Embed Size (px)
Citation preview

Vol 30, No.2, 2008
A journal ofmedical informationand internationalcommunicationfrom Servier
87
95
100
106
112
116
121
127
131
Contents continued overleaf...
95I S S U E
ISSN 0243-3397
Medicographia
EDITORIAL
VENOUS VALVE INCOMPETENCE: THE FIRST CULPRIT
IN THE PATHOPHYSIOLOGY OF PRIMARY CHRONIC
VENOUS INSUFFICIENCY. INSUFFISANCE VALVULAIRE
VEINEUSE : PREMIER CHAÎNON DANS LA GÉNÈSE DE
LA MALADIE VEINEUSE CHRONIQUE PRIMAIRE
THE FUNCTIONING OF VENOUS VALVES IN NORMAL
AND PATHOLOGICAL CONDITIONS
EMBRYOLOGY AND DISTRIBUTION OF LOWER LIMB
VENOUS VALVES IN HUMANS
VENOUS VALVE INCOMPETENCE AND REFLUX IN
CHILDHOOD
THE STUDY OF THE SAPHENOFEMORAL JUNCTION
TO UNDERSTAND THE DISTRIBUTION OF REFLUXES
IN CHRONIC VENOUS DISEASE
IMAGING OF VENOUS VALVES: B-FLOW
TRIGGERING MECHANISMS OF VENOUS VALVE
INCOMPETENCE
VENOUS VALVE INCOMPETENCE: THE ROLE OF
GENETIC FACTORS
TREATMENT OF VENOUS VALVE INCOMPETENCE: PAST,CURRENT, AND FUTURE. A REFLECTION ON ITS EVOLU-TION IN COMPARISON WITH PEPTIC ULCER DISEASE
J. BERGAN, USA
F. LURIE, USA
A. CAGGIATI, ITALY
M. SCHADECK, FRANCE
L. TESSARI AND
M. CAPPELLI, ITALY
F. FERRARA AND
M. MIDIRI, ITALY
G. W. SCHMID-SCHÖNBEIN, USA
M. A. PISTORIUS, FRANCE
A. JAWIEN, POLAND
The Venous Valve and Primary Chronic Venous Disease

Vol 30, No.2, 2008 Medicographia
95I S S U E
P. PAI, INDIA /A. S. SABBOUR, EGYPT /A. MANSILHA, PORTUGAL /P. PITTALUGA AND
S. CHASTANET, FRANCE /A. MASEGOSA, SPAIN /A. OBERMAYER, AUSTRIA /K. L. KATSENIS, GREECE /L. VEVERKOVA, CZECH
REPUBLIC / A. K. BOZKURT,TURKEY / C. E. VIRGINI-MAGALHÃES, BRAZIL
F. PITSCH, FRANCE
G. T. JONES,NEW ZEALAND
N. LABROPOULOS, USA
M. R. PERRIN,FRANCE
C. RÉGNIER,FRANCE
I. SPAAK, FRANCE
CONTROVERSIAL QUESTION
THE SAPHENOFEMORAL JUNCTION: TO LIGATE
OR NOT TO LIGATE?
DAFLON 500 MG
DAFLON 500 MG: PROTECTIVE AGAINST VENOUS
VALVE FAILURE
INTERVIEW
ANIMAL MODELS IN CHRONIC VENOUS DISEASE
FOCUS
CUT POINT ON NORMAL AND PATHOLOGICAL VALUES
OF REFLUX
UPDATE
VENOUS VALVE DYSFUNCTION RESTORATION BY
SURGERY IN PRIMARY CHRONIC VENOUS DISEASE
A TOUCH OF FRANCE
THE SCIENCES UNDER LOUIS XVI. A KING TORN
BETWEEN ENLIGHTENMENT AND REVOLUTION
A TOUCH OF FRANCE
MARIE-ANTOINETTE, QUEEN OF FRANCE, QUEEN
OF STYLE
137
149
154
157
163
169
179
...Contents continued from cover page
The Venous Valve andPrimary Chronic Venous Disease

87Venous valve incompetence and primary chronic venous insufficiency – Bergan MEDICOGRAPHIA, VOL 30, No. 2, 2008
CHRONIC VENOUS INSUFFICIENCY (CVI) IS MANIFESTED IN THElower extremities. Its most obvious sign is protuberant, saccularvaricose veins. These fail to fulfill their assigned function of trans-porting blood from the lower extremities to the heart. Instead, they
allow the weight of the column of blood from the right atrium as it is transmitted through thevalveless vena cava and iliac veins to be expressed in the thigh and leg. There, the venous hyper-tension initiates a cascade of inflammatory reactions that may progress to edema, venous eczema,ankle skin hyperpigmentation, atrophie blanche, and other manifestations such as lipoderma-tosclerosis and venous leg ulcers.
Recently, considerable progress has been made in understanding the pathophysiological pro-cesses at the cellular and molecular level that cause these diverse manifestations. These may be-come targets for preventative pharmacologic intervention. If so, there will be a change in focusfrom ablation to preservation. The goal of this editorial is to explain how the processes of venousinsufficiency begin because of initial venous valve failure and how they are perpetuated by thatvalve failure.
Venous hypertensionIn spite of the diversity of signs and symptoms associated with CVI, it is likely that they are allrelated to venous hypertension. Venous hypertension involves reflux through incompetentvalves.1,2 Pressure in the veins of the leg is determined by two components, a hydrostatic compo-nent, described above, and a hydrodynamic component related to pressure generated by contrac-tion of the skeletal muscles of the leg that is transmitted to the venular capillary network. Bothcomponents are profoundly modified by the action of the venous valves. During standing with-out skeletal muscle activity, venous pressures in the leg are determined by the hydrostatic com-ponent and capillary flow. Skeletal muscle contractions, as during ambulation or exercise, in-crease pressure within the deep leg veins. Competent venous valves ensure that the resultingblood flow is toward the heart, leading to emptying of the deep and superficial venous systemsand a fall in venous pressure. Even quite small leg movements can provide significant pumpingaction. However, in the absence of competent valves, venous pressure fails to fall with leg move-ments, and the pressures generated by muscle contraction are transmitted to the skin micro-circulation. Skin changes in CVI stem from venous pressures in the leg that reach higher thannormal levels and are elevated for abnormally prolonged periods of time.
Valvular incompetenceVenous valve incompetence is a central feature of venous hypertension that in turn underlies mostof the signs characteristic of chronic venous disease (CVD). Alterations and damage to valves havebeen noted angioscopically. These include stretching, splitting, tearing, thinning, and adhesionof valve leaflets.3 Reduction in the number of valves has been observed in segments of saphenousveins from patients with CVI.4
E D I T O R I A L
Address for correspondence:John Bergan, MD, 9850 Genesee, Suite 410, La Jolla, CA 92037, USA(e-mail: [email protected])
Medicographia.2008;30:87-94.
Venous valve incompetence: the first culprit in the pathophysiology of primary chronic venous insufficiency
b y J . B e r g a n , U S A
John BERGAN, MD The Vein Institute of La JollaDepartment of SurgeryUCSD School of MedicineLa Jolla, CA, USA

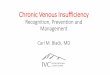
These observations do not reveal the mechanism of valvular disappearance or how such re-modeling fits into the pathophysiological sequence of events in CVD. However, an important stepforward came when we examined valves from great saphenous veins removed from patients withCVD.5 Using a monoclonal antibody specific for monocytes and tissue macrophages, we foundinfiltration of valve leaflets and the venous wall by monocytes and macrophages in all vein spec-imens from CVD patients and in none from controls with normal veins. Infiltration was greaterin the valve sinus and proximal venous wall than in the distal aspect of the valve leaflet and dis-tal vein wall (Figure 1A). This suggested a link with elevated venous pressure. Further investi-gations have shown that inflammation and subsequent remodeling of the venous valves and wallare the fundamental mechanisms underlying valve damage and the lesions seen angioscopically.6
Molecular mechanismsHemodynamic forces, such as blood pressure changesin the wall and sheer stress, as well as varying planesof laminar and turbulent flow, induce activation ofthe leukocytes and endothelial cells. Integrins appearto act as intermediaries, and expression of adhesionmolecules has been observed. Breakdown of the extra-cellular matrix of the media and adventitia throughactivation of matrix metalloproteases (MMPs) hasbeen observed. In particular, expression of MMP-1,MMP-2, MMP-9, and tissue inhibitors of metallopro-teinase (TIMP) have been studied. Telangiectasias,reticular veins, and true varicose veins appear to be aconsequence of the changes induced by venous hy-pertension and sheer stress (Figure 1B). As describedabove, when saphenous vein valves are observed an-gioscopically at the time of vein stripping, they show
severe deformities. The animal model of induced venous hypertension that we have workedwith demonstrates early venous valve changes that replicate those observed in humans.
This observation provides a link from venous hypertension to an induced inflammatory re-action that stimulates the valve damage. Thus the model has been useful for defining the fun-damental mechanisms that cause venous valve failure and varicose veins. In the future it mayprove useful in pharmacologic testing to identify agents that will be useful to prevent or treat ve-nous insufficiency.
Primary venous insufficiencyA dysfunctional venous system is caused for the main part by functional failure of venous valves.The molecular mechanisms uncovered recently that enter into functional valve failure are men-tioned above. Other factors are traditionally cited as contributing to venous valve failure; theseinclude female sex, pregnancy, obesity, a standing occupation in women,7 and heredity.8,9 An in-crease in vein diameter is one cause of valve dysfunction and reflux. Progesterone inhibits smoothmuscle contraction. This is useful in preventing uterine contraction and spontaneous abortionin pregnancy. However, preventing vein wall smooth muscle contraction allows passive dilationof veins and when a critical diameter is reached, a functioning venous valve becomes dysfunc-tional or incompetent. As half of a women’s adult lifetime is under the influence of progesterone,and this is exacerbated markedly during pregnancy, it is no wonder that primary venous insuf-ficiency is twice as common in women than in men.7
The effect of persistent valvular reflux is a chronic increase in distal venous pressure. This ve-nous pressure increases as one proceeds from the inguinal ligament past the knee to the ankle.The prolonged venous hypertension initiates a cascade of pathologic events. These manifestthemselves clinically as lower extremity edema, pain, itching, skin discoloration, and ulceration.10
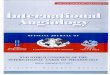
The earliest signs of venous insufficiency are often varicose veins in the epidermis and dermis,and these are called telangiectasias (Figure 2). Slightly deeper, are flat, blue-green veins of thereticular (network) system. These may become varicose as well. Finally, deeper yet, are the vari-cose veins themselves. All of these abnormal veins and venules have one thing in common: theyare elongated, tortuous, and have dysfunctional venous valves.
Manifestations of telangiectasias, reticular varicosities, and varicose veins are grouped to-gether under the term primary venous insufficiency.
E D I T O R I A L
88 Venous valve incompetence and primary chronic venous insufficiency – BerganMEDICOGRAPHIA, VOL 30, No. 2, 2008
Figure 1. A. A normalvenous valve is remarkably
adapted to its function ofallowing blood transport
proximally and haltingblood flow in a distal direc-tion. Note the vein wall and
its enclosed valve sinus.B. Venous hypertension is
responsible for initiating theinflammatory reaction that
results in vein wall weaken-ing, elongation, and dila-
tion. Also, such hyperten-sion triggers the inflamma-
tory reaction that causesvalve damage and eventualdisappearance of the valve.
A B

Chronic venous insufficiencySkin changes of hyperpigmentation, scarring fromprevious ulceration, and active ulcerations aregrouped together under the term CVI. Numeroustheories have been postulated regarding the causeof CVI and that of venous ulceration.10,11
Some theories proposed in the last centuryhave shown remarkable prescience. An exampleis the theory of venous stasis first published in amanuscript by John Homans of Harvard in 1917.12
It was a treatise on diagnosis and management ofpatients with CVI, and in it, Dr Homans coinedthe term “postphlebitic syndrome” to describe theskin changes of CVI. He stated that, “Overstretch-ing of the vein walls and destruction of thevalves… interferes with the nutritionof the skin…therefore, skin which is bathed under pressurewith stagnant venous blood will form permanentopen sores or ulcers.” That he called attention todestruction of valves was remarkable. However,that statement, like many others that describe venous conditions and their treatments, is steepedin dogma, and apart from the description of damaged valves, is short on observational fact. Ac-tually, it is unlikely that Homans observed valve damage as we know it in primary venous in-sufficiency. He may have seen the ravages of the phlebitic valve destruction with adherence ofleaflets to one another and to the vein wall. The term stasis ulcer honors that misconception, asdo the terms venous stasis disease and stasis dermatitis.
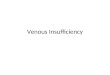
Alfred Blalock, who later developed pericardiac surgery, disproved the theory of stagnantblood by studying oxygen content from varicose veins and normal veins.13 He pointed out thatthe oxygen content of the femoral vein in patients with severe CVI was greater than the oxygencontent of the contralateral nonaffected limb. Because oxygen content was higher, some inves-tigators thought that arteriovenous fistulas caused venous stasis and varicose veins. That theory,though disproved, has some basis in fact, sincethe entire thermoregulatory apparatus in limbsdepends on the opening and closing of arterialvenous shunts (Figure 3). These shunts are im-portant, as they explain some terrible accidentsthat happen during sclerotherapy when sclerosantentering a vein is shunted into the arterial sys-tem and distributed in its normal arborization.14
Microsphere investigations have failed to showsuch shunting, and the theory of arteriovenouscommunications has died despite the fact thatthese shunts actually exist and do open and closeunder the influence of venous hypertension andambient temperature.
Hypoxia and its part in causation of CVI wereinvestigated throughout the last 25 years of the20th century. English investigators thought thata fibrin cuff, observed histologically, blockedtransport of oxygen and was responsible for skinchanges in CVI at the ankles and distally.10 Thattheory has been abandoned.
There are two elements that interact to causeall of the manifestations of lower extremity severe CVI. These are failure of the vein valves, thefirst culprit, and subsequently the skin changes of hyperpigmentation, atrophie blanche, andskin ulceration at the ankles. Both of these are related to venous hypertension. Our work sug-gests that venous hypertension causes a shear stress–dependent leukocyte-endothelial inter-action, which has all of the manifestations of chronic inflammation.15 These are leukocyte rolling,firm adhesion to endothelium, and subsequent migration of the cells through the endothelial
E D I T O R I A L
89Venous valve incompetence and primary chronic venous insufficiency – Bergan MEDICOGRAPHIA, VOL 30, No. 2, 2008
Figure 3. This diagram illustrates the close relationships betweenarterioles, capillaries, venules, veins, and adjacent nerves. A-V shunting is easy to imagine, as is the effect of dilated venousvaricosities on adjacent nerves.
Figure 2. This diagram, drawn courtesy of George Somjen ofVictoria, Australia, shows the intimate relationships of telang-iectasias, reticular veins, varicose tributary veins, and direct andindirect perforating veins. Note how venous hypertension in anysegment affects related segments. LSV, long saphenous vein.
Capillary
Lymphatic
Nerve
Arteriole
Precapillarysphincter
ThermoregulatoryA-V shunt
Venule
Perforatingvein
Perforatingvein
Varicosetributary
Reticular vein
Deep vein
Telangiectasia
Dermis
Superficialfascia
Deep fascia

E D I T O R I A L
90 Venous valve incompetence and primary chronic venous insufficiency – BerganMEDICOGRAPHIA, VOL 30, No. 2, 2008
barrier into parenchyma of valves and vein walls.16 There, macrophages elaborate MMPs, whichdestroy elastin and possibly collagen as well. Vein walls become stretched and elongated. Veinvalves become perforated, torn, and even scarred to the point of near total absence. These changesare seen both macroscopically and angioscopically15 and have been produced experimentally byconstructing an arteriovenous fistula.
The second manifestation of CVI is expressed in the skin. There, leukocytes are also respon-sible for the observed changes. Skin biopsies showed that in liposclerotic eczematous skin,macrophages and lymphocytes were predominant.17 Infiltration of leukocytes into the extra-cellular space has been documented by observing the localization of these leukocytes aroundcapillaries and postcapillary venules. Accompanying the leukocytes is a disorganized collagendeposition. Clearly, CVI of the skin and its subcutaneous tissues is a disease of chronic inflam-mation, again, dependent upon venous hypertension. The injury involves extravasation of macro-molecules and red blood cells into the dermal interstitium. Red blood cell degradation productsand interstitial protein extravasations are potent chemoattractants and represent the initialchronic inflammatory signal responsible for leukocyte recruitment.18 As indicated, these followvalve failure, the first culprit in primary and secondary venous insufficiency.
ConclusionsThe processes of valve and vein wall damage and the advanced skin changes of CVI are the resultof sterile inflammatory reactions. Valve failure is triggered by venous hypertension and, in turn,causes distal venous hypertension. Therefore, future therapy must be directed at preventing suchvenous hypertension by preventing valve failure. �
REFERENCES1. Labropoulos N. Hemodynamic changes according to the CEAPclassification. Phlebolymphology. 2003;40:130-136.2. Kistner RL, Eklof B, Masuda EM. Diagnosis of chronic venousdisease of the lower extremities: “CEAP” classification. Mayo ClinProc. 1996;71:338-345.3. Van Cleef JF, Hugentobler JP, Desvaux P, Griton P, Cloarec M.Étude endoscopique des reflux valvulaires saphéniens. J Mal Vasc.1992;17(suppl B):113-116.4. Sales CM, Rosenthal D, Petrillo KA, et al. The valvular appa-ratus in venous insufficiency: a problem of quantity? Ann VascSurg. 1998;12:153-155.5. Ono T, Bergan JJ, Schmid-Schönbein GW, Takase S. Monocyteinfiltration into venous valves. J Vasc Surg. 1998;27:158-166.6. Pascarella L, Schmid-Schonbein GW, Bergan J. An animalmodel of venous hypertension: the role of inflammation in ve-nous valve failure. J Vasc Surg. 2005;41:303-311.7. Criqui M, Denenberg JO, Bergan JJ, Langer RD, Fronek A. Riskfactors for chronic venous disease: the San Diego populationstudy. J Vasc Surg. 2007;46:551-337.8. Mellor RH, Brice G, Stanton AW, et al; Lymphoedema ResearchConsortium. Mutations in FOXC2 are strongly associated withprimary valve failure in veins of the lower limb. Circulation.2007;115:1912-1920.9. Saiki S, Sakai K, Saiki M, et al. Varicose veins associated withCADASIL result from a novel mutation in the Notch3 gene. Neu-rology. 2006;67:337-339.
10. Browse NL, Burnand KG. The cause of venous ulceration.Lancet.1982;320:243-245.11. Coleridge Smith PD. Treatment of microcirculation disordersin venous leg ulcer. In: Messmer K, ed. Microcirculation in Chron-ic Venous Insufficiency. Basel, Switzerland: Karger Publishers;2001:1-10.12. Homans J. The aetiology and treatment of venous ulcers ofthe leg. Surg Gynec Obst. 1917;24:300-311.13. Blalock A. Oxygen content of blood in patients with varicoseveins. Arch Surg. 1929;19:898-904.14. Bergan JJ, Weiss RA, Goldman MP. Extensive tissue necrosisfollowing high-concentration sclerotherapy for varicose veins.Dermatol Surg. 2000;26:535-542.15. Schmid-Schönbein GW, Takase S, Bergan JJ. New advances inunderstanding the pathophysiology of chronic venous insuffi-ciency. Angiology. 2001;52(suppl 1):S27-S34.16. Takase S, Lerond L, Bergan JJ, Schmid-Schönbein GW. Theinflammatory reaction during venous hypertension in the rat.Microcirculation. 2000;7:41-52.17. Wilkerson LS, Bunker C, Edward JCW, Scurr JH, ColeridgeSmith PD. Leukocutes: their role in the etiopathogenesis of skindamage in venous disease. J Vasc Surg. 1993;27:669-675.18. Hoshino S, Satokawa H, Ono T, Igari T. Surgical treatmentfor varicose veins of the legs using intraoperative angioscopy. In:Raymond-Martimbeau P, Prescott R, Zummo M, eds. Phlebolo-gie 92. Paris, France: John Libbey Eurotext; 1992:1083-1085.
Keywords: venous valve incompetence; venous hypertension; venous insufficiency; molecular mechanisms; inflammation

L’ INSUFFISANCE VEINEUSE CHRONIQUE (IVC) SE MANIFESTEdans les membres inférieurs. Son signe le plus évident est la pré-sence de veines variqueuses saillantes et sacciformes. Ces veinesn’arrivent pas à remplir leur fonction, qui consiste à transporter
le sang des membres inférieurs vers le cœur. Au lieu de cela, elles permettent au poids de la co-lonne de sang provenant de l’oreillette droite par l’intermédiaire de la veine cave et des veinesiliaques sans valvules de se manifester dans la cuisse et la jambe. Là, l’hypertension veineuseamorce une cascade de réactions inflammatoires susceptibles de progresser vers un œdème, uneczéma veineux, une hyperpigmentation cutanée de la cheville, une atrophie blanche et d’autresmanifestations telles qu’une lipodermatosclérose et des ulcères veineux de jambes.
Ces derniers temps, des progrès considérables ont été faits dans la compréhension des pro-cessus physiopathologiques à l’origine de ces diverses manifestations aux niveaux cellulaire etmoléculaire. Ces processus sont susceptibles de devenir les cibles d’une intervention pharma-cologique préventive faisant glisser le traitement de l’ablation à la conservation. L’objectif decet éditorial est d’expliquer comment l’insuffisance veineuse enclenche et entretient une insuf-fisance valvulaire veineuse initiale.
Hypertension veineuseIl est probable que tous les signes et symptômes associés à l’IVC soient liés à l’hypertension vei-neuse. L’hypertension veineuse implique un reflux dû à une insuffisance valvulaire1,2. La pres-sion dans les veines de la jambe est déterminée par deux composantes, une composante hydro-statique, décrite ci-dessus, et une composante hydrodynamique en rapport avec la pressiongénérée par la contraction des muscles squelettiques de la jambe et transmise jusqu’au réseaucapillaire (formé de veinules). Ces deux composantes sont profondément modifiées par l’actiondes valvules veineuses. En position debout sans activité des muscles squelettiques, les pressionsveineuses de la jambe sont déterminées par la composante hydrostatique et le débit capillaire.Les contractions des muscles squelettiques, telles qu’elles existent pendant la marche ou l’exer-cice, augmentent la pression à l’intérieur des veines profondes de la jambe. L’étanchéité des val-vules veineuses garantit que le flux sanguin qui en résulte est dirigé vers le cœur, ce qui conduità la vidange des systèmes veineux profond et superficiel et à une chute de la pression veineuse.Même des mouvements de jambe relativement petits peuvent faire fonctionner la pompe defaçon significative.
Cependant, en l’absence de valvules étanches, la pression veineuse ne chute pas avec lesmouvements de la jambe et les pressions générées par la contraction musculaire sont transmisesà la microcirculation cutanée. Les changements cutanés de l’IVC sont dus aux pressions vei-neuses de la jambe, qui atteignent des niveaux supérieurs à la normale et restent élevés pendantdes durées anormalement prolongées.
É D I T O R I A L
91Insuffisance valvulaire veineuse et maladie veineuse chronique primaire – Bergan MEDICOGRAPHIA, VOL 30, No. 2, 2008
Insuffisance valvulaire veineuse : premier chaînon dans lagénèse de la maladie veineuse chronique primaire
p a r J . B e r g a n , É t a t s - U n i s

Insuffisance veineuseL’insuffisance valvulaire veineuse est une caractéristique centrale de l’hypertension veineusequi, à son tour, est une cause sous-jacente de la plupart des signes caractéristiques de la mala-die veineuse chronique (MVC). Des modifications et des lésions des valvules ont été observées parangioscopie. Celles-ci incluent l’étirement, la rupture, la déchirure, l’amincissement et l’adhé-rence des valvules 3. Une réduction du nombre des valves a été observée dans des segments deveines saphènes de patients présentant une insuffisance veineuse chronique 4.
Ces observations n’expliquent pas comment les valves disparaissent ni comment ce remo-delage s’intègre dans l’enchaînement des événements qui aboutissent à la MVC. Cependant,un pas important a été fait lorsque nous 5 avons examiné les valvules des grands veines sa-phènes retirées de patients atteints de MVC. En nous servant d’un anticorps monoclonal spé-cifique pour les monocytes et les macrophages tissulaires, nous avons trouvé une infiltrationdes valves des valvules et de la paroi veineuse par des monocytes et des macrophages dans tousles échantillons de veines provenant de patients atteints de MVC, alors qu’aucune n’a été retrou-vée dans les échantillons des témoins avec des veines normales. L’infiltration était plus impor-tante dans le sinus valvulaire et la paroi veineuse proximale que dans le côté distal de la valvede la valvule et la paroi veineuse distale (Figure 1A). Cette découverte nous a fait envisagerl’existence d’un lien avec une pression veineuse élevée. D’autres recherches ont fait apparaîtrel’inflammation et le remodelage ultérieur des valvules veineuses et de la paroi veineuse commeles mécanismes fondamentaux sous-jacents à l’atteinte et aux lésions valvulaires observéespar angioscopie6.
Mécanismes moléculairesDes forces hémodynamiques, telles que des chan-gements de la pression sanguine dans la paroi et lacontrainte de cisaillement, ainsi que des plans chan-geants d’écoulement laminaire et turbulent, indui-sent l’activation des leucocytes et des cellules endo-théliales. Les intégrines semblent agir comme desintermédiaires et l’expression de molécules d’adhé-sion a été observée. Une dégradation de la matriceextracellulaire de la média et de l’adventice au tra-vers de l’activation des métalloprotéases matricielles(MMPs) a été observée. En particulier, les expressionsdes MMP-1, MMP-2, MMP-9 et des inhibiteurs tissu-laires des métalloprotéinases (TIMP) ont été étudiée.Les télangiectasies, les veines réticulaires et les vé-ritables varices semblent être une conséquence deschangements induits par l’hypertension veineuse et
par la contrainte de cisaillement (Figure 1B). Comme indiqué ci-dessus, l’observation angiosco-pique des valvules des veines saphènes lors de l’éveinage des veines a fait apparaître les sévèresdéformations décrites. Le modèle animal de l’hypertension veineuse induite sur lequel nous avonstravaillé démontre des changements précoces dans les valvules veineuses qui reproduisent ceuxobservés chez les humains.
Cette observation lie l’hypertension veineuse et la réaction inflammatoire induite qui sti-mule l’atteinte valvulaire. Par conséquent, le modèle s’est révélé utile pour définir les méca-nismes fondamentaux à l’origine de l’insuffisance valvulaire veineuse et des varices. À l’avenir,il pourrait se révéler utile lors des essais pharmacologiques pour identifier les agents suscep-tibles d’être efficaces dans la prévention ou le traitement de l’insuffisance veineuse.
Insuffisance veineuse primaireLe dysfonctionnement du système veineux est principalement provoqué par l’insuffisance fonc-tionnelle des valvules veineuses. Les mécanismes moléculaires, récemment découverts, qui en-trent dans l’insuffisance valvulaire fonctionnelle sont mentionnés ci-dessus. Les autres facteurstraditionnellement cités comme contribuant à l’insuffisance valvulaire veineuse incluent le sexeféminin, la grossesse, l’obésité, un métier pratiqué en position debout chez les femmes7 et l’hé-rédité8,9. Une augmentation du diamètre de la veine représente une cause de dysfonction et dereflux valvulaires. La progestérone inhibe la contraction des muscles lisses. Elle est utile dansla prévention des contractions utérines et de l’avortement spontané au cours de la grossesse.
É D I T O R I A L
92 Insuffisance valvulaire veineuse et maladie veineuse chronique primaire – BerganMEDICOGRAPHIA, VOL 30, No. 2, 2008
Figure 1. A. Une valvule dusinus veineux normale est
remarquablement bien adaptée à sa fonction, qui
consiste à permettre le transport du sang à proxi-
mité et à arrêter le flux san-guin en direction distale.
Remarquez la paroi veineuseet le sinus valvulaire qu’elle entoure. B. L’hypertension
veineuse est responsable de l’amorce de la réaction inflam-matoire qui se traduit par un
affaiblissement, un allonge-ment et une dilatation de la
paroi veineuse. En outre, cette hypertension déclenche
la réaction inflammatoire à l’origine de l’atteinte valv
laire et de la disparition ultérieure de la valvule.
A B

Toutefois, l’obstacle à la contraction des muscleslisses de la paroi veineuse entraîne une dilatationpassive des veines et, lorsqu’un diamètre critiqueest atteint, une valvule veineuse jusqu’alors fonc-tionnelle présente un dysfonctionnement ou uneinsuffisance. Dans la mesure où la moitié de la vieadulte des femmes est sous l’influence de la pro-gestérone et où celle-ci est fortement exacerbéependant la grossesse, on ne s’étonnera pas quel’insuffisance veineuse primaire soit deux fois plusfréquente chez les femmes que chez les hommes7.
Le reflux valvulaire persistant entraîne uneaugmentation chronique de la pression veineusedistale. Cette pression veineuse augmente à me-sure que l’on passe du pilier du canal inguinal àla cheville, en passant par le genou. L’hyperten-sion veineuse prolongée amorce une cascaded’événements pathologiques. Ces événements semanifestent cliniquement sous forme d’œdèmes,de douleurs, de démangeaisons, de décolorationcutanée et d’ulcération des membres inférieurs.10
Les premiers signes de l’insuffisance veineuse sont souvent l’apparition de varices dans l’épi-derme et le derme, ces dernières étant appelées télangiectasies (Figure 2). Un peu plus profon-dément, on trouve les veines bleu-vert plates du système (réseau) réticulaire. Ces veines sont éga-lement susceptibles de devenir variqueuses. Enfin, encore plus profond, on trouve les variceselles-mêmes. Toutes ces veines et veinules anormales ont un point commun : elles sont allon-gées, sinueuses et présentent un dysfonctionnement des valvules veineuses.
Les manifestations des télangiectasies, les varicosités réticulaires et les varices sont regrou-pées sous le même terme d’insuffisance veineuse primaire.
Insuffisance veineuse chroniqueLes changements cutanés liés à l’hyperpigmentation, les cicatrices dues à une ulcération an-térieure et les ulcérations actives sont regroupés sous le même terme d’insuffisance veineusechronique (IVC). De nombreuses théories ont été avancées sur la cause de l’insuffisance veineusechronique et des ulcères veineux10,11.
Certaines des théories proposées au siècle dernier ont fait preuve d’une remarquable pres-cience. À titre d’exemple, la théorie de la stase veineuse, publiée pour la première fois dans unmanuscrit de John Homans, de Harvard, en 1917 12. Il s’agissait d’un traité portant sur le dia-gnostic et la prise en charge de patients présentant une insuffisance veineuse chronique, danslequel le Dr Homans a inventé le terme de « syndrome post-phlébitique » pour décrire leschangements cutanés de l’IVC. Il affirmait alors que « L’étirement excessif des parois veineuseset la destruction des valvules… interfèrent avec la nutrition de la peau… par conséquent, lapeau soumise à un bain sous pression avec du sang veineux stagnant forme des plaies ouvertespermanentes ou des ulcères ». Le fait d’avoir attiré l’attention sur la destruction des valvulesétait remarquable. Cependant, cette affirmation, comme de nombreuses autres qui décriventles pathologies veineuses et leurs traitements, relève du dogme et, à l’exception de la descrip-tion de l’atteinte des valvules, manque de faits d’observation. En fait, il est peu probable queHomans ait observé les atteintes valvulaires telles que nous les connaissons dans l’insuffisanceveineuse primaire. Il est possible qu’il ait vu les ravages de la destruction valvulaire phlébi-tique avec adhérence des valves l’une sur l’autre et sur la paroi veineuse. Le terme d’ulcère destase fait honneur à cette idée fausse, tout comme les termes de maladie de stase veineuse et dedermite de stase.
Alfred Blalock, qui, plus tard, a développé la chirurgie péricardiaque, a contesté la théoriedu sang stagnant en étudiant la teneur en oxygène des varices et des veines normales 13. Il anotamment fait remarquer que la teneur en oxygène de la veine fémorale des patients présen-tant une insuffisance veineuse chronique sévère était supérieure à la teneur en oxygène dumembre opposé non atteint. La teneur en oxygène étant plus élevée, certains investigateurs ontpensé que les fistules artérioveineuses pouvaient être à l’origine de la stase veineuse et des va-rices. Cette théorie, bien que réfutée, n’est pas dénuée de fondement, dans la mesure où l’inté-
É D I T O R I A L
93Insuffisance valvulaire veineuse et maladie veineuse chronique primaire – Bergan MEDICOGRAPHIA, VOL 30, No. 2, 2008
Figure 2. Ce schéma, dessiné par George Somjen de Victoria(Australie), montre les relations étroites entre les télangiectasies,les veines réticulaires, les veines collatérales variqueuses et lesveines perforantes directes et indirectes. Remarquez commentl’hypertension veineuse de n’importe quel segment touche lessegments en rapport.
Veine perforante
Veineperforante
Veine collatéralevariqueuse
Veine réticulaire
Veine profonde
Télangiectasie
Derme
Aponévrosesuperficielle
Aponévroseprofonde

gralité de l’appareil thermorégulateur des membres dépend de l’ouverture et de la fermeturede shunts artérioveineux (Figure 3). Ces shunts sont importants, dans la mesure où ils expli-quent certains accidents terribles qui se produisent pendant les injections sclérosantes lorsquele produit sclérosant qui pénètre dans une veine est dérivé dans le système artériel et distribuédans sa ramification normale14. Des études sur microsphères n’ont pas permis de mettre enévidence une telle dérivation et la théorie des communications artérioveineuses a été aban-
donnée bien que ces shunts existent réellement etqu’ils s’ouvrent et se ferment sous l’influence de l’hy-pertension veineuse et de la température ambiante.
L’hypoxie et le rôle qu’elle joue dans la causalitéde l’insuffisance veineuse chronique ont été étudiéspendant les 25 dernières années du XXe siècle. Deschercheurs anglais ont pensé qu’un manchon de fi-brine, observé histologiquement, bloquait le trans-port de l’oxygène et était responsable des change-ments cutanés de l’IVC aux chevilles et à distance10.Cette théorie a été abandonnée.
Toutes les manifestations de l’IVC sévère desmembres inférieurs sont provoquées par l’interactionde deux éléments. Ces éléments sont l’insuffisancedes valvules veineuses, le principal coupable, et plustard, les changements cutanés entraînés par l’hyper-pigmentation, l’atrophie blanche et l’ulcération cu-tanée des chevilles. Tous deux sont liés à l’hyperten-sion veineuse. Notre travail nous autorise à penserque l’hypertension veineuse cause une contraintede cisaillement dépendante de l’interaction leuco-cytes - cellules endothéliales, qui comporte toutes les
manifestations d’une inflammation chronique15. Ces manifestations sont le roulement des leu-cocytes, une solide adhérence à l’endothélium et la migration ultérieure des cellules à traversla barrière endothéliale jusqu’au parenchyme des parois des valvules et des veines16. Là, les ma-crophages élaborent les métalloprotéases matricielles, qui détruisent l’élastine et peut-êtreégalement le collagène. Les parois veineuses subissent un étirement et un allongement. Les val-vules du sinus veineux présentent des perforations, des déchirures et même des cicatrices si im-portantes que les valvules disparaissent quasi-totalement. Ces changements s’observent auxniveaux macroscopique et angioscopique 15 et ont été produits de façon expérimentale par laconstitution d’une fistule artérioveineuse.
La seconde manifestation de l’insuffisance veineuse chronique s’exprime dans la peau. Là,les leucocytes sont également responsables des changements observés. Des biopsies cutanées ontmontré qu’il y avait une prédominance de macrophages et de lymphocytes dans une peau lipo-sclérosée et eczémateuse 17. Une infiltration de leucocytes dans l’espace extracellulaire a étéétablie en observant la localisation de ces leucocytes autour des veinules capillaires et post-ca-pillaires. Les leucocytes sont accompagnés d’un dépôt de collagène désorganisé. À l’évidence,l’insuffisance veineuse chronique de la peau et de ses tissus sous-cutanés est une pathologie in-flammatoire chronique qui, rappelons-le, dépend de l’hypertension veineuse. Elle se traduit parun épanchement de macromolécules et de globules rouges dans l’interstitium dermique. Lesproduits de dégradation des globules rouges et les épanchements des protéines interstitielles sontde puissants chimioattractifs et représentent le signal inflammatoire chronique initial respon-sable du recrutement des leucocytes18. Comme indiqué, ceux-ci font suite à une insuffisance val-vulaire, coupable initiale de l’insuffisance veineuse primaire et secondaire.
ConclusionsLes processus d’atteinte des parois des valvules et des veines, ainsi que les changements cutanésavancés de l’IVC, sont la conséquence de réactions inflammatoires stériles. L’insuffisance valvu-laire est déclenchée par une hypertension veineuse et, à son tour, provoque une hypertensionveineuse à distance. Par conséquent, les traitements futurs devront s’orienter vers la préventiond’une telle hypertension veineuse, en empêchant l’insuffisance valvulaire. �
É D I T O R I A L
94 Insuffisance valvulaire veineuse et maladie veineuse chronique primaire – BerganMEDICOGRAPHIA, VOL 30, No. 2, 2008
Figure 3. Ce schéma illustre les relations étroites entre les arté-rioles, les capillaires, les veinules, les veines et les nerfs adjacents.Le shunt A-V est facile à imaginer, tout comme l’est l’effet desvaricosités veineuses dilatées sur les nerfs adjacents.
Capillaire
Lymphatique
Nerf
Artériole
Sphincterprécapillaire
Shunt A-V thermorégulateur
Veinule

The challenge to this concept came centuries lat-er, when direct observation of valve movements andin vivo measurement of blood flow velocity revealedsome intriguing phenomena. In 1926, E. B. Carrierdescribed an intricate blood flow pattern aroundthe venous valve leaflets, by direct observation of redblood cell movement in the wing of the bat.3 Thiswas exactly the same pattern as predicted by Leo-nardo da Vinci, and confirmed by K. D. Kele for ageometrically similar aortic valve.4 While the roleof this flow phenomenon in the functioning of theaortic valve was understood, in the case of the ve-nous valve, it was simply ignored. Carrier’s observa-tions that venous valve leaflets do not open all theway out to touch the sinus wall were confirmed byin vitro experimentation with human saphenousvalves.5 These findings demonstrated the complex-ity of the hemodynamics around the valve that farexceeded the simple sequence of forward and back-ward flow, and challenged the simplicity of the thencurrent concept of the physics behind the closingof the venous valve.
Development of modern diagnostic ultrasoundtechniques opened up the opportunity to detectvalvular incompetence in patients with chronic ve-nous diseases.6 At the time of the original work inthis area, ultrasound equipment did not allow re-liable visualization of the valve itself. Instead, Dop-pler-based registration of reverse blood flow in thevenous segment in response to Valsalva or rapidcompression-decompression maneuvers was usedto define valvular insufficiency. This approach ad-vanced venous diagnosis by providing a reliable toolfor reflux detection that is used to this day. Unfor-tunately, the indirect approach also created con-fusion between the presence of reverse flow in thevein and the function of the valve itself. The terms“reflux time” and “valve closure time” were incor-rectly used interchangeably. As a consequence, theview that reverse flow through the valve is neces-sary for valve closure was promulgated.7
Increasing awareness of chronic venous diseaseas a growing public health problem in an agingpopulation has uncovered significant gaps in our
understanding of the physiology and pathophysiol-ogy of the venous system. Among the many featuresdistinguishing the venous system from other vas-culature, is the unique and most intriguing delicatestructure of the venous valve.
The apparent simplicity of this apparatus leavesvery little room for speculation regarding its func-tion. Long before Harvey, the venous valve wasviewed as a passive membrane that opened andclosed the vessel’s lumen.1 An elegant and convinc-ing demonstration of unidirectional venous flow,first formulated in Excercitarto Anatomicae deMotu Cordis et Sangunis in Animalibus, was an es-sential part of the modern understanding of thecardiovascular system.2
95The functioning of venous valves in normal and pathological conditions – Lurie MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
B ased on recent observations, a new concept of the mechanism of venousvalve closure and the role of valves in the circulation has been proposed.In healthy individuals, valve geometry and pulsatile venous flow deter-
mine the mechanical forces that act on the valve’s cusps, causing their move-ments. Under physiological conditions, the venous valve creates a complex lo-cal flow pattern that facilitates forward movement of blood, increases the supplyof oxygenated blood to valve pockets, and causes the cyclic closure of the valveitself, securing the pulsatile nature of venous flow. In rare circumstances ofreverse flow, valves close, securing unidirectional flow. Dysfunction of thevalve can lead to disruption of a normal flow pattern. This changes the oxy-genation of valve pockets, potentially leading to thrombi formation, or causesasymmetrical jets of reverse flow through an incompetent valve, producing shearstress–mediated pro-inflammatory and pro-thrombotic endothelial transfor-mations.Medicographia. 2008;30:95-99. (see French abstract on page 99)
Keywords: venous valve function; physiology; reverse flow; pathology
Fedor LURIE, MD, PhDJohn A. Burns School of Medicine University of Hawaii Hawaii, USA
Address for correspondence: Prof Fedor Lurie, Clinical Professor of Surgery, John A. Burns School of Medicine, University of Hawaii, Hawaii, USA(e-mail: [email protected])
The functioning of venous valves in normal
and pathological conditions b y F. L u r i e , U S A

cept of unidirectional flow in veins, in addition tothe alternative interpretations of Doppler-based flowmeasurements were never seriously studied.
The engineering of artificial valves revived theinterest in the study of the mechanism of valveclosure. Experimental and computational modelsshowed that the geometry of the valve plays an im-portant role in its function. The depth of valve pock-ets, for example, determines the valve competency:deeper sinuses provide better reaction to reverseflow. At the same time, deep sinuses increase thechances of blood stagnation.12 A compromise is hardto reach when artificial valves are designed, but thevariety of configurations in natural valves demon-strates that not all of them are optimized to reactto reverse flow. Interestingly, the depth of the valvepockets has little effect on antegrade flow.
� Valve closure by antegrade flow: the valve cycleBy observing valves in femoral and great saphe-nous veins of healthy volunteers, we identified aconsistent pattern of flow events as the blood passesthrough a valve station during rhythmic openingand closing of the valve cusps. The flow and themovements of the valve appear to be two parts of thesame physiologic process of the “valve cycle”— thetime period between two consecutive closures ofthe valve, which we arbitrarily divided into fourphases (Figure 1).13
� Opening phaseDuring the opening phase, the cusps move fromthe closed position toward the sinus wall. This phaselasts on average for 0.3 seconds when the patient isin the horizontal position.� Equilibrium phaseAfter reaching a certain point in this phase, thevalves cease opening and enter the equilibriumphase. During this phase, the leading edges remainsuspended in the flowing stream and undergo oscil-lations that resemble the flutter of flags in the wind.The valve is maximally open during this phase. Stillcusps maintain their position at some distance fromthe wall, creating a funnel-like narrowing of the lu-men. The cross-sectional area between the leafletsis about two thirds of the cross-sectional area of thevein distal to the valve. The flow accelerates in thisstenotic area, forming a proximally-directed jet.Upon impact of the jet against a layer of much slow-er-moving blood proximal to the valve, reflection offlow occurs in the mural parts of the stream. Whilethe larger stream located in the center of the vesselis directed proximally along the axis of the vein, thesmaller part of the flow turns into the sinus pocketbehind the valve cusp. This part of the stream formsa vortex along the sinus wall and the mural side ofthe valve cusp before re-emerging into the mainstream in the vein.
As vortical flow persists, it applies pressure uponthe mural surface of the valve cusps. When the pres-sure on the mural side of the cusp and the pressureon the luminal side of the cusp are in equilibrium,the valve remains open and the cusps float in thestream. This dynamic equilibrium is sustained by anequilibrium in the velocities of the two streams—
A new generation of ultrasound equipment, par-ticularly the introduction of B-flow modality, hasmade it possible to observe venous valves and bloodflow in the area of the valve in undisturbed physi-ologic conditions. Artificial maneuvers to force theblood backward to check the competency of thevalve are no longer needed for normal valve obser-vations. One can simultaneously observe the mo-tions of valve leaflets, changes in venous sinus shapeand size, and blood flow through the valve duringa normal respiratory cycle, in different positions ofthe body and during exercises such as dorsal andplantar flexion of the foot.
Function of the normal valve
� Valve closure by reverse flowThe ability of the venous valve to close in reactionto reverse flow or a distally directed pressure gra-dient has been used for the diagnosis of venous in-sufficiency ever since Brodie and Trendelenburg de-veloped their simple and useful clinical test.8,9 20scentury plethysmographic techniques involvedchanging the patient’s position from horizontal tovertical to measure the refill time as an indicator
of valvular competency. A more physiologic methodof emptying the calf veins using exercise was addedlater. These techniques were not convenient for ul-trasound-based investigations, however, and werereplaced by the Valsalva maneuver, compression ofthe extremity proximal to the segment of interest,or compression of the extremity distally, followedby rapid decompression.10
Widespread use of ultrasound-based diagnosticsexposed the existence of retrograde flow in clini-cally healthy extremities under test conditions. Toresolve this issue, cut-off values were proposed todifferentiate pathologic reflux from physiologicallynormal reverse flow.11 Surprisingly, very little at-tention had been paid to such an interesting phe-nomenon as the existence of reverse flow in veins.The exception is a single report postulating thatunless a certain “critical” velocity of reverse flow isreached, the valve remains open.7 Both the apparentdisagreement between these findings and the con-
96 The functioning of venous valves in normal and pathological conditions – LurieMEDICOGRAPHIA, VOL 30, No. 2, 2008
Figure 1.The four phasesof the valve cycle.
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
Closed phase Equilibrium phase
Opening phase
Closing phase
Valve cycle

� Valve functions other than prevention of refluxThe blood flow in peripheral veins is much morecomplex than that in arteries and capillaries. At anygiven time, it can be continuous, pulsatile, or ab-sent. The transitions from one state to another pro-duce even more complex fluid dynamic phenom-ena. The presence of valves complicates this evenfurther, as valves are not only moved by the flow,but participate in flow changes. In this sense, wecan postulate that the venous valve has physiologicfunctions other than securing unidirectional flow,broadly characterized as flow modulation. Respon-sibility for the central role in providing this func-tion belongs to the geometry of the valve and to thedistinct mechanical properties of leaflets, walls ofthe sinus, and walls of adjoining segments.
During the opening and equilibrium phases ofthe valve cycle, a proximally-directed jet forms inthe valve orifice. The shape of this orifice with fusedleaflets on both sides and gradual widening towardthe center significantly differs from a circular cross-section of adjoining venous segments. As bloodpasses through the valve orifice, its velocity profileflattens. This makes possible the formation of or-ganized flow patterns, for example spiral flow in thegreat saphenous vein where valves are positioned ata small angle to one another, thus rotating the flowas it passes proximally. This is more likely to happenin segments with several closely located valves, suchas crural veins. The existence of such organized flowpatterns may conserve a significant amount of en-ergy, facilitating venous return. As of now, this re-mains a theoretical construct awaiting experimen-tal confirmation.
The flow inside the valve pocket deserves specialattention. It is essential for keeping valve leafletsaway from the venous wall, and for closing the valve.It also provides “flushing” of the valve pocket dur-ing each valve cycle. Experiments have shown thatwhen this flushing does not happen regularly, theoxygen content of the blood inside the valve pock-ets drops. This occurs during a period of continuousflow. With pulsatile flow, the flushing happens reg-ularly, and the oxygen content in valve pockets isnot different from the rest of the venous blood.14
Avascularity of the valve leaflets predisposes themto ischemic damage, thus, prolonged time periodsof continuous flow followed by reperfusion of valvepockets may play an important role in the forma-tion of venous thrombi.15 This is one of the likelyexplanations for the established fact that valve pock-ets are often the site of initial thrombus develop-
vortex on the mural side, and axial flow on the lu-minal side of the valve cusps. Changes in either ofthese streams can lead to the closure of the valve.Self-excited oscillations of the leading edges of theleaflets that occur during this equilibrium phasemake this balance unstable and very sensitive tosmall changes in flow.� Closing phase and closed phaseWhen the venous flow rate increases distal to thevalve, as occurs during foot movements, the veloc-ity of the flow between the valve cusps rapidly in-creases. This causes a fall in the pressure on the lu-minal side of the cusp, and the cusps start movingtoward the axis of the vessel, further constrictingthe lumen (Figure 2). With rising pressures on themural side and falling pressures on the luminal sideof the cusps, valve closure is favored. The closingphase ensues. The leaflets move synchronously to-ward the center. The cusps of the valve assume asymmetrical position at an equal distance from thewalls on both sides of the sinus. This phase lasts 0.4seconds when the subject is at rest, and is shorterwhen foot movements are performed. The last phaseis the closed phase, during which, the cusps remainclosed.
The duration of the valve cycle and each of its fourphases depends upon the position of the body. In thestanding position, we found that the duration of thecycle was from 2.9 seconds to 3.2 seconds (95% con-fidence interval [CI]), which corresponds to a fre-quency of 18.8 to 20.4 cycles per minute (similar torespiration frequency). In a horizontal position, theduration of the cycle was from 1.7 seconds to 1.8seconds (95% CI). This rhythm (34.2 to 36.1 cyclesper minute) is most likely influenced by both res-piratory and cardiac cycles. Muscle activity (dorsaland plantar flexions of the foot) causes shorteningof the closing phase. As we observed, every singlefoot movement causes a significant increase in ve-locity and closure of the valve.
Based on our observations, we proposed a newconcept of the mechanism of venous valve closureand the role of the valve in circulation. In the ab-sence of forced reverse flow, the valve cusps con-sistently undergo the four phases constituting thevalve cycle. The local hemodynamic events, such asvortical flow in the sinus pocket, play importantroles in the valve operation. These hemodynamicevents are predetermined by the shape and me-chanical properties of the sinus and the valve cusps,and they constitute a self-sustained mechanism forcompetent valve operation.
Figure 2. Forces acting on thevalve leaflets. Axial flow (Vaxial)produces pressure directed towardthe sinus wall (P0), while vortexflow inside the pocket (Vvortex)generates pressure directed insidethe lumen (Pi). An increase in Vaxialcauses a decrease in P0, while Piremains unchanged. The resultingpressure gradient moves the leaflettoward the axis of the vein, closingthe valve.
97The functioning of venous valves in normal and pathological conditions – Lurie MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
Vvortex
Vaxial
Po
Pi

retrograde jet cause changes in the distal venoussegment. The biological plausibility of this hypoth-esis was recently demonstrated experimentally. Ithas been shown that disturbed flow, and especiallyflow in the reverse direction or oscillatory flow, hasa pro-inflammatory action via its promotion of aninflammatory endothelial phenotype. By contrast,unidirectional flow—either continuous or pul-satile—produces shear stress that is transduced byendothelial cells, and thus has an anti-inflammato-ry action.20
The role of inflammation in the development ofpathological changes in the venous wall and valvehas been known for a long time. Saphire demon-strated inflammation and leukocyte infiltration inthe venous valve, even suggesting the term “valvuli-tis” to describe these changes.21 A similar process atthe microcirculatory level demonstrated a relation-ship between abnormal flow and the developmentof skin changes in chronic venous disease.22 How-ever, the exact mechanisms of flow-mediated in-flammation in veins remain unclear. Recent exper-imental work utilizing an animal model of increasedvenous flow rate and pressure provided promisingdirection in the discovery of such mechanisms. Itdemonstrated that shear stress–mediated changesin the venous wall and valves in such a model areremarkably similar to those in humans with chron-ic venous disease.23
It is now becoming evident that the role of valvesin venous circulation exceeds that of a simple reac-tion to reverse flow. The valve’s geometry and themechanical properties of its components determinea series of hemodynamic events in, and possiblybeyond, the valve’s vicinity. In disease, valvularincompetence not only leads to recirculation andinefficiency of the muscular pump, but promotesinflammatory changes in the venous wall and pro-gression of the disease. �
ment.16 By closing in reaction to increasing flowvelocity, venous valves interrupt continuous flowconverting it into pulsatile flow, which secures ad-equate oxygenation of valve pockets and preventsformation of thrombi.
The abnormal valve
The predominant concept of venous valve physiolo-gy holds that the venous valve reacts to reverse flowby closing, ensuring unidirectional flow in veins.Not surprisingly, the role of the venous valve in thedevelopment of chronic venous disease is viewed asa simple failure to close, leading to recirculation,venous hypertension, or both. Ceaseless discussionof whether changes in the venous wall lead to valvu-lar incompetence or whether valves undergo inde-pendent pathological changes, rarely, if ever, con-centrates on the third possible scenario—namely,that valvular incompetence causes changes in thevenous wall. This is despite existing evidence thatin superficial veins, varices and dilations are locat-ed distally to valves, and not proximally, as one wouldexpect if the hydrostatic pressure induced prima-ry changes.17 Dilation of deep veins is much lesscommon, but the severity of changes in the valvesis similar.18,19
Observation of incompetent valves with B-flowultrasound convinced us that with the exception ofadvanced valvular degeneration, the reflux is asym-metrical. Retrograde flow through incompetentvalves occurs as a jet directed toward the venouswall. One of the two cusps remains in the normalposition, while the other cusp prolapses, directingreflux along the lumenal surface of the “normal”cusp (Figure 3).
This is strikingly similar to the flow pattern invenous dilations (Figure 4), allowing the hypothe-sis that valvular incompetence and the resulting
98 The functioning of venous valves in normal and pathological conditions – LurieMEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
REFERENCES1. Scultetus AH, Villavicencio JL, Rich NM. Facts and fictionsurrounding the discovery of the venous valves. J Vasc Surg.2001;33:435-441.2. Harvey W. Exercitato Anatomica de Motu Cordis et Sanguinisin Animalibus. In: The Keynes English Translation of 1928.Birmingham, England: Leslie B. Adams, Jr (publisher); 1978.3. Carrier EB. Observation of living cells in the bat’s wing. In:Physiological Papers Dedicated to Prof August Krogh. London,England: WM Heinemann Ltd; 1926. Cited by: Franklin KJ. TheValves in Veins. A Monograph on Veins. Springfield, Ill: Charles C.
Thomas; 1937:72.4. Kele KD. Leonardo da Vinci on Moment of the Heart andBlood. London, England: Harvey and Blythe Ltd; 1952. Cited by:Bellhouse BJ, Bellhouse FH. Mechanism of closure of the aorticvalve. Nature. 1968;217:86-87.5. McCaughan JJ, Walsh DB, Edgcomb LP, Garrett HE. In vitroobservations of greater saphenous vein valves during pulsatileand nonpulsatile flow and following lysis. J Vasc Surg. 1984;1:356-361.6. Van Bemmelen PS, Bedford G, Beach K, Strandness DE. Quan-
Figure 3. B-flow image
of reflux jetdirected towardthe venous wall.
Figure 4. B-flow image of reflux jet ina saphenousaneurysm.

99The functioning of venous valves in normal and pathological conditions – Lurie MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
titative segmental evaluation of venous valvular reflux with du-plex ultrasound scanning. J Vasc Surg. 1989;10:425-431.7. Van Bemmelen PS, Beach K, Bedford G, Strandness DE Jr.The mechanism of venous valve closure. Its relationship to thevelocity of reverse flow. Arch Surg. 1990;125:617-619.8. Brodie B. Lectures Illustrative of Various Subjects in Pathol-ogy and Surgery. London, England: Longman; 1846.9. Trendelenburg F. Über die Unterbindung der Vena saphenamagna bei Unterschenkelvaricen. Beiträge zur klinischen Chi-rurgie.1891;7:195-210.10. Samner DS. Diagnosis of deep venous thrombosis. In: Ruther-ford RB, ed. Vascular Surgery. 4th ed. Philadelphia, Pa: WB Saun-ders; 1995:1698-1743.11. Labropoulos N, Tiongson J, Pryor L, et al. Definition of venousreflux in lower-extremity veins. J Vasc Surg. 2003;38:793-798.12. Buescher CD, Nachiappan B, Brumbaugh JM, Hoo KA, JanssenHF. Experimental studies of the effects of abnormal venous valveson fluid flow. Biotechnol Prog. 2005;21:938-945.13. Lurie F, Kistner RL, Eklof B, Kessler D. Mechanism of venousvalve closure and role of the valve in circulation: a new concept.J Vasc Surg. 2003;38:955-961.14. Hamer JD, Malone PC, Silver IA. The PO2 in venous valvepockets: its possible bearing on thrombogenesis. Br J Surg.1981;68:166-170.
15. Malone PC, Agutter PS. The aetiology of deep venous throm-bosis. QJM. 2006;99:581-593.16. Sevitt S. The structure and growth of valve-pocket throm-bi in femoral veins. J Clin Pathol. 1974;27:517-528.17. Porto LC, da Silveira PR, de Carvalho JJ, Panico MD. Con-nective tissue accumulation in the muscle layer in normal andvaricose saphenous veins. Angiology. 1995;46:243-249.18. Perrin M. Reconstructive surgery for deep venous reflux: areport on 144 cases. Cardiovasc Surg. 2000;8:246-255.19. Hoshino S, Satakawa H, Iwaya F, Igari T, Ono T, Takase S.External valvuloplasty under preoperative angioscopic control.Phlebologie. 1993;46:521-529.20. Bergan JJ, Schmid-Schônbein G, Coleridge-Smith P, Nico-laides A, Boisseau M, Eklof B. Chronic venous disease. N Engl JMed. 2006;355:488-498.21. Saphir O, Lev M. Venous valvulitis. AMA Arch Pathol.1952;53:456-469.22. Coleridge Smith PD. Deleterious effects of white cells in thecourse of skin damage in CVI. Int Angiol. 2002;21(suppl 1):26-32.23. Takase S, Pascarella L, Lerond L, Bergan JJ, Schmid-Schon-bein GW. Venous hypertension, inflammation and valve remod-eling. Eur J Vasc Endovasc Surg. 2004;28:484-493.
LE FONCTIONNEMENT DES VALVULESEN CONDITIONS NORMALES ET PATHOLOGIQUES
U n nouveau concept du mécanisme de fermeture des valvules et de leurrôle dans la circulation, fondé sur des observations récentes, a été pro-posé. Chez les personnes en bonne santé, la géométrie valvulaire et le
débit veineux pulsatile déterminent les forces mécaniques qui interviennentsur les valves des valvules, provoquant leurs mouvements. En conditions phy-siologiques, les valvules créent un débit local complexe qui favorise un mouve-ment sanguin vers l’avant, augmente l’apport de sang oxygéné aux cavités val-vulaires et provoque la fermeture cyclique des valvules elles-mêmes, préservantla nature pulsatile du débit veineux. En cas de reflux, les valvules se ferment,garantissant un débit unidirectionnel. Le dysfonctionnement d’une valvulepeut conduire à la perturbation du débit normal. Ceci modifie l’oxygénationdes cavités valvulaires, pouvant conduire à la formation de thrombi, ou pro-voque des jets asymétriques de reflux inverse dans une valvule incontinente,produisant des transformations endothéliales prothrombotiques et pro-inflam-matoires médiées par des contraintes de cisaillement.

