Embed Size (px)
Citation preview

Patient journey in acute heart failure – Yu and Fang MEDICOGRAPHIA, Vol 40, No. 1, 2018 5
E vidence-based therapies have resulted in improvements in the outpa-tient management of heart failure (HF). The management of acute HF mayoften be a challenge for the clinician. Nevertheless, despite an increas-
ingly complex population of patients, the overall length of hospital stay has de-creased. The patient journey with an acute HF encompasses the entire se-quence of steps taken to relieve symptoms, to manage precipitating factors,and to provide a post-discharge management plan. This review attempts toprovide clinicians with a concise and practical roadmap for the in-hospitalmanagement of acute HF, focusing on clinical and laboratory criteria that maybe used for the evaluation of patients, the different phases of care, and basictherapeutic algorithms that reflect the available evidence and guidelines.
Medicographia. 2018;40:5-12
Heart failure (HF) is a complex global pandemic characterized by the decreasedability of the heart to pump and/or fill with blood and is associated with highmortality, frequent hospitalization, and reduced quality of life for the individual
and caregiver.1,2 It is a clinical syndrome caused by a structural and/or functionalcardiac abnormality often leading to reduced cardiac output and/or elevated intra-cardiac pressures with a characteristic constellation of symptoms (dyspnea, orthop-nea, lower limb swelling) and signs (elevated jugular venous pressure, pulmonarycongestion).3 Acute HF (AHF) is a life-threatening condition identified as the rapidonset or worsening of symptoms and signs of HF that requires immediate medicalattention.4 On the basis of presence or absence of previous HF, AHF is grouped intoacute decompensated HF—which is a sudden worsening of preexisting stable HF—and de novo HF, which refers to a sudden onset of HF after an acute event.5 HF hasbecome a major health issue in the current society affecting about one in every fivepersons at some point during their lifetime.6 Approximately 26 million people glob-ally are affected with HF, resulting in about 1 million hospitalizations annually in theUnited States and Europe alone.7
There is a significant difference in the prevalence of HF across the world, with ratesas low as 1% in countries such as India and Japan and as high as 4.5% and 6.7%in Singapore and Malaysia, respectively.6,8,9 It has been reported that the Asian HFpopulation is increasing, especially in Hong Kong, due to an aging society and moreinnovative therapy focused on improving survival of cardiovascular diseases. Co-morbidities such as diabetes mellitus and chronic obstructive pulmonary disease(COPD) are also highly prevalent among AHF patients.10 Median length of hospital
Address for correspondence:Cheuk-Man Yu, MD, FRCP, FRACP,Director of Chiu Hin Kwong HeartCenter, Hong Kong Baptist Hospital,Hong Kong & Honorary ClinicalProfessor, Department of Medicine andTherapeutics, The Chinese Universityof Hong Kong, China(email: [email protected])
www.medicographia.com
M A N A G I N G T H E C H A L L E N G E S
O F T H E H E A R T F A I L U R E P A T I E N T ’ S J O U R N E Y
[In an effort to avoid read-missions], patients should be dis-charged in a stable, euvolemichemodynamic state and undergooptimal oral therapy for at least 24hours and have stable renal func-tion. Comorbidities and psycho-logical and social factors shouldalso be carefully evaluated and thecaregivers informed about the eti-ology of the disease, diet, medi-cation use, factors contributing todecompensation of heart failure,and symptoms and signs of heartfailure.”
‘‘ The patient journeyafter admission for acute
heart failure
by C. M. Yu and F. Fang, China
▲
Cheuk-Man YU,1 MD, FRCP, FRACP
Fang FANG,2 PhD1Chiu Hin Kwong Center Hong Kong Baptist Hospital Hong Kong 2Beijing AnZhen Hospital Beijing Institute of Heart, Lung and Blood Vessel, Beijing
CHINA
Medicographia 134 Yu(1)_Mise en page 1 20/03/18 18:23 Page5

M A N A G I N G T H E C H A L L E N G E S
O F T H E H E A R T F A I L U R E P A T I E N T ’ S J O U R N E Y
MEDICOGRAPHIA, Vol 40, No. 1, 2018 Patient journey in acute heart failure – Yu and Fang6
stay in most of the registries ranged between 4 and 11 days,and the mortality rate was 4% to 7%. Mortality within 2 to 3months after discharge was in the range of 7% to 11%,3,10,11
and in some cases, it was 36% at 1 year.12
In the United States, the overall cost for HF hospitalizationsaccounts for about 2% of the health care budget, and hos-pitalization expenses are estimated to double by 2030.6 HFmanagement costs account for about £980 million per yearin the United Kingdom and about $108 billion per annumacross the globe.3 AHF is the most significant contributor as-sociated with the enormous financial burden of HF. Approxi-mately 69% of the total HF costs results from hospital charges,whereas only 18% is attributable to charges for medicine.10
Etiology and signs and symptomsThe etiology of AHF is diverse. A wide range of cardiac struc-tural or functional abnormalities—including disorders of theheart muscle, valves, and rhythm—and other noncardiac caus-es conspire to cause HF (Table I).5,6 Acute myocardial dys-function, acute valve insufficiency, and pericardial tampon-ade are among the most frequent acute primary cardiaccauses of AHF.4 Acute decompensated HF is primarily causedby uncontrolled hypertension (10.7%), nonadherence to di-etary (5.5%) and/or pharmaceutical recommendations (8.9%),pericardial tamponade, aortic dissection, arrhythmias (13.5%),ischemia, and acute coronary syndrome (ACS) (14.7%).5
Arrhythmias, particularly atrial fibrillation (AF), are most com-mon in acute decompensated HF.
