Embed Size (px)
Citation preview

Mechanisms affecting neuroendocrine and epigeneticregulation of body weight and onset of puberty: Potentialimplications in the child born small for gestational age (SGA)
Christian L. Roth & Sheela Sathyanarayana
Published online: 14 March 2012# Springer Science+Business Media, LLC 2012
Abstract Signaling peptides produced in peripheral tissuessuch as gut, adipose tissue, and pancreas communicate withbrain centers, such as hypothalamus and hindbrain to manageenergy homeostasis. These regulatory mechanisms of energyintake and storage have evolved during long periods of hungerin the evolution of man to protect the species from extinction. Itis now clear that these circuitries are influenced by prenatal andpostnatal environmental factors including endocrine disruptivechemicals. Hypothalamic appetite regulatory systems developand mature in utero and early infancy, and involve signalingpathways that are important also for the regulation of pubertyonset. Recent studies in humans and animals have shown thatmetabolic pathways involved in regulation of growth, bodyweight gain and sexual maturation are largely affected byepigenetic programming that can impact both current and futuregenerations. In particular, intrauterine and early infantile devel-opmental phases of high plasticity are susceptible to factors thataffect metabolic programming that therefore, affect metabolicfunction throughout life. In children born small for gestationalage, poor nutritional conditions during gestation can modify
metabolic systems to adapt to expectations of chronic undernu-trition. These children are potentially poorly equipped to copewith energy-dense diets and are possibly programmed to storeas much energy as possible, leading to later obesity, metabolicsyndrome, disturbed regulation of normal puberty and earlyonset of cardiovascular disease. Most cases of disturbed energybalance are likely a result of a combination of genetics, epige-netics and environment. This review will discuss potentialmechanisms linking intrauterine growth retardation withchanges in growth, energy homeostasis and sexual maturation.
Keywords Intrauterine growth retardation . Hypothalamus .
Energy homeostasis . Epigenetics . Endocrine disruptingchemicals
1 Introduction
Children born small for gestational age (SGA) are at risk for ahost of endocrine abnormalities including decreased growthhormone (GH) responsiveness, premature or exaggeratedadrenarche, early and rapidly progressive puberty (higherfollicle stimulating hormone (FSH), lower inhibin B, but alsohigher luteinizing hormone (LH)) as well as short stature[1–4]. Girls also are at risk for polycystic ovarian diseaseand early menarche (5–12 months earlier), and boys a higherrate of undescended testicles [4, 5]. Furthermore, childrenborn SGA are more likely to develop central adiposity, insulinand leptin resistance, metabolic syndrome, dyslipidemia, dia-betes, and cardiovascular disease later in life than childrenborn of a normal weight [6–9].
This review will summarize important findings includingmechanisms and environmental factors that can cause alteredgrowth, weight gain and pubertal onset in particular in childrenborn SGA. The first part will summarize how hormonal
C. L. Roth (*)Division of Endocrinology,Seattle Children’s Hospital Research Institute,1900 Ninth Avenue,Seattle, WA 98101, USAe-mail: [email protected]
C. L. Roth : S. SathyanarayanaDepartment of Pediatrics, University of Washington,Seattle, WA, USAe-mail: [email protected]
S. SathyanarayanaGeneral Pediatrics, University of Washington/Seattle Children’sResearch Institute, Seattle Children’s Hospital Research Institute,1900 Ninth Avenue,Seattle, WA 98101, USA
Rev Endocr Metab Disord (2012) 13:129–140DOI 10.1007/s11154-012-9212-x

regulatory pathways can be affected by intrauterine growthretardation (IUGR) and the second part will focus on mecha-nisms involved in the adverse effects of exposure to endocrinedisrupting chemical (EDCs) in early life. Given that metabolicprogramming is likely explained by nutritional and environ-mental factors, the common thread that may tie them together isepigenetic programming which will be explored in this review.
2 Endocrine regulation
2.1 Endocrine mechanisms of body weight regulationand growth—implications in the child born SGA
2.1.1 Central mechanisms regulating food intakeand energy homeostasis
The hypothalamus is central to regulation of energy homeosta-sis. Hypothalamic nuclei are the target of nutrients such as freefatty acids, glucose, and amino acids, circulating peptides,including leptin, insulin, as well as gut hormones such aspeptide YY (PYY) and ghrelin [10–13]. Changes in the circu-lating level of these metabolic signals can trigger potentresponses affecting both food intake (FI) and energy expendi-ture (EE). It is well established that insulin and leptin in partic-ular play critical roles in FI and EE in that levels of both areproportionate to body fat and that they interact with theirrespective receptors expressed in the arcuate nucleus (ARC), akey hypothalamic brain area which transmits peripheral weight-regulating signals to other areas of the brain [10]. Many neuronsare regulated by insulin and leptin, and central administration ofeither hormone reduces FI and body weight. However, the mainneuronal phenotypes in the hypothalamic regulation of energyintake and EE appear to be proopiomelanocortin (POMC) andneuropeptide Y/agouti-related peptide (NPY/AgRP) producingneurons, which are concentrated in the ARC. Additionally,alpha-melanocyte stimulating hormone (α-MSH), a posttrans-lational product of the prohormone POMC, is also a keyweight-regulating neuropeptide [10, 14–16].
Other brain regions known to play a role in energy homeo-stasis include the ventromedial nucleus (VMN), which con-tains gamma-amino butyric acid- (GABA)ergic andanorexigenic brain-derived neurotrophic factor (BDNF) neu-rons and is important for insulin dependent neurotransmissionand regulation of the autonomic nervous system outflow fromthe brain. The paraventricular nucleus (PVN) contains a varietyof appetite suppressing peptides, such as corticotrophin-releasing factor (CRF) and thyrotropin-releasing hormone(TRH) and thereby regulates peripheral endocrine secretion[12, 17]. There is a close interaction between BDNF and leptin,thus, BDNF plays an important role in appetite regulation [18].Two classes of PVN neurons responsive to melanocortins andNPY have been identified- the tonically firing neurosecretory
(NS) cells, and the burst-firing preautonomic (PA) cells. Inrodents, changes in the sensitivity of energy balance-relatedinhibitory inputs to these cells alter their firing properties withage [19]. NPYergic regulation dominates in neonates, therebylikely promoting the positive energy balance necessary forgrowth, while later in development NPY inputs decrease asmelanocortin inputs increase. These changes indicate a “devel-opmental switch” in the regulation of energy balance [19].