100 Embryology and distribution of lower limb venous valves in humans – CaggiatiMEDICOGRAPHIA, VOL 30, No. 2, 2008
meticulously described VV anatomy and topogra-phy in the whole venous system. More importantly,Fabricius described a test to evaluate VV compe-tence (Figure 1) that led his student William Harvey(De Motu Cordis, 1628) to discover the circulationof the blood.2
Embryology of venous valves
Very few studies have investigated the developmentof VVs in the human embryo. According to Kamp-meier and Birch (1926), VVs arise from the mediaof the primordial tube.3 By contrast, Czarniawska-Grzesinska and Bruska stated in 2002 that VVs orig-inate as a “condensation” of the endothelium.4 Dueto the presence of endothelium, elastic laminae,connective tissue, and smooth muscle cells withinthe cusps, VVs actually appear to arise via differen-tiation of the whole intima.
In 1926, Jaeger stated that “a certain pressuregradient along the vein” is necessary for VV devel-opment.5 This is why the development of VVs occursonly after the heart begins to beat and the primor-dial muscles begin to move the limb buds. In hu-mans, VVs arise in the peripheral veins after approx-imately 3 to 4 months of prenatal development.3
Kampmeier and Birch state that the earliest valvesof the lower extremity appear in the deep veins ofthe femoral trigone and popliteal fossa, and in theupper end of the great saphenous vein (GSV).3
Historical background
Venous valves (VVs) were first mentioned in1544 by the Spanish anatomist LudovicusVassaeus in his De Anatomen Corporis Hu-
mani tabulae quator.1 Sylvius Ambianus (1478-1555) is quoted as being the first to describe thepresence of valves in the veins of the lower limbs.The function of VVs was clearly identified in 1559 byAndrea Cesalpino in his De Re Anatomica: “...cer-tain membranes placed at the openings of the ves-sels prevent the blood from returning.” The Ger-man Salomon Alberti published the first drawingsof a VV in 1585. In 1603, Hyeronimus Fabricius abAquapendente (1533-1619) published the first trea-tise on VVs entitled De Venarum Ostiolis. Fabricius
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
V enous valves appear in the embryo after the heart begins to beat and theprimordial muscles begin to move the limb buds. The pressure gradientalong the vein triggers a five-step process of valve development. Prena-
tal and perinatal morphological and numerical rearrangements have been de-scribed, but they have still to be clearly demonstrated. The cusps of the venousvalves consist of thin collagen half moon–shaped folds covered by endothelium,which spring from the wall of the vein very close to each other. The vein wall isthicker at the base of the valve cusps, due to larger quantities of smooth musclecells of the media. With increasing age, the loose areolar collagen stroma of thecusp is gradually replaced by thick and fibrous tissue. Data from different au-thors regarding the distribution of valves in the deep, superficial, and perfo-rating veins of the lower limbs are summarized. Finally, valves located in themicroveins of the skin of the lower limbs are described. Medicographia. 2008;30:100-105. (see French abstract on page 105)
Keywords: embryology; human venous valve; morphology; aging; microvein;varicose disease
Alberto CAGGIATI, MD, PhDDepartment of Anatomy La Sapienza University Rome, ITALY
Address for correspondence: Alberto Caggiati, Department of Anatomy, La Sapienza University, Rome, Italy(e-mail: [email protected])
Embryology and distribution of lower limb venous valves
in humans b y A . C a g g i a t i , I t a l y
SELECTED ABBREVIATIONS
GSV great saphenous vein
MVV microscopic venous valve
PTV preterminal valve
SFJ saphenofemoral junction
VV venous valve

tinuation of the internal elastic lamina. The pari-etalis is lined by a layer of endothelial cells, whichare elongated transversely. The remainder of theparietalis consists of loose connective tissue. At thebase of the cusp, the parietalis contains scatteredsmooth muscle cells extended from the longitudi-nal muscular bundles of the vein intima. The lu-minalis and the parietalis join or fuse at the distalend of the cusp, which is thinner than the rest of thecusp; elastic and connective fibers are thinner heretoo. No blood vessels are found within the cusps.
The vein wall is thicker at the base of the valvecusps, due to an increase in smooth muscle cells ofthe media (Figure 4). Some of these cells run cir-cumferentially in bundles and some run longitu-dinally and seem to split off from the inner portionof the media to extend into the cusp for a variableextension. Above the agger, the muscular tissue ofthe vein wall decreases. Elastic fibers from the in-ternal elastic lamina of the vein extend along thecusp close to the basement membrane of the en-dothelium. In addition, elastic bundles reinforce thebase of the cusps. Due to its thickness and mus-cular content, the valvular agger is credited as pre-venting venous dilation, as firstly stated in 1603 by
According to Kampmeier and Birch, the pressuregradient along the vein triggers a five-step processof valve development (Figure 2):3 (i) thickeningof the endothelium, which forms a pair of ridgesplaced transverse to the axis of the vessel; (ii)growth of the endothelial ridges due to their inva-sion by the underlying mesenchyma, which bulgesout of the valvular anlage; (iii) the evolving valvedirects itself toward the heart; (iv) the valvular cuspswiden into a nodular shape, while the valvular sacgains in capacity; and (v) the venous wall thinsdown considerably in the region of the valvular si-nus, mainly due to thickening of the media.
VVs increase in number during prenatal life. Dif-ferences with regard to their distribution and char-acteristics in different areas of the human body startimmediately after birth. In 1981, Maros pointed outthat “Certain findings suggest a reorganization af-ter birth of the venous valves which are frequentlymet in fetus. The close relation between hemody-namic mechanisms and the blood guiding struc-tures may explain the changes (disappearance orpersistence) of venous valves in some areas afterbirth.”6
Morphology of the venous valves
“The shape of valves is such that they resemblethe nail of the index or other three fingers.”
Hyeronimus Fabricius ab Aquapendente, 1603.
According to Saphir and Lev (1952), the cusps ofthe VV consist of thin collagen half moon–shapedfolds covered by endothelium, which spring fromthe wall of the vein very close to each other.7 Theirfree margins diverge to become attached again atthe opposite section of the vein wall. The space be-tween the attachment of the free margins of thecusps is called the commissure (Figure 3, page 102).The commissure itself is slightly raised because ofa thickening of the vein wall in that area. The cuspsare thicker at their bases, where they join the wallof the vein. This thickened attachment of the cuspframework was named “agger” by Franklin,8 and“limbus” or “tuberculum” by others. It is shaped likea double horseshoe, with the convex sides arrangeddistally, and contains smooth muscle cells. The con-tinuations of the free border of the cusp where itmeets the vein wall are named “cornua.” The valvu-lar sinus (or pocket) is the space between the cuspsand venous wall, which at that level is particularlythin (Figure 4, page 102). According to Franklin,8
the vertical length of the cusps will often be twicethe diameter of the vessel (Figures 3 and 4).
The cusps can be designated into two faces: lu-minalis, that part of the cusp close to the lumen ofthe vein and facing the circulating blood stream,and parietalis, that part of the cusp facing the veinwall of the sinus. The luminalis is lined by one lay-er of endothelial cells, which is elongated alongthe major axis of the vessel. Beneath this layer ofendothelial cells is a small amount of connectivetissue that is especially noticeable in childhood.Immediately beneath the tissue, there are moder-ately thick, slightly wavy elastic lamellae, the con-
Figure 1. Plate 2 of Fabricius’ De venarum ostiolis was modified byWilliam Harvey (insert) to demonstrate the direction of flow intothe veins.
Figure 2. The five steps of venous valve development.Modified from reference 3: Kampmeier OF, Birch LF. The origin and developmentof the venous valves, with particular reference to the saphenous district. Am JAnat. 1927;38:451-499. Copyright © 1927, Wiley-Liss, Inc.
101Embryology and distribution of lower limb venous valves in humans – Caggiati MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E

102 Embryology and distribution of lower limb venous valves in humans – CaggiatiMEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
formance, such as in the veins of the extremitiesand stomach.”3 Many studies have dealt with thenumber and location of VVs in the inferior venacava region.11-18 Data provided by different authorsregarding the distribution of valves in the veins ofthe lower limbs are summarized in the followingparagraphs. Unfortunately, these data are difficult tocompare, mainly due to the different topographicdesignation of the veins.
� Addomino-pelvic regionThe inferior vena cava is without VVs. Sporadicmonocuspid valves have been exceptionally report-ed.8 Occasionally, one sporadic and mostly incom-plete valve, similar to a spur, is reported in thecommon iliac vein (in 1% to 7% of limbs).15,16 OneVV is located in the external iliac vein of about aquarter of white subjects. Friederich noted in 1882that one VV is located in about 35% of external iliacveins, “but often mainly decadent.”17 La Page andcolleagues reported one well-developed VV locatedwithin 2 cm distal to the entrance of the internaliliac vein in 26% of legs.18 The right external iliacvein has almost three times as many valves as theleft (39.6% vs 14.6%). According to Kampmeier andBirch, the internal iliac vein is avalvular, whereasits main tributaries (gluteal, sacral, and obturatorveins) are valvular.3 By contrast, more recently LaPage and colleagues18 stated that in 7.6% of indi-viduals, a well-developed ostial valve is present, andparietal valves are found in only 2.2%. Finally, itstributaries will be valvular in only 10% of cases.
� Deep veinsThe common femoral vein shows one VV abovethe saphenofemoral junction (SFJ), known as the“supra-saphenic valve.” It protects the saphenousaxis against rises in intra-abdominal venous pres-sure.19 According to Basmajan, two VVs are locatedin the same tract in about 5% of normal limbs.11
The femoral vein shows about three valves. Themost constant valve (found in about 90%-100% ofcases, according to Banjo16), is located just belowthe conjunction of the deep femoral vein.16 No dataare available with regard to the lateral and medialcircumflex veins. The deep femoral vein and thedeep femoral perforators are valvular.20 The popli-teal vein displays one to three VVs. Finally, the deep
Hyeronimus Fabricius ab Acquapendente: “Quoquevenarum distensionem fuisse ostiola a Summo Opi-fice fabrefacta” (“The Supreme Artificer made valvesto prevent venous distension”). Moreover, the tis-sue organization of the valve sites suggests that theaction of valves is not merely that of passive flaps,but that they can also actively regulate the flow, es-pecially in conditions of low velocity. According toFegan:9
Contraction of the circular bundles at the base ofthe cusps reduces the diameter of the vein. Con-traction of the longitudinal muscular fibers ofthe cusps reduces their length and increases theirthickness. In addition, the cusps are drawn downtowards their roots, and away from each other,but the sphincteric action of the circular bundlescompensates for this. The upper free parts of thecusps press against the vein wall at the lateralattachments of the valve, and thus, with the in-timal cushions, help to seal the potential leaks.
� Age-related structural changes of venous valvesAge-related morphological changes in VV leafletswere comprehensively described by Saphir and Lev:7
Starting after the age of 30, the loose areolar col-lagen stroma of the cusp is gradually replacedby thick and fibrous tissue. After 40, an increasein elastic tissue starts at the base of the cusp, togradually spar the free margin. In the parietalportion of the leaflet, accumulation of dense-collagenous fibers. In the luminal, deposition ofcollagen between endothelium and elastic mem-brane.
These changes are similar to those described inthe superficial veins of aged individuals.10 Theycan be attributed to the physiologic hemodynamicstress related to standing and muscular contrac-tions. However, changes related to senility do notimply VV dysfunction with significant reflux.
Distribution of venous valves in the lower limbs
Kampmeier and Birch correctly stated that, as ageneral rule, “Valves are present in those vesselswhich are subject to pressure from without andin those in the immediate sphere of muscular per-
Figure 3. The nomenclature of venous valves (Panels A and B), showing the sinus (A), free (B), and attached (C)borders. D indicates the cornua, E indicates the valve cusps, and F indicates the agger. Panel C shows that thelength of the cusps is about twice the diameter of the vessel. Courtesy of Alessandro Pieri.
Figure 4. Scanning elec-tron microscopy demon-strating the difference inwall thickness betweenthe agger and the sinus.
A
Agger
Sinuswall
B C
F A

veins of the leg are richly valvular. According toGottlob and May, 8 to 19 VVs are located in each ofthe posterior tibial veins, and 8 to 11 VVs in boththe anterior tibial and peroneal veins.20
� Superficial veinsCotton calculated that 7.2 ±2.3 valves are locatedalong the entire length of the GSV.21 According toRaivio, between 1 and 7 valves are located along thethigh portion of the GSV (mean number, 3.5), 2 to6 valves are located along the leg (mean number,4), and finally 1 to 4 valves are located at the foot(along the marginal veins).22 The valves of the SFJare of particular clinical relevance. In 1603, Fabri-cius stated that the terminal portion of the GSV hasa bicuspid valve at the orifice, then at two fingers’distance, a further set of twin valves (Figure 5). Thefirst is the well-known terminal valve situated atthe termination of the GSV to prevent reflux fromthe femoral vein. The more distal one is the preter-minal valve (PTV), which lies just below the open-ings of the SFJ tributaries. The PTV prevents venousreflux from the tributaries of the SFJ into the GSVtrunk while the terminal valve is closed. Incompe-tence of the PTV is the reason for reflux into theGSV in cases in which the terminal valve is stillcompetent.19 The terminal valve is present in 98%to 99% of normal legs, whereas the PTV is presentin only about 70% to 85%. Finally, in about 2% oflimbs, no valves are present in the last portion ofthe GSV.23
According to Raivio, the global number of VVsalong the small saphenous vein is an average of8.2.22 The terminal valve is located in all legs witha saphenopopliteal junction. No data are availableon the presence of VVs along the thigh extensionof the small saphenous vein, which shows, in nor-mal conditions, an antegrade flow directed towardthe GSV or toward tributaries of the internal iliacvein (inferior gluteal or ischiatic veins).
� Saphenous accessories and other superficial veinsFabricius affirmed that smaller superficial veins(saphenous tributaries, communicating veins, andreticular veins) are avalvular. By contrast, Bouchetaffirmed that they are valvular at their end, along
Figure 5. The valves of the inguinal area, as depicted by Fabricius in 1603 (Panel A), and in a schematic drawing(Panel B). The confluence of junctional tributaries is between the two last valves of the great saphenous vein.Panel C: incompetence of the preterminal valve explains a varicose great saphenous vein with a normal terminal valve.Abbreviations: ptv, preterminal valve; ssv, supra-safenic valve; tv, terminal valve.
their course, and at the point of entry of a small-er vein.24 Avalvular superficial veins connect mainvalvular superficial veins (oscillating veins).25
� Perforating veinsIt is well known that perforating veins are furnishedwith valves. The number of VVs in perforating veinsranges between 1 and 5 (the mean is 2). In 1978,Pirner affirmed that “all valves were found in thesubfascial part of the perforating veins.”26 In thesame year, Van Limborgh and Hage noted that “thenumber of valves in the epifascial part of the perfo-rators was significantly less in those (perforating)veins which frequently become incompetent.”27
However, Raivio reported that only 75% of theperforating veins are valvular.22 Avalvular perforat-ing veins are found mainly in the foot, hand, andforearm. However, avalvular perforating veins arereported elsewhere in the human body, and worklike oscillating veins connecting deep and super-ficial districts. This was confirmed by duplex in-vestigations that demonstrated bidirectional flowin perforating veins of people without any sign ofvenous disease.28-30
Number of venous valves and varicose desease
While valvular agenesis is a known, but rare causeof venous insufficiency, the relationship betweenthe number of VVs and varicose disease has beenpoorly investigated. Sales and colleagues demon-strated that the mean number of valves in varicosesaphenous veins differed from that of nonvaricoseones (2.3 ±0.83 vs 4.8 ±2.01, respectively).31 Banjocomparatively evaluated the presence of VVs inwhites and black Africans, and demonstrated thatthe number of valves is higher in the latter.16 Thismay account for the high prevalence of varicoseveins (between 10% and 18%) in whites, and the lowprevalence (1% to 2%) of the condition in Africans.
Age-related changes in the number of venous valves
A reduction in the number of VVs as a function ofaging is a debated topic. The theory proposed by
103Embryology and distribution of lower limb venous valves in humans – Caggiati MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
A B C

104 Embryology and distribution of lower limb venous valves in humans – CaggiatiMEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
tenth of their total quantity of VVs; in the superfi-cial veins, the amount is 1.5 to 2 times higher thanin the deep veins.37 These regressive phenomenaare subject to regional differences. According toGottlob and May, “venous systems, in which unidi-rectional flow conditions are prevalent, tend to losetheir ‘superfluous’ valves more readily, whereassystems, in which heavier strain is exerted on thevalves due to hydrostatic stress or reversed flow,preserve their valves throughout life.”20
Valves in microveins
Anatomists, physiologists, and clinicians considerthe venous bed to be “valveless” from the venularlevel up to 2 mm large veins. On the contrary, mi-croscopic venous valves (MVVs) have been describedin the microvascular bed (postcapillary venules andvenulae efferents of arteriovenous anastomoses), incollecting venules, and in small caliber veins (withdiameters up to 800 to 1000 μM).38 MVVs have beenfound in the subcutaneous layer and in musclesof various areas of the human body (Table I).
Generally, MVVs are described as bicuspid. MVVsare arranged in series along a vein or are situatedat the merging point of two veins. The valves al-ways point in the direction of the larger vessel, asin the collecting veins. Two layers of endothelialcells surround a core of basement membrane ma-terial, in which bundles of collagen fibrils are em-bedded.
MVVs are identical in structure, location, and ori-entation to the VVs of the leg macroscopic veins.This has led to the hypothesis that their role is toresist blood reflux in small sized veins and collect-ing venulae, and to prevent reflux from postcapil-lary venulae to the capillary bed and arteriovenousanastomosis.38 This hypothesis is corroborated bytwo pieces of evidence: (i) the absence of MVVs inregions with a favorable venous return; and (ii) theabundance of MVVs in regions subject to gravita-tional backflow and where blood flow is irregularor altered by muscular contraction, as with VVs.The absence of MVVs, as well as their incompetence,could explain clinical syndromes characterized bysigns and symptoms of chronic venous insufficien-cy in limbs with competent VVs in large veins.38 �
Bardeleben in 188032 and reconsidered by Powelland Linn in 1951,33 which proposed a lifelong andprogressive reduction in the number of VVs dueto involutive noninflammatory phenomena, wasstrongly denied by Leu and colleagues in 1979,34 andhas been definitively abandoned. Leu and colleaguesconfirmed what Klotz demonstrated in 1887; ie, thenumber of VVs does not decrease with age, but thenumber of incompetent VVs increases with age.35
According to Gottlob and May, “venous valvescannot disappear but pathological processes maycause them to become incompetent.”20 This canbe a result of the well-known effects of a massivethrombosis, but also because of subclinical local-ized thrombosis of the valvular sinus, as describedby Sevitt in 1974,36 dilation of the valvular anlage(as in varicose veins), and other regressive phe-nomena currently not well defined.
Senile involution of VVs was investigated in depthby Marinov in 1973.37 He established that in parallelwith aging, the number of fully developed valvesreduces, while that of “partial” valves increases, withthe highest intensity of the process being recordedduring the period between 25 and 60 years of age.37
In subjects older than 60 years, the number of par-tial valves represents between one fifth and one
Author (year discovered) Area of the body
Popoff (1934) Digital skin
Pirro (1950) Calf muscles
Miani and Ruberti (1958) Foot sole skin
Braverman, et al. (1983) Abdominal wall
Curri, et al. (1987) Vastus lateralis, Gastrocnemius
Caggiati, et al. (1987) Vastus lateralis
Miyake, et al. (1996) Human maxillo face
Aharinejad, et al. (1997) Exocrine pancreas
Aharinejad, et al. (1997) Human dorsal thoracic fascia
Aharinejad, et al. (1998) Skin of the scapular area
Aharinejad, et al. (2001) Skin of the inferior limb
Shangkuan, et al. (2001) Tongue
Phillips, et al. (2004) Skin of the inferior limb
Table I. Areas of the human body found to
contain microscopic venous valves.
REFERENCES1. Caggiati A, Bertocchi P. Regarding “fact and fiction surround-ing the discovery of the venous valves.” J Vasc Surg. 2001;33:1317.2. Caggiati A, Rippa Bonati M, Pieri A, Riva A. 1603-2003: fourcenturies of valves. Eur J Vasc Endovasc Surg. 2004;28:439-441.3. Kampmeier OF, Birch LF. The origin and development of thevenous valves, with particular reference to the saphenous district.Am J Anat. 1927;38:451-499.4. Czarniawska-Grzesinska M, Bruska M. The structure of thecusps of valves in the human foetal great saphenous vein. FoliaMorphol (Warsz). 2003;62:275-276.5. Jaeger O. Die entwicklung der veneklappen. Morph Jahrbuch.1926;56:250.6. Maros T. Data regarding the typology and functional signifi-cance of the venous valves. Morphol Embryol.1981;27:195-214.7. Shapir O, Lev M. The venous valve in the aged. Am Heart J.1953;51:843-850.8. Franklin KJ. A Monograph on Veins. Springfield, Ill: CharlesC. Thomas; 1937.9. Fegan WG and Kline L. The course of varicosities in superfi-cial veins of the lower limb. Brit J Surg. 1952;59:798.
10. Macchiarelli G, Nottola SA, Familiari G, Caggiati A. Aging ofthe human long saphenous vein. A light and scanning electronmicroscopy study. Cardiovasc Imaging. 1998;10:83-86.11. Basmaijan JV. The distribution of valves in the femoral, ex-ternal iliac and common iliac veins and their relationship to vari-cose veins. Surg Gynecol Obstet. 1952;95:537-542.12. Ludbrook J. Functional aspects of the veins of the leg. AmHeart J. 1962;64:706-713. 13. Reagan B, Folse R. Lower limb venous dynamics in normalpersons and children of patients with varicose veins. Surg Gy-necol Obstet.1971;132:15-18.14. Staubesand J. Kleiner atlas zur vascularen anatomie der li-estengegend. In: Brunner U, ed. Die Liste. Bern, Switzerland:Huber; 1979:12-23.15. Lodin A, Lindvall N. Congenital absence of valves in the deepveins of the leg. Acta Derm Venereol Suppl (Stockh).1961;41(suppl 45):1-83.16. Banjo AO. Comparative study of the distribution of venousvalves in the lower extremities of black Africans and Caucasians:pathogenetic correlates of prevalence of primary varicose veins inthe two races. Anat Rec.1987;217:407-412.

EMBRYOLOGIE ET RÉPARTITION DES VALVULES VEINEUSESDU MEMBRE INFÉRIEUR CHEZ L’HOMME
E n embryologie, les valvules veineuses apparaissent après les premiersbattements cardiaques et les premiers mouvements des bourgeons desmembres commandés par les principaux muscles. Le gradient de pres-
sion le long de la veine déclenche le développement de la valvule en cinq étapes.Les réarrangements morphologiques et numériques prénataux et périnataux,déjà décrits, demandent à être démontrés. Les valvules veineuses sont consti-tuées de fins replis de collagène, en demi-lune, recouverts d’endothélium, quisurgissent de la paroi veineuse, très proches l’un de l’autre. La paroi veineuseest plus fine à la base des valvules en raison du plus grand nombre de cellulesmusculaires lisses de la média. Avec l’âge, le stroma collagène aréolaire de lavalvule disparaît progressivement au profit d’un tissu épais et fibreux. Sont ré-sumées ici les données de différents auteurs sur la répartition des valvules dansles veines profondes, superficielles et perforantes des membres inférieurs. Enfin,les valvules des microveines cutanées des membres inférieurs sont décrites.
17. Friederick N. Ueber das verhalten der klappen in den crural-venen. Morph Jahrbuch. 1882;7:323-325. 18. La Page PA, Villavicencio JL, Gomez ER, Sheridan MN,Rich NM. The valvular anatomy of the iliac venous system andits clinical implications. J Vasc Surg. 1991;14:678-683.19. Caggiati A, Bergan JJ, Gloviczki P, Eklof B, Allegra C, PartschH. Nomenclature of the veins of the lower limbs: extensions,refinements and clinical application. J Vasc Surg. 2005;41:719-724.20. Gottlob R, May R. Venous Valves. New York, NY: Springer; 1986.21. Cotton LT. Varicose veins: gross anatomy and development.Br J Surg. 1961;48:589-598.22. Raivio E. Untersuchungen uder die venen der unteren ex-tremitaten. Ann Med Exp Fenn. 1948;26(suppl 4):213-216.23. Hesse E, Schaack W. Die Klappenverhaltnisse der Ober-schenkel-vene und der Vena Saphena Magna. Vircow’s Archiv.1911;205:145-154. 24. Bouchet A. Anatomie morphologique des valvules des mem-bres inferieurs. Phlebologie. 1992;45:233-245.25. Taylor GI, Caddy CM, Watterson PA, Crock JC. The venousterritories (venosomes) of the human body: experimental studyand clinical implications. Plast Reconstr Surg.1990;86:185-213.26. Pirner F. On the valves of the perforating veins. In: May R,Partsch H, Staubesand J, eds. Perforating Veins. Munich, Ger-many: Urban & Schwarzenberg; 1979:208-213. 27. Van Limborgh J, Hage RW. Anatomical features of those per-forating veins of the leg which frequently or infrequently becomeincompetent. In. May R, Partsch H, Staubesand J, eds. PerforatingVeins.Munich, Germany: Urban & Schwarzenberg; 1979:49-59.28. Sarin S, Scurr JH, Smith PD. Medial calf perforators in ve-
nous disease: the significance of outward flow. J Vasc Surg.1992;16:40-46.29. Stuart WP, Adam DJ, Allan PL, Ruckley CV, Bradbury AW. Therelationship between the number, competence, and diameter ofmedial calf perforating veins and the clinical status in healthysubjects and patients with lower-limb venous disease. J Vasc Surg.2000;32:138-143.30. van Neer PA, Veraart JC, Neumann HC. Venae perforantes: aclinical review. Dermatol Surg. 2003;9:931-942.31. Sales CM, Rosenthal D, Petrillo KA, et al. The valvular ap-paratus in venous insufficiency: a problem of quantity? Ann VascSurg. 1998;12:153-155.32. Bardeleben K. Das Klappen-Distanz-Gesetz. Jenaische Ztschr.Naturwisse. 1880;12:467-529.33. Powell T, Lynn RB. The valves of the external iliac, femoraland upper third of the popliteal veins. Surg Gynecol Obstet.1951;92:453-455.34. Leu HJ, Vogt M, Pfrundes H. Morphological alterations of non-varicose and varicose veins. Basic Res Cardiol.1979;74:435-443.35. Klotz K. Unteresuchungen uber die Vena Saphena Magnabein Menschen. Arch Anat Physiol Anat Abt.1887;159:174-178.36. Sevitt S. Organization of valve pocket thrombi and the ano-malies of double thrombi and valve cusp involvement. Br J Surg.1974;61:641-649.37. Marinov G. Changes with age in the valvular apparatus of thesuperficial and deep veins of the leg. Eksp Med Morfol.1973;12:86-91.38. Caggiati A, Phillips M, Lametschwandtner A, Allegra C. Valvesin small veins and venules. Eur J Vasc Endovasc Surg. 2006;32:447-452.
105Embryology and distribution of lower limb venous valves in humans – Caggiati MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E

106 Venous valve incompetence and reflux in childhood – SchadeckMEDICOGRAPHIA, VOL 30, No. 2, 2008
This literature review, which includes some ofour own work, sets out to show that chronicvenous insufficiency (CVI) can begin very ear-
ly in childhood and adolescence and that reflux isan excellent indicator of its progression. Althoughhemodynamics is our main concern, we shall alsodiscuss epidemiology and heredity, before advocat-ing the grading of CVI based on hemodynamic andclinical characteristics.
Epidemiology
Venous angiodysplasia and deep vein thrombosisdominate the venous disease literature.1,2 Few evenrecent studies have specifically addressed CVI inchildren and adolescents. Most cohorts range inage from 18 years to over 90 years, as if CVI onlystarts after adolescence.3-8 A few large-scale studieshave included subjects from the ages of 12 or 15years upward, but without drawing any conclusionsspecific to this age group.9,10 However, clinical signssuch as small varices, and even hyperplasia of thegreat saphenous vein (GSV), began to be recognizedas heralding CVI11 when continuous-wave Dopplerentered standard practice.
A key epidemiological study in the young was thatof Heede in 1989, carried out in 8- to 18-year-olds.12
Clinical examination revealed varices or telangiec-tases from the foot to the groin, with 52% in thepopliteal region, confirming results of a 1978 Praguestudy.13 The overall prevalence of varicose veins was14% and appeared to increase with age: 2.3% of theoverall population showed reflux at the sapheno-femoral junction (SFJ) versus 3.2% in the 14- to18-year-old subgroup, consistent with the 1981study by Fischer.14
The prospective Bochum Study15 monitored 740pupils aged 10 to 12 years from 11 secondary schoolsfor 9 years from 1982. It combined clinical exam-ination with photoplethysmography and contin-uous-wave Doppler assessment of reflux. Resultswere identical to those of Heede, with GSV refluxbeing observed in 2.9% of the youngest subjectsin Bochum Study I. Four years later, in BochumStudy II, reflux had risen to 10.4%, with primaryvalve failure being diagnosed in 1% to 2%. The au-thors considered reflux to be the first sign of trun-cal varicosis, while the mainly popliteal reticularvarices were earlier in onset but not directly relat-ed to the reflux observed later. Another 1989 study,in 741 6- to 14-year-olds, found truncal or perfora-tor incompetence in 13.9%, but failed to detail themethods used.16 In 2006, we published a clinical andduplex ultrasound study of 142 young subjects,
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
C hronic venous insufficiency (CVI) is common in children and adoles-cents, often beginning very early. Reflux is a major item in the initialassessment and follow-up. This article proposes an investigation and
management plan. Continuous-wave Doppler ultrasound has been used in asmall number of epidemiological studies to determine the prevalence of greatsaphenous vein reflux in children and adolescents and its progression with age,which has been confirmed using the Clinical-Etiology-Anatomy-Pathophysiol-ogy (CEAP) classification. Duplex scanning, although unable to truly quantifyreflux, has since helped to classify it by type, height, outcome, topography, andthe relationship between subject age and topography. These parameters arecombined with clinical examination to score the severity at presentation andmonitor the disease course. The results show that the frequency of CVI in theyoung depends on the study population and ranges from 3% to 10%, depend-ing on age; it may exceed 50% in those with one or two varicose parents. Re-flux generally begins around the knee and progresses proximally with age. Itmay appear before or after puberty. Despite the substantial advance in charac-terization of CVI and reflux in the young, a consensus has yet to be reached asto treatment indications and modalities.Medicographia. 2008;30:106-111. (see French abstract on page 111)
Keywords: childhood; chronic venous disease; saphenous reflux; varicoseveins; venous valve incompetence
Michel SCHADECK, MD, FACPhPast President of the French Society of Phlebology Paris, FRANCE
Address for correspondence: Michel Schadeck, 5 rue Michel Chasles, F-75012 Paris, France(e-mail: [email protected])
Venous valve incompetence andreflux in childhood b y M . S c h a d e c k , F r a n c e
SELECTED ABBREVIATIONS AND ACRONYMS
CEAP Clinical-Etiology-Anatomy-Pathophysiology (classification)
CVI chronic venous insufficiency
GSV great saphenous vein
IMT intima-media thickness
SFJ saphenofemoral junction

linked inheritance with female predominance, al-though most authors at that time believed that whatwas inherited was a susceptibility syndrome ratherthan CVI itself. However, the epidemiological dataon which inheritance hypotheses were based wereobtained largely by interview, not examination. In1994, a French case-control study provided a clearanswer to the inheritance issue by examining 402subjects from 134 families.19 It included the non-varicose spouses of affected cases in an attempt tocontrol for confounders such as diet and lifestyle.Clinical examination in children and parents wascomplemented in manycases by Doppler ultrasound(although these results were not an inclusion cri-terion). Statistical analysis showed that the risk ofCVI in children, depending on the presence or ab-sence of parental disease, was 20% if neither parentwas affected, 25% in boys and 62% in girls (mean45%) if one parent was affected, and 90% if bothparents were affected. Inheritance is therefore a sig-nificant factor (P<0.001), and an indication for themonitoring of children with a strong family history.
Investigations
Prospective randomized controlled trials are notfeasible in children. We were initially confined tohemodynamic observations that were empirical
with significant GSV reflux (>0.5 seconds) in 92cases, and none in the remaining 50 cases.17 The af-fected population comprised 77 girls (83.7%) and15 boys (16.3%) aged 14±2 (8-18) years. We dividedthe leg into seven segments: reflux was found to ex-tend over more than two segments of the thigh orleg in 16 patients (Group 1), and it was confined toone segment (short reflux) in 76 patients (Group 2).All patients were classified by age and Clinical-Etiology-Anatomy-Pathophysiology (CEAP) score,ranging from asymptomatic C0 (C0a) to symp-tomatic C2 (C2s). Scores differed significantly be-tween the groups, with 0.0% C0a in Group 1 versus58.7% in Group 2 (P<0.0001), and 56.3% C2s inGroup 1 versus 2.7% in Group 2 (P<0.0001) (Fig-ure 1A). Division into three age groups (8-13 yearsold, 14-15 years old, and 16-18 years old) showed acorrelation between age and CVI severity (P<0.01)(Figure 1B), confirmed by the anatomical, clinical,and disability scores (Figure 1C).
Heredity
Heredity has been considered to play a major rolein CVI, with well-established evidence of transmis-sion, although acquired factors have remained para-mount for some authors. In 1937, Troisier andLe Bayon (cited by Merlen et al18) postulated sex-
107Venous valve incompetence and reflux in childhood – Schadeck MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
Figure 1. Relationship between reflux severity and Clinical-Etiology-Anatomy-Pathophysiology (CEAP) classification, age distribution, andother scores in the 92 subjects (77 girls [83.7%] and 15 boys [16.3%] aged 14±2 [8-18] years) with significant great saphenous vein (GSV)reflux (>0.5 seconds) in a population of 142 children/adolescents. Affected subjects were divided into 2 groups: those with reflux extendingover more than two segments of the thigh or leg (Group 1; n=16), and those in whom reflux was confined to one segment (Group 2; n=76).A, CEAP classification and reflux severity, ranging from asymptomatic C0 (C0a) to symptomatic C2 (C2s); B, age and reflux severity; C, otherscores and reflux severity.After reference 17: Schadeck M, Allaert FA. CEAP classification applied to children and teenagers. Phlebologie. 2006;35:A41. Copyright © 2006, Schattauer.
C0a C0s C1a C1s C2a C2s
60%
50%
40%
30%
20%
10%
0%
Group 1Group 2
P<0.05
Disab.0Disab.1
P<0.001
Clin.0Clin.1
Anat.
P<0.01P<0.01
Group 1Group 2
P<0.0001
8-13 14-15 16-18 Years
Affe
cted
sub
ject
s (%
)
Affe
cted
sub
ject
s (%
)
100908070605040302010
0
7.1%
92.9%
56.3%58.7%
A
C
B
2.7%0.0%
12.9%
87.1%
30.3%
69.7%
54.6%45.4%
8-13 14-15 16-18
Clin
ical
sco
re (%
)
Dis
abili
ty s
core
(%)
100908070605040302010
0
92.9%
7.1%
87.1%
12.9%
57.6%
42.4%
8-13 14-15 16-18 years years years
Ana
tom
ical
sco
re
1.81.61.41.21.00.80.60.40.20.0
1.1±0.3
1.5±0.61.7±0.8
8-13 14-15 16-18
100908070605040302010
0
92.9%
7.1%
87.1%
12.9%

108 Venous valve incompetence and reflux in childhood – SchadeckMEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
and detailed instructions for examining venous re-gions of interest. It defines significant pathologicalreflux in the great or small saphenous vein as beingretrograde flow in the anti-physiological directionlasting for more than 0.5 seconds.26 This is the onlyinformation on reflux in the consensus document.However, retrograde reflux does not necessarily im-ply true reflux, still less valve incompetence. It isalso important to know whether the superficial ve-nous reflux is spontaneous or induced, transientor permanent, and where it occurs.27 These are allhemodynamic parameters that we need to consid-er if we are to make as comprehensive an analysisas possible. They are as applicable to young subjectsas to adults.
Reflux
� Spontaneous and induced refluxColor Doppler scanning may reveal spontaneous re-flux when the subject is mobilized. It can be con-firmed and assessed using compression-decom-pression maneuvers. Reflux in young people is oftenfound below the knee along the GSV trajectory.Compression of the muscle compartments drainedby the GSV will demonstrate its actual origin. How-ever, this may require displacing a substantial vol-ume of blood, which should not be repeated tooforcefully in somewhat timid young subjects, forfear of triggering a vasovagal reaction.
� Intervalvular and commissural refluxIntervalvular reflux is associated with incompetentvalve leaflets that are damaged and no longer func-tional. Reflux is always pathological if it lasts morethan 0.5 seconds.
Commissural reflux28,29 through oneorbothspacesbetween the valve leaflets can often be demonstrat-ed in the standing position in the lower third of thethigh. This high-intensity reflux shows as frequencysaturation in pulsed Doppler mode and as a bright-ly colored stream on one or both sides of the valvein color Doppler mode (Figure 3). Endoscopy cancorroborate commissural reflux.30 Although it mim-ics pathological reflux hemodynamically in that itsduration greatly exceeds 0.5 seconds, it remains lo-calized to the valve, with no distal extension, mak-ing it difficult to interpret. It could be that it re-flects no more than slow closure of the commissuralspace, in no way heralding the development of CVI.It is therefore essential to recognize it for what itis and not mistake it for pathology.
� Transient and permanent refluxIt is important to differentiate between transientand permanent reflux in the young, as one is a harm-less sign, while the other marks the onset of irre-versible CVI.
Reversible transient reflux always exceeds 1 sec-ond but is not consistently reproducible. It can oc-cur after prolonged standing, and may be presentone day and absent the next. It fully meets the def-inition of reflux through a healthy valve demon-strated in the GSV terminal segment.31 It reflects nomore than functional dilatation of the perivalvu-
rather than strictly scientific. Clinical examinationwas the cornerstone procedure, as it is now. Overthe years, it has been complemented by three typesof investigation.
� PhotoplethysmographyThis technique failed to improve understanding ofCVI in the young. Even in combination with Dopplerultrasound, it could not differentiate between nor-mal results and various forms of incipient CVI.20 Theconsensus is that muscle immaturity in the youngmakes it impossible to use the data collected.14,20-22
� UltrasoundUltrasound soon replaced radiology as the standardstructural investigation.23 It maps the anatomy ofthe diseased superficial venous system and identi-fies the defective valves. It provides an initial score,which can be supplemented by vessel diameter val-ues. Intima-media thickness (IMT) provides a mea-sure of the vein wall changes induced by the disease,and is significantly increased in affected young sub-jects compared with normal adults.24
� Doppler ultrasoundEver since its introduction, Doppler ultrasound hasbeen the essential hemodynamic investigation forconfirming the diagnosis of CVI. From 1985 to 1990,it was used in continuous-wave mode,25 but accord-ing to no standard technique or specific recom-mendations (Figure 2). The patient’s position dur-ing the examination and the maneuvers employedwere not clearly specified. Only the Valsalva maneu-ver was regularly mentioned. This explains why pa-tients were generally examined for reflux at the SFJor saphenopopliteal junction. The duration of sig-nificant reflux was not considered an importantparameter. Nevertheless, it was the hemodynamicstudies using continuous-wave Doppler that yield-ed the epidemiological results cited above.
Today, not only do we have color duplex scanning,we also have a consensus document, Duplex ultra-sound investigation of the veins in chronic venousdisease of the lower limbs,23 which lays down clear
Figure 2. Continuous-wave Doppler recording made in 1988 of reflux atthe saphenofemoral junction in an 11-year-old girl showing a saphenousvein diameter of 6 mm.

all, in detecting CVI as early as possible. We havealso included height as an indication for ultra-sound-guided sclerotherapy when reflux reaches orexceeds two limb segments.33
� Age and reflux topographyLongitudinal monitoring is difficult in practice, butwe have monitored pathological reflux in severalyoung patients at yearly intervals. The reflux under-went progressively proximal ascent to the SFJ,29,34,38
confirmed statistically by the correlation betweensubject age and ascending reflux topography. Chil-dren with reflux in the terminal GSV segment wereolder than those with reflux either side of the knee(14.4 years versus 13.2 years). The mean age of ourgeneral population, including normal and patho-logical subjects, was 13.7 years; this compared with14.4 years for those with reflux, and 16.2 years forthose with reflux involving two limb segments.These results are consistent with those showing acorrelation between SFJ reflux and higher age inadults.39 Puberty, which was long assumed to be animportant determinant of reflux, has an inconclu-sive role: in 156 adolescent girls, 77 had significantreflux, of whom 53.3% were prepubertal and 59.5%postpubertal.16
Management
Based on the epidemiological and genetic data, andthe current structural and hemodynamic studiesof early-onset CVI, we propose the following man-agement guidelines:� Mandatory screening for all girls with one CVI-positive parent and all children with two affectedparents.19
� Diagnostic structural and hemodynamic stud-ies to confirm reflux and determine its topography,height, origin, and score severity in conjunctionwith the CEAP classification as a basis for a rationalmanagement strategy.38
� Follow-up at 6 or 12 months to confirm initialfindings and check for progression.� Curative treatment for adolescents with docu-mented GSV incompetence,33,40,41 in the absence ofother consensus as to treatment indications andmodalities. Ultrasound-guided sclerotherapy wassuccessful in 15 out of 16 of our patients with refluxexceeding two limb segments; the remaining pa-tient required surgery.17 This approach remains rel-
lar wall ring with no valve lesion. Such reflux isreadily identified using continuous-wave Doppler,but is more difficult in pulsed Doppler mode.
Permanent and irreversible reflux reflects a struc-tural valve lesion, and is therefore present at everyexamination.
� Reflux topographySuperficial venous reflux arises fromvarious sources,including the saphenous veins, accessory saphenousveins, perforators, pelvic veins, and nonsaphenousveins.27,32 In children, it can also originate from col-lateral branches mainly below the knee.29
Reflux often begins at the knee or anywherealong the course of the GSV and its branches. In aprospective clinical and Doppler study in 81 5- to18-year-olds (89% girls) with a positive family his-tory, we identified the site of reflux by compres-sion-decompression of the thigh or calf.29 Reflux wassignificant in 38% of cases, and was distributedalong the entire GSV. In 55.5% of cases, it occurredon either side of the knee, where it was slow andconfined to a single intervalvular interval. The verylow incidence of SFJ reflux (5.7%) would seem toeliminate femoral reflux as a cause of saphenousreflux. A fuller study 6 years later in 161 subjectsamply confirmed these results, with reflux aroundthe knee in 75.3% of cases, and proximal reflux upto the SFJ in the remainder.33
Detailed hemodynamic analysis at the SFJ is rel-atively recent.34-36 There have been no specific stud-ies of terminal and/or subterminal valve lesions inyoung patients, although we have observed sever-al cases of terminal valve incompetence. Saphenousreflux in youths may also be associated with a varic-ocele.37
� Height of refluxBy dividing the limb into seven segments, threeabove and three below the knee, and one for theankle and below, reflux height can be used to com-pare two successive investigations and plot the dis-ease course.33 Height reflects severity. An ultra-sound study used height to define three types ofreflux in young subjects:38 type 0, no reflux; type 1,reflux limited to one limb segment; type 2, refluxstretching over more than one segment. The au-thors combined these data with other anatomicalor structural parameters into a composite diseasescore that can be used in monitoring and, above
109Venous valve incompetence and reflux in childhood – Schadeck MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
Figure 3. Color Dopplerrecording of commissuralreflux in the saphenoustrunk.

110 Venous valve incompetence and reflux in childhood – SchadeckMEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
CVI cannot be scored on the basis of reflux alone,but only as a composite, in combination with thestructural data, CEAP classification, and geneticfactors.
Although no consensus exists as to treatment in-dications or modalities, we consider that GSV abla-tion can be offered from age 14 upward, given thedata established by the few published studies, name-ly: the evidence in the young of ineluctable CVIprogression with age,14,16,17,20 the body weight andheight of affected adolescents (which generally ex-ceed those of adult controls),24 and their sometimesgrossly dilated GSV diameters (5-10 mm). Althoughthese indications require further discussion, sincefew patients have been treated to date, even inten-sive monitoring should not delay curative treat-ment that may alone be able to prevent diseaseprogression.
Conclusion
Doppler ultrasound has transformed our under-standing of CVI in children and adolescents in re-cent years, although the topic remains generallyunderstudied. Analysis of valve incompetence inthe GSV has revealed a number of useful parame-ters for diagnosing and monitoring early reflux,itself a key parameter in the diagnosis and gradingof CVI. This can then be combined with the CEAPclassification and the structural and genetic data toproduce a composite severity score giving an accu-rate prognosis. This approach is a precondition forreaching a consensus on treatment indications andmodalities. �
atively rare but is increasing. When we reported ourongoing study of 4311 cases treated by ultrasound-guided sclerotherapy, only 0.7% were under 24years of age, with adolescents accounting for 0.2%.42
Today, however, children and adolescents make up0.5% of my patients treated by echosclerosis, whosenumber now exceeds 5000.
Discussion
The epidemiological data, reinforced by studies ap-plying the CEAP classification, show that CVI canbegin in early childhood and that it progresses withage. Clinical evidence from before the ultrasoundera12,14 indicated that varicose disease did not orig-inate at the SFJ, but tended to be distributed in thepopliteal region, where reticular varices were pre-dictive of CVI. Doppler ultrasound then confirmedthe marked predominance (75%) of GSV reflux ei-ther side of the knee on presentation in children.Reflux that has reached the SFJ is evidence of al-ready advanced disease and is characteristic of olderchildren and adolescents.
Commissural reflux needs to be differentiatedfrom pathological reflux, since follow-up in manyof our young patients shows that it disappears after1 to 2 years. Height is a marker of reflux severityand a useful monitoring tool. Pathological refluxmay occur from earliest childhood onward, withno direct relationship to puberty.
This confirms Heede’s 1989 study showing noevidence for significant hormonal influence.11 How-ever, puberty may be an aggravating factor in incip-ient or established pathological reflux. In any event,
REFERENCES1. Rabe E. Venous insufficiency in childhood. Phlebology.1987;2:249-256.2. Brightwell RE, Brightwell A, Davies AH. Venous disease inchildhood. Phlebology. 2007;22:145-147.3. Cesarone MR, Belcaro G, Nicolaides AN, et al. ‘Real’ epidemi-ology of varicose veins and chronic venous diseases: the SanValentino Vascular Screening Project. Angiology. 2002;53:119-130.4. Ruckley CV, Evans CJ, Allan PL, Fowkes FG. Chronic venousinsufficiency: clinical and duplex correlations. The EdinburghVein Study of venous disorders in the general population. J VascSurg. 2002;36:520-525.5. Carpentier P, Cornu-Thénard A, Uhl J, Partsch H, Antignani P.Appraisal of the information content of the C classes of CEAP clin-ical classification of chronic venous disorders: a multicenter eval-uation of 872 patients. J Vasc Surg. 2003;37:827-833.6. Rabe E, Pannier-Fischer F, Bromen K, et al. Bonner Venen-studie der Deuteschen Gesellschaft für Phlebologie: epidemiol-ogische untersuchung zur frage der häufigkeit und ausprägungvon chronischen venenkrankheiten in der städtischen und länd-lichen wohnbevölkerung. [Bonn Vein Study by the German Soci-ety of Phlebology: epidemiological study to investigate the preva-lence and severity of chronic venous disorders in the urban andrural residential populations]. Phlebologie. 2003;32:1-14.7. Chiesa R, Marone EM, Limoni C, Volonte M, Schaefer E,Petrini O. Chronic venous insufficiency in Italy: the 24-cities co-hort study. Eur J Vasc Endovasc Surg. 2005;30:422-429.8. Schoevaerdts JC, Staelens I. Programme for detecting chron-ic venous insufficiency in Belgium. Phlebology.2007;22:171-176.9. Cooper DG, Hillman-Cooper CS, Barker SG, Hollingsworth SJ.Primary varicose veins: the sapheno-femoral junction, distribu-tion of varicosities and pattern of incompetence. Eur J Vasc En-dovasc Surg. 2003;25:53-59.10. Lacroix P, Aboyans V, Preux PM, Houles MB, Laskar M. Epi-demiology of venous insufficiency in an occupational population.Int Angiol. 2003;22:172-176.11. Griton P, Schadeck M. L’hyperplasie des saphènes et les pre-miers signes de maladie variqueuse chez l’enfant. [Hyperplasia of
the saphenous vein and the initial signs of varicose disease inchildren]. Phlébologie. 1990;43:561-571.12. Heede G. Prevaricose epidemiological symptoms in 8 to 18-aged pupils. In: Davy A, Stemmer R, eds. Phlébologie.Montrouge,France: John Libbey Eurotext Ltd; 1989:157-159.13. Horakova-Nedvikova M, Hlouskova Z. Makromorphologis-che veränderungen der oberflächlichen beinvenen im kindalter[Macromorphological changes of superficial leg veins in child-hood]. In: Sefeld K, ed. Ergebnisse der Angiologie [AngiologyResults]. Stuttgart, Germany-New York, NY: F.K. Schattauer;1978:19-23.14. Fischer H, ed. Venenleiden—Eine Repräsentative Unter-suchung in der Bevölkerung der Bundesrepublik Deutschland(Tübinger Studie) [Venous Disease—A Representative Study inthe Population of the Federal Republic of Germany (TübingenStudy)]. Munich, Germany-Vienna, Austria-Baltimore, Md: Urban& Schwarzenberg; 1981.15. Schultz-Ehrenburg U, Weindorf N, Von Uslar D, Hirche H.Prospektive epidemiologische studie über die entstehungsweiseder krampfadern bei kindern und jungendlichen (BochumerStudie I und II) [Prospective epidemiological study on varicosevein development in children and adolescents (Bochum Study Iand II)]. Phlebol Proktol. 1989;8:3-11.16. Horakova M. Social and medical importance of varices in chil-dren and adolescents. In: Davy A, Stemmer R, eds. UIP ‘89.Mont-rouge, France: John Libbey Eurotext; 1989:193.17. Schadeck M, Allaert FA. CEAP classification applied to chil-dren and teenagers. Phlebologie. 2006;35:A41.18. Merlen JF, Coget J, Larere J. L’hérédité des varices [Heredityof varices]. Phlébologie. 1967;20:213-216.19. Cornu-Thénard A, Boivin P, Baud JM, et al. Importance of thefamilial factor in varicose disease. Clinical study of 134 families.J Dermatol Surg Oncol. 1994;20:318-326.20. Weindorf N, Schultz-Ehrenburg U. Le développement de lavaricose chez les enfants et les adolescents [The development ofvaricose veins in children and adolescents]. Phlébologie.1990;43:573-577.21. Stücker M, Reich S, Robak-Pawelczyk B, et al. Changes in

111Venous valve incompetence and reflux in childhood – Schadeck MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
L’INCONTINENCE VALVULAIRE VEINEUSEET LE REFLUX CHEZ L’ENFANT
L a maladie veineuse chronique de l’enfant et de l’adolescent (MVC) est unepathologie qui commence très tôt, et le reflux représente un élément ma-jeur dans l’évaluation initiale et sa surveillance. Dans cet article, nous
proposons une méthodologie d’examen et une conduite à tenir. Comme le mon-trent de rares études épidémiologiques, le Doppler continu permet d’évaluer lepourcentage de jeunes présentant un reflux au niveau des grandes saphènes etde montrer que cette pathologie progresse avec l’âge. La classification CEAP(Clinique; Étiologique; Anatomique; Physiopathologique) confirme cette évo-lution. Malgré l’absence d’une véritable quantification du reflux, l’écho-Dopplerpeut définir son type, sa nature, sa topographie, son évolution, son« âge ». As-sociés à l’examen morphologique, ces différents paramètres permettent d’éta-blir un score initial de sévérité et d’observer ainsi l’évolution de la MVC. Il ap-paraît ainsi que la fréquence de cette pathologie chez le jeune dépend de lapopulation étudiée et varie de 3 à 10% en fonction de l’âge du patient. Chez lesjeunes dont un ou deux parents sont variqueux, cette fréquence peut dépasser50%. Le reflux débute généralement au niveau du genou. Sa progression est enrapport avec l’âge, tout en sachant qu’il peut apparaître avant la puberté. Autotal, la MVC débute très tôt chez le jeune et évolue avec l’âge. L’analyse dureflux associée à l’étude morphologique permet d’établir un score de sévéritéde la pathologie. Toutefois, il n’existe à ce jour aucun consensus sur l’attitudethérapeutique.
34. Vin F, Lemasle P, Lefèbrve-Vilardebo M, Uhl JF. Niveau de re-flux de la grande veine saphène : indications thérapeutiques [Lev-el of incompetence in the great saphenous vein: therapeutic con-sequences]. Phlébologie. 2004;57:255-259.35. Capelli M, Molino Lova R, Ermini S, Giangrandi F, Gian-nelli F, Zamboni P. Hemodynamics of the saphenofemoral com-plex: an operational diagnosis of proximal femoral valve function.Int Angiol. 2006;25:356-360.36. Pieri A, Vannuzzi A, Moretti R, Gatti R, Caillard P, Vin F. As-pects échographiques de la jonction saphéno-fémorale et de lajonction saphéno-poplitée. Valvule et rapports avec les collatéralesaccessoires [Color duplex investigation of saphenofemoral andsaphenopopliteal junctions. Venous valves and collateral veins].Phlébologie. 2002;55:317-328.37. Karadeniz-Bilgili MY, Basar H, Simsir I, Unal B, Batislam E.Assessment of saphenofemoral junction continence in patientswith primary adolescent varicocoele. Pediatr Radiol. 2003;33:603-606.38. Ricci S, Casoni P. Étude ultrasonique du système veineux su-perficiel des membres inférieurs en période pré-pubértaire. Re-cherche de possibles critères de prévision de la maladie vari-queuse [Ultrasound study of the superficial venous system of thelower limbs in the prepubertal period to identify possible pre-dictors of varicose disease]. Phlébologie. 2007;60:335-343.39. Pittaluga P, Chastanet S, Rea B, Barber R, Guex JJ, Locret T.Corrélation entre l’âge, les signes et symptômes de l’insuffisanceveineuse superficielle et les résultats de l’exploration écho-doppler[Duplex ultrasonography scanning for superficial venous insuf-ficiency: Correlation of mapping with age, symptoms and signs].Phlébologie. 2006;59:149-156.40. Schadeck M. Indications: sclérothérapie chez l’enfant et l’ado-lescent [Indications: sclerotherapy in children and adolescents].In: Gobin JP, Benigni JP, eds. Sclérothérapie et Maladie VeineuseChronique Superficielle [Sclerotherapy and Superficial ChronicVenous Insufficiency]. Eska Ed; 2007:161-165.41. Schadeck M, Allaert FA. Prise en charge de la MVCS chez l’en-fant et l’adolescente [Management of superficial chronic venousinsufficiency in children and adolescents]. In : Abstracts of theFrench Phlebology Society meeting. Venous Pathology in Gyne-cology and Obstetrics; June 3, 2006; Lyon, France; Abstract P19.42. Schadeck M. Evolution de la pathologie veineuse chez lafemme depuis 1985 [Evolution of venous disease in women since1985]. Phlébologie. 2007;60:149-154.
venous refilling time from childhood to adulthood in subjectswith apparently normal veins. J Vasc Surg. 2005;41:296-302.22. Rabe E, Trumm A. La photopléthysmographie chez l’adoles-cent. Réalisation active et passive [Photoplethysmography in theadolescent]. Phlébologie. 1998;51:135-138.23. Coleridge-Smith P, Labropoulos N, Partsch H, Myers K,Nicolaides A, Cavezzi A. Duplex ultrasound investigation of theveins in chronic venous disease of the lower limbs—UIP Consen-sus Document Part I: Basic principles. Phlebology. 2006;21:158-167.24. Schadeck M, Massonneau M, Caillard P. Etude comparative del’épaisseur intima-média de la grande saphène entre un grouped’enfants et d’adolescents et un groupe d’adultes [Comparativestudy of intima-media thickness of the long saphenous vein in agroup of children and adolescents and a group of adults]. Phlé-bologie. 1998;51:191-196.25. Schadeck M. Doppler and echotomography in sclerosis of thesaphenous veins. Phlebology. 1987;2:221-240.26. Van Bemmelen PS, Bedford G, Beach K, Strandness DE.Quantitative segmental evaluation of venous valvular reflux withultrasound scanning. J Vasc Surg. 1989;10:425-431.27. Guias B, Schadeck M, Bressolette L. Reflux veineux superfi-ciel et explorations ultrasonores. Revue de la littérature [Super-ficial venous reflux and ultrasound investigations. A review ofthe literature]. Phlébologie. 1998;51:147-154.28. Schadeck M. Hemodynamic aspects. In: Duplex and Phle-bology. Naples, Italy: Gnocchi; 1994:53-55.29. Schadeck M. Etude par le duplex des grandes saphènes de l’en-fant: calibres, reflux et conséquences thérapeutiques [Duplexscanning study of great saphenous veins in children: diameter,reflux and influence on therapy]. Phlébologie.1996;49:413-418.30. Van Cleef JF, Hugentobler JP, Desvaux P, Griton P, Cloarec M.Etude endoscopique des reflux valvulaires saphèniens [Endoscop-ic study of reflux of the saphenous valve]. J Mal Vasc.1992;17:113-116.31. Schadeck M. Le reflux sur valvules saines en grande saphène[Reflux in healthy valves of the great saphenous vein]. Phlé-bologie. 1991;44:603-613.32. Labropoulos N, Tiongson J, Pryor L, et al. Nonsaphenous su-perficial vein reflux. J Vasc Surg. 2001;34:872-877.33. Schadeck M. Indications de la sclérothérapie chez l’enfant etl’adolescent [Indications of sclerotherapy in children and teen-agers]. Phlébologie. 2002;55:33-39.