The cardinal manifestations of HF are dyspnea at rest or onexertion, fatigue, and worsening fluid retention, apparent aslung congestion and/or swollen ankles and legs.6,13 These
might be accompanied by clinical signs, such aselevated jugular venous pressure, pulmonarycrackles, and peripheral edema.4,13 AHF pa-tients present with signs and symptoms of sys-temic and/or pulmonary congestion.5 Dyspnea,orthopnea, rales, and a third heart sound arethe main clinical signs of pulmonary congestion.The Acute Decompensated Heart Failure Na-tional Registry (ADHERE) data indicate that 89%of patients hospitalized for AHF complained ofshortness of breath, 68% had pulmonary crack-les, and 66% had peripheral edema.12 In ad-dition, pleural effusions, a third heart sound,tachycardia, and congested neck veins are alsotypically observed during AHF. A heart mur-mur is indicative of a significant valvular prob-lem. Percussion and auscultation of the chestmay arouse suspicion of a large pleural effu-sion, pulmonary congestion, or pulmonary ede-ma.14 Signs and symptoms observed in thepatients with AHF are given in Table II.4 On thebasis of clinical signs or symptoms of organ
congestion (wet/dry) and/or peripheral hypoperfusion (cold/warm), patients can be classified into four groups: wet-warm(congested but not hypoperfused), wet-cold (both congest-ed and hypoperfused), dry-cold (hypoperfused but not con-gested), and dry-warm (decongested and well perfused).15
This classification of patients guides in initiating the therapyand also helps in prognostic evaluation.
The patient’s journey in acute heart failureThe journey of AHF patients begins when they consult theemergency department and ends once they are providedappropriate treatment and discharged.16 It encompasses allthe necessary steps taken during the hospital stay and dis-charge. The time course of AHF management once the pa-tient is admitted into a hospital can be categorized into threephases: immediate (in the emergency department, intensivecare unit [ICU], coronary care unit [CCU]), intermediate (in thehospital ward and before discharge), and long-term manage-
SELECTED ABBREVIATIONS AND ACRONYMS
ACS acute coronary syndromeADHERE Acute Decompensated Heart Failure National
RegistryAHF acute heart failureANP atrial natriuretic peptideBNP B-type natriuretic peptideCOPD chronic obstructive pulmonary diseaseECG electrocardiogramHF heart failureICU intensive care unitNP natriuretic peptide
Cardiac causes
• Acute coronary syndrome (ACS)
• Tachyarrhythmia
• Bradyarrhythmia
• Excessive rise in blood pressure
• Nonadherence to treatment
• Valvular heart diseases
• Cardiomyopathies
• Concomitant use of negative inotropic drugs
• Acute mechanical cause: myocardial rupture complicatingACS (free wall rupture, ventricularseptal defect, acute mitral regur-gitation), chest trauma or cardiacintervention, acute native or prosthetic valve incompetencesecondary to endocarditis, aorticdissection or thrombosis
Noncardiac causes
• Infections
• Toxic substances
• Exacerbation of chronic obstruc-tive pulmonary disease
• Pulmonary embolism
• Metabolic/hormonal derangements(eg, thyroid dysfunction, diabeticketosis, adrenal dysfunction,pregnancy and peripartum-relatedabnormalities)
• Cerebrovascular insult
• Surgical interventions
• Renal failure drugs and addictions
• Conditions such as anemia,shunts, and beriberi that increaseblood volume
Table I. Precipitating factors of acute heart failure.
Medicographia 134 Yu(1)_Mise en page 1 20/03/18 18:23 Page6

M A N A G I N G T H E C H A L L E N G E S
O F T H E H E A R T F A I L U R E P A T I E N T ’ S J O U R N E Y
Patient journey in acute heart failure – Yu and Fang MEDICOGRAPHIA, Vol 40, No. 1, 2018 7
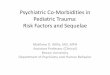
ment.4 During the immediate phase, the patient is given emer-gency care to stabilize the condition, minimize the deteriora-tion of organs, and alleviate the symptoms; diagnostic testsare also performed. In the intermediate stage, the acute eti-ology is diagnosed, and the therapy is titrated/modified ac-cordingly. The last phase constitutes design of a care plan,and patient and caregiver education about measures to im-prove symptoms, quality of life, survival, and to avoid read-missions. A detailed diagnostic and management algorithmfor AHF is given in Figure 1 (page 8).4,6,17
DiagnosisAs AHF can arise from various cardiac abnormalities, identi-fication of actual cause is pivotal in planning of a therapeuticprotocol. Because of the complex nature of HF, variability ofsymptoms among patients, and the fact that symptoms arenot specific to HF only, it is difficult to precisely define HF.4
HF is usually not seen in patients that do not have a relevantmedical history; for example, a previous myocardial infarctionincreases the chances of HF without related signs and symp-toms.4 Life-threatening comorbid conditions should be imme-diately identified and attended to. There is no single diagnos-tic test for HF, rather the clinical diagnosis should constitutecareful historical assessment, including the chronology of theonset of any symptoms, any already diagnosed cardiac illness,and precipitating factors combined with physical examina-tion.14 To facilitate the diagnosis in a timely manner and initiatethe appropriate treatment, the diagnostic workup of AHFneeds to be started in the pre-hospital setting and contin-ued in the emergency department.4 The initial step in the di-agnostic process of AHF is to exclude alternative causes ofthe signs and symptoms. Moreover, the initial clinical evalu-ation of patients should aim to (i) confirm the presence ofAHF; (ii) assess severity of AHF; and (iii) identify precipitatingfactors.18 Patient history and physical examination should pri-marily focus on congestion, as it is a typical feature of AHFand would support the diagnosis of AHF. Symptoms and signsof hypoperfusion indicate severity, and the presence of inap-
propriate stroke volume and clinical and biological signs ofhypoperfusion in AHF defines cardiogenic shock, the mostsevere form of cardiac dysfunction.18 In spite of all these as-sessments, additional tests are required, as the sensitivityand specificity of symptoms are usually not satisfactory.4
u Additional testsu ElectrocardiogramAn electrocardiogram (ECG) is rarely normal in AHF patients,and it helps in identifying cardiac causes and potential pre-cipitants.5,19 Initial evaluation in all suspected AHF patientsshould include a 12-lead ECG to monitor cardiac rhythm.5 Im-mediate ECG is compulsory only in patients with hemody-namic instability and in patients with acute life-threateningcardiac abnormalities.
