasonable specificity (>40%)This is a determinant of clinical usefulness (prevent too many false-positives)
• Validated in appropriate clinical studies: Accuracy study vs. reference method- to determine optimal cut-off levelProspective clinical outcome study - to demonstrate safety of VTE exclusion; i.e. the 3-month thrombosis event rate in patients excluded on the basis of a normal D-dimer should not exceed 3% (upper limit of 95% confidence interval)
with suspected VTE in the emergency department, preference is given to quantitative observer-independent systems with a short TAT and the lowest coefficient of variation (CV) at the cut-off point. A rapid, automated and quantitative ELISA such as VIDAS® D-DimerExclusion™ fits these requirements.
2. Selection of optimal cut-off point; accuracy study versus the reference method
The optimal discriminating D-dimer level for VTE exclusion (cut-off point)needs to be determined by a blinded prospective observational study in the target population (i.e. outpatients with suspected VTE). The presence or absence of VTE is confirmed by accepted referencemethods such as serial CUS and multi-slice CTPA. The optimal cut-offpoint and the corresponding sensitivity (true positives) and specificity(true negatives) are then determined by standard statistical methods. The sensitivity determines the safety of the D-dimer assay for VTEexclusion and should be close to 100% to minimize the number of falsenegatives (i.e. ensure a high NPV). The NPV, however, not onlydepends on the sensitivity of the assay but also on the prevalence ofthe disease: the higher the pre-test probability of VTE, the lower theNPV. Consequently, even a highly sensitive D-dimer assay may notsafely rule out VTE in patients with a high clinical probability (20).Therefore, D-dimer should not be used indiscriminately for VTE exclusionand needs to be combined with clinical PTP assessment (13).
The specificity determines the clinical usefulness of the assay; i.e. theproportion of patients in a suspected population that is below the cut-offpoint and can potentially be excluded, provided the PTP is low or moderate.In outpatients, the specificity of highly sensitive D-dimer assays is usuallyaround 40% (i.e. 60% false positives). This means that in a typical outpatient population, with a VTE prevalence of 20%, about 1/3rd canbe excluded with a high-sensitivity assay (4). Because specificity is muchlower in the elderly, pregnant women, patients with cancer and hospitalisedpatients, D-dimer has limited utility for VTE exclusion in these populations (19).
3. Prospective clinical management study (outcome study)Once a D-dimer test has been selected based on its technical and operational merits (step 1) and accuracy criteria (step 2), its actual utilityfor VTE exclusion in terms of safety (thrombotic event rate on follow-up)and efficacy (reduced need for imaging) needs to be demonstrated in real life. This requires a prospective clinical outcome study in which further diagnostic imaging and anticoagulation are withheld in patientswith suspected VTE who exhibit a low or moderate PTP and normal D-dimer test result (4). A systematic 3-month follow-up is required inexcluded patients to allow detection of delayed thrombotic events andestablish the true diagnostic performance of the test. The exclusion procedure is considered safe if the upper 95% confidence limit of the 3-month event rate does not exceed 3% (21).
11
Not all D-dimer assays are equal
To safely exclude VTE, assay sensitivity shouldapproach 100%: “For every 2% decrease in sensitivity, 1 per 1000 patients studied will die ofrecurrent PE as a result of inappropriately withholding anticoagulant therapy” (22).
D-dimer assays vary in sensitivity (3). Basically, a D-dimer assay with thehighest sensitivity will provide the best safety (highest NPV). The ELISA D-dimer method is considered to be the ‘gold standard’ anddominates the comparative ranking among D-dimer assays for sensitivityand NPV:
“For excluding PE or DVT, a negative result on quantitative rapid ELISAis as diagnostically useful as a normal lung scan or negative duplexultrasonography finding” (3).
VIDAS® D-Dimer Exclusion™, a rapid quantitative ELISA, offers an NPV> 99% at a cut-off of 500 ng/mL. This has been proven in more than 50published peer-reviewed accuracy studies involving over 11,000 patients.
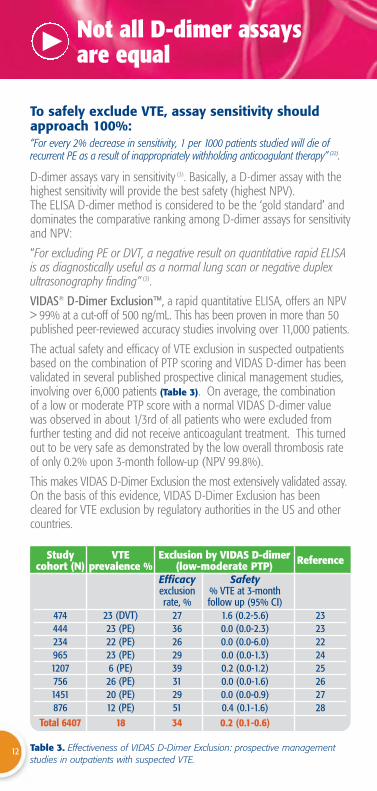
The actual safety and efficacy of VTE exclusion in suspected outpatientsbased on the combination of PTP scoring and VIDAS D-dimer has beenvalidated in several published prospective clinical management studies,involving over 6,000 patients (Table 3). On average, the combination of a low or moderate PTP score with a normal VIDAS D-dimer valuewas observed in about 1/3rd of all patients who were excluded fromfurther testing and did not receive anticoagulant treatment. This turnedout to be very safe as demonstrated by the low overall thrombosis rateof only 0.2% upon 3-month follow-up (NPV 99.8%).
This makes VIDAS D-Dimer Exclusion the most extensively validated assay.On the basis of this evidence, VIDAS D-Dimer Exclusion has beencleared for VTE exclusion by regulatory authorities in the US and othercountries.
Table 3. Effectiveness of VIDAS D-Dimer Exclusion: prospective managementstudies in outpatients with suspected VTE.