112 Study of the saphenofemoral junction to understand reflux distribution in CVD – Tessari and Cappelli MEDICOGRAPHIA, VOL 30, No. 2, 2008
In the first years of the 21st century, several newtechniques for varicose vein treatment have alsobeen developed, both in the surgical field (hemo-dynamic conservative surgery according to theConservative Hemodynamic treatment of Incompe-tent Varicose veins in Ambulatory patients [CHIVA]strategy) and in the sclerotherapy area. The latterhas recently been gaining great success, thanks toechographic techniques and the use of foam.
At present, the most commonly used techniquesfor treatment of the saphenous varices are those in-volving endovascular obliteration (laser, radiofre-quency, and sclerosant foam with either a long orshort catheter). These techniques have in commonthe inability to completely occlude the saphenousjunction properly, and they therefore expose the pa-tient to a risk of possible relapse, traditional scle-rotherapy with liquid being a notable example. Thisis what happens whenever the surgical disconnec-tion of the saphenofemoral junction is not per-formed completely flush on the femoral vein. Theremaining stump can be the cause of a possible evo-lution of the varicose disease. On the other hand, itmust be pointed out that many surgical proceduresinvolving the saphenofemoral junction do not showany evolution signs, even if they have not been cor-rectly performed.
These differences can be explained by the fact thatendovascular procedures as well as surgery are fre-quently performed without any preventive hemo-dynamic analysis, so the same therapeutic plan is
Some of the techniques currently in use for thetreatment of the varices of the lower extrem-ities were introduced at the beginning of the
20th century: the Narath technique in 1904 (mul-tiple stab incisions phlebectomy), the Keller tech-nique in 1905 (invaginated stripping on thread),the Mayo technique in 1906 (external stripping),and the Babcock technique in 1907 (internal strip-ping).1
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
B efore any decision can be made regarding the appropriate therapeutictechnique for a varicose patient, it is necessary to define how a specificarea (for instance, the saphenofemoral complex) should be assessed in
the patient. We are going to consider two different aspects: first, how to studyan incontinent segment, and second, how to study the saphenofemoral com-plex (on the basis of the general criteria described for an incontinent segment).Valvular continence must be studied in the orthostatic position so as to devel-op a transvalvular retrograde gradient (opposite to the orientation of valvularplanes). Retrograde gradients are studied in two different ways: (i) a high pres-sure test, such as the Valsalva test; and (ii) a gravitational test, which exploitsthe weight of the hematic column once it has been mobilized. Analysis of 1294patients with incontinent great saphenous vein crosses (saphenofemoral com-plexes) revealed complete incontinence of the saphenofemoral junction in only55% of cases. In 6% of cases, a dissociation pattern was noted. Using the samecriteria, the proximal femoral valve (ie, the valve in the common femoral veinlocated above the saphenofemoral junction) was also studied. This turned outto be continent in the saphenofemoral junction and in the saphenous vein archin 58.4% of complete incontinence cases. In cases of continence of the upperfemoral valve, the saphenous trunks (measured at the mid thigh area) mostlyexhibit a diameter that is less than 7 mm.Medicographia. 2008;30:112-115. (see French abstract on page 115)
Keywords: assessment; saphenofemoral complex; reflux; valvular continence;Valsalva maneuver; gravitational test
Address for correspondence: Lorenzo Tessari, Localité Broglie 8 F, 37019 Peschiera du Garda (VR), Italy(e-mail: [email protected])
The study of the sapheno-femoral junction to understand the distribution of refluxes in
chronic venous disease b y L . Te s s a r i a n d M . C a p p e l l i , I t a l y
SELECTED ABBREVIATIONS AND ACRONYMS
CHIVA Conservative Hemodynamic treatment of Incompetent Varicose veins in Am-bulatory patients (French acronym)
C/R (test) compression release (test)
Lorenzo TESSARI, MD Fondazione Glauco BassiTrieste, ITALY
Massimo CAPPELLI, MDStudio FlebologicoFlorence, ITALY

soon as the maneuver is completed. This shows thatthe hypertensive charge (ie, the blocking of antero-grade physiologic flux)hasbeen properly performed.
It is essential to highlight here that transcom-partmental reflux assessment can only be performedif at the moment of application of a retrograde gra-dient, a re-entry system toward a compartment withlower pressure is present (which could be the deepvenous system too), and the lower pressure in the“recipient” system is possible thanks to the closureof its valvular planes (dynamic subdivision of thepressure column).
The above statement can be tested in every pa-tient. Closure through digital compression of thereflux re-entry, eg, the saphenous trunk, bringsabout the disappearance of the reflux in many tests,mostly the gravitational ones.2
� Gravitational gradientIt must be underlined that dynamic tests, throughthe activation of muscle-joint pumps, will mobilizemuch more blood at a deeper level than the C/Rtest, particularly in big dimension calves. We willtherefore have a larger subdivision of the deep hy-drostatic column through the closure of the valvu-lar planes, with a consequent decrease in pressure,and consequently there will be the development ofa much higher re-entry gradient (in the case of in-continence of the superficial net) than the one de-veloped in the C/R test. Hence, in order to detectreflux, the dynamic tests will be much more effec-tive than the C/R test.3
Gravitational tests will point out valvular inconti-nence in a zone distal to the position of the Dopplersample. They will not give any information on thefunctioning of the proximal valvular plane. Thusone must position the Doppler sample on the prox-imal side of the valve that is to be studied (eg, onthe femoral side if we are going to analyze the func-tioning of the terminal saphenous valve).4
We can therefore state that the gravitational testspoint out valvular incontinence in general, while apositive Valsalva test shows how this incontinenceis mostly associated with points of reflux, which arein fact the incontinent compartment passages. Fur-thermore, it should be remembered that the incon-tinence of the venous axes is not always associat-ed with points of reflux, in which case there will benegative Valsalva refluxes. As a consequence of thesefindings, it is argued that the multiple tests we cur-rently use aimed at the elicitation of the reflux can-not be used indifferently in order to establish a di-agnosis of valvular incontinence. Some valves showeither commissural or complete incontinence dur-ing the Valsalva maneuver, but they turn out to becontinent if exposed to a transvalvular gradient ofthe gravitational type.
The observation of this different valvular behav-ior during the execution of different tests can indi-cate a partial incontinence of valvular planes. Thesevalves may as a result be continent to normal grav-itational gradients caused by movement, while they“leak” under the high-pressure gradients developedwith the Valsalva maneuver. These valves are thusnot completely incontinent, and they have a high
applied in different hemodynamic conditions, re-sulting in different long-term outcomes. The oftenanimated discussion regarding how to determinethe best therapeutic technique has resulted in a se-ries of publications about personalized technolog-ical approaches.
Unfortunately, these studies have often not beensupported by accurate color-duplex ultrasound re-search of valvular functions and reflux dynamics,which could have otherwise helped to plan a moreconservative and personalized therapeutic strate-gy. A personalized therapy should be based on anaccurate color-duplex ultrasound analysis of the pa-tient’s varicose situation; this assessment leads toa morphological and, in particular, hemodynamicmap, which represents the basic element for defin-ing the therapeutic plan.
Before any decision can be made regarding theappropriate therapeutic technique to use, it is nec-essary to define how a specific area (eg, the saphe-nofemoral complex) should be studied in a varicosepatient. We are going to consider two different as-pects: (i) how to study an incontinent segment; and(ii) how to study the saphenofemoral complex ac-cording to the general criteria listed in point (i).
Study of an incontinent segment
Valvular continence must be studied with the sub-ject in the orthostatic position, to develop a trans-valvular retrograde gradient (opposite to the orien-tation of valvular planes). Retrograde gradients areof two different types; either that with a high pres-sure test, such as the Valsalva test, or that with agravitational test, which exploits the weight of thehematic column once it has been mobilized. Themobilization of the column may occur in a staticway through the compression/release (C/R) test(static test) or in a dynamic manner through acti-vation of the muscular pump using any of the fol-lowing: (i) Parana test; (ii) Oscillation test; (iii) Lift-ing on Tiptoes test; and (iv) Toes Dorsiflexion test.
� High pressure gradient (Valsalva maneuver)The high pressure charge developed during the Val-salva maneuver is transmitted in a distal way inde-pendent of the continence of the proximal valvularplanes. This is possible thanks to the closure iner-tia of valvular planes themselves, which permits thepassage of the pressure wave. Its propagation speedis definitively superior to the speed of the hematicflux, as is clearly shown in the arterial system. Wecan see that the Valsalva test always determines dis-tal transmission of the pressure wave. When valvu-lar incontinence among different compartments ispresent (eg, between the deep and the superficialnets), the pressure wave is associated with the ap-pearance of transcompartmental reflux. The pas-sages among compartments (between the deep andsuperficial nets and between the saphenous systemand its secondary ramifications), which are inconti-nent with theValsalva test, are called pointsof reflux.
The evaluation of the correct execution of theValsalva test is shown by the appearance of an an-terograde flux, that is, the restarting of the flux as
113Study of the saphenofemoral junction to understand reflux distribution in CVD – Tessari and Cappelli MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E

114 Study of the saphenofemoral junction to understand reflux distribution in CVD – Tessari and Cappelli MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
� The extension of the incontinence, ie, whetherthe reflux is limited to the preterminal, terminal orfemoral valve. The study of either the continence orthe incontinence/absence of the proximal femoralvalve is performed by positioning the Doppler sam-ple under the inguinal ligament. The probe mustbe directed from the groin upward in order to bein a proximal position with respect to the femoralvalve and for subsequent application of a combina-tion of the two maneuvers: the Valsalva and dynam-ic tests.9 The incontinence extension will conditiondifferent pressure columns, with a consequent dif-ference in the reflux hydrodynamic energy; indeedpressure is one of the energy components, togeth-er with the retrograde volume (energy = pressure�volume). The hydrodynamic energy, together withparietal factors, determines the vessel diameter. Infact there is a correlation between the incontinenceextension and the saphenous vein diameter.9
� The level at which the upper arch tributariesdrain toward the saphenofemoral junction. Thislevel has been defined as the “geometrical dischargeheight of the upper arch tributaries.” The discon-nection of tributaries at a high geometrical heightcould cause the formation of a collateral circle thatis vicarious because of the obstruction (iatrogenic-surgical), and this could be the source of retrogradeflow either after crossectomy or after stripping-crossectomy. In such cases, the reflux is not asso-ciated with points of reflux, as is often shown inmaps referring to patients operated on with exces-sively ablative methods. In fact, in these tributaries,the pressure components are represented not onlyby the residual venular pressure, but also by a highhydrostatic column. By contrast, the hydrostaticcolumn is very low in the tributaries that are locat-ed at low geometrical height. The evolution of thesecollateral circles can cause cavernomas (“neovascu-larization”), which represent the re-entry of the re-lapse itself. These are negative Valsalva cavernomas.In subsequent years, these areas can become refluxpoints from the common femoral vein, and they cantherefore become Valsalva positive reflux points.Valsalva positive reflux points can also be those cav-ernomas that originate from tributary disconnec-tion from a pelvic shunt.
As a consequence of the aforementioned specu-lations and findings, it could be argued that thestudy of inflow level of the tributaries may condi-tion the choice between tie/no tie of these archtributaries and, in the case of their conservation, itwill be of importance to decide where to let themdrain—either in the common femoral vein or inthe saphenous vein.
In an analysis of 1294 patients with incontinentgreat saphenous vein crosses (saphenofemoral com-plexes), complete incontinence of the saphenofe-moral junction was noticed in only 55% of cases.9
In 6% of cases, a dissociation pattern (see above)was noted. Using the same criteria, the proximalfemoral valve (ie, the valve in the common femoralvein located above the saphenofemoral junction)was also studied. In 58.4% of complete incontinencecases, it was found to be continent in the sapheno-femoral junction and the saphenous vein arch. In
probability of recovery with reduction of the diam-eter of the venous axis through targeted surgicalinterventions on saphenous collaterals.5
Study of the saphenofemoral complex
It must be pointed out that the saphenofemoraljunction is just a part of the so-called “sapheno-femoral complex.” The hemodynamics of this re-gion are both physiologically and pathologically in-fluenced by other structures. By saphenofemoralcomplex we mean:� The saphenous arch (saphenofemoral cross withits two valves—the terminal valve and the preter-minal valve, differently positioned). The sapheno-femoral junction is part of the cross. It representsthe passage between the great saphenous vein andthe common femoral vein.� The femoral valve proximal to (above) the saphe-nofemoral junction. This valve may not be presentin 20% to 24% of patients.6,7
� The femoral valve distal to (under) the sapheno-femoral junction.� The upper tributaries of the saphenous arch,which in a variable way drain the superficial bloodfrom the lower half of the abdomen. In fact, phys-iologically, a descending flow toward the arch canbe observed. The physiological direction of flux isstated by the orientation of valvular planes.8
The hemodynamic study of the saphenofemoralcomplex consists in the positioning of the Dopplersample above and below the valve to be studied andin the application of all the aforementioned inves-tigative methods. All these tests should point outvalvular incontinence in the various parts of thecomplex. In this way, the hemodynamics of the re-gion can be exactly described. The purpose of thesetests is to determine a targeted therapeutic ap-proach, which may help to avoid either incompleteor useless radical surgery, which can in fact acceler-ate the evolution of the varicose disease, common-ly called “relapse.” The study of the hemodynamicsof the saphenofemoral complex must determine:� The presence of points of reflux represented notonly by the incontinence of the saphenofemoraljunction but also by the connection that somepelvic points of reflux have with the great saphe-nous vein through the arch tributaries. In such cas-es, we will find arch tributaries that show a Valsalvapositive reflux. The exact position of pelvic shuntsmust also be pointed out on the map of the leg.� The incontinence/continence state of the ter-minal valve—that is, the valve situated in the areaof the saphenofemoral junction. This can vary; wemay have: (i) complete continence both in the Val-salva and dynamic tests performed with the Dopplersample positioned on the femoral side of the valve.In this case, both tests will be negative; (ii) com-plete incontinence, when both tests are positive; or(iii) dissociated findings with a leaking terminalvalve under a high pressure charge, but a resistingterminal valve when gravitational gradients are ap-plied. In this case, we have a positive Valsalva testand a negative gravitational test, particularly whena dynamic test is applied.

preferred (chosen?). Last, 45% of the genericallytermed “cross incontinence” in the great saphe-nous vein is in reality associated with continenceof the terminal saphenous valve. In these cases, thetherapeutic gold standard is treatment of pelvic re-flux and/or suppression of incontinent peripheraltributaries (first time CHIVA 2), and surgical treat-ment of the cross would not be recommended. En-dovenous ablative treatments could be indicated incases where the terminal valve of the great saphe-nous vein is continent, although we would like tohighlight the ethical problem regarding the pos-sible demolition of these saphenous veins, whichhave a diameter that is normally less than 6 mm.Hence, either disconnection or sclerotherapy pro-cedures on the incontinent tributaries can be per-formed, without any treatment of the saphenoustrunk.10 �
most cases of continence of the upper femoral valve,the saphenous trunks (measured at the mid thigharea) exhibit a diameter that is lower than 7 mm.9
These observations outline some important con-siderations: first, 42% of incontinence in the greatsaphenous vein with incontinence of the sapheno-femoral junction is associated with the absence ofincontinence of the femoral valve located above thesaphenofemoral junction. In such cases, the hydro-static column is of relevance, and a saphenofemoralsurgical disconnection (eg, crossectomy or crosso-tomy) would be appropriate. Second, 58% of incon-tinence of the great saphenous vein with inconti-nence of the saphenofemoral junction is associatedwith continence of the proximal femoral valve. Inthese cases, where the hydrostatic femoral columnis low, any of the endovenous procedures can berecommended when a “demolishing” operation is
ÉTUDE DE LA JONCTION SAPHÉNOFÉMORALEPOUR COMPRENDRE LA DISTRIBUTION DES REFLUX
DANS LA MALADIE VEINEUSE CHRONIQUE
A vant de prendre une décision concernant le traitement adéquat pourun patient variqueux, il est nécessaire de définir comment une aire spé-cifique (par exemple le complexe saphénofémoral) peut être évaluée
chez le patient. Nous allons envisager deux aspects différents : d’abord, com-ment étudier un segment incontinent, ensuite, comment observer le complexesaphénofémoral, en se fondant sur les critères généraux décrits pour un seg-ment incontinent. La continence valvulaire doit être étudiée en orthostatismede façon à développer un gradient transvalvulaire rétrograde (opposé à l’orien-tation du plan valvulaire). Le gradient rétrograde est étudié de deux façonsdifférentes : 1) un test de haute pression, tel que le test de Valsalva ; et 2) un testde gravitation, qui exploite le poids de la colonne sanguine une fois qu’elle a étémobilisée. L’analyse de 1294 patients ayant une incontinence de la crosse dela grande veine saphène (complexe saphénofémoral) n’a révélé l’incontinencecomplète de la jonction saphénofémorale que dans seulement 55 % des cas. Unedissociation n’était notée que dans 6 % des cas. La valvule fémorale proximalea aussi été étudiée en utilisant les mêmes critères (par ex. la valvule de la veinefémorale commune située au-dessus de la jonction saphénofémorale). Elle s’estavérée être continente à la jonction saphénofémorale et au niveau de la voûtede la veine saphène dans 58,4 % des cas d’incontinence complète. Lorsque lavalvule fémorale supérieure est continente, les troncs saphènes (mesurés au mi-lieu de la cuisse) présentent un diamètre inférieur à 7 mm.
REFERENCES1. Tessari L. Histoire des éveinages: des origines au début duXXe siècle. Phlébologie. 2000;2:259-265.2. Cappelli M, Molino Lova R, Ermini S, et al. Ambulatory con-servative hemodynamic management of varicose veins: criticalanalysis of results at 3 years. Ann Vasc Surg. 2000;14:376-384.3. Cappelli M, Molino Lova R, Ermini S, Zamboni P. Hemody-namics of the saphenous-femoral junction. Patterns of reflux andtheir clinical implications. Int Angiol. 2004;23:25-28.4. Escribano JM, Juan J, Bofill R, Maeso J, Rodriguez-Mori A,Matas M. Durability of reflux elimination by a minimal invasiveCHIVA procedure on patients with varicose veins. A 3-yearprospective case study. Eur J Vasc Endovasc Surg. 2003;25:159-163.5. Criado E, Juan J, Fontcuberta J, Escribano JM. Haemodynam-ic surgery for varicose veins: Rationale and anatomic and haemo-dynamic basis. Phlebology. 2003;18:158-166.6. Cappelli M, Molino Lova R, Ermini S, Zamboni P. Relationshipbetween the caliber of the greater saphenous vein and the com-
petence, or absence/incompetence of femoral valve in subjectwith incompetence of the sapheno-femoral junction. 5th meet-ing of the European Venous Forum. June 25-June 27, 2004;Warsaw, Poland. Abstract.7. Reagan B, Folse R. Lower limb venous dynamics in normalpersons and children of patients with varicose veins. Surg GynecolObstet. 1971;132:15-18.8. Genovese G. Chirurgia delle Vene e dei Linfatici. Masson Edit;2005.9. Cappelli M, Molino Lova R, Ermini S, Giangrandi I, GiannelliF, Zamboni P. Hemodynamics of the sapheno-femoral complex:an operational diagnosis of femoral valve function. Int Angiol.2006;25:356-360.10. Tessari L. Empleo de esclerosantes en forma de microespumasen la terapéutica de los grandes ejes venosos superficiales. Magis-tral lecture at the 2nd International Course on Subdiaphrag-matic Chronic Venous Insufficiency: Abdominopelvic and LowerLimbs. October, 2004; Madrid, Spain.
115Study of the saphenofemoral junction to understand reflux distribution in CVD – Tessari and Cappelli MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E

116 Imaging of venous valves: B-Flow – Ferrara and MidiriMEDICOGRAPHIA, VOL 30, No. 2, 2008
The different pathological conditions affect-ing the venous system of the lower limbs canbe complicated to diagnose because of the
anatomical and physiological characteristics of thisarea.
The superficial venous system of the lower limbs,which statistically is more affected by parietal andvalvular alterations than other venous regions ofthe body, is made up of two main veins, the greatand the small saphenous veins, and various collat-eral veins. It is linked to the deep venous system bythe perforating system, which although we cannotdefine as a superficial venous system, is often in-volved in the pathological processes of this system.
Moreover, 6% of individuals are carriers of ano-malies of the internal saphena, such as the doublesaphena or triple saphena, or irregularities of cali-bre or position.1 Similar considerations can be madewith regard to the external saphena in terms of ano-malies or the number of collaterals2; these anoma-lies are often more complex than those of the in-ternal saphena. Absence of the saphenopoplitealjunction, with an implantation of the externalsaphena in other veins (perforations of the leg or in-ternal saphena)3 or anastomosis with the poplitealvein at a different level from normal, represent someof the challenges in diagnostics and in surgicaltherapy.4
To these anatomical observations we need to addothers regarding physiological aspects. The firstconsideration is regarding the force of gravity,which obstructs the venous return to the right atri-um. The return of venous blood to the right atriumis a result of the equilibrium between the centrifu-gal and the centripetal forces, the first being rep-resented most importantly and constantly by theforce of gravity, but also by accidental forces, suchas coughing or certain movements such as jump-ing to one’s feet or going up or down the stairs. Thecentripetal force is represented by the “vis a tergo”and the “vis a fronte:” plantar pressure reductionduring walking,5 the calf muscle pump,6-9 venoustone, and the pulse of the contiguous arteries.10 Thereturn of venous blood to the right atrium is alsohelped by the venous valves. These valves are bicus-pid plicae of endothelium and they serve to blockthe centrifugal forces and to ensure the one-wayflow of blood.
Venous circulation is regulated by the Poiseuillelaw, which organizes liquid flow in the vessels; itsapplication is more complicated than in the arte-rial system, because of the anatomical and physio-logical considerations described above. In the 1930s,engineering and medical research focused its at-tention on diagnostic systems that would be able todetect anatomical and hemodynamic alterations tothe venous system.
Doppler evaluation of the venous system
� Continuous wave DopplerIn the 1970s, the first applications of continuouswave Doppler were described in venous diagnostics;this method demonstrated important limitations,
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
D iagnosis of the different pathological conditions of the lower limb ve-nous system is complicated, because of the anatomical and physiolog-ical characteristics of this region. A total of 6% of individuals have an
anatomical anomaly of the internal or external saphena (ie, double or triplesaphena, irregularities of calibre or position), and in addition, there are phys-iological aspects that need to be considered regarding the return of blood tothe right atrium, which is important for the equilibrium between the centrifu-gal and centripetal forces. In the 1930s, engineering and medical research wasbased on diagnostic systems that detected anatomical and hemodynamic al-terations. The introduction of the echo-color Doppler systems represented animportant evolution. Nevertheless, conventional B-mode and color flow imag-ing have inherent limitations that degrade their utility: B-mode and color flowinvolve compromises in either axial resolution or penetration; in addition, acous-tic noise artifacts may mask out the extremely weak echoes from red bloodcells. This is an important limitation, especially in the evaluation of the venoussystem. B-Flow imaging is a new technique that uses digitally encoded sono-graphic technology to provide direct visualization of blood echoes in grayscale.This technique allows simultaneous imaging of blood flow, vessel walls, andneighboring tissues. Compared with color Doppler sonography, B-Flow sonog-raphy has a higher frame rate and better spatial resolution. Major limitationsof color Doppler sonography, such as aliasing, signal dropout at high Dopplerangles, color flash, and perivascular color artifacts, are eliminated with thistechnique.Medicographia. 2008;30:116-120. (see French abstract on page 120)
Keywords: venous valve; blood echo; color flow Doppler; B-Flow imaging;spatial resolution
Filippo FERRARA, MD Department of Internal MedicineCardiovascular disease and Nephro-urology
Massimo MIDIRI, MDDepartment of Radiological Science
University of Palermo, ITALY
Address for correspondence: Prof Filippo Ferrara, Via Autonomia Siciliana 94, 90143 Palermo, Italy(e-mail: [email protected])
Imaging of venousvalves: B-Flow b y F. F e r r a r a a n d M . M i d i r i ,I t a l y
�

tive velocity and power information, its temporaland spatial resolution is very limited. In an attemptto combine the better aspects of each mode, the con-ventional approach is to acquire and overlay colorflow data on B-mode data. But this approach alsoposes significant snags. Alternating between thesetwo modes inevitably compromises the scanner’sframe rate. In addition, any large tissue motion inthe color flow overlay may be displayed as a “colorflash artifact,” overshadowing the true flow data.Finally, because color flow has lower resolution, fill-ing in the vessels with color will almost always re-sult in some overwriting of the vessel walls in theB-mode image, which can conceal subtle lesions inthe vessel being studied.
B-Flow imaging
B-Flow imaging11 is a relatively new technique thatuses digitally encoded sonographic technology toprovide direct visualization of blood echoes in gray-scale. This technique allows simultaneous imagingof blood flow, vessel walls, and neighboring tissues.When compared with color Doppler sonography,B-Flow sonography has a higher frame rate andbetter spatial resolution. Major limitations of colorDoppler sonography, such as aliasing, signal drop-out at high Doppler angles, color flash, and perivas-cular color artifacts, are eliminated with this tech-nique.12
With B-Flow imaging, we enhance weak signalsand suppress unwanted echoes. As illustrated inFigure 2, the digitally encoded ultrasound beam-
however. It was not able to demonstrate the mor-phological alterations of the vein walls, and it couldnot identify all of the low-velocity flow.
� B-mode and color flow DopplerIn subsequent years, the introduction of the echo-color Doppler systems represented an importantevolution, especially when new tools were used withcolor module and pulsed wave Doppler. These toolscan directly and immediately identify alterations inthe morphology of the vein wall and valves, and canstudy the venous flow, even with the Valsalva testor A-sound and S-sound squashing applications.Nevertheless, despite many improvements over thepast two decades, conventional B-mode and colorflow Doppler imaging have a number of inherentlimitations that degrade their utility for assessinghemodynamics in major blood vessels.� LimitationsFirst, both B-mode and color flow imaging involvecompromises in either axial resolution or penetra-tion.This fundamental trade-off is illustrated in Fig-ure 1. In general, the shorter the transmit pulse,the better the axial resolution (ability to resolve twoclosely spaced objects). On the other hand, in or-der to improve penetration, more signal energy isneeded. The problem is that the pulse amplitude(instantaneous sound pressure) must be kept with-in some maximum allowable limit in accordancewith regulatory requirements. This means that theonly way to increase the energy of the pulse is totransmit a longer pulse. As a result, improved pen-etration invariably compromises axial resolution.In addition, in B-mode, acoustic noise artifactsmay mask out the extremely weak echoes from redblood cells—echoes that are typically 1/1000th thestrength of signals from the vessel wall and sur-rounding tissue. This is an important limitation inthe evaluation of the venous system.
By using large “packets” of longer transmit puls-es, along with special filtering and signal process-ing, color flow imaging is able to offer far better vi-sualization of weak blood echoes. However, thereare drawbacks to this improvement in flow sensi-tivity: the large packets limit frame rate, and thelonger transmit pulses degrade spatial resolution.So while color flow imaging may be very sensitiveto flow signals, thereby yielding valuable quantita-
Figure 1. With conventional B-mode and color flow Doppler, usersmust choose between good axial resolution and good penetration.With less energy there is poorer penetration, and with more energy,there is better penetration. With wideband, there is good axial reso-lution, with narrowband, there is poor axial resolution.
117Imaging of venous valves: B-Flow – Ferrara and Midiri MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
Less energy:poor penetration
Wideband:good axial resolution
More energy:good penetration
Narrowband:poor axial resolution
Figure 2. The B-Flow imageformation process.After reference 13:GE Ultrasound Europe. B-Flow: A New Way of Visualizing Blood Flow:Ultrasound TechnologyUpdate. Solinger, Ger-many: GE UltrasoundEurope; 1999. Copyright© 1999, GE UltrasoundEurope.
Electronic focusing
Receive decoder
Transmitencoder
Sensitivityincrease
Equalizetissue-blood
B-modeprocessing
Displaymonitor
Probe
Flow vessel

118 Imaging of venous valves: B-Flow – Ferrara and MidiriMEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
structed view of the vessel lumen. The grayscalepresentation of the flow data is also very intuitive,requiring no mental translation of the pixel datainto velocity or power information.
� B-Flow pixel brightnessTwo primary factors determine the pixel brightnessin B-Flow images: the strength of echoes from theblood, and the velocity of blood. In arterial flow, theblood echo in each pixel represents the summedeffect of backscattered sound waves from tens of
former consists of a transmit encoder and a re-ceive decoder in addition to the array focusingelectronics. Sending coded pulse sequences intothe body, the system decodes the returning signalsto enhance sensitivity to weak signals, and to sup-press nonmoving tissue signals. The rest of the dataprocessing is essentially the same as with conven-tional B-mode. To form a two-dimensional B-Flowimage, the B-mode processor accumulates the de-coded and processed signals from the transducerarray, reformats them into a pixel display—a processknown as scan conversion—and produces an inten-sity mapping of the resultant data using B-mode’sfinely graded grayscale.
For each scan line in the image, the scannertransmits not one, but a coded sequence of wide-band pulses that are amplitude-modulated accord-ing to a special digital code (saw-tooth pattern inbold line, Figure 3). Clearly, the coded pulse se-quence carries much more energy than a singlepulse, which translates directly into better signal-to-noise ratio or sensitivity.
Now imagine the coded pulse sequence bouncingback from a single perfect reflector. The receivedecoder recognizes the code, disassembles the pulsesequence into individual amplitude-modulated pulseunits, and effectively stacks them up to form a sin-gle pulse of amplitude given by the sum of the indi-vidual code units. Notice that the higher amplitudepulse has the same temporal length as the originalwideband pulse. Therefore, after decoding, one seesan imaging pulse of increased energy while main-taining wideband resolution.
By itself, the aforementioned operation wouldincrease both tissue and blood flow echoes by thesame amount, which could make the large tissuesignals look saturated in the display. Thus, for eachscan line, the decoder further preferentially sup-presses the signal samples that show a high degreeof similarity between successive pulse sequences,which are indicative of nonmoving tissue. The de-gree of tissue suppression is adjustable. The pre-ferred mode is to reduce nonmoving tissue signalsto a level comparable with that of flow signals, butas an option, the decoder can also completely re-move all background tissue, resulting in an angio-gram-like display.
B-Flow provides direct visualization of bloodechoes in a display just like that of B-mode. Becauseit images blood flow and its surrounding anatomysimultaneously and eliminates the need for over-lays, the resulting images provide a clear, unob-
Figure 3. Illustrationof the mechanism
behind coded excitationencoding and decoding.
After reference 13: GE UltrasoundEurope. B-Flow: A New Way of Visualizing Blood Flow: Ultra-
sound Technology Update.Solinger, Germany: GE Ultra-
sound Europe; 1999. Copyright ©1999, GE Ultrasound Europe.
Figure 4. Superiority of B-Flow (B and C) over colorDoppler imaging (A) in the visualization of venousflow and the venous wall.
Transmit Receive
Widebandpulse
Enhancedwideband pulse
Coded sequence of 8 pulses
Digitalencoder
1 1 1 0 01 1 1Sensitivityincrease
A
B
C

lenging in these situations, but it may also revealhemodynamics that have yet to be understood andused for diagnosis. B-Flow offers a number of ad-vantages over conventional imaging techniques.Compared with conventional color techniques, B-Flow delivers superior spatial resolution and framerate, allowing far better appreciation of the venoushemodynamics. B-Flow is much less dependent onthe user or scanning angle.16 There is no need tomanipulate complex color control parameters suchas packet size, wall filters, and color write-prioritythreshold—in fact, the vessel-wall overwriting prob-lem is completely eliminated, as B-Flow is not anoverlay technique.
Although Doppler processing can clearly providevaluable diagnostic information in terms of detect-ing blood flow, it is susceptible to such limitationsas aliasing, signal dropout at orthogonal detectionangles, and wall-filter limitations. As a B-modeimaging technique, B-Flow provides direct visua-lization of blood echoes without these limitations.17
Clinical applications
B-Flow has especially been used to demonstrate ul-cerated plaque and vessel-wall irregularities, as wellas being used to measure stenoses.18,19 It shouldpermit clinicians to measure the progression ofstenoses with greater precision, which will help tobetter determine the appropriate follow-up inter-vals. B-Flow also has the potential to minimize theneed for angiography as well as its inherent costsand risks.20,21
B-Flow’s ability to scan at high frame rates is im-portant for visualizing not only vascular hemody-namics, but also the interaction of blood flow with
thousands of red blood cells. The fine-grained ap-pearance of the blood echoes is therefore similarto the “speckle” texture one sees in conventionalB-mode images of soft tissue.
In general, blood echogenicity varies with a num-ber of interrelated blood conditions, includinghematocrit, the degree of red blood cell aggrega-tion14 (rouleaux formation), and flow state (laminaror turbulent).15 For example, the extensive red bloodcell aggregations that occur in low shear venousflow can significantly enhance blood echoes.
The velocity of blood relative to the ultrasoundbeam determines the degree of similarity betweenechoes from successive coded sequences. As theblood velocity increases, the red blood cells willmove in and out of each resolution volume of the ul-trasound beam faster. As a result, the echoes fromthe resolution volume will change by a greateramount from one coded sequence to the next. Sincethe change in echo information is used by the de-coder to achieve tissue-blood equalization, the B-Flow pixel brightness generally varies with both thespeed and direction of blood flow relative to the ul-trasound beam. In general, as flow velocity increas-es, the B-Flow signal tends to increase. As the ve-locity becomes so high that the signal samples fromsuccessive firings are uncorrelated, the correspond-ing B-Flow pixel brightness approaches a maximum.
Finally, extra care should be exercised in inter-preting B-Flow images of disturbed or diseased flowstates. For example, rouleaux formation may bepromoted in the stagnant flow regions around a ma-jor blockage, which can enhance the B-Flow signal.Flow turbulence that occurs distal to a significantocclusion can, in theory, also enhance blood echo-genicity. B-Flow interpretation is clearly more chal-
119Imaging of venous valves: B-Flow – Ferrara and Midiri MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
Figure 5. Ability of B-Flowimaging to highlight slowvenous flow. Panels A and Bshow color Doppler imageswith A-sound and S-soundmaneuvering, while panels Cand D show B-Flow images.
A B
C D

120 Imaging of venous valves: B-Flow – Ferrara and MidiriMEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
which cannot be visualized by color Doppler with-out the aid of A-sound and S-sound maneuvering(Figures 5A and B). This permits an anatomical andfunctional study of the valvular apparatus and ve-nous hemodynamics in the functional conditions inwhich the apparatus is to be found at the momentof observation, and avoids the need to resort to theaforementioned accelerations in flow that can resultin an overestimation of the extent of valvular insuf-ficiency.
The usefulness of B-Flow will continue to evolveas sonographers and physicians evaluate its utilityin new clinical situations. Its unique advantagespromise to make it an invaluable complement tocolor flow imaging techniques in peripheral vascu-lar applications. Its continued development also in-dicates that it might hold potential for other clini-cal applications and for contrast agent imaging. �
anatomical structures inside the vessel such as ve-nous valve cusps and thrombi. These fine structuresare usually masked by the color overlay in color flowimaging.22
In Figure 4A (page 118), color-Doppler evaluationshows a flow signal that is not contained within thevenous walls, thus hampering the visualization ofthe vessel’s borders. B-flow technique improvesimaging quality, and can depict venous flow and thevessel wall without the presence of “overwriting”artifacts. Figure 4B illustrates B-flow evaluation be-fore the Valsalva maneuver, and Figure 4C illus-trates B-flow evaluation after the Valsalva maneu-ver: in addition to the reflux, the venous valve canbe seen as a slightly hypoechoic linear image (whitearrow).
Another advantage of B-Flow is that it can high-light slow venous flow (Figures 5C and D, page 119),
REFERENCES1. Bouchet A. Anatomie normale et variations du système veineuxdes membres inférieurs. I Artères et Veines.1988;3:246-261.2. De Simone J. Anatomie des veines musculaires du mollet. Phlé-bologie. 1996;49:299-308.3. Dortu JA, Dortu J. Anatomie clinique du complexe saphéniena la cuisse. Phlébologie. 1993;46:91-100.4. Pfeifer JR. The anatomy and physiology of the venous systemof the lower extremities. Phlébologie. 1992;45:12-19.5. Van Cleef JF. Modele dynamique de la pompe musculaire demollet dans l’insuffisance veineuse profunde. Phlébologie.1992;45:259-263.6. Clayes R. Activitès de la musculature jambière dans la vie cou-rante. Phlébologie. 1990;42:55-62.7. Yang D, Vandongen YK, Stacey MC. Effect of exercise on calfmuscle pump function in patients with chronic venous disease.Br J Surg. 1999;86:338-341.8. Padberg FT Jr, Johnston MV, Sisto SA. Structured exercise im-proves calf muscle pump function in chronic venous insufficien-cy: a randomized trial. J Vasc Surg. 2004;39:79-87.9. Labropoulos N, Giannoukas AD, Nicolaides AN, Veller M, LeonM, Volteas N. The role of venous reflux and calf muscle pumpfunction in nonthrombotic chronic venous insufficiency. Corre-lation with severity of signs and symptoms. Arch Surg.1996;131:403-406.10. Van der Stricht J, Staelens I. Veines musculaires du mollet.Phlébologie. 1994;47:135-142.11. Chiao R, Mo L, Hall A, et al. “B-mode Blood Flow Imaging,”AIUM Annual Convention, San Francisco, 2000 April 2-5. Abstract.12. Clevert DA, Rupp N, Reiser M, Jung EM. Improved diagnosisof vascular dissection by ultrasound B flow: a comparison withcolor-coded Doppler and power Doppler sonography. Eur Radiol.2005;15:342-347.13. GE Ultrasound Europe. B-Flow: A New Way of VisualizingBlood Flow: Ultrasound Technology Update. Solinger, Germany:GE Ultrasound Europe; 1999.14. Yuan YW and Shung KK. Ultrasonic backscatter from flow-ing whole blood. I: dependence on shear rate and hematocrit.J Acoust Soc Am. 1988,84:52-58.15. Sigel B, Machi J, Beitler JC, Justin JR, Coelho JCU. Variableultrasound echogenicity in flowing blood. Science. 1982;218:1321-1323.16. Whittinghan TA. Medical diagnostic applications and sources.Prog Biophys Mol Biol. 2007;93:84-110.17. Yucel C, Oktar SO, Erten Y, et al. B-flow sonographic evalu-ation of hemodialysis fistulas: a comparison with low- and high-pulse repetition frequency color and power Doppler sonography.J Ultrasound Med. 2005;24:1503-1508.
18. Clevert DA, Johnson T, Jung EM, et al. Color Doppler, powerDoppler and B-flow ultrasound in the assessment of ICA stenosis:comparison with 64-MD-CT angiography. Eur Radiol. 2007;17:2149-2159.19. Jung EM, Kubale R, Ritter G, et al. Diagnostics and charac-terization of preocclusive stenoses and occlusions of the internalcarotid artery with B-flow. Eur Radiol. 2007;17:439-447.20. Yurdakul M, Tola M, Cumhur T. B-flow imaging of internalcarotid artery stenosis: comparison with power Doppler imagingand digital subtraction angiography. J Clin Ultrasound. 2004;32:243-248.21. Wachsberg RH. B-flow, a non-Doppler technology for flowmapping: early experience in the abdomen. Ultrasound Q. 2003;19:114-122.22. Graiche JA, Lane RJ, Cuzzilla MI, Coroneos JC, Berney CR.Incompetent venous valves: ultrasound imaging and exo-stentrepair. Phlébologie. 2004;57:237-252.
IMAGERIE DES VALVULES VEINEUSES : LE MODE B
L e diagnostic des différentes pathologies du système veineux du membreinférieur est compliqué en raison des caractéristiques anatomiques etphysiologiques de cette région. Six pour cent d’individus au total présen-
tent des anomalies anatomiques des saphènes interne ou externe (par exemple,saphène triple ou double, des irrégularités de calibre ou de situation) et en plus,certains aspects physiologiques doivent être pris en compte en ce qui concernele retour veineux dans l’oreillette droite, important pour l’équilibre entre lesforces centrifuge et centripète. Dans les années 30, la recherche industrielle etmédicale était basée sur des systèmes de diagnostic qui détectaient les alté-rations anatomiques et hémodynamiques. L’introduction de l’écho-Dopplercouleur est une évolution importante. Les limites inhérentes à l’imagerie enmode B conventionnel et en couleur diminuent néanmoins leur utilité : le Dop-pler couleur et en mode B font un compromis entre la résolution axiale ou lapénétration ; de plus, les artéfacts acoustiques sonores peuvent masquer leséchos extrêmement faibles venant des globules rouges. Cette limite est impor-tante surtout dans l’évaluation du système veineux. L’imagerie en mode B estune nouvelle technique qui utilise une technologie échographique numériséequi permet de visualiser directement les échos sanguins en échelle de gris. Ellepermet d’obtenir simultanément des images du flux sanguin, de la paroi desvaisseaux et des tissus environnants. Comparée à l’écho-Doppler couleur, l’échoen mode B a une vitesse de lecture d’images supérieure et une meilleure réso-lution spatiale. Elle élimine les principales limites de l’écho-Doppler couleur,tels le repliement spectral, la disparition du signal aux angles Doppler élevés,le flash couleur et les artéfacts de couleur périvasculaires.

R obust evidence has now been gathered to in-dicate that chronic venous disease (CVD) ofthe lower limb is a noninfectious inflamma-
tory disease.1 This picture has opened the door tofurther investigation that may lead to an under-standing of the trigger mechanisms of inflamma-tion in CVD—the cause of its earliest manifesta-tions—to form a basis for prevention and design ofnew interventions. Markers of inflammation accom-pany every stage of the disease—from telangiec-tasia, venous eczema, ankle skin hyperpigmenta-tion, atrophie blanche, and lipodermatosclerosis, tothe most severe forms involving varicose veins andvenous leg ulcers. This picture facilitates our un-derstanding of the pathophysiological processesthat underlie these diverse manifestations, particu-larly at the cellular and molecular levels.
The inflammatory process is a repair mechanism
As a background to the following discussion, it isimportant to remember that the inflammatory cas-cade,with its stereotypic steps, is designed toachievethe initial removal of damaged tissue and the even-tual generation and deposition of new tissue in the“resolution of the inflammation.” As such, it servesas the main biological repair mechanism in livingorganisms. Every tissue can mount an inflamma-tory cascade and it is the only repair mechanismpresent in mammalian tissue; it is used over andagain, from birth and through all the injuries sus-tained over a lifetime. Many individual steps in theinflammatory cascade are required to achieve reso-lution of the inflammation. For example, the gener-ation of new proteins, such as acute phase proteins,cytokines, chemokines, or growth factors, formspart of the repair aspect of the inflammatory cas-cade. If markers of inflammation persist over time,and CVD is a prime example in this regard as it maylast for many years, we have to ask the question asto what mechanisms exist to prevent resolution ofthe inflammation and instead continue to causeinjury. It is not until we understand the initial in-jury mechanisms that we will be able to find themost effective intervention. Otherwise, we are rel-egated to treatment of the disease symptoms only.
Early microvascular manifestations of inflammation
One of the early signs of CVD at the microvascu-lar level is elevated endothelial permeability, a statethat tends to be caused by the opening of interen-dothelial tight junctions as well as endothelial poreformation. This can be readily observed in acute
121Triggering mechanisms of venous valve incompetence – Schmid-Schönbein MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
G enetic risk factors, hormonal impregnation, prolonged hydrostatic pres-sure, and abnormal fluid shear stress in chronic venous insufficiencymay all serve as mechanisms that lead to the cascade of events asso-
ciated with aseptic inflammation. The inflammation is manifest in the form ofactivated endothelium, leukocyte adhesion to the endothelium and migrationinto the tissue, mast cell degranulation, and T-lymphocyte and monocyte in-filtration with macrophage transformation. Fibroblasts target the extracellularmatrix as well as parenchymal cells, and produce a spectrum of inflammatorymediators and metabolites, cell membrane adhesion molecules, prothrombot-ic receptors, growth factors, and chemotactic agents. The inflammatory cas-cade serves fundamentally as a tissue repair mechanism. However, in chronicvenous insufficiency with development of valvular incompetence, the inflam-mation does not resolve, and instead leads to clinical manifestations that rangefrom varicosities to the eventual occurrence of ulcers. The factors that triggerthe inflammation in chronic venous insufficiency are still uncertain.Medicographia. 2008;30:121-126. (see French abstract on page 126)
Keywords: inflammation; endothelium; growth factor; leukocyte; adhesionmolecule; proteinase; fluid shear stress; venous wall stretch
Geert W. SCHMID-SCHÖNBEIN, PhDThe Whitaker Institute of Biomedical EngineeringUniversity of California San DiegoLa Jolla, CA, USA
Address for correspondence: Geert W. Schmid-Schönbein, Department of Bioengineering, Whitaker Institute of Biomedical Engineering, University of California San Diego, La Jolla, CA 92093-0412, USA(e-mail: [email protected])
Triggering mechanismsof venous valve incompetence b y G . W. S c h m i d - S c h ö n b e i n , U S A
SELECTED ABBREVIATIONS AND ACRONYMS
CVD chronic venous diseaseICAM-1 intercellular adhesion molecule–1 MMP matrix metalloproteinaseTGFβ1 transforming growth factor β-1VEGF vascular endothelial growth factor

� Circulating cell entrapment and membraneadhesionThe structural changes in the capillary network arealso accompanied by erythrocyte packing in thelumen of capillaries, leukocyte entrapment withincapillaries and adhesion to the venular endotheli-um and valve leaflets, and even white cell/plateletaggregate formation that can fill the lumen of mi-crovessels. Leukocytes may be found in pericapillarytissue in patients with CVD.13 Skin biopsies fromCVD limbs show elevated numbers of macrophages,T-lymphocytes, and mast cells.14 The same patternhas been observed in both acute15 and chronic16 ex-perimental rat models of venous hypertension thatdepend predominantly on pressure and fluid shear,with elevated levels of tissue leukocytes in skin sam-ples from affected limbs, but not from sham-oper-ated controls.
The leukocyte entrapment within capillaries isa result of the stiff cytoplasmic properties of theleukocytes and their ability to express membraneadhesion molecules. As a consequence, leukocytes(eg, neutrophils, monocytes, T-lymphocytes) accu-mulate in the lower extremities under conditions ofhigh venous pressure. Their accumulation in mi-crovessels is enhanced by the fact that the cells mayalready be activated in the central circulation in pa-tients with CVD,17 a process that further enhancesthe stiffness of the cytoplasm as well as the mem-brane adhesion.18 At the microvascular level, thereare important details to consider regarding micro-vascular entrapment in the skin. Leukocyte entrap-ment in the narrow, single file capillaries can becaused by a simple stiffening of the cytoplasm or byprojection of cytoplasmic pseudopods.19 No mem-brane adhesion is required. Since entrapment ofleukocytes by cytoplasmic stiffening is limited tocapillaries, the cytotoxic properties of leukocyteshave a bearing on the tissue parenchyma that sur-rounds the capillary network.
By contrast, attachment of leukocytes to postcap-illary venules in the skin microcirculation requiresmembrane adhesion to the endothelium via L-se-lectin on the leukocyte membrane and E-selectinon endothelial cells. In this case, the venules arethe major site for the cytotoxic activity of leuko-cytes. The initial transient membrane attachmentis followed by firm adhesion via integrins, the start-ing point for leukocyte migration out of the vascu-lature and degranulation. In CVD, the evidence sug-gests that avarietyof membrane adhesionmoleculeson endothelial cells and leukocytes (intercellularadhesion molecule-1 [ICAM-1], vascular cell adhe-sion molecule-1 [VCAM-1], lymphocyte function–associated antigen–1 [LFA-1], very late antigen–4[VLA-4], Mac 1, and others) appear to facilitate theadhesion and stimulate the projection of pseudo-podia as a requirement for transmigration of theleukocyte into the venous wall. Basal plasma lev-els of the adhesion molecules ICAM-1, endothe-lial leukocyte adhesion molecule–1 (ELAM-1) andVCAM-1 are higher in CVD patients than in con-trols, and are increased significantly in response tovenous hypertension provoked by standing.20 Anycombination of leukocyte cytoplasmic stiffening
models of venous hypertension. There are a largenumber of mediators (histamine, complement pro-tein, platelet activating factor, vascular endothe-lial growth factor [VEGF], cytokines) with the abil-ity to elevate endothelial permeability; most of themwhen applied to a venule, act transiently via nitricoxide,2 actin polymerization, and selected smallGTPases.3,4 These early events in CVD may alreadybe driven by mechanisms that have the ability toproduce chronic inflammation. Elevation of endo-thelial permeability, with the opening of leakagesites between endothelial cells, depends on the in-terendothelial adhesion molecule VE-cadherin,5 anendothelial glycocalyx layer that is sensitive to en-zyme degradation,6 the specific venular genotypes,7
and on exercise training.8 Thus, the reduction of en-dothelial permeability may be a target opportunityfor early intervention in CVD.
� Angiogenesis and microvascular restructuringA rich record exists of the relatively early event inthe inflammatory process in CVD that involves li-posclerotic skin formed via capillary angiogenesisand apoptosis in superficial layers of the skin. Areasof white atrophy, known as atrophie blanche, mayshow a loss of capillaries, while in other areas, thecapillaries become dilated, elongated, coiled, andtortuous.9 This goes hand in hand with the occur-rence of lesions in endothelial cells, with irregularcell shapes and distortion of the luminal surface, in-creased intracytoplasmic vesicles, and intracellularedema. Basement membranes fuse with the sur-rounding tissue. Pericapillary spaces are filled witha fluid that can contain cellular fragments and pro-teins. Fibrinogen deposits known as fibrin cuffs canbe observed in the pericapillary spaces and aroundcapillaries.10
In lipodermatosclerosis, the skin capillaries areelongated and tortuous, and even have a glomerularappearance with proliferation of the capillary endo-thelium. VEGF is an obvious candidate for involve-ment in these changes, a factor that has also beenshown to increase microvascular permeability.Plasma levels of VEGF increase during acute venoushypertension11 and are higher in CVD patients withskin changes than in CVD patients with normalskin. Both VEGF expression and expression of itsreceptor, Flk-1, are influenced by blood shear stressand an inflammatory reaction. VEGF levels increasewith the severity of the disease and the CEAP score(Clinical condition, Etiology, Anatomic location andPathophysiology).
It should be mentioned that in CVD, the skin isassociated with dermal tissue fibrosis. Immuno-cytochemical analysis of punch biopsy specimenshas shown that skin from the lower calf of CVD pa-tients has significantly elevated active transforminggrowth factor β–1 (TGFβ1) levels compared withnormal skin or skin taken from the thigh region ofthe same patients. The TGFβ1 is located in leuko-cytes and fibroblasts, and on collagen fibrils. Acti-vated leukocytes migrate out of the vasculature (seenext section) and release TGFβ1, stimulating in-creased collagen production by dermal fibroblasts,leading to dermal fibrosis.12
122 Triggering mechanisms of venous valve incompetence – Schmid-SchönbeinMEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E

The sensing mechanisms that allow cells to respondto such small fluid mechanical forces involve G-protein–coupled receptors.27 The phenomenon maybe quite relevant with respect to CVD, because ofthe strong hemodynamic components of the dis-ease. In the presence of a biophysical response tofluid shear stress, a mere shift in the blood flowfield in venules may itself be a proinflammatorystimulus.
There is now a large body of evidence to suggestthat virtually all functions of endothelial cells arecontrolled by fluid shear stress.28,29 Steady shearstress within a normal physiological range of about10 dyn/cm2 is largely anti-inflammatory. In contrast,low flow or flow disturbances, especially if they in-volve instances of reversed flow direction with for-ward and backward shear, cause a loss of this phe-notype. Instead, the endothelial cell becomes moresusceptible to inflammatory mediators. Stretch ofendothelial cells and smooth muscle cells also hasa direct effect on many aspects of their biology,30 in-cluding synthesis and release of inflammatory mole-cules such as leukotrienes, prostaglandin, brady-kinin, free oxygen radicals, and cytokines.
Finally, we should note that in addition to localbiochemical or biophysical factors operating dur-ing venous hypertension, CVD patients have a ten-dency toward systemically elevated leukocyte adhe-sion outside the veins in the affected leg. Centralvenous plasma obtained from CVD patients has beenshown to induce higher degrees of activation (as-sessed by oxygen-free radical production and pseu-dopod formation) in healthy, naive granulocytesthan did plasma taken from normal subjects.17 Thenature of the plasma factor(s) responsible for theactivation is currently unknown.
Valve failure
A key event in CVD is the loss of the ability to prop-erly close venous valves. Failure of valves may bebrought about by dilation of the venous wall andthe valvular annulus with remodeling of the valveleaflets, bulging and stretching of valve leaflets,commissural dilation, shortening, tearing and per-foration of leaflets and, finally, complete destruc-tion of the valve.31,32 Furthermore, ultrastructuraland immunohistochemical studies of valves and thevenous wall have revealed the presence of leuko-cytes adhering and transmigrating into the venouswall.17,33 The leukocyte infiltration of the venousparenchyma is accompanied by remodeling of theextracellular matrix, a process that may in part beresponsible for the destruction of venous valves.
Tissue proteolytic activity
Chronic dermal ulcers involve proteolytic activitythat degrades extracellular matrix proteins. Proteas-es are also of major interest in this context, becauseof their involvement in both the inflammatory re-action and the remodeling of cutaneous tissue.34,35
The overexpression of Ca/Zn-dependent endopro-teinases (matrix metalloproteinases, MMPs), MMP-3(stromelysin-1), and MMP-13 (collagenase-3) is as-
and pseudopod formation together with enhancedmembrane adhesion molecule expression serves tofurther enhance leukocyte trapping both in capil-laries and in venules.
Little is currently known about the adhesionmolecules expressed on venous valve leaflets, al-though it is known that the valves require specifictranscription factors to be formed and that the en-dothelium on valve leaflets may have a differentphenotype to that of the endothelium on adjacentblood vessels.21
� Leukocyte activationLeukocytes that accumulate in the microcirculationbecome activated and are key players in the inflam-matory reaction, provoking skin changes in CVD.Although cytokines are part of the inflammatory re-action in CVD,22 no clear picture exists about theirexact role. For example, treatment with granulo-cyte/monocyte colony stimulating factor (GM-CSF)to heal ulcers leads to mixed results. Tumor necro-sis factor–α (TNFα), whose expression is enhancedin many inflammatory reactions, stimulates the ex-pression of inflammatory adhesion molecules, thesynthesis and release of other cytokines, and thechemotaxis of neutrophils and macrophages. Theexpression of TNFα appears to be upregulated inpatients with venous ulcers, and healing of the ul-cer may reduce the level of TNFα.23 It is importantto remember that cytokine expression forms part ofthe repair aspect of the inflammatory cascade, andtherefore no clear correlation with the degree of thedisease may exist.
Treatment of CVD patients by compression ban-dage wrapped around the diseased leg has a dis-tinct anti-inflammatory effect.24 Although the exactmechanism by which compression therapy operatesis unknown, the evidence indicates that we need toconsider mechanical stress as a mechanism for in-flammation. Indeed, the transition from a normalinactivated state to an activated state may not onlybe facilitated by inflammatory mediators releasedfrom the endothelium or from adjacent tissue (eg,release of platelet activating factor, TNFα, and oth-ers) but also be caused by mechanical fluid shearstress25 in the absence of chemical mediators.
Fluid shear stress is a tangential force (per unitarea), and it is present in all parts of a venule; on theendothelium, in the wall of the venule, in the valveleaflets, and elsewhere. Among the many mecha-nisms responsible, it can be produced by the move-ment of blood acting on the endothelial surface, inwhich case it is a function of the velocity gradient ofblood near the endothelial surface and the bloodviscosity. This particular fluid shear stress is rela-tively low, ie, of the order of 10 dyn/cm2, a quantitythat is ~1/100th of the stress caused by the weightof 1 cm H2O! Yet the lack of such low, but still phys-iologically relevant, levels of fluid shear stress canlead to leukocyte activation even in the absence ofbiochemical inflammatory mediators.26 The abilityof leukocytes and other cardiovascular cells to re-spond either to chemical or physical stimulationhas led to a significant deviation from past thinkingregarding trigger mechanisms for inflammation.
123Triggering mechanisms of venous valve incompetence – Schmid-Schönbein MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E

and venules, but also of the capillary network feed-ing the venules. An issue quite relevant, therefore,is the fact that the expression levels of MMPs can becontrolled by mechanical stretch of cells in a waythat depends on the time course of the strain. Thishas been studied in vitro in smooth muscle cells sub-jected to oscillatory and constant strain. Stationarystrain significantly increases MMP-2 mRNA levelsat all time points, whereas cyclic strain decreases itafter 48 hours. Both secreted and cell-associatedpro-MMP-2 levels are increased by stationary strainat all time points, whereas cyclic strain decreasessecreted levels after 48 hours. MMP-9 mRNA levelsand pro-MMP-9 protein are increased after 48 hoursof stationary strain compared with no strain andcyclic strain.47 Endothelial cells also respond tostretch by restructuring the cell cytoplasm.48
Trigger mechanisms for inflammation in chronic venous disease
Inflammation in CVD may continue without reso-lution for months and years. Our understanding ofthe mechanisms that serve to maintain such an in-flammatory state needs to be improved. The discus-sion above suggests that elevation of venous pres-sure per se, eg, after the loss of venous valves, withstretching of endothelial cells and development ofan abnormal fluid shear stress pattern, may itself bean injurious inflammatory stimulus. The availableevidence is compatible with this proposal, but de-tailed analysis with realistic models of the mechan-ical pattern of fluid in human veins is not current-ly available.
But one is compelled to ask the question “Whatmechanisms may lead to destruction of a venousvalve in the first place?” (Figure 1). There is the pos-sibility of venous wall distension by blood pressureelevation, caused by posture or inadequate lowerlimb activity (prolonged standing with lack of ve-nous compression by muscle contraction). Somepatients may have obstructed proximal venouspathways (eg, due to obesity) that cause chronical-ly elevated pressure in veins of the lower limbs, and
sociated with nonhealing wounds.36 There is in-creased expression of MMP-2 and tissue inhibitorof metalloproteinase (TIMP)–1 in liposclerotic skin,venous leg ulcers, and wound fluid from nonheal-ing venous ulcers.37 An upregulation of the expres-sion of MMP-9 has been observed on the edges ofvenous ulcers, and the plasma of patients with se-vere CVD has an increased rate of MMP-9 activation.Levels of TIMP-2 are lower in lipodermatoscleroticskin and ulcers.37 Uncontrolled MMP activity maycontribute to extracellular matrix protein break-down, which impairs healing.
MMPs are positioned on extracellular matrix pro-teins, and may be released from preexisting poolsor may be newly synthesized. The inactive pro-en-zymes are activated by other proteinases, includingthose produced by mast cells.38 Neutrophils havegelatinolytic activity discharged by MMP-9, MMP-8(a neutrophil collagenase), and leukolysin (a mem-brane-type MMP). Knockout experiments suggestthat MMP-9 acts upstream of neutrophil elastase byproteolytically inactivating neutrophil elastase in-hibitor A1PI,39 and that it can activate other MMPs.40
Extracellular MMP inducer (EMMPRIN; CD147) hasbeen observed to increase MMP expression, andmembrane type 1 MMP (MT1-MMP) was implicatedin the activation of MMPs. Venous leg ulcers haveelevated expression of EMMPRIN, MMP-2, MT1-MMP, and MT2-MMP.41
An important issue is the activation of inactiveproenzymes in CVD. As discussed above, leukocyteactivation in patients with chronic venous insuffi-ciency manifests itself in the form of degranulation,with an increase in neutrophil elastase and lactofer-rin release.42 The enzymes have been proposed to beeffective activators of other proenzymes, such asMMPs.43 Other mechanisms by which MMPs are ac-tivated may involve serine proteases, such as tryp-sin,44 MMP-3, and MMP-13.45 Plasmin stimulatespro-MMP enzyme conversion to the active form.46
Plasmin hyperactivity caused by decreased plas-minogen activator inhibitor–1 (PAI-1) may thuscause uncontrolled MMP activity. Elevated venouspressure in CVD causes stretch not only of the veins
124 Triggering mechanisms of venous valve incompetence – Schmid-SchönbeinMEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
Vein wall
• Orthostatic pressure• Proximal venous obstruction
Venous pressure elevation by
Valve leaflet destructionA B
C DVein wall distension by
proteolytic tissue weakeningVein wall distension by pressure
Vein valve
• Progesterone• Genetic and environmental
• Leukocyte adhesion
Mechanisms for MMP
Altered fluid shearstress on endothelium
Figure 1. A schematicdiagram illustrating selected
mechanisms that may controlinflammation of the vein walland valve leaflet. Normal vein
and valve leaflets (A). Valveleaflets may be subject toinflammatory damage by
alteration in magnitude anddirection of fluid shear stress
on the endothelium (B).Venous valves may become
unable to close their leafletsdue to vein wall distension by(C) elevated venous pressure
or by (D) weakening of thevein wall due to proteolytic
degradation of its extra-cellular matrix. MMP, matrix
metalloproteinase.

tracellular matrix was restructured. Over the periodof time required to develop manifestations of CVD,it is likely that more than one mechanism may beresponsible for the injury and inflammation in veins.The challenge is to identify the prevailing mecha-nism underlying CVD in each individual. �
Acknowledgement: I would like to thank my colleagues,Drs John J. Bergan, Luigi Pascarella, Shinya Takase,Takeshi Ono, Thomas Alsaigh, and Alexander Penn whocarried out the experimental studies summarized inthis report.
may thus be candidates for venous stents. Long-term measurements in real-life environments arerequired to fully understand the role of such fac-tors in the disease. The venous wall may also bedistended because its mechanical properties areweakened or because its smooth muscle is dilated.The underlying mechanisms may be derived froma genetic defect49 or the presence of a hormonalload during early pregnancy (eg, progesterone50).The distension of veins after pregnancy may re-main without recovery if during pregnancy the ex-
125Triggering mechanisms of venous valve incompetence – Schmid-Schönbein MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
REFERENCES1. Bergan JJ, Schmid-Schönbein GW, Smith PD, Nicolaides AN,Boisseau MR, Eklof B. Chronic venous disease. N Engl J Med.2006;355:488-498.2. Al-Naemi H, Baldwin AL. Nitric oxide protects venules againsthistamine-induced leaks. Microcirculation. 2000;7:215-223.3. Waschke J, Burger S, Curry FR, Drenckhahn D, Adamson RH.Activation of Rac-1 and Cdc42 stabilizes the microvascular en-dothelial barrier. Histochem Cell Biol. 2006;125:397-406.4. Curry FE, Zeng M, Adamson RH. Thrombin increases perme-ability only in venules exposed to inflammatory conditions. Am JPhysiol Heart Circ Physiol. 2003;285:H2446-H2453.5. Corada M, Mariotti M, Thurston G, et al. Vascular endothelial-cadherin is an important determinant of microvascular integri-ty in vivo. Proc Natl Acad Sci U S A. 1999;96:9815-9820.6. Huxley VH, Williams DA. Role of a glycocalyx on coronary ar-teriole permeability to proteins: evidence from enzyme treatments.Am J Physiol Heart Circ Physiol. 2000;278:H1177-H1185.7. Thurston G, Baluk P, McDonald DM. Determinants of endothe-lial cell phenotype in venules. Microcirculation. 2000;7:67-80.8. Laughlin MH, McAllister RM, Jasperse JL, Crader SE, WilliamsDA, Huxley VH. Endothelium-medicated control of the coronarycirculation.Exercise training-inducedvascularadaptations.SportsMed.1996;22:228-250.9. Leu AJ, Leu HJ, Franzeck UK, Bollinger A. Microvascularchanges in chronic venous insufficiency—a review. CardiovascSurg.1995;3:237-245.10. Bollinger A, Leu AJ, Hoffmann U, Franzeck UK. Microvascularchanges in venous disease: an update. Angiology.1997;48:27-32.11. Shoab SS, Scurr JH, Coleridge-Smith PD. Increased plasmavascular endothelial growth factor among patients with chronicvenous disease. J Vasc Surg. 1998;28:535-540.12. Pappas PJ, You R, Rameshwar P, et al. Dermal tissue fibrosisin patients with chronic venous insufficiency is associated withincreased transforming growth factor-beta1 gene expression andprotein production. J Vasc Surg. 1999;30:1129-1145.13. Moyses C, Cederholm-Williams SA, Michel CC. Haemocon-centration and accumulation of white cells in the feet during ve-nous stasis. Int J Microcirc Clin Exp.1987;5:311-320.14. Pappas PJ, DeFouw DO, Venezio LM, et al. Morphometric as-sessment of the dermal microcirculation in patients with chron-ic venous insufficiency. J Vasc Surg. 1997;26:784-795.15. Takase S, Lerond L, Bergan JJ, Schmid-Schönbein GW. Theinflammatory reaction during venous hypertension in the rat.Microcirculation. 2000;7:41-52.16. Hahn TL, Unthank JL, Lalka SG. Increased hindlimb leuko-cyte concentration in a chronic rodent model of venous hyper-tension. J Surg Res. 1999;81:38-41.17. Takase S, Schmid-Schönbein G, Bergan JJ. Leukocyte activa-tion in patients with venous insufficiency. J Vasc Surg.1999;30:148-156.18. Schmid-Schönbein GW, Lee J. Leukocytes in capillary flow.Int J Microcirc Clin Exp.1995;15:255-264.19. Worthen GS, Schwab B, Elson EL, Downey GP. Cellular me-chanics of stimulated neutrophil: stiffening of cells induces re-tention in pores in vitro and lung capillaries in vivo. Science.1989;245:183-186.20. Saharay M, Shields DA, Georgiannos SN, Porter JB, Scurr JH,Coleridge Smith PD. Endothelial activation in patients with chron-ic venous disease. Eur J Vasc Endovasc Surg.1998;15:342-349.21. Butcher JT, Tressel S, Johnson T, et al. Transcriptional profilesof valvular and vascular endothelial cells reveal phenotypic differ-ences: influence of shear stress. Arterioscler Thromb Vasc Biol.2006;26:69-77.22. Quatresooz P, Henry F, Paquet P, Pierard-Franchimont C,Harding K, Pierard GE. Deciphering the impaired cytokine cas-cades in chronic leg ulcers (review). Int J Mol Med.2003;11:411-418.
23. Murphy MA, Joyce WP, Condron C, Bouchier-Hayes D. A re-duction in serum cytokine levels parallels healing of venous ulcersin patients undergoing compression therapy. Eur J Vasc EndovascSurg. 2002;23:349-352.24. Junger M, Steins A, Hahn M, Hafner HM. Microcirculatorydysfunction in chronic venous insufficiency (CVI). Microcircula-tion. 2000;7:S3-S12.25. Moazzam F, DeLano FA, Zweifach BW, Schmid-SchönbeinGW. The leukocyte response to fluid stress. PNAS.1997;94:5338-5343.26. Fukuda S, Yasu T, Predescu DN, Schmid-Schönbein GW.Mechanisms for regulation of fluid shear stress response in cir-culating leukocytes. Circulation Research. 2000;86:E13-E18.27. Makino A, Prossnitz ER, Bunemann M, Wang JM, Yao W,Schmid-Schönbein GW. G protein-coupled receptors serve asmechanosensors for fluid shear stress in neutrophils. Am J Phys-iol Cell Physiol. 2006;290:C1633-C1639.28. Kakisis JD, Liapis CD, Sumpio BE. Effects of cyclic strain onvascular cells. Endothelium. 2004;11:17-28.29. Resnick N, Yahav H, Shay-Salit A, et al. Fluid shear stress andthe vascular endothelium: for better and for worse. Prog BiophysMol Biol. 2003;81:177-199.30. Sasamoto A, Nagino M, Kobayashi S, Naruse K, Nimura Y,Sokabe M. Mechanotransduction by integrin is essential for IL-6secretion from endothelial cells in response to uniaxial continu-ous stretch. Am J Physiol Cell Physiol. 2005;288:C1012-C1022.31. Van Cleef JF, Desvaux P, Hugentobler JP, et al. Étude endo-scopique des reflux valvulaires sapheniens. J Mal Vasc.1992;17:113-116.32. Blanchemaison P. Interet de L’endoscopie veineuse dans l’ex-ploration et le traitement de l’insuffisance veineuse des membresinferieurs. [Significance of venous endoscopy in the explorationand the treatment of venous insufficiency of the legs]. J Mal Vasc.1992;17(suppl B):109-112.33. Ono T, Bergan JJ, Schmid-Schönbein GW, Takase S. Monocyteinfiltration into venous valves. J Vasc Surg. 1998;27:158-166.34. Woodside KJ, Hu M, Burke A, et al. Morphologic character-istics of varicose veins: possible role of metalloproteinases. J VascSurg. 2003;38:162-169.35. Saito S, Trovato MJ, You R, et al. Role of matrix metallopro-teinases 1, 2, and 9 and tissue inhibitor of matrix metallopro-teinase-1 in chronic venous insufficiency. J Vasc Surg. 2001;34:930-938.36. Fray MJ, Dickinson RP, Huggins JP, Occleston NL. A potent,selective inhibitor of matrix metalloproteinase-3 for the topicaltreatment of chronic dermal ulcers. J Med Chem. 2003;46:3514-3525.37. Mwaura B, Mahendran B, Hynes N, et al. The impact of dif-ferential expression of extracellular matrix metalloproteinase in-ducer, matrix metalloproteinase-2, tissue inhibitor of matrix met-alloproteinase-2 and PDGF-AA on the chronicity of venous legulcers. Eur J Vasc Endovasc Surg. 2006;31:306-310.38. Lees M, Taylor DJ, Woolley DE. Mast cell proteinases activateprecursor forms of collagenase and stromelysin, but not of gelati-nases A and B. Eur J Biochem.1994;223:171-177.39. Liu Z, Zhou X, Shapiro SD, et al. The serpin alpha1-proteinaseinhibitor is a critical substrate for gelatinase B/MMP-9 in vivo.Cell. 2000;102:647-655.40. Velasco G, Cal S, Merlos-Suarez A, et al. Human MT6-matrixmetalloproteinase: identification, progelatinase A activation, andexpression in brain tumors. Cancer Res. 2000;60:877-882.41. Norgauer J, Hildenbrand T, Idzko M, et al. Elevated expres-sion of extracellular matrix metalloproteinase inducer (CD147)and membrane-type matrix metalloproteinases in venous leg ul-cers. Br J Dermatol. 2002;147:1180-1186.42. Shields DA, Andaz SK, Abeysinghe RD, Porter JB, Scurr JH,Coleridge-Smith PD. Plasma lactoferrin as a marker of white cell

tients. J Thromb Thrombolysis. 2004;17:207-211.47. Asanuma K, Magid R, Johnson C, Nerem RM, Galis ZS. Uni-axial strain upregulates matrix-degrading enzymes produced byhuman vascular smooth muscle cells. Am J Physiol Heart CircPhysiol. 2003;284:H1778-H1784.48. Kaunas R, Nguyen P, Usami S, Chien S. Cooperative effects ofRho and mechanical stretch on stress fiber organization. ProcNatl Acad Sci U S A. 2005;102:15895-15900.49. Sansilvestri-Morel P, Rupin A, Badier-Commander C, et al.Imbalance in the synthesis of collagen type I and collagen type IIIin smooth muscle cells derived from human varicose veins. J VascRes. 2001;38:560-568.50. Miller AP, Feng W, Xing D, et al. Estrogen modulates inflam-matory mediator expression and neutrophil chemotaxis in injuredarteries. Circulation. 2004;110:1664-1669.
degranulation in venous disease. Phlebology. 1994;9:55-58.43. Sansilvestri-Morel P, Rupin A, Jullien ND, et al. Decreasedproduction of collagen Type III in cultured smooth muscle cellsfrom varicose vein patients is due to a degradation by MMPs: pos-sible implication of MMP-3. J Vasc Res. 2005;42:388-398.44. Rosario HS, Waldo SW, Becker SA, Schmid-Schönbein GW.Pancreatic trypsin increases matrix metalloproteinase-9 accu-mulation and activation during acute intestinal ischemia-reper-fusion in the rat. Am J Pathol. 2004;164:1707-1716.45. Vaalamo M, Mattila L, Johansson N, et al. Distinct populationsof stromal cells express collagenase-3 (MMP-13) and collagenase-1(MMP-1) in chronic ulcers but not in normally healing wounds.J Invest Dermatol.1997;109:96-101.46. Ercan E, Tengiz I, Duman C, et al. Decreased plasminogenactivator inhibitor-1 levels in coronary artery aneurysmatic pa-
126 Triggering mechanisms of venous valve incompetence – Schmid-SchönbeinMEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
MÉCANISMES DÉCLENCHANTL’INCONTINENCE VALVULAIRE VEINEUSE
L es mécanismes conduisant à la cascade d’événements associés à l’in-flammation aseptique au cours de l’insuffisance veineuse chronique sontles facteurs de risque génétiques, l’imprégnation hormonale, la pression
hydrostatique prolongée et la contrainte liquide de cisaillement anormale. L’in-flammation se manifeste par l’activation endothéliale, l’adhésion leucocytaireà l’endothélium et la migration dans les tissus, la dégranulation des mastocyteset l’infiltration des monocytes et des T-lymphocytes avec transformation desmacrophages. Les fibroblastes ciblent la matrice extracellulaire ainsi que lescellules parenchymateuses, et produisent un ensemble de métabolites et de mé-diateurs inflammatoires, de molécules d’adhésion des membranes cellulaires,de récepteurs prothrombotiques, de facteurs de croissance et d’agents chimio-tactiques. La cascade inflammatoire sert de façon fondamentale comme mé-canisme de réparation tissulaire. Cependant, en cas d’insuffisance veineusechronique associée au développement d’une incontinence valvulaire, l’inflam-mation ne résoud pas et au contraire conduit à des manifestations cliniquespouvant aller de la présence de varicosités à d’éventuels ulcères. Les facteursdéclenchant l’inflammation dans l’insuffisance veineuse chronique restent en-core incertains.