u EchocardiographyImmediate echocardiography is compulsory in patients withhemodynamic instability and with suspected acute life-threat-ening structural or functional cardiac abnormalities.4 Earlyechocardiography is recommended in de novo AHF and dur-ing unknown cardiac function.
u Chest X-rayEven though chest X-ray is nearly normal in 20% of AHF pa-tients, it can identify some of the most specific features andthe severity of AHF, such as pulmonary venous congestion,pleural effusion, pulmonary edema, and cardiomegaly.20 It canalso identify noncardiac causes of dyspnea, such as pneu-monia or COPD.21
u Natriuretic peptides (NPs)The plasma levels of B-type natriuretic peptide (BNP), N-ter-minal pro–B-type NP (NT-proBNP), or mid-regional proatrialNPs (MR-proANP) should be measured in all patients withacute dyspnea admitted to the emergency department orICU in order to differentiate cardiac causes from noncardiaccauses.18,22,23 NPs have high diagnostic accuracy, and nor-mal levels in suspected patients indicate an unlikely diagnosisof AHF (thresholds: BNP, 100 pg/mL; NT-proBNP, 300 pg/mL;MR-proANP, 120 pg/mL).18 Nonetheless, elevated NP levelsdo not confirm the diagnosis of AHF, as high levels are as-sociated with a variety of cardiac and noncardiac causes.4,18
Moreover, NP levels should be carefully interpreted in obeseand flash pulmonary edema patients, as their levels are ex-ceedingly low in these patients.
u Other laboratory testsOther laboratory tests are also discussed in the 2016 Euro-pean Society of Cardiology (ESC) guidelines.4 Checking of ar-terial blood gas levels should be restricted to patients in whomassessing oxygenation by pulse oximetry is difficult. Cardiactroponin measurements are useful for detecting ACS as anunderlying cause of AHF. Moreover, troponin levels are use-ful for risk stratification and decision making in patients with
Condition
Left-sided congestion
Right-sided congestion
Hypoperfusion
Symptoms/signs
Orthopnea, paroxysmal nocturnal dyspnea,dyspnea on exertion, pulmonary rales (bilateral), peripheral edema (bilateral)
Jugular venous dilatation, peripheral edema,congested hepatomegaly, hepatojugularreflux, ascites, and symptoms of gut congestion
Clinical: cold sweated extremities, oliguria,mental confusion, dizziness, narrow pulsepressure
Laboratory measures: metabolic acidosis,elevated serum lactate, elevated serumcreatinine
Table II. Signs and symptoms of acute heart failure.
Medicographia 134 Yu(1)_Mise en page 1 20/03/18 18:23 Page7

M A N A G I N G T H E C H A L L E N G E S
O F T H E H E A R T F A I L U R E P A T I E N T ’ S J O U R N E Y
MEDICOGRAPHIA, Vol 40, No. 1, 2018 Patient journey in acute heart failure – Yu and Fang8
Figure 1. Diagnostic and management algorithm for acute heart failure. Abbreviations: ACS, acute coronary syndrome; AHF, acute heart failure; BiPAP, bilevel positive airway pressure; CCU, coronary care unit; CPAP, continuous positiveairway pressure; CRP, C-reactive protein; ECG, electrocardiogram; ECLS, extracorporeal life support; ECMO, extracorporeal membrane oxygenation; eGFR, estimatedglomerular filtration rate; HR, heart rate; ICU, intensive care unit; MCS, mechanical circulatory support; SBP, systolic blood pressure; SpO2, peripheral capillary oxygensaturation.