12
VTE prevalence %
23 (DVT)23 (PE)22 (PE)23 (PE)6 (PE)26 (PE)20 (PE)12 (PE)
18
Exclusion by VIDAS D-dimer(low-moderate PTP)
Efficacy Safetyexclusion % VTE at 3-month rate, % follow up (95% CI)
27 1.6 (0.2-5.6)36 0.0 (0.0-2.3)26 0.0 (0.0-6.0)29 0.0 (0.0-1.3)39 0.2 (0.0-1.2)31 0.0 (0.0-1.6)29 0.0 (0.0-0.9)51 0.4 (0.1-1.6)34 0.2 (0.1-0.6)
Reference
2323222425262728
Study cohort (N)
47444423496512077561451876
Total 6407
D-dimer in non-invasive strategies to diagnose VTE
Utility of clinical assessment
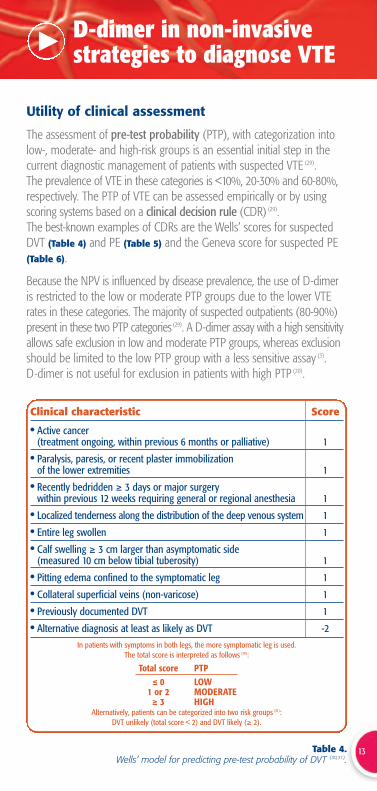
The assessment of pre-test probability (PTP), with categorization intolow-, moderate- and high-risk groups is an essential initial step in thecurrent diagnostic management of patients with suspected VTE (29). The prevalence of VTE in these categories is <10%, 20-30% and 60-80%,respectively. The PTP of VTE can be assessed empirically or by usingscoring systems based on a clinical decision rule (CDR) (29).The best-known examples of CDRs are the Wells’ scores for suspectedDVT (Table 4) and PE (Table 5) and the Geneva score for suspected PE(Table 6).
Because the NPV is influenced by disease prevalence, the use of D-dimeris restricted to the low or moderate PTP groups due to the lower VTErates in these categories. The majority of suspected outpatients (80-90%)present in these two PTP categories (29). A D-dimer assay with a high sensitivityallows safe exclusion in low and moderate PTP groups, whereas exclusionshould be limited to the low PTP group with a less sensitive assay (3). D-dimer is not useful for exclusion in patients with high PTP (20).
Table 4. Wells’ model for predicting pre-test probability of DVT (30,31).
13
Clinical characteristic Score
• Active cancer (treatment ongoing, within previous 6 months or palliative) 1
• Paralysis, paresis, or recent plaster immobilization of the lower extremities 1
• Recently bedridden ≥ 3 days or major surgery within previous 12 weeks requiring general or regional anesthesia 1
• Localized tenderness along the distribution of the deep venous system 1
• Entire leg swollen 1
• Calf swelling ≥ 3 cm larger than asymptomatic side (measured 10 cm below tibial tuberosity) 1
• Pitting edema confined to the symptomatic leg 1
• Collateral superficial veins (non-varicose) 1
• Previously documented DVT 1
• Alternative diagnosis at least as likely as DVT -2In patients with symptoms in both legs, the more symptomatic leg is used.
The total score is interpreted as follows (30):
Total score PTP ≤ 0 LOW
1 or 2 MODERATE≥ 3 HIGH
Alternatively, patients can be categorized into two risk groups (31): DVT unlikely (total score < 2) and DVT likely (≥ 2).
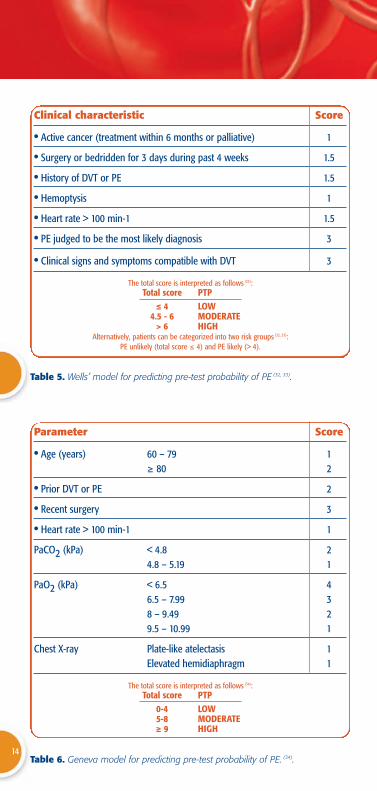
Table 6. Geneva model for predicting pre-test probability of PE. (34).
Table 5. Wells’ model for predicting pre-test probability of PE (32, 33).
14
Clinical characteristic Score
• Active cancer (treatment within 6 months or palliative) 1
• Surgery or bedridden for 3 days during past 4 weeks 1.5
• History of DVT or PE 1.5
• Hemoptysis 1
• Heart rate > 100 min-1 1.5
• PE judged to be the most likely diagnosis 3
• Clinical signs and symptoms compatible with DVT 3
The total score is interpreted as follows (33):Total score PTP
≤ 4 LOW4.5 - 6 MODERATE
> 6 HIGHAlternatively, patients can be categorized into two risk groups (32, 33):
PE unlikely (total score ≤ 4) and PE likely (> 4).
Parameter Score
• Age (years) 60 – 79 1≥ 80 2
• Prior DVT or PE 2
• Recent surgery 3
• Heart rate > 100 min-1 1
PaCO2 (kPa) < 4.8 24.8 – 5.19 1
PaO2 (kPa) < 6.5 46.5 – 7.99 38 – 9.49 29.5 – 10.99 1
Chest X-ray Plate-like atelectasis 1Elevated hemidiaphragm 1
The total score is interpreted as follows (34):Total score PTP
0-4 LOW5-8 MODERATE≥ 9 HIGH
Decision protocolsCost-effective diagnostic algorithms have been validated based on a rational sequential combination of several non-invasive tests (10). D-dimer testing combined with clinical probability assessment is generallyrecommended as the first step (13-17). It allows rapid and safe exclusion in about 1/3rd of suspected outpatients (4). Importantly, D-dimer assays cannot be used indiscriminately for VTEexclusion and the result should always be interpreted in the clinical contextof the patient (35). D-dimer is not considered useful in patients with highPTP and a negative D-dimer in this category always requires furtherinvestigation. Long duration of symptoms and concomitant use of anticoagulants are other conditions that may potentially lead to falsenegative D-dimer results.