Types of inheritance: the hypotheses
Predisposing factors play a currently well-rec-ognized role in varicose veins. The clinicalconsensus is that primary varicose disease is
probably genetic in origin. As early as 1851, RudolfVirchow (1821-1902) observed an excess of familycases, and in 1868, the pedigrees of two affectedfamilies were reported. However, nongenetic fac-tors probably play an important modulating role,compounding the task of analysis. Late onset is en-tirely compatible with a genetic origin, as has beenshown in other common diseases (eg, familial atri-oventricular block).1 The few twin studies provideadditional information: what data are available showmarkedly higher concordance rates in monozygot-ic twins (75%) than in dizygotic twins (52%), al-though the difference is not statistically significantgiven the small sample size.2 Impedance plethys-mography of venous distensibility in twins has alsorevealed that heredity plays an important role.3
The genetic factor thus appears to weigh heavily,but its nature remains unelucidated. What is themode of transmission? Clues from family tree stud-ies point to different types of inheritance: some ear-ly investigators suggested an autosomal dominantmode of transmission,4-6 whereas others reportedfindings more consistent with recessive transmis-sion.7-9 It may therefore be that mode of transmis-sion differs between families. Indeed, in 1969, Haugeand Gundersen10 proposed a polygenic inheritancehypothesis, based on cooperation between a num-ber of independent genes each having minor patho-genic effect, but which collectively, when presentin sufficient numbers, resulted in varicose vein dis-ease, just as in other common diseases in which in-heritance plays a major role. The literature on vari-cose vein inheritance allows little in the way ofrobust conclusions, given the numerous forms ofbias in data collection depending on the diagnosticcriteria used, the population selected, and whetherdata about previous family members have been ob-tained by questioning the patient or by examiningthe relative concerned. The reference study by Cor-nu-Thénard et al was based on 134 families whosemembers were examined.11 Even if the multifacto-rial hypothesis readily accounts for a large num-ber of family patterns, this does not mean that thisis the actual mode of transmission. In 1998, a Chi-nese study attempted a conclusive breakdown ofmodes of varicose disease transmission:12 nuclearfamily analysis was consistent with dominant auto-somal transmission with 70% to 92% penetrance;other pedigrees were consistent with autosomal re-cessive transmission, and 37% of cases were spo-radic. These family transmission studies are fun-damental because they inform molecular geneticstrategy, which can be either direct or indirect.
127Venous valve incompetence: the role of genetic factors – Pistorius MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
T he role of inheritance in primary varicose veins is now well recognized,although uncertainty persists as to the type of inheritance involved. Clearunderstanding of the mode of transmission is essential in informing ge-
netic research strategy. When the disease mechanism is known, direct meth-ods can be used, but this does not apply to varicose veins; indirect methods mustbe used instead. As in other common diseases, several types of inheritance maybe involved. In some families, transmission is dominant, strongly expressed,and with a homogeneous phenotype. In such cases, a reverse genetic techniquecan be applied known as linkage analysis, based on the study of large families.We have used this to identify several loci potentially related to varicose veins,but despite the presence of candidate genes within these regions of interest,we have not yet identified a mutation within these families. At the same time,other methods of investigation (transcription products of tissue samples, differ-ential expression studies using deoxyribonucleic acid chips) may help to identifynew candidate genes. However, in most cases, the mode of segregation appearsnonMendelian, and associated with the environmental factors traditionallydescribed. This suggests polygenic or multifactorial inheritance. The molec-ular genetic techniques that can be used to identify one or more susceptibilitygenes are more complex (sib-pair and association methods) and require a largenumber of samples.Medicographia. 2008;30:127-130. (see French abstract on page 130)
Keywords: extracellular matrix; genetics; inheritance; smooth muscle cell;transmission; varicose vein disease
Marc A. PISTORIUS, MDDepartment of Vascular MedicineCentre Hospitalier Universitaire de Nantes Hôtel-Dieu Nantes, FRANCE
Address for correspondence: Prof Marc Pistorius, Médecine Vasculaire, CHU Hôtel-Dieu, F-44000 Nantes, France(e-mail: [email protected])
Venous valve incompetence: the roleof genetic factors b y M . A . P i s t o r i u s , F r a n c e
SELECTED ABBREVIATIONS AND ACRONYMS
ECM extracellular matrixMMP matrix metalloproteinaseSMC smooth muscle cell

cules,31 leading to valvular and vein wall infiltra-tion by mononuclear cells (monocytes and mastcells), which in turn are responsible for the pro-duction of growth factors, including transforminggrowth factor β1 (TGFβ1).32,33 TGFβ1 is an impor-tant modulator of MMP/TIMP balance and is actu-ally involved in the regulation of cellular apoptosisand proliferation, a pivotal element in vascular re-modeling. Several studies have in fact documentedinhibition of apoptosis in varicose wall myocytes.34,35
Many variations have been described in the ex-pression of various proteins in varicose vein disease,but differential gene expression has been less stud-ied. Nevertheless, certain recently targeted abnor-malities deserve our attention: what is the impactof variations in the repeated nucleotide sequencesmodulating the expression of structural genes (eg,for connective tissue and elastic tissue) in the de-velopment of primary varicose veins?36 What is therole of the transcriptional changes in vascular en-dothelial growth factor (VEGF) and its receptors,37
or of the mutations recently identified in the genecoding for forkhead box C2 (FOXC2), a transcrip-tion factor specifically involved in valve develop-ment and maintenance?38 Other mutations or poly-morphisms of candidate genes have been describedin the literature: MMP3 (stromelysin-1) polymor-phism,39 the spondin 1 gene,40 or the thrombomod-ulin gene promoter,41 although with no conclusive-ly identified pathophysiological implications. Eachof these molecular targets represents a potentialline of research, such as in functional SMC studies(messenger ribonucleic acid, proteins), or compar-ative studies between varicose and healthy veins,whether of differential ECM and SMC gene expres-sion or of the signaling pathways involved. Directstudy of the molecular mechanism(s) leading tovaricose veins thus offers multiple interesting leadsbut has limitations: what is the primary abnormal-ity? Is it single or multiple? Are we not too focusedon disruption of a secondary control system?
� Reverse geneticsWhen the pathophysiological mechanism behind acondition is unknown, we can use a reverse genet-ic approach that identifies a potential culprit geneby studying patients; once a gene is identified, wecan then elucidate the molecular mechanism be-hind the disease concerned. The multifactorial hy-pothesis accounts for a number of situations but,as in other common diseases, there also appear tobe other modes of transmission. Several molecularbiology strategies are complementary and thereforeneed to be conducted in parallel.
Bearing in mind the genetic heterogeneity seenin other common conditions, we cannot rule outthe involvement in certain families of a single ormajor gene with dominant effect, whose expressionis modulated by age and sex. Such families showa clearly dominant and strongly expressed mode oftransmission, with a strikingly homogeneous phe-notype.42 The reverse genetic technique of linkageanalysis can then be used.43 It is based on the studyof large data-rich families, with plenty of affected in-dividuals and healthy controls, stretching over sev-
Molecular genetic strategy
� Direct methodsDirect methods can be used if the pathophysiologyof a particular disease has been elucidated, as whenan abnormal protein is shown to have a direct patho-logical role, and gene sequencing identifies a mu-tation (eg, hereditary hemoglobinopathy). Suchmethods do not extrapolate to varicose veins, be-cause the molecular mechanism is complex and re-mains unelucidated. Numerous pathophysiologicalmechanisms have been described. Some investiga-tors have differentiated primary changes that beginin the vessel wall from those that begin in the valves.Such an approach appears oversimplistic, since thesituation is rarely unambiguous. Even if valve le-sions are recognized to be early and crucial eventsin varicose disease, more widespread changes havebeen identified in varicose patients, involving valveinsertions in the vein wall, changes in the vein wallitself, and even the skin.13 Varicosedisease is apatho-logical entity in its own right.14 It is not secondaryto physiological aging, but an instance of genuinevascular dysplasia, comprising disorganization ofthe vessel wall and a specific ratio of fibrillar tobasement membrane collagen that remains stableover time.15
The first and most visible changes to have beenidentified were abnormalities in extracellular ma-trix (ECM) metabolism, notably with a well-docu-mented imbalance between types I and III collagen.16
This dysregulation in connective tissue synthesisconcerns abnormalities in ECM remodeling, main-ly dependent on matrix metalloproteinases (MMPs)and tissue inhibitors of metalloproteinases (TIMP).17
Abnormalities of MMP expression have been iden-tified in varicose compared with control vessel wall:increased expression of MMP1, and decreased ex-pression of MMP9, each unevenly distributed withinthe wall and varying between varicose segments.18,19
MMP imbalance within the ECM (in particular withan accumulation of type I collagen and a decreasein type III collagen) is found in the varicose wall(myocytes), but also in the skin (fibroblasts),13,20 in-dicating a more general disorder of connective tis-sue synthesis in varicose patients.
After the ECM, the next most obvious abnormal-ities involve the smooth muscle cell (SMC) itself,given its major role in ECM metabolism. Manychanges, both morphological21 and functional,22-24
have been demonstrated in varicose SMC. In addi-tion, specific mutationsmay affect thecomplex, two-way, integrin pathway relationships between SMCand ECM, with major potential impact on remodel-ing of the ECM and reorganization of the SMC cyto-skeleton.25 More recently, the importance has beenemphasized of cell infiltration of the varicose wall,in particular by monocytes and macrophages.26-28
The detailed role of this inflammatory infiltrate invaricose vein remodeling has been elucidated: ve-nous hypertension induces a leukocytic and endo-thelial inflammatory cascade via a mechanism thatcombines valvular and vein wall hypoxia and slow-ing of blood flow (decreased shear stress).29,30 Thisinduces the expression of leukocyte adhesion mole-
128 Venous valve incompetence: the role of genetic factors – PistoriusMEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E

entity in terms of inheritance: isolated reticularvarices that remain stable despite several pregnan-cies have little in common with severe, early-onset,progressive great vein incompetence. Some fami-lies or twin pairs can show remarkable anatomicaland morphological concordance at the start of thedisease. It is also worth noting that the loci of in-terest that we have identified differ between fami-lies, which again indicates that the disease may begenetically heterogeneous.
On the other hand, in most of the population,clinical presentation is more polymorphous andvariable, and the number of family members affect-ed is low or quite low, making it impossible to con-clude that a single genetic abnormality is present,and even less that it is dominant. The mode of seg-regation appears nonMendelian, and associatedwith the environmental factors traditionally de-scribed. This suggests that inheritance is polygenic(involving major and minor genes) or multifacto-rial (involving environmental determinants). Themolecular genetic techniques available for identi-fying one or more susceptibility genes are morecomplex, but do not require a mode of transmissionto be specified in advance. Their main drawback liesin the number of samples needed for this kind ofanalysis (300 to 500, depending on the epidemio-logical and hereditary characteristics of the diseaseconcerned). Options include sib-pair and associa-tion methods.46 The sib-pair method screens genet-ic marker allele frequencies in affected and healthysibs for an imbalance, in one or more given mark-ers, between the expected theoretical frequenciesand those actually observed, to identify a locus(genome region) potentially related to the disease.Association methods screen markers close to select-ed candidate genes for a binding imbalance, or studymarker allele frequencies in affected and healthysubjects in small families (nuclear families). Thesecomplementary approaches are currently underdevelopment.
Conclusion
Despite its methodological limitations, genetic re-search heralds the time when we will eventuallyelucidate the process(es) leading to varicose dis-ease. This should enable us to identify subjects atrisk who could benefit from prevention, given thatvaricose disease is associated with some long andexpensive complications, but it should also enableus to explore new drug therapy avenues, or evenconsider gene therapy. �
eral generations. Linkage analysis is an indirectstatistical method based on two fundamental biolog-ical phenomena: meiotic recombination (ie, the in-tense exchange of chromosome segments at meio-sis), and the presence of polymorphic markersthroughout the genome (these are repeat sequencesthat vary in length between individuals and arefound at regular intervals throughout the genome).44
The analysis searches for a statistical relationshipbetween one of these markers and the culprit gene,reflected in the family tree by an affected pheno-type. The result, expressed as the logarithm of theodds (LOD) score, reflects the probability of a statis-tical linkage for each marker. The next step, whichis essential in pursuing the search for candidategenes, consists of recruiting new families in order tonarrow these broad regions of interest by determin-ing the shortest linkage interval shared by the dif-ferent families. Once narrowed to a minimum, theseregions of interest can be searched for candidategenes usingcomputerizeddatabases,using sequenc-ing to detect a mutation in one of them.
From theory to practice:our experience
In 2000, we began our study of six extended fami-lies in whom varicose disease segregated accordingto a strongly expressed autosomal dominant modeof transmission, with a particularly homogeneousphenotype and high penetrance.42 We have man-aged to identify several loci potentially associatedwith varicose disease, based on the phenocopy hy-pothesis (subjects with the same phenotype basedon a different genetic abnormality—a plausible hy-pothesis given the high frequency of the disease inthe general population) and the assumption of non-penetrance in some subjects (ie, carriers of the mu-tant gene who do not express the disease). However,despite the presence of candidate genes within theseregions of interest (genes involved in ECM metab-olism, such as those coding for TIMP2, spondin-1,elastases, integrins, and different types of collagen),we have not yet identified a mutation in our fam-ilies. Nor have our families shown the mutationspreviously cited in the literature.39-41 Alternatively,new candidate genes can be identified using paral-lel and complementary techniques, such as studiesof tissue sample transcription products36 or of dif-ferential expression using deoxyribonucleic acidchips.45 Varicose vein disease also appears to be het-erogeneous, both clinically and genetically. Likeothers, we consider it to be a highly heterogeneous
129Venous valve incompetence: the role of genetic factors – Pistorius MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
REFERENCES1. Schott JJ, Alshinawi C, Kyndt F, et al. Cardiac conduction de-fects associate with mutations in SCN5A. Nat Genet.1999;23:20-21.2. Niermann H. Eine studie uber den erblichkeitsgrad bei 89hautkrankheiten nach untersuchung von 370 zwillingspaaren[Twin dermatology: an inheritability study of 89 skin diseases in370 twin pairs]. In: Zwillingsdermatologie. Heidelberg, Germany:Springer-Verlag; 1964:32-33.3. Brinsuk M, Tank J, Luft FC, Busjahn A, Jordan J. Heritabilityof venous function in humans. Arterioscler Thromb Vasc Biol.2004;24:207-211.4. Curtius F. Untersuchungen über das menschliche Venensys-tem. I Mitteilung: Die hereditäre Aetiologie der menschlichen
Beinphlebektasien. II Mitteilung: Die allgemeine ererbte Venen-wanddysplasie (Status varicosus). III. Mitteilung. Septumvaricenund Oslersche Krankheit als Teilerscheinung allgemeiner ererb-ter Venenwanddysplasie (Status varicosus) [Studies on the hu-man venous system. I: The hereditary etiology of lower limb vari-cose veins in humans. II. General hereditary vein wall dysplasia(status varicosus). III. Septal varices and hereditary haemorrhag-ic telangiectasis as partial manifestations of general hereditaryvein wall dysplasia (status varicosus)]. Dtsch Arch Klin Med.1928;162:194-196 & 330-354.5. Arnoldi CC. The heredity of venous insufficiency. Danish MedBull. 1958;5:169-176.6. Matousek V, Prerovsky I. A contribution to the problem of the

130 Venous valve incompetence: the role of genetic factors – PistoriusMEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
33. Jacob T, Hingorani A, Ascher E. Overexpression of transform-ing growth factor-beta1 correlates with increased synthesis ofnitric oxide synthase in varicose veins. J Vasc Surg.2005;41:523-530.34. Ascher E, Jacob T, Hingorani A, Tsemekhin B, Gunduz Y. Ex-pression of molecular mediators of apoptosis and their role inthe pathogenesis of lower-extremity varicose veins. J Vasc Surg.2001;33:1080-1086.35. Urbanek T, Skop B, Wiaderkiewicz R, et al. Smooth musclecell apoptosis in primary varicose veins. Eur J Vasc EndovascSurg. 2004;28:600-611.36. Kim DI, Eo HS, Joh JH. Identification of differentially ex-pressed genes in primary varicose veins. J Surg Res. 2005;123:222-226.37. Hollingsworth SJ, Powell G, Barker SG, Cooper DG. Primaryvaricose veins: altered transcription of VEGF and its receptors(KDR, flt-1, soluble flt-1) with sapheno-femoral junction incom-petence. Eur J Vasc Endovasc Surg. 2004;27:259-268.38. Mellor RH, Brice G, Stanton AWB, et al. Mutations in FOXC2are strongly associated with primary valve failure in veins of thelower limb. Circulation. 2007;115:1912-1920.39. Dunleavey L, Beyzade S, Ye S. Rapid genotype analysis of thestromelysin gene 5A/6A polymorphism. Atherosclerosis. 2000;151:587-589.40. Terai Y, Miyamoto K, Koike M, et al. Vascular smooth musclecell growth-promoting factor/F-spondin inhibits angiogenesisvia the blockade of integrin αVβ3 on vascular endothelial cells.J Cell Physiol. 2001;188:394-402.41. Le Flem L, Mennen L, Aubry ML, et al. Thrombomodulinpromoter mutations, venous thrombosis, and varicose veins. Ar-terioscler Thromb Vasc Biol. 2001;21:445-451.42. Pistorius MA. Chronic venous insufficiency: the genetic in-fluence. Angiology. 2003;54(suppl 1):S5-S12.43. Lathrop GM, Lalouel JM. Easy calculations of lod scores andgenetic risks on small computers. Am J Hum Genet. 1984;36:460-465.44. Dib C, Faure S, Fizames C, et al. A comprehensive genetic mapof the human genome based on 5,264 microsatellites. Nature.1996;380:152-154.45. Lee S, Lee W, Choe Y, et al. Gene expression profiles in vari-cose veins using complementary DNA microarray. DermatolSurg. 2005;31:391-395.46. Kruglyak L, Lander ES. Complete multipoint sib-pair analysisof qualitative and quantitative traits. Am J Hum Genet.1995;57:439-454.
inheritance of primary varicose veins. Hum Hered.1974;24:225-235.7. Troisier J, Le Bayon H. [Genetic study of varices]. Ann Med.1937;41:30-41.8. Florian J. [Varicose vein disease, a hereditary clinical entity].Rev Med.1966;9:518.9. Salleras V. [Heredity and varicose disease]. Rev Med.1966;9:463-464.10. Hauge M, Gundersen J. Genetics of varicose veins of the low-er extremities. Hum Hered.1969;19:573-580.11. Cornu-Thénard A, Boivin P, Baud JM, De Vincenzi I, Carpen-tier PH. Importance of the familial factor in varicose disease.Clinical study of 134 families. J Dermatol Surg Oncol.1994;20:318-326.12. Guo Q, Guo C. [Genetic analysis of varicose vein of lowerextremities]. Chung Hua I Hsueh I Chuan Hsueh Tsa Chih.1998;15:221-223.13. Sansilvestri-Morel P, Rupin A, Jaisson S, et al. Synthesis ofcollagen is dysregulated in cultured fibroblasts derived from skinof subjects with varicose veins as it is in venous smooth musclecells. Circulation. 2002;106:479-483.14. Milroy CM, Scott DJ, Beard JD, Horrocks M, Bradfield JW.Histological appearances of the long saphenous vein. J Pathol.1989;159:311-316.15. Maurel E, Azema C, Deloly J, Bouissou H. Collagen of thenormal and the varicose human saphenous vein: a biochemicalstudy. Clin Chim Acta.1990;193:27-37.16. Venturi M, Bonavina L, Annoni F, et al. Biochemical assay ofcollagen and elastin in the normal and varicose vein wall. J SurgRes.1996;60:245-248.17. Badier-Commander C, Verbeuren T, Lebard C, Michel JB,Jacob MP. Increased TIMP/MMP ratio in varicose veins: a possibleexplanation for extracellular matrix accumulation. J Pathol.2000;192:105-112.18. Gillespie DL, Patel A, Fileta B, et al. Varicose veins possessgreater quantities of MMP-1 than normal veins and demonstrateregional variation in MMP-1 and MMP-13. J Surg Res. 2002;106:233-238.19. Woodside KJ, Hu M, Burke A, et al. Morphologic character-istics of varicose veins: possible role of metalloproteinases. J VascSurg. 2003;38:162-169.20. Sansilvestri-Morel P, Fioretti F, Rupin A, et al. Comparison ofextracellular matrix in skin and saphenous veins from patientswith varicose veins: does the skin reflect venous matrix changes?Clin Sci. 2007;112:229-239.21. Kockx MM, Knaapen MW, Bortier HE, Cromheeke KM,Boutherin-Falson O, Finet M. Vascular remodeling in varicoseveins. Angiology. 1998;49:871-877.22. Rizzi A, Ouaglio D, Vasquez G, et al. Effects of vasoactiveagents in healthy and diseased human saphenous veins. J VascSurg.1998;28:855-861.23. Boittin FX, Coussin F, Macrez N, Mironneau C, Mironneau J.Inositol 1,4,5-trisphosphate- and ryanodine-sensitive Ca2+ releasechannel-dependent Ca2+ signalling in rat portal vein myocytes.Cell Calcium.1998;23:303-311.24. Carey JD. Control of growth and differentiation of vascularcells by extracellular matrix proteins. Ann Rev Physiol.1991;53:161-177.25. Boudreau NJ, Jones PL. Extracellular matrix and integrinsignalling: the shape of things to come. Biochem J.1999;339:481-488.26. Takase S, Lerond L, Bergan J, Schmid-Schönbein GW. Theinflammatory reaction during venous hypertension in the rat.Microcirculation. 2000;7:41-52.27. Pascarella L, Schmid-Schönbein GW, Bergan J. An animalmodel of venous hypertension: the role of inflammation in ve-nous valve failure. J Vasc Surg. 2005;41:303-311.28. Bergan J. Molecular mechanisms in CVI. Ann Vasc Surg.2007;21:260-266.29. Fukuda S, Yasu T, Predescu DN, Schmid-Schönbein GW.Mechanisms for regulation of fluid shear stress response in cir-culating leukocytes. Circ Res. 2000;86:E13-E18.30. Nicolaides AN. Chronic venous disease and the leukocyte-endothelium interaction: from symptoms to ulceration. Angiol-ogy. 2005;56(suppl 1):S11-S19.31. Saharay M, Shields DA, Porte JB, Scurr JH, Coleridge-SmithPD. Leukocyte activity in the microcirculation of the leg in pa-tients with chronic venous disease. J Vasc Surg.1997;26:265-273.32. Boisseau MR, de La Giclais B. Chronic venous disease: rolesof various pathophysiological factors. Clin Hemorheol Micro-circ. 2004;31:67-74.
L’INCONTINENCE VALVULAIRE VEINEUSE :LE RÔLE DES FACTEURS GÉNÉTIQUES
L’ importance de l’hérédité dans l’origine des varices primitives est actuel-lement admise. Des incertitudes persistent cependant concernant le typed’hérédité en cause. Une bonne connaissance du mode de transmission
est cependant indispensable car cette étape guide la stratégie de recherche gé-nétique. Les méthodes directes peuvent être appliquées lorsque le mécanismed’une maladie est connu, ce qui n’est pas le cas de la maladie variqueuse. Le re-cours aux méthodes indirectes s’impose. Comme dans d’autres maladies com-munes, plusieurs modes d’hérédité semblent exister. On observe en effet danscertaines familles une transmission de type dominant, avec une expressionforte et un phénotype homogène. On peut alors appliquer une technique degénétique inverse appelée « analyse de liaison », menée à partir de l’étude degrandes familles. Elle a permis d’identifier plusieurs locus potentiellement liésà la maladie variqueuse ; cependant, malgré la présence de gènes candidats ausein de ces régions d’intérêt, aucune mutation n’a été identifiée pour l’instantau sein de ces familles. Parallèlement, d’autres méthodes d’investigation (pro-duits de transcription à partir de prélèvements tissulaires, étude de l’expressiondifférentielle sur puces à DNA), sont actuellement en cours et peuvent contri-buer à identifier de nouveaux gènes candidats. Cependant, dans la majorité descas, le mode de ségrégation semble non mendélien, associé aux facteurs en-vironnementaux classiquement décrits. Ceci fait appel aux notion d’héréditépolygénique ou multifactorielle. Les méthodes de génétique moléculaire quel’on peut mettre en œuvre pour identifier un ou plusieurs gènes de prédisposi-tion sont plus complexes (méthode des « sib-pairs », méthode d’association) etnécessitent un grand nombre d’échantillons.

gy, or pharmacogenotherapy. This is clearly the fu-ture, yet today, state-of-the-art treatment in venousdisease mirrors that of gastric surgery 25 years ago,when gastric resection was the method of choicefor all patients with a peptic ulcer. I do not know ifour achievement in the next 25 years within the ve-nous field will be comparable to that achieved ingastric and duodenal ulcer therapy, but certainlyour patients will expect us to make much biggerprogress in the avoidance of surgery and the im-provement of varicose vein treatment to make it
Improving the management of chronic venousdisorders is a timely topic, and our knowledge ofthe disease remains incomplete. This is acknowl-
edged by many experts in venous disease world-wide.1 With this in mind, I will attempt to establisha parallel in this paper between research and ad-vances in peptic ulcer disease and those in chronicvenous disease. The idea is to demonstrate that to-day, we have become “reflux hunters,” but the caus-es of diseased veins most probably lie elsewhere, andmight be approached via genetics, molecular biolo-
131Evolution of treatment of venous valve incompetence compared with peptic ulcer disease – Jawien MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
Arkadiusz JAWIEN, MDKlinika Chirurgii OgolnejBydgoszcz, POLAND
Address for correspondence: Prof Arkadiusz Jawien, Szpital Wojewodzki, SP ZOZ, Klinika Chirurgii Ogolnej, ul. Ujejskiego 75, 85-168 Bydgoszcz, Poland(e-mail: [email protected])
Treatment of venous valve incompetence:
past, current, and future A reflection on its evolution in
comparison with peptic ulcer diseaseb y A . J a w i e n , P o l a n d
T he aim of this article is to establish a parallel between thedramatic evolution of treatment for peptic ulcer disease andthat of refluxing veins. Treatment of acid peptic disease has
involved a series of attempts to control gastric acid secretion inorder to heal and prevent recurrence of duodenal ulcers. Likewise,it is believed that repair of refluxing valves and even more pre-vention of valve damage are the future of chronic venous diseasetreatment. To come back to acid peptic disease, surgeons likePean, Rydygier, and Billroth began performing gastric resectionsin the second half of the 19th century. In 1943, the first truncalvagotomy was performed to limit cholinergic stimulation of gas-tric acid secretion. This led to surgery that combined gastric re-sections with vagotomy. In 1970, the first microsurgical techniquewas performed, consisting of parietal cell vagotomy. This was ableto limit vagal initiation of acid secretion, while minimizing theimpact on other gastrointestinal functions. By the 1960s, phar-macological intervention included antacids to neutralize acid,and anticholinergics to reduce the amount of acid produced. In1976, treatment of acid peptic disease began a new phase, withthe introduction of the first H2 receptor antagonist. Since 1982,the discovery of Helicobacter pylori has dramatically altered therole of surgery in the management of peptic ulcer disease. In mostcases, medical treatment is undertaken with the use of specificdrugs aimed at managing Helicobacter pylori and acid secretion,and interventional methods are mostly reserved for the treatmentof ulcer perforation. Today, surgeons are left only with surgical
treatment of gastric ulcer complications (eg, perforations, bleed-ing, or neoplasmatic transformation of gastric ulcers). With re-gard to management of venous disease, a similar evolution overtime has been seen. For years, the method used for the elimi-nation of superficial refluxes has been the stripping of the veins inwhich the diseased valves were located. The high recurrence rateafter great saphenous vein surgery, together with the dramaticimprovement in the imaging of venous valves by means of sophis-ticated duplex scanning methods, has made it possible to recon-struct the diseased valve rather than remove it. The future re-mains to bedetermined in the fieldof venousdiseasemanagement.Strategies focused on the prevention of valve damage rather thanits reparation or resection might be envisaged. Similar to pepticulcer disease management, it is possible to contemplate that spe-cific drugs aimed at correcting genetic defects, reinforcing venoustone or preventing the inflammatory events that cause damageto the valves could replace current treatment methods.Medicographia. 2008;30:131-136. (see French abstract on page 136)
Keywords: acid peptic disease; venous valve incompetence; reflux; pharmacological intervention; proton pump inhibitor;progress

dor Billroth, performed a similar operation and lat-er introduced another type of gastric resection con-sisting of a gastroenterostomy with oversewing ofthe duodenal stump (known today as a Billroth IIgastric resection). Following the observation thatonly partial gastrectomy made a hyperacid stomachpermanently anacid, by the 1930s, the removal of66% to 75% of the distal stomach became the stan-dard operation for peptic ulcer disease.2
In addition to many other people, Dragstedt knewthat peptic ulcers were caused by excess acid in thestomach. Because of the known action of the vagusnerves on gastric secretion, in 1943, he performedthe first truncal vagotomy to limit cholinergic stim-ulation of gastric acid secretion. This operation re-duced 12-hour overnight gastric secretion by 50%to 60% in all patients. After Dragstedt’s introduc-tion of the vagotomy, it was simply a matter of timebefore it was combined with gastric resections.2
In the early 1900s, Edkins reported that an antralhormone, which he named gastrin, caused gastricresection. Further experiments in dogs showed that
antrectomy caused a marked reduction in gastricsecretion. In 1976, Herrington published the resultsof a large series of vagotomies and antrectomies,following which, a more conservative vagotomy wasperformed to prevent the nerves of the antrum andpylorus from being injured. In 1970, the first pari-etal cell vagotomy was performed. This microsur-gical technique limited vagal initiation of acid se-cretion, while minimizing the impact on othergastrointestinal functions.2
Today, surgery for intractable or chronic ulcerdisease is rarely necessary; as a consequence, suchcomplex procedures as vagotomy with antrectomyor highly selective vagotomy are virtually nonexis-tent. Surgery is now reserved for the treatment of
more pleasant and effective, and with less recur-rence. This raises the questions: what do we know,what do we not know, what should we know toprogress in the management of venous disease, andwhat can be contemplated in the near future to im-prove the management of our patients?
The history of peptic ulcer therapy
The history of the treatment of acid peptic diseasehas involved a series of attempts to control gastricacid secretion in order to heal gastric and duode-nal ulcers and prevent their recurrence (Figure 1).Gastric secretion is mediated by way of the vagusnerves, gastrin, and protein derivatives of the di-gestion process.
� Early treatmentEarly treatment attempted to heal the disease byneutralizing gastric acid with diet modification—the Sippy diet, and Doll’s milk drip. Just before theturn of the century, surgeons began performing gas-tric resections.
� Resection proceduresBlalock gave a very good review of the history ofpeptic ulcer surgery.2 On November 21, 1881, thePolish surgeon, Ludwik Rydygier (Figure 2), be-came the first to excise the pylorus of a 30-year-oldwoman with a gastric ulcer and successfully anas-tomose the stomach with the duodenum. This wasthe first successful gastric resection ever performedfor a gastric ulcer, and the patient lived for the next17 years without any clinical symptoms or signs. Atalmost the same time, an Austrian surgeon, Theo-
Figure 1. X-ray imageof a gastric ulcer.
Copyright © WellcomePhoto Library, Wellcome
Images, The Wellcome Trust.
132 Evolution of treatment of venous valve incompetence compared with peptic ulcer disease – JawienMEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
SELECTED ABBREVIATIONS AND ACRONYMS
CHIVA Conservative Hemodynamic treatment of Incompetent Varicose veins in Am-bulatory patients (French acronym)
DVR deep venous reflux
GSV great saphenous vein
PPI proton pump inhibitor
Figure 2. Professor Ludwik Rydygier, the pioneer ofstomach surgery, who performed the first successful gas-tric resection for a gastric ulcer in 1881. Oil on canvas,by the Polish painter Leon Wyczolkowski (1852-1936).

bleeding for intensive care patients, and should fa-cilitate healing in those with bleeding ulcers of theupper gastrointestinal tract.5 A great step forwardwas made when two Australian clinical researchers,Warren and Marshall, discovered spiral bacteria inthe stomach, named Helicobacter pylori (H. pylori)(Figure 4). They received the third Nobel prize inthe field of gastrology in the past century for thefinding that this bacterium is related to the patho-genesis of gastritis and peptic ulcer.6 They docu-mented that the eradication of H. pylori from thestomach, using antibiotics and potent gastric in-hibitors, not only accelerates healing of the ulcerbut also prevents its recurrence, a finding consid-ered to be the greatest practical discovery in gas-trology during the last century. Thus, the outstand-ing achievements in gastroenterology during thelast century have resulted in three Nobel prizes andhave been appreciated by millions of ulcer patientsall over the world. Infection with H. pylori caus-es most duodenal ulcers (95%) and gastric ulcers(70%). It is also likely to cause around 9% of dys-pepsia cases in which no ulcers are detected.7
The dramatic success of pharmacological acidsuppression in the healing of peptic ulcers and themanagement of patients with gastroesophageal re-flux disease has been reflected in the virtual aboli-tion of elective surgery for ulcer disease, a reductionin nonsteroidal anti-inflammatory drug–associatedgastropathy, and the decision by most patients withreflux symptoms to continue medical therapy ratherthan undergo surgical intervention.8 The latter iscurrently reserved only for gastric ulcer complica-tions, namely perforation, bleeding, and neoplas-matic transformation of a gastric ulcer.
A number of challenges remain in the manage-ment of acid-related disorders, however, and a num-ber of new drugs are currently being investigatedto provide a significant advance on current treat-ments. Some of them (namely, potassium-compet-itive acid blockers and cholecystokinin 2 [CCK2]–
complications of the acute ulcer (eg, bleeding, per-foration, and obstruction).3 Regarding duodenal ul-cer perforation, the most common operative treat-ment is an omental (Graham) patch. More definitivemanagement is rarely necessary.
� Pharmacological interventionProgress in gastroenterological research over thepast century started as a consequence of the discov-eries by Prout in the early 18th century of the pres-ence of inorganic hydrochloric acid in the stomachand Pavlov at the end of the 19th century of the neu-roreflex stimulation of its secretion, for which hewas awarded the Nobel prize in 1904. The discoveryof H2 receptor antagonists by Black (Figure 3) andtheir usefulness in the control of gastric secretionand ulcer healing, was a real breakthrough both forthe elucidation of gastric secretory mechanisms andfor ulcer therapy. He was awarded the Nobel Prizefor this discovery, which opened the path to phar-macological intervention for gastric ulcers.
By the 1960s, pharmacological intervention in-cluded antacids to neutralize acid and anticholiner-gics to reduce the amount of acid produced. Thesetreatments varied in their effectiveness, and some ofthem caused significant side effects. In 1976, treat-ment of acid peptic disease began a new phase, withthe introduction of the first H2 receptor antagonist,cimetidine, which partially suppresses basal andmeal-stimulated acid secretion. Ranitidine, the sec-ond H2 receptor antagonist, produced greater acidsuppression capable of inducing an intragastric pHlevel greater than 3, lasting for approximately 10hours per day when given twice daily at recom-mended doses. This level of acid suppression canfacilitate the healing of duodenal ulcers, but haslimited efficacy for other indications (eg, gastroin-testinal bleeding). The knowledge that there is a cir-cadian pattern in acid production, with higher lev-els between 10 PM and 2 AM, further resulted in thedevelopment and use of a single evening dose ofranitidine.4
Research continued to be carried out to inves-tigate the effects of dose timing and the influenceof more potent acid-suppressing agents. In thelate 1980s, a more potent class of acid-suppressingagents was developed, the proton pump inhibitors(PPIs). PPIs can induce an intragastric pH above 3that lasts for approximately 17 hours per day, andan intragastric pH above 5 that lasts for approxi-mately 9 hours per day after once-daily oral admin-istration of recommended doses. It is possible to at-tain even higher target pH values with large dosesand with continuous intravenous infusion. Thus,PPIs are the agents of choice for the treatment ofmany acid-related disorders, including peptic ulcerdisease and moderate-to-severe gastroesophagealreflux disease, and for prevention of rebleeding inpatients with upper gastrointestinal bleeding. Avail-ability of an intravenous formulation, pantoprazole,enables hospitalized patients for whom oral admin-istration is not feasible to benefit from the superiorpotency of PPIs. It was suggested that intravenousPPIs may be more effective than H2 receptor an-tagonist prophylaxis against stress-related ulcer
133Evolution of treatment of venous valve incompetence compared with peptic ulcer disease – Jawien MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
Figure 3. Sir James W.Black, who developed thefirst clinically useful H2receptor antagonist,cimetidine, for the treat-ment of gastric ulcer.Copyright © The NobelFoundation.
Figure 4. Helicobacter pylori, discovered in the early1980s by Robin Warren and Barrie Marshall to be thecause of the majority of gastric and duodenal ulcers viainfection of the lower stomach and upper duodenum.Copyright © 2006, Australian Academy of Science.

procedures, endovenous ablation was developed inthe 1990s. This procedure was found to be safe andeffective in eliminating the GSV from the venouscirculation. The two currently available methodsused to achieve ablation of the GSV are the Closure®
procedure using a radiofrequency catheter and gen-erator, and endovenous laser ablation using a laserfiber and generator (Figure 6). Both systems useelectromagnetic energy to destroy the GSV in situ.
We are presently lacking follow-up data to verifywhether these endovenous procedures lead to lessneovascularization than open surgery, but patientacceptance of these minimally invasive proceduresis overwhelmingly better than with stripping. Inthis regard, one can say that a step forward has beenmade in the treatment of venous insufficiency, withless invasive methods that are more comfortablefor patients.
� Valve repair in superficial and deep venous insufficiencySpecialists in venous disease dreamt of a valve re-pair or valve restoration process that could spare thevein itself, much like the patches that were devel-oped for perforation of duodenal ulcers. Direct andindirect restoration of valve function was eventu-ally performed.
Methods for indirect valve function restorationall have in common the fact that they preserve thesaphenous trunk and restore its valve function viamodification of the hemodynamics. ConservativeHemodynamic treatment of Incompetent Varicoseveins in Ambulatory patients (CHIVA) is a techniquethat seeks to normalize venous pressure by ligationof points of venous reflux at re-entry perforators.9
High ligation plus tributary phlebectomy plus/mi-nus a perforator ablation procedure was first report-ed by Hammarsten, and was only used for treatingGSV insufficiency. The CHIVA procedure was laterfurther developed and popularized by Franchesci,Zamboni, and Cappelli (see article by Perrin in thecurrent issue). Another vein-sparing technique isexternal banding, which aims to restore proximalvalvular competence of the GSV. These proceduresare not widely practiced, however.
For deep venous insufficiency, the goal is to cor-rect the deep venous reflux (DVR) at the subin-guinal level. This reflux leads to a permanent in-crease in venous pressure, unaffected by the activityof the calf venomuscular pump. But it must be keptin mind that DVR is frequently combined with su-perficial and perforator reflux, consequently allthese mechanisms have to be corrected in order toreduce the permanent increased venous pressure.Several methods are used: internal valvuloplasty,venous segment transfer, vein valve transplantation,neo valve, and allograft. All these methods are asso-ciated with phlebectomy, while valvuloplasty andpercutaneous placed devices do not need associat-ed phlebectomy.
� Chemical interventions: sclerotherapyUntil now, chemical intervention has been limitedto liquid and foam sclerotherapy. Liquid sclerother-apy is mostly used in the treatment of telangiec-
receptor antagonists) have already reached theclinical testing stage, while others (for instance, theantigastrin vaccine, H3-receptor ligands, and gas-trin-releasing peptide receptor antagonists) are stillin preclinical development, requiring proof-of-con-cept in human beings. Of the current approachesto acid secretion reduction, potassium-competitiveacid blockers and CCK2-receptor antagonists cer-tainly hold the greatest promise, with several com-pounds already in clinical trials.
A parallel with the treatment of superficial venous valve incompetence
The aim of treatment in chronic venous disease isto eliminate sources of venous hypertension.9
� Resection of the diseased superficial veinIn superficial venous insufficiency, the aim of treat-ment is to suppress reflux in the superficial diseasedveins (varicose veins).10 Reflux in superficial veins ismostly responsible for venous hypertension. Until10 years ago, the usual way to suppress reflux in dis-eased superficial veins was the following: first, sup-press leakage points in the deep venous network
that could be responsible for reflux in the superfi-cial system; next, strip pathologic superficial veins,either by stripping the great saphenous vein (GSV)of the thigh or at the other end of the spectrum,stripping the entire saphenous vein from the ankleto the groin, along with stab avulsion of varices. InFrance, the two most performed procedures in 2001were high ligation plus saphenous trunk strippingand tributary stab avulsion (71.9%), and high liga-tion plus saphenous trunk stripping (17.3%).11 Bycontrast, in the USA, high ligation alone at thesaphenofemoral junction has been widely practiced.9
Thus, type of procedures varied greatly dependingon countries and the dominant thinking amongphlebologists and surgeons. For a long time anduntil recently, saphenofemoral ligation (Figure 5)associated with stripping of the GSV was consideredthe best procedure to achieve the goal of suppress-ing reflux in the superficial system.
Recurrent varicose veins after surgery are ac-knowledged to be a major problem for patients andsociety. In an attempt to perform less bloody surgery
134 Evolution of treatment of venous valve incompetence compared with peptic ulcer disease – JawienMEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
Figure 5. Incision in thegroin crease with exposure
of the great saphenous vein(ligature surrounds it)at the saphenofemoral
junction.Reproduced from reference 12:
Goldman MP, Bergan JJ, Guex JJ,eds. Role of surgery in treatment of
varicose veins. In: SclerotherapyTreatment of Varicose and
Telangiectatic Leg Veins, 4th ed.Philadelphia, Pa: Mosby Elsevier;
2007:285-306. Copyright© 2007, Elsevier Inc.

terms of fundamental research. Recent studies inchronic venous disease have illuminated our un-derstanding of the underlying mechanisms re-sponsible for the progression of such disease tothe extent that it was useful for us to review cur-rent knowledge, with particular regard to the rolesof the key players namely the leukocyte, its in-flammatory products, and biomechanical factors.
It appears that inflammatory processes involvingleukocyte/endothelial interactions, triggered large-ly in response to abnormal venous flow, are im-portant in causing the adverse changes in venousvalves and vein walls. Elevated venous pressure andchanges in shear stress are involved in the controlof inflammatory reactions in endothelial cells andcirculating leukocytes. Decreased shear stress mod-ifies gene expression at the endothelial surface,promoting an inflammatory endothelial phenotype.Normal shear stress prevents leukocyte adhesion tovalves, while inflammatory mediators suppress theresponse of leukocytes to shear stress. Thus the in-teraction between leukocytes and valve endotheli-um is facilitated. Inflammation unmasks cell adhe-sion molecules at the surface of the endothelium,promoting leukocyte adhesion to the endothelium.In addition, chronic venous disease patients have atendency for systematically elevated leukocyte ad-hesion.14
The practical purpose of elucidating the molec-ular steps involved in the development of valve le-sions is to intervene with a targeted treatment. Thesequence of leukocyte adhesion, endothelial inter-action, activation, and migration, and its associa-tion with valvular damage, has focused attention onavailable molecules with known activity to modifythis chain of events. It is high time we stopped ourrole as venous reflux hunters and became wise, mod-ern pharmacogeno-healers, armed with new molec-ular biology and nanotechnology tools. Let us hopethat this will be realized in the coming years. �
tases. The results of such treatment for saphenousvein insufficiency have been disappointing andlong-term results are missing. Ultrasound-guidedsclerotherapy with foam can be considered as a newtreatment for varicose veins.9 The principle of scle-rosing agents is that they produce a lesion of thevenous wall, predominantly of the endothelium.Venous spasm is observed within minutes, and is as-sociated with endothelial cell destruction. The earlyresults seem to be very promising, but again, thereare few studies assessing the long-time results. Nev-ertheless, at least in Europe, the ultrasound-guidedsclerotherapy with foam has dramatically reducedthe number of varicose vein surgical operations andhas opened the door to minimally invasive, highlyeffective treatment that can replace saphenecto-my and eliminate reflux in the superficial venoussystem.
Conclusion
If dramatic progress has been made over the lastdecade in the treatment of venous insufficiency,moving from open surgery to minimally invasiveinterventions, a great step remains if we are to ac-complish an advance that is comparable with thatachieved in the treatment of peptic ulcers. This is inlarge part due to a lack of research into the funda-mental mechanisms of chronic venous disease pro-gression. As says Professor John Bergan, the firstauthor of an outstanding review on chronic venousdisease:14
It is an unfortunate fact that research interestand funding attracted by chronic venous diseasehas been in inverse proportion to its prevalenceand socioeconomic burden. It has enormous ca-pacity to impair the quality of patients’ lives, mild-ly in most cases, moderately in many, and severe-ly in the cases of the significant number with legulceration. This state of affairs is unwarranted,not simply for humanitarian reasons, but also in
135Evolution of treatment of venous valve incompetence compared with peptic ulcer disease – Jawien MEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
Greatsaphenousvein
Saphenous femoraljunction
Saphenous femoraljunction Digital compression
A B
Femoralvein
Withdrawfiber andsheath
Femoralvein
Aimingbeam
Figure 6. Endovenous laser treatment. A. Fiber optic starting position, before applying laser energy and withdraw-ing, in the great saphenous vein. B. Catheter and fiber withdrawal in pulsed mode.Reproduced from reference 13: Goldman MP, Bergan JJ, Guex JJ, eds. Intravascular approaches to the treatment of varicose veins: radio-frequency and lasers. In: Sclerotherapy Treatment of Varicose and Telangiectatic Leg Veins, 4th ed. Philadelphia, Pa: Mosby Elsevier; 2007:307-316. Copyright © 2007, Elsevier Inc.

136 Evolution of treatment of venous valve incompetence compared with peptic ulcer disease – JawienMEDICOGRAPHIA, VOL 30, No. 2, 2008
T H E V E N O U S V A L V E A N D P R I M A R Y C H R O N I C V E N O U S D I S E A S E
REFERENCES1. Padberg FT. Improving the management of chronic venousdisorders: exploration, description, and understanding. Parallelsin the worlds of the Renaissance and the American Venous Fo-rum. J Vasc Surg. 2005;41:355-365.2. Blalock J. History and evolution of peptic ulcer surgery. AmJ Surg. 1981;141:317-322.3. Ramsay Camp E, Hochwald SN. Gastroduodenal procedures.Available at: http://www.medscape.com. Accessed September 17,2007.4. Warner CW, McIsaac RL. The evolution of peptic ulcer thera-py. A role for temporal control of drug delivery. Ann N Y Acad Sci.1991;618:504-516.5. Garnett WR. History of acid suppression: focus on the hospitalsetting. Pharmacotherapy. 2003;23:56S-60S.6. Konturek SJ, Konturek PC, Brzozowski T, Konturek JW, Paw-lik WW. From nerves and hormones to bacteria in the stomach;Nobel prize for achievements in gastrology during last century.J Physiol Pharmacol. 2005;56:507-530.7. Shah R. Dyspepsia and helicobacter pylori. BMJ. 2007;334:41-43.
8. Scarpignato C, Pelosini I, Di Mario F. Acid suppression thera-py: where do we go from here? Dig Dis. 2006;24:11-46.9. Zimmet SE. Principles of treatment of varicose veins by scle-rotherapy and surgery. In: Bergan JJ, ed. The Vein Book.London,England: Elsevier; 2007:227-230.10. Perrin M. Cure chirurgicale des varices des membres infé-rieurs par stripping des veines saphènes. Ann Chir.1997;7:735-744.11. Bergan JJ. Inversion stripping of the saphenous vein. In:Bergan JJ, ed. The Vein Book. London, England: Elsevier; 2007:231-237.12. Goldman MP, Bergan JJ, Guex JJ, eds. Role of surgery in treat-ment of varicose veins. In: Sclerotherapy Treatment of Varicoseand Telangiectatic Leg Veins,4th ed. Philadelphia, Pa: Mosby El-sevier; 2007;285-306.13. Goldman MP, Bergan JJ, Guex JJ, eds. Intravascular approach-es to the treatment of varicose veins: radiofrequency and lasers.In: Sclerotherapy Treatment of Varicose and Telangiectatic LegVeins, 4th ed. Philadelphia, Pa: Mosby Elsevier; 2007;307-316.14. Bergan JJ, Schmid-Schônbein G, Coleridge-Smith P, Nico-laides A, Boisseau M, Eklof B. Chronic venous disease. N EnglJ Med. 2006;355:488-498.
TRAITEMENT DE L’INSUFFISANCE VALVULAIRE VEINEUSE : PASSÉ, PRÉSENT ET FUTURUNE RÉFLEXION SUR SON ÉVOLUTION COMPARÉE À L’ULCÈRE GASTRODUODÉNAL
C et article veut établir un parallèle entre l’évolution remar-quable du traitement de l’ulcère gastroduodénal et celuides veines refluantes. Pour traiter la maladie acido-pep-
tique, on a tenté de contrôler la sécrétion gastrique acide afin deguérir et prévenir la récidive d’ulcères duodénaux. De même, laréparation de valvules refluantes et même plus, la prévention deslésions valvulaires sont présentées comme l’avenir du traitementde la maladie veineuse chronique. Pour revenir à la maladie aci-do-peptique, des chirurgiens comme Pean, Rydygier et Billrothont réalisé leurs premières résections gastriques dans la deuxièmemoitié du XIXe siècle. En 1943, la première vagotomie troncu-laire a été effectuée pour limiter la stimulation cholinergique dela sécrétion gastrique acide. Ceci a mené à une chirurgie qui a as-socié résections gastriques et vagotomie. En 1970, la premièretechnique microchirurgicale est apparue sous la forme d’une va-gotomie cellulaire pariétale. Elle permettait de limiter la compo-sante vagale de départ de la sécrétion acide en minimisant l’im-pact sur les autres fonctions gastro-intestinales. Dans les années60, les antiacides pour neutraliser l’acide et les anticholinergiquespour diminuer la quantité d’acide produite ont fait partie des trai-tements pharmacologiques. En 1976, une nouvelle phase du trai-tement de la maladie acido-peptique voit le jour avec l’introduc-tion du premier antagoniste des récepteurs H2. Depuis 1982, ladécouverte d’Helicobacter pylori a complètement bouleversé le
rôle de la chirurgie dans la prise en charge de l’ulcère gastroduo-dénal. Dans la plupart des cas, le traitement médical est entreprisavec des molécules spécifiques destinées à Helicobacter pylori etla sécrétion acide et les méthodes interventionnelles sont princi-palement réservées au traitement de l’ulcère perforé. De nos jours,les chirurgiens ne s’occupent que du traitement chirurgical descomplications de l’ulcère gastrique (par exemple, perforations,saignement ou transformation maligne des ulcères gastriques).La même évolution au cours du temps a eu lieu en ce qui concernela prise en charge de la maladie veineuse. Depuis des années, lestripping des veines abritant des valvules pathologiques a été laméthode utilisée pour l’élimination des reflux superficiels. Le tauxélevé de récidive après chirurgie de la grande veine saphène asso-cié à l’amélioration très importante de l’imagerie des valvulesveineuses grâce à des méthodes sophistiquées d’écho-Doppler pul-sé, ont permis d’envisager la reconstruction de la valve maladeplutôt que sa résection. Les perspectives dans le cadre de la priseen charge de la maladie veineuse restent à préciser et il faudraitcréer des stragégies de prévention des lésions valvulaires plutôtque la résection ou la réparation. Comme pour l’ulcère gastroduo-dénal, il est possible de considérer que les médicaments spéci-fiques destinés à corriger les défauts génétiques, renforcer le tonusveineux ou prévenir l’inflammation qui endommage les valvules,pourraient remplacer les méthodes de traitement actuelles.