Medicographia 134 Yu(1)_Mise en page 1 20/03/18 18:23 Page8

acute pulmonary embolism as the cause of acute decompen-sated HF. Measuring creatinine, blood urea nitrogen (BUN),and electrolytes every 1 to 2 days during hospitalization un-til discharge is recommended. Frequent measurements aresuggested in severe cases. Procalcitonin levels may be as-sessed in AHF patients with suspected coinfection, such aspneumonia, to guide antibiotic therapy. Liver dysfunction isdetected in about 75% of AHF patients and is closely associ-ated with the severity of the disease.5 Patients at risk of poorprognosis can be identified with abnormal liver function tests,and they may help in optimal management. Thyroid stimulat-ing hormone (TSH) should be measured in patients with new-ly detected AHF, as both hyperthyroidism and hypothyroidismprecipitate AHF. Even though several other biomarkers havebeen investigated for their diagnostic and prognostic valuesin AHF, conclusive evidence that would support recommend-ing them in clinical practice has yet to be generated.
u Acoustic cardiographyAcoustic cardiography is a new technology that is based onthe scientific interpretation of heart sound signals (in partic-ular, the intensity of a third heart sound) and their timing withrespect to the ECG signals or electromechanical activationtime. Recent studies have validated its role in accurate diag-nosis and prognostication of AHF in patients with both im-paired and preserved systolic function.24,25
u Hemodynamic evaluationInvasive hemodynamic evaluation with a pulmonary arterycatheter is not indicated for the routine diagnosis of AHF. Itmay be helpful in select cases of hemodynamically unstablepatients. Noninvasive blood pressure and urine monitoring inhospitalized AHF patients during the acute management pe-riod is recommended.5
u Biomarker studies in Hong KongSince the 1990s, Hong Kong investigators led by ProfessorsCheuk-Man Yu and John E Sanderson have produced asteady stream of original reports addressing circulating bio-markers in HF. They collaborated with other renowned cen-ters for biomarker studies, including the University of OtagoCardioendocrine Laboratory in Christchurch, New Zealand.
The group has elucidated the relationship between cardiacNPs (ANP and BNP) and nitric oxide to measure left ventricu-lar diastolic dysfunction, confirmed the relationship of increas-ing plasma BNP and mortality in acute decompensated HF,and reported the increased levels of a range of other biomark-ers in HF, including adrenomedullin. It has also assessed theneurohormonal response to introduction of b-blocker therapyin HF, examined the relationship between changes in plas-ma NT-proBNP level and response to cardiac resynchroniza-tion therapy in HF, and more recently, the prognostic signifi-cance of serum albumin in HF with preserved ejection fraction(HFpEF).26-32
Post-discharge follow-up of AHF patients should include clin-ical follow-up for symptoms and quality of life scores, serialechocardiographic imaging, serial blood measurement forbiomarkers and their changes, and assessment for clinicaloutcomes.
Management of heart failureAHF is a life-threatening complication requiring immediatemedical attention, presumably within the CCU or ICU. Diag-nostic workup and appropriate pharmacological and non-pharmacological treatment should be initiated in parallel in allpatients with suspected AHF.4 Initial evaluation seeks to iden-tify those patients with severe respiratory distress and poten-tial respiratory failure, as well as severe hypotension. Primaryobjectives in patients with acute symptoms are to provide im-mediate respiratory and cardiovascular support to stabilizethe patient and thereby facilitate symptomatic relief and he-modynamic recovery.4,5,21 Improving oxygenation to requiredlevels, restriction of organ damage, and decreasing the dura-tion of ICU stay are also the aims of initial treatment.5 The ini-tial treatment should include specific therapy (eg, revascular-ization for ACS, antiarrhythmic treatments, antibiotics) directedtoward the etiological factors of AHF and decongestive ther-apy (eg, vasodilators and/or diuretics).18
u Management of precipitating factorsImmediately after the patient is stabilized (usually within 60-120 minutes), precipitating factors that lead to AHF have to beidentified and attended to so as to further reduce the dam-age. The important etiologies that have to be looked for in-clude ACS, hypertensive emergency, arrhythmia, valvular heartdisease, cardiomyopathies and myocardial disease, acute me-chanical cause, and pulmonary embolism. Patients present-ing with ACS should be managed according to the standardguideline-recommended therapy, eg, medical therapy. Con-comitance of AHF and ACS constitute a very-high-risk group,therefore an immediate invasive strategy with an intention toperform percutaneous coronary intervention is recommend-ed.4 AHF caused by severe hypertension typically manifestsas acute pulmonary edema. Prompt and aggressive reduction(25% in the first few hours and cautiously thereafter) with in-travenously administered vasodilators in combination with loopdiuretics is recommended.33-35 Arrhythmias in AHF patientsshould be corrected immediately with medical treatment, elec-trical cardioversion, or temporary pacing.36 Acute mechanicalfailure is essentially diagnosed with echocardiography, andthe treatment typically involves circulatory support with sur-gical or percutaneous intervention.4 Pulmonary embolism inAHF patients should be treated as per standard guidelines,which typically involves primary reperfusion with thromboly-sis—a catheter-based approach—or surgical embolectomy.37
u Oxygen therapy/ventilator support during the early phaseOxygen use in AHF patients should be restricted to hypox-emic patients and acid-base imbalance, and transcutaneous
M A N A G I N G T H E C H A L L E N G E S