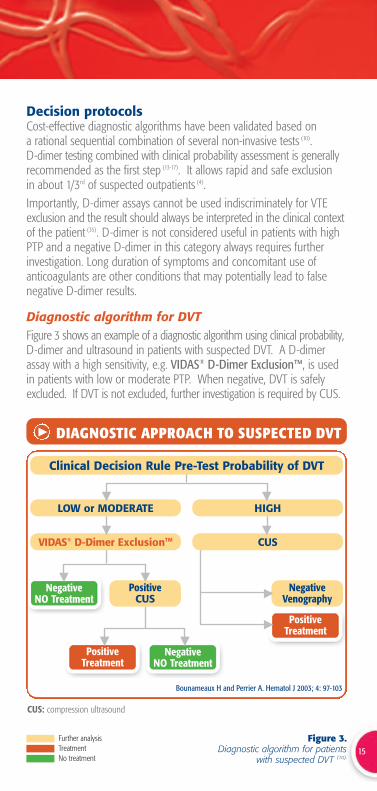
Diagnostic algorithm for DVTFigure 3 shows an example of a diagnostic algorithm using clinical probability,D-dimer and ultrasound in patients with suspected DVT. A D-dimerassay with a high sensitivity, e.g. VIDAS® D-Dimer Exclusion™, is usedin patients with low or moderate PTP. When negative, DVT is safelyexcluded. If DVT is not excluded, further investigation is required by CUS.
Figure 3.Diagnostic algorithm for patients
with suspected DVT (10).15
Further analysisTreatmentNo treatment
PositiveTreatment
NegativeNO Treatment
CUS: compression ultrasound
DIAGNOSTIC APPROACH TO SUSPECTED DVT
NegativeNO Treatment
Clinical Decision Rule Pre-Test Probability of DVT
LOW or MODERATE HIGH
VIDAS® D-Dimer ExclusionTM
PositiveTreatment
NegativeVenography
CUS
PositiveCUS
Bounameaux H and Perrier A. Hematol J 2003; 4: 97-103

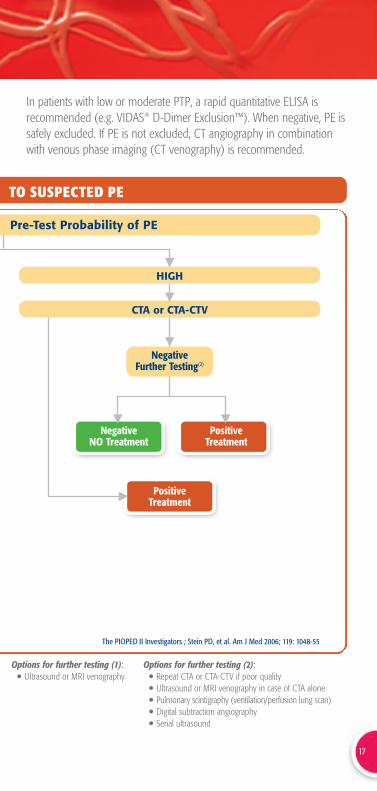
Diagnostic algorithm for PEFigure 4 shows the diagnostic pathways recommended by the PIOPED IIInvestigators in patients with suspected acute PE.Patients are first stratified according to an objective clinical assessment.
Figure 4. Diagnostic algorithm for patients with suspected PE (17).16
LOW or MODERATE
VIDAS® D-Dimer ExclusionTM
CTA: contrast-enhanced multidetector computed tomographic angiographyCTV: venous-phase multidetector CT venography
DIAGNOSTIC APPROACH
Clinical Decision Rule
Negative NO Treatment Positive CTA or CTA-CTV
(Sub)Segmental)Further Testing(2) Main/Lobar
PositiveTreatment
NegativeNO Treatment
PositiveTreatment
PositiveConsider Location
Negative NO Treatment
Further Testing(1)
if Moderate PTP & CTA alone
Further analysisTreatmentNo treatment
17
In patients with low or moderate PTP, a rapid quantitative ELISA isrecommended (e.g. VIDAS® D-Dimer Exclusion™). When negative, PE issafely excluded. If PE is not excluded, CT angiography in combinationwith venous phase imaging (CT venography) is recommended.
HIGH
The PIOPED II Investigators ; Stein PD, et al. Am J Med 2006; 119: 1048-55
Options for further testing (1):• Ultrasound or MRI venography
Options for further testing (2): • Repeat CTA or CTA-CTV if poor quality• Ultrasound or MRI venography in case of CTA alone• Pulmonary scintigraphy (ventilation/perfusion lung scan)• Digital subtraction angiography• Serial ultrasound
TO SUSPECTED PE
Pre-Test Probability of PE
NegativeFurther Testing(2)
PositiveTreatment
NegativeNO Treatment
CTA or CTA-CTV
PositiveTreatment
18
Frequently asked questions
1. Is it safe to exclude VTE in suspected patientsbased on a negative D-dimer result?
Yes, VTE exclusion will be safe with a negative D-dimer.However, there are a number of restrictions that should bekept in mind. First, the recommended cut-off level that isused to interpret whether the D-dimer result is negative must
have been properly validated (18, 19). Second, D-dimer has onlybeen validated for VTE exclusion in suspected
outpatients (4). In hospitalized patients, the diagnostic accuracy of D-dimer forVTE is questionable (36) and the diagnostic yield (proportion below the cut-off)will be too low (37). Finally, to avoid false negatives, it is of vital importance tointerpret any negative D-dimer finding in the clinical context of the patient.This requires proper observation of the following patient-related factors (35):
• Clinical pre-test probability (PTP)D-dimer cannot be used as a stand-alone test for VTE exclusion andneeds to be combined with an assessment of clinical PTP (4, 13).Depending on the sensitivity of the D-dimer assay, exclusion should berestricted to patients with low PTP or can be extended to patients withmoderate PTP. D-dimer is not considered useful in patients with highPTP (20).