2.1.2 Consequences of IUGR on body compositionand metabolic programming
It is well established that IUGR and small birth weight andsize are associated with increased rates of, obesity, coronaryheart disease and stroke in adult life [20]. IUGR induced bylack of adequate nutrition, is also associated with increasedrisk for developing reduced beta cell mass and type 2 diabetes.Beta cell mass reduction can either be present at birth ordevelop later during adolescence. The largest expansion ofthe beta cell mass has been shown to take place in the secondhalf of prenatal development [21]. Compromises to this ex-pansion results in a smaller beta cell mass at birth, which maylead to deficient insulin secretion later in life [22, 23]. Chil-dren can compensate for their small birth weight by catch-upgrowth if, after birth, they are exposed to improved nutrition,however rapid childhood growth aggravates the risk of thedescribed diseases [20]. Furthermore, higher caloric intake byformula compared to breastfeeding in infants has been shownto be associated with a greater risk of obesity in later life [24].
In an animal model of food-restriction, energy depleted ratswere pair-fed to normal-weight controls which resulted in thesame rate of protein deposition but a two-fold higher fataccretion, potentially caused by sustained suppression of ther-mogenesis and EE [25]. Additionally, IUGR in sheep, wasassociated with lower peroxisome proliferator activated recep-tor γ (PPARγ) and leptin expression in perirenal visceral fat inmale but not female lambs at the age of 21 days. It wassuggested that this leads to a decrease in hepatic insulinsensitivity, particularly during periods of high caloric intakewhich might predispose male IUGR lambs to the subsequentdevelopment of an insulin resistant phenotype [26]. Thethrifty metabolism that leads to a ‘catch-up’ in weight gain,but disproportionate fat accumulation is characterized by lep-tin and skeletal muscle insulin resistance as well as adiposetissue insulin hyper-responsiveness. These alterations in leptinand insulin metabolism allow for both blood glucose homeo-stasis and the rapid replenishment of fat stores; but bear therisk of consequences such as obesity and cardiovascular dis-ease, in particular in the context of aWesternized lifestyle withlow physical activity and high intake of energy-dense dietsrich in fat and refined carbohydrates [25].
In addition to SGA, increased birth weight, maternalstarvation as well as maternal obesity and diabetes mellitus
130 Rev Endocr Metab Disord (2012) 13:129–140

have been identified as risk factors for long-term metabolicconsequences and obesity in children [27–29]. In a U.S.cohort study of over 14,881 adolescents, a 1 kg incrementin birth weight over average in full-term babies was associ-ated with an approximately 40% increase in the risk of beingoverweight at ages 9 to 14 years [29]. Ibanez et al. showeddisproportional rapid expansion of fat mass in comparisonto lean body mass in children born SGA vs. appropriate forgestational age (AGA) [30]. Furthermore, paternal and ma-ternal adiposity are correlated with a higher birth weight ofthe offspring, with a much stronger association for themother compared with the father, suggesting that besidesgenetic factors the intrauterine environment plays an impor-tant role in the later development of obesity [31]. In a studyof female monozygotic twins, higher birth weight was pos-itively correlated with adult BMI. Within twin pairs, thetwin who was heavier at birth was taller and slightly heavierin adult life, which was more marked if the birth weightdifference between the twins exceeded 15% [32].
In perinatal life, exposure to a disturbed metabolic envi-ronment holds consequences to the programming ofoffspring’s energy regulatory circuits. Exogenous inductionof hyperleptinemia during the first 10 d of life in rats led toleptin resistance at adult age and was associated with a de-creased expression of the hypothalamic leptin receptor and anincreased expression of SOCS-3, a regulator of leptin signal-ing that mediates leptin resistance [33]. Streptozotocin-induced insulin-deficient diabetes during pregnancy producedoffspring that displayed hyperphagia and overweight duringlater life. These offspring showed alterations of hypothalamicneurons expressing orexigenic neuropeptides such as NPY inthe ARC [34]. Prenatal undernutrition also has long-termmetabolic consequences as it results in increased body fatdeposition as well as enhanced plasma leptin and triglycerideconcentrations [35]. Furthermore, IUGR exposure results instunted birth weight, increased fat mass early in life, hyper-phagia, increased hypothalamic NPY levels and reduced hy-pothalamic expression of signal transducer and activator oftranscription 3 (STAT3), a downstream effector of POMCsignaling [36–38].
Adaptation enabling the fetus to survive in a limitedenergy environment might also involve reprogramming ofmitochondrial function as energy expenditure is decreasedand IUGR animals exhibit marked insulin resistance early inlife. Decreased oxidation rates of pyruvate, glutamate, suc-cinate, and alpha-ketoglutarate have been found in mito-chondria isolated from the liver in IUGR pups before theonset of diabetes [39]. In contrast, nutrient excess also bearsthe risk for changed energy homeostatic set points leading toinappropriate perception of starvation. Increased nutrientexposure can lead to cellular inflammation in the hypothal-amus activating nuclear factor κB (NF κB) signaling, andlead to central insulin and leptin resistance, and disturbed
satiety resulting in obesity [40, 41]. Mice exposed to earlypostnatal overnutrition exhibited leptin and insulin resis-tance as well as increased propensity to development ofobesity after exposure to high-fat diet [42]. These mechanismsmight explain the increased risk for developing obesity inchildren born SGA. Once obesity is achieved the weightregulatory pathways become even more altered which furtherperpetuates excessive caloric intake and weight gain. Wefound that in overweight children, disturbed physiology ofappetite-regulating peripheral hormones can be found evenbefore changes in blood glucose levels occur, including anexaggerated rise of insulin, a blunted rise of satiety hormonePYY and a blunted decrease of hunger hormone ghrelin afteran oral glucose load in obese vs. lean children [43].
Human growth is regulated by insulin, GH, insulin-likegrowth factor (IGF)-I and, particularly during fetal life, IGF-II. We studied twin babies with twin-to-twin-transfusionsyndrome and found that fetal IGF-1, IGF-binding protein-2 (IGFBP2), IGF-II, adiponectin, leptin and ghrelin(assessed in umbilical cord blood at time of birth) wereassociated with birth weight and postnatal growth in mono-zygotic twins with discordant growth. In our studies, weidentified IGF-I as a good indicator for fetal growth. Birthweight correlated positively with IGF-I but negatively withIGFBP2. Although we found a strong correlation betweenIGF-II of donor and recipient, there was no significant corre-lation between birth weight and IGF-II serum levels overall[44]. Birth weight was a strong predictor of growth in the firstyear of life. We investigated peptides that play an importantrole in energy homeostasis at birth and after one year. Adipo-nectin levels were reduced in SGA, ghrelin had a strongprognostic value for postnatal catch-up growth (r00.97; p00.0035), and gain in head circumference was significantlycorrelated to gain in IGF-I (r00.46; p<0.01) as well as to gainin leptin (r00.47; p<0.01), a hormone that plays a critical rolein neuronal development and intrahypothalamic connectionsand maturation [44–47].