O F T H E H E A R T F A I L U R E P A T I E N T ’ S J O U R N E Y
Patient journey in acute heart failure – Yu and Fang MEDICOGRAPHIA, Vol 40, No. 1, 2018 9
Medicographia 134 Yu(1)_Mise en page 1 20/03/18 18:23 Page9

peripheral capillary oxygen saturation (SpO2) should be reg-ularly monitored during oxygen therapy.4 When oxygen is ad-ministered, it is recommended to maintain an O2 saturation lev-el above 95%.21 Noninvasive ventilation (NIV) may be used totemporize severe respiratory distress, hypoxia, or respiratoryacidosis in cooperative patients.21 Two types of NIV, continu-ous positive airway pressure (CPAP) and bilevel positive air-way pressure (BiPAP), are commonly used. Evidence indicatesthat NIV and CPAP are associated with significant reductionsin hospital mortality and the need for intubation in acute pul-monary edema patients.38,39 Anesthetic drugs should be care-fully used, as some of them (eg, propofol) can induce hypo-tension and have cardiodepressive side effects.4
u Pharmacological management of acute heart failureDiuretics, vasodilators, and inotropic agents constitute thefundamental pharmacotherapy of AHF.6 Since diuretics pro-mote diuresis, they are specifically needed in AHF patientswith pulmonary and peripheral edema who require the re-moval of excess fluid to relieve symptoms.6
u DiureticsDiuretic therapy can be initiated in the emergency depart-ment after considering the patient’s systolic blood pressure(SBP) and congestive status. Diuretics should be avoided be-fore adequate perfusion is attained in patients with AHF andsigns of hypoperfusion.4 Intravenous furosemide is the mostcommonly used first-line diuretic in AHF patients. Most pa-tients respond to a bolus dose of 20 to 40 mg. As an alter-native, 10 to 20 mg intravenously administered torasemidemay be considered.4 Dose escalation or addition of a sec-
ond diuretic might be required if symptoms persist. Howev-er, care should be taken to avoid excessive fluid loss andhypokalemia.6
u VasodilatorsIntravenous vasodilators are the second most commonly usedpharmacological agents in AHF.4 Since vasodilators widenblood vessels, they can be used along with diuretics to re-duce edema in lungs and peripheral tissues.6 They are ben-eficial in hypertensive AHF patients and should be avoided inhypotensive patients (SBP <90 mm Hg). Careful monitoringis needed to avoid excessive decreases in blood pressure,and they should be used with caution in mitral and aortic
stenosis.13 Details about different vaso-dilators that are commonly used aregiven in Table III.4
u Inotropes and vasoconstrictorsInotropic agents are the other group ofagents that are recommended in patientswith severe reduction in cardiac outputor cardiogenic shock, which result in re-duced blood flow to vital organs.13 Theseagents are not recommended when hy-povolemia is the underlying cause of hy-potensive AHF. Some of the inotropeswith adrenergic mechanisms could causesinus tachycardia and may induce my-ocardial ischemia and arrhythmias. Asinotropes are associated with increasedmortality risk, they have to be used withcaution by starting with low doses anduptitrating slowly with careful monitor-ing.4,40 Further information on differentinotropes is available in Table III.
Norepinephrine and dopamine, whichare peripheral arterial vasoconstrictors,
are recommended in hypotensive or cardiogenic shock pa-tients to raise blood pressure and redistribute blood to vitalorgans. Norepinephrine is associated with fewer side effectsand lesser mortality risk than dopamine.41
u Other agentsProphylaxis for thromboembolism with heparin or other anti-coagulants is recommended unless contraindicated. In pa-tients with a rapid ventricular rate (>110 beats per minute[bpm]), an intravenous bolus of digoxin (0.25-0.5 mg) is rec-ommended. Vasopressin antagonists, such as tolvaptan, maybe used to treat patients with volume overload and resistanthyponatremia.4 Opiates might be cautiously used to relievedyspnea and anxiety in patients with severe shortness ofbreath, mostly with pulmonary edema. Anxiolytics or seda-tives, such as benzodiazepines (diazepam, lorazepam), canbe cautiously used in patients with agitation or delirium.4
M A N A G I N G T H E C H A L L E N G E S
O F T H E H E A R T F A I L U R E P A T I E N T ’ S J O U R N E Y
MEDICOGRAPHIA, Vol 40, No. 1, 2018 Patient journey in acute heart failure – Yu and Fang10
Table III. Intravenous vasodilators, inotropes and vasopressors recommended in acuteheart failure. *Also a vasodilator. IV, intravenous; SBP, systolic blood pressure.
Initial/loading dose
10-20 mg/min
1 mg/h
0.3 mg/kg/min
2 mg/kg (bolus)
None
None
Optional (6-12 mg/kg, >10 min time)
Optional (25-75 mg/kg)
None
During resuscitation 1 mg IV, (can be repeat-ed every 3-5 min)
Infusion dose
5-200 mg/min
1-10 mg/h
0.3-5 mg/kg/min
0.01 mg/kg/min
<3 mg/kg/min: renal diuretic effect3-5 mg/kg/min: inotropic effect>5 mg/kg/min: inotropic + vasopressor effect
2-20 mg/kg/min
0.1 mg/kg/min (can be increased 0.2 mg/ kg/min or decreased 0.05 mg/kg/min according to SBP)
0.375-0.75 mg/kg/min
0.2-1.0 mg/kg/min
0.05-0.5 mg/kg/min
Drug
Vasodilators
Nitroglycerin
Isosorbide dinitrate
Nitroprusside
Nesiritide
Dopamine
Dobutamine
Levosimendan*
Milrinone*
Norepinephrine
Epinephrine
Inotropes and/or vasopressors
Medicographia 134 Yu(1)_Mise en page 1 20/03/18 18:23 Page10

M A N A G I N G T H E C H A L L E N G E S
O F T H E H E A R T F A I L U R E P A T I E N T ’ S J O U R N E Y
Patient journey in acute heart failure – Yu and Fang MEDICOGRAPHIA, Vol 40, No. 1, 2018 11
u UltrafiltrationUltrafiltration involves the removal of fluid and molecules withlow molecular weight (<20 kDa) across a semipermeable mem-brane by a transmembrane pressure gradient.5,13 Ultrafiltra-tion is not routinely recommended, and it is reserved for hyper-volemic patients in whom diuretic therapy is unsuccessful.