• Duration of symptomsThe age of the clot is relevant when interpreting test results, becauseD-dimer decreases with the time elapsed from the onset ofsymptoms (38). The effect of the duration of symptoms has not beensystematically investigated and, therefore, exact recommendations onwhen D-dimer will no longer be reliable for exclusion cannot be given.Lower sensitivities (false negatives) have been reported when D-dimerwas measured 4 to 15 days after the onset of symptoms (39-41).
• Prior use of anticoagulationBecause D-dimer and other objective tests are not always immediatelyavailable (e.g. at night), patients with suspected VTE are often given aninitial dose of heparin. This practice can potentially cause falsenegative results because D-dimer decreases by about 25% within24 hours after heparin injection (42). Therefore, the D-dimer resultreported from blood obtained after starting heparin treatment shouldbe interpreted with caution. D-dimer is also decreased by vitamin K antago-nists (43).
The importance of the sensitivity of D-dimer to the location of the clot hasbeen a matter of debate. D-dimer has a lower sensitivity for smaller clots indistal DVT (44) and subsegmental PE (45). Missing small distal clots, however,is considered to be of low concern because of uncertainty as to clinicalsignificance and lack of data on the benefit of treatment (46, 47).
19
2. Does a positive D-dimer result indicatethat my patient has a VTE?
No, D-dimer is not specific for VTE and can be elevatedin many other circumstances, in particular: • Old age
• Pregnancy• Cancer
• Arterial disease (peripheral arteriopathy, coronary artery disease,stroke)
• Disseminated intravascular coagulation (DIC)• Liver disease• Infection • Inflammation
Thus, a positive D-dimer result cannot be used to rule-in VTE and furtherobjective imaging tests are needed to confirm the presence of a thrombus.
The implication of this diagnostic behavior is that the specificity of D-dimer forVTE (i.e. proportion of negative results in patients without VTE) does notreach 100%. The specificity of D-dimer for VTE depends on the method usedand shows an inverse relationship with sensitivity. The specificity varies from40-50% for high-sensitivity quantitative assays up to about 70% forlow-sensitivity qualitative and semi-quantitative D-dimer assays (48).
The specificity is a determinant of the clinical usefulness of D-dimer for VTEexclusion (37). In a hypothetical outpatient population of 100 patients,with a typical 20% VTE prevalence, 32 patients can be excluded witha high-sensitivity D-dimer assay with a specificity of 40%. In other words, the number of patients that need to be tested (NNT) in the entire cohort torule out one VTE would be three (NNT=3). If the specificity drops to 12%,the diagnostic yield will be much lower and then only 10 patients can beexcluded (NNT=10).

20
Frequently asked questions
3. Can D-dimer be used for VTE exclusion insubgroups of outpatients with conditions
such as pregnancy, cancer, previous VTEand the elderly?
Yes, this is possible because there are no data thatindicate that the sensitivity is affected by these clinical
conditions. On the other hand, the specificity will drop at theusual cut-off that has been validated for the entire
outpatient population (e.g. 500 ng/mL for VIDAS® D-Dimer Exclusion™). Thisaffects the clinical usefulness in terms of the proportion of patients that canbe excluded, which may be as low as 10% (NNT=10). Despite the lowerdiagnostic yield in various patient subgroups, it could nevertheless beworthwhile to perform a D-dimer test because it is rapid, inexpensive andmay still prevent an imaging test in at least one out of every ten patientstested. This is particularly the case if the routine diagnostic strategy is basedon upfront D-dimer in combination with a clinical decision rule.On the other hand, if the clinical setting is more imaging orientedand D-dimer results are not readily available, it might be more efficient todirectly proceed to scanning procedures.
• PregnancyNormal pregnancy causes a progressive increase in circulatingD-dimer, which peaks at delivery and gradually decreases to normalwithin 4 weeks after delivery (49-51). D-dimer increases with eachtrimester, so that only about 50% and 25% of women are belowthe usual cut-off in the 1st and 2nd trimester, respectively. D-dimerhas no utility to rule out VTE in the 3rd trimester and the immediatepost-partum period. Because of the limited potential utility and lack ofproper validation studies, D-dimer testing is not part of recentlypublished evidence-based recommendations on diagnostic testing ofpregnant women with clinically suspected VTE (52).
• CancerCancer is a common cause of VTE and has been shown to occur in10-14% of outpatients with suspected VTE (53-55). In these studies,the prevalence of VTE in the cancer subgroups was on average 1.5-foldhigher compared with non-cancer patients. The combination ofD-dimer and clinical PTP assessment appears to be safe to rule outPE (53, 54) or DVT (55) in suspected outpatients with cancer. The exclusion rate,however, was 2 to 3-fold lower compared with non-cancer patients: NNT=10vs. NNT=3 in suspected PE and NNT=4 vs. NNT=2 in suspected DVT.
• Previous VTE (VTE recurrence)Patients with a first VTE event are at increased risk of having a second event (7).Studies in outpatients with suspected PE reported previous VTE episodes in 14% (53)
and 18% (56) of the total cohort. D-dimer levels remain elevated in many patientsafter completion of the standard anticoagulant drug course for a first VTEepisode (57). This may limit the clinical usefulness of D-dimer for exclusion ofrecurrent VTE. Subgroup analysis of large prospective outcome studies in patientswith suspected PE have demonstrated that a negative D-dimer result allows safeexclusion of a recurrent event, albeit with a 2-fold lower exclusion rate (53, 56).A single-center management study has shown that D-dimer also allowed safeexclusion of suspected recurrent DVT, apparently without compromising thediagnostic yield (NNT=2) (58).
• Elderly patients (>70 years)Both D-dimer and the prevalence of VTE increase with age and thismay affect the clinical usefulness of the D-dimer test in the elderly (59).Subgroup analysis of studies in outpatients showed thatthe combination of PTP assessment and D-dimer allows safe exclusionin the elderly, albeit with a much lower efficacy (exclusion rate 10-14%;NNT=7-10) (53, 60, 61).