2.2 Endocrine mechanisms of the regulation of onsetof puberty
In primates, including humans, gonadotropin secretion is ele-vated during neonatal development and early infancy, presum-ably as a consequence of enhanced pulsatile release ofgonadotropin releasing hormone (GnRH). This phase of in-creased activity is followed by a rather protracted pause duringchildhood, which ends with the reactivation of the pulse gen-erator—first during the sleep hours, and then during the day—at the beginning of the second decade of postnatal life. Such achange in pulsatile gonadotropin secretion is necessary fornormal gonadal development and function, and is determinedby an increased pulsatile GnRH release from the hypothalamus[48–55]. In turn, GnRH secretion is regulated by both
Rev Endocr Metab Disord (2012) 13:129–140 131

transsynaptic and glial inputs. The search for the neuronalnetworks most critically involved in controlling GnRH releaseduring sexual development has been narrowed down to thosesystems utilizing excitatory/inhibitory amino acids, and therecently identified neuropeptide metastin/kisspeptin [56, 57],for neurotransmission (see model Fig. 1). Examples include,GABAergic and glutamatergic neurons, neurons responsive toleptin, NPY-producing neurons and prostaglandins [58, 59].GABAergic neurons acting via GABAA receptors provide themost important inhibitory transsynaptic influence controllingGnRH secretion during prepubertal development. This inhib-itory mechanism, most elegantly demonstrated in rhesusmonkeys [60], appears to play a major role in restraining theinitiation of primate puberty, as evidenced by the dramaticadvancement of female sexual development induced by theintrahypothalamic blockade of GABAA receptors [60, 61]. Asin the case of glutamate, GABAmodulates GnRH secretion byacting directly on GnRH neurons and on neurons synapticallyconnected to the GnRH neuronal network. Opiatergic neuronalsystems (such as that formed by enkephalin-containing neu-rons) also appear to contribute to the inhibitory control ofpuberty [62, 63].
Appetite inhibiting hormone leptin stimulates GnRH se-cretion, whereas orexigenic neuropeptide NPY inhibits the
onset of puberty [64]. Insulin-like growth factor I (IGF-I) isproduced by both glial cells and peripheral tissues, and hasbeen shown to directly regulate GnRH physiology (seemodel Fig. 1). Intraventricularly administered IGF-I effec-tively induced LH release in both juvenile and peripubertalfemale rats [65]. However, the onset of puberty is notdependent on IGF-I or growth hormone secretion. Leptinhas effects upon GnRH secretion and is a permissive factorin the onset of mammalian puberty and potentially menar-che [66], as serum levels of GnRH and thereby LH dependon a critical accumulation of fat mass as resource to start awoman’s reproductive life. This could explain why in-creased adiposity, as in girls born SGA, might be associatedwith a younger age at menarche (via higher leptin). Addi-tionally, in leptin deficiency delayed pubertal maturationdue to low LH levels has been observed which can be cor-rected by leptin treatment [67–69]. By comparative and phy-logenetic approach it has been shown that GnRH andadipokinetic hormone signalling share a common evolution-ary origin [70].
Genes controlling puberty are organized in functionalnetworks that are internally organized in a hierarchical fash-ion. One of these networks includes tumor suppressor genesas important regulators of transsynaptic information and glia
KISS
Transcriptional Regulators of Neural and Glial Networks
Upstream Regulators
Inhibitory Neurons
Excitatory Neurons
OPR
GABAR
GluR GPR54 IGFR FGFR
TGFR
PGER
Glia Glu
GABA
Prepro ENK
IGF-I
FGF
TGFα,ß
PGE2 GnRH Neuron
Pulsatile GnRH Secretion
Childhood (prepubertal) Puberty
I. Upstream Regulation
• Repressors of Repressors • Repressors • Activators
II. Subordinate Genes
+ -
+ -
+ + -
-
+ -
III. Hormone Secretion
IV. Pubertal Phenotype
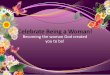
Fig. 1 Proposed hierarchical arrangement of the neuroendocrine net-work controlling the initiation of mammalian puberty. The secretoryactivity of GnRH neurons depends on both transsynaptic and glialinputs, which are in turn controlled by upper-echelon genes. It isspeculated that developmental changes include inputs from genes thatunderlie imprinting. At time of onset of puberty, repressors of repress-ors become more activated causing decreased activity of repressors and
increased activity of activators of the subordinate gene network thatcontrols GnRH secretion. These genes, that are differentially expressedin neurons and glia, are necessary for the integration of neuron-toneuron, glia-neuron, and glia to-glia communication. It is envisionedthat such a functional integration is required to initiate and maintain anenhanced level of pulsatile GnRH secretion at puberty [50, 72, 125]
132 Rev Endocr Metab Disord (2012) 13:129–140

to GnRH communication [50, 71, 72]. The networks core iscomposed of both trans-activational and repressive nodes (seemodel Fig. 1). Activators represent the driving principle whilethe repressors likely encompass tone preventing prematurestimulation [72]. Results from a recent study suggest, thatapproximately half of the variation in age at menarche isattributable to inherited genes, the remainder half attributableto environmental effects [73]. At least 30 genes appear to playa role in the age at which girls reach puberty and menarche[74]. Recent genome-wide association studies (GWAS) iden-tified LIN28B (6q21), a gene that is involved in controllingcell self-renewal and cell differentiation and signaling effectsof early-life environmental exposures on tempo of growth andtiming of puberty, and long-term disease risks [75–78]. Singlenucleotide polymorphism (SNP) studies showed for some ofthe obesity risk genes such as LIN28B and FTO, that the samevariant can be identified as obesity-susceptibility allele andmenarche age decreasing allele [74].
Conclusion derived from these investigative efforts is thatthe onset of puberty is likely exerted by complex regulatorygene networks (polygenic) [72]. Recent identification of keyquantitative trait loci regulating the abundance of multipletranscripts in the nervous system in a tissue-specific manner[79] adds considerable credence to the idea that both thetiming (and perhaps the progression of the pubertal process)is determined by the functional integration of gene networksthat—controlled by a set of “upper echelon” regulatory loci—operates within both neuronal and glial populations involvedin the control of GnRH secretion. In addition, recent researchshowed that imprinting patterns of several genes affect puber-tal timing and thereby reflect an important link between envi-ronmental and neurobiological factors (see details outlinedbelow). Girls who are overweight are more likely to gothrough puberty at young ages.
3 Epigenetic regulation
3.1 Epigenetic contribution to regulation of weightand growth
Through GWAS, variants of several genes were identifiedthat a linked to the risk for developing obesity [80]. Somegenetic risk markers of adult obesity have been shown to beassociated with weight gain and growth as early as ininfancy [81]. However, in addition on the underlying genet-ic background, fetal and neonatal life are characterized by atremendous plasticity and ability to respond to nutritionaland other environmental factors [82]. A high grade of plas-ticity in particular during important transitions of humandevelopment can be postulated and will be discussed in thissection (see Fig. 2). Early life programming of adult diseaseand metabolic processes was described by the well-known
Barker hypothesis in 2004 [83]. It states that prenatal expo-sures to nutritional extremes or environmental exposuresduring in utero development can program subsequent phys-iologic and metabolic homeostasis in adult life. This haslong been recognized with the observation that low birthweight children are at increased risk for metabolic andcardiovascular disease as adults [83]. Our current under-standing has now expanded to incorporate new mechanismsincluding an interplay between genetic and environmentalfactors that influence in utero programming of adult disease.