u Mechanical assist devicesWhen medical therapy fails to stabilize the AHF patients, me-chanical circulatory support devices can be used to gain atherapeutic window. Usually, short-term mechanical supportdevices are preferred in AHF. Long-term assist devices areoccasionally used in AHF patients with immediate death riskuntil a thorough clinical evaluation is completed and a thera-peutic protocol is designed.5 Short-term support devices—including percutaneous cardiac support devices, extracor-poreal life support (ECLS), and extracorporeal membraneoxygenation (ECMO)—may be used (typically for few days toweeks) to support AHF or cardiogenic shock patients with leftor biventricular failure until cardiac and other organ functionhave recovered.4 The mechanical circulatory support systems,particularly ECLS and ECMO, can be used as a “bridge to de-cision” during acute and rapidly deteriorating HF or cardiogenicshock in order to stabilize hemodynamics and recover end-organ function while further management plans are decided.42
u Intra-aortic balloon pumpThe intra-aortic balloon pump (IABP) is the most commonlyused percutaneous circulatory assist device that improvesblood supply to coronary arteries and myocardium.5 The ESCguidelines recommend an IABP to support the circulation be-fore the acute mechanical problems are corrected surgical-ly, during severe acute myocarditis, and in selected patientswith acute myocardial ischemia or infarction before, during,and after percutaneous or surgical revascularization.4
Managing cardiogenic shock patientsEchocardiography and ECG are recommended during sus-pected cardiogenic shock. Immediate coronary angiogra-phy with an intent to perform coronary revascularization isrecommended in patients with cardiogenic shock compli-cating ACS.43 Pharmacologic therapy should aim to in-crease cardiac output and blood pressure so as to improveorgan perfusion.4 The ESC guidelines recommend fluidchallenge as the first-line therapy when overt fluid overloadis not evident. After this, an inotropic agent (dobutamine)and a vasopressor (norepinephrine) can be added as need-ed. Organ perfusion and hemodynamics have to be moni-tored continuously during the treatment.
Evidence-based oral neurohormonal therapymanagementUnless hemodynamic instability (SBP <85 mm Hg; heart rate<50 bpm; hypoperfusion), hyperkalemia, or severe renal dys-function is present, oral neurohormonal blockers should not be
terminated in AHF patients.4 Under these circumstances, oralneurohormonal blockers may be temporarily stopped or dailydosage reduced until the patient is stabilized. Except duringcardiogenic shock, b-blockers can be safely continued in AHF.
As neurohormonal blockers have been proven to improveprognosis of HF patients—in particular, HF hospitalization and/or mortality—these drugs should be initiated, resumed, or up-titrated as much as the patient can tolerate before discharge.Management of AHF would not be complete without the op-timization of disease-modifying therapies during the late stageof inpatient therapy when patients are stabilized, which hasbeen stressed in current ESC/ACC (American College of Car-diology)/AHA (American Heart Association) Guidelines. Avail-able therapies include angiotensin-converting enzyme (ACE)inhibitors or angiotensin II receptor blockers (ARBs), b-block-ers, mineralocorticoid receptor antagonists, angiotensin re-ceptor–neprilysin inhibitor, and ivabradine (if heart rate is el-evated). Studies have unequivocally shown that initiation ofguideline-recommended disease-modifying chronic therapiesbefore discharge was associated with significantly better clin-ical outcomes than patients discharged without these med-ications. It implies that hospitalization is an important time tooptimize HF medication for patients with HF.
During the initiation and uptitration of neurohormonal block-ers in the in-hospital therapy, monitoring of vital signs is im-portant. Equal attention should be paid to heart rate controlapart from the tolerability of blood pressure and monitoringof laboratory parameters. Studies have illustrated that heartrate reduction seems to be a partly missed target in the man-agement of HF, as at least 50% of discharged HF patientshave elevated heart rate despite the use of b-blockers.
Patient dischargeAlthough a reduction in duration of in-hospital stay of AHF pa-tients is desirable, discharging patients too early might resultin readmissions.44 Therefore, patients should be dischargedin a stable, euvolemic hemodynamic state under optimal oraltherapy for at least 24 hours and have stable renal function.17
Moreover, comorbidities and psychological and social factorsshould also be carefully evaluated, and the caregivers shouldbe informed about the etiology of the disease, diet, medica-tion use, factors contributing to decompensation of HF, andsymptoms and signs of HF.44
ConclusionAHF is a life-threatening clinical condition associated with sig-nificant mortality. The patient’s journey in AHF involves a thor-ough history and a physical and clinical evaluation to diagnosethe actual cause of the condition, which is followed by cause-specific treatment to reduce/eliminate the acute symptoms.Following the evidence-based guidelines, specific care path-ways ensure that the in-hospital stay and mortality rates arereduced. n
Medicographia 134 Yu(1)_Mise en page 1 20/03/18 18:23 Page11

M A N A G I N G T H E C H A L L E N G E S
O F T H E H E A R T F A I L U R E P A T I E N T ’ S J O U R N E Y
MEDICOGRAPHIA, Vol 40, No. 1, 2018 Patient journey in acute heart failure – Yu and Fang12
References1. Savarese G, Lund LH. Global public health burden of heart failure. Card Fail
Rev. 2017;3(1):7-11.2. National Heart Foundation of Australia. A systematic approach to chronic heart
failure care: a consensus statement. Available at: https://www.heartfoundation.org.au/images/uploads/publications/HF_CHF_consensus_web_FINAL_SP.pdf.Published August 2013. Accessed January 18, 2018.