4. Can D-dimer be used to guide the durationof anticoagulation?
No, not yet (62), despite promising data from prospectiveobservational studies (57, 63-65) and a randomized trial (66).The optimal duration of oral anticoagulation is uncertain,particularly in patients with a first idiopathic VTE event.
The risk of recurrence is greatest in the first 6-12 months butgradually diminishes thereafter. The benefit of an extended
duration of anticoagulation may be offset by an increased risk of bleeding.It is therefore important to find those patients in whom extendedanticoagulation may be warranted based on predictors of increased risk.D-dimer is emerging as a promising risk predictor for VTE recurrence, mostnotably to identify patients at low risk (57, 63-66). However, further studies areneeded before it can be introduced into routine clinical practice to gaugethe duration of anticoagulation. Critical parameters include the time ofmeasurement (during anticoagulation or after anticoagulation withdrawal) (67),the optimal cut-off (68) and the effect of other risk predictors such as gender (69).Studies are ongoing to address these issues and define an optimal riskprediction rule to select low-risk patients in whom anticoagulation can besafely stopped after the standard 6-month course.
5. Is there a potential future value for D-dimerin arterial thrombosis?
Yes, arterial thrombosis can be considered as a disease areawhere D-dimer has potential to add valuableadditional information for the treating physician. Heart
attack and stroke, the most devastating consequences ofatherosclerosis, are caused by acute thrombus formation
resulting from plaque rupture (70). Epidemiological studies have demonstratedthat D-dimer is an independent predictor for future coronary heart disease inthe general population (71). However, it is unlikely that D-dimer will play a rolein cardiovascular risk stratification in asymptomatic individuals. Morepromising is a role for D-dimer in optimizing risk stratification in acute settingssuch as patients presenting with chest pain due to acute coronarysyndromes (72-74) or patients with stroke (75-78). D-dimer may also have aprognostic role in atrial fibrillation (79) and heart failure (80,81).
21
22
References
1. Bounameaux H, Slosman D, de Moerloose P, Reber G. Diagnostic value of plasma D-dimer insuspected pulmonary embolism. Lancet 1998; 2(8611): 628-29.
2. Bounameaux H, Schneider PA, Reber G, de Moerloose P, Krahenbuhl B. Measurement of plasmaD-dimer for diagnosis of deep venous thrombosis. Am J Clin Pathol 1989; 91: 82-85.
3. Stein PD, Hull RD, Patel KC, Olson RE, Ghali WA, Brant R, Biel RK, Bharadia V, Kalra NK. D-dimerfor the exclusion of acute venous thrombosis and pulmonary embolism: a systematic review.Ann Intern Med 2004;140:589-602.
4. ten Cate-Hoek AJ, Prins MH. Management studies using a combination of D-dimer test result andclinical probability to rule out venous thromboembolism. J Thromb Haemost 2005; 3: 2465-70.
5. Perrier A, Nendaz M, Sarasin FP, Howarth N, Bounameaux H. Diagnostic strategies for suspectedpulmonary embolism including helical computed tomography: a cost-effectiveness analysis.Am J Respir Crit Care Med 2003; 167: 39-44.
6. White RH. The epidemiology of venous thromboembolism. Circulation 2003; 107: I-4-I-8. 7. Kearon C. Natural history of venous thromboembolism. Circulation 2003; 107: I-22-I-30. 8. Anderson C., Spencer F.A. Risk factors for venous thromboembolism. Circulation. 2003;107:I-9-I-16.9. Bates SM, Ginsberg JS. Treatment of deep-vein thrombosis. N Engl J Med 2004; 351: 268-77. 10. Bounameaux H, Perrier A. Diagnostic approaches to suspected deep vein thrombosis and
pulmonary embolism. Hematol J 2003; 4: 97-103. 11. Bockenstedt P. D-dimer in venous thromboembolism. N Engl J Med. 349;12:1203-4. 12. Dempfle CE. Validation, calibration, and specificity of quantitative D-dimer assays. Semin Vasc
Med 2005; 5: 315-20. 13. Kelly J, Hunt B. A clinical probability assessment and D-dimer measurement should be the initial
step in the investigation of suspected venous thromboembolism. Chest 2003; 124: 1116-9. 14. Keeling DM, Mackie IJ, Moody A, Watson HG; The Haemostasis and Thrombosis Task Force of
the British Committee for Standards in Haematology. The Diagnosis of deep vein thrombosis insymptomatic outpatients and the potential for clinical assessment and D-dimer assays to reducethe need for diagnostic imaging. Br J Haematol 2004; 124: 15-25.
15. American College of Emergency Physicians (ACEP) Clinical Policies Committee; Clinical PoliciesSubcommittee on Suspected Pulmonary Embolism. Clinical policy: critical issues in the evaluationand management of adult patients presenting with suspected pulmonary embolism. Ann EmergMed 2003; 41: 257-70.
16. American College of Emergency Physicians (ACEP) Clinical Policies Committee; Clinical PoliciesSubcommittee on Suspected Lower-Extremity Deep Venous Thrombosis. Clinical policy: criticalissues in the evaluation and management of adult patients presenting with suspectedlower-extremity venous thrombosis. Ann Emerg Med 2003; 42: 124-35.
17. Stein PD, Woodard PK, Weg JG, Wakefield TW, Tapson VF, Sostman HD, Sos TA, Quinn DA,Leeper KV Jr, Hull RD, Hales CA, Gottschalk A, Goodman LR, Fowler SE, Buckley JD; PIOPED IIInvestigators. Diagnostic pathways in acute pulmonary embolism: recommendations of thePIOPED II investigators. Am J Med 2006; 119: 1048-55.
18. Reber G, de Moerloose P. D-dimer assays for the exclusion of venous thromboembolism. SeminThromb Hemost 2000;26:619-24.
19. de Moerloose P, Bounameaux H, Wells PH. D-dimer testing and venous thromboembolism: fourview points. J Thromb Haemost 2005; 3: 380-2.
20. Righini M, Aujesky D, Roy PM, Cornuz J, de Moerloose P, Bounameaux H, Perrier A. Clinicalusefulness of D-dimer depending on clinical probability and cutoff value in outpatients withsuspected pulmonary embolism. Arch Intern Med 2004; 164: 2483-7.