The traditional focus of genetics on disease developmenthas emphasized changes in DNA sequence such as polymor-phisms, mutations, deletions, and insertions. In recent years, anew concept in genetic change and heritability has emergedthat enhances our ability to understand how all cells cancontain the same DNA but have varied gene expressiondepending on specific tissue and environment. Epigenetics isthe study of heritable changes in gene expression potential thatcan occur without changes in DNA sequence [84]. Exogenousfactors that cause epigenetic changes can occur over thecourse of a lifetime such as stress and environmental toxicantexposures [85]. Cells respond to signals through endogenoushormones, nutritional factors, and environmental exposuresand gene expression changes accordingly. Waterland and
Inherited Genotype
Postnatal Environment
Epigenotype
Hormonal/enzymatic control
Changes of multiple set-points allow high “plasticity” of metabolome
Growth
Weight Gain
Sexual Maturation
Fetal growth Infancy Childhood Adolescence
Prenatal Environment
Ph
eno
typ
e
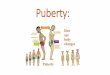
Fig. 2 Model of normal and disturbed development. On the basis onan inherited genotype, prenatal and postnatal environmental factorsthat include nutrition, maternal health, environmental chemicals, stressand lifestyle, cause epigenetic adaptations. These epigenetic changesallow plasticity, which is critically important in particular during tran-sitions of development, i.e. change from pre- to postnatal environment.Changes of the epigenotype can be transient or permanent and affectthe expression and secretion of hormones and enzymes and result inmultiple metabolic adaptations. They are responsible for metabolicprogramming that affects phenotypic outcomes later in life includinggrowth, adiposity and sexual maturation and also diseases such ascardiovascular disease, type 2 diabetes and cancer
Rev Endocr Metab Disord (2012) 13:129–140 133

Michels put forth “epigenetic epidemiology” as a novel areathat explores the epigenetic mechanisms in the developmentalorigins of health and disease [84].
The most easily described and well-known example ofepigenetic inheritance is genomic imprinting in which thereis silencing of one parental allele at a single locus in germstem cells resulting in monoallelic gene expression in off-spring. Abnormal genomic imprinting has been observed indisorders such as Prader-Willi and Beckwith-WiedemanSyndrome. Current epigenetic research focuses on metabol-ic imprinting where effects on gene expression andprogramming of metabolism occur [86]. Gene expressioncan be affected by multiple epigenetic mechanisms, two ofwhich, DNA methylation and histone modification, are welldescribed in mammalian systems in the scientific literature.We will briefly describe each and how it can impact devel-opmental processes.
DNA methylation is the best described mechanism formetabolic imprinting and usually occurs at cytosines withinCytosine-Guanine (CpG) islands of the genome. CpGs areregions of more than 500 base pairs with GC content greaterthan 55% in DNA sequences that are located in promoterregions of 40% of mammalian genes making their functionextremely important for normal gene expression [87]. Meth-ylation (addition of a –CH3 methyl group by covalent bond)of these islands can lead to silencing of gene expression, andde novo methylation of CpG islands is a hallmark of humancancers. Hypomethylation has been associated with reducedchromosomal stability and changed genome function. InFragile X syndrome, methylation of the CGG repeat inFMR1 causes the gene to be silenced [87]. DNA methylationcan regulate numerous cellular processes, including chromatinstructure/remodeling, X chromosome inactivation, and ge-nomic imprinting.
The direct contribution of epigenetic change to growth andweight balance remains to be determined, but several studiesdo cite preliminary evidence of epigenetic influence on met-abolic programming. For example, cloned mice are born withnormal birth weights but develop adult onset obesity withhyperinsulinemia at higher rates than non-cloned mice, indi-cating that cloning may result in epigenetic abnormalities thataffect metabolic set-points [88]. Mutations in the genes encod-ing leptin can cause obesity in humans, and the promoterregion of this gene has a high density of CpG sites making ithighly susceptible to DNA methylation [88]. In transientneonatal diabetes, studies found abnormal methylation pat-terns in several imprinted genes within white blood cells [84].In addition, nutrition in one generation can change risks fordiabetes in the future, suggesting that epigenetic changes canimpact diabetes risk. Prader-Willi syndrome is characterizedby hyperphagic obesity, and specific cases have resulted froman imprinted region of chromosome 15 as classical example ofepigenetic silencing [84].
Histone modification is another epigenetic mechanismwhich may function on its own or in combination withDNA methylation to lead to changes in gene expression.In its normal physical structure, DNA is wrapped aroundhistone proteins in a form called chromatin. Chromatinstructure is regulated by modifications to the tails of histoneproteins that undergo post-translational modifications thataffect their interaction with other molecules. Histone modifi-cations such as acetylation, methylation, and phosphorylationcan inactivate or activate transcription. Acetylation of tails ofthe H3 and H4 proteins generally tends to signify activetranscriptionally competent regions and hypoacetylation hasbeen found in transcriptionally inactive regions. Methylationof histones can be a marker of increased chromatin activity[89].
Epigenetics explain modulating of gene transcription bymechanisms other than changes in the underlying DNAsequence. This will allow some plasticity, i.e. necessaryfor metabolic compensations to respond to IUGR elicitingsubtle modifications in the phenotype (see model in Fig. 2).IUGR is accompanied by changes in the quantity and activityof enzymes responsible for epigenetic changes. In the IUGRrat brain at birth, global decreases in DNA methylation andincreases in histone acetylation are observed, accompanied bya concomitant decrease in the DNA methyltransferaseDNMT1, a major regulator to maintain methylation, themethyl-CpG binding protein MeCP2, and also the histonedeacetylase HDAC1 [90]. IUGR was also associated withchromatin modifications in the liver showing persistentincreases in acetylation and reduced hepatic expression ofDNMT1. IUGR was furthermore associated with specificchanges in the IUGR promoter histones of skeletal muscleglucose transporter GLUT4 and β-cell Pdx1 (for review see[91]). Several transcription factors are essential for normalpancreas development and beta cell differentiation. PDX, akey gene in pancreas development, was downregulated bymore than 50% at birth in IUGR rat pups, while the beta cellmass remained unaltered at birth but significantly reducedwhen the rats became adult [92]. It has been demonstratedthat the initial downregulation was caused by histone-deacetylation of the Pdx1 promoter, an epigenetic modifica-tion that was initially reversible but could lead later to perma-nent modifications by DNA methylation resulting in Pdx1silencing [93].