137The saphenofemoral junction: to ligate or not to ligate? MEDICOGRAPHIA, VOL 30, No. 2, 2008
C O N T R O V E R S I A L Q U E S T I O N
The saphenofemoral junction: to ligate or not to ligate?
tributaries coming from the SFJ, and only 3.2%showed neovascularization. Bradbury et al11 foundthat of 71 patients undergoing repeat groin dis-section, only 20 (28%) had a ligated SFJ, 31 (44%)had intact major tributaries, and 52 (73%) hadan intact GSV in the thigh. Neovascularization isconsidered to be the cause of recurrence whenHL is technically perfect.9,12 However, Egan et al13
found that DUS identified neovascularization inonly 8.2% limbs with recurrence. Surgical explo-ration revealed a residual GSV stump with oneor more significant tributaries in 27 out of 41 re-current limbs. Each of the remaining 14 limbs hada residual incompetent thigh GSV. Two prospec-tive studies by De Maeseneer et al suggested thatthe incidence of neovascularization after SFJligation is much higher in both the short term 12
(14% of cases at 1 year) and long term14 (68% ofcases at 5 years). Neovascularization is also seenafter radiofrequency ablation of the GSV and,surprisingly, is more common when the SFJ isnot ligated (67% vs 34% when ligated).15 Neovas-cularization after HL may be reduced by usingbarrier techniques such as polytetrafluoroethylene(PTFE),16 silicon17 patches, and endoablation ofthe intima of the ligated SFJ stump by under-run-ning the mouth with prolene sutures.18 In sum-mary, at this stage, it may be premature to con-demn HL as a cause of neovascularization and/orrecurrence. Technical modifications with betterpreoperative assessment to identify other factorsresponsible for high hydrostatic and hemodynam-ic forces will probably give better recurrence-freeresults after HL. More prospective randomizedtrials with periodic and regular DUS follow-upare needed before the concept of sparing the SFJcan be proved to be effective and acceptable. �
L igation of the saphenofemoral junction(SFJ) was first proposed by Trendelenburgin 1890 and modified to its current form
by Moore and Thomas in 1896.1 Extended flushhigh ligation (HL), taking care to cauterize or tieall the tributaries right up to the first or secondlevel, is the current recommended technique.2 HLwith removal of the great saphenous vein (GSV)has been the universally accepted surgical treat-ment of axial venous reflux for almost a century.HL alone aimed at preserving the GSV for futureuse is associated with poor results, because refluxpersists,3 resulting in recurrent varicose veins.4-7
HL with stripping of the thigh GSV gives betterresults than HL with sclerotherapy or stab avul-sions.8 These results suggest that removal of thethigh portion of the GSV with detachment of itsperforator tributaries is more important than HLitself and it remains a crucial step in the treat-ment of axial reflux.2 Two issues now threaten thisprocedure after almost 100 years. First, there isthe need among surgeons who treat venous re-flux to use minimally invasive methods, ablatingonly the GSV and leaving the SFJ untouched.The second is the duplex ultrasonography (DUS)-based observation that significant varicose veinrecurrence9 is due to neovascularization, even af-ter technically correct HL. Several aspects need tobe answered in deciding for or against HL: (i) whatare the causes of recurrence after SFJ ligation?(ii) is the risk of neovascularization sufficient toabandon the procedure? (iii) does neovasculariza-tion also occur if the SFJ is left untouched? and(iv) what are the alternative procedures available?Most recurrence is due to technical failure. Vianiet al 10 reported that in 61 patients with recur-rence, 50.8% had an intact SFJ, 44.2% had intact
1� P. Pai, India
Paresh PAI, MSThe Vascular Clinic15 Dar-Ul-Muluk26 Pandita Ramabai RoadMumbai 400 007, INDIA(e-mail:[email protected])
Stripping the long saphenous vein reduces the rate of re-op-eration for recurrent varicose veins: Five-year results of arandomised trial. J Vasc Surg. 1999;29:589-592.7. Winterborn RJ, Foy C, Earnshaw JJ. Causes of varicose veinrecurrence: Late results of a randomised trial of stripping ofthe long saphenous vein. J Vasc Surg. 2004;40:634-639.8. Rutgers PH, Kitslaar PJ. Randomized trial of stripping versushigh ligation combined with sclerotherapy in the treatmentof the incompetent greater saphenous vein. Am J Surg. 1994;168:311-315.9. De Maeseneer M. Neovascularisation: an adverse responseto proper groin dissection. In: Bergan JJ, ed. The vein book.Oxford, UK: Elsevier Academic Press; 2007:239-246.10. Viani MP, Poggi RV, Pinto A, Andreani SM, Spagnoli C,Maruotti RA. Re-exploration of the sapheno-femoral junctionin the treatment of recurrent varicose veins. Int Surg.1996;81:382-384.11. Bradbury AW, Stonebridge PA, Ruckley CV, Beggs I. Re-
REFERENCES1. Caggiati A, Allegra C. Historical introduction. In: BerganJJ ed. The vein book. Oxford, UK: Elsevier Academic Press;2007:1-14.2. Bergan JJ, Kumins NH, Owens EL, Sparks SR. Surgicaland endovascular treatment of lower extremity venous insuf-ficiency. J Vasc Interv Radiol. 2002;13:563-568.3. Fligelston L, Carolan G, Pugh N, Minst P, Shandall A, Lane I.An assessment of the long saphenous vein for potential useas a vascular conduit after varicose vein surgery. J Vasc Surg.1993;18:836-840.4. McMullin GM, Coleridge-Smith PD, Scurr JH. Objectiveassessment of high ligation without stripping the long saphe-nous vein. Br J Surg. 1991;78:1139-1142.5. Jones L, Braithwaithe BD, Selwyn D, Cooke S, Earnshaw JJ.Neovascularisation is the principal cause of varicose vein re-currence. Results of a randomised trial of stripping of the longsaphenous vein. Eur J Vasc Endovasc Surg. 1996;12:442-445.6. Dwerryhouse S, Davies B, Harradine K, Earnshaw JJ.

C O N T R O V E R S I A L Q U E S T I O N
138 The saphenofemoral junction: to ligate or not to ligate?MEDICOGRAPHIA, VOL 30, No. 2, 2008
15. Salles-Cunha SX, Comerota AJ, Tzilinis A, et al. Ultrasoundfindings after radiofrequency ablation of the great saphenousvein: Descriptive analysis. J Vasc Surg. 2004;40:1166-1173.16. Earnshaw JJ, Davies B, Harradine K, Heather BP. Prelim-inary results of PTFE patch saphenoplasty to prevent neovas-cularisation leading to recurrent varicose veins. Phlebology.1998;13:10-13.17. De Maeseneer MG, Vandenbroeck CP, Van Schil PE. Siliconpatch saphenoplasty to prevent repeat recurrence after surgeryto treat saphenofemoral incompetence. Long-term follow-upstudy. J Vasc Surg. 2004;40:98-105.18. Frings N, Nelle A, Tran P, Fischer R, Krug W. Reduction ofneoreflux after correctly performed ligation of the sapheno-femoral junction. A randomized trial. Eur J Vasc EndovascSurg. 2004;28:246-252.
current varicose veins: correlation between preoperative clin-ical and hand-held Doppler ultrasonographic examination,and anatomical findings at surgery. Br J Surg. 1993;80:849-851.12. De Maeseneer MG, Ongena KP, van den Brande F, VanSchil PE, De Hert SG, Eyskens EJ. Duplex ultrasound assess-ment of neovascularisation after sapheno-femoral or saphe-no-popliteal junction ligation. Phlebology. 1997;12:64-68.13. Egan B, Donnelly M, Bresnihan M, Tierney S, Feeley M.Neovascularization: an “innocent bystander” in recurrentvaricose veins. J Vasc Surg. 2006;44:1279-1284.14. De Maeseneer MG, Tielliu IF, Van Schil PE, De Hert SG,Eyskens EJ. Clinical relevance of neovascularisation on duplexultrasound in the long-term follow-up after varicose vein op-eration. Phlebology. 1999;14:118-122.
quency endovenous obliteration. J Vasc Surg. 2004;39:189-195.4. Salles-Cunha SX, Comerota AJ, Tzilinis A, et al. Ultra-sound findings after radiofrequency ablation of the greatsaphenous vein: descriptive analysis. J Vasc Surg. 2004;40:1166-1173.5. Pannier F, Rabe E. Endovenous laser therapy and radiofre-quency ablation of saphenous varicose veins. J CardiovascSurg. 2006;47:3-8.
REFERENCES1. Perrin M, Gobin JP, Nicolini P. Recurrent varicose veins inthe groin after surgery. J Mal Vasc. 1997;22:303-312.2. Hartmann K, Klode J, Pfister R, et al. Recurrent varicoseveins: sonography-based re-examination of 210 patients 14years after ligation and saphenous vein stripping. Vasa. 2006;35:21-26.3. Pichot O, Kabnick LS, Creton D, et al. Duplex ultrasoundscan findings two years after great saphenous vein radiofre-
larization is the cause of recurrence in such cases,in the absence of surgical error. By contrast, onlyshort-term follow-up is available for patientstreated with radiofrequency ablation,3 and veryfew studies after endolaser ablation. Comparedwith stripping and SFJ ligation, radiofrequencyablation leaves physiologic tributary flow relative-ly undisturbed. Two year follow-up showed noevidence of inguinal neovascularization.3 Wewould do well to ask whether longer follow-upwould produce the same results. Descriptive anal-ysis of ultrasound findings after radiofrequencyablation showed small-vessel networks adjacentor connected to the ablated GSV in most cases.SFJ ligation, on the other hand, was associatedwith fewer small-vessel networks and proximalGSV recanalization when examined after a simi-lar follow-up period.4 Whether these small net-works will develop into large-caliber refluxingveins needs long-term follow-up. At present, thetrend not to ligate the SFJ and its tributaries isstrongly supported by the growing endoluminalablation market. The technique is definitely lessinvasive and gives results comparable to conven-tional surgery in terms of venous reflux elimi-nation and patient satisfaction.5 Only time willtell its effect on late recurrence. As the pendulumswings between different emerging techniques,it is clear that the ideal treatment for varicoseveins, based on a proper understanding of theunderlying pathology and hemodynamics, con-tinues to elude us. �
A main aim of venous surgery is to elimi-nate venous reflux. However, with alltreatment modalities, long-term recur-
rence remains a challenging problem, and onewith a relatively high incidence, for reasons thathave attracted many explanations,1 in particularpoor surgical technique and neovascularization.During my surgical residency 25 years ago, “Toligate or not to ligate” was not a question thatwould ever have been proposed. Saphenofemoralflush ligation, with meticulous ligation of alltributaries at that level, was combined with greatsaphenous vein (GSV) stripping as the standardsurgical technique. The growing trend toward lessinvasive low-morbidity intervention, day surgery,and outpatient procedures has combined withthe refinement of endoluminal vascular instru-ments to favor the introduction and increaseduse of endoluminal ablation for GSV reflux. Itwas these emerging techniques that promptedthe question “To ligate or not to ligate” since itbecame impossible to ligate the saphenofemoraljunction (SFJ) and we therefore ignored the nu-merous venous tributaries around it. Researchsought to determine the effect of ligation and non-ligation on the incidence of recurrence, and waspushed a step forward to postulate that if recur-rence was caused by neovascularization, then thesolution was to avoid surgical groin hematoma.In the case of conventional surgery, we have long-term studies of patients’ groins up to 14 yearspostoperatively.2 The consensus is that neovascu-
2� A. S. Sabbour, Egypt
Ali S. SABBOUR, MDProfessor of Vascular SurgeryAin Shams UniversityCairo, EGYPT(e-mail: [email protected])

C O N T R O V E R S I A L Q U E S T I O N
139The saphenofemoral junction: to ligate or not to ligate? MEDICOGRAPHIA, VOL 30, No. 2, 2008
access or advancement, transient heat, bruising,pain, paresthesia, thermal skin damage, superfi-cial thrombophlebitis, lymphedema, and deepvein thrombosis. Some randomized trials haveconcluded that endoluminal thermal vein abla-tion is as effective as conventional stripping.3,4
Some enthusiasts of ultrasound guidance andintravenous foam injection have expanded theindications for conventional sclerotherapy to in-clude treatment of an incompetent GSV. Theyargue that saphenofemoral occlusion using ex-ternal compression or a balloon-tipped catheterpermits retention of foam sclerosant in the veinlong enough to produce sufficient damage tocause sclerosis. Side effects are infrequent, usuallyresolve spontaneously, and can include chest dis-comfort, nausea, dry cough, headache, dizziness,visual disturbance, and psychogenic reactions.Recently some authors have shown that ultra-sound-guided foam sclerotherapy can be effectiveeven if GSV diameter at the saphenofemoral junc-tion exceeds 10 mm, to a maximum of 16 mm,5
but further information is needed regarding bub-ble emboli and long-term follow-up. Procedurecosts appear highest for radiofrequency ablation,somewhat lower for laser ablation, and signifi-cantly lower for chemical ablation. The answerto the question “To ligate or not to ligate?” hangson the definition of neovascularization or recur-rence. Some authors agree that neovasculariza-tion is secondary to “frustrated” venous drainagefrom the abdominal wall and perineum, whileothers believe that recurrence is the issue, due tothe enlargement of previously existing veins thatwere ineffectively ligated and consequently causerecurrent reflux in the thigh. The literature con-tains various reports of neovascularization orrecurrence after ligation and stripping 6 and alsoafter radiofrequency/laser procedures.7 In my viewthe answer also depends on the definition of suc-cessful treatment, including the entire procedure,the method of screening for treatment failure,and the reporting of results. Recent advances inultrasound technology allow more critical eval-uation of clinical results than in the past. Weneed more high-quality randomized multicenterstudies, and long-term follow-up of endoluminalablation, both thermal and chemical, before wecan define their role and costs compared withmodern minimally-invasive GSV stripping. �
V arious interventions have been describedto correct the underlying pathophysiologi-cal abnormalities that lead to varicose
veins. Appropriate patient selection is crucial forsuccess. Treatment planning should be directedby the presence/absence and location of axialreflux, and the extent and location of the super-ficial venous pathology. Duplex ultrasonography(DUS) has become the gold standard for this pur-pose and in most patients is the only diagnosticinvestigation necessary in selecting the mostappropriate intervention. The parameters evalu-ated by DUS comprise: patency of the deep venoussystem, evidence of prior deep vein thrombosisor deep venous system reflux, great saphenousvein (GSV) reflux and anatomy (eg, double GSV),GSV diameter and distance from skin, smallsaphenous vein reflux, anatomy of the sapheno-popliteal junction, and perforator incompetenceand location. Treatment options include (i) forGSV reflux: ligation and stripping, radiofrequencyor laser endovenous thermal ablation, and endo-venous chemical ablation with a foam detergent;(ii) for perforator incompetence: minimally in-vasive ligation, subfascial endoscopic perforatorsurgery, sclerotherapy or even the Linton proce-dure; and (iii) for superficial varicosities andvaricose veins: stab avulsion phlebectomy, sclero-therapy and/or laser therapy. Management of GSVincompetence has historically been treated withhigh ligation of the GSV at the saphenofemoraljunction, ligation of all tributaries, and groin-to-ankle stripping of the saphenous vein.1 Thissurgery was highly invasive and associated withsevere pain and bruising, swelling, and disfiguringscars. However, modern stripping techniques havegreatly reduced the associated trauma and mor-bidity. Stripping can now be performed as anoutpatient procedure in the above-knee segmentof the GSV without a distal incision for a bettercosmetic result. Early ambulation with elasticstockings is encouraged. Endoluminal laser orradiofrequency thermal ablation requires percu-taneous access to the vein lumen. Initially, inthese ambulatory procedures, there was a concernto use limited energy to restore competence tothe saphenofemoral valve, but this did not proveeffective in the long term.2 Intraoperative andpostoperative complications are infrequent, gen-erally well tolerated, and include difficult device
3� A. Mansilha, Portugal
Armando MANSILHA, MDPhD, FEBVS, Department of Vascular SurgeryOporto Medical SchoolHospital S. João, AlamedaProf. Hernâni Monteiro4200-319 Porto, PORTUGAL(e-mail:[email protected])
low-up. Eur J Vasc Endovasc Surg. 2005;29:67-73.5. Barrett JM, Allen B, Ockelford A, Goldman MP. Microfoamultrasound-guided sclerotherapy treatment for varicose veinsin a subgroup with diameters at the junction of 10 mm orgreater compared with a subgroup of less than 10 mm. Derma-tol Surg. 2004;30:1386-1390.6. Fischer R, Chandler JG, De Maeseneer MG, et al. The un-resolved problem of recurrent saphenofemoral reflux. J AmColl Surg. 2002;195:80-94.7. Pichot O, Kabnick LS, Creton D, et al. Duplex ultrasoundscan findings two years after great saphenous vein radio-frequency endovenous obliteration. J Vasc Surg. 2004;39:189-195.
REFERENCES1. Sarin S, Scurr JH, Coleridge-Smith PD. Stripping of thelong saphenous vein in the treatment of primary varicose veins.Br J Surg. 1994;81:1455-1458.2. Danielsson G, Jungbeck C, Peterson K, Norgren L. Venousfunction after restoring valve competence of the great saphe-nous vein. J Endovasc Ther. 2003;10:350-355.3. Rautio T, Ohinmaa A, Perala J, et al. Endovenous oblitera-tion versus conventional stripping operation in the treatmentof primary varicose veins: a randomized controlled trial withcomparison of the costs. J Vasc Surg. 2002;35:958-965.4. Lurie F, Creton D, Eklof B, et al. Prospective randomisedstudy of endovenous radiofrequency obliteration (closure)versus ligation and vein stripping (EVOLVeS) : two-year fol-

C O N T R O V E R S I A L Q U E S T I O N
140 The saphenofemoral junction: to ligate or not to ligate?MEDICOGRAPHIA, VOL 30, No. 2, 2008
since it preserves the drainage of SFJ collateralsinto the femoral vein. Our clinical recurrencerate (6.3%) can be compared with stripping com-bined with extended high ligation, where thefigures vary from 10% to 25% after 2 years.15,18
Our recurrence rate is also better than the 12%to 15% observed after endovenous treatment withan identical follow-up.9-11 It is difficult to comparethe different studies because none have quanti-fied either the preoperative varices or varicosereservoir resection. Moreover, in our study, clin-ical recurrence was independent of SFJ reflux in6 cases out of 7, just as GSV ablation did not leadto recurrence in the studies of endovenous treat-ment.9-11 These observations support the increas-ingly propounded theory that varicose diseasedevelops from the superficial distal venous net-work,3-6,19 rather than downwards from the junc-tions between deep and superficial venous net-works, as in the conventional view.20,21 However,we did observe one serious postoperative compli-cation: SFJ thrombosis extending into the femoralvein, with pulmonary embolism, but fortunatelyno further serious sequelae. This potentially se-rious complication has been reported after endo-venous treatment 9,22-24 and should probably betaken into account by targeted prevention whenpreserving the SFJ, for example by using lowmolecular weight heparin or conventional highligation with multiple phlebectomy in patientswith thrombophilia, a history of thrombosis, ora very dilated junction (>20 mm). Early postop-erative Doppler ultrasonography (after 24-48hours) could also be recommended for detectingthromboembolic complications.24 In endovenoustreatment, conserving the SFJ is beneficial duringsurgical ablation of the GSV because it preservesphysiological venous drainage of the inguinalregion and minimizes the mid-term risk of neo-vascularization and varicose recurrence. Furtherstudies are needed in order to assess the postop-erative risk of SFJ thrombosis and the long-termhemodynamic results of this surgical approachand of SFJ-preserving endovenous techniques. �
I n cases of great saphenous vein (GSV) reflux,the ostial valve is often competent. The fre-quency of subostial or more distal trunk reflux
is estimated at around 50% in the literature.1-6
Endovenous treatments for GSV reflux that sparethe saphenofemoral junction (SFJ) during GSVablation have called into question the principleof high ligation of the SFJ.7,8 Midterm results us-ing endovenous techniques show anterogradedrainage of the SFJ collaterals toward the deepvein in 85% to 100% of cases.9-11 Yet high liga-tion of the SFJ remains the rule when strippingthe GSV. Since October 2003, given the resultsof endovenous treatment, we have stopped com-bining high ligation with surgical stripping, evenin cases of ostial reflux. We recently reported thehemodynamic and clinical results of this new ap-proach at the 19 th Annual Congress of the Amer-ican Venous Forum, in San Diego, CA, USA. Weobserved no reflux in the preserved SFJ in 98%of cases over a mean follow-up of 24.4 months.These results are at least comparable with, oreven superior to, the 80% to 97% absence of SFJreflux reported 2 years after endovenous radiofre-quency or laser treatment.8-13 This prompts thequestion: Does surgical stripping combined withextensive phlebectomy improve the hemody-namics of the preserved SFJ, given that the GSVcannot recanalize and, perhaps especially, thatthe varicose reservoir has been ablated? Thehemodynamic benefits of varicose reservoir ab-lation are mentioned in the literature.14 Despiteinguinal surgery, the rate of inguinal neovascu-larization was very low in our series (1.8% at 2years). This figure is no higher than the 0% to2.8% recorded after endovenous treatment,8-11 andmuch lower than in surgical studies of extendedhigh ligation with rates of 20% to 53%.15-17 Pre-serving the superficial abdominal and perinealvenous drainage by not dissecting the SFJ andnot disconnecting the collaterals appears to avoidneovascularization. Using a limited inguinal ap-proach without dissecting the SFJ does not there-fore seem to cause more neovascularization
4� P. Pittaluga and S. Chastanet, France
�Paul PITTALUGA, MD Sylvain CHASTANET, MD
Corresponding author:Paul PittalugaRiviera Vein Institute6 rue Gounod Nice06000 Nice, FRANCE(e-mail: [email protected])
2002;55:239-243.8. Pichot O, Kabnick LS, Creton D, Merchant RF, Schuller-Petroviae S, Chandler JG. Duplex ultrasound scan findings twoyears after great saphenous vein radiofrequency endovenousobliteration. J Vasc Surg. 2004;39:189-195.9. Merchant RF, Pichot O. Long-term outcomes of endovenousradiofrequency obliteration of saphenous reflux as a treatmentfor superficial venous insufficiency. J Vasc Surg. 2005;42:502-509.10. Nicolini P; Closure Group. Treatment of primary varicoseveins by endovenous obliteration with the VNUS closure sys-tem: results of a prospective multicentre study. Eur J VascEndovasc Surg. 2005;29:433-439.11. Creton D; Closure Group. [Treatment of primary venousinsufficiency by radiofrequency obliteration with the VNUS-Closure® system. Results of a 5-year multicenter prospectivestudy]. Phlebologie. 2006;59:67-72.12. Min RJ, Khilnani N, Zimmet SE. Endovenous laser treatment of saphenous vein reflux: long-term results. J VascInterv Radiol. 2003;14:991-996.13. Proebstle TM, Moehler T, Herdemann S. Reduced recanal-
REFERENCES1. Abu-Own A, Scurr JH, Coleridge-Smith PD. Saphenous veinreflux without incompetence at the saphenofemoral junction.Br J Surg. 1994;81:1452-1454.2. Labropoulos N, Delis K, Nicolaides AN, Leon M, RamaswamiG. The role of the distribution and anatomic extent of refluxin the development of signs and symptoms in chronic venousinsufficiency. J Vasc Surg. 1996;23:504-510.3. Labropoulos N, Giannoukas AD, Delis K, et al. Where doesvenous reflux start? J Vasc Surg. 1997;26:736-742.4. Engelhorn CA, Engelhorn AL, Cassou MF, Salles-Cunha SX.Patterns of saphenous reflux in women with primary varicoseveins. J Vasc Surg. 2005;41:645-651.5. Labropoulos N, Leon L, Kwon S, et al. Study of the venousreflux progression. J Vasc Surg. 2005;41:291-295.6. Pittaluga P, Chastanet S, Réa B, Barbe R, Guex JJ, Locret T.[Duplex ultrasonography scanning for superficial venous in-sufficiency: Correlation of mapping with age, symptoms andsigns]. Phlebologie. 2006;59:149-156.7. Guex JJ, Min RJ, Pittaluga P, et al. [Treatment of greatsaphenous vein incompetence by endovenous laser treat-ment: Technique and indications. Discussion]. Phlebologie.

C O N T R O V E R S I A L Q U E S T I O N
141The saphenofemoral junction: to ligate or not to ligate? MEDICOGRAPHIA, VOL 30, No. 2, 2008
recurrence: late results of a randomized controlled trial ofstripping the long saphenous vein. J Vasc Surg. 2004;40:634-639.4. Egan B, Donnelly M, Bresnihan M, Tierney S, Feeley M.Neovascularization: an “innocent bystander” in recurrentvaricose veins. J Vasc Surg. 2006;44:1279-1284.5. De Maeseneer MG, Vandenbroeck CP, Van Schil PE. Siliconepatch saphenoplasty to prevent repeat recurrence after surgeryto treat recurrent saphenofemoral incompetence: long-termfollow-up study. J Vasc Surg. 2004;40:98-105.
REFERENCES1. Allegra C, Antignani PL, Carlizza A. Recurrent varicoseveins following surgical treatment: our experience with fiveyears follow-up. Eur J Vasc Endovasc Surg. 2007;33:751-756.2. De Maeseneer MG, Vandenbroeck CP, Hendriks JM, LauwersPR, Van Schil PE. Accuracy of duplex evaluation one year af-ter varicose vein surgery to predict recurrence at the sapheno-femoral junction after five years. Eur J Vasc Endovasc Surg.2005;29:308-312.3. Winterborn R, Foy C, Earnshaw JJ. Causes of varicose vein
of the odds of long-term relapse at the SFJ. Win-terborn et al 3 monitored outcome 11 years aftersurgery in 51 out of an original population of100 patients, concluding that recurrence and theneed for reintervention were due to incompetencein the groin, the commonest cause being neo-vascularization. They suggested that the presenceof a residual GSV may be contributory, a viewconfirmed by Egan et al 4 who observed that allrecurrent varicose veins associated with duplex-diagnosed neovascularization are also associatedwith persistent reflux in the GSV stump tribu-taries, thigh GSV, or both. These data force theconclusion that so long as we continue to ligatethe SFJ, we must use correct surgical technique,avoid leaving tributaries or incompetent GSVsegments in the thigh, develop a better under-standing of neovascularization, and use postop-erative color Doppler ultrasound scanning infollow-up. Some authors believe that the use ofphysical barriers, such as silicone patches, maydiminish neovascularization, particularly in re-peat recurrence.5 Techniques such as endoluminalradiofrequency, laser or sclerosing foam ablationof the GSV avoid SFJ ligation. They have yieldedpromising short-term results, but only long-termcomparative studies will ultimately determinewhether SFJ ligation is unnecessary. �
L igation of the saphenofemoral junction(SFJ) has for many years been considereda mandatory part of the surgical treatment
for varicose veins. The need to ligate the greatsaphenous vein (GSV) at this level is being ques-tioned on the basis of better awareness of neo-vascularization in the groin and the developmentof alternative techniques. The conventional andperhaps oversimplified view is that neovasculariza-tion results from poor surgical technique. How-ever, the evidence now suggests that it can occurdespite correct surgical technique. It is thereforeimportant to determine its frequency and identifyits causes, with particular regard to the follow-ing factors: stimulation of angiogenesis by the en-dothelium in the GSV stump, the role of inguinallymphovenous connections, the vasa vasorum ofthe femoral vein, altered physiological drainageof inguinal GSV tributaries, and constitutionalfactors. Color Doppler ultrasonography is a par-ticularly useful monitoring tool. In a follow-up of1326 patients, Allegra et al found no residual re-flux in the GSV trunk 3 weeks after varicose veinsurgery, but a 13% relapse rate at the SFJ after5 years.1 Using the same technique in 100 patients,De Maeseneer et al 2 noted that neovasculariza-tion was unlikely ever to develop in those in whomit was not present at 1 year, thus giving an idea
5� A. Masegosa, Spain
Alberto MASEGOSA, MDServicio de Angiologia yCirurgía VascularHospital General de AlbaceteC/ Hermanos Falco, s/n02002 Albacete, SPAIN(e-mail: [email protected])
Am J Surg. 1994;168:311-315.19. Cooper DG, Hillman-Cooper CS, Barker SG, HollingsworthSJ. Primary varicose veins: the sapheno-femoral junction,distribution of varicosities and patterns of incompetence. Eur JVasc Endovasc Surg. 2003;25:53-59.20. Trendelenburg F. Ueber die Unterbindung der Vena saphenamagna bei Unterschenkelvaricen. Beitr Klin Chir. 1890;7:195-210.21. Ludbrook J, Beale G. Femoral venous valves in relationto varicose veins. Lancet. 1962;1:79-81.22. de Medeiros CA, Luccas GC. Comparison of endovenoustreatment with an 810 nm laser versus conventional strippingof the great saphenous vein in patients with primary varicoseveins. Dermatol Surg. 2005;31:1685-1694.23. Lurie F, Creton D, Eklof B, et al. Prospective randomisedstudy of endovenous radiofrequency obliteration (Closure)versus ligation and vein stripping (EVOLVeS): two-year follow-up. Eur J Vasc Endovasc Surg. 2005;29:67-73.24. Puggioni A, Kalra M, Carmo M, Mozes G, Gloviczki P. Endovenous laser therapy and radiofrequency ablation of thegreat saphenous vein: analysis of early efficacy and compli-cations. J Vasc Surg. 2005;42:488-493.
ization rates of the great saphenous vein after endovenouslaser treatment with increased energy dosing: definition of athreshold for the endovenous fluence equivalent. J Vasc Surg.2006;44:834-839.14. Pittaluga P, Réa B, Barbe R, Guex JJ. A.S.V.A.L. method:principles and preliminary results. In: Becquemin JP, Alimi YS,Watelet J, eds. Updates and Controversies in Vascular Surgery.Turin, Italy: Minerva Medica; 2005:182-189.15. Jones L, Braithwaite BD, Selwyn D, Cooke S, Earnshaw JJ.Neovascularisation is the principal cause of varicose vein recurrence: result of a randomised trial of stripping the longsaphenous vein. Eur J Vasc Endovasc Surg. 1996;12:442-445.16. van Rij AM, Jiang P, Solomon C, Christie RA, Hill GB. Recurrence after varicose vein surgery: a prospective long-term clinical study with duplex ultrasound scanning and airplethysmography. J Vasc Surg. 2003;38:935-943.17. Perrin MR, Labropoulos N, Leon LR Jr. Presentation ofthe patient with recurrent varices after surgery (REVAS).J Vasc Surg. 2006;43:327-334.18. Rutgers PH, Kitslaar PJ. Randomized trial of strippingversus high ligation combined with sclerotherapy in the treatment of the incompetent greater saphenous vein.

C O N T R O V E R S I A L Q U E S T I O N
142 The saphenofemoral junction: to ligate or not to ligate?MEDICOGRAPHIA, VOL 30, No. 2, 2008
5. El Wajeh Y, Giannoukas AD, Gulliford CJ, Suvarna SK,Chan P. Saphenofemoral venous channels associated with recurrent varicose veins are not neovascular. Eur J Vasc En-dovasc Surg. 2004;28:590-594.6. Lurie F, Creton D, Eklof B, et al. Prospective randomizedstudy of endovenous radiofrequency obliteration (closureprocedure) versus ligation and stripping in a selected patientpopulation (EVOLVeS Study). J Vasc Surg. 2003;38:207-214.7. Proebstle TM, Gul D, Kargl A, Knop J. Endovenous lasertreatment of the lesser saphenous vein with a 940-nm diodelaser: early results. Dermatol Surg. 2003;29:357-361.
REFERENCES1. Noppeney T, Rewerk S, Winkler M, Nullen H, Schmedt HC.[Primary varicosis]. Chirurg. 2007;78:620-629.2. Winterborn RJ, Earnshaw JJ. Crossectomy and greatsaphenous vein stripping. J Cardiovasc Surg. 2006;47:19-33.3. Egan B, Donnelly M, Bresnihan M, Tierney S, Feeley M.Neovascularization: an “innocent bystander” in recurrentvaricose veins. J Vasc Surg. 2006;44:1279-1284.4. Nyamekye I, Shephard NA, Davies B, Heather BP, Earn-shaw JJ. Clinicopathological evidence that neovascularisationis a cause of recurrent varicose veins. Eur J Vasc EndovascSurg. 1998;15:412-415.
sulting in recurrent varicose veins. Another ar-gument favoring endovenous obliteration is therapid recovery from a minor procedure underlocal or regional anesthesia, hence an improvedquality of life.6 Our experience has also shownsimilarly good results after minimally invasivesurgery under tumescent anesthesia. We wouldconfirm the long periods of pain along the GSVreported by Proebstle et al 7 after endovenouslaser treatment, even if most studies have foundless pain than after conventional surgery.1,6
Whether the phlebologist chooses to ligate ornot to ligate is mainly a question of anatomy,and it is solved by duplex scanning. In our expe-rience, a diameter >10 mm, aneurysm, or non-linear GSV close to the SFJ are indications forminimally invasive surgery. In very slim patientswith light skin, hyperpigmentation may be anegative cosmetic side effect of endovascularobliteration. As for duplex-guided foam sclero-therapy, we use it routinely in the elderly, pa-tients with comorbidities, and those who refusea minimally invasive technique. Short-term suc-cess can be measured by various parameters, include closure of the culprit venous valves, ve-nous reflux, visible varicose veins, quality of life,recovery time, and pain. The main parameter oflong-term success is the recurrence rate, diag-nosed by duplex scanning and described by thepresence of venous reflux. Although the short-and midterm results of endovenous obliterationare good, we know that the recurrence rate aftervenous surgery increases significantly after 10years. Accurate comparison will require long-term results.1 Provided that endovascular GSVobliteration works, the new nonligation tech-niques are highly promising because they do notappear to induce neovascularization and recur-rence is lower. It is therefore extremely aston-ishing that some practitioners combine GSVobliteration with saphenofemoral ligation. Com-bining two great methods may not end up witha result that is greater still, but with completecancellation of their respective benefits! �
D uplex scanning has greatly enhancedphlebology practice in recent years. Newendoluminal techniques such as duplex-
guided foam sclerotherapy have been developedor modified for treating great saphenous vein(GSV) incompetence. Current treatment optionsinclude minimally invasive surgery with flushligation of the saphenofemoral junction (SFJ) andall the tributaries, inversion stripping, mini-phlebectomy, and various ultrasound-guided endovascular procedures using heat (producedby laser, radiofrequency, immersion, or steam)or sclerosant foam, each of which approximatesand shrinks the vein walls, resulting in occlusionof the incompetent GSV trunk. These proceduresdispense with the conventional surgical practiceof ligating all tributaries. Irrespective of the op-tion chosen, every phlebologist faces the prob-lem of recurrence. Published recurrence ratesvary from 5% to 60% depending on method andtime frame, but all treatments aim to eradicatevenous insufficiency.1,2 Recurrence can be due todisease progression and technical error, but alsoto neovascularization, since Nature seeks ways torebuild what surgeons extirpate.3 Angiogenesisis a feature of all healing wounds and the re-maining intimal cells of the saphenous stumpproduce endothelial growth factor.4 The mainadvantage of endovenous obliteration is that itdoes not excise the incompetent trunk or shedendothelial cells into tissue. Short- and midtermoutcome is comparable to that of minimally invasive surgery, and with less recurrence, evenif the tributaries remain. El Wajeh et al5 and Eganet al 3 have suggested that a main factor in re-currence, rather than or in addition to neovas-cularization, lies in the abnormal hemodynamicforces in the saphenofemoral area, such as thehigh pressure in the first femoral segment distalto the inguinal ligament and above the proximalfemoral valve, the so-called “unprotected venoussegment.” Activity-induced peaks of abdominalpressure impact this unprotected venous segmentand escape through neovascular capillaries, re-
6� A. Obermayer, Austria
Alfred OBERMAYER, MDInstitute of FunctionalPhlebologic SurgeryKarl Landsteiner SocietyHimmelreichstrasse 15A-3390 Melk, AUSTRIA(e-mail: [email protected])

C O N T R O V E R S I A L Q U E S T I O N
143The saphenofemoral junction: to ligate or not to ligate? MEDICOGRAPHIA, VOL 30, No. 2, 2008
sewing the ligated SFJ with prolene to preventcontact with surrounding tissue,13 inserting apolytetrafluoroethylene (PTFE) patch over theligated junction,14 and closing the cribriformfascia.15 In recent years, endovenous ablation ofthe GSV without ligation has proved safe and effective in eliminating the proximal portion ofthe GSV from the venous circulation, giving evenfaster recovery and better cosmetic results thanstripping.16,17 The two currently available methodsare the Closure® procedure using a radiofrequencycatheter and generator (VNUS Medical Technolo-gies) and endovenous laser ablation, using alaser fiber and generator (various manufactur-ers). The goal of endovenous treatment is theablation of abnormal blood reflux by durable oc-clusion of the vein lumen. This can be achievedeither by shrinking the vein until the lumen hasvanished completely, or by substantially damag-ing the endothelium and inner vein wall leadingto secondary occlusion of the lumen by throm-bus, similar to the effect of a sclerosant. The de-gree of vein wall shrinkage appears importantbecause the residual lumen occluded by endovas-cular thrombus could be recanalized. The largerthe thrombus, the higher the risk of recanaliza-tion. Results are promising, both early (GSV oc-clusion was achieved in >90% of cases after bothprocedures at 1 month) and in the midterm (re-currence at 36 months appeared similar to thatafter conventional surgical management), al-though long-term follow-up and comparison withstandard GSV stripping are required to confirmthe durability of these endovenous procedures.However, the absence of neovascularization isstriking, and these minimally invasive proceduresare also well accepted by both doctors and pa-tients. The literature emphasizes the need for ear-ly ultrasound scanning in all patients after en-dovenous GSV ablation: veins still occluded 1 yearafter the procedure remained occluded at furtherfollow-up to 3 years.18,19 Relevant complicationsreported with endovenous treatment are rare. Themost important is deep vein thrombosis, whichfurther emphasizes the need for ultrasound B-scanning after surgery. Thrombus protrusioninto the femoral vein is an indication for anti-thrombotic therapy. Deep vein thrombosis prophy-laxis may be considered in patients >50 yearsold.20 In the absence of significant complications,endovenous procedures have important advan-tages in selected patients, offering less postoper-ative pain, earlier return to work and normalactivities, and apparent cost-effectiveness. En-dovenous treatment can be combined with anyother technique (Muller’s phlebectomy, all formsof sclerotherapy, perforator surgery, subfascialendoscopic perforator surgery, and endovenouslaser occlusion of incompetent perforators). Con-comitant tumescent anesthesia enables the vastmajority of patients to be treated in-office with-out general anesthesia or surgical incisions, at
T he most common source of ambulatory ve-nous hypertension is an incompetent super-ficial system, usually the great saphenous
vein (GSV). Alternatively, vein reflux may origi-nate from the deep veins, perforating veins, orany combination of the superficial, perforating,and deep vein systems. It is critical to identifythe origin of venous hypertension and the mostproximal point of reflux by performing a thor-ough evaluation with duplex ultrasound imaging.Superficial axial vein reflux may be correctedby surgical, thermal, or chemical means. Inter-ventions on the GSV at the saphenofemoral junc-tion (SFJ) have been widely performed in thebelief that this could control gravitational refluxand remove the hydrodynamic forces of perfora-tor vein reflux. A cornerstone of varicose veinsurgery is high ligation of the GSV with tributarystab avulsion, GSV stripping, and perforator liga-tion, with removal of bulging varicose veins whenvisible and palpable on the skin surface.1 Simpleligation of the GSV at the SFJ has been practicedto control gravitational reflux while preservingthe vein for possible subsequent arterial bypass.2
It is true that the GSV is largely preserved afterproximal ligation. Unfortunately, reflux continuesand hydrodynamic forces are not controlled. Lessreflux persists when the GSV is stripped.3,4 Ran-domized trials confirm that stripping is associ-ated with less recurrence than simple proximalligation.5,6 However, the period of disability afterstripping is greater than that after simple liga-tion.7 Attention eventually focused on the saphe-nous nerve injury associated with ankle to groinstripping.8 It was concluded that stripping fromgroin to ankle,9 or to the knee, caused less nerveinjury and did not adversely affect early venoushemodynamic improvement.10,11 One disappoint-ing outcome for surgeons and patients is recur-rence, defined as the presence of varicose veins ina lower limb previously operated on for varices,with or without adjuvant therapies. This clinicaldefinition includes true recurrence, residual veins,and varicose veins due to disease progression.Some causes are obvious: insufficient understand-ing of venous anatomy and hemodynamics, in-adequate preoperative assessment, and incorrector insufficient surgery. In the absence of surgicalerror, junctional recurrence is found in less thanone third of re-examined extremities. Duplex ul-trasound or re-exploration of the groin at thelevel of the SFJ frequently shows neovasculariza-tion as the cause of recurrence.12 Research needsto focus on the pathophysiological mechanismsthat could explain how new veins can developafter correct SFJ ligation: angiogenic stimulationin the free endothelium of the ligated stump,transnodal lymphovenous connection, dilation ofsmall adventitial vessels in the vasa vasorum ofthe femoral vein, or disturbed venous drainageof the ligated tributaries of the SFJ. Neovascular-ization in the groin has been reduced by over-
7� K. L. Katsenis, Greece
Konstantinos L. KATSENIS MD, Head of Vascular Unit2nd Surgical Clinic ofUniversity of AthensAretaieion Hospital76 Vas. Sophias Avenue Athens, GREECE(e-mail:[email protected])

C O N T R O V E R S I A L Q U E S T I O N
144 The saphenofemoral junction: to ligate or not to ligate?MEDICOGRAPHIA, VOL 30, No. 2, 2008
ing but still inconclusive.22 Thus endovenousmethods may be promising but GSV ligation andstripping remains the gold standard. However,there is an urgent need for prospective random-ized trials of endovenous laser therapy againstconventional surgery, high ligation at the sametreatment session, and other endovenous tech-niques such as radiofrequency closure and scle-rotherapy.23 �
the same time as maximizing outcome andminimizing recurrence.21 Ultrasound-guided foamsclerotherapy was introduced as a third alterna-tive treatment. Foam is more effective than liquid sclerotherapy and can be used to treatlarge-diameter veins and even main superficialtrunks. Most vascular surgeons agree that scle-rotherapy has been used for a very long time fortreating recurrent veins. The results are promis-
eration. Phlebology. 1999;14:118-122.13. Frings N, Nelle A, Tran P, Fischer R, Krug W. Reductionof neoreflux after correctly performed ligation of the saphe-nofemoral junction. A randomized trial. Eur J Vasc EndovascSurg. 2004;28:246-252.14. Winterborn RJ, Earnshaw JJ. Randomised trial of polyte-trafluoroethylene patch insertion for recurrent great saphenousvaricose veins. Eur J Vasc Endovasc Surg. 2007;34:367-373.15. De Maeseneer MG, Philipsen TE, Vandenbroek CP, et al.Closure of the cribriform fascia: an efficient anatomical barrieragainst postoperative neovascularisation at the saphenofemoraljunction. Eur J Vasc Endovasc Surg. 2007;34:361-366.16. Lurie F, Creton D, Eklof B, et al. Prospective randomizedstudy of endovenous radiofrequency obliteration (Closureprocedure) versus ligation and stripping in a selected patientpopulation (EVOLVeS Study). J Vasc Surg. 2003;38:207-214.17. Morrison N. Saphenous ablation: what are the choices,laser or RF energy? Semin Vasc Surg. 2005;18:15-18.18. Min RJ, Khilnani NM, Zimmet SE. Endovenous laser treat-ment of saphenous vein reflux: long term results. J Vasc In-terv Radiol. 2003;14:991-996.19. Pichot O, Kabnick LS, Creton D, Merchant RF, Schuller-Petrovic S, Chandler JG. Duplex ultrasound findings twoyears after great saphenous vein radiofrequency endovenousobliteration. J Vasc Surg. 2004;39:189-195.20. Puggioni A, Kalra M, Carmo M, Moses G, Glovinski P. Endovenous laser therapy and radiofrequency ablation of thegreat saphenous vein: analysis of early efficacy and compli-cations. J Vasc Surg. 2005;42:488-493.21. Chon MS, Seiger E, Goldman S. Ambulatory phlebecto-my using the tumescent technique for local anesthesia. Der-matol Surg. 1995;21:315-318.22. Rigby KA, Palfreyman SJ, Beverley C, Michaels JA. Surgeryversus sclerotherapy for the treatment of varicose veins.Cochrane Database of Systematic Reviews. 2004;Issue 4:Art.No.: CD004980. DOI: 10.1002/14651858.CD004980.23. Bergan JJ. The Vein Book. San Diego, CA: Elsevier Aca-demic Press; 2007.
REFERENCES1. Perrin M, Guidicelli H, Rastel D. Surgical techniques usedfor the treatment of varicose veins: survey of practice in France.J Mal Vasc. 2003;28:277-286.2. McMullin GM, Coleridge-Smith PD, Scurr JH. Objectiveassessment of high ligation without stripping the long saphe-nous vein. Br J Surg. 1991;78:1139-1142.3. Saarinen J, Heikkinen M, Suominen V, et al. Clinical dis-ability scores and reflux in complicated and uncomplicatedprimary varicose veins. Phlebology. 2003;18:73-77.4. Cheatle T. The long saphenous vein: to strip or not to strip?Semin Vasc Surg. 2005;18:10-14.5. Winterborn RJ, Foy C, Earnshaw JJ. Causes of varicoseveins recurrence: late results of a randomized controlled trialof stripping the long saphenous vein. J Vasc Surg. 2004;40:634-639.6. Butler CM, Scurr JH, Coleridge-Smith PD. Prospectiverandomized trial comparing conventional (Babcock) strippingwith inverting stripping of the long saphenous vein. Phlebology.2002;17:59-63.7. Jakobsen BH. The value of different forms of treatment forvaricose veins. Br J Surg. 1979;66:182-184.8. Munn SR, Morton JB, MacBeth WAAG, McLeish AR. To stripor not to strip the long saphenous vein? A varicose veins trial.Br J Surg. 1981;68:426-428.9. Holme JB, Skajaa K, Holme K. Incidence of lesions of thesaphenous nerve after partial or complete stripping of thelong saphenous vein. Acta Chir Scand. 1990;156:145-148.10. Rhodes JM, Gloviczki P, Canton L, Heaser TV, Rooke TW.Endoscopic perforator vein division with ablation of superfi-cial reflux improves venous hemodynamics. J Vasc Surg.1998;28:839-847.11. Miyazaki K, Nishibe T, Kudo F, et al. Hemodynamicchanges in stripping operation or saphenofemoral ligation ofthe greater saphenous vein for primary varicose veins. AnnVasc Surg. 2004;18:465-469.12. De Maesneer MG, Tielliu IF, Van Schil PE, De Hert SG,Eyskens EJ. Clinical relevance of neovascularisation on duplexultrasound in the long term follow up after varicose vein op-

C O N T R O V E R S I A L Q U E S T I O N
145The saphenofemoral junction: to ligate or not to ligate? MEDICOGRAPHIA, VOL 30, No. 2, 2008
therefore not suitable for all patients. One limi-tation is the diameter and tortuosity of the treat-ed vein. The risk of thermal damage to surround-ing structures should also be taken into account.There are two schools of surgeons: one performsstandard ligation of the GSV followed by endove-nous therapy, the other omits ligation, but bothclaim comparable midterm results. No long-termstudies are available. Radiofrequency ablation(the Closure® procedure) is based on endolumi-nal destruction of the endothelium and does notcomprise GSV ligation. In my experience, endo-vascular methods are often confined to patientsin stage C2 with no symptoms of chronic venousinsufficiency, thus clearly biasing results in themethod’s favor. Supporters of endovascular meth-ods without GSV ligation claim that they avoidneovascularization. However, Labropoulos et al failed to confirm this.2 Improved diagnosticmethods give us a more accurate overview ofthe hemodynamics, anatomy, and pathophysiol-ogy of the venous system of the lower extremi-ties and thus help us to select the appropriatetherapeutic method. Crossectomy, conventionalstripping and external stenting to the SFJ willdefinitely remain irreplaceable treatments for cer-tain groups of patients, particularly in the lightof their favorable long-term results.3 Endovascularprocedures have proved to be good alternativesto stripping, while sclerotherapy continues toplay an irreplaceable role. In addition, the thera-peutic spectrum comprises venotonics and com-pression therapy. Treatment choice also dependson the specific anatomic characteristics of thepatient’s venous system. The optimal procedureis the one that most improves a particular pa-tient’s quality of life. Only long-term comparativestudies that include a quality of life measurecan provide a conclusive answer to the question“To ligate or not to ligate.” �
REFERENCES1. Donnelly M, Tierney S, Feeley TM. Anatomical variation atthe saphenofemoral junction. Br J Surg. 2005;92:322-325.2. Labropoulos N, Bhatti A, Leon L. Neovascularization aftergreat saphenous vein ablation. Eur J Vasc Endovasc Surg.2006;31:219-222.3. Lurie F, Creton D, Eklof B, et al. Prospective randomizedstudy of endovenous radiofrequency obliteration (closureprocedure) versus ligation and stripping in a selected patientpopulation (EVOLVeS Study). J Vasc Surg. 2003;38:207-214.
O ptimal treatment of varicose veins requiresexact identification of the source of venousreflux. One of the biggest problems in
treatment is recurrence, which can reach 65%within 5 years and currently accounts for 25%of all varicose vein surgery. The best guaranteeof a good result lies in accurately identifying thesource of reflux and in removing it in the firstsurgical procedure. Duplex scanning of the lowerextremity plays an important role in reducing therate of varicose recurrence. Duplex ultrasoundmapping is much more accurate than other meth-ods of venous system examination. However, itis still not accepted by all general or vascular sur-geons because of the time and expense involved.In my view, clinical examination and manualDoppler ultrasound are insufficient in patientswith primary varicose veins. Duplex ultrasoundshould be considered as standard, and as abso-lutely essential in patients with varicose recur-rence. The problem of angiogenesis in the saphe-nofemoral junction (SFJ) stump following ligationof the great saphenous vein (GSV) is a hot topic.Experience tells us that primary surgery is oftenincorrectly performed, predisposing to recurrence.On the other hand, all surgeons have a propor-tion of patients with recurrence, whether or notthey believe the procedure they performed wasflawless. Perfect anatomical knowledge is essen-tial, given the multiplicity of venous variants inthe SFJ region. The GSV has tributaries subin-guinally—the medial and lateral accessory saphe-nous veins—as well as inguinally—superficialcircumflex iliac vein, superficial epigastric vein,and external pudendal vein, including its super-ficial and deep branches. The external pudendalvein can be double or triple, as can the GSV(18.1% of cases). The number of SFJ tributariesis also not constant. In 33.4% of cases, one ormore (junctional) tributaries join the GSV orcommon femoral vein deep to the deep fascia.Anatomical variation in the SFJ is important inensuring safe and appropriate management.1
Venous insufficiency is best treated using the leastinvasive methods, such as percutaneous endove-nous techniques which improve patient comfortand accelerate return to work. Endovascular ther-apy gives promising midterm results for GSVreflux. However, it also has certain pitfalls and is
8� L. Veverkova, Czech Republic
Lenka VEVERKOVA, MD, PhD1st Department of SurgerySt Anne’s University HospitalPekarska 53, 60200 BrnoCZECH REPUBLIC(e-mail: [email protected])

C O N T R O V E R S I A L Q U E S T I O N
146 The saphenofemoral junction: to ligate or not to ligate?MEDICOGRAPHIA, VOL 30, No. 2, 2008
physical examination and duplex findings. Fol-low-up at 42±5 months showed recurrence rates,defined by clinical and duplex findings, of 12%in the stripping group vs 20% in the high liga-tion group (P<0.05). However, duplex scanningshowed that the preserved GSV was suitable foruse as an arterial conduit in most cases. Theseresults suggest that it is possible to performelective vein surgery for varicose veins with rea-sonably good results and preserve the GSV foreventual arterial reconstruction. What is the roleof crossectomy and stripping in the modern era?Revascularization in the strip track after GSVstripping is a new concept in recurrence, and itoccurred in 3 of our 50 patients. Munasingheet al reported strip-track revascularization in23% of patients at 1 year, all with duplex-provenreflux.6 As an alternative to crossectomy andstripping, minimally invasive saphenous ablation,using endovenous radiofrequency or laser treat-ment, corrects and/or significantly improves thehemodynamic abnormality and clinical symp-toms associated with superficial venous reflux inover 95% of cases. These techniques may alsoreduce neovascularization in the groin. The crit-ical question is what is the role of simple highligation in preserving the GSV? Despite currentrecommendations, we still tend to perform thisprocedure on patients with severe saphenofemoraljunction reflux, below-knee varicosities, and anear normal-sized and normal-looking GSV. Wealso discuss the situation with the patient andexplain the higher rate of recurrence. In theevent of recurrence, endovenous laser or radio-frequency obliteration is readily performed as anoutpatient procedure after high ligation of thesaphenofemoral junction. �
T he aim of varicose vein surgery is to removereflux and visible varicosities in order toachieve the most favorable hemodynamic
and cosmetic result. High ligation is the crucialstep because it restores normal hemodynamics.However, if the incompetent saphenous trunk in the thigh is not stripped at the same time, itremains patent and incompetent after surgery,
and may provoke recurrent reflux. For this rea-son, high ligation combined with stripping becamethe standard treatment for truncal varicosities.1-3
On the other hand, venous grafts retrieved fromthe great saphenous vein (GSV) are the bestconduits for vascular and some coronary recon-structions. The demand for such grafts is contin-uously rising as the population ages, confrontingsurgeons with the problem of whether the saphe-nous trunk in patients with varicose veins maybe used for grafting or not, and if yes, what is theprice to be paid for preserving it? Hammarstenet al showed that 78% of preserved saphenousveins were suitable for use as arterial conduitsalmost 5 years after high ligation,4 althoughlowering the radicality of varicose vein surgeryincreases recurrence. The saphenous trunk inprimary varicose veins is not always degenerate,and may basically be compatible for use as a vas-cular or coronary artery conduit. Interestingly,it does not dilate aneurysmatically when trans-planted into the arterial circulation.5 We per-formed a prospective study to evaluate the long-term results of GSV-sparing surgery comparedwith above-knee stripping. Fifty patients withvaricose veins were randomly treated with stan-dard stripping of the GSV or high ligation. In bothgroups, miniphlebectomies were carried out andincompetent perforators ligated on the basis of
9� A. K. Bozkurt, Turkey
A. Kursat BOZKURT, MDProfessor of CardiovascularSurgery, Istanbul UniversityCerrahpasa, Medical FacultyIstanbul, TURKEY(e-mail:[email protected])
4. Hammarsten J, Pedersen P, Cederlund CG, Campanello M.Long saphenous vein saving surgery for varicose veins. Along-term follow-up. J Vasc Surg. 1990;4:361-364.5. Recek C. Does saphenous vein saving surgery have a rolein the therapy of primary varices? Rozhl Chir. 2003;82:591-595.6. Munasinghe A, Smith C, Kianifard B, Price BA, HoldstockJM, Whiteley MS. Strip-track revascularization after strip-ping of the great saphenous vein. Br J Surg. 2007;94:840-843.
REFERENCES1. Sarin S, Scurr JH, Coleridge-Smith PD. Stripping of thelong saphenous vein in the treatment of primary varicoseveins. Br J Surg. 1994;81:1455-1458.2. Dwerryhouse S, Davies B, Harradine K, Earnshaw JJ.Stripping the long saphenous vein reduces the rate of reoper-ation for recurrent varicose veins: five-year results of a ran-domized trial. J Vasc Surg. 1999;29:589-592.3. Bergan J. Inversion stripping of the saphenous vein. In:Bergan JJ, ed. The Vein Book. San Diego, Ca: Elsevier AcademicPress; 2007:231-237.