3. Kurmani S, Squire I. Acute heart failure: definition, classification and epidemi-ology. Current Heart Failure Reports. 2017;14(5):385-392.
4. Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagno-sis and treatment of acute and chronic heart failure: the Task Force for the di-agnosis and treatment of acute and chronic heart failure of the European So-ciety of Cardiology (ESC) Developed with the special contribution of the HeartFailure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129-2200.
5. Ural D, Çavuşoğlu Y, Eren M, et al. Diagnosis and management of acute heartfailure. Anatol J Cardiol. 2015;15(11):860-889.
6. Cowie MR, Anker SD, Cleland JG, et al. Improving care for patients with acuteheart failure: before, during and after hospitalization. ESC Heart Failure. 2014;1(2):110-145.
7. Ambrosy AP, Fonarow GC, Butler J, et al. The global health and economic bur-den of hospitalizations for heart failure: lessons learned from hospitalized heartfailure registries. J Am Coll Cardiol. 2014;63(12):1123-1133.
8. Chaturvedi V, Parakh N, Seth S, et al. Heart failure in India: the INDUS (INDiaUkieri Study) study. J Pract Cardiovasc Sci. 2016;2(1):28-35.
9. Lam CS. Heart failure in Southeast Asia: facts and numbers. ESC Heart Failure.2015;2(2):46-49.
10. Farmakis D, Parissis J, Lekakis J, Filippatos G. Acute heart failure: epidemiology,risk factors, and prevention. Rev Esp Cardiol (Engl Ed). 2015;68(3):245-248.
11. Farmakis D, Papingiotis G, Parissis J. Acute heart failure: epidemiology andsocioeconomic burden. Continuing Cardiol Educ. 2017;3(3):88-92.
12. Adams KF, Fonarow GC, et al. ADHERE Scientific Advisory Committee andInvestigators. Characteristics and outcomes of patients hospitalized for heartfailure in the United States: rationale, design, and preliminary observations fromthe first 100,000 cases in the Acute Decompensated Heart Failure NationalRegistry (ADHERE). Am Heart J. 2005;149(2):209-216.
13. Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the man-agement of heart failure. J Am Coll Cardiol. 2013;62(16):e147-e239.
14. Hummel A, Empen K, Dörr M, Felix SB. De novo acute heart failure and acutelydecompensated chronic heart failure. Dtsch Arztebl Int. 2015;112(17):298-310.
15. Nohria A, Lewis E, Stevenson LW. Medical management of advanced heartfailure. JAMA. 2002;287(5):628-640.
16. Lansang EZ, Horsburgh D, Lee YN, et al. Physicians’ perception of the patientcare pathway for acute heart failure in Asian countries: implications for resourceallocation, preventive strategies and clinical trial design. ASEAN Heart J. 2014;22(1):99-111.
17. Mebazaa A, Yilmaz MB, Levy P, et al. Recommendations on pre-hospital &early hospital management of acute heart failure: a consensus paper from theHeart Failure Association of the European Society of Cardiology, the EuropeanSociety of Emergency Medicine and the Society of Academic Emergency Med-icine. Eur J Heart Fail. 2015;17(6):544-558.
18. Arrigo M, Parissis JT, Akiyama E, Mebazaa A. Understanding acute heart failure:pathophysiology and diagnosis. Eur Heart J Suppl. 2016;18(suppl G):G11-G18.
19. Wang CS, FitzGerald JM, Schulzer M, Mak E, Ayas NT. Does this dyspneicpatient in the emergency department have congestive heart failure? JAMA.2005;294(15):1944-1956.
20. Chakko S, Woska D, Martinez H, et al. Clinical, radiographic, and hemodynam-ic correlations in chronic congestive heart failure: conflicting results may leadto inappropriate care. Am J Med. 1991;90(3):353-359.
21. Kuo DC, Peacock WF. Diagnosing and managing acute heart failure in the emer-gency department. Clin Exp Emerg Med. 2015;2(3):141-149.
22. Gustafsson F, Steensgaard-Hansen F, Badskjaer J, Poulsen AH, Corell P, Hilde-brandt P. Diagnostic and prognostic performance of N-terminal ProBNP in pri-mary care patients with suspected heart failure. J Card Fail. 2005;11(5 suppl):S15-S20.
23. Nielsen OW, Rasmussen V, Christensen NJ, Hansen JF. Neuroendocrine test-ing in community patients with heart disease: plasma N-terminal proatrial natri-uretic peptide predicts morbidity and mortality stronger than catecholaminesand heart rate variability. Scand J Clin Lab Invest. 2004;64(7):619-628.
24. Wang S, Fang F, Liu M, et al. Rapid bedside identification of high-risk popu-lation in heart failure with reduced ejection fraction by acoustic cardiography.Int J Cardiol. 2013;168(3):1881-1886.