Adult final height is dependent on critical phases of growth.Most adult shortness is a result of subnormal growth in multi-ple phases, such as intrauterine growth retardation and growthstunting in early life [94]. Even if the mechanisms are not yetdetermined it has been shown that early postnatal nutrition hasprofound effects on somatotropic function in mice [95]. In ratsit has been demonstrated that the metabolic programminginduced by IUGR causes changes in histone acetylation inthe IGF-I promotor region [96]. Disruption of imprinting in
134 Rev Endocr Metab Disord (2012) 13:129–140

chromosome 11p15 results in two fetal growth disorders withopposite phenotypes: the Beckwith-Wiedemann (BWS) obe-sity phenotype and the Silver-Russell (SRS) short stature/failure to thrive phenotype. In both syndromes defectiveIGF2 imprinting has been demonstrated [97–99] which aretwo more classical examples of gene imprinting.
3.2 Epigenetic regulation of the onset of puberty
In recent years it became clear that the onset of puberty isalso regulated by genes that underlie imprinting. Epigeneticmechanisms can provide gene-specific gate- keeper mecha-nisms [100]. It has been demonstrated in female rhesusmonkeys, that the onset of puberty is associated with lowerhypothalamic expression of methylation regulating enzymeDNMT1 [71]. The onset of puberty is accompanied bychanges of DNA methylation and histone modification oftranscriptional repressors resulting in activation of genesthat are known to be critically involved in the onset ofpuberty such as KISS1 [63, 72]. Genome-wide analysis ofhypothalamic DNA methylation revealed profound changesin methylation patterns associated with the onset of femalepuberty. Pharmacological disruption of two epigeneticmarkers associated with gene silencing (DNA methylationand histone deacetylation) resulted in pubertal failure, sug-gesting that disruption of these two silencing mechanismsleads to activation of repressor genes whose expressionwould normally decrease at puberty [63]. Ojeda et al. estab-lished the new concept that both inhibitory and stimulatorypathways of transcriptional and posttranscriptional regula-tion operate within neuronal and glial populations that playa role in controlling the onset of puberty. This level ofregulation is provided by layers of activators and repressorsacting in concert with epigenetic mechanisms. In addition, itis proposed that more centrally located genes can act asrepressors of repressors, where their activation results inactivation of GnRH secretion [63, 72].
3.3 Heritability of epigenetic changes
Several environmental chemicals have been observed to causetransgenerational effects without known etiology because tra-ditional genetic mutation changes to the DNA sequencewould occur over long periods of time. Heritable epigeneticshas been proposed as a mechanism for transgenerational phe-notypic changes and refers to the transmission of a biologicaltrait to subsequent generations via epigenetic modifications inthe germline [89]. These changes occur via altered program-ming within germ cells/imprinted genes or through alteredexpression of RNAwithin gametes [101]. Male rats exposedto vinclozolin (an anti-androgen chemotherapeutic agent) dur-ing gonadal development resulted in the expected reducedsperm counts and decreased fertility in adulthood, but the loss
of fertility was maintained through the male germline for fourgenerations. Sperm DNA methylation patterns were inheritedand observed throughout the generations [102].
4 Environmental chemicals
4.1 Environmental chemicals affecting growth& development
Proper hormonal signaling during the in utero developmen-tal period is integral for normal reproductive and endocrinedevelopment from early childhood to adulthood. Endocrinedisrupting chemical (EDC) are a class of compounds thatcan act through a variety of mechanisms to adversely impactnormal endocrine function leading to effects that can bepassed on to future generations. Because normal hormonalfunction is essential for normal growth and development,EDC exposures during fetal life have been implicated inprogramming of metabolic set points in relation to growthand development (see model Fig. 2). Grun and Blumbergput forth the “obesogen hypothesis” which postulates thatadipose tissue is an active endocrine organ in which EDCscan promote obesity by increasing adipose cell number orstorage of fat, program metabolic rates, and alter hormonalcontrol of appetite. Obesogens may affect basal metabolicrate by shifting energy balance to increase calorie storageand changing hormonal control of appetite [103]. Severalchemicals such as diethylstilbestrol (DES), genistein, andbisphenol A (BPA) have been implicated in animal studiesas obesogens [103–106]. Human epidemiologic studies doc-ument an association between exposures to environmentalchemicals such as phthalates and DES and increased weightor waist circumference [107, 108]. We present some keyexamples of how endocrine disrupting chemicals can affectgrowth and metabolism.
Perinatal exposure to BPA resulted in increased adipo-genesis in rats [109]. BPA is known to cross the blood–brain-barrier [110], and in addition to its estrogenic effects,it antagonizes the thyroid hormone receptor and inhibitstranscriptional activity of triiodothyronine [111]. BecauseBPA exposure is ubiquitous, BPA might play a significantpublic health concern regarding the childhood obesity epi-demic and reproductive endocrine function [112].
Nuclear PPARs α, γ, δ regulate adipogenesis in the body.Individuals with certain variants of PPARγ show obesityand insulin sensitivity while others have low body mass[113]. Grun has observed that tributyltin, a persistent organicpollutant found in paints, plasticizers and in foods, is anagonist for PPARγ. In a murine model, tributyltin exposurein utero is associatedwith early lipid accumulation and hepaticsteatosis in newborn mice [113]. In addition, some phthalatechemicals (ubiquitous man-made chemicals found in soft
Rev Endocr Metab Disord (2012) 13:129–140 135

plastics and cosmetics) increase lipid mobilization and fattyacid oxidation [114], which can lead to reduced adipose massand body weight. This is an interesting finding given that lowbirth weight and malnutrition are predictors of obesity later inlife. If phthalate exposure in utero leads to reduced growth andbody weight in fetal life, this could be an important risk factorfor obesity in the future. One human study documented across-sectional association between phthalate exposure andincreased waist circumference and markers of insulin resis-tance in men [107]. Therefore, early life exposures to endo-crine disrupting chemicals may program metabolicphysiology through the PPARγ mechanism.
An interesting study demonstrating how nutritional factorscan affect body composition and weight gain was performedby Jirtle and colleagues [115], who reported that in micematernal dietary exposure to genistein (an isoflavone withestrogenic actions found mostly in soy) during gestation, atlevels comparable with humans consuming high-soy diets,was associated with increased cytosine methylation at a retro-transposon upstream of the transcription start site of the Agoutigene [115]. Hypermethylation induced by genistein resultedin decreased ectopic Agouti expression, which reduced yellowphaeomelanin production resulting in a darker coat color andprotected against adult-onset obesity by silencing the Agoutigene. In other words, in utero dietary genistein protected theoffspring from obesity because, genistein induced hyperme-thylation that persisted into adulthood [115].