21. Kruip MJ, Leclercq MG, van der Heul C, Prins MH, Büller HR. Diagnostic strategies for excludingpulmonary embolism in clinical outcome studies. A systematic review. Ann Intern Med 2003; 138: 941-51.
22. Kruip MJ, Slob MJ, Schijen JH, van der Heul C, Büller HR. Use of a clinical decision rule incombination with D-dimer concentration in diagnostic workup of patients with suspectedpulmonary embolism: a prospective management study. Arch Intern Med 2002; 162: 1631-5.
23. Perrier A, Desmarais S, Miron MJ, de Moerloose P, Lepage R, Slosman D, Didier D, Unger PF,Patenaude JV, Bounameaux H. Non-invasive diagnosis of venous thromboembolism inoutpatients. Lancet 1999;353:190-5.
24. Perrier A, Roy PM, Aujesky D, Chagnon I, Howarth N, Gourdier AL, Leftheriotis G, Barghouth G,Cornuz J, Hayoz D, Bounameaux H. Diagnosing pulmonary embolism in outpatients with clinicalassessment, D-dimer measurement, venous ultrasound, and helical computed tomography: amulticenter management study. Am J Med 2004;116:291-9.
23
25. Brown MD, Vance SJ, Kline JA. An emergency department guideline for the diagnosis ofpulmonary embolism: an outcome study. Acad Emerg Med 2005; 12: 20-5.
26. Perrier A, Roy PM, Sanchez O, Le Gal G, Meyer G, Gourdier AL, Furber A, Revel MP, Howarth N,Davido A, Bounameaux H. Multidetector-row computed tomography in suspected pulmonaryembolism. N Engl J Med 2005; 352: 1760-8.
27. van Belle A, Büller HR, Huisman MV, Huisman PM, Kaasjager K, Kamphuisen PW, Kramer MH,Kruip MJ, Kwakkel-van Erp JM, Leebeek FW, Nijkeuter M, Prins MH, Söhne M, Tick LW;Christopher Study Investigators. Effectiveness of managing suspected pulmonary embolism usingan algorithm combining clinical probability, D-dimer testing, and computed tomography. JAMA2006; 295: 172-9.
28. Goekoop RJ, Steeghs N, Niessen RW, Jonkers GJ, Dik H, Castel A, Werker-van Gelder L, VlasveldT, van Klink RC, Planken EV, Huisman MV. Simple and safe exclusion of pulmonary embolism inoutpatients using quantitative D-dimer and Wells’ simplified decision rule. Thromb Haemost2007; 97: 146-50.
29. Kelly J, Hunt BJ. The utility of pretest probability assessment in patients with clinically suspectedvenous thromboembolism. J Thromb Haemost 2003; 1: 1888-96.
30. Anderson DR, Kovacs MJ, Kovacs G, Stiell I, Mitchell M, Khoury V, Dryer J, Ward J, Wells PS.Combined use of clinical assessment and D-dimer to improve the management of patientspresenting to the emergency department with suspected deep vein thrombosis (the EDITEDStudy). J Thromb Haemost 2003; 1: 645-51.
31. Wells PS, Anderson DR, Rodger M, Forgie M, Kearon C, Dreyer J, Kovacs G, Mitchell M,Lewandowski B, Kovacs MJ. Evaluation of D-dimer in the diagnosis of suspected deep-veinthrombosis. N Engl J Med 2003; 349: 1227-35.
32. Wells PS, Anderson DR, Rodger M, Ginsberg JS, Kearon C, Gent M, Turpie AG, Bormanis J, WeitzJ, Chamberlain M, Bowie D, Barnes D, Hirsh J. Derivation of a simple clinical model to categorizepatients probability of pulmonary embolism: increasing the models utility with the SimpliREDD-dimer. Thromb Haemost 2000; 83: 416-20.
33. Kearon C, Ginsberg JS, Douketis J, Turpie AG, Bates SM, Lee AY, Crowther MA, Weitz JI, Brill-Edwards P, Wells P, Anderson DR, Kovacs MJ, Linkins LA, Julian JA, Bonilla LR, Gent M; CanadianPulmonary Embolism Diagnosis Study (CANPEDS) Group. An evaluation of D-dimer in thediagnosis of pulmonary embolism: a randomized trial. Ann Intern Med 2006; 144: 812-21.
34. Wicki J, Perneger TV, Junod AF, Bounameaux H, Perrier A. Assessing clinical probability ofpulmonary embolism in the emergency ward: a simple score. Arch Intern Med 2001; 161: 92-7.
35. Houdijk WP. Proper observation of patient-related factors is an important determinant in the useof the D-dimer test for exclusion of venous thromboembolism in the ED. Am J Emerg Med 2007;25: 255-6.
36. Schrecengost JE, LeGallo RD, Boyd JC, Moons KG, Gonias SL, Rose CE Jr, Bruns DE. Comparisonof diagnostic accuracies in outpatients and hospitalized patients of D-dimer testing forthe evaluation of suspected pulmonary embolism. Clin Chem 2003; 49: 1483-90.
37. Perrier A. D-dimer for suspected pulmonary embolism. Whom should we test? Chest 2004; 125:807-9.
38. D’Angelo A, D’Allessandro G, Tomassini L, Pittet JL, Dupuy G, Crippa L. Evaluation of a new rapidquantitative D-dimer assay in patients with clinically suspected deep vein thrombosis.Thromb Haemost 1996; 75: 412-6.
39. Heit JA, Minor T, Andrews JC, Larson DR, Li H, Nichols WL. Determinants of plasma fibrinD-dimer sensitivity for acute pulmonary embolism as defined by pulmonary angiography. ArchPathol Lab Med 1999; 123: 235-40.
40. Siragusa S, Terulla V, Pirrelli S, Porta C, Falaschi F, Anastasio R, Guarnone R, Scarabelli M, Odero A,Bressan MA. A rapid D-dimer assay in patients presenting at an emergency room with suspectedacute venous thrombosis: accuracy and relation to clinical variables. Haematologica 2001; 86: 856-61.