25. Wang S, Lam YY, Liu M, et al. Acoustic cardiography helps to identify heartfailure and its phenotypes. Int J Cardiol. 2013;167(3):681-686.
26. Yu CM, Sanderson JE, Shum IO, et al. Diastolic dysfunction and natriuretic pep-tides in systolic heart failure. Higher ANP and BNP levels are associated withthe restrictive filling pattern. Eur Heart J.1996:17(11):1694-1702.
27. Yu CM, Sanderson JE. Plasma brain natriuretic peptide—an independent pre-dictor of cardiovascular mortality in acute heart failure. Eur J Heart Fail. 1999;1(1):59-65.
28. Yu CM, Cheung BM, Leung R, et al. Increase in plasma adrenomedullin in pa-tients with heart failure characterised by diastolic dysfunction. Heart. 2001;86(2):155-160.
29. Yu CM, Fung PC, Chan G, et al. Plasma nitric oxide level in heart failure second-ary to left ventricular diastolic dysfunction. Am J Cardiol. 2001;88(8):867-870.
30. Fung JW, Yu CM, Yip G, et al. Effect of beta blockade (carvedilol or metoprolol)on activation of the renin-angiotensin-aldosterone system and natriuretic pep-tides in chronic heart failure. Am J Cardiol. 2003;92(4):406-410.
31. Yu CM, Fung JW, Zhang Q, et al. Improvement of serum NT-ProBNP predictsimprovement in cardiac function and favorable prognosis after cardiac re-syn-chronization therapy for heart failure. J Card Fail. 2005;11(5 suppl):S42-S46.
32. Liu CM, Chan CP, Yan BP, et al. Albumin levels predict survival in patients withheart failure and preserved ejection fraction. Eur J Heart Fail. 2012;14(1):39-44.
33. Mancia G, Fagard R, Narkiewicz K, et al. 2013 ESH/ESC guidelines for the man-agement of arterial hypertension: the Task Force for the Management of Arte-rial Hypertension of the European Society of Hypertension (ESH) and of theEuropean Society of Cardiology (ESC). Eur Heart J. 2013;34(28):2159-2219.
34. Levy P, Compton S, Welch R, et al. Treatment of severe decompensated heartfailure with high-dose intravenous nitroglycerin: a feasibility and outcome analy-sis. Ann Emerg Med. 2007;50(2):144-152.
35. Cotter G, Metzkor E, Kaluski E, et al. Randomised trial of high-dose isosorbidedinitrate plus low-dose furosemide versus high-dose furosemide plus low-doseisosorbide dinitrate in severe pulmonary oedema. Lancet. 1998;351(9100):389-393.
36. Priori SG, Blomstro¨m-Lundqvist C, Mazzanti A, et al. 2015 ESC Guidelinesfor the management of patients with ventricular arrhythmias and the preven-tion of sudden cardiac death: the Task Force for the Management of Patientswith Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death ofthe European Society of Cardiology (ESC). Eur Heart J. 2015;36(41):2793-2867.
37. Konstantinides SV, Torbicki A, Agnelli G, et al. 2014 ESC Guidelines on thediagnosis and management of acute pulmonary embolism: the Task Force forthe Diagnosis and Management of Acute Pulmonary Embolism of the Euro-pean Society of Cardiology (ESC) Endorsed by the European Respiratory So-ciety (ERS). Eur Heart J. 2014;35(43):3033-3073.
38. Vital FM, Saconato H, Ladeira MT, et al. Non-invasive positive pressure ventila-tion (CPAP or bilevel NPPV) for cardiogenic pulmonary edema. Cochrane Data-base Syst Rev. 2008;(3):CD005351. doi:10.1002/14651858.CD005351.pub2.
39. Vital FM, Ladeira MT, Atallah ÁN. Non-invasive positive pressure ventilation (CPAPor bilevel NPPV) for cardiogenic pulmonary oedema. Cochrane Database SystRev. 2013;(5):CD005351. doi:10.1002/14651858.CD005351.pub3.
40. Delaney A, Bradford C, McCaffrey J, Bagshaw SM, Lee R. Levosimendan for thetreatment of acute severe heart failure: a meta-analysis of randomised con-trolled trials. Int J Cardiol. 2010;138(3):281-289.
41. De Backer D, Biston P, Devriendt J, et al. Comparison of dopamine and nor-epinephrine in the treatment of shock. N Engl J Med. 2010;362(9):779-789.
42. Riebandt J, Haberl T, Mahr S, et al. Preoperative patient optimization using ex-tracorporeal life support improves outcomes of INTERMACS level I patientsreceiving a permanent ventricular assist device. Eur J Cardiothorac Surg.2014;46(3):486-492.
43. Roffi M, Patrono C, Collet JP, et al. 2015 ESC Guidelines for the managementof acute coronary syndromes in patients presenting without persistent ST-seg-ment elevation: Task Force for the Management of Acute Coronary Syndromesin Patients Presenting without Persistent ST-Segment Elevation of the Euro-pean Society of Cardiology (ESC). Eur Heart J. 2016;37(3):267-315.
44. Kaya H, Yilmaz MB. In-hospital journey of patients with heart failure. Int J Car-diovas Acad. 2015;1(1):31-35.
Keywords: acute heart failure; evidence-based management; patient journey
Medicographia 134 Yu(1)_Mise en page 1 20/03/18 18:23 Page12