4.2 EDCs and puberty
An international panel of experts to review the impact ofenvironmental influences on the regulation of pubertal onsetand progression identified that body size, adiposity and EDCsmay be associated with pubertal disturbances in humans [116,117]. Many activate parts of the endocrine system whichstimulate the estrogen receptor [118]. EDCs can be estrogenic,anti-estrogenic, anti-androgenic, androgenic, or directly stim-ulate GnRH production [116, 119]. EDCs are also known toalter hormone secretion by epigenetic, i.e. DNA methylationand histone modifications. EDCs that target the hypothalamic-pituitary-axis can affect normal pubertal hormonal signaling.It has been well established that exogenous estrogens can leadto premature breast development and exogenous androgensare related to virilization phenotypes. EDCs may act to affectpuberty via stimulation of estrogen sensitive cells includinghypothalamic neurons, which release kisspeptin which accel-erates pubertal onset [120]. Dichloro-diphenyltrichloroethane(DDT) is a well known pesticide that is estrogenic and hasnow been banned due to its harmful health effects [121]. Inrats, exposure to DDT resulted in increased GnRH pulsatilesecretion, which could lead to early puberty. Other EDCs suchas bisphenol A are associated with early puberty in animals[122].
Diethylstilbestrol (DES) is one of the best known estrogen-ic agents. With developmental exposures, infants developedsevere reproductive tract abnormalities and clear cell adeno-carcinoma [123]. The third generation is being studied cur-rently and also has also been observed to have reproductivetract abnormalities including irregular menses [124]. Thesenew findings emphasize the transgenerational effects ofEDCs. The mechanism is currently unknown but likelyinvolves epigenetic changes induced by the initial DES expo-sures that are heritable. There are multiple mechanisms ofaction put forth in the literature regarding the physiologicchanges that DES can initiate, specifically methylation anddemethylation of key regions on genes that are involved inhormonal homeostasis.
5 Conclusions
It has now been observed that some individuals have differentmetabolic set points that predispose them to obesity andsubsequent adverse health outcomes. These set points can beinfluenced as early as in utero by environmental, genetic, andnutritional factors (see model Fig. 2). Furthermore, IUGR cancause metabolic reprogramming that can lead to phenotypicchanges including growth, weight gain and sexual maturation.Future research should incorporate both IUGR and environ-mental chemicals and their potential impacts on the genomeinto the complex set of factors that can program growth andmetabolism. For example, animal studies may want to exam-ine growth restriction in combination with environmentalchemical exposures to determine resulting epigenetic changesthat impact hormonal physiologic development of future ab-normal growth, metabolic and pubertal phenotypes. Severalexpert bodies including the Endocrine Society have releasedstatements highlighting concern regarding human exposuresto EDCs and calling for future research that incorporatesEDCs in a metabolic framework. Human epidemiologic stud-ies should also incorporate multiple etiologic factors includingnutrition as well as environmental chemical exposures.
6 Key statements
There is a significant overlap between neuroendocrine mech-anisms in the regulation of growth, energy homeostasis andpuberty. Fetal undernutrition is accompanied by changes ofhormonal secretion and epigenetics and results in a thriftyphenotype. This adaption can be inappropriate for the postnatalenvironmental conditions resulting in accumulation of bodyfat, altered growth and sexual maturation, as well as develop-ment of obesity and cardiovascular disease later in life. Theobesogenic rapid catch–up growthmay originate from pre- andearly postnatal metabolic programming of important set points
136 Rev Endocr Metab Disord (2012) 13:129–140

resulting in insulin and leptin resistance. Growth, energy ho-meostasis and sexual maturation are regulated by hormones,genes and epigenetics and are susceptible to alterations due toenvironmental factors, including EDCs. The overlapping reg-ulatory pathways between neuroendocrine mechanisms thatregulate energy homeostasis and puberty onset might explainwhy IUGR affects not only the postnatal growth and weightgain but also the onset of puberty.
7 Key unanswered questions
Exact mechanisms linking nutritional factors and environmen-tal chemicals with epigenetics and neuroendocrine function arelargely unknown. In addition to identification of risk factorsthat promote aberrant metabolic programs, novel preventivestrategies need to be developed. For example, it is still un-known what would be the optimal trajectory for weight andheight gain in children born SGA in order to prevent detrimen-tal effects later in life (rapid vs. “controlled” catch-up growthand weight gain). Future research should include complexmodels of human growth pattern analysis and also of metabolicprogramming potentially by utilizing high-throughput geneticand epigenetic approaches as well as sytems biology andmetabolomic approaches.
References
1. Hernandez MI, Mericq V. Impact of being born small for gesta-tional age on onset and progression of puberty. Best Pract ResClin Endocrinol Metab. 2008;22:463–76.
2. Ranke MB, Cutfield WS, Lindberg A, Cowell CT, Albertsson-Wikland K, Reiter EO, et al. A growth prediction model for shortchildren born small for gestational age. J Pediatr EndocrinolMetab. 2002;15 Suppl 5:1273.
3. Ibanez L, Potau N, Marcos MV, de Zegher F. Exaggerated adre-narche and hyperinsulinism in adolescent girls born small forgestational age. J Clin Endocrinol Metab. 1999;84:4739–41.
4. van Weissenbruch MM, de Waal HA Delemarre-van. Early influ-ences on the tempo of puberty. HormRes. 2006;65 Suppl 3:105–11.
5. Main KM, Jensen RB, Asklund C, Hoi-Hansen CE, SkakkebaekNE. Low birth weight and male reproductive function. Horm Res.2006;65 Suppl 3:116–22.
6. Martinez-Aguayo A, Capurro T, Pena V, Iniguez G, HernandezMI, Avila A, et al. Comparison of leptin levels, body compositionand insulin sensitivity and secretion by OGTT in healthy, earlypubertal girls born at either appropriate- or small-for-gestationalage. Clin Endocrinol (Oxf). 2007;67:526–32.
7. Hofman PL, Cutfield WS. Insulin sensitivity in people born pre-term, with low or very low birth weight and small for gestationalage. J Endocrinol Invest. 2006;29:2–8.
8. Cutfield WS, Hofman PL, Mitchell M, Morison IM. Could epi-genetics play a role in the developmental origins of health anddisease? Pediatr Res. 2007;61:68R–75R.
9. Evagelidou EN, Giapros VI, Challa AS, Kiortsis DN, Tsatsoulis AA,Andronikou SK. Serum adiponectin levels, insulin resistance, andlipid profile in children born small for gestational age are affected by
the severity of growth retardation at birth. Eur J Endocrinol.2007;156:271–7.
10. Schwartz MW, Woods SC, Porte Jr D, Seeley RJ, Baskin DG.Central nervous system control of food intake. Nature.2000;404:661–71.
11. Cota D, Proulx K, Smith KA, Kozma SC, Thomas G,Woods SC, etal. Hypothalamic mTOR signaling regulates food intake. Science.2006;312:927–30.
12. Morton GJ, Cummings DE, Baskin DG, Barsh GS, SchwartzMW. Central nervous system control of food intake and bodyweight. Nature. 2006;443:289–95.