41. De Bastos M, De Bastos MR, Bogutchi T, Carneiro-Proietti AB, Rezende SM. Duration ofsymptoms and D-dimer testing in the ruling-out of venous thromboembolism. J ThrombHaemost 2006; 4: 2079-80.
42. Couturaud F, Kearon C, Bates SM, Ginsberg JS. Decrease in sensitivity of D-dimer for acute venousthromboembolism after starting anticoagulant therapy. Blood Coagul Fibrinolysis 2002; 13: 241-6.
43. Kevorkian JP, Halimi C, Segrestaa JM, Drouet L, Soria C. Monitoring of patients with deep-veinthrombosis during and after anticoagulation with D-dimer. Lancet 1998; 351: 571-2.
24
References
44. Jennersjo CM, Fagerberg IH, Karlander SG, Lindahl TL. Normal D-dimer concentration is acommon finding in symptomatic outpatients with distal deep vein thrombosis. Blood CoagulFibrinolysis 2005; 16: 517-23.
45. De Monyé W, Sanson BJ, MacGillavry MR, Pattynama PM, Büller HR, van den Berg-HuysmansAA, Huisman MV, ANTELOPE Study Group. Embolus location affects the sensitivity of a rapidquantitative D-dimer assay in the diagnosis of pulmonary embolism. Am J Respir Crit Care Med2002; 165: 345-8.
46. Righini M, Paris S, Le Gal G, Laroche JP, Perrier A, Bounameaux H. Clinical relevance of distaldeep vein thrombosis. Review of literature data. Thromb Haemost 2006; 95: 56-64.
47. Le Gal G, Righini M, Parent F, van Strijen M, Couturaud F. Diagnosis and management ofsubsegmental pulmonary embolism. J Thromb Haemost 2006; 4: 724-31.
48. Di Nisio M, Squizzato A, Rutjes AW, Büller HR, Zwinderman AH, Bossuyt PM. Diagnostic accuracyof D-dimer test for exclusion of venous thromboembolism: a systematic review. J ThrombHaemost 2007; 5: 296-304.
49. Chabloz P, Reber G, Boehlen F, Hohlfeld P, de Moerloose P. TAFI antigen and D-dimer levelsduring normal pregnancy and at delivery. Br J Haematol 2001; 115: 150-2.
50. Kline JA, Williams GW, Hernandez-Nino J. D-dimer concentrations in normal pregnancy: newdiagnostic thresholds are needed. Clin Chem 2005; 51: 825-9.
51. Epiney M, Boehlen F, Boulvain M, Reber G, Antonelli E, Morales M, Irion O, de MoerlooseP. D-dimer levels during delivery and the post-partum. J Thromb Haemost 2005; 3: 268-71.
52. Nijkeuter M, Ginsberg JS, Huisman MV. Diagnosis of deep vein thrombosis and pulmonaryembolism in pregnancy: a systematic review. J Thromb Haemost 2006; 4: 496-500.
53. Söhne M, Kruip MJ, Nijkeuter M, Tick L, Kwakkel H, Halkes SJ, Huisman MV, Büller HR, TheCHRISTOPHER Study Group. Accuracy of clinical decision rule, D-dimer and spiral computedtomography in patients with malignancy, previous venous thromboembolism, COPD or heart failureand in older patients with suspected pulmonary embolism. J Thromb Haemost 2006; 4: 1042-6.
54. Righini M, Le Gal G, De Lucia S, Roy PM, Meyer G, Aujesky D, Bounameaux H, Perrier A. Clinicalusefulness of D-dimer testing in cancer patients with suspected pulmonary embolism. ThrombHaemost 2006; 95: 715-9.
55. Di Nisio M, Rutjes AW, Büller HR. Combined use of clinical pretest probability and D-dimer testin cancer patients with clinically suspected deep venous thrombosis. J Thromb Haemost 2006; 4:52-7.
56. Le Gal G, Righini M, Roy PM, Sanchez O, Aujesky D, Perrier A, Bounameaux H. Value of D-dimertesting for the exclusion of pulmonary embolism in patients with previous venous thromboem-bolism. Arch Intern Med 2006; 166: 176-80.
57. Palareti G, Legnani C, Cosmi B, Guazzaloca G, Pancani C, Coccheri S. Risk of venous thromboem-bolism recurrence: high negative predictive value of D-dimer performed after oralanticoagulation is stopped. Thromb Haemost 2002; 87: 7-12.
58. Rathbun SW, Whitsett TL, Raskob GE. Negative D-dimer result to exclude recurrent deep venousthrombosis: a management trial. Ann Intern Med 2004; 141: 839-45.
59. Righini M, Goehring C, Bounameaux H, Perrier A. Effects of age on the performance of commondiagnostic tests for pulmonary embolism. Am J Med 2000; 109: 357-61.
60. Söhne M Kamphuisen PW, van Mierlo PJ, Büller HR. Diagnostic stategy using a modified clinicaldecision rule and D-dimer test to rule out pulmonary embolism in elderly in- and outpatients.Thromb Haemost 2005; 94: 206-10.
61. Schutgens RE, Haas FJ, Biesma DH. Reduced efficacy of clinical probability score and D-dimer assay inelderly subjects suspected of having deep vein thrombosis. Br J Haematol 2005; 129: 653-7.
62. Baglin T. Value of D-dimer testing to decide duration of anticoagulation after deep vein thrombosis:not yet. J Thromb Haemost 2006; 4: 2530-2.
63. Palareti G, Legnani C, Cosmi B, Valdré L, Lunghi B, Bernardi F, Coccheri S. Predictive value ofD-dimer test for recurrent venous thromboembolism after anticoagulation withdrawal in subjectswith a previous idiopathic event and in carriers of congenital thrombophilia. Circulation 2003;108: 313-8.
64. Eichinger S, Minar E, Bialonczyk C, Hirschl M, Quehenberger P, Schneider B, Weltermann A,Wagner O, Kyrle PA. D-dimer levels and risk of recurrent venous thromboembolism. JAMA 2003;290: 1071-4.