C O N T R O V E R S I A L Q U E S T I O N
147The saphenofemoral junction: to ligate or not to ligate? MEDICOGRAPHIA, VOL 30, No. 2, 2008
For these reasons, further studies are still neces-sary for a better understanding of the postopera-tive clinical course of GSV ablation and the mech-anisms underlying postoperative thrombosis.12,13,15
Neovascularization and recurrenceRecurrence is a common problem in the treat-ment of chronic venous disease.18 The use of min-imally invasive techniques has led to a debateover the role of inguinal surgical access and trib-utary ligation as causes of neovascularizationand recurrent varicose veins. Neovascularizationis an essential component of wound healing.19
New vessels arise due to angiogenic stimuli pro-duced during surgery; arteriovenous connectionsdevelop, promoting wound perfusion and healing.Van Rij et al have argued that neovascularizationoccurs not only at major ligation sites but alsowherever superficial veins are stripped, avulsed,or injected with adjuvant sclerotherapy.20 Newvessels can extend significant distances in thelower limb to make their reconnections and de-velop varicosities, although this process is stillthe subject of debate and skepticism. Neovascu-larization has been implicated as the cause of re-currence in up to 94% of cases. Occluding the SFJusing an endovascular technique free of the po-tential angiogenic stimuli in conventional surgeryis a very attractive option, at least in theory.20
Early results of EVLT and RFA do suggest thatrecurrence is reduced. Even so, there are reportsof recurrent incompetence at the SFJ and of ul-trasound evidence of neovascularization.21,22
Labropoulos et al found a 5% prevalence of smallarteriovenous fistulas following endovasculartreatments of the GSV. Such fistulas may be re-sponsible for recanalizing ablated venous seg-ments and subsequent recurrence.22 Winterbornet al showed that neovascularization is a dynamicand continuous phenomenon not restricted tothe healing period after surgery. They found in-creasing rates of neovascularization as a cause ofrecurrence: 36%, 54%, and 65% at 2, 5, and 11years of follow-up, respectively.18 Some authorsargue that ligation of competent tributaries isunnecessary and can promote neovasculariza-tion.23 Theivacumar et al showed that despite SFJtributaries remaining patent and competent in59% of 81 EVLT procedures, the overall numberof recurrences did not increase after 1 year offollow-up.24 In conclusion, longer-term resultsfrom prospective randomized studies comparingstripping with new minimally invasive methodsare needed to determine the ultimate fate of theGSV after EVLT and RFA. We still do not know ifSFJ ligation will become the villain or hero. �
U ntil recently, saphenofemoral junction(SFJ) ligation, with or without greatsaphenous vein (GSV) stripping, was con-
sidered the treatment of choice for varicose veinsin the presence of an incompetent GSV, despitethe persistent and unacceptably high recurrencerate after surgery.1-5 Endovenous laser treatment(EVLT) and radiofrequency ablation (RFA) of the GSV have brought new perspectives and newquestions concerning chronic venous disease in-tervention.6 Backed by the success and safety ofthe first published results using these techniques,most practitioners now perform these proceduresin the office setting under vascular ultrasoundguidance without SFJ ligation, to greater patientsatisfaction in terms of simplicity, comfort, andcosmetic outcome.7-11 Nevertheless, the immediatefate of the SFJ after endovenous treatment re-mains unclear, with many questions still unan-swered. What is the real risk of pulmonary em-bolism with these new procedures? What is theexact role of dissection and high ligation of theSFJ as a cause of recurrent varicose veins?
Deep venous thrombosis and pulmonary embolismWith EVLT or RFA, the SFJ can be occluded andligated under direct vision through an inguinalincision, or the catheter can be advanced underduplex scanning control to just below the SFJ,without the inguinal region needing to be surgical-ly accessed. The duplex-guided procedure is sim-pler, faster, and more esthetic, but it carries therisk of extending the thrombus from the SFJ intothe common femoral vein and may cause pul-monary embolism. In the literature, RFA has beenassociated with 21 cases of deep vein thrombosis(DVT) and at least two episodes of pulmonary em-bolism: Hingorani et al reported a 16% incidenceof DVT in 66 patients,12 while Mozes et al esti-mated the cumulative incidence of DVT as 2.1%and of pulmonary embolism as 0.2%.13 As forEVLT, a Mayo Clinic report cited three cases ofDVT, equivalent to 2.3% in 130 treated limbs.14
Conventional varicose surgery was associated with5.7% DVT in 377 patients in a study by van Rijet al.15 Other studies using duplex scanning citedrates of 3% and 5%.16,17 Most cases associatedwith conventional surgery are distal DVT in thecalf veins with a low tendency for propagation,whereas those associated with EVLT and RFA in-volve the protrusion of thrombus originating inthe SFJ into the common femoral vein, represent-ing a theoretical risk of pulmonary embolism.Some reports have advocated the use of temporaryvena cava filters and prophylactic anticoagulation.
10� C. E. Virgini-Magalhães, Brazil
Carlos E. VIRGINI-MAGALHÃES, MDHospital Universitário Pedro Ernesto, Secretaria da Disciplina de CirurgiaVascular e EndovascularBoulevard Vinte e Oito de Setembro 77 sala 448CEP: 20.551-030 Rio de Janeiro, BRAZIL(e-mail: [email protected])
vein reflux after varicose vein surgery. J Vasc Surg. 2005;42:315-320.3. Cheatle T. The long saphenous vein: to strip or not strip?Semin Vasc Surg. 2005;18:10-14.4. Lo YF, Yang CH. Stripping and ligation of the saphenous
REFERENCES1. Stucker M, Netz K, Breuckmann F, Altmeyer P, Mumme A.Histomorphologic classification of recurrent saphenofemoralreflux. J Vasc Surg. 2004;39:816-822.2. Blomgren L, Johanson G, Dahlberg-Akerman A, Thermae-nius P, Berqvist D. Changes in superficial and perforating

C O N T R O V E R S I A L Q U E S T I O N
148 The saphenofemoral junction: to ligate or not to ligate?MEDICOGRAPHIA, VOL 30, No. 2, 2008
dovenous laser therapy and radiofrequency ablation of thegreat saphenous vein: analysis of early efficacy and compli-cations. J Vasc Surg. 2005;42:488-493.15. Van Rij AM, Chai J, Hill GB, Christie RA. Incidence ofdeep vein thrombosis after varicose vein surgery. Br J Surg.2004;91:1582-1585.16. Gillet JL, Perrin M, Hiltbrand B, et al. Pre- and postopera-tive contribution of Doppler ultrasonography in superficialvenous surgery of the popliteal fossa. J Mal Vasc. 1997;22:330-335.17. Puttaswamy V, Fishe C, Applebery M. Venous thrombo-embolism following varicose vein surgery: a prospective anal-ysis. Aust N Z J Surg. 2000;70(suppl). Abstract A150.18. Winterborn RJ, Foy C, Earnshaw JJ. Causes of varicose veinsrecurrence: late results of a randomized controlled trial of strip-ping the long saphenous vein. J Vasc Surg. 2004;40:634-639.19. Wilmer NA, van Blijswik BC, Daí J, et al. VEGFR-3 inadult angiogenesis. J Pathol. 2001;195:490-497.20. van Rij AM, Jones GT, Hill GB, Jiang P. Neovascularizationand recurrent varicose veins: more histologic and ultrasoundevidence. J Vasc Surg. 2004;40:296-302.21. Proebstle TM, Gul D, Lehr HÁ, Kargl A, Knop J. Infrequentrecanalization of greater saphenous vein after endovenouslaser treatment. J Vasc Surg. 2003;38:511-516.22. Labropoulos N, Bhatti A, Leon L, Borge M, Rodriguez H,Kalman P. Neovascularization after great saphenous vein ab-lation. Eur J Vasc Surg. 2006;31:219-222.23. Chandler JG, Pichot O, Sessa C, Schuller-Petrovic S, OsseFJ, Bergan JJ. Defining the role of extended saphenofemoraljunction ligation: a prospective comparative study. J VascSurg. 2001;32:941-953.24. Theivacumar NS, Dellagrammaticas D, Beale RJ, MavorAI, Gough MJ. Fate and clinical significance of sapheno-femoral junction tributaries following endovenous laser abla-tion of great saphenous vein. Br J Surg. 2007;94:722-725.
vein. Semin Cutan Med Surg. 2005;24:200-208.5. Perrin MR, Labropoulos N, Leon LR. Presentation of thepatient with recurrent varices after surgery (REVAS). J VascSurg. 2006;43:327-334.6. Huang Y, Jiang M, Li W, Lu X, Huang X, Lu M. Endovenouslaser treatment combined with a surgical treatment of venousinsufficiency in lower extremity: a report of 208 cases. J VascSurg. 2005;42:494-501.7. Merchant RF, DePalma RG, Kabnick LS. Endovascularobliteration of saphenous reflux: a multicenter study. J VascSurg. 2002;35:1190-1196.8. Lurie F, Creton D, Eklof B, et al. Prospective randomizedstudy of endovenous radiofrequency obliteration (closureprocedure) versus ligation and stripping in a selected patientpopulation (EVOLVeS Study). J Vasc Surg. 2003;38:207-214.9. Agus GB, Mancini S, Magi G. The first 1000 cases of ItalianEndovenous-laser Working Group (IEWG). Rationale, andlong-term outcomes for the 1999-2003 period. Int Angiol. 2006;25:209. Abstract.10. Sharif MA, Soong CV, Lau LL, Corvan R, Lee B, Hannon RJ.Endovenous laser treatment for long saphenous vein incom-petence. Br J Surg. 2006;93:831-835.11. Rasmussen LH, Bjoern L, Lawaetz M, Blemings A,Lawaetz B, Eklof B. Randomized trial comparing endovenouslaser ablation of the great saphenous vein with high ligationand stripping in patients with varicose veins: short-term results. J Vasc Surg. 2007;46:308-315.12. Hingorani AP, Ascher E, Markevich N, et al. Deep venousthrombosis after radiofrequency ablation of greater saphe-nous vein: a word of caution. J Vasc Surg. 2004;40:500-504.13. Mozes G, Kalra M, Carmo M, Swenson L, Gloviczki P. Ex-tension of saphenous thrombus into the femoral vein: a poten-tial complication of new endovenous ablation techniques. J Vasc Surg. 2005;41:130-135.14. Puggioni A, Kalra M, Carmo M, Mozes G, Gloviczki P. En-

mitted to peaks of pressures, generated in this caseby abdominal pressure. Both components are pro-foundly influenced by the action of the venousvalves.
Many factors may play a role in raising hydro-static pressure in the superficial venous system ofthe lower limbs; in particular, prolonged standingor sitting occupations, pathologic conditions of in-creased abdominal pressure and decreased calf pumpas is found in morbid obesity, and hormonal status.3
Genetic inheritance must be considered, becauseCVD is seen in patients with a family history of vari-cose veins.4,5 In line with the observations regard-ing genetic influence, a deficiency has been foundin collagen type III in cultured venous smooth mus-cle cells from patients with varicose veins.6 The de-fect was found to be generalized within differenttissues in the same patients. One of the theoriesthus put forward regarding the development of vari-cose veins is that the veins of affected individualsare genetically more distensible than those of peo-ple with normal veins.2
Chronic venous disease (CVD) is an umbrellaterm that encompasses a variety of clinicalpresentations, which include venous symp-
toms and signs. A review of the literature shows thatthe most commonly expressed CVD-related symp-toms are heaviness, pain, sensation of swelling, rest-less legs, paresthesias, night time cramps, tiredness,throbbing, and itching. The signs of chronic venousdisorders are described in the Clinical, Etiological,Anatomical, Pathophysiological (CEAP) classifica-tion1 and comprise telangiectasia, varicose veins,edema, skin changes, and healed and active venousleg ulcers.
It seems likely that the progression of CVD stemsfrom prolonged periods of increased venous pres-sure in the legs. The abnormally elevated venouspressure is called venous hypertension, and thislinks all theories regarding the pathogenesis of thedisease.2
Hypertension is central to the pathogenesis of chronic venous disease
During periods of standing without skeletal mus-cle activity, venous pressures in the legs are deter-mined by capillary flow and the hydrostatic com-ponent that is related to the weight of the columnof blood from the right atrium to the foot. The pres-sure may reach 80 to 90 mm Hg. In addition to thehydrostatic component, distal veins are submittedto transiently increased pressures generated by con-tractions of the skeletal muscles of the leg that mayreach 150 mm Hg. Proximal veins may also be sub-
149Daflon 500 mg: protective against venous valve failure – Pitsch MEDICOGRAPHIA, VOL 30, No. 2, 2008
D A F L O N 5 0 0 M G
P rimary chronic venous disease is a widespread disorder.Its manifestations include symptoms in the form of painand heaviness, and signs in the form of telangiectasia,
varicose veins, skin changes, and chronic leg ulcers. Recent ad-vances in the understanding of its pathophysiology have shownthat molecular mechanisms in the inflammatory cascade under-lie these diverse manifestations. Venous hypertension and alter-ation of hemodynamic forces, such as blood pressure changes inthe wall and sheer stress, induce activation of leukocytes andendothelial cells. This may initiate the cascade of inflammationthat results in adverse changes in the venous valve, venous wall,and skin and leads to the many clinical manifestations of the dis-ease. The disease symptoms and the telangiectasia, varicose veins,and eventual venous leg ulcers appear to be a consequence of thechanges induced by venous hypertension and shear stress. Treat-
ment to inhibit inflammation may offer the greatest opportunityto prevent progression of the disease and its related complica-tions. Daflon 500 mg, an oral phlebotropic medication, attenuatesvarious elements of the inflammatory cascade, particularly theleukocyte-endothelium interactions that are important in manyaspects of the disease. Such medication deserves more detailedstudy to confirm its protective effect on venous structures. Medicographia. 2008;30:149-153. (see French abstract on page 153)
Keywords: primary chronic venous disease; venous valve failure; inflammatory cascade; leukocyte-endothelium inter-action; protective effect; Daflon 500 mg
DAFLON 500 MG: PROTECTIVE AGAINSTVENOUS VALVE FAILURE
b y F. P i t s c h , F r a n c e
Address for correspondence: Françoise Pitsch, Servier International, 192 avenue Charles de Gaulle, 92578 Neuilly-sur-Seine Cedex, France(e-mail: [email protected])
SELECTED ABBREVIATIONS AND ACRONYMS
AVF arteriovenous fistula CEAP Clinical, Etiological, Anatomical,
Pathophysiological classificationCVD chronic venous diseaseRELIEF Reflux assEssment and quaLity of lIfe
improvEment with micronized Flavonoids (study)
Françoise PITSCHServier International
Neuilly-sur-Seine FRANCE

To elucidate the possible mechanisms involvedin the destruction of valves in chronic venous hy-pertension, Takase et al examined saphenous veinvalves in a rat model in which femoral venous hy-pertension was elevated for a period of 3 weeks by afemoral arteriovenous fistula (AVF).15 In this mod-el, venous reflux developed in response to venoushypertension. Examination of vein morphology re-vealed that valve failure occurred as a result of di-lation of the venous wall and shortening of valveleaflets to the point of incomplete valve closureand subsequent reflux. Assessment of the valves formolecular inflammatory markers revealed enhancedleukocyte infiltration with granulocytes, monocytes,and T-lymphocytes. In addition, the expression ofthe endothelial cell membrane adhesion moleculesP-selectin and ICAM-1 on the endothelial cells of thesaphenous vein wall was increased. In this study, theleaflets were still able to close properly in the earlystages after placement of the AVF, suggesting thatpressure per se is not necessarily the variable thatcan compromise the leaflets. However, at the timethe leaflets failed and reflux occurred, a reduction inthe leaflet dimensions was observed. A possible ex-planation for the sequence of events that leads tothe morphologic abnormalities in venous valvesis that as the venous wall dilates, a point may bereached at which reflux develops across the leaflets.An abnormal fluid shear field produced at the sur-face of the leaflets during venous reflux would behighly inflammatory for the endothelial cells on thevalve leaflets, and could trigger destruction of theleaflets, increasing venous hypertension. This wouldmaintain a vicious circle of venous hypertension/venous inflammation (Figure 1).
The inflammatory reaction in chronic venous disease might be
a new target for drugs
Intervention in the inflammatory reaction that oc-curs as part of the progress of the disease may be anew pharmacological target. For this reason, themodel by Takase et al was used to assess the effectof a drug treatment: Daflon 500 mg*.
There might also be a genetic component to thealteration of remodeling in venous valves. A theorylinking the various observations to describe thechronology of venous valve failure and venous in-sufficiency is, however, lacking.
A strong link is evoked between venous hypertension and valve failure
In most cases, venous hypertension is caused by re-flux through incompetent venous valves.7 Exami-nation of surgical specimens removed from limbswith chronic venous insufficiency and, more re-cently, the direct observation offered by angioscopy,has revealed lesions involving the venous wall, thevalvular annulus, and the valve cusps.8,9 Failure ofthe valve and its annulus is responsible for progres-sion of the disease via maintenance and furtherincrease of venous hypertension. Immunohisto-chemical studies using monoclonal antibodies spe-cific for monocytes and macrophages have demon-strated monocyte/macrophage infiltration into thevalve leaflets and venous wall of patients with vari-cose veins (CEAP Class 2).10 Monoclonal antibodystudies have found that leukocyte infiltration isgreater within the base of the valve leaflets and inthe proximal venous wall. Venous valves have beenfound to be prominent in regions of low shear stresswith venous eddies and recirculation.11 It may bethat these phenomena explain how the leukocytesare preferentially deposited in these regions.
Ultimately, macrophages become the instrumentof tissue damage that softens the venous wall andfavors valve destruction.12 Venous valve failure andsubsequent reflux causing distal venous hyperten-sion may contribute to the sustained and chronichypertension that is responsible for leukocyte ac-tivation within the endothelium and leukocyte de-struction of skin and subcutaneous tissues at theankle. In addition to leukocyte activation, increasedmast cell infiltration into the venous wall may havea role to play in the development of varicose veins.Increased expression of intercellular adhesion mole-cule–1 (ICAM-1) and the presence of CD-68 on theendothelial surface of venous walls in patients withvenous insufficiency has been confirmed and maybe related to this.12 These findings suggest a contin-uing inflammatory reaction that is related to ve-nous wall remodeling.13,14 On the other hand, endo-thelial cells must be activated to allow leukocytesto migrate through the cells into the tissue.12 It isbelieved that endothelial stretching may induceactivation of the endothelium; as blood flow itself isaffected, fluid shear stress may change. Fluid shearstress is a key regulatory component of endothelialcells and a reduction in shear rates leads to enhancedadhesion of leukocytes on the endothelium.10
Clinical observations are confirmed by animal models
Since the mechanisms responsible for venous valvefailure in primary CVD cannot be investigated invivo in human beings, animal models were set upfor the purpose of experimental research.
D A F L O N 5 0 0 M G
150 Daflon 500 mg: protective against venous valve failure – PitschMEDICOGRAPHIA, VOL 30, No. 2, 2008
Venous hypertension Venous dilation
Increased hypertension
Increased inflammation Skin changes
Capillary leakage
Capillary hypertension
Valve and wall changes
Edema
Ulcer
INFLAMMATION
Risk factors for chronic venous disease
Altered blood flow and shear stress
Valve distortion and leakage
Valve reflux
*Also registered as Ardium®,Alvenor®, Arvenum® 500,
Capiven®, Detralex®, Elatec®,Flebotropin®, Variton®,
and Venitol®.
Figure 1. The vicious circle of venous hypertension/venous inflammation.Adapted from reference 7:Bergan JJ, Schmid-SchönbeinG, Coleridge-Smith P, Nico-laides A, Boisseau M, Eklof B.Chronic venous disease. N Engl J Med. 2006;355:488-498. Copyright © 2006,Massachusetts Medical Society.

score) and separated symptom scores (P value dif-ferent depending on the symptom, from P<0.001for functional discomfort to P=0.033 for sensationof burning). In this trial, the presence of venous dis-ease and treatment efficacy were confirmed by test-ing parameters using strain gauge plethysmogra-phy and edema measurement.
Another double-blind, placebo-controlled, ran-domized study20 included 160 symptomatic patientswith CVD related to either post-thrombotic syn-drome (24 patients), primary varicose veins (59 pa-tients) or other conditions (77 patients). Patientswere equally distributed into 2 groups and treatedeither with placebo or with Daflon 500 mg, 2 tabletsdaily for 8 weeks. Evaluation of venous symptomswas the primary end point of the study. Each symp-tom (functional discomfort, heaviness, pain, nightcramps, sensation of swelling, paresthesia, redness
and/or cyanosis, sensation of heat and/or burning)was rated 0 (no symptom), 1 (moderate symptomswithout repercussion on daily activities), 2 (appre-ciable symptoms but allowing daily activities) or 3(severe symptoms, causing discomfort or hamper-ing daily activities). At the end of the study andcompared with the placebo group, the changes inthe symptoms were significantly better in the Daflon500 mg group (from P<0.001 for functional discom-fort, sensation of heaviness, and sensation of swell-ing, up to P=0.027 for pain; the only symptom with-out significant improvement was redness/cyanosis).Thesechangesweresignificant after 4weeks of treat-ment for the functional discomfort, sensation ofheaviness, nocturnal cramps, and sensation of swell-ing. Improvement in other objective parameters ofedema and trophic skin changes paralleled the im-provement in symptoms.
The Reflux assEssment and quaLity of lIfe im-provEment with micronized Flavonoids (RELIEF)study21 involved 5052 symptomatic patients from
The ability of Daflon 500 mg to mitigate or evenblock the effects of chronic inflammation at the lev-el of both the micro- and macrocirculation has beendemonstrated in rat models of venous hypertension.In a model of venous occlusion and reperfusion, thesubsequent elevation of venous blood pressure in-creased the inflammatory cascade and tissue in-jury.16 In Daflon 500 mg–treated animals, markersof inflammation were decreased in a dose-depen-dent manner. Daflon 500 mg also served to signif-icantly reduce parenchymal cell death as well as leu-kocyte rolling, adhesion to postcapillary venules,and migration.17
Important data supporting the protective effectof Daflon 500 mg at the level of the macrocircula-tion have been provided by the rat fistula model ofvenous hypertension.15 In this model, the venoushypertension caused by a femoral AVF resulted inthe development of venous reflux and an inflamma-tory reaction in venous valves. In animals treatedwith Daflon 500 mg, there was a significant, dose-dependent reduction in the reflux rate (Figure 2).Daflon 500 mg also reduced several indicators ofthe inflammatory reaction including expression ofthe endothelial cell adhesion molecules, P-selectinand ICAM-1, and leukocyte infiltration, and reducedthe level of apoptosis in a dose-dependent manner.By delaying and even blocking the inflammatoryreaction, these data suggest that Daflon 500 mg maydelay the development of reflux and suppress dam-age to the valve structures in the rat model of ve-nous hypertension. These observations were recent-ly confirmed in a new study using the same animalmodel. The administration of Daflon 500 mg re-duced the edema and the fistula blood flow pro-duced by the acute AVF. Daflon 500 mg also reducedgranulocyte and macrophage infiltration to thevalves, in line with the previous study.18 Daflon500 mg may be protective against valve alterations.
Therapeutic consequences of the protective effect of Daflon 500 mg
Daflon 500 mg is the only venoactive drug withproven early protective properties on venous valvesand the venous wall. This is probably one of themechanisms by which Daflon 500 mg is efficientright from the early symptoms of CVD.
In one double-blind, placebo-controlled, random-ized study19 including 40 patients with CVD, sever-al symptoms were considered, and were classifiedinto “functional” symptoms (functional discomfort,leg heaviness, pain, fatigue when standing, nightcramps, paresthesia, burning sensation, itching)and “objective” symptoms (sensation of edema inthe evening, redness and cyanosis, sensation of heat,and sensation of skin induration). According to theintensity of each parameter and its repercussion ondaily activities, the patient quantified the parame-ters using a 4-point scale. Global scores were calcu-lated for functional and objective symptoms. In theDaflon 500 mg group, after a 2-month period oftreatment, patients demonstrated a significantlybetter improvement in global (P<0.001 for func-tional score and P=0.034 for objective symptom
D A F L O N 5 0 0 M G
151Daflon 500 mg: protective against venous valve failure – Pitsch MEDICOGRAPHIA, VOL 30, No. 2, 2008
Figure 2. Reflux flow rates across the saphenous venousvalve measured after 3 weeks of venous hypertensionin vehicle control and Daflon 500 mg treatment groupsat a dose of 50 mg/kg/day and 100 mg/kg/day. N is thenumber of rats in each treatment group. P<0.05 com-pared with control. MPFF, micronized purified flavonoidfraction.Reproduced from reference 15: Takase S, Pascarella L, Bergan J,Schmid-Schönbein G. Venous hypertension, inflammation and valveremodeling. Eur J Vasc Endovasc Surg. 2004;28:484-493. Copy-right © 2004, Elsevier Ltd.
12
10
8
6
4
2
0
Free
ref
lux
rate
(mL/
min
)
Vehicle (n=6)
MPFF 50 (n=6)
MPFF 100 (n=6)

nous insufficiency. (chronic venous insufficiencyimplies that reflux is present). Although other the-ories exist, the fundamental cause of skin damagein CVD has been ascribed to leukocyte trapping, ad-hesion of leukocytes to the endothelium and neu-trophils, and their subsequent activation.23 It ishypothesized that the primary injury to the skin iscaused by extravasation of macromolecules such asfibrinogen, α-macroglobulin, and red blood cellsinto the dermal interstitium. Red blood cell degra-dation products and interstitial protein extravasa-tion are potent chemoattractants and presumablypresent the initial inflammatory signal that resultsin leukocyte recruitment and migration into thedermis.5 The cascade of pathologic events occursduring leukocyte migration into the dermis, and theend product of these is dermal fibrosis.
Systemic medications have been used in additionto standard treatments, because of a theoretical abil-ity to address one or more of the factors that havebeen identified in the pathophysiology of venous ul-ceration. A small number of drugs have been usedwith varying success. The way in which Daflon 500mg speeds ulcer healing might be to modulateleukocyte-L-selectin interaction with endothelialselectins responsible for the initial stages of adhe-sion. By reducing the likelihood of leukocyte adhe-sion, Daflon 500 mg presumably acts through ananti-inflammatory mechanism.24 Thus, among themany mechanisms at work in the pathogenesis ofvenous ulceration, the mechanism involving leu-kocyte activation and interaction with the endothe-lium seems currently to be the one most responsiveto pharmacological treatment.
A meta-analysis of randomized prospective stud-ies using Daflon 500 mg in adjunction to conven-tional treatment confirmed the results of previoustrials; namely, that such oral medication acceleratesthe healing of leg ulcers.25 Five prospective, ran-domized, controlled studies involving 723 patientswith venous ulcers who had received treatment be-tween 1996 and 2001 were included in the analy-
23 countries treated for 6 months with Daflon 500mg. In this study, the sensation of swelling, cramps,and leg heaviness were assessed by a 4-point scale(0=absent, 1=mild, 2=significant, 3=severe). Painwas measured using a 10 cm visual analog scale (0representing “no pain” and 10 cm “maximal pain”).All symptoms showed a significant and progressiveimprovement. Improvement in the patients’ qual-ity of life was paralleled by symptom improvement(Figure 3).
Daflon 500 mg has demonstrated its efficacy onsymptoms in the long term. Two tablets of Daflon500 mg daily maintained its efficacy in the long-term treatment of patients with symptoms of CVDin a nonblind, multicenter trial of 12 months’ dura-tion.22 In this 1-year trial in 170 evaluable patients,a significant reduction from baseline values inphysician-assessed clinical symptoms (functionaldiscomfort, cramps, and evening edema), ankle andcalf circumference, and patient overall assessmentof symptom severity was demonstrated at each 2-month evaluation (P<0.001). The rapid reductionsobserved during the first 2 months of treatment rep-resented approximately 50% of the total improve-ments ultimately observed after 1 year of treatment.
The skin is the final target of chronic venous hypertension
The complications of CVD are expressed in the skinand are related to chronic venous hypertension. Theskin is the final target of chronic venous hyperten-sion. The hypertension is a cause of chronic inflam-mation manifested by persistent and sustained in-jury. Ultimately it is the capillary circulation thatis most severely impaired in limbs with chronic ve-
D A F L O N 5 0 0 M G
152 Daflon 500 mg: protective against venous valve failure – PitschMEDICOGRAPHIA, VOL 30, No. 2, 2008
Figure 3. Improvement in health-related quality-of-life scores with Daflon500 mg. Improvements in the global index score of the ChronIc Venous In-sufficiency Questionnaire (CIVIQ) with two tablets of Daflon 500 mg dailyfor 6 months in 3656 patients with symptoms of chronic venous disease withor without venous reflux able to be evaluated in an unblinded multinationalstudy. CIVIQ scores range from 0-100 where 100 indicates a very good health-related quality of life. *P=0.0001 versus baseline.Reproduced from reference 21: Jantet G; the RELIEF Study Group. Chronic venous insuffi-ciency—worldwide results of the RELIEF study. Angiology. 2002;53:245-256. Copyright ©2002, Sage Publications.
Figure 4. Life-table analysis showing the cumulative percentage of patientswith complete ulcer healing. Comparison of cumulative healing rates betweenthe Daflon 500 mg group (green line) and the control group (gray line).Adapted from reference 25: Coleridge-Smith P, Lok C, Ramelet AA. Venous leg ulcer : a meta-analysis of adjunctive therapy with micronized purified flavonoid fraction. Eur J Vasc EndovascSurg. 2005;30:198-208. Copyright © 2005, Elsevier Ltd.
190
80
70
60
50
40
30
20
10
0
**
*
Glo
bal i
ndex
sco
re o
n C
IVIQ
(poi
nts)
Patients withvenous reflux
Patients withoutvenous reflux
**
*Baseline
Month 2Month 4
Month 6
Time to recovery (weeks)
Prob
abili
ty
Control1.0
0.8
0.6
0.4
0.2
00 6 12 18 24 30 36
Daflon 500148209
349TreatmentEventsPatients
372

Venous valve protection is to be closely studied since it opens up
the perspective of targeted pharmacological intervention
The practical purpose of elucidating the molecularsteps involved in the development of valve lesionsis to intervene with a targeted treatment. The se-quence of leukocyte adhesion, endothelial interac-tion, activation, and migration and its associationwith valvular damage has focused attention onavailable molecules with known ability to modifythis chain of events.
Daflon 500 mg currently possess the most appro-priate profile, since the previously published obser-vations of an anti-inflammatory effect of Daflon 500mg under acute situations show that it may havea protective effect on the venous valves in chronicconditions of venous hypertension. �
sis. Conventional treatment (compression and localcare) in addition to Daflon 500 mg was comparedwith conventional treatment plus placebo in twostudies (n=309), and with conventional treatmentalone in three studies (n=414). The primary endpoint was complete ulcer healing at 6 months. Theresults were expressed as a reduction in the relativerisk (RRR) of healing, which should be positive toindicate a benefit for adjunctive Daflon 500 mgtherapy over conventional therapy alone. At 2months, the results were statistically significantand the chance of an ulcer healing was 44% betterin patients treated with adjunctive Daflon 500 mgthan in those managed by conventional therapyalone (RRR, 44%; confidence interval [CI], 7%-94%;P=0.015). This difference was present at month 6(RRR, 32%; CI, 3%-70%; P=0.0035), and was asso-ciated with a shorter time to healing (16 weeks vs21 weeks; P=0.0034) (Figure 4).
D A F L O N 5 0 0 M G
153Daflon 500 mg: protective against venous valve failure – Pitsch MEDICOGRAPHIA, VOL 30, No. 2, 2008
REFERENCES1. Porter JM, Moneta GL; International ConsensusCommittee on Chronic Venous Disease. Reportingstandards in venous disease: an update. J Vasc Surg.1995;21:635-645.2. Nicolaides AN. Investigation of chronic venous in-sufficiency; a consensus statement. Circulation.2000;102:e126-e163.3. Pascarella L, Schmid-Schönbein G. Causes of telan-giectasias, reticular veins, and varicose veins. SeminVasc Surg. 2005;18:2-4.4. Cornu-Thénard A, Boivin P, Baud JM, et al. Impor-tance of the familial factor in varicose disease. Clin-ical study of 134 families. J Dermatol Surg Oncol.1994;20:318-326.5. Pistorius MA. Chronic venous insufficiency: the ge-netic influence. Angiology. 2003;54:S5-S12.6. Sansilvestri-Morel P, Rupin A, Jaisson S, et al. Syn-thesis of collagen is dysregulated in cultured fibrob-lasts derived from skin of subjects with varicose veinsas it is in venous smooth muscle cells. Circulation.2002;106:479-483.7. Bergan JJ, Schmid-Schönbein G, Coleridge-SmithP, Nicolaides A, Boisseau M, Eklof B. Chronic venousdisease. N Engl J Med. 2006;355:488-498.8. Corcos L, De Anna D, Dini M, Macchi C, Ferrari PA,Dini S. Proximal long saphenous vein valves in pri-mary venous insufficiency. J Mal Vasc.2000;25:27-36.9. Van Cleef JF, Hugentobler JP, Desvaux P, Griton P,Cloarec M. Endoscopic study of reflux of the saphe-nous valve. J Mal Vasc. 1992;17(suppl B):113-116.
tite Meeting of the European Venous Forum, June 29-July 1, 2006. London, England: Edizioni Minerva Med-ica (Turin) ;2006:16.19. Chassignolle JF, Amiel M, Lanfranchi G, et al. Acti-vité thérapeutique de Daflon 500mg dans l’insuffisanceveineuse fonctionnelle. JIM. 1987;99(suppl): 32-35.20. Gilly R, Pillion G, Frileux C. Evaluation of a newvasoactive micronized flavonoid fraction (S 5682) insymptomatic disturbances of the venolymphatic cir-culation of the lower limb: a double-blind, placebo-controlled study. Phlebology. 1994;9:67-70.21. Jantet G; the RELIEF Study Group. Chronic ve-nous insufficiency—worldwide results of the RELIEFstudy. Angiology. 2002;53:245-256.22. Guillot B, Guilhou JJ, de Champvallins M, et al. Along term treatment with a venotropic drug: resultson efficacy and safety of Daflon 500 mg in chronic ve-nous insufficiency. Int Angiol.1989;8(suppl 4):67-71.23. Coleridge-Smith PD, Thomas P, Scurr JH, Do-mandy JA. Causes of venous ulceration: a new hypoth-esis. BMJ.1988;296:1693-1695.24. Shoab SS, Porter J, Scurr JH, Coleridge-SmithPD. Endothelial activation response to oral micro-nised flavonoid therapy in patients with chronic ve-nous disease—a prospective study. Eur J Vasc Endo-vasc Surg. 1999;17:313-318.25. Coleridge-Smith P, Lok C, Ramelet AA. Venous legulcer : a meta-analysis of adjunctive therapy with mi-cronized purified flavonoid fraction. Eur J Vasc En-dovasc Surg. 2005;30:198-208.
10. Ono T, Bergan JJ, Schmid-Schönbein GN, TakaseS. Monocyte infiltration into venous valves. J VascSurg.1998;27:158-166.11. Lurie F, Kistner RL, Eklof B, Kessler D. Mechanismof venous valve closure and role of the valve in circu-lation: a new concept. J Vasc Surg. 2003;38:955-96112. Takase S, Bergan JJ, Schmid-Schönbein GW.Expression of adhesion molecules and cytokines onsaphenous veins in chronic venous insufficiency. AnnVasc Surg. 2000;14:427-435.13. Jacobs MP, Badier-Commander C, Fontaine V, etal. Extracellular matrix remodeling in the vascularwall. Pathol Biol. 2001;49:326-332.14. Badier-Commander C, Jacobs MP, Michel JB. Vari-cose remodeling [translated from French]. MT. 2000;6:718-723.15. Takase S, Pascarella L, Bergan J, Schmid-Schön-bein G. Venous hypertension, inflammation and valveremodeling. Eur J Vasc Endovasc Surg. 2004;28:484-493.16. Takase S, Lerond L, Bergan JJ, Schmid-Schön-bein GW. Enhancement of reperfusion injury by ele-vation of microvascular pressures. Am J Physiol HeartCirc. 2002;282:H1387-H1394.17. Takase S, Delano FA, Lerond L, et al. Inflammationin chronic venous insufficiency: is the problem in-surmountable? J Vasc Res. 1999;36(suppl 1):3-10.18. Pascarella L, Lulic D, Alsaigh T, et al. Venous hy-pertension induced venous insufficiency amelioratedby Daflon 500 mg. In: Book of Abstracts of the Tripar-
DAFLON 500 MG : PROTÈGE CONTRE LA MALADIE VALVULAIRE VEINEUSE
L a maladie veineuse chronique essentielle est très répandue.Elle est définie par la présence de symptômes tels que dou-leurs et lourdeurs de jambes, et/ou de signes tels que télan-
gectasies, varices, troubles trophiques et ulcère veineux. La phy-siopathologie de cette maladie reste encore mal connue mais derécentes avancées ont mis le doigt sur le rôle déterminant des mé-canismes inflammatoires dans son déclenchement et sa progres-sion. L’action conjuguée de l’hyperpression veineuse et des mo-difications des forces hémodynamiques exercées sur la paroi desveines et des valves peuvent induire une activation des leucocyteset de l’endothélium pariétal, initiant une cascade inflammatoire.Il en résulte un profond remaniement des structures valvulaireset pariétales, puis des capillaires de la peau, ce remodelage se tra-duit par les diverses manifestations cliniques décrites dans cettemaladie. Ainsi les symptômes veineux, les télangectasies, les va-
rices puis les complications ulcéreuses sont-ils la conséquencedes changements induits par les modifications des forces hémo-dynamiques et de pression. Le rôle prédominant de l’inflamma-tion dans la genèse et la progression de cette maladie pourraitavoir d’importantes implications thérapeutiques. Des traitementspharmacologiques capables d’enrayer le cercle vicieux de l’in-flammation permettraient de prévenir les complications. Daflon500 mg, un phlébotrope largement utilisé dans le traitement dessymptômes et de l’œdème liés à la maladie veineuse, a démontrésa capacité à atténuer l’inflammation veineuse, et plus particu-lièrement l’intéraction leucocyte-endothélium dont on connaîtl’impact dans le mécanisme de développement de la maladie. Cemécanisme d’action prometteur nécessite d’être approfondi pourconfirmer les effets protecteurs du produit sur les structures vei-neuses et plus particulièrement les valves.

154 Animal models in chronic venous disease – JonesMEDICOGRAPHIA, VOL 30, No. 2, 2008
a consistent pattern radiating out fromthe saphenous vein. These veins progres-sively enlarge, resulting in the formationof an extensive network of large (1-5 mmin diameter), tortuous, superficial vari-cose veins overlying the medial thighand extending into the superficial epigas-tic veins. Although animals are initiallyoperated upon at a body weight of 35 kg,they grow rapidly and are typically 80 to100 kg by the time measurements aremade (8-15 weeks postoperatively). Anadvantage of this model is that the sizeof the animal and associated veins allowsfor physiological (pressure and ultra-sound) evaluation, which would not bepossible in smaller animals.
Physiologically, these vessels are char-acterized by retrograde flow with a mildnonpulsatile venous hypertension (20-35 mm Hg in a supine position). Venouspressures decline with increased distancefrom the fistula-fed saphenous vein. In-creased intra-abdominal pressure elevates
oped by other investigators, and there isa need to be very clear as to which con-dition each model is trying to mimic.
Our model, which is of the chronic su-perficial varicose vein, involves the fash-ioning of a femoral arteriovenous fistulain adult pigs. The fistula is fashionedadjacent to the intact saphenofemoraljunction (SFJ). It is interesting that inthe pig, the saphenous vein is formed bysuperficial tributaries and passes moredeeply into its own fascial compartmentin the thigh before penetrating the fasciacribrosa and joining the femoral vein.Unlike the human situation, the saphe-nous vein runs parallel to a small saphe-nous artery, forming a saphenous bun-dle within its own fascia. What is alsoslightly unusual about the pig is that thisparticular length of saphenous vein hasnumerous (8-10) valves. We believe thatthese valves are critical to the model, asthey appear to fail sequentially followingcreation of the femoral fistulae. As such,they appear to “protect” the vessels with-in the superficial compartment from di-rect arterialization in the acute phase offistula maturation. After approximately1 to 2 weeks, the superficial saphenoustributaries begin to become varicose in
Tell us about the animal model youhave set up
Our group is interested in thepathobiology of varicose veins.
In order to study the complete timecourse of this condition, it is necessaryto examine veins early in their pathogen-esis and preferably with reference tocontrol material. Clearly it is not possibleto use human material for such studies,and a suitable animal model has, there-fore, been sought. Unfortunately varicoseveins do not occur spontaneously in low-er animals1 and it has been necessary todevelop experimental animal models inan attempt to mimic the human state. Assuch, we have aimed to establish a chron-ic, large animal model of primary super-ficial varicose veins. It is important to beaware that there have been a number ofanimal models for venous disease devel-
I N T E R V I E W
P revious animal models of venous disease, while suited tothe study of venous hypertension and valvular insufficien-cy, do not produce superficial varicose veins. Our group
aimed to develop a pig-based model of superficial varicose veins.The pathophysiology of this model was assessed by intravenousblood pressure measurement, duplex ultrasound, and histolo-gy, and was compared with that of the human condition. Rightfemoral arteriovenous fistulae were surgically fashioned in adultpigs. Patency of the fistulae was confirmed by transcutaneousultrasound. Animals were re-examined postoperatively for up to15 weeks to determine both pressure and blood flow velocitieswithin the superficial thigh veins. Histology was used to char-acterize the resulting structural venous alterations with thoseof human superficial varicose veins. In this model, gross superfi-cial varicosities developed after an initial lag period of1 to2 weeks.Varices appeared to have a postural component to their filling andwere associated with a mild (nonpulsatile) venous hypertension.This physiological profile is distinct from the near-arterial pres-
sure profiles typically observed in smaller animals with arteri-ovenous fistulae. Venous blood flow velocities were elevated to15 to 25 cm/second in varicose veins. Structurally, pig varicoseveins were enlarged, tortuous, had focal medial atrophy with orwithout overlying intimal thickening, and valvular degenera-tion. In conclusion, the superficial varicose veins, which developedwithin this porcine model, have a pathophysiology that is consis-tent with that observed in humans. The suitability of other ani-mal models of venous disease for the evaluation of therapeuticagents for the treatment of varicose veins is discussed.Medicographia. 2008;30:154-156. (see French abstract on page 156)
Keywords: animal model; arteriovenous fistula; chronic venousdisease; superficial varicose vein; therapeutic evaluation
ANIMAL MODELSIN CHRONIC VENOUS DISEASE
I n t e r v i e w w i t h G . T . J o n e s , N e w Z e a l a n d
Gregory Thomas JONES,PhDVascular Research GroupOtago Medical SchoolOtago, NEW ZEALAND
Address for correspondence: Gregory T. Jones, Research Director, Vascular Research Group, Otago Medical School, New Zealand.(e-mail: [email protected])
SELECTED ABBREVIATIONS AND ACRONYMS
AVF arteriovenous fistulaeSFJ saphenofemoral junction

I N T E R V I E W
155Animal models in chronic venous disease – Jones MEDICOGRAPHIA, VOL 30, No. 2, 2008
that was associated with sustained rest-ing and ambulatory pressures.5 Unfortu-nately, the associated acute phase arte-rial pressure profile is inconsistent withchronic venous disease. More important-ly, none of these AVF venous diseasemodels have reported the formation ofassociated superficial varicose veins.
Models combining the above mecha-nisms have also been developed. Mostnotably, the combination of AVF and out-flow obstruction has been used in orderto produce sustained venous hyperten-sion. Van Bemmelen applied this modelto rats in order to study valve remodel-ing.8 Although valve incompetence andremodeling were noted as early as 24hours postoperatively, no pressure pro-files were recorded and the animals didnot develop varicosities. More recently,a detailed series of studies conducted byBergan’s group has utilized the samemodel and reported arterial-like pressureprofiles with mean venous pressures inthe order of 100 mm Hg.9 Vein alterationsreported included media atrophy, wallfibrosis, increased protease expression,progressive valve degeneration, and dila-tion of the commissures. Using this ratmodel, valvular inflammation has beenidentified as a key pathologic feature inthe development of reflux.9
What does this new model bring thatthe others did not?
The principal feature of the pigfemoral AVF model is the for-
mation of chronic superficial varicoseveins. Such pathological changes havenot been reported in any previous mod-el of venous disease. The heterogenousvenous pathohistology of this model isconsistent with the range of alterationsobserved in human superficial varicoseveins, including medial atrophy, intimalthickening, connective tissue degenera-tion, fibrosis, and chronic valvular de-generation. These changes appear to bedue to physiological alterations that arenot simply an acute arterialization, butare more consistent with that associatedwith chronic varicose veins in humans.Venous filling has an intermittent pattern,influenced by posture, and driven by amild nonpulsatile venous hypertension.
The use of a human sized experimen-tal animal allows for a greater range ofphysiological evaluations to be performedand results in much larger tissue vol-umes for biochemical evaluation.
Another exciting feature is the sugges-tion that venular changes also occur inthe draining tissues, comparable withsome of the changes seen in chronic
Tell us about previous animal modelsof venous disease
Previous animal models of ve-nous disease can be categorized
into four groups; those utilizing (i) ves-sel occlusion/obstruction; (ii) valvularincompetence; (iii) augmented hemody-namics; or (iv) a combination of thesemodels. Depending on the desired out-come, each method has its own strengthsand weaknesses. Our approach has beento focus on the development of a modelof varicose veins, and only secondarilyon the generation of the tissue changesof chronic venous insufficiency. Unfor-tunately, other models have not achievedthis, although they have contributed tothe study of other venous conditions,such as acute venous obstruction, throm-bophlebitis or valvular insufficiency.
Since chronic venous hypertension is widely accepted as a key pathologicalmechanism of chronic venous insuffi-ciency, venous occlusion models havebeen employed in an attempt to raisevenous pressures by limiting outflow.Despite an acute elevation, venous occlu-sion models in themselves do not appearto maintain chronically elevated venouspressures.5,6 Burnand concluded thatthis was due to the formation of collat-eral drainage, which he demonstratedon phlebograms.5
Valvular incompetence is a commonfeature of chronic venous insufficiency.Lalka, Dalsing, and colleagues7 describeda simple, reproducible model of hind-limb valve disruption (in the greyhound)that represents a useful model of venousvalvular insufficiency, particularly in theevaluation of valve reconstruction pro-cedures. Animals developed an immedi-ate increase in post-stimulation seg-mental venous pressure that persistedfor as long as 14 weeks. While phlebog-raphy demonstrated reflux in the seg-ments with the disrupted valves, therewas no indication of extension into trib-utaries and no evidence of varicose veins,even at the most chronic time point.Other aspects that should be consideredwhen assessing this model’s suitabilityinclude the acute nature of the valve de-generation, which abruptly exposes thevein to increased pressure, and the rela-tively short hydrostatic column presentin the quadruped hind limb. The thirdgroup of venous disease models involvesthe fashioning of arteriovenous fistulae(AVF). Dart and colleagues formed acuteAVF in the dog, but noted an arterializedpressure profile within the distal veins.Burnand produced a more mild chronicvenous hypertension in the greyhound
superficial venous pressures. Supine su-perficial venous blood flow velocities wereelevated from approximately 1 to 4 cm/second in controls to 15 to 25 cm/secondin animals with patent fistulae. While du-plex waveforms within the saphenous veindisplayed an arterialized pattern, particu-larly at the proximal end near the fistula,the waveforms within the superficial veinsindicated continuous (elevated) flow.
An important feature of this model is the intermittent distension noted inrelation to posture. In the supine anes-thetized pigs, the enlarged superficialveins are clearly visible but not distended.When the unconscious animal is liftedinto an erect position, the veins becomenoticeably more filled. Lateral flank vari-cose veins were only observed in ambu-lating animals, particularly postexercise.The most pronounced, distended veinswere noted in conscious animals placedin an erect position; this induced a Val-salva-like maneuver in all animals, result-ing in extensive bulging of the superfi-cial varices.
We examined the global soluble proteinexpression profile of pig varicose veinsusing two-dimensional electrophoresis.An advantage of conducting such exper-iments in an animal model system wasthe availability of completely healthy ve-nous tissue for use as reference materi-al. Proteins upregulated in pig varicoseveins included smooth muscle motility-related proteins, heat shock proteins, andATP synthases. Taken together, this pro-file suggests a process of inflammatory-induced fibrosis in the developing pigvaricose veins. These observations are en-couraging as they match the reportedgene expression profiles of human pri-mary varicose veins.2
Histopathological changes in superfi-cial vein structure included increaseddiameter and tortuosity of veins withinthe hypodermis, focal medial atrophy withor without overlying intimal thickening,valve degeneration (tearing and fibrosis),mild periadventitial inflammation, andloss of elastic tissue constituents in boththe media and adventitia. Alterationswere not limited to the large hypoder-mal venous drainage network, but alsoextended into tributaries of these veins.Corrosion vascular casts demonstratedterminal tributary valvular incompetenceleading to reflux in incompetent micro-venous networks. As such, this modelmay not only have utility with regard toprimary varicose veins, but also chronicvenous insufficiency. All these histopatho-logical changes were consistent withthose typically observed in human pri-mary varicose veins.3,4

terbalanced by the quality and relevanceof the resulting pathophysiological infor-mation compared with that obtained inother venous disease models in smalleranimals.
Could results drawn from the new modelbe easily translated to human beings?
While no animal model is a per-fect representation of the
human pathophysiological state, we be-lieve that drug evaluation study resultsbased on our pig model of varicose veinswill translate well to humans, because ofthe similarities in the underlying patho-biology. The model also has the distinctadvantage that the primary outcomes,namely, the development and severity ofsuperficial varicose veins, match the keyclinical features that any phlebotrophicdrug would aim to target. �
clusion. The pig model is clearly preferredfor the study of the effect of drugs on theformation of varicose veins.
In addition, smaller animals such asthe rat, and to a lesser extent the dog,have always been considered to have anadvantage for drug evaluation studiesbecause large numbers can be evaluatedat a reasonable cost. However, we wouldargue that the similar size and physiologyof the pig to humans also makes themsuitable for use in studying drug effects.Drug delivery and tissue/fluid samplingfor bioavailability studies is straightfor-ward, and large sample volumes can beobtained for analysis. Physiological andultrasound evaluations are also not onlymore comparable but also more reliablydone in the larger animal. While adultpigs are associated with a high per animalcost, we believe that in the case of ourvaricose vein model, this is easily coun-
venous insufficiency. This does raise animportant issue with regard to venousdisease models and the likelihood of be-ing able to produce skin changes thatare comparable with those seen in hu-mans. Most animals studied are youngand have a very dense hypodermis, sothat even in the presence of appropriatevenous hypertension in the larger super-ficial veins, the microcirculation is ex-tremely well protected.
In your opinion, which model is themost appropriate for the study of drugs?
This depends of course on whatparticular action of a drug is to
be tested, whether it is to demonstrateeffects on chronic degeneration of the ve-nous valves and wall and the formationof varicose veins, or the effects on acuteevents of valve disruption or venous oc-
I N T E R V I E W
156 Animal models in chronic venous disease – JonesMEDICOGRAPHIA, VOL 30, No. 2, 2008
L es précédents modèles animaux de maladie veineuse conve-naient à l’étude de l’hypertension veineuse et de l’insuffi-sance valvulaire mais ne s’appliquent pas aux varices su-
perficielles. C’était le but de notre groupe de développer un mo-dèle porcin de varices superficielles. La physiopathologie de cemodèle a été évaluée par mesure de la pression sanguine intra-veineuse, écho-Doppler et histologie ; elle a été comparée à la phy-siopathologie humaine. Des fistules artérioveineuses fémoralesdroites ont été créées chirurgicalement chez des porcs adultes.La perméabilité de la fistule a été confirmée par Doppler trans-cutané. Pression et débit veineux des veines superficielles de lacuisse ont été déterminés en postopératoire jusqu’à 15 semainesaprès. Les altérations veineuses structurales résultantes ont étécomparées histologiquement avec celles des varices humaines su-perficielles. Dans ce modèle, les grosses varices superficielles se
sont développées après un décalage initial de 1 à 2 semaines, ellesavaient une composante posturale en phase de remplissage etétaient associées à une légère hypertension veineuse (non pulsa-tile). Ce profil physiologique diffère des profils de pression presqueartérielle typiquement observés chez des animaux plus petits avecfistule artérioveineuse. Les débits veineux s’élevaient à 15 à 25cm/s dans les varices. La structure des varices porcines est large,tortueuse, atrophique au niveau de la media avec ou sans épais-sissement sus-jacent de l’intima et il existe une dégénérescencevalvulaire. En conclusion, la physiopathologie des varices super-ficielles développées dans ce modèle porcin est cohérente aveccelle des varices humaines. La pertinence d’autres modèles ani-maux de maladie veineuse pour l’évaluation des médicaments dutraitement des varices est discutée.
LES MODÈLES ANIMAUX DANS LA MALADIE VEINEUSE CHRONIQUE
REFERENCES1. Foote RR. Varicose Veins, a Practical Manual. 2nded. London, England: Butterworth; 1954.2. Lee S, Lee W, Choe Y, et al. Gene expression profilesin varicose veins using complementary DNA micro-array. Dermatol Surg. 2005;31:391-395.3. Bergan JJ, Schmid-Schonbein GW, Smith PD, et al.Chronic venous disease. New Engl J Med. 2006;355:488-498.4. Jones GT, Solomon C, Moaveni A, et al. Venous mor-phology predicts class of chronic venous insufficien-
hemodynamics in a chronic venous valvular insuffi-ciency model. Arch Surg. 1990;125:1579-1583.8. van Bemmelen SP, Hoynck van Papendrecht AA,Hodde KC, et al. A study of valve incompetence thatdeveloped in an experimental model of venous hyper-tension. Arch Surg. 1986;121:1048-1052.9. Pascarella L, Schmid-Schonbein GW, Bergan J. Ananimal model of venous hypertension: the role of in-flammation in venous valve failure. J Vasc Surg.2005;41:303-311.
cy. Eur J Vasc Endovasc Surg. 1999;18:349-354.5. Burnand KG, Clemenson G, Whimster I, et al. Theeffect of sustained venous hypertension on the skincapillaries of the canine hind limb. Brit J Surg.1982;69:41-44.6. Hobson RW 2nd, Howard EW, Wright CB, et al.Hemodynamics of canine femoral venous ligation: sig-nificance in combined arterial and venous injuries.Surgery.1973;74:824-829.7. Lalka SG, Unthank JL, Dalsing MC, et al. Venous

order to better understand their function, the cy-cle of the venous valve has to be explained: this wascarried out in detail by Lurie et al,9 who studied themost proximal femoral vein valve and a proximalvein valve from the great saphenous vein in 20 nor-mal volunteers (10 males and 10 females). It wasshown that the pattern of flow events was consis-tent in every cycle as the blood passes through thevalves. The characteristics of this pattern were relat-ed to the variations in flow velocity in and aroundthe valve. The flow pattern also varied with the bodyposition and the limb activity. The valve cycle wasdefined as the time taken to complete two valve clo-sures. Four phases were identified: the openingphase, during which the cusps move from the closedposition toward the wall (mean duration 0.025±0.05 s). When the valves cease opening, they enterthe equilibrium phase, during which the leaflets aresuspended, with oscillations in the flowing blood(mean duration 0.65±0.08 s). Then the closing phasebegins, during which the leaflets move toward thecenter of the lumen and take a symmetric position,having the same distance from the opposing walls(mean duration 0.41 ±0.07 s). At the end, the closedphase occurs, during which the cusps remain closed(mean duration 0.45±0.05 s).
Most veins in the human body contain valves.The number and size of the valves varieswith their location.1 Their function is to al-
low blood flow toward the heart and to prevent backflow. Normal valves in the lower extremity allowsome retrograde flow (RF) before their closure. Theduration of the RF varies with the location and sizeof the vein and valve. Reflux is a prolonged dura-tion of RF beyond the normal limits. It occurs as aresult of valve absence or incompetence from re-canalization, dilatation or denervation.2 Severalstudies on the definition of reflux in the superficialand deep veins have reported cutoff values of >0.5second or >1.0 second.2-5 The sample size of thesereports has been small, however, and only a few siteshave been assessed in the lower extremity veins.Limited work has been done to define perforatorvein reflux. These veins—particularly in the calfand ankle—exhibit inward and outward flow, butincompetent perforating veins have shown a netflow toward the superficial veins.6 A later study frommy group determined the upper limits of normal interms of duration and maximum velocity of RF inlower extremity veins.7 The results of these and oth-er recent relevant studies will be presented and dis-cussed.
Function of the venous valve
The venous valves are stationed in different veinsegments, some of which are constant such as theterminal valve in the saphenofemoral junction orthe most proximal valve in the femoral vein.8 In
157Cut point on normal and pathological values of reflux – Labropoulos MEDICOGRAPHIA, VOL 30, No. 2, 2008
F O C U S
T he lower extremity veins can develop retrograde flow thatcontinues for longer than a normal valve closure wouldallow. The increased pressure in the veins during activity
leads to signs and symptoms of chronic venous disease. The dura-tion of retrograde flow that determines what is normal and whatis pathological has been evaluated in a few studies with duplex ul-trasound, which has been shown to be the best method for eval-uating reflux. The results of these studies are examined here, to-gether with the largest and only prospective study on this subject.It was found that for superficial veins, the deep femoral veins,and the deep calf veins, the best cutoff value for abnormal retro-grade flow duration was >500 ms. For the perforator veins, mostexperts have extrapolated the same value as is used for the super-ficial veins. However, the best value that separates normal frompathological was found to be >350 ms. In the common femoral,
femoral, and popliteal veins, the best value was found to be>1000 ms. The best position for performing the reflux test wasstanding. The duration and the peak retrograde flow velocityhad great variability, while the latter had no association with thepresence of prolonged retrograde flow. Reflux development andprogression affects all the veins, and it can occur in an ascend-ing, descending, and multifocal manner.Medicographia. 2008;30:157-162. (see French abstract on page 162)
Keywords: retrograde flow; pathophysiologic; reflux; venousvalve; venous segment; cutoff point
CUT POINT ON NORMAL ANDPATHOLOGICAL VALUES OF REFLUX
b y N . L a b r o p o u l o s , U S A
Address for correspondence: Nicos Labropoulos, Professor of Surgery and Radiology,Vascular Laboratory, Department of Surgery, HSC T19 Room 91, Stony BrookUniversity Medical Center, Stony Brook, NY 11794-8191, USA(e-mail: [email protected])
SELECTED ABBREVIATIONS AND ACRONYMS
CVD chronic venous disease DU duplex ultrasoundRF retrograde flow
Nicos LABROPOULOS, MDVascular Laboratory
Department of SurgeryStony Brook University
Medical CenterStony Brook, NY USA

strain gauge, and photoplethysmography, light re-flection rheography, and foot volumetry.23 The ple-thysmographic tests measure the refilling time, andthe percentage or absolute change in volume fromthe supine to standing position or after knee bendsor tiptoe movements. The shorter the refilling timethe more severe the amount of reflux. These meth-ods are very good for evaluating the overall venoushemodynamics, and are great for use in natural his-tory studies or to assess the effect of treatment. How-ever, when used alone, they cannot guide treatmentas they cannot evaluate which veins are affected.
The imaging tests involve phlebography and du-plex ultrasound (DU). Descending and ascendingphlebography are invasive and are used only in se-lected cases requiring deep vein reconstruction.Currently, the method of choice for detecting refluxin all the lower extremity veins is DU. The distribu-tion and extent of reflux is determined so that treat-ment can be tailored to the individual patient needs.In addition, a differentiation between primary andsecondary disease can be made. The names of theveins,24 the anatomic definitions as visualized byDU, and the methods of testing have been describedin detail.25,26 The best position for determining re-flux with DU is standing.7 In this position, the hy-drostatic column is highest and the veins have theirlargest diameter. Also, dilated veins and varicositiesare more easily seen and it therefore makes the ex-amination more accurate. With the patient rotat-ing in various positions, it is best to access all areasin the lower extremity.
Different maneuvers are used to elicit reflux.Manual compression followed by sudden release be-low the tested vein segment is good to determinereflux in routine examinations. However, standard-ized pressure with the same inflation and deflationduration is necessary when longitudinal studies areperformed, particularly when different types of treat-ment are tested. The Valsalva maneuver is used onlyin the groin. Other tests, such as dorsi/plantar flex-ion, are useful in the calf and ankle in patients withedema.7 Other factors that affect the duration of RFand that should be taken into consideration, are thetime of day that the test is performed, the temper-ature of the examining room, and in females ofchildbearing age, the time of their menstrual cycle.
Criteria for venous reflux
Relatively few studies have been performed regard-ing the definition of venous reflux in the lower ex-tremity veins and its standardization.2-5,7 All of thereports are in agreement regarding the best cutoffvalue in the superficial veins, which is >0.5 second.Even fewer studies have assessed the perforator,muscular, and deep axial veins. The results of theonly study to have evaluated all of the veins is pre-sented below.
Patients and methods
A total of 80 limbs in 40 healthy volunteers and 60limbs in 45 patients with CVD were examined withDU in the standing and supine positions. Reflux was
The valve cycle and the duration of the four phas-es are affected by the position of the body. Duringstanding, the cycle lasts 2.9 to 3.2 seconds, givinga frequency of 18.8 to 20.4 cycles per minute. In thesupine position, the cycle duration is 1.7 to 1.8 sec-onds, giving a frequency of 34.2 to 36.1 cycles perminute. In the latter position, both respiration andthe pressure in the right atrium influence the valvecycle. Dorsal and plantar flexion of the foot reducethe closing phase. The venous valve causes a steno-sis that occupies about a third of the lumen. Thisleads to an increased velocity at the exit of thestenosis (end of leaflets), which enhances the out-flow. The rhythmic activity of the valve cusps andthe pulsatility of the venous flow create vorticalstreams and prevent stasis in the valve pockets, thusdecreasing the chance for thrombus formation.
Changes in venous valves
Venous reflux is important in the development ofvenous hypertension, which is responsible for thesigns and symptoms of chronic venous disease(CVD).10 Many studies have shown that valve dys-function leads to venous reflux, which increases theambulatory pressure in the lower extremity veins.11,12
Valvular dysfunction is most often primary and me-diated by changes in the venous wall, the valveleaflets or a combination of both. With the use of anangioscope, changes and damage to the valves havebeen observed such as stretching, splitting, tear-ing, thinning, and adhesion of valve leaflets.13 Pa-tients with CVD may have fewer valves per unitlength.14 Infiltration of the venous wall and the valveleaflets by monocytes and macrophages has beendemonstrated in all vein specimens from patientswith CVD, but not in those specimens from con-trols.15 Infiltration from the inflammatory cells wasfound in areas of endothelium that expressed inter-cellular adhesion molecule–1 (ICAM-1).16
Changes in the valves are also seen after veinthrombosis.17 This is due to the direct effect ofthrombus on the valves and the vein wall. Manynatural history studies have demonstrated the dam-aging effect of thrombosis on the valve/wall lead-ing to reflux.18,19 Reflux is seen after both partial orcomplete recanalization of the previously throm-bosed segments. More evidence regarding this hasbeen provided by the effects of early thrombus re-moval with chemical and pharmacomechanicalthrombolysis, which reduces the development ofpostthrombotic reflux.20,21
Valve atrophy and aplasia have also been report-ed.22 In these cases, the affected vein segments arefound to have severe reflux. The reasons for the fail-ure of the valves to develop are not known, but thiscondition is very rare and only small series or casesreports have been published.
Methods for diagnosing reflux
There are both physiologic and imaging methodsfor diagnosing reflux. The physiologic evaluation in-cludes invasive tests with direct vein pressure mea-surements, and plethysmographic tests such as air,
F O C U S
158 Cut point on normal and pathological values of reflux – LabropoulosMEDICOGRAPHIA, VOL 30, No. 2, 2008

of a vein, the higher the chance of it being incom-petent. However, many vein segments with a nor-mal diameter, and also some with a small diameter,can have reflux. This has been observed in all typesof superficial veins (saphenous, accessory, tribu-taries, and nonsaphenous veins) in many locationsin the lower extremity.
� Perforator veinsBecause it has been shown that perforator veins canexhibit bidirectional flow,4,6 the outward flow com-ponent was taken as the RF. Most perforator veinswere found below the knee (n=214; thigh, n=59).The mean RF duration in the control group was170 ms, ranging from 0 to 760 ms. Only 3 perfora-tor veins (1%) in the calf and none in the thigh hadRF >500 ms. RF duration in the calf (180 ms, 95%CI, 176-184) was longer than in the thigh (150 ms,95% CI 145-155; P<0.0001). The best cutoff valuefor reflux was RF >350 ms. In the patients, 71 of 312perforator veins had RF >500 ms (P>0.0001 com-pared with controls). Setting the cutoff at 350 ms,82 perforator veins would have had abnormal RF.
Incompetence in the perforator veins is contro-versial, as the impact of these veins on CVD is notclear. However, the number of incompetent perfo-rator veins and their size increase with the severityof the disease.27,28 The diameter of a perforator veinhas been found to correlate well with the presenceof reflux, as those >3.0 mm are most often incom-petent.6,29 However, as in the superficial veins, manyincompetent perforators have a smaller diameter.In patients with primary CVD, the perforator refluxdevelops in continuity with that of the superficialveins.30 In the absence of superficial vein reflux, theperforator veins are normal.
� Deep veinsIn the deep veins, RF ranged from 0 to 2600 ms.Deep femoral and calf veins had a mean RF dura-tion of 190 ms (95% CI, 188-192). The RF was>500 ms in only 1 deep femoral vein (1.2%) and 7calf veins (2.2%). Common femoral, femoral, andpopliteal veins had a mean RF duration of 280 ms(95% CI, 375-385), which was significantly longerthan all other veins (P<0.0001). In 21 of 400 femo-ropopliteal segments in controls, the RF durationranged from 510 to 2600 ms, but in 99% of theseveins, RF was <990 ms. Using 1000 ms as the cut-off for abnormal RF, only 4 of 400 segments (1%)would have reflux. In the patients, 152 of 600 seg-ments had RF >500 ms (P<0.0001 compared withcontrols). In the femoropopliteal veins, the preva-lence of RF >500 ms was 29% (87 of 300 veins;P<0.0001 compared with controls). Using a cutoffvalue of 1000 ms, the prevalence of abnormal RFwas significantly reduced at 18% (54 of 300 veins;P<0.002).
In primary CVD, reflux in deep veins is associat-ed with reflux in superficial veins.31 In fact, it hasbeen shown that correction of superficial vein re-flux corrects deep vein reflux in most patients.32,33
The prevalence of deep vein reflux increases withseverity of CVD, and is significantly more commonin patients with skin damage.28 This is probably
assessed at 16 vein segments: the common femoral,deep femoral, and proximal and distal femoral veins;the proximal and distal popliteal veins; the gastro-cnemial vein; the anterior and posterior tibial veins;the peroneal vein; the great saphenous vein at thesaphenofemoral junction, thigh, upper calf, andlower calf; and the small saphenous vein at thesaphenopopliteal junction and mid calf. Perforatorveins detected along the course of these veins werealso evaluated.
In healthy volunteers, 1553 vein segments wereassessed, including 480 superficial vein segments,800 deep vein segments, and 273 perforator veinsegments. In the patients, 1272 vein segments wereassessed, including 360 superficial vein segments,600 deep vein segments, and 312 perforator veinsegments. Rapid-inflation pneumatic cuffs (Aircast,Summit NJ) with pressure set at 80 mm Hg wereused to elicit reflux. The cuffs were placed on thelower thigh for groin and proximal thigh vein mea-surements, and for the other veins, they were placedon the lower calf. The inflation time to maximalpressure was 0.3 second, inflation was maintainedfor 1.0 second, and deflation was achieved in lessthan 1.0 second.
The Doppler tracings were set so as not to haveovergain, with the background appearing dark andthe signal bright. The scale was reduced to the low-est necessary point to detect low flow velocities, andwas optimized to show the whole trace. Immediate-ly after release of compression, the tracings wereallowed to run until the RF ended. At this point, thedurations of RF and peak vein velocity were mea-sured in both the standing and supine positions.
Results and interpretation
All data for each vein segment were analyzed indi-vidually for the supine and standing positions. Thedefinition of abnormal RF was calculated at the bestseparation point and in comparison with the datafrom the healthy controls. Statistical analysis of thedata was performed for the differences in propor-tions using the chi-squared test and with 95% con-fidence intervals (CI). Examples of different wave-forms and flow patterns obtained are shown inFigures 1 to 8 (page 160).
� Superficial veinsIn the control group, the mean duration of RF was210 ms (range, 0-2400 ms; 95% CI, 206-214), and in16 vein segments (3.3%), RF was >500 ms. In thepatients, RF was >500 ms in 202 segments (56%;P<0.0001 compared with controls). If other seg-ments of the main saphenous veins, tributary ves-sels, and nonsaphenous superficial veins were in-cluded in the analysis, then 93% would have RF>500 ms. Varicose veins had RF >500 ms. It is im-portant to note that of the 202 segments with RF>500 ms, 114 segments (56%) were dilated but hadno varicosities, and 18 segments (9%) had a nor-mal diameter or had a diameter of <2.5 mm.
From the above findings and in accord with oth-ers, RF >500 ms identifies reflux with great certain-ty. It has been shown that the larger the diameter
F O C U S
159Cut point on normal and pathological values of reflux – Labropoulos MEDICOGRAPHIA, VOL 30, No. 2, 2008

