Embed Size (px)
Citation preview

1
The following pathways have been developed through multidisciplinary efforts with physicians from the Mary Bird Perkins – Our Lady of the Lake Cancer Center. These pathways should be used as a supplemental guide for treatment for physicians at the Mary Bird Perkins – Our Lady of the Lake Cancer Center, and are not intended to replace the independent medical or professional judgment of physicians or other health care providers
Mesothelioma Clinical Pathways
Source: National Comprehensive Cancer Network. Malignant Pleural Mesothelioma (Version 3.2016). https://www.nccn.org/professionals/physician_gls/pdf/mpm_blocks.pdf.
*Approved by the Mesothelioma Specialty Treatment Team December 2016

2
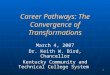
MPM-1
• Chest CT with contrast
Diagnostic Options:• Thoracentesis• Pleural biopsy• VATS
Malignant pleural mesothelioma (MPM) confirmed
Clinical or radiologic findings suspicious of malignant pleural mesothelioma
• Management by a multidisciplinary team with experience in MPM recommended See Pretreatment Evaluation (MPM-2)
• Patient should be referred for psychosocial support, nutritional support/consult, mind/body medicine, and palliative care.
aThere are no data to suggest that screening improves survival
Note: All recommendations are category 2A unless otherwise indicated. NCCN believes that the best management of any cancer patient is in a clinical trialClinical Trials: NCCN believes that the best management of any patient with cancer is in a clinical trial. Participation in clinical trials is especially encouraged.
DIAGNOSTIC EVALUATIONa
MPM-1
• VATS
YES
NO

3
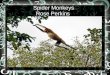
MPM-2
• Abdominal CT with contrast• If suggested by imaging
studies, consider VATSand/or laparascopy ifsuspicion of contralateralor peritoneal disease
• If feasible, med onc/rad onc IP consult; if not, navigator meets with the patient and schedules the following: OP PET/CT, Med Onc consult, and Rad Oncconsult
• Chest MRI with contrast• PFTs including DLCO• PET-CTd
• Mediastinoscopy orEBUS FNA of mediastinallymph nodes
• If PFT is inadequate, perfusion scanning (only if FEV1 <80%)
• Cardiac stress test• ECHO
Clinical stage IV or Sarcomatoidhistology orMedically inoperable
PATHOLOGIC DIAGNOSIS
MPM-2
Malignant pleuralmesothelioma
Clinical stage I-IIIand Epithelial orMixed (biphasic) histologyc,*
Considerobservation for progressiong
orChemotherapyf
Chemotherapyf
Best supportivecaree
See Evidence Blocks on MPM-B (EB-1)
PRETREATMENT EVALUATION
CLINICALASSESSMENT
SURGICALEVALUATION
TREATMENTe
aThere are no data to suggest that screening improves survivalbFor further evaluation of possible chest, spinal, diaphragmatic, or vascular involvement based on CT imaging.cAssessment by multidisciplinary team with experience in malignant pleural mesotheliomadPET-CT should be performed before any pleurodesiseSee Principles of Supportive Care (MPM-A)fSee Principles of Chemotherapy (MPM-B)gObservation may be considered for patients who are asymptomatic with minimal burden of disease if chemotherapy is planned at the time of symptomatic or radiographic progression.
• See Primary Treatment (MPM-3)
PS 3-4
PS 0-2
*Mixed histology defined as ≥ 10% each of epithelioid and sarcomatoidpatterns

4
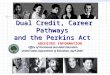
MPM-3
Inductionchemotherapyf
with pemetrexedand cisplatin
Surgicalexploration(preferred)
Resectable
CLINICAL STAGE
MPM-3
Clinical stage I-IIIMedically operable
• Chest CT with contrast
• PET-CT for mediastinalassessment based on CT
Sequentialchemotherapyf +Hemithoracic Rti,1
Chemotherapy
See Evidence Blocks on MPM-B (EB-1)
PRIMARY TREATMENTe
ADJUVANTTREATMENT
eSee Principles of Supportive Care (MPM-A)fSee Principles of Chemotherapy (MPM-B)hSee Principles of Surgery (MPM-C)iSee Principles of Radiation Therapy (MPM-D)1Phase II Study of Hemithoracic Intensity-Modulated Pleural Radiation Therapy (IMPRINT) As Part of Lung-Sparing Multimodality Therapy in Patients With Malignant Pleural Mesothelioma
Pleurectomy/decorticationh
orExtrapleuralpneumonectomyh
(Intraop decision dependent on bulkiness, location of primary tumor, etc.)
Surgicalexplorationh
or
Unresectable
Resectable
Unresectable
Pleurectomy/decorticationh
orExtrapleuralpneumonectomyh
Hemithoracic Rti,1
Chemotherapyf
Based on multidisciplinary
discussion:

5
MPM-A
• Pleural effusions: Talc pleurodesis or pleural catheter, if required for management of pleural effusiona
• Smoking cessation counseling and intervention (http://www.smokefree.gov/). See the NCCN Guidelines for Lung Cancer Screening.
• Pain management: See NCCN Guidelines for Adult Cancer Pain
• Nausea/vomiting: See NCCN Guidelines for Antiemesis
• Psychosocial distress: See NCCN Guidelines for Distress Management
• See NCCN Guidelines for Palliative Care as indicated
MPM-A
PRINCIPLES OF SUPPORTIVE CARE
aRecommend obtaining PET/CT before pleurodesis. Confirm diagnosis of malignant pleural mesothelioma (MPM) prior to pleurodesis. If MPM is suspected, consider evaluation by a multidisciplinary team with expertise in MPM.

6
MPM-B, 1 of 2
PRINCIPLES OF CHEMOTHERAPY (1 of 2)
See Evidence Blocks for First-Line Therapy on MPM-B (EB-1)MPM-B1 OF 2

7
MPM-B, EB-1
MPM-BEB-1
EVIDENCE BLOCK FOR FIRST-LINE CHEMOTHERAPY

8
MPM-B, 2 of 2
PRINCIPLES OF CHEMOTHERAPY (2 of 2)References
MPM-B2 OF 2

9
MPM-C
PRINCIPLES OF SURGERY1
MPM-C

10
MPM-D, 1 of 3
PRINCIPLES OF RADIATION THERAPY (1 of 3)
MPM-D1 OF 3

11
MPM-D, 2 of 3
PRINCIPLES OF RADIATION THERAPY (2 of 3)
MPM-D2 OF 3

12
MPM-D, 3 of 3
PRINCIPLES OF RADIATION THERAPY (3 of 3) - References
MPM-D3 OF 3