13. Parton LE, Ye CP, Coppari R, Enriori PJ, Choi B, Zhang CY, etal. Glucose sensing by POMC neurons regulates glucose homeo-stasis and is impaired in obesity. Nature. 2007;449:228–32.
14. Schwartz MW, Gelling RW. Rats lighten up with MCH antago-nist. Nat Med. 2002;8:779–81.
15. Bai FL, Yamano M, Shiotani Y, Emson PC, Smith AD, Powell JF,et al. An arcuato-paraventricular and -dorsomedial hypothalamicneuropeptide Y-containing system which lacks noradrenaline inthe rat. Brain Res. 1985;331:172–5.
16. Kerkerian L, Pelletier G. Effects of monosodium L-glutamateadministration on neuropeptide Y-containing neurons in the rathypothalamus. Brain Res. 1986;369:388–90.
17. Berthoud HR, Morrison C. The brain, appetite, and obesity. AnnuRev Psychol. 2008;59:55–92.
18. Komori T, Morikawa Y, Nanjo K, Senba E. Induction of brain-derived neurotrophic factor by leptin in the ventromedial hypo-thalamus. Neuroscience. 2006;139:1107–15.
19. Melnick I, Pronchuk N, Cowley MA, Grove KL, Colmers WF.Developmental switch in neuropeptide Y and melanocortin effectsin the paraventricular nucleus of the hypothalamus. Neuron.2007;56:1103–15.
20. Barker DJ, Osmond C. Infant mortality, childhood nutrition, andischaemic heart disease in England andWales. Lancet. 1986;1:1077–81.
21. Stefan Y, Grasso S, Perrelet A, Orci L. A quantitative immuno-fluorescent study of the endocrine cell populations in the devel-oping human pancreas. Diabetes. 1983;32:293–301.
22. Breant B, Gesina E, Blondeau B. Nutrition, glucocorticoids andpancreas development. Horm Res. 2006;65 Suppl 3:98–104.
23. Ackermann AM, Gannon M. Molecular regulation of pancreaticbeta-cell mass development, maintenance, and expansion. J MolEndocrinol. 2007;38:193–206.
24. Harder T, Bergmann R, Kallischnigg G, Plagemann A. Durationof breastfeeding and risk of overweight: a meta-analysis. Am JEpidemiol. 2005;162:397–403.
25. Dulloo AG. Thrifty energy metabolism in catch-up growth tra-jectories to insulin and leptin resistance. Best Pract Res ClinEndocrinol Metab. 2008;22:155–71.
26. Duffield JA, Vuocolo T, Tellam R, McFarlane JR, Kauter KG,Muhlhausler BS, et al. Intrauterine growth restriction and the sexspecific programming of leptin and peroxisome proliferator-activated receptor gamma (PPARgamma) mRNA expression invisceral fat in the lamb. Pediatr Res. 2009;66:59–65.
27. Barker DJ. The developmental origins of adult disease. J Am CollNutr. 2004;23:588S–95S.
28. Catalano PM, Thomas A, Huston-Presley L, Amini SB. Increasedfetal adiposity: a very sensitive marker of abnormal in uterodevelopment. Am J Obstet Gynecol. 2003;189:1698–704.
29. Gillman MW, Rifas-Shiman S, Berkey CS, Field AE, ColditzGA. Maternal gestational diabetes, birth weight, and adolescentobesity. Pediatrics. 2003;111:e221–6.
30. Ibanez L, Ong K, Dunger DB, de Zegher F. Early development ofadiposity and insulin resistance after catch-up weight gain insmall-for-gestational-age children. J Clin Endocrinol Metab.2006;91:2153–8.
Rev Endocr Metab Disord (2012) 13:129–140 137

31. Parsons TJ, Power C, Manor O. Fetal and early life growth andbody mass index from birth to early adulthood in 1958 Britishcohort: longitudinal study. BMJ. 2001;323:1331–5.
32. Loos RJ, Beunen G, Fagard R, Derom C, Vlietinck R. Birthweight and body composition in young women: a prospectivetwin study. Am J Clin Nutr. 2002;75:676–82.
33. Passos MC, Toste FP, Dutra SC, Trotta PA, Lisboa PC, de MouraEG. Role of neonatal hyperleptinaemia on serum adiponectin andsuppressor of cytokine signalling-3 expression in young rats. Br JNutr. 2009;101:250–6.
34. Plagemann A, Harder T, Janert U, Rake A, Rittel F, Rohde W, etal. Malformations of hypothalamic nuclei in hyperinsulinemicoffspring of rats with gestational diabetes. Dev Neurosci.1999;21:58–67.
35. Miles JL, Huber K, Thompson NM, Davison M, Breier BH.Moderate daily exercise activates metabolic flexibility to preventprenatally induced obesity. Endocrinology. 2009;150:179–86.
36. Puglianiello A, Germani D, Cianfarani S. Exposure to uteropla-cental insufficiency reduces the expression of signal transducerand activator of transcription 3 and proopiomelanocortin in thehypothalamus of newborn rats. Pediatr Res. 2009;66:208–11.
37. Simmons RA, Templeton LJ, Gertz SJ. Intrauterine growth retar-dation leads to the development of type 2 diabetes in the rat.Diabetes. 2001;50:2279–86.
38. Rajakumar PA, He J, Simmons RA, Devaskar SU. Effect ofuteroplacental insufficiency upon brain neuropeptide Y andcorticotropin-releasing factor gene expression and concentra-tions. Pediatr Res. 1998;44:168–74.
39. Peterside IE, Selak MA, Simmons RA. Impaired oxidative phos-phorylation in hepatic mitochondria in growth-retarded rats. Am JPhysiol Endocrinol Metab. 2003;285:E1258–66.
40. Thaler JP, Schwartz MW. Minireview: inflammation andobesity pathogenesis: the hypothalamus heats up. Endocrinology.2010;151:4109–15.
41. Posey KA, Clegg DJ, Printz RL, Byun J, Morton GJ,Vivekanandan-Giri A, et al. Hypothalamic proinflammatory lipidaccumulation, inflammation, and insulin resistance in rats fed ahigh-fat diet. Am J Physiol Endocrinol Metab. 2009;296:E1003–12.
42. Glavas MM, Kirigiti MA, Xiao XQ, Enriori PJ, Fisher SK, EvansAE, et al. Early overnutrition results in early-onset arcuate leptinresistance and increased sensitivity to high-fat diet. Endocrinology.2010;151:1598–610.
43. Roth CL, Bongiovanni KD, Gohlke B, Woelfle J. Changes indynamic insulin and gastrointestinal hormone secretion in obesechildren. J Pediatr Endocrinol Metab. 2010;23:1299–309.
44. Gohlke BC, Huber A, Hecher K, Fimmers R, Bartmann P, RothCL. Fetal insulin-like growth factor (IGF)-I, IGF-II, and ghrelinin association with birth weight and postnatal growth in mono-zygotic twins with discordant growth. J Clin Endocrinol Metab.2005;90:2270–4.