F O C U S
160 Cut point on normal and pathological values of reflux – LabropoulosMEDICOGRAPHIA, VOL 30, No. 2, 2008
Figure 1. Normal popliteal vein, without any retrogradeflow.
Figure 4. Proximal femoral vein reflux with a retrogradeflow duration of 1.84 seconds.
Figure 3. Popliteal vein reflux with a retrograde flow du-ration of 1.4 seconds.
Figure 2. Normal popliteal vein with a retrograde flowduration of 820 ms.
Figure 5. Reflux in the saphenopopliteal junction with aretrograde flow duration of 3.5 seconds. The poplitealvein just distal to the junction is normal, whereas at thejunctional level, it is incompetent. After treatment of thesmall saphenous vein, the popliteal vein became normal.
Figure 8. A nonfunctioning valve in a posteromedial trib-utary overlying the medial head of the gastrocnemiusmuscle. The valve in the near wall has become atrophicand in the far wall it is elongated and frozen.
Figure 7. Reflux in the great saphenous vein in continuitywith a tributary in the lower thigh. On Doppler spectrum,the retrograde flow duration was 5.2 seconds and the peakflow velocity was 34 cm/s. The proximal incompetent veinsegment has a larger diameter than the distal normal veinsegment just below the tributary (4.6 mm vs 3.4 mm).
Figure 6. Reflux in the small saphenous vein in the uppercalf with a retrograde flow duration of 1.8 seconds. Thevein has a small diameter measuring only 2.2 mm.

nuity. Also, the severity of the disease and the degreeof inflammation may affect these values, as bloodflow in the limb may be affected locally or in its en-tirety.37 Other RF parameters may be important forthe severity of the disease, but do not discriminatebetween normal and pathologic values.38 It wasshown that the RF duration has a qualitative value,whereas the peak RF velocity and the average flowvelocity better reflected the severity of venous in-competence.
� Effect of different maneuversManual compression or rapid inflation cuffs maynot be adequate stimulus to elicit reflux in somepatients. In 13 vein segments (great saphenous vein,3; small saphenous vein, 1; femoral vein, 1; poplitealvein, 1; gastrocnemial veins, 2; peroneal vein, 1; per-forator veins, 4) in patients with significant pittingedema, RF was normal. RF became abnormal onlyduring active dorsiflexion or plantar flexion. Wehave also observed this in routine clinical practice,where some very obese patients and those with ede-ma may need active dorsi/plantar flexion where thedeep veins are compressed with higher force direct-ly from the muscles. In the groin area, if the test isnegative with distal compression, the Valsalva ma-neuver is performed, because the challenge to thevalves at that level is stronger and reflux may onlybe demonstrated in this manner.
Progression of reflux
Reflux develops in an ascending, descending, andmultifocal manner.39,40 It can also exist in indepen-dent locations that do not anatomically communi-cate. It has also been shown that the progression ofreflux occurs in the same manner.30,41 All veins canbe affected by reflux, but the superficial veins aremost often involved in primary disease. In patientswith thrombosis, reflux progresses in the post-thrombotic veins, but reflux in veins that were re-mote to thrombosis can be affected as well. Acrossthe whole spectrum of CVD, reflux is most commonin the superficial veins. Superficial vein reflux af-fects the perforator veins either in an ascendingmanner as progression of vein wall disease, in a de-scending manner at a re-entry point via the highflow rate that may dilate the perforator veins, or inboth directions. In the descending path, wall dis-ease may also be important, together with, or sepa-rate from, increased flow. The perforator veins, inturn, affect the deep veins that they are communi-cating with, and in time will render these incom-petent as well. In a similar manner, the saphenousand gastrocnemial junctions can make the femoraland popliteal veins incompetent. �
because the extent of superficial disease and theduration of CVD are longer, and the prevalence ofthrombosis is significantly higher compared withpatients presenting with varicose veins.28
� Supine compared with standing positionIn the control group, 37 vein segments (2.4%) hadRF >500 ms in the supine position. Of these seg-ments, only 22 (59%) had RF >500 ms in the stand-ing position. Of the 48 vein segments (3.1%) withRF >500 ms in the standing position, RF was <500ms in 6 of these (13%) in the supine position. Sim-ilar observations were noted in patient veins, wheresome vein segments with reflux in the supine po-sition became normal in the standing position, andsome others became worse in the standing position.
These findings indicate that both the specificityand sensitivity for detecting pathologic reflux arebest in the standing position. Standing is a morephysiologic position and more meaningful in clin-ical practice, as the hydrostatic pressure in the low-er limbs is highest and the diameter of all veins islarger. This allows a longer period of RF to occur indiseased vein segments. During standing, there isa definitive closure of competent valves and clearlymore challenge is offered to incompetent valves. Acutoff value of >2 seconds was suggested for veinstested in the supine position.34 Given our findingsand the reasons discussed above, when possible, re-flux should only be tested in the standing position.Another smaller study that examined patients inboth positions also found that the standing positionwas superior for reflux testing.35
� Waveform characteristicsThe peak RF velocity, which was identified imme-diately after the release of the compression, showeda wide range in both controls (8-35 cm/s) and pa-tients (9-83 cm/s). Vein segments with reflux hadhigher peak velocity (mean 23.5 cm/s; 95% CI, 20.2-26.8) compared with normal vein segments (mean15 cm/s; 95% CI, 14.8-15.2; P<0.0001). In the pa-tients, vein segments with reflux had a mean peakRF velocity of 41 cm/s; 95% CI, 36-48.5, comparedwith 18 cm/s; 95% CI, 14.5-24.2, in the normal veinsegments (P<0.0001). It was not possible to deter-mine peak RF cutoff velocity values for reflux, asRF duration and peak RF velocity had great varia-tion. More importantly, reflux occurred at both lowand high peak RF velocities. In a previous study, noassociation was found between the peak RF veloc-ity and reflux.36 Many factors are responsible for thevelocity characteristics, such as the diameter andlength of the incompetent vein segment, wall com-pliance, the network of veins where this segmentempties, and the condition of other veins in conti-
F O C U S
161Cut point on normal and pathological values of reflux – Labropoulos MEDICOGRAPHIA, VOL 30, No. 2, 2008
REFERENCES1. Gottlob R, May R. Occurrence and distribution ofvenous valves. In: Gottlob and May, eds.Venous Valves.Vienna, Austria: Springer-Verlag; 1986:16-24.2. van Bemmelen PS, Bedford G, Beach K, StrandnessDE. Quantitative segmental evaluation of venous val-vular reflux with duplex ultrasound scanning. J VascSurg.1989;10:425-431.3. Araki CT, Back TL, Padberg FT, Thompson PN,Duran WN, Hobson RW. Refinement in the ultrason-
6. Labropoulos N, Mansour MA, Kang SS, Gloviczki P,Baker WH. New insights into perforator vein incom-petence. Eur J Vasc Endovasc Surg.1999;18:228-234.7. Labropoulos N, Tiongson J, Landon P, et al. Defi-nition of venous reflux in lower extremity veins. J VascSurg. 2003;38:793-798.8. Maros T. Data regarding the typology and function-al significance of the venous valves. Morphol Embry-ol (Bucur).1981;27:195-214.
ic detection of popliteal vein reflux. J Vasc Surg.1993;18:742-748.4. Sarin S, Sommerville K, Farrah J, Scurr JH, Co-leridge Smith PD. Duplex ultrasonography for assess-ment of venous valvular function of the lower limb.Br J Surg. 1994;81:1591-1595.5. Lagattolla NR, Donald A, Lockhart S, Burnand KG.Retrograde flow in the deep veins of subjects withnormal venous function. Br J Surg. 1997;84:36-39.

F O C U S
162 Cut point on normal and pathological values of reflux – LabropoulosMEDICOGRAPHIA, VOL 30, No. 2, 2008
SEUIL DES VALEURS NORMALES ET PATHOLOGIQUES DU REFLUX
U n reflux se prolongeant plus longtemps que ne le permet-trait une fermeture valvulaire normale peut se développerdans les membres inférieurs. Des signes et symptômes de
maladie veineuse chronique surviennent pendant l’activité à cau-se de l’augmentation de la pression veineuse. L’écho-Doppler, lameilleure méthode d’évaluation du reflux, a évalué sa durée dansquelques études, déterminant les situations normale et patholo-gique. La plus grande et seule étude prospective sur le sujet estanalysée ici avec les résultats de ces études. La meilleure valeurseuil pour la durée d’un reflux anormal était supérieure à 500 mspour les veines superficielles, les veines fémorales profondes et les
veines profondes du mollet. Pour les veines perforantes, la plupartdes experts ont extrapolé la même valeur que celle utilisée pourles veines superficielles. La meilleure valeur séparant le normaldu pathologique est néanmoins celle supérieure à 350 ms. En cequi concerne les veines fémorale commune, fémorale et poplitée,la meilleure valeur est celle supérieure à 1 000 ms. L’orthosta-tisme est la meilleure position pour réaliser le test du reflux. Ladurée et la vitesse maximale du reflux sont très variables, la vi-tesse n’ayant aucun rapport avec la présence d’un reflux prolon-gé. La progression et le développement du reflux touchent toutesles veines et de façon ascendante, descendante et multifocale.
9. Lurie F, Kistner RL, Eklof B, Kessler D. Mechanismof venous valve closure and role of the valve in circu-lation: a new concept. J Vasc Surg. 2003;38:955-961.10. Bergan JJ, Schmid-Schonbein GW, Smith PD,Nicolaides AN, Boisseau MR, Eklof B. Chronic venousdisease. N Engl J Med. 2006:355:488-498.11. Nicolaides AN, Hussein MK, Szendro G, Christo-poulos D, Vasdekis S, Clarke H. The relation of venousulceration with ambulatory venous pressure mea-surements. J Vasc Surg. 1993;17:414-419.12. Neglen P, Rajus S. Differences in pressures of thepopliteal, long saphenous, and dorsal foot veins. J VascSurg. 2000;32:894-901.13. Van Cleef JF, Hugentobler JP, Desvaux P, Griton P,Cloarec M. Étude endoscopique des reflux valvulairessaphéniens. J Mal Vasc. 1992;17(suppl B):113-116.14. Sales CM, Rosenthal D, Petrillo KA, et al. Thevalvular apparatus in venous insufficiency: a problemof quantity? Ann Vasc Surg. 1998;12:153-155.15. Ono T, Bergan JJ, Schmid-Schönbein GW, TakaseS. Monocyte infiltration into venous valves. J VascSurg.1998;27:158-166.16. Takase S, Bergan JJ, Schmid-Schönbein GW.Expression of adhesion molecules and cytokines onsaphenous veins in chronic venous insufficiency. AnnVasc Surg. 2000;14:427-435.17. Prandoni P, Lensing A, Cogo A, et al. The long-term clinical course of acute deep venous thrombosis.Ann Intern Med.1996;125:1-7.18. Johnson B, Manzo R, Bergelin O, Strandness D.The site of residual abnormalities in the leg veins inlong term follow-up after deep vein thrombosis andtheir relationship to the development of the post-thrombotic syndrome. Intern Angiol.1996;15:14-19.19. Meissner M, Caps M, Zierler B, et al. Determinantsof chronic venous disease after acute deep venousthrombosis. J Vasc Surg. 1998;28:826-833.20. Comerota AJ, Gravett MH. Iliofemoral venousthrombosis. J Vasc Surg. 2007;46:1065-1076.21. Laiho MK, Oinonen A, Sugano N, et al. Preserva-
Development of reflux in the perforator veins in pri-mary venous disease. J Vasc Surg. 2006;43:558-562.31. Labropoulos N, Tassiopoulos AK, Kang SS, Man-sour MA, Littooy FN, Baker WH. Prevalence of deepvenous reflux in patients with primary superficialvein incompetence. J Vasc Surg. 2000;32:663-668.32. Walsh JC, Bergan JJ, Beeman S, Comer TP.Femoral venous reflux abolished by greater saphenousvein stripping. Ann Vasc Surg. 1994;8:566-570.33. Sales CM, Bilof ML, Petrillo KA, Luka NL. Cor-rection of lower extremity deep venous incompetenceby ablation of superficial venous reflux. Ann VascSurg.1996;10:186-189.34. Manzo R. Duplex evaluation of chronic venousdisease. In: Strandness DE, ed. Duplex Scanning inVascular Disorders. Philadelphia, Pa: Lippincott Wil-liams & Wilkins; 2002:368-378.35. Foldes MS, Blackburn MC, Hogan J, et al. Stand-ing versus supine positioning in venous reflux eval-uation. J Vasc Tech. 1991;15:321-324.36. van Ramshorst B, van Bemmelen PS, HoeneveldH, Eikelboom BC. The development of valvular in-competence after deep vein thrombosis: a follow-upstudy with duplex scanning. J Vasc Surg. 1994;19:1059-1066.37. Labropoulos N, Leder DM, Kang SS, Mansour MA,Baker WH. Inflammation parallels severity of chron-ic venous insufficiency. Phlebology. 2003;18:78-82.38. Neglén P, Egger JF 3rd, Olivier J, Raju S. Hemody-namic and clinical impact of ultrasound-derived venousreflux parameters. J Vasc Surg. 2004;40:303-310.39. Labropoulos N, Giannoukas AD, Delis K, et al.Where does venous reflux start? J Vasc Surg.1997;26:736-742.40. Caggiati A, Rosi C, Heyn R, Franceschini M, Ac-concia MC. Age-related variations of varicose veinsanatomy. J Vasc Surg. 2006;44:1291-1295.41. Labropoulos N, Leon L, Kwon S, et al. Study of thevenous reflux progression. J Vasc Surg. 2005;41:291-295.
tion of venous valve function after catheter-directedand systemic thrombolysis for deep venous thrombo-sis. Eur J Vasc Endovasc Surg. 2004;28:391-396.22. Plate G, Brudin L, Eklöf B, Jensen R, Ohlin P.Physiologic and therapeutic aspects in congenital veinvalve aplasia of the lower limb. Ann Surg.1983;198:229-233.23. Nicolaides AN. Investigation of chronic venousinsufficiency: a consensus statement. Circulation.2000;102:E126-E163.24. Caggiati A, Bergan JJ, Gloviczki P, Eklof B, AllegraC, Partsch H; International Interdisciplinary Con-sensus Committee on Venous Anatomical Terminol-ogy. Nomenclature of the veins of the lower limb: ex-tensions, refinements, and clinical application. J VascSurg. 2005;41:719-724.25. Coleridge-Smith P, Labropoulos N, Partsch H,Myers K, Nicolaides A, Cavezzi A. Duplex ultrasoundinvestigation of the veins in chronic venous disease ofthe lower limbs—UIP Consensus Document. Part I.Basic principles. Eur J Vasc Endovasc Surg. 2006;31:83-92.26. Cavezzi A, Labropoulos N, Partsch H, et al. Duplexultrasound investigation of the veins in chronic ve-nous disease of the lower limbs—UIP Consensus Doc-ument. Part II. Anatomy. Eur J Vasc Endovasc Surg.2006;31:288-299.27. Labropoulos N. Hemodynamic changes accordingto the CEAP classification. Phlebolymphology. 2003;40:103-106.28. Labropoulos N, Patel PJ, Tiongson JE, Pryor L,Leon LR Jr, Tassiopoulos AK. Patterns of venous re-flux and obstruction in patients with skin damage dueto chronic venous disease. Vasc Endovascular Surg.2007;41:33-40.29. Sandri JL, Barros FS, Pontes S, Jacques C, Salles-Cunha SX. Diameter-reflux relationship in perforat-ing veins of patients with varicose veins. J Vasc Surg.1999;30:867-874.30. Labropoulos N, Tassiopoulos AK, Bhatti A, Leon L.

be identified in both the upper and lower limbs, theother veins in the thorax and abdomen being most-ly valveless, but the adverse consequences result-ing in chronic venous disease are only found in thelower limbs.
Below the inguinal ligament, there are three ve-nous systems: the superficial, perforator, and deepsystems. Consequently, valve dysfunction can beidentified in all of them, but restoration of valvefunction by surgery is only performed in the super-ficial and deep systems.
Surgical methods for treatment of valve dysfunction
� Superficial venous systemIn the superficial venous system, two kinds of treat-ment methods can be used—indirect and direct.� Indirect proceduresIndirect procedures have in common the preser-vation of the saphenous trunk with restoration ofits valve function via modification of the hemody-namics (Figure 1, page 164). All of these proceduresneed a very precise preoperative duplex scanning(DS) evaluation and mapping.
Valve dysfunction can be described as an ab-normality that is responsible for reflux in theaffected vein. Primary venous insufficiency is
chronic venous dysfunction whose cause is neithercongenital nor clearly identifiable. Valve dysfunc-tion is the result of structural abnormalities in thevein wall and in the valve itself. Redundant, mal-opposed cusps and venous dilation permit valve pro-lapse and reflux. Unlike in the post-thrombotic syn-drome, there is no evidence of previous thrombosisnear the valve. A rare cause of reflux is the completeor partial absence of valves. This anomaly can beprimary or congenital. Valvular incompetence can
163Venous valve dysfunction restoration by surgery in primary chronic venous disease – Perrin MEDICOGRAPHIA, VOL 30, No. 2, 2008
U P D A T E
A s stated by Arkadiusz Jawien in this issue of Medicogra-phia, surgical techniques for venous valve dysfunctionhave evolved. Resection surgery, consisting of ablation of
the impaired organ or system when it was not indispensable interms of survival or normal physiological function, has progres-sively been replaced by organ or system repair. Incompetent ve-nous valves responsible for disabling reflux, which can lead tochronic venous disease, can be mainly found in two systems; thesuperficial and the deep venous systems. As it is known that ab-lation of the superficial venous system can be performed withoutmajor disturbance to the venous circulation, this method becamethe gold standard up until 20 years ago, when new proceduresincluding direct or indirect valve function restoration were de-veloped and used. Indirect restoration of valve function in the su-perficial venous system can be achieved by two methods: sup-pression of the leak points from the deep system to the superficialsystem without ablation of the saphenous trunk (ConservativeHemodynamic treatment of Incompetent Varicose veins in Am-bulatory patients [CHIVA], high ligation plus tributaries phle-bectomy plus/ minus perforator ablation), or suppression of the
distal reservoir, ie, stab avulsion of the incompetent tributariesto restore valve competence by reducing the diameter of thesaphenous trunk (ambulatory phlebectomy, Selective Ablationof Varices under Local Anesthesia [ASVAL]). Direct valve repairin the superficial venous system can be achieved through vein ex-ternal cuffing or bandaging at the valve station. Extensive deepvenous system ablation is not possible without major perturba-tion of the venous return function, and ligation has proven to beineffective. The most common procedure used in this situation isvalve repair, with valve transfer or use of a prosthetic venous valvealso used less frequently. Techniques, treatment outcomes, andindications for venous valve restoration by surgery will be dis-cussed with respect to primary chronic venous disease.Medicographia. 2008;30:163-168. (see French abstract on page 168)
Keywords: primary chronic venous disease; venous reflux,valvuloplasty; valve transfer; valve bandaging; venous surgery;phlebectomy; varicose vein
VENOUS VALVE DYSFUNCTIONRESTORATION BY SURGERY
IN PRIMARY CHRONIC VENOUS DISEASE
b y M . R . P e r r i n , F r a n c e
Address for correspondence: Michel R. Perrin, 26 Chemin de Décines, 69680 Chassieu, France (e-mail: [email protected])
SELECTED ABBREVIATIONS AND ACRONYMS
ASVAL Selective Ablation of Varices under Local Anesthesia (French acronym)
CHIVA Conservative Hemodynamic treatment of Incompetent Varicose veins in Am-bulatory patients (French acronym)
DS duplex scanningDVR deep venous refluxRCT randomized controlled trialSFJ saphenofemoral junction
Michel R. PERRIN, MDClinique du Grand Large
Décines, FRANCE

which involved stab avulsion of incompetent trib-utaries in patients presenting with incompetentvalves in the saphenous trunk. He updated his ex-perience in 1996.7 Recently, Pittaluga has promot-ed this technique with some refinement on the ba-sis of information provided by DS investigation.8
� Direct proceduresVarious direct techniques have been used, includ-ing SFJ plication plus/minus tributary phlebecto-my,9,10 and SFJ wrapping or bandaging with Dacron,polytetrafluoroethylene (PTFE) or a specific device(Venocuff I and II) plus/minus tributary phlebec-tomy plus/minus perforator ligation (Figure 1C,Figure 2).11-19
� Deep venous systemIn the deep venous system, valve repair techniquesfor treating deep venous reflux (DVR) can be classi-fied into three groups: those that involve phleboto-my, those that do not involve phlebotomy, and thoseutilizing percutaneous placed devices.� Techniques with phlebotomy– Internal valvuloplastySince the first internal valvuloplasty procedure de-scribed in 1968 by Kistner, involving the use of alongitudinal phlebotomy (Figure 3),21 various pro-cedures have been proposed. Raju22 advocated asupravalvular transverse venotomy, while Sottiu-rai23 utilized a hybrid T-shaped supravalvular inci-sion (Figure 4). In 2002, Tripathi proposed the useof an internal trapdoor valvuloplasty.24 In all cases,the redundant valve cup is plicated to the vein wallusing multiple interrupted or continuous 7-0 Pro-lene reefing sutures. It has been estimated that pli-cation of approximately 20% of the leaflet lengthshould restore competence, although the best gaugeremains visual inspection.– Venous segment transferVenous segment transfer was devised for patientswith a competent great saphenous or deep femoralvein valve in their proximal segment (Figure 5) andDVR in the femoropopliteal axis. The purpose ofvenous segment transfer is to transpose a compe-tent valve-bearing venous segment into the axialdeep venous system, ie, the femoropopliteal axis atthe groin level. Several surgical variations of venous
– Conservative Hemodynamic treatment of Incompetent Varicose veins in Ambulatory patients (CHIVA) The CHIVA procedure (Figure 1B), developed byFranceschi, is based on the fact that even thoughvaricose disease is associated with weakness of thevein wall, the breaking of the pressure column andthe suppression of venous shunting can restore thevalve function in the saphenous trunk.2 Accordingto the different patterns of reflux in the superficialsystem identified by DS, various procedures can betailored to the individual patient.3-5
– High ligation plus tributaries phlebectomyplus/minus perforator ablationHigh ligation plus tributaries phlebectomy plus/minus perforator ablation (Figure 1D), first report-ed by Hammarsten, is used only for treating insuf-ficiency in the great saphenous vein.6 The maindifference between this procedure and the CHIVAprocedure is the systematic ligation-resection of thesaphenofemoral junction (SFJ).– Tributaries stab avulsion, Selective Ablation ofVarices under Local Anesthesia (ASVAL)In 1956, Muller brought back a very ancient methodknown as tributaries stab avulsion (Figure 1E),
U P D A T E
164 Venous valve dysfunction restoration by surgery in primary chronic venous disease – PerrinMEDICOGRAPHIA, VOL 30, No. 2, 2008
Figure 1. Hemodynamic techniques for restoration of the valves of the saphenoustrunk. A shows a diagram of primary varicose veins. 1, deep vein; 2, great saphenousvein (GSV) or short saphenous vein (SSV) trunk; 3, GSV or SSV tributaries; 4, perfo-rator. B illustrates the CHIVA technique: high ligation plus ligation of the saphenoustrunk below the re-entry perforator plus disconnection of the venous shunts or trib-utary phlebectomy. C illustrates valvuloplasty or wrapping (shown here) of the GSVtermination plus tributary phlebectomy plus perforator ligation. D illustrates highligation resection plus tributary phlebectomy plus perforator ligation. E shows tribu-tary phlebectomy (ASVAL). X, vein resection; , ligation.
Figure 3. Internal valvuloplasty according to Kistner. Using a longitu-dinal phlebotomy, each valve is repaired by interrupting a series of sutures placed at the commissures. Each suture progressively shortensthe leading edge of the cusp.
A
1
4
3
2
B C D E
3 cm
Figure 2. External stenting. Left panel: above, the Venocuff II set. Be-low, schematics of incompetent venous valve (BEFORE) and competentvalve following external stenting (AFTER). Right panel: angioscopic viewafter stenting.
�
�
Figure 1 and Figure 2 repro-duced from reference 1:Perrin M. Chirurgie à ciel ou-vert de l’insuffisance veineusesuperficielle. Principes. Techniques. Résultats. EMC(Elsevier Masson SAS, Paris),Techniques Chirurgicales—Chirurgie Vasculaire. 2007;43-161-B. Copyright © 2007, Elsevier Masson SAS.

was developed initially for saphenous vein incom-petence, and later for primary deep vein incompe-tence.27,28
– External valvuloplastyThe first step in external valvuloplasty consists ofadventitial dissection until the valve’s insertion linesare clearly identifiable as an inverted V shape. Thecommissural angle is normally acute, but in reflux-ive valves it is widened. Kistner introduced externalvalvuloplasty in 1990.29 In the transmural valvulo-plasty technique, an external rowof sutures is placedalong the diverging margins of the valve cusp inthe vein wall. Sutures for external repair are com-menced at each commissure on both sides of thevein. The interrupted sutures are carried inferiorlyuntil the valve becomes competent by strip testing(Figure 8, page 166).
Transcommissural valvuloplasty (Figure 9, page166), developed by Raju, differs from transmuralvalvuloplasty by the use of a transluminal suture.As described in his paper; “A through-and-throughtransluminal resuspension suture (7-0 Prolene) wasplaced obliquely across the inverted V, traversingthe valve cusps ‘blindly’ near their wall attachmentto pull them up.”31
segment transfer have been employed using end-to-end or side-to-end anastomosis according to thestate of competence of the different valves in theveins of the groin.25
– Vein valve transplantationIn vein valve transplantation (Figure 6), a 2-3 cmsegment of axillary vein is inserted as an interpo-sition graft at the termination of the femoral veinjust below the junction between the deep femoralvein and the femoral vein or at the popliteal vein.– Neovalve creationMaleti created a valvular cusp by dissection of thefemoral venous wall to obtain a single or a bicuspidvalve (Figure 7).26 He has used this technique main-ly in cases of secondary etiology (post-thromboticsyndrome) but also in valvular agenesis that is prob-ably not primary but congenital, but this originaltechnique deserves to be mentioned.� Techniques without phlebotomy– Wrapping, banding, cuffing, and external stentingWrapping, banding, cuffing, and external stenting
U P D A T E
165Venous valve dysfunction restoration by surgery in primary chronic venous disease – Perrin MEDICOGRAPHIA, VOL 30, No. 2, 2008
Figure 5. Venous segment transfer. The refluxive femoral vein (c) maybe transposed into the great saphenous vein (d) or the profunda femoralvein (b), provided they have a competent proximal valve at their termi-nation. a, common femoral vein.
Figure 4. Internal valvuloplasty according to Sottiurai. Left panel: (i)T-shaped phlebotomy; (ii) a bird’s eye view of the floppy valve. Rightpanel: (i) after clamping and systemic heparinization, a vertical phle-botomy originating from the midpoint of the transverse phlebotomy ismade extending into the valvular sinus using right angle Potts’ scissors;(ii) the needle of a double-ended suture (7-0 polypropylene suture) is inserted to penetrate both cusps of the valve at the commissure;(iii) after completion of 3 to 4 tackings at each commissure, the valvecusp apposition is obtained.
(i) (ii)
(i)
(ii)
(iii)
Figure 6. Valve transplant. Above-knee or below-knee axillary vein-to-popliteal vein transplantation with end-to-end anastomosis.
Figure 7. Valve construction according to Maleti (by courtesy). Leftpanel: valve agenesia. The flap is created. Right panel: the flap is fixedat the opposite site to create a neovalve.
Poplitealvein
Posteriortibial vein
Posteriortibial arteryDistal
superficialfemoral vein
a
c
d
b
a
c
db
Figure 3, Figure 4, Figure 5,and Figure 6 reproduced fromreference 20:Perrin M. Repair of venousvalves in severe chronic venousinsufficiency. In: Bergan JJ,Shortell CK, eds. Venous Ulcers.Amsterdam, Holland; Boston,Ma: Elsevier Academic Press;2007:243-257. Copyright ©2007, Elsevier, Ltd.

comparing this method with conventional surgerydid not show any statistical difference in terms ofclinical results at 4-year follow-up.6,36 Two case seriesusing ASVAL have been reported with 7.8 (mean),and 36 months follow-up, respectively.8,37 The recur-rence rate was found to be less than 10% in both.� Direct proceduresIt is more difficult to assess the outcome of directprocedures, as a variety of procedures have beenused. However, three RCTs comparing valve ban-daging to classical surgery are available, with 9.4(mean), 12, and 42 months of follow-up, respective-ly.13,15,16 No difference in terms of outcome—includ-ing varices recurrence—has been found.
� Deep venous systemThe results of DVR surgery are somewhat difficultto assess, as superficial venous surgery and/or per-forator surgery are often performed in combina-tion with DVR surgery. In primary DVR, the mostfrequent procedure used is valvuloplasty. Results aresummarized in Table I.24,31,38-43 On the whole, valvu-loplasty is credited with achieving a good result in70% of cases in terms of clinical outcome, definedas freedom from ulcer recurrence and a reductionin pain, valve competence, and hemodynamic im-provement over a follow-up period of more than 5years. In all series, a good correlation was observedamong these three criteria. External transmuralvalvuloplasty does not seem to be as reliable as in-ternal valvuloplasty for providing long-term valvecompetence or ulcer-free survival.41
Only two series provide information about theoutcome of patients presenting with severe chron-ic venous insufficiency without ulcer who are treat-ed with valvuloplasty.40,42 No patients in either seriesdeveloped an ulcer during the long-term follow-up,presumably due to successful prevention of diseaseprogression by the operative intervention. Otherprocedures used in primary deep reflux, includingangioscopic repair and wrapping, are more difficultto assess, because the case series have a relativelyshort follow-up, with the exception of Lane’s series(Table II).27,28,41,44
As valve transfer has been used mainly in post-thrombotic syndrome, the outcomes in primaryDVR cannot be precisely assessed.
Recommended indications
� Primary superficial venous insufficiencyAs very few RCTs are available comparing director indirect valve restoration procedures to classicalsurgery, only weak recommendations can be statedconcerning their use. Furthermore, new techniquessuch as echo-guided foam sclerotherapy and endo-venous techniques such as radiofrequency and en-dovenous laser have recently emerged as valuablealternatives to traditional vein stripping.
It therefore looks difficult to recommend any par-ticular proceduresparing the saphenous trunk(usu-ally the great saphenous vein), but in young patientsand particularly in women who have children andare considering future pregnancies, ablation surgerymight not be the ideal recommendation.
– Angioscopy-assisted external valve repairIn angioscopy-assisted external valve repair, the su-tures are passed from outside to inside the lumen,directed by video-enhanced, magnified angioscopicimaging, allowing for precise approximation of thevalve cusps.32
� Percutaneous placed devicesThe percutaneous placed device, the Portland valve,consists of a square stent and porcine small intesti-nal submucosa covering, and is currently in a clin-ical phase I study.33
Clinical trial outcomes for surgical procedures
� Superficial venous systemIn all case series involving surgery to the superficialvenous system in which the outcome on varices wasreported, no assessment data is available on the val-ue of the saphenous trunk as a potential arterialsubstitute. � Indirect proceduresSeveral nonrandomized controlled studies have beenreported on the use of CHIVA, with both good clin-ical and hemodynamic outcomes at 3-year follow-up.3,4,34,35 Unfortunately, no randomized controlledtrial (RCT) versus conventional surgery is available.With regard to high ligation plus tributaries phle-bectomy plus/minus perforator ablation, two RCTs
U P D A T E
166 Venous valve dysfunction restoration by surgery in primary chronic venous disease – PerrinMEDICOGRAPHIA, VOL 30, No. 2, 2008
Figure 8. External valvu-loplasty: the transmuraltechnique according toKistner.Reproduced from reference 30:Bergan JJ. The Vein Book. SanDiego, CA: Elsevier AcademicPress; 2007. Copyright © 2007,Elsevier, Ltd.
Figure 9. External valvuloplasty: the transcommissural technique ac-cording to Raju and Neglen.Reproduced from reference 31: Raju S, Berry MA, Neglen P. Transcommissural valvulo-plasty: technique and results. J Vasc Surg. 2000;32:969-976. Copyright © 2000, Societyfor Vascular Surgery and The American Association for Vascular Surgery, a Chapterof the International Society for Cardiovascular Surgery.
A
A
B
A B
DC
B C

must be less than 12 seconds, and the difference be-tween pressure at rest and after standardized exer-cise in the standing position must be less than 40%.The decision to operate should be based on the clin-ical status of the patient, not the noninvasive data,since the patient’s symptoms and signs may not cor-relate with the laboratory findings.46 In addition tomeeting the clinical criteria, patients selected forsurgery should be highly motivated to participatein their recovery, since ultimate success is depen-dent on their compliance with postoperative man-agement.
In summary, primary reflux reconstructive sur-gery is recommended after failure of conservativetreatment and in young and active patients reluc-tant to wear permanent compression. Valvuloplastyis the most suitable technique, with Tripathi, Kist-ner, Perrin, and Sottiurai favoring internal valvulo-plasty,24,39,40,43 Raju recommends transcommissuralexternal valvuloplasty31 and Rosales favors transmu-ral valuloplasty.42 Some, but not all, authors recom-mend repairing several valves.24,42 �
� Primary deep venous insufficiencyIndications for deep valve repair are based on clin-ical severity, hemodynamics, and imaging.� Clinical severityMost authors recommend surgery in patients clas-sified as C6, and particularly with recurrent ulcer.In addition, given the good results associated withvalve repair for primary reflux, I feel that valve repairshould be considered in young and active patientspresenting with severe edema or C4b findings, inorder to avoid the lifetime use of compression gar-ments. When superficial and perforator venous in-sufficiencyoccur in association with DVR, they mustbe treated as well, either as the first step in therapyor in a staged fashion. Contraindications to recon-structive surgery include uncorrectable hypercoag-ulable state or ineffective calf pump of any etiology.� Hemodynamics and imagingOnly reflux that is considered grade 3 to 4 based onKistner’s criteria45 is usually appropriate for DVRsurgery. It is generally recognized that to be signif-icantly abnormal, the value for venous refill time
U P D A T E
167Venous valve dysfunction restoration by surgery in primary chronic venous disease – Perrin MEDICOGRAPHIA, VOL 30, No. 2, 2008
Number of limbs Follow-up Ulcer Hemodynamic results
Surgical treated (number of Etiology months recurrence or Competent �� AVPStudy author technique valves repaired) PVI/Total (mean) unhealed ulcer (%) valve (%) � VRT
Eriksson38 I 27 27/27 (49) N/A 19/27 (70) �� 81% (av)� 50% (av)
Masuda39 I 32 N/A 48-252 (127) (28) 24/31 (77)* �� 81% (av)� 56% (av)
Perrin40 I 85 (94) 65/85 12-96 (58) 10/35 (29) 64/83 (77) � Normalized56% (av)
Raju31,41 I 68 (71) N/A 12-144 16/68 (26) 30/71 (42) N/ATMEV 47 (111) N/A 12-70 14/47 (30) 72/111 N/ATCEV 141 (179) 98/41 1-42 (37) (59) �� 81% (av)
� Normalized100%
Rosales42 TMEV 17 (40) 17/17 3-122 (60) 3/7 (43) (52) �� 50% (av)
Sottiurai43 I 143 17/17 3-122 (60) 3/7 (43) (52) N/A
Tripathi 24 I 90 (144) 96/118 (24) (372) (79.8) N/ATMEV 12 (19) (50) (31.5) N/ATCEV
* no reflux or moderate reflux (<1 s) in 9 patients.
��
��
��
Number of extremities Follow-up Ulcer Hemodynamic results
Study author treated (number of Etiology months recurrence or Competent �� AVP(material used) valves repaired) Site PVI /Total (mean) unhealed ulcer (%) valve (%) � VRT
Akesson 27 20 (27) F, P 7/20 5-32 (19) 2/10 (20) PVI 7/7(100) PVI(Venocuff I) both PTS PTS 7/10 (4) �� 81% (av)
� 50% (av)PVI
�� 81% (av)� 50% (av)
Camilli44 (Dacron) 54 F 54/54 4-63 N/A 41/54 (76) N/A
Lane28 (Venocuff II) 42 (125) F, P 36/42 64-141 (93) (20) (90) �� ?� 100% (av)
Raju41 (Dacron) 28 F, P, T N/A 12-134 6/22 (27) 60/72 (83) N/A
��
��
��
Table I. Valvuloplastyclinical study results.Abbreviations: av, average; AVP,ambulatory venous pressure; I,internal valvuloplasty ; N/A, notapplicable; PVI, primary venousinsufficiency; TCEV, transcom-missural external valvuloplasty;TMEV, transmural external val-vuloplasty; VRT, venous refilltime; improved.
Table II. Banding, cuffing,external stent, and wrap-ping clinical study results.Abbreviations: av, average; AVP,ambulatory venous pressure; F, femoral; N/A, not applicable;P, popliteal; PTS, post-throm-botic syndrome; PVI, primaryvenous insufficiency; T, tibial(posterior); improved.
�
Table I.
Table II.
�

U P D A T E
168 Venous valve dysfunction restoration by surgery in primary chronic venous disease – PerrinMEDICOGRAPHIA, VOL 30, No. 2, 2008
LA CHIRURGIE RESTAURATRICE DANS LE TRAITEMENT DU REFLUX VEINEUX D’ÉTIOLOGIE PRIMITIVE
C omme le souligne Arkadiusz Jawien dans ce numéro deMedicographia, les techniques chirurgicales ont évolué dansla mesure où la restauration de la fonction d’un organe ou
d’un système a remplacé son exérèse. Cette dernière était la tech-nique la plus souvent utilisée dans la mesure où sa suppressionétait possible en termes de survie ou n’entraînait pas de pertur-bations physiologiques majeures. L’incompétence valvulaire estessentiellement identifiée dans les réseaux veineux superficiel etprofond ; elle est la cause d’un reflux qui peut entraîner une ma-ladie veineuse chronique. La suppression du réseau veineux su-perficiel pathologique était la technique de base jusqu’à ces 20dernières années car elle n’entraînait pas de trouble majeur de lacirculation de retour, mais depuis des techniques nouvelles se sontdéveloppées qui visent à supprimer le reflux par des procédés di-rects ou indirects. Deux types de méthodes indirectes peuvent êtreidentifiées : (1) celles qui visent à supprimer les points de fuitedu réseau veineux profond vers le réseau veineux superficiel enconservant le tronc saphène : cure hémodynamique de l’insuffi-
sance veineuse ambulatoire (CHIVA), ligature résection de lajonction saphéno-fémorale et/ou saphéno-poplitée associée à unephlébectomie des collatérales +/– ligature des perforantes ; (2)celles qui se proposent de restaurer la fonction valvulaire en ré-duisant le calibre des troncs saphènes par suppression du ré-servoir distal : phlébectomie ambulatoire, ablation sélective desvarices sous anesthésie locale (ASVAL). La réparation directevalvulaire par manchonnage ou valvuloplastie externe est plusrarement entreprise pour traiter l’insuffisance veineuse super-ficielle. La suppression du réseau veineux profond incontinentn’est pas possible car elle entraîne des troubles majeurs de la cir-culation de retour et sa ligature n’est pas efficace. La techniquede choix est donc la reconstruction valvulaire ou valvuloplastie ;le transfert valvulaire ou les valves prothétiques sont exception-nellement réalisés dans cette étiologie. Sont successivement dé-veloppés dans cet article les techniques, les résultats et enfin lesindications de la chirurgie restauratrice de la fonction valvulairedans l’insuffisance veineuse primitive.
Surg.1991;14:645-648.33. Pavcnik D, Uchida BT, Timmermans HA, et al. Per-cutaneous bioprosthetic venous valve: a long termstudy in sheep. J Vasc Surg. 2002;35:598-602.34. Escribano JM, Juan J, Bofill R, et al. Durability ofreflux by a minimal invasive CHIVA procedure on pa-tients with varicose veins. Eur J Vasc Endovasc Surg.2003;25:159-163.35. Maeso J, Juan J, Escribano JL, et al. Résultats cli-niques comparés du stripping et de la cure CHIVAdans le traitement des varices des membres inférieurs.Ann Chir Vasc. 2001;15:661-665.36. Campanello M, Hammarsten J, Forsberg C, Bern-land P, Henrikson O, Jensen J. Standard stripping ver-sus long saphenous vein saving surgery for primaryvaricose veins: a prospective, randomized study withthe patients as their own controls. Phlebology.1996;11:45-49.37. Large J. Surgical treatment of the saphenousvarices, with preservation of the main great saphenoustrunk. J Vasc Surg. 1985;2:886-891.38. Eriksson I, Almgren B. Surgical reconstruction ofincompetent deep vein valves. Ups J Med Sci.1988;93:139-143.39. Masuda EM, Kistner RL. Long term results of ve-nous valve reconstruction: a four to twenty-one yearfollow-up. J Vasc Surg. 1994;19:391-403.40. Perrin M. Reconstructive surgery for deep venousreflux. Cardiovasc Surg. 2000;8:246-255.41. Raju S, Fredericks R, Neglen P, Bass JD. Durabil-ity of venous valve reconstruction for primary andpostthrombotic reflux. J Vasc Surg.1996;23:357-367.42. Rosales A, Slagsvold CE, Kroese AJ, Stranden E,Risum O, Jorgensen JJ. External venous valveplasty(EVVP) on patients with primary chronic venous insuf-ficiency (PCVI). Eur J Vasc Endovasc Surg.2006;32:570-576.43. Sottiurai VS. Current surgical approaches to ve-nous hypertension and valvular reflux. J Int Angiol.1996;5:49-54.44. Camilli S, Guarnera G. External banding valvulo-plasty of the superficial femoral vein in the treatmentof primary deep valvular incompetence. Int Angiol.1994;13:218-222.45. Kistner RL, Ferris RG, Randhawa G, Kamida CB.A method of performing descending venography. J VascSurg. 1986;4:464-468.46. Iafrati MD, Welch H, O’Donnel TF, Belkin M, Um-phrey S, MacLaughlin R. Correlation of venous non-invasive tests with the Society for Vascular Surgeryclinical classification of chronic venous insufficiency.J Vasc Surg. 1994;19:1001-1007.
REFERENCES1. Perrin M. Chirurgie à ciel ouvert de l’insuffisanceveineuse superficielle. Principes. Techniques. Résul-tats. EMC (Elsevier Masson SAS, Paris), TechniquesChirurgicales—Chirurgie Vasculaire. 2007;43-161-B. 2. Francheschi C. Theorie et Pratique de la Cure Hé-modynamique de l’Insuffisance Veineuse en Ambula-toire. Paris, France: De l’Armançon; 1989.3. Zamboni P, Marcellino MG, Cappelli M, et al. Saphe-nous vein sparing surgery : principles, techniques andresults. J Cardiovasc Surg. 1998;39:151-162.4. Zamboni P, Cisno C, Marchetti F, Quaglio D, MazzaP, Liboni A. Reflux elimination without any ablationor disconnection of the saphenous vein. A haemody-namic model for venous surgery. Eur J Vasc EndovascSurg. 2001 ;21:361-369.5. Franceschi C. Fractionnement dynamique de lapression hydrostatique, shunts fermés et ouverts, évo-lutivité veineuse vicariante. En quoi ces concepts ont-ils fait évoluer le traitement des varices? Phlébologie.2003;56:61-66.6. Hammarsten J, Pederson P, Cederlund CG, Cam-panello M. Long saphenous vein saving surgery forvaricose vein. A long term follow-up. Eur J Vasc Surg.1990;4:361-364.7. Muller R. Mise au point sur la phlébectomie ambu-latoire selon Muller. Phlébologie. 1996;49:335-344.8. Pittaluga P, Rea B, Barbe C. Méthode ASVAL (ab-lation selective des varices sous anesthésie locale).Principes et résultats préliminaires. Phlébologie. 2005;58:175-181.9. Belcaro G. Plication of the saphenofemoral junctionPhlebology. 1991;7:121-124.10. Belcaro G, Errichi BM. Selective saphenous valverepair: a 5-year follow-up study. Phlebology.1992;7:121-124.11. Zamboni P, Liboni A. External valvuloplasty of thesaphenofemoral junction using perforated prosthe-sis. Phlebology. 1991;6:159-165.12. Lane RJ, McMahon C, Cuzilla M. The treatment ofvaricose veins using the venous valve cuff. Phlebol-ogy.1994;9:136-145.13. Schanzer H, Skladany M. Varicose vein surgerywith preservation of the saphenous vein : a compari-son between high ligation-avulsion versus sapheno-femoral banding valvuloplasty avulsion. J Vasc Surg.1994;20:684-687.14. Sakatowa H, Hoshino S, Igari T, Takase S, OgawaT. Angioscopic external valvuloplasty in the treatmentof varicose veins. Phlebology. 1997;12:136-141.15. Corcos L, De Anna D, Zamboni P, et al. Repara-tive surgery of valves in the treatment of superficialvenous insufficiency. J Mal Vasc. 1997;22:128-136.
16. Agus GB, Bavera PM, Mondani P, Santuari D. Ex-ternal valve-support for saphenofemoral junction in-competence: randomized trial at 3 years follow-up.Acta Phlebologica. 2002;3:101-106.17. Camilli S. Le manchonnage périveineux de la ter-minaison saphéno-fémorale dans le traitement de l’in-suffisance de la grande veine saphène et la préventiondes récidives. Phlébologie. 2002;55:343-349.18. Geier B, Geier B, Voigt I, et al. External valvulo-plasty in the treatment of greater saphenous insuffi-ciency: a five-year follow-up. Phlebology. 2003;18:137-142.19. Lane RJ, Graiche JA, Coroneos JC, Cuzilla ML.Long term comparison of external valvular stentingand stripping of varicose veins. ANZ J Surg. 2003;73:605-609.20. Perrin M. Repair of venous valves in severe chron-ic venous insufficiency. In: Bergan JJ, Shortell CK, eds.Venous Ulcers. Amsterdam, Holland; Boston, Ma: El-sevier Academic Press; 2007:243-257.21. Kistner RL. Surgical repair of a venous valve.Straub Clin Proc. 1968;24:41-43.22. Raju S. Venous insufficiency of the lower limband stasis ulceration. Ann Surg. 1983;197:688-697.23. Sottiurai VS. Technique in direct venous valvulo-plasty. J Vasc Surg. 1988;8:646-648.24. Tripathi R, Sieunarine K, Abbas M, Durrani N. Deepvenous valve reconstruction for non-healing leg ulcers:techniques and results. ANZ J Surg. 2004;74:34-39.25. Kistner RL. Transposition techniques. In: JJ Ber-gan, RL Kistner, eds. Atlas of Venous Surgery.Philadel-phia, PA: WB Saunders; 1992:153-156.26. Maleti O. Venous valvular reconstruction in post-thrombotic syndrome. A new technique. J Mal Vasc.2002;27:218-221.27. Akesson A, Risberg B, Bjôrgell O. External supportvalvuloplasty in the treatment of chronic deep vein in-competence of the legs. Intern Angiol.1999;18:233-238.28. Lane RJ, Cuzilla ML, McMahon CG. Intermediateto long-term results of repairing incompetent mul-tiple deep venous valves using external stenting. ANZJ Surg. 2003;73:267-274.29. Kistner RL. Surgical technique of external venousvalve repair. Straub Found Proc. 1990;55:15-16.30. Bergan JJ. The Vein Book. San Diego, CA: ElsevierAcademic Press; 2007. 31. Raju S, Berry MA, Neglen P. Transcommissuralvalvuloplasty: technique and results. J Vasc Surg.2000;32:969-976.32. Gloviczki P, Merrel SW, Bower TC. Femoral veinvalve repair under direct vision without venotomy:a modified technique with use of angioscopy. J Vasc

ouis XVI was 20 years of age when he acceded to the throne of France and Navarre in 1774 on thedeath of his grandfather Louis XV the well-beloved (born in 1710). Born at Versailles on August 23,
1754, Louis XVI lost his father when he was 11 years old and his mother when he was 13 years old.As Duke of Berry, he received a strict religious education under the guardianship of the obscureDuke de La Vauguyon (1706-1772) and Bishop Jean Gilles de Coëtlosquet (1700-1784), who also
saw to the education of his three brothers. He was a hard-working pupil whose favorite subjectswere Latin, mathematics, physics, the maritime sciences, history, and geography. He was a frequent visi-tor to the workshop that Jean-Antoine Nollet (1700-1770), priest and experimental physicist, had installedin Versailles. He was the first French monarch to be fluent in English, reading House of Commons debates,translating English works, and building a collection of English periodicals and newspapers. In addition,and on his own initiative, he learned Italian and Spanish. Although his tutor, de La Vauguyon, took greatcare to isolate him from the philosophy of the Enlightenment, he nevertheless read The Spirit of the Laws(L’Esprit des Lois) by Montesquieu (1689-1785). The future Louis XVI was not keen on the military arts,despite his reputation as an excellent horseman.
169The sciences under Louis XVI. A king torn between enlightenment and revolution – Régnier MEDICOGRAPHIA, VOL 30, No. 2, 2008
A T O U C H O F F R A N C E
he main political problem during the reign of Louis XVI, compounded by the expense of Frenchaid during the American War of Independence, was the constant undermining by the nobility
and senior clergy of attempts to abolish their privileges. The forces most hostile to change were for-ever marshaled against the King, who failed to attract support from the more enlightened elements of
the nobility. Reserved, shy, and modest, Louis XVI knew what he wanted but was loath to give orders.He was a reluctant participant in Court ceremonial, thus indirectly depriving the nobility of their rep-
resentational social role. His main failing was an inability to command. He was forever torn between thereformist ideas of the Enlightenment and deep attachment to tradition. Although respectful of the fun-damental laws of the land and unwilling to contravene them, he appointed reforming ministers—only todismiss them shortly afterward. The last absolute French monarch by divine right, he had a natural in-terest in scientific experiment, research, and discovery. He lost no opportunity of offering moral and fi-nancial support to new undertakings that might advance human knowledge and improve the conditionof the masses: expansion of the Academy of Sciences, creation of the Royal Society of Medicine, the hot-air balloon and steam engine trials, the voyage of La Pérouse, implementation of hospital hygiene, andinstitutions for the blind and deaf-and-dumb. Long misunderstood in French history and often despised,the biographies of Louis XVI and Marie-Antoinette in the pre-Revolution political context are now beingrewritten. Medicographia. 2008;30:169-178. (see French abstract on page 178)
T
Christian RÉGNIER, MDPraticien Attaché des Hôpitaux de ParisSociété Internationale d’Histoire de la Médecine9 rue Bachaumont, 75002 Paris, FRANCE(e-mail: [email protected])
The sciences underLouis XVI
A king torn between enlightenment and revolution
b y C . R é g n i e r , F r a n c e
L

On May 16, 1770, he married Archduchess Marie-Antoinette of Austria (1755-1793), the younger daugh-ter of Emperor Francis I of Lorraine. Husband and wife were 15 and 14 years of age. Their marriage em-bodied the alliance between the kingdoms of France and Austria. Louis XVI and Marie-Antoinette had fourchildren: Marie Thérèse (1778-1851), known as Madame Royale, Louis Joseph (1781-1789), Louis Charles(1785-1795), the future Louis XVII, who was to meet a tragic fate, and Sophie Béatrice (1786-1787).1-4
The years in waiting: an unconventional princeWhen 2 years old, the young Duke had teething problemsand was losing weight. The Genevan physician ThéodoreTronchin (1709-1781), author of the article on “inocu-lation” in the Encyclopédie and senior physician to theDuke of Orléans, was visiting Versailles at the time. Herecommended exposing the royal children to fresh air.Tronchin had the ear of the Court, yet was also a friendof Voltaire (1694-1778), Denis Diderot (1713-1784), andJean-Jacques Rousseau (1712-1778). He was an Enlight-enment physician and an advocate of smallpox inocula-tion using Variola minor (variolation).
After staying nearby to Meudon Forest, the youngDuke of Berry and his brothers returned to Versailles.Louis was brought up with his elder brother, the Dukeof Burgundy, who died in 1761 from pulmonary tuber-culosis aged 10, leaving Louis to inherit the crown bydefault. His childhood was marked by loneliness, lack ofaffection, and a succession of bereavements: after hiselder brother, came his father (1765), mother (1767), andgrandfather Louis XV (1774).1,2
“My grandson is not very passionate,” Louis XV wrotethe Infant of Parma in June 1770, deploring the futureKing’s lack of alacrity in consummating his marriage toMarie-Antoinette, “…[he is] unlike other men.” In July,2 months after the wedding, the Dauphin was examinedby Germain Pichault de la Martinière (1697-1783), sur-geon to the King, for any anatomical abnormality that
might explain the absence of sexual relations (the young Duke was almost 16 and Marie-Antoinette 14).The surgeon found no abnormality, in particular no phimosis (“narrowness of the passage”). He suggestedthat “constitutional frigidity” might be responsible, a diagnosis confirmed in 1773 by the King’s physician,Jean-Marie François de Lassonne (1717-1778). We should recall that the young prince was being educatedin the puritanical Jansenist moral code by a tutor who taught that “children conceived by too young afather are of a delicate constitution and do not live long,” and that “there is also a risk that their fatherbecomes a libertine.” The unconsummated marriage became an affair of State and the focus of all mali-cious gossip at Court; the Count of Fuentès, the Spanish ambassador, saw it as a case of “constitutionalfrigidity induced by the teachings of Duke de La Vauguyon.”1,2,4
Other factors included the fact that the young prince’s interests were not shared by his wife. Whereasher tastes ran to singing, dancing, balls, music, and fine clothes, Louis liked hunting and all kinds of man-ual work, with locks, clocks, and carpentry. His cabinet was equipped with a forge, workbench, a coupleof anvils, and numerous tools. He took untold pleasure in joining craftsmen at their work “moving ma-terials, planks, and cobblestones, and undertaking such heavy exercise for hours at a time that he some-times came back more exhausted than any laborer forced into such work.” In 1773, de Lassonne prescribedthe young prince some cinchona and “Mars balls” (alcoholic concoctions of iron filings and tartar) in anattempt to kick-start his libido.3,4
As for the Dauphine, she was somewhat offhand in her compliance with the practices of the French court.She kept company with a coterie of young people with scant respect for etiquette. This attitude broughtreprimands from her mother, Maria-Theresa, who wrote to her: “It is said that you are beginning to makefun of people, to burst out laughing in their faces… By going out of your way to please five or six youngladies or gentlemen, you risk alienating everyone else.”4
On May 10, 1774, Louis XV died of smallpox, having refused to inoculate his family (only the Duke ofOrléans, who was more open to modern ideas, had had variolation performed on his children). “The Kingis dead! Long live the King!”
A T O U C H O F F R A N C E
170 The sciences under Louis XVI. A king torn between enlightenment and revolution – RégnierMEDICOGRAPHIA, VOL 30, No. 2, 2008
Portrait of Louis XVI byAntoine-François Callet,
1788. © Krause, Johansen/Archivo Iconografico,
SA/CORBIS.