25
65. Shrivastava S, Ridker PM, Glynn RJ, Goldhaber SZ, Moll S, Bounameaux H, Bauer KA, Kessler CM,Cushman M. D-dimer, factor VIII coagulant activity, low-intensity warfarin and the risk ofrecurrent venous thromboembolism. J Thromb Haemost 2006; 4: 1208-14.
66. Palareti G, Cosmi B, Legnani C, Tosetto A, Brusi C, Lorio A, Pengo V, Ghirarduzzi A, Pattacini C,Testa S, Lensing AW, Tripodi A, the PROLONG Investigators. D-dimer testing to determine theduration of anticoagulation therapy. N Engl J Med 2006; 355: 1780-9.
67. Kamphuisen PW. Can anticoagulant treatment be tailored with biomarkers in patients withvenous thromboembolism? J Thromb Haemost 2006; 4: 1206-7.
68. Le Gal G, Bounameaux H. D-dimer testing to predict recurrence risk in venous thromboem-bolism: looking for a useful threshold: a rebuttal. J Thromb Haemost 2004; 2: 1670-2.
69. McRae S, Tran H, Schulman S, Ginsberg J, Kearon C. Effect of patient’s sex on risk of recurrentvenous thromboembolism: a meta-analysis. Lancet 2006; 368: 371-8.
70. Falk E. Pathogenesis of atherosclerosis. J Am Coll Cardiol 2006; 47: C7-12.
71. Danesh J, Whincup P, Walker M, Lennon L, Thomson A, Appleby P, Rumley A, Lowe GD. FibrinD-dimer and coronary heart disease. Prospective study and meta-analysis. Circulation 2001; 103:2323-7.
72. Bayes-Genis A, Mateo J, Santaló M, Oliver A, Guindo J, Badimon L, Martínez-Rubio A,Fontcuberta J, Schwartz RS, Bayés de Luna A. D-dimer is an early diagnostic marker of coronaryischemia in patients with chest pain. Am Heart J 2000; 140; 379-84.
73. Menown IB, Mathew TP, Gracey HM, Nesbitt GS, Murray P, Young IS, Adgey J. Prediction ofrecurrent events by D-dimer and inflammatory markers in patients with normal cardiac troponin I(PREDICT) study. Am Heart J 2003; 145: 986-92.
74. Shitrit AB, Tzivony D, Shilon Y, Rudensky B, Sulkes J, Gutterer N, Shitrit D. The role of enzyme-linked immunosorbent assay D-dimer in patients with acute coronary syndrome presenting withnormal cardiac enzymes. Blood Coagul Fibrinolysis 2006; 17: 621-4.
75. Ageno W, Finazzi S, Steidl S, Steidl L, Biotti M, Mera V, Melzi d’Eril G, Venco A. Plasma measurement ofD-dimer levels for the early diagnosis of ischemic stroke subtypes. Arch Intern Med 2002; 162: 2589-93.
76. Kelly J, Rudd A, Lewis RR, Coshall C, Parmar K, Moody A, Hunt BJ. Screening for proximal deepvein thrombosis after acute ischemic stroke: a prospective study using clinical factors and plasmaD-dimer. J Thromb Haemost 2004; 2: 1321-6.
77. Barber M, Langhorne P, Rumley A, Lowe GD, Stott DJ. D-dimer predicts early clinical progressionin ischemic stroke. Confirmation using routine clinical assays. Stroke 2006; 37: 1113-5.
78. Delgado P, Alvarez-Sabin J, Abilleira S, Santamarina E, Purroy F, Arenillas JF, Molina CA,Fernandez-Cadenas I, Rosell A, Montaner J. Plasma D-dimer predicts poor outcome after acuteintracerebral hemorrhage. Neurology 2006; 67: 94-8.
79. Tait RC, Rumley A, McMahon AD, Murdoch DL, O’Neill KF, Wallace IW, Lowe GDO. FibrinD-dimer, by three different assays, is an independent predictor of future stroke in patients withatrial fibrillation. J Thromb Haemost 2005; 3 (Suppl. 1): OR195.
80. Alehagen U, Dahlström U, Lindahl TL. Elevated D-dimer is an independent risk factor forcardiovascular death in out-patients with symptoms compatible with heart failure. ThrombHaemost 2004; 92: 1250-8.
81. Marcucci R, Gori AM, Giannotti F, Baldi M, Verdiani V, Del Pace S, Nozzoli C,Abbate R. Markers of hypercoagulability and inflammation predict mortality in patients with heartfailure. J Thromb Haemost 2006; 4: 1017-22.

bioMérieux S.A.69280 Marcy l’EtoileFranceTel. : 33 (0)4 78 87 20 00Fax : 33 (0)4 78 87 20 90
www.biomerieux.com06-0
7 /
010G
B990
13A
/ Th
is d
ocum
ent i
s no
t leg
ally
bin
ding
. bio
Mér
ieux
res
erve
s th
e rig
ht to
mod
ify s
peci
ficat
ions
with
out n
otic
e /
BIO
MER
IEU
X, th
e bl
ue lo
go a
nd V
IDAS
and
VID
ASD
-Dim
er E
xclu
sion
are
use
d, p
endi
ng a
nd/o
r re
gist
ered
trad
emar
ks b
elon
ging
tobi
oMér
ieux
S.A
. or
one
of it
s su
bsid
iarie
s /
Clin
ical
sco
res
by k
ind
perm
issi
on o
f Dr
Wel
ls a
nd D
r Pe
rrier
/ b
ioM
érie
ux S
A RC
S Ly
on 6
73 6
20 3
99 /
Pho
to: N
. Bou
chut
/ P
rinte
d in
Fra
nce
/ TL
McC
ANN
SAN
TE LY
ON
/ RC
S Ly
on B
398
160
242
The information in this booklet is given as a guideline only and is not intended to be exhaustive.
It in no way binds bioMérieux S.A. to the diagnosis established or the treatment prescribed by the physician.
Your stamp





![Prospective evaluation of Innovance D-dimer in the exclusion of venous thromboembolism [VTE]. Robert Gosselin, CLS Department of Clinical Pathology and](https://img.pdfslide.us/doc/110x75/56649ddc5503460f94ad3d3c/prospective-evaluation-of-innovance-d-dimer-in-the-exclusion-of-venous-thromboembolism.jpg)