Louis XVI was crowned in Reims on June 10, 1715. Four days later, he conducted the age-old ceremonyof the royal touch, a time-honored rite performed by French kings since Robert the Pious in the 10th cen-tury. In the park of the abbey of Saint Rémi in Reims, bareheaded and wearing the cloak of the Holy Ghost,he touched some 2400 patients afflicted with scrofula, the “King’s evil,” making the sign of the Cross overthem, and speaking the words: “The King toucheth thee; the Lord healeth thee” (the chronicle of the eventrecorded four cures). Louis XVI repeated this medieval ceremony five times in the course of his reign.4
Successes and setbacks in the reignLouis’ grandfather, Louis XV, his father (the Dauphin), and his tutor, de La Vauguyon, inculcated the youngprince with their patriarchal monarchy ethic. Kings were both shepherd and father to their flock. Thisconception of the exercise of royal power was influenced by a religiously inspired moral philosophy thattaught the subservience of the temporal domain to the demands of its spiritual counterpart. Clearly, nosuch principle had been espoused by the Sun King, Louis XIV, for whom radiance of the monarch, reasonof State, preeminence of law, and national prestige outweighed all other moral or religious considerations.
A diligent worker and regular attendee at the Council of Dispatches (which received administrativereports from provincial governors) and Council of State, Louis XVI set about becoming an exemplary “goodking.” He sought to do good and keep to the fundamental laws of the kingdom. His reign was dotted with
gestures of generosity: restoration of the regional or cityparliaments (1774), creation of the pawnshop in Paris todiscourage usury (1777), abolition of torture (1780), abo-lition of craft guild privileges and of the corvée royale,by which peasants donated their labor on royal high-ways (1780), institution of an extensive public worksprogram, abolition of the poll tax on Jews (1784), andthe granting of civil status to Protestants (1788).3
Louis XVI’s intelligence shone best in foreign policy.He built up a royal navy powerful enough to rival thatof England, as shown during the American War of In-dependence. Signed at Versailles on September 3, 1783,the Treaty of Paris marked the creation of the UnitedStates of America. It reflected France’s military and eco-nomic commitment to the rebels and erased the humil-iation of the Treaty of Paris signed 20 years previously,marking the loss of the French possessions in NorthAmerica. It also signaled the return of France as an ar-biter of European policy.2,4
However clear-sighted he may have been in foreignpolicy, Louis XVI had difficulty in imposing his author-ity within France. He dismissed his ministers as soon
A T O U C H O F F R A N C E
171The sciences under Louis XVI. A king torn between enlightenment and revolution – Régnier MEDICOGRAPHIA, VOL 30, No. 2, 2008
King Henri IV touching scrofula sufferers. Engravingby André de Laurens, 1609.The « Royal Touch » was believed to cure scrofula, or“King’s Evil,” aka, cervical tuberculous lymphadenopathy.Philip I was the first Frenchking to start the practice,which all French kings, includ-ing Louis XI, continued up to King Charles X on 29 May1825. © Roger Viollet.
French Map of the Battle of the Chesapeake on September 5, 1781,between a French fleet led by Rear-Admiral Comte de Grasse and aBritish fleet, led by Rear-Admiral Sir Thomas Graves. As a result,the Royal Navy was unable to resupply the forces of General LordCornwallis, who surrendered after at Yorktown to George Washing-ton and his French ally, General Rochambeau. The battle ended 6 years of war and won American independence. © CORBIS.

as any obstacle emerged that appeared insurmount-able, in particular, resistance by the parliaments. Yethe did not hesitate to appoint men of the Enlighten-ment as his ministers. Determined to push throughfiscal reforms, he called on Jacques Turgot (1727-1781) in 1774, then on the Geneva banker JacquesNecker (1732-1804) in 1776, dismissing both beforethey could complete their stabilization of the royalfinances. At the instigation of the Controller-Gener-al of Finance, Charles Alexandre de Calonne (1734-1802), the King convened the Assembly of Notablesin 1787 with a view to carrying out fiscal and finan-cial reform. King and minister sought to establishequality in taxation by seeking contributions fromthe notables themselves, setting up provincial as-semblies that would rule on public finance issues, abolishing internal customs barriers, and freeing upthe grain trade. The Assembly disbanded without reaching a conclusion. Senior clergy and nobility refusedto pay the tax. Calonne was dismissed. His successor, Bishop Étienne Charles Loménie de Brienne (1727-1794), faced a parliamentary revolt. On the advice of Necker, Louis XVI convened the Estates-General, com-prising clergy, nobility, and Third Estate (middle class). However, voting was to proceed by estate, enablingthe clergy and nobility to outvote the Third Estate, rather than by overall poll, which would have enabledthe numerically much superior Third Estate to carry the day.1,3,5
Louis XVI was not against a measure of reform. On July 17, 1789, 3 days after the Paris insurrection thatfollowed the dismissal of Necker, the King went to the city hall proudly sporting the revolutionary cocade(white, the French royal color, framed by red and blue, the colors of Paris). But this well-received gesturewas marred on August 4 by his refusal to sign the Declaration of the Rights of Man or the decree abolish-
ing feudal privileges. Forced back to Paris fromVersailles, Louis XVI appeared to accept his roleas constitutional monarch, no longer King ofFrance by divine right, but King of the French.At the Champ-de-Mars, on July 14, 1790, theKing went to the feast of the Federation, tookhis oath to the Constitution, and was acclaimedby the crowd. But his faith could not accept thetransformation of the clergy into civil servants.His last hopes resting with an armed coup deforce, he fled with his family in the night ofJune 20 to 21, 1791. His prestige and creditwere at rock bottom, and he was imprisoned inthe Temple prison. On August 10, 1792, he wascondemned to death, then guillotined on Jan-uary 21, 1793. His bravery in the face of deathsent a wave of emotion sweeping through Eu-ropean courts and inspired the first militarycoalition against the fledgling republic.1,2,4,5
Influence of the Encyclopédie on the intellectual climateWith its 600 000 inhabitants, Paris was the largest city in the Western world after London. The Bourboncapital was the center of intellectual and financial life, a hub for the arts and sciences. It was only naturalthat Paris should have been the setting for a remarkable intellectual event: the publication of the sum ofhuman knowledge, revised and corrected in the light of philosophical thought.
In the 1750s, triggered by the writings of Voltaire, a break occurred in the customs and traditions ofconventional philosophical thought. Cornerstones of this enlightened thinking included: a belief in theelimination of ignorance through scientific progress; trust in observation and experimentation; aspira-tion to individual happiness; glorification of reason as opposed to religious dogma; and concern for a newcivil and democratic morality.
This was the intellectual climate that welcomed the birth of a monument to Western knowledge. Thefirst volume of the Encyclopédie (Encyclopedia, or a systematic dictionary of the sciences, arts, and crafts)appeared in 1751; 28 volumes of text and 15 volumes of plates were published up to 1780. This unprece-
A T O U C H O F F R A N C E
172 The sciences under Louis XVI. A king torn between enlightenment and revolution – RégnierMEDICOGRAPHIA, VOL 30, No. 2, 2008
MAXIMS AND THOUGHTS OF LOUIS XVI
“A country can never be governed against itshabits.”
“An absolutely essential maxim in govern-ment is to prevent the population from fallinginto the sort of indifference that makes themthink that it matters not whether they live un-der one kind of dominion or another.”
“A sovereign can do nothing more usefulthan inspire the idea of their own greatness inhis people.”
“It’s legal because I want it.”
Execution of King Louis XVI, on today’s
Place de la Concorde, inParis, on January 21,
1793. © Bettmann/CORBIS

dented publication comprised 17 000 articles written by 140 contributors of differing backgrounds andspecialties. According to Diderot and Jean le Rond d’Alembert (1717-1783), the Encyclopédie aimed “togather together the knowledge scattered across the surface of the globe and expose its general system tothose who will come after us so that the work of centuries past will not have been in vain for the centuriesthat follow.” What was novel about the Encyclopédie was not only its exhaustive determination to recordthe sum of human knowledge, but to articulate theory closely with practice “in one and the same visionof progress.” The publication was also innovatory in its systemic cross-referencing, thereby emphasizingits determination to break down the barriers between the different disciplines within human knowledge.The Encyclopédie interpreted the sum of knowledge in the light of critical reason and integrated thisknowledge into a consistent philosophical system. “All our di-rect knowledge can be reduced to what we receive through oursenses,” wrote D’Alembert, “whence it follows that we owe allour ideas to our sensations.”6,7
Financed by subscription, the work was published in Paris(first seven volumes), then from March 1759 onward in Neu-châtel (Switzerland). Because it espoused sensualist and ma-terialist theories that questioned the spirituality of the souland justified atheism, the Encyclopédie was not well receivedby the authorities. The Paris Parliament issued a ban in 1759and ordered the seven volumes already published to be de-stroyed. Despite bans and other forms of obstruction, the En-cyclopédie and its numerous pirated foreign versions founda wide public among notables, including magistrates, civil ser-vants, cultured bourgeois, artists, merchants, and the enlight-ened nobility (ie, those sectors who were to prove most activein the Revolution). It was even supported in many circles upto and including the Court: a portrait by Maurice Quentin dela Tour (1704-1788) depicted Louis XV’s favorite, Madame dePompadour, turning the pages of the Encyclopédie. The En-cyclopedists also received unfailing backing from Malesherbes(1721-1794), the director of the book trade and royal censor-ship from 1750 to 1763, who enjoyed the esteem of the youngLouis XVI. After first reading the Encyclopédie in 1777, andrecognizing its scientific and technical qualities, the King or-dered the establishment of a Museum of Sciences and Technology in 1781. It was the forerunner of thepresent-day Museum of Arts and Crafts (Musée des Arts et Métiers).6,7 The philosophy of the Enlightenment,embodied in the Encyclopédie, bore within it the seeds of the 1789 revolution: the progress of universalknowledge would free mankind from the irrational beliefs responsible for fanaticism. The philosophersof the Enlightenment did not separate the order of reason and nature from the moral and social order. Menwere born free and equal, and social rank was to be determined on merit alone. The implications behindan intellectual project of this kind could not escape the notice of those in power, and they also won overa number of enlightened minds.
On the other hand, there are historians who believe that the Revolution invented the Enlightenmentin order to legitimize itself through a corpus of philosophical knowledge. In defense of this view, it must berecognized that the Enlightenment never addressed the masses.4,6,7
The King as enlightened protector of the sciencesUnder Louis XVI, the Academy of Sciences, which had been founded in 1666 by Jean-Baptiste Colbert (1619-1683), grew by three new sections: general physics, natural history, and mineralogy, thereby complement-ing its six other sections (geometry, astronomy, mechanics, anatomy, chemistry, and botany). Scientistsfrom around the world working in the leading learned societies came to Paris to test and add to their knowl-edge. Between 1720 and 1780, the proportion of scientific publications doubled, to the detriment of theirtheological counterparts. In the spirit of the Encyclopédie, during the reign of Louis XVI, the 39 academiesin Paris and the provinces were keen to report any scientific discoveries and innovations with the poten-tial for directly transforming daily life. The King took a great interest in the activities of these engineersand scientists and encouraged their experiments and initiatives.4
Louis XVI had been fascinated by science since childhood. He could handle calculations in algebra, hada solid grounding in physics, was acquainted with Boyle’s law, and knew how to do section drawings ofbuildings and instruments. Proud of his epoch’s discoveries, he had no hesitation in sporting a bouquet of
A T O U C H O F F R A N C E
173The sciences under Louis XVI. A king torn between enlightenment and revolution – Régnier MEDICOGRAPHIA, VOL 30, No. 2, 2008
Engraved plate from Diderot’s Encyclopedia.Louis XVI was a fervent amateur locksmith,and enjoyed lockwork as much as he didhunting. All rights reserved.

potato blossom in his buttonhole in honor of the tu-ber raised from pigsty to dining table by the chemistAntoine Parmentier (1737-1813). Following therecognition by the Paris Faculty of Medicine in 1772(for which Parmentier was largely responsible) thatthe potato was harmless to human health, the Kinggranted Parmentier the Sablons plain near Neuillyto develop his crop. Large-scale potato cultivationwas to play a considerable role in eradicating the
famines that periodically ravaged the French countryside when climatic disasters decimated the grainharvest; during such crises, potato replaced cereal in the baking of bread (the staple food of the French).Even so, during the Revolution, Louis XVI’s endorsement of Parmentier was to make the chemist suspectin the new regime’s eyes.8,9
In 1783, Louis XVI drew on his own resources to finance the hot-air balloon experiments by the Mont-golfier brothers. The first test of a spherical balloon took place in Annonay on June 5. The 800 m3 ballooninflated with hot air weighed 225 kg. It rose 1000 meters into the sky and traveled 2 kilometers. Lookingfor financial backing, and supported by the Academy of Sciences, Jacques-Étienne Montgolfier (1745-1799)went to Paris and gave a demonstration at Versailles on September 19 before King and Court. This time,the blue taffeta balloon decorated with fleur-de-lis was larger (1000 m3), and carried a sheep, rooster, andduck in a basket. The King asked for explanations, and was shown the huge straw-fired stove that producedhot air to propel the balloon. The trial was successful, with the animals returning alive. The King gavepermission for an experiment with a human being. On June 23, 1784, the Marie-Antoinette, a balloon dec-orated with the French and Swedish coats of arms, lifted off in Versailles in front of the royal family andGustav III, King of Sweden. It transported its two passengers, Jean-François Pilâtre de Rozier (1754-1785)and Louis Proust (1754-1826), senior pharmacist at the Salpêtrière Hospital, all the way to the Forest ofChantilly, a distance of 52 kilometers. Bowled over by the invention, the King awarded Jacques-Étiennethe ribbon of St Michael, gifted an annuity to his brother Joseph Michel (1740-1810), ennobled their father,
and granted the two brothers a substantial sum to continue their hot-air experiments.8,10 Louis XVI also encouraged industrial applicationsof the steam engine. He would regularly arrange to be presented withnovel ideas, in some cases supporting them from the privy purse. Thiswas not the case for the Périer brothers, Jacques-Constantin (1742-1818)and Auguste Charles, who had to use their own funds to build a pumpat Chaillot to supply Paris with water from the Seine; the pump wasdriven by two steam engines. The Périer brothers were skilled mechan-ics, and they applied their pressurized steam method to blast furnaces,enabling them to manufacture cylinders, pendulums, and new cottonspinning machines.8,11
In 1783, Louis XVI backed attempts by the Marquis Jouffroy d’Abbans(1751-1832) to fit the steam engine into boats. Newspapers of the timereported the progress of a paddle steamer, the Pyroscaphe, on the Saônenear Mâcon. Unfortunately, opposition from the Academy of Sciencesand the intervention of the Revolution meant that glory never came theway of Jouffroy d’Abbans.8,12
“Have we any news of Monsieur de la Pérouse?”During his adolescence, Louis XVI read the account published in 1771by Louis Antoine de Bougainville (1729-1811) of his circumnavigationof the globe (1766-1769). He was also interested in the archipelago thatYves-Joseph de Kerguelen de Trémarec (1734-1797) discovered in thesouthern Indian Ocean. In his apartments in Versailles, Louis XVI wassurrounded by astrolabes, barometers, thermometers, chronometers,
A T O U C H O F F R A N C E
174 The sciences under Louis XVI. A king torn between enlightenment and revolution – RégnierMEDICOGRAPHIA, VOL 30, No. 2, 2008
Agronomist Antoine Augustin Parmentier presentingLouis XVI with a bunch of potato flowers. Potatoes werefirst grown in France in the sandy ground at Les Sablons,in Neuilly, near Paris.Legend has it that the crop wasguarded by heavily armed royal troops so that the popu-lace, very mistrustful of the palatability of this new plant,would be convinced it was very precious, for it to be soprotected. © Roger-Viollet.
Man’s first ascent from Earth, on November 21,1783. Pilâtre de Rozier and Marquis d’Arlandeswave from the gallery of their Montgolfier airballoon as they set out from Paris. © Bettman/CORBIS.

sighting instruments, and Delille’s nautical charts (renowned for their accuracy). He even translated thejournals of Captain James Cook (1728-1779), having a particular appreciation for the scientific objec-tives behind Cook’s travels (the attempts to resolve certain problems of astronomy and mathematics inorder to correct longitude errors on nautical charts).4,8 Louis was keen for France to punch at its weight inadvancing geographic and maritime science. His personal choice for this mission fell on Jean-Françoisde Galaup, Comte de La Pérouse (1741-?1788). He annotated the report by the Minister for Naval Affairsin his own hand and set the commercial and maritime aims of the voyage:
As for the reconnoitering part, the main points are reconnoitering the north west part of America, whichconverges with the commercial part, and reconnoitering the Sea of Japan, which also converges with thecommercial part; but for that, I think that the season proposed in the Report is a poor choice for reconnoi-tering the Solomon Islands and the south west of New Holland (Australia). All the other points ought to besubordinated to the former; we should restrict ourselves to what is most useful, and to what can be done com-fortably, within the three years proposed.8,13,14
After the Anglo-French peace treaty of 1783, Louis XVI developed an ambitious colonial policy andmapped out clear political and commercial objectives for the expedition: monitoring English navy activ-ity; inspecting Dutch and Spanish trading posts; studying Russian trade in the Kamchatka peninsula;moving into the fur trade; and setting up a network of safe and strategic ports and trading posts across
the Pacific for expanding trade with Rus-sia and China. The expedition also hada medical objective: to test a diet thatwould prevent scurvy, typhus, and ty-phoid fever. Special attention was paidto the method of storing water, flour,and food; molasses were loaded againstscurvy, modeled on Cook’s success inpreventing the disease.
Four surgeons were recruited; theirmedicine chests contained 157 differentremedies, and the King insisted that hewould regard “completion without theloss of a single life as the expedition’shappiest outcome.”13,14 Alas, there wereto be no survivors from the expedition,but up to his final log, filed from BotanyBay, La Pérouse reported virtually no caseof scurvy.
On August 1, 1785, the Boussole andthe Astrolabe left Brest, carrying scien-tists, botanists, cartographers, natural-ists, and watchmakers (to ensure the ac-
curacy of the marine chronometers that were essential for plotting longitude). At each port of call, LaPérouse sent the King a copy of his logbook. The expedition lasted over 21/2 years and finished with thedisappearance of the 200 crew off Vanikoro (Solomon Islands) in February 1788. Legend has it that a fewhours before his execution, Louis XVI asked: “Have we any news of Monsieur de La Pérouse?”8,13,14
The King’s creation of the Royal Society of MedicineNumerous epidemics had ravaged France since the last visit by plague in 1720: smallpox (1776-1786),measles (1776-1786), dysentery (1779, 1792), and pneumonia (1784-1785). On April 29, 1776, in an attemptto study and prevent such afflictions, the King set up a Commission of medicine in Paris to maintain cor-respondence with physicians in the provinces on all that may pertain to human and animal epidemicdisease. Turgot, Controller-General of Finances, entrusted the anatomist Félix Vicq d’Azyr (1748-1794) withthe founding of the Commission that became the Royal Society of Medicine by letters patent on August 20,1778. A member of the Academy of Sciences, Vicq d’Azyr was the author of the article on morbid anatomyin the Encyclopédie. The Royal Society of Medicine (half-way between academy and government think-tank) boasted the most progressive physicians of the Enlightenment era among its members. It met inthe Louvre in the courtroom of the Secretary of State for the King’s Household. Attacked from its incep-tion by the Paris Faculty of Medicine, the Society was inspired by a pioneering spirit. Its aim was to collectserial data on the epidemiology of infectious disease, the state of the soil and water supply, medical topog-raphy, and meteorology, all on a monthly basis, right across France. The survey was hugely ambitious in
A T O U C H O F F R A N C E
175The sciences under Louis XVI. A king torn between enlightenment and revolution – Régnier MEDICOGRAPHIA, VOL 30, No. 2, 2008
Louis XVI, on June 29, 1785, giving his instructions to La Pérouse about to set out on his voyage around the world. Painting by Monsiau Nicolas André, oil on canvas,2.72�2.7 m, at the Musée du Château de Versailles, 1817. © Gérard Blot/RMN.

that it sought not only to map French epidemiological risk but to lay down general principles of hygieneapplicable to prisons, hospitals, schools, barracks, ports, and ships. In return, corresponding physicians inFrance and abroad were to receive information on the clinical aspects of infections and their treatment.Considered as the largest administrative survey ever undertaken in the 18th century, the study remainedunder the authority of the Controller-General of Finances who authorized no other institution, even theAcademy of Sciences, to concern itself with statistics in its place. As a result, the conduct of the study re-mained under the supervision of royal civil servants.15-17
To ensure that measurements were reliable, Vicq d’Azyr asked physicians to purchase mercury instru-ments from Paris or London and to calibrate them using the method of Charles Messier (1730-1817) inthe case of barometers and the method of René de Réaumur (1683-1757) in the case of thermometers. In
practice, many corresponding physicians did not have the instrumentsfor recording temperature, hygrometry, pluviometry, or pressure threetimes a day, once a month, for 15 years (!). However, the archives of theRoyal Society of Medicine (119 boxes and 12 registers stored in theAcademy of Medicine) reflect on the part of the physicians, despite theirlittle training in data recording and management, a fierce determina-tion to achieve accuracy, as if they were shot through by absolute con-fidence in the idea of progress. Of the near 200 physicians who took partin the survey, around 50 performed their measurements for nearly10 years. From 1776 to 1792, the Society collected almost 8300 of the35 000 anticipated report cards. The comments and observations thatphysicians included with their data contained much information onmedical practice and the state of French society in the immediate pre-Revolutionary era.15-17
Although the great disparity in responses made it impossible to drawup the comprehensive epidemiological map of France that the surveysponsors had intended, the partial information collected threw accuratelight on the routes of contamination of certain infections. The reportsreceived by the Royal Society of Medicine inspired Vicq d’Azyr in 1790when he drafted his New plan for the constitution of medicine in France.Antoine de Fourcroy (1755-1809), physician, chemist, and Conventiondeputy, was to draw on this text when instigating the decree of 4 Fri-maire Year III (December 4, 1794) that reopened the faculties of medicinein Paris, Montpellier, and Strasbourg as Schools of Health.
By demanding meticulous attention to measurement and emphasiz-ing the importance of the results, the Royal Society of Medicine accel-erated the switch from a medicine of philosophical and nosologicalspeculation to one of enlightened scientific reasoning.15-17
Medicine held little interest for Louis XVI as a “science”—unsurpris-ingly, in that the healing art, in the late 18th century, was still deeplyenmeshed in abstruse philosophical considerations. As a profoundlyreligious person, the King was moved by the fate of the ill and infirm.The measures he took were dictated mainly by pragmatism, charity, andreligiously inspired commiseration. In 1778, Louis gifted 6000 livres to
Charles-Michel de l’Épée (Abbé de l’Épée) (1712-1789), the inventor of a more comprehensive signing lan-guage, to help found an institution to care for the young deaf-and-dumb. The same year, he made an iden-tical grant to Valentin Hauÿ (1745-1822) to found a school for the blind; years later, on December 26, 1786,26 blind youngsters who had learned to read and write were presented to the King at Versailles.
In 1780, the King commanded military hospitals to treat enemy wounded as “the King’s own subjects.”The same year, he ordered “light and well-ventilated infirmaries” to be constructed at his expense in thekingdom’s prisons.
In 1781, after an incognito visit to the Hôtel-Dieu Hospital in Paris, Louis was upset to see patientspiled three or four to a bed in unhealthy rooms. He decided to set up a system of individual beds and toseparate patients by type of infection. The same year, he approved the creation in Paris of a hospital forchildren with infectious disease, the Sick Children’s Hospital. It was in this public health spirit, in 1785,after the Hôtel-Dieu Hospital was destroyed by fire, that Louis XVI entrusted the surgeon Jacques RenéTenon (1724-1816) and seven other members of the Academy of Sciences with drafting a report on the re-construction of the Hôtel-Dieu. This report inspired Tenon’s celebrated 1788 Memoirs on the hospitalsof Paris itemizing the concrete measures to be applied for refitting Paris hospitals according to the new
A T O U C H O F F R A N C E
176 The sciences under Louis XVI. A king torn between enlightenment and revolution – RégnierMEDICOGRAPHIA, VOL 30, No. 2, 2008
Félix Vicq d’Azyr(1746-1794),
physician andanatomist, and the
last physicianof Queen Marie-
Antoinette, whomhe tried to protect.Founded the Royal
Society of Medicine,which did ground-
breaking work inepidemiology.
© BibliothèqueNationale, Paris,France/Lauros/Giraudon/The
Bridgeman ArtLibrary.
Colored engravingof the brain, by
Vicq d’Azyr, in hisTraité d’Anatomie
et de Physiology(1786). He described
the locus ceruleus,the locus niger, and
the band of Vicqd’Azyr. © Bridgeman
Art Library.

principles of hygiene: ventilated wards with high ceilings and a fixed number of patients, reorganizationof nursing duties, isolation of contagious patients, and special arrangements for obstetric deliveries, cater-ing, staff and patient clothing, baths, showers, and disinfection facilities.4,17,18
EpilogueMilitant hagiographies penned by die-hard monarchists aside, the royal couple suffers from an appallingimage in French historiography. Studies offering an objective and subtle analysis of the personalities of thetwo monarchs are relatively rare. Louis XVI is often described as a somewhat weak and insignificant kingwhose sole hobbies were hunting and the dismantling and repairing of locks. When hunting, he preferredthe company of his masters of hounds and stablemen to that of his guests. His master locksmith reportedthat he had to help the King hide from Court and Queen “to file and forge with me. (…) The King was good,shy, tolerant, and inquisitive.” Louis has also been depicted as improvident, indecisive, overburdened byresponsibilities, and under the dual influence of courtiers’ intrigues and Marie-Antoinette.4
During his lifetime, this image was bandied about (in amplified form) by the Court, the Paris circlesclose to the Viennese throne, and both his brothers, the Counts of Provence (the future Louis XVIII) andArtois (the future Charles X). The economic and institutional reforms proposed by his ministers (Turgot,Necker) threatened the privileges to which his 10 000 courtiers were so attached.2,3
Louis XVI was unrestrainedly caricatured. Shortsightedness compounded his tendency to absentmind-edness. He was sometimes unable to put a name to those he spoke to. His great height, chubbiness, and“noble features tinged by melancholy” increased the distance that he created with those who came intocontact with him. The King’s personality was complex. He often appeared retiring. Liking jokes, he gave
A T O U C H O F F R A N C E
177The sciences under Louis XVI. A king torn between enlightenment and revolution – Régnier MEDICOGRAPHIA, VOL 30, No. 2, 2008
Hand signs for the deaf “signes méthodiques,” created by Abbé de l’Épée,now known as “Old French Sign Language,” the precursor of all thesign languages used throughout the world today, such as the “AmericanSign Language (ASL). © Roger-Viollet.
Abbé (Father) Charles-Michel de l’Épée(1712-1789), trained as a Catholic priestbut denied ordination because he refusedto condemn Jansenism, dedicated himselfto the education of the deaf and foundedthe world’s first school for the deaf, whichexists to this day, in Paris. © BibliothèqueInter-Universitaire de Médecine (BIUM).
Frontispiecefrom the Mémoire surles Hôpitauxde Paris, byJacques RenéTenon (1788).© Coll. Inter-Activités.
Bernard Poyet’s plans for the reconstruction of the Hôtel-Dieuhospital, in Paris (1785). © Archives de l’AP-HP.

an impression of familiarity, but in fact detested it. In 1774, Lord Stormont, the English ambassador toParis, wrote: “As he is very reserved and indeed proud to be so, one guesses rather than knows what he isthinking.” His style was curt, terse, and plain. Often he did not answer those with whom he was speaking.“I prefer my silences to be interpreted rather than my words,” he told Malesherbes, who defended him athis trial in 1792. His memory was formidable, allowing him to correct and annotate memoranda and dis-patches from his ministers and advisers with considerable ease and accuracy.1,3,4 However, his faults are hardto conceal: the King was shy and awkward in public and did not look his interlocutors in the eye. He lackedself-confidence and resolve. “There were two men in him, the man who knew and the man who wanted,”wrote his biographer, Jean-Louis Soulavie (1751-1813), priest, geologist, and historian. “The qualities ofthe first were most varied and extensive. But in the great affairs of state, the King who wanted and com-manded was almost never to be found.” Louis’ excess of modesty and discretion probably aided the declinein the prestige and cult of the monarchy.4,19 The blurred image of Louis XVI is not helped by the meagerwritings he left behind him: a diary began as Dauphin in January 1766, and a diary continued as King,which ended on July 31, 1792 with the word “Nothing.” There is little if anything else. Both diaries weresimply hunting notebooks. They were not diaries in the proper sense, nor chronicles of a reign. Louis alsokept a book of the annuities and gifts he bestowed, and another for private expenditure. In the followingcenturies, the void was filled by a multitude of counterfeit manuscripts, circulated in attempts either torehabilitate the King or to flesh out the portrait of a weak and conspiratorial monarch.1,3,4 �
A T O U C H O F F R A N C E
178 The sciences under Louis XVI. A king torn between enlightenment and revolution – RégnierMEDICOGRAPHIA, VOL 30, No. 2, 2008
e problème politique majeur du règne de Louis XVI réside dans ce travail de sape incessant de lanoblesse et du haut clergé contre l’abolition de certains de leurs privilèges. La question écono-
mique occupe une place essentielle dans ce règne marquée par la très coûteuse guerre d’Indépen-dance américaine (1776-1783). Le roi trouve toujours dressé devant lui les forces les plus hos-tiles au changement; il ne sait pas s’appuyer sur la frange éclairée de la noblesse. Secret, timide
et modeste, Louis XVI veut mais n’ordonne pas. Le roi se plie difficilement au cérémonial de lacour privant indirectement la noblesse de son rôle social de représentation. Louis XVI présente le princi-pal défaut de ne pas savoir commander les hommes; sensible à la modernité des Lumières, il est constam-ment écartelé entre ses idées réformistes et son attachement profond à la tradition. Le roi demeure respec-tueux des lois fondamentales du royaume et refuse de les transgresser; il nomme pourtant des ministresréformateurs mais les congédie prématurément. Par goût et par nécessité, Louis XVI, dernier monarquefrançaise de droit divin au pouvoir absolu, se passionne pour les expériences, les recherches et les décou-vertes scientifiques. Il ne manque aucune occasion d’apporter son appui moral et financier à de nouveauxprojets susceptibles de faire progresser les connaissances humaines et d’améliorer le sort de la multitude.C’est ainsi qu’il favorise le développement de l’Académie des sciences, la création de la Société Royalede Médecine, les expérimentations de l’aérostat et de la machine à vapeur, l’expédition maritime de LaPérouse, l’application des règles d’hygiène aux hôpitaux, la fondation d’institutions pour aveugles et sourds-muets. Personnages incompris et souvent méprisés de l’histoire de France, Louis XVI et Marie-Antoinettebénéficient aujourd’hui d’une réécriture de leurs biographies dans le contexte politique qui précède laRévolution française.
LLES SCIENCES SOUS LOUIS XVI. UN ROI ENTRE LUMIÈRES ET RÉVOLUTION
REFERENCES1. Lever E. Louis XVI. Paris, France: Éditions Fayard; 1985.2. Taillemite É. Louis XVI ou le Navigateur Immobile. Paris,France: Payot; 2002.3. Félix J. Louis XVI et Marie-Antoinette: un Couple en Politique.Paris, France: Payot & Rivages; 2006.4. Petitfils JC. Louis XVI. Paris, France: Perrin; 2005.5. de Viguerie J. Louis XVI, le Roi Bienfaisant.Paris, France: Édi-tions du Rocher; 2003.6. Corcos M. Comment la grande encyclopédie mène à la révolu-tion de 1789. Médecine Pratique.1989;87:7.7. Moureau F. Le Roman Vrai de l’Encyclopédie. Paris, France:Gallimard; 1990.8. Capefigue M. Louis XVI. Paris, France: Belin-Leprieur; 1844.9. Muratori-Philip A. Parmentier,2nd ed. Paris, France: Plon; 2006.10. Reynaud MH. Les Frères Montgolfier et leurs Étonnantes Ma-chines. Paris, France: De Plein Vent; 1982.11. Payen J. Capital et Machine à Vapeur au 18e Siècle. Paris,France: Éditions de l’École des Hautes Études en Sciences So-ciales; 1969.12. Mologni J. Claude Dorothée de Jouffroy d’Abbans, le GénialMarquis. Besançon, France: Éditions du Sekoya; 2007.
13. Minguet H. Le Voyage au Tour du Monde de Lapérouse. Paris,France: Maspero; 1989.14. Gaziello C. L’Expédition Lapérouse, Réplique Française auxVoyages de Cook. Paris, France: Comité des Travaux Historiqueset Scientifiques; 1988.15. Meyer P, Triadou P. Leçons d’Histoire de la Pensée Médicale.Paris, France: Éditions Odile Jacob; 1996.16. Desaive JP, Goubert JP, Le Roy Ladurie E, Meyer J, Muller O,Peter JP. Médecins, Climat et Epidémies à la Fin du XVIIIe Siècle.Paris, France: Éditions de l’École Pratique des Hautes Études –Mouton; 1972.17. Goubert JP, Rey R, Bertrand J, Laclau A. Atlas de la Révolu-tion Française – Médecine et Santé, vol 7. Paris, France: Éditionsde l’École Pratique des Hautes Études en Sciences Sociales; 1993.18. Tenon J. Mémoires sur les Hôpitaux de Paris (facsimile of the1788 edition). Paris, France: Doin-Assistance Publique-Hôpitauxde Paris; 1998 [English translation: Tenon J. Memoirs on ParisHospitals, Weiner DB, ed. Canton, Ma : Science History Publica-tions; 1996].19. Soulavie JL. Mémoires Historiques et Politiques du Règne deLouis XVI. Paris, France: Treuttel & Würtz; 1801.

o reach the Petit Trianon, you need to leave the Château ofVersailles behind you, leave the straight lines of the formal gar-
dens, and bid farewell to the geometrical precision of the landscapesand vistas designed by Le Nôtre. Walk along the edge of the Orna-
mental Pools on the Terrace, go around the Latona Basin, make yourway between the Chestnut Grove and the Dauphin’s Grove, carry on
between the Colonnade Grove and the Dome Grove, head toward the GrandCanal, and turn off to the right. The Pavilion is straight ahead of you, at theend of the path. A masterpiece of neoclassical architecture, this modestly pro-portioned palace was built between 1763 and 1768 by Ange-Jacques Gabriel(1698-1782) at the request of Louis XV, who wanted to give it to Madame dePompadour, his favorite. But the marquise died too soon and never had thechance to enjoy her beautiful gift. The Comtesse du Barry, another of theKing’s mistresses, enjoyed it in her stead. With this stunning, square build-ing, embellished with Corinthian pillars on the court side and columns over-
looking the formal garden, the King’s architect, who also designed the buildings of the Place de la Concordeand the Ecole Militaire, as well as the “Grand Project” in Versailles, surpassed himself. The harmony is per-fect. The accommodation is delightful, the rooms on the bel étage perfectly proportioned and tastefullydecorated. The residence was designed, first and foremost, to be in harmony with nature. Surrounded bya veritable botanical laboratory entrusted from 1759 to the great naturalist Bernard Jussieu, who was com-missioned to classify the species so carefully nurtured and maintained by the domain’s gardeners, the
179Marie-Antoinette, Queen of France, Queen of Style – Spaak MEDICOGRAPHIA, VOL 30, No. 2, 2008
A T O U C H O F F R A N C E
wenty-five minutes at a slow walking pace. That’s all it takes to pass from one world into an-other, to leave behind the glitz of the Château of Versailles and step into the simplicity of the Petit
Trianon. It’s a journey that Queen Marie-Antoinette made a thousand times to escape the Court for-malities. Here, just minutes from the salons where the courtiers conducted their intrigues, the Aus-
trian princess born in Vienna on November 2, 1755 who became Queen of France on May 10, 1774 atthe age of 19 years, created a small paradise for herself, away from the stringencies of etiquette that
she found intolerable. Surrounded by the charm of the French Pavilion designed by Gabriel, the landscapedgarden, and the contrived simplicity of the cottages in the Queen’s Hamlet where she played the shep-herdess, Marie-Antoinette would say: “I am not the Queen, I am me.” The Petit Trianon was her personaldomain, a thoughtful gift from Louis XVI that released his capricious bride from the yoke of monarchy.Today, despite the ravages of time and the Revolution, the place still reflects the Queen’s personality, tastes,and aspirations. “To know someone, you must visit their home. The Trianon is Marie-Antoinette,” noteshistorian Evelyne Lever. Here, in her carefully restored domain, in the exquisite apartments or the gardenshe loved so much, visitors come close to this beautiful woman who was so passionate about the arts andthe pleasures of life, but whose life was changed from frivolity to martyrdom by history. Medicographia. 2008;30:179-185. (see French abstract on page 185)
T
Isabelle SPAAK, Journalist37 rue des Plantes745014 Paris, FRANCE(e-mail: [email protected])
Portrait ofMarie-Antoinette deHabsbourg-Lorraine(1755-1793). Frenchschool, 18th century.
Musée Antoine Lécuyer,Saint-Quentin, France.
© Bridgeman Art Library.
T
Marie-Antoinette Queen of France, Queen of Style
b y I . S p a a k , F r a n c e

building is a celebration of the plant world even in its internal decor. The paneling in the great dining roomis decorated with carvings of orange tree branches and bowls of fruit; and the drawing room walls aredecorated with the cipher of Louis XV intertwined with a crown of wild lilies. Garlands of flowers, birds, andrustic motifs are a recurring theme in the fabrics, paneling, furniture, and wall paintings.
Marie-Antoinette received this magnificent gift from her husband on August 15, 1774, just a few monthsafter his accession to the throne. “You love flowers, and I have a whole bouquet of them for you!” he saidgallantly as he handed her a key encrusted with 531 diamonds. The Queen could not have imagined amore beautiful tribute. She who so detested the Court now reigned over a kingdom modeled in her image,where she could live as she wished.
Freedom to bloomIt was a relief. The young Queen struggled with the rigors of etiquette. In Versailles, closely watched by herMistress of the Household, Madame de Noailles, life weighed heavily on her. The Queen found it difficultto accept “that she belonged not to herself but entirely to the kingdom of France,” explains Evelyne Lever.“Placed above mere mortals in a society organized along extreme hierarchical lines, her slightest gesturehad the significance of a public act.” She could not get used to it.
From what she wore to what she ate, from the moment she got up in the morning to the moment shewent to bed at night, her every gesture was scrutinized, and regulated down to the finest detail by im-mutable rules. The old nobility vied for her favors, and encroached upon her privacy. Her daily life tookplace under the eyes of a host of courtiers, ladies-in-waiting, valets, and footmen.
At the Trianon, she shut them out so that she could live as she wished and give free rein to her own de-sires and personality. She reclaimed her right to a private life and imposed her own style. Her kingdombelonged to her. Nothing and no one could enter this small, enchanted domain without her permission.
Even her husband was allowed in by her invitation only. As a rule, he came simply to dine. He was neverto sleep in the bedroom with the red silk drapes that Marie-Antoinette had set aside for him on the secondfloor. To the great horror of all the courtiers, rules were posted in the gardens. They were rules set “by orderof the Queen” and not “by order of the King.”
Marie-Antoinette withdrew, surrounding herself with a clique of young intriguers whom she liked tothink of as her friends. Nobody spied on her, nobody judged her. So at least she thought. But tongues werewagging. Her solitary retreats displeased the Court, and its members distanced themselves, injured by herneglect. The Queen didn’t care. Ignoring all the gossip, she continued to assert her freedom as a woman.She even went as far as endowing a boudoir with “movable mirrors,” where an elaborate system of slidingpanels enabled her to cover the windows. She restricted access to the sumptuous feasts she held in herhaven of peace, even though the Court was, by tradition, public. She shut herself away.
Far from all the conventions, but also far from her subjects. “Trianon is a world in miniature,” wroteAustrian novelist Stefan Zweig in his classic biography of his compatriot, published in 1933. “From herwindows—symbolically and literally—she could not see the town, or Paris, or the countryside, or anythingthat had any connection with real life. Her little patch of land could be crossed in a few moments, yet this
A T O U C H O F F R A N C E
180 Marie-Antoinette, Queen of France, Queen of Style – SpaakMEDICOGRAPHIA, VOL 30, No. 2, 2008
The Château de Versailles,with, in the foreground,
a fountain with an allegoricalfigure of a French river
holding a staff. © RobertHolmes/CORBIS.

tiny space was of enormous significance and meant more to Marie-Antoinette than all of France and itstwenty million inhabitants,” continued Zweig. Ah, the garden! Although, initially, the Queen did not alterthe decor of the French Pavilion designed by Gabriel for Madame du Barry, the same did not apply tothe parkland surrounding her new residence. She did not like the precision of Le Nôtre’s landscapes andvistas—his straight pathways and alleys, his contrived use of perspective, his trimmed boxwood, and ar-tificial groves. Marie-Antoinette dreamed of intricate, fairytale landscapes. The squares of rare plants soscrupulously collected since 1759 by the botanist, Charles Jussieu, by the order of Louis XV, were too se-vere. They had to go. The young woman was a romantic. She fell in love with the landscaped gardens of theEnglish, and adored a mass of rambling, untamed vegetation. She ordered her architect, Mique, to redesignthe gardens, drawing inspiration from the works of the Comte de Caraman (whose designs included theParc Monceau in Paris, which still exists today), and from the ancient ruins depicted in the paintings byHubert Robert, who was enamored of Italy.
“Hurried on by the Queen’s impatience, hundreds of workers began to implement the architects’ anddesigners’ plans, undertaking works that would, like magic, make the real world disappear, to be replacedby the most natural and picturesque landscape imaginable,” wrote Stefan Zweig.
The place was transformed. A gentle stream meandered through fields where the air was now scentedwith the rare fragrances of plants from North America, such as the tulip tree from Virginia, cypress fromLouisiana, massive oaks. Paths wound their way between overflowing flowerbeds. Broad clearings offeredviews of the follies built here and there according to the Queen’s fancy, ravishing buildings made for con-versation and amusement. There was, for example, The Temple of Love, built on a little island surroundedby reeds; a charming octagonal belvedere overlooking an ornamental lake; and a Chinese tilting ring, agame in which players try to mount multicolored wooden horses made to look like peacocks or dragons.
A T O U C H O F F R A N C E
181Marie-Antoinette, Queen of France, Queen of Style – Spaak MEDICOGRAPHIA, VOL 30, No. 2, 2008
The Petit Trianon,built for Louis XVbetween 1751 and1768, was given to
Marie-Antoinette byLouis XVI and became
her favorite retreat.© Adam Woolfit/
CORBIS.
The Queen’s playground: one of the cottages, built in 1783, in the “modelvillage” where Marie-Antoinette would dress up as a peasant. The villagetotaled 12 cottages and a watermill, and was situated near the Petit Trianon.© Guy Thouvenin/ Robert Harding World Imagery/CORBIS.
Harp belonging to Marie-Antoinette.Musée de la Ville de Paris, MuséeCarnavalet, Paris. © Bridgeman Art Library.

And finally, the Grotto. Designed for romantic encounters and intimate conversations, the Grotto wasMarie-Antoinette’s secret refuge. You approach it via a little hidden pathway that enables you to see beforebeing seen. This is where she was, some 15 years later on October 5, 1789, when she received the news thatthe people were marching on Versailles.
A refined worldMeanwhile, with all its charm and contrived delicacy, this little patch of land just a few kilometers squarebecame the Queen’s entire universe. Equipped even with its own theater, the “world in miniature” en-chanted her. “Trianon is for Marie-Antoinette a secret, blessed land dedicated entirely to chivalry and plea-sure,” noted Stefan Zweig ironically. For the whims of a frivolous girl barely 20 years old were not to every-one’s liking. The expenditure was profligate. To the extreme.
“I thought I had gone mad or was dreaming when I found that the large greenhouse (the most costlyand best designed in Europe) had been replaced by tall mountains, a large rock, waterfalls, and a stream.Never have two acres of land been so totally changed, nor cost so much money,” lamented the Duc de Croÿ
A T O U C H O F F R A N C E
182 Marie-Antoinette, Queen of France, Queen of Style – SpaakMEDICOGRAPHIA, VOL 30, No. 2, 2008
Marie-Antoinette knew nothing about painting. She judged artists’ talent simply by their ability to render herlikeness or at least a reflection of her own notion of her beauty. Several well-known artists tried their hand. Liotard,Jean-Baptiste Charpentier, François-Hubert Drouais, and Joseph Krantzinger, whose depiction of the young Queenas an amazon so shocked Empress Maria Teresa. “I’m fated to find no painter able to capture my likeness,” the youngQueen complained to her mother.
In 1778, Elisabeth Vigée-Lebrun, a fashionable young portrait artist, tried her luck. The initial meeting went well.“At the first sitting, I found the Queen’s imposing air prodigiously intimidating to begin with,” wrote the artist.“But Her Majesty spoke to me so kindly that her gentle good grace soon dispelled this feeling.” She forgot etiquetteto focus on the gracious features and perfect figure of her model. “The most striking thing about her face was theradiance of her complexion,” she said later. The two young women were the same age. They became friends. Dur-ing the long sittings, Elisabeth Vigée-Lebrun was to become the Queen’s confidante. They shared the same love ofsinging, and of freedom. It is to Madame Vigée-Lebrun that we owe a painting of the Queen wearing a simple muslindress and a straw hat decorated with feathers and bound by a ribbon. This was the kind of costume that the Queenloved to wear in her gardens at the Trianon. Exhibited in 1783, the canvas was found shocking in its simplicity.It had to be quickly replaced by an identical picture of the Queen with a rose in her hand, but this time wearing adress of blue-grey satin trimmed with an abundance of lace.
PORTRAITS OF A QUEEN
Portrait ofMarie-Antoinette
“À la Rose” byElisabeth Louise
Vigée-Le Brun, whowas to become the
confidante of the Queen. Oil on canvas,
113�87 cm,Château de Versailles.
© Photo RMN.
Marie-Antoinette and her Children, by Elisa-beth Louise Vigée-Le Brun, painted as anattempt to portray the Queen as an affec-tionate mother and so ingratiate her withpublic opinion. The empty cradle alludes tothe death of Sophie-Beatrix, who died whilethe painting was being executed. From leftto right, daughter Madame Royale, and twosons, Louis-Joseph and the future Louis XVII.Oil on canvas, 275�215 cm, Château deVersailles. © Bridgeman Art Library.

when he discovered the extent of the works ordered by Marie-Antoinette. A style icon, obsessed by herclothes and appearance, infatuated with hairstyles, jewelry, finery, and especially herself, the Queen nextlaunched herself with equal enthusiasm into redesigning the interior of her home. It was the ideal activi-ty to stave off boredom and give meaning to her life, and she devoted herself to it wholeheartedly. Beforetackling the refurbishment of her cherished Trianon, she began with a makeover of her apartments in theChâteau de Versailles. She fitted doors and windows with locks bearing her cipher, ordered new furniture,
A T O U C H O F F R A N C E
183Marie-Antoinette, Queen of France, Queen of Style – Spaak MEDICOGRAPHIA, VOL 30, No. 2, 2008
The Salon des Nobles at Versailles,redecorated in 1785by Marie-Antoinette. © Bridgeman ArtLibrary.
From feather-brained macaroon addict to a woman with a passion for pleasure and consumption,from “the Austrian woman” to the victim of the liturgy of Versailles, the public image of Marie-An-toinette is many-faceted and has constantly changed over the centuries.
The author of several biographies of the Queen, including “Marie-Antoinette, the last Queen ofFrance” (Framan, Strauss & Giroux, 2000), which inspired film director Sofia Coppola, French his-torian Evelyne Lever takes stock of these shifts in public opinion.
Marie-Antoinette has always fascinated people. But perceptions of her have changed. In the 19th century, she wasseen as a martyred queen whose cult was maintained by the nobility. They were not looking at her life; she wasmerely being held up as a symbol of a murderous Republic. This version was cultivated in every aristocratic fam-ily. At the same time, in Republican circles following the Second Empire, Marie-Antoinette was seen as a bad queenwho sucked the people’s blood. The two currents of thought co-existed during the same period. They merely var-ied from one circle to another. In 1858, the Goncourt brothers published the first real biography of the Queen in
this expiatory spirit. It was not until the end of the First World War thatthe historian and curator of Versailles, Pierre de Nolhac, did some properresearch. He drew on several works by scholars who had begun to classifyMarie-Antoinette’s letters. He succeeded in providing a coherent pictureof the Queen, demonstrating that she was not simply a saint. Certainly shewas a victim of the Republicans, but he stressed her political role, her sen-sitivity, and her growth into maturity.
It was the Austrian novelist Stefan Zweig, influenced by psychoanalysis,who wrote the finest biography in the 1930s. In the Viennese archives, hehad discovered some letters that had been censored but cast a fascinatinglight on her sexual life, and on the problems she had had with Louis XVIbefore she succeeded in providing an heir to the throne of France. Accord-
ing to Zweig, Marie-Antoinette was a princess of unexceptional intelligence whose tragic destiny transformed herinto an exceptional person. In his view, the Queen played a genuine political role from 1787 onwards.
In the 1950s, the French public fell in love with this woman who arrived in a carriage and was taken to thescaffold in a cart. Today, Sofia Coppola’s film has turned Marie-Antoinette into a fashion icon. The exaggeratedfrivolity and whirlwind of pleasure fascinates young people, who now appear to confuse the Queen’s fate withthat of Lady Diana. Insufficiently loved in life, she is now never more adored than in death.
MONSTER OR MARTYR? FROM THE REVOLUTION TO SOFIA COPPOLA
Kirsten Dunst starringas Marie-Antoinette,
in the film written anddirected by Sofia Coppolaand released by ColumbiaPictures in 2006. © SonyPictures Entertainment/
Columbia Pictures/SIPA Press.

and selected the finest silks. In 1781, she transformed her library and refurbished the former cabinet ofQueen Marie Leszcynska. Overlooking a dark and gloomy courtyard, the somber room became a charmingboudoir lit up by the careful use of mirrors and pale-colored paneling. Known as “La Meridienne,” it is amodel of elegance. Visitors can still admire the pretty little sofa tucked into its corner, the mirrors framedwith stems of roses and bronze foliage accompanied by the eagle of the Hapsburgs and the attributes ofLove. Of course, Marie-Antoinette often changed her mind. She hesitated, reconsidered, started again, spent
fortunes, gave orders, and counter-orders. But the result was delightful.In 1783, some 230 craftsmen were employed in transforming the innerGrand Cabinet (the Gold Room) at Versailles. In the Chamber of Cere-monies, Marie-Antoinette had the walls and chairs covered with sump-tuous white satin brocaded with arabesques and embroidered with wildflowers. It was not to last. Four years later, she tired of it. The whole roomwas empanelled in white and gold.
Entranced by novelty, she bought lots of expensive trinkets. Chineselacquers and porcelains, boxes, fans, seashells with gilt bronze mounts,jaspers, crystals, and fossilized wood littered every available surface. Andevery item of furniture bore a famous name. Jean-Henri Riesener washer cabinetmaker, supplying magnificent roll-top writing desks, tablesof every shape and kind, and all sorts of corner pieces embellished withbronzes by Gouthière. Sofas, armchairs, and love seats bore the signa-tures of Georges Jacob, Foliot, and Boulard. The silks came from theworkshops of Jean Charton. Faithful to her suppliers, Marie-Antoinettewas midwife to a new style. Combining the elegant and the rococo, itwas inspired by the classical world but adapted to offer the comfort andfeminine grace of which she prided herself on being the finest exam-ple. Obsessed with her image, she reigned over the decorative arts withthe same blend of sophistication and simplicity that she liked to express
in her clothes. She imposed her tastes. “She doesn’t really deserve the credit,” Evelyne Lever reminded us.“As Queen, she had only to choose among the items presented to her by the most talented craftsmen of theperiod. She never actually influenced them.” That may well be so. But she was their patron. She introducednew blood, swept away the cobwebs, did away with the heaviness of the rocaille style. She let in a breath offresh, more lighthearted air. She loved simple lines, wall hangings, and foliage. She had bouquets embroi-dered on curtains, chairs, and bedspreads. Lightness, sophistication, and delicacy became her trademark.
In 1786 at Versailles, she had the Salon des Jeux stripped of its marble decor. She wanted to give therooms “a light, clean feeling,” and banish the “mean and heavy feel of the bronze and lead” ornamentscommissioned by Louis XV. She didn’t like Lebrun’s ceiling. So she had it painted over in sky blue.
At the Petit Trianon, she made few changes to the original decor. She contented herself with affirminga style, introducing daylight and delicacy. She had a preference for rustic designs, which she used andabused, both for her numerous sets of porcelain tableware with their background of gold, and for her fa-mous “wheat-ear” furniture, whose polychromatic shapes are laden with lily of the valley, jasmine, and fircones, while the chairs were covered with pale silk embroidered with bouquets and garlands of flowers.
A T O U C H O F F R A N C E
184 Marie-Antoinette, Queen of France, Queen of Style – SpaakMEDICOGRAPHIA, VOL 30, No. 2, 2008
Copy of the famous diamond necklace that was at thecenter of an intrigue to discredit Marie-Antoinette,with rumors of lovers’ trysts and embezzlement,and which led to the banishment of a Cardinal andlingering suspicion against the Queen. © PhotoRMN/ All rights reserved.
MARIE-ANTOINETTEExhibition at the Galeries Nationales du Grand Palais,
March 15 through June 16, 2008
Bringing together more than 300 works from all over Europe,including an extraordinary collection of paintings (Vigée LeBrun), sculptures (Lemoyne, Boizot, and Lecomte), and deco-rative arts (Carlin, Riesener, Weisweiler), the exhibition seeksto convey the various aspects of Marie-Antoinette’s personali-ty, in terms of her education and upbringing and as regards thearts and politics. It invites the public to walk in this exception-al woman’s footsteps, from her birth in 1755 at the AustrianCourt to her last days at the Conciergerie, and her death on Oc-tober 16, 1793. Not since 1955 will she have received such daz-zling homage.
MARIE-ANTOINETTE’S ESTATEAT VERSAILLES
The creation of “Marie-Antoinette’s Estate”is part of the “Grand Versailles.” It includesaccess to the Petit Trianon, Chapel, FrenchPavilion, Queen’s Theatre, Belvedere, Templeof Love, Grotto, Landscaped Garden, Refresh-ments Dairy, Queen’s Hamlet, and Farm.
The Estate and Petit Trianon are open daily,except on some French public holidays andduring official ceremonies. April 3 throughOctober 31: noon to 7.30 PM.
Information: 01.30.83.78.00
www.chateauversailles.fr

There was nothing pompous or particularly sumptuous in her choices, rather “a perfect harmony, frombed to powder case, from harpsichord to ivory fan, from chaise longue to miniature, using only the finestmaterials in the most discreet forms, fragile in appearance yet long-lasting.” Incorrectly called Louis XVI,this style owes much to the Queen, since it is wholly associated with her light and elegant silhouette.
Too frivolous a gameIn her Petit Trianon domain, known as the “little Schœnbrunn” in acknowledgement of her Austrian ori-gins, she wore charming muslin dresses and straw hats, favoring modesty. “Compared with the luxury ofVersailles, the Petit Trianon seemed simplicity itself,” comments historian Jean-Christian Petitfils. “A bed-chamber full of muslin and silk embroideries, a boudoir, several cabinets and garde-robes, an elegant li-brary, a bathroom with a white marble bath. And throughout, a symphony of soft pastel tones of green,lilac, blue, white, and gold.”
Her cardboard cutout haven became an obsession. Very soon, Gabriel’s French Pavilion, the garden, andits novelties were no longer enough for her. To “make the fantasy even more real,” joked Stefan Zweig,she commissioned her architect, Mique, to build eleven cottages and a tower to satisfy her need for rus-ticity. Thatched roofs, fake lizards on the walls, pigs, sheep, and peasants were all included in this puppetshow in which the Queen entertained herself by playing the farmer. This final caprice cost her her throne.Wrapped up in her escapist dreams, she failed to face reality. The more she amused herself, the worse thepolitical situation became. In 1785, the Low Countries revolted, putting the Franco-Austrian allianceseverely to the test. Poverty knocked on the doors of her domain. She was deaf and blind to it all. After herdifficulties in giving the realm an heir, her unbridled behavior and romantic escapades, whether real orimaginary, offended both Court and people. That same year, the “Diamond Necklace Affair,” a ludicrousconspiracy against her, marked the beginning of her fall from grace. Her private paradise could do nothingto save her. Lies proliferated. The people’s hatred multiplied tenfold. The nobility distanced itself. Despitethe courage she was to show on October 6, 1789 before the market women who came to seek her and herfamily at the Château de Versailles, despite her years of imprisonment, her separation from her children,her isolation, and the dignity of her last momentsbefore the scaffold, nothing could make people for-get the heedlessness of her youth. She was to paywith her life, the symbol of her frivolity. �
A T O U C H O F F R A N C E
185Marie-Antoinette, Queen of France, Queen of Style – Spaak MEDICOGRAPHIA, VOL 30, No. 2, 2008
ingt-cinq minutes en marchant à petits pas. Il n’en faut pas plus pour passer d’un mondeà un autre, pour quitter les dorures du château de Versailles et rallier la simplicité du petit
Trianon. Un trajet que la Reine Marie-Antoinette a fait maintes fois pour échapper à la rigiditéde la Cour. Ici, à quelques minutes des salons où se disputaient les courtisans, la petite princesse
autrichienne née à Vienne le 2 novembre 1755 et devenue Reine de France, le 10 mai 1774 à 19 ans,s’était aménagé un petit paradis intime loin des lourdeurs de l’étiquette qu’elle ne supportait pas.
Entre le charme du pavillon Gabriel, les jardins à l’anglaise et la simplicité factice des chaumières duHameau où elle se plaisait à jouer à la bergère, Marie-Antoinette aimait répéter « Je ne suis pas la reine,je suis moi ». Le petit Trianon, c’est son domaine. Louis XVI le lui avait offert en juin 1774, au début deson règne. L’attention était délicate. Le cadre était idéal pour permettre à sa jeune épouse capricieusede se libérer du joug sacré de la monarchie. Aujourd’hui, malgré les assauts du temps et ceux de la révo-lution, ce domaine reste emprunt de la personnalité de la reine. Il reflète ses goûts, témoigne de ses aspi-rations. « Pour connaître quelqu’un, il faut visiter sa maison. Trianon, c’est la reine », rappelle l’historienneEvelyne Lever, spécialiste de Marie-Antoinette. Ici, dans son domaine réhabilité minutieusement, dansl’atmosphère exquise de ses appartements ou dans ce jardin qu’elle chérissait, le visiteur fait véritable-ment connaissance avec cette jolie femme férue d’art et de plaisirs dont l’histoire bascula de la frivolitéau martyr.
MARIE-ANTOINETTE, REINE DE FRANCE, REINE DU STYLE
V
Queen Marie-Antoinette’s poignant last note hastilywritten shortly before her execution. “This 16th of Oc-
tober at 41/2 in the morning. My God! Have mercy uponme! My eyes have no tears left to cry over you, over my
poor children! Farewell, farewell! Marie-Antoinette.”Châlons-sur-Marne Library. © Roger-Viollet.

General instructions�Manuscripts should be provided by e-mail ([email protected]) or by CD double-spaced, with 2.5-cm margins. Pages mustbe numbered. Standard typed page = 25 lines of 90 characters(including spaces) double-spaced, 2.5-cm margins = a total ofabout 320 words per page.� All texts should be submitted in English.� Provide 1 color photograph of main author.� On the title page, provide: a title (concise and informative); fullnames of authors (first name, middle name initial, and last name);highest academic degrees (in country-of-origin language); affilia-tions (names of department[s] and institution[s] at the time the workwas done); a short running title (no more than 50 letters and spaces),keywords (5-10); corresponding author’s complete mailing addressand telephone No., fax No., and e-mail address; acknowledgments(on title page, or at end of main text).� Include an Abstract of 200-230 words for all texts except Edito-rials and replies to the Controversial Question.� Figures and Tables. Figures should be of good quality or profes-sionally prepared, numbered according to their order, with properorientation indicated (eg, "top," or "left"). Figures may be providedas pdf files (printing resolution = 300 dpi scans, on CDrom, or viae-mail; screen resolution = 72 dpi scans acceptable only if large-sized format [A4]). Provide fully explicit legends, not repetitive oftext. All abbreviations used should be explained in the legends. Asfigures and graphs may need to be reduced or enlarged, all absolutevalues and statistics should be provided. Illustrations will be repro-duced in full color only when clearly necessary, eg, images from nu-clear medicine or histology. Provide each table on a separate sheet,with title above and description below. All figures and tables shouldbe cited in the text, with distinct numbering for figures and tables.� Note that Editorials and Abstracts will be published in Englishand French. Translations into French will be provided by the Pub-lisher’s Editorial Department.� Include Headings using a consistent style for the various levelsof headings, to highlight key points and facilitate comprehension ofthe text. The Editorial Department reserves the right to add or deleteheadings when necessary.� Abbreviations should be used sparingly and expanded at firstmention. A list of selected abbreviations and acronyms should beprovided (or will be prepared by the Editorial Department) wherenecessary.� Use Système International (SI) units.� Use generic names of drugs.� All references should be cited in the text and numbered con-secutively using superscript arabic numerals. Presentation of thereferences should be based on the Uniform Requirements for Man-uscripts Submitted to Biomedical Journals. Ann Intern Med. 1997;126:36-47 (“Vancouver style”). The author-date system of citationis NOT acceptable. In press references are to be avoided. In thebibliography, titles of journals should be abbreviated according tothe Index Medicus. All authors should be listed up to six; if thereare more, only the first three should be listed, followed by “et al.”
Where necessary, references will be styled by the Editorial Depart-ment to Medicographia copyediting requirements. Authors beartotal responsibility for the accuracy and completeness of all refer-ences and for correct text citation. Example of style for references:1. Ouriel K, Geary K, Green RM, Geary JE, DeWeese JA. Factorsdetermining survival after ruptured abdominal aneurysm. J Vasc Surg.1990;11:493-496.2. Darling RC, Brewster DC, Ottinger LW. Autopsy study of unop-erated abdominal aortic aneurysms: the case for early resection.Circulation. 1977;56(suppl II):II161-II164.3. Schulman JL. Immunology of influenza. In: Kilbourne ED, AlfadeRT, eds. The Influenza Viruses and Influenza.Orlando, Fla: AcademicPress Inc; 1975:373-393.
Specific formats�Editorial: 1500 words.No abstract or illustrations should be includ-ed. A French translation of the Editorial will be provided by the Ed-itorial Department and submitted to the author.� Theme - Focus - Update - Therapeutic outlook article - Touchof France: Abstract: 200-230 words.Main text: 2800-3200 words.References: their number should not exceed 50. Illustrations (fig-ures and tables): their number should not exceed 5 unless clearlynecessary.� Interview: Abstract: 200-230 words. Main text: 2000-2500 words.Headings are the questions posed at the interview. References, ifcited, should in no case exceed 10. No illustrations.� Replies to the Controversial Question: 400-600 words. No ab-stract or illustrations should be included. References, if cited, shouldin no case exceed 6.
Editorial processing� Editorial style: All contributions to Medicographia will be styledby the Editorial Department according to the specifications of the cur-rent edition of the American Medical Association Manual of Style,Williams & Wilkins.� Page proofs and editorial queries will be sent to the correspond-ing author for approval. Corrections should be returned within 48hours by e-mail, and fax or express mail. If this deadline is not met,changes made by the Editorial Department will be assumed to beaccepted by the author. Authors are responsible for all statementsmade in their work, including changes made by the Editorial Depart-ment and authorized by the author. Articles and abstracts will be ed-ited to required length or returned to the author if specific requirementsare not complied with.
Copyright� Copyright of articles will be transferred to the Publisher of Medico-graphia. The Copyright Transfer Agreement must be signed by themain author and all coauthors and returned to the Publisher.� For reproduction of copyrighted work, it is the author’s respon-sibility to obtain authorizations from the author(s) (including self) andthe publisher(s) and provide copies of these authorizations with themanuscript.
I nst ruct ions for authors
A S e r v i e r p u b l i c a t i o n
Medicographia