45. Gohlke BC, Bartmann P, Fimmers R, Huber A, Hecher K, RothCL. Fetal adiponectin and resistin in correlation with birth weightdifference in monozygotic twins with discordant growth. HormRes. 2008;69:37–44.
46. Gohlke BC, Huber A, Bartmann P, Fimmers R, Hecher K, BouretSG, et al. Cord blood leptin and IGF-I in relation to birth weightdifferences and head circumference in monozygotic twins. JPediatr Endocrinol Metab. 2006;19:3–9.
47. Bouret SG, Gorski JN, Patterson CM, Chen S, Levin BE, SimerlyRB. Hypothalamic neural projections are permanently disruptedin diet-induced obese rats. Cell Metab. 2008;7:179–85.
48. Bourguignon JP, Gerard A, Franchimont P. Maturation of thehypothalamic control of pulsatile gonadotropin-releasing hor-mone secretion at onset of puberty: II. Reduced potency of aninhibitory autofeedback. Endocrinology. 1990;127:2884–90.
49. Bourguignon JP, Gerard A, Mathieu J, Mathieu A, Franchimont P.Maturation of the hypothalamic control of pulsatile gonadotropin-releasing hormone secretion at onset of puberty. I. Increasedactivation of N-methyl-D-aspartate receptors. Endocrinology.1990;127:873–81.
50. Ojeda SR, Lomniczi A, Mastronardi C, Heger S, Roth C, ParentAS, et al. Minireview: the neuroendocrine regulation of puberty:is the time ripe for a systems biology approach? Endocrinology.2006;147:1166–74.
51. Ojeda SR, Roth C, Mungenast A, Heger S, Mastronardi C, ParentAS, et al. Neuroendocrine mechanisms controlling female puberty:new approaches, new concepts. Int J Androl. 2006;29:256–63.discussion 286-290.
52. Bourguignon JP, Gerard A, Alvarez Gonzalez ML, FranchimontP. Neuroendocrine mechanism of onset of puberty. Sequentialreduction in activity of inhibitory and facilitatory N-methyl-D-aspartate receptors. J Clin Invest. 1992;90:1736–44.
53. Terasawa E, Fernandez DL. Neurobiological mechanisms of theonset of puberty in primates. Endocr Rev. 2001;22:111–51.
54. Wuttke W, Honma K, Lamberts R, Hohn KG. The role of mono-amines in female puberty. Fed Proc. 1980;39:2378–83.
55. Wildt L, Marshall G, Knobil E. Experimental induction of pubertyin the infantile female rhesus monkey. Science. 1980;207:1373–5.
56. Plant TM. The role of KiSS-1 in the regulation of puberty inhigher primates. Eur J Endocrinol. 2006;155 Suppl 1:S11–6.
57. Shahab M, Mastronardi C, Seminara SB, Crowley WF, Ojeda SR,Plant TM. Increased hypothalamic GPR54 signaling: a potentialmechanism for initiation of puberty in primates. Proc Natl AcadSci U S A. 2005;102:2129–34.
58. El Majdoubi M, Sahu A, Ramaswamy S, Plant TM. NeuropeptideY: a hypothalamic brake restraining the onset of puberty inprimates. Proc Natl Acad Sci U S A. 2000;97:6179–84.
59. Plant TM. Leptin, growth hormone, and the onset of primatepuberty. J Clin Endocrinol Metab. 2001;86:458–60.
60. Keen KL, Burich AJ, Mitsushima D, Kasuya E, Terasawa E.Effects of pulsatile infusion of the GABA(A) receptor blockerbicuculline on the onset of puberty in female rhesus monkeys.Endocrinology. 1999;140:5257–66.
61. Terasawa E. Role of GABA in the mechanism of the onset ofpuberty in non-human primates. Int Rev Neurobiol. 2005;71:113–29.
62. Ojeda SR, Lomniczi A, Loche A, Matagne V, Kaidar G, SandauUS, et al. The transcriptional control of female puberty. BrainRes. 2010;1364:164–74.
63. Ojeda SR, Lomniczi A, Sandau U, Matagne V. New concepts onthe control of the onset of puberty. Endocr Dev. 2010;17:44–51.
64. Pierroz DD, Aebi AC, Huhtaniemi IT, Aubert ML. Many LHpeaks are needed to physiologically stimulate testosterone secre-tion: modulation by fasting and NPY. Am J Physiol. 1999;276:E603–10.
65. Hiney JK, Srivastava V, Nyberg CL, Ojeda SR, Dees WL. Insulin-like growth factor I of peripheral origin acts centrally to acceleratethe initiation of female puberty. Endocrinology. 1996;137:3717–28.
66. Casanueva FF, Dieguez C. Neuroendocrine regulation andactions of leptin. Front Neuroendocrinol. 1999;20:317–63.
67. Farooqi IS, Jebb SA, Langmack G, Lawrence E, Cheetham CH,Prentice AM, et al. Effects of recombinant leptin therapy in a childwith congenital leptin deficiency. N Engl J Med. 1999;341:879–84.
68. Licinio J, Caglayan S, Ozata M, Yildiz BO, de Miranda PB,O'Kirwan F, et al. Phenotypic effects of leptin replacement onmorbid obesity, diabetes mellitus, hypogonadism, and behavior inleptin-deficient adults. Proc Natl Acad Sci U S A. 2004;101:4531–6.
69. Clayton PE, Trueman JA. Leptin and puberty. Arch Dis Child.2000;83:1–4.
70. Lindemans M, Liu F, Janssen T, Husson SJ, Mertens I, Gade G, etal. Adipokinetic hormone signaling through the gonadotropin-
138 Rev Endocr Metab Disord (2012) 13:129–140

releasing hormone receptor modulates egg-laying in Caenorhab-ditis elegans. Proc Natl Acad Sci U S A. 2009;106:1642–7.
71. Roth CL, Mastronardi C, Lomniczi A, Wright H, Cabrera R,Mungenast AE, et al. Expression of a tumor-related gene networkincreases in the mammalian hypothalamus at the time of femalepuberty. Endocrinology. 2007;148:5147–61.
72. Ojeda SR, Dubay C, Lomniczi A, Kaidar G, Matagne V, SandauUS, et al. Gene networks and the neuroendocrine regulation ofpuberty. Mol Cell Endocrinol. 2010;324:3–11.
73. Morris DH, Jones ME, Schoemaker MJ, Ashworth A, SwerdlowAJ. Familial concordance for age at menarche: analyses from theBreakthrough Generations Study. Paediatr Perinat Epidemiol.2011;25:306–11.
74. Elks CE, Perry JR, Sulem P, Chasman DI, Franceschini N, He C,et al. Thirty new loci for age at menarche identified by a meta-analysis of genome-wide association studies. Nat Genet.2010;42:1077–85.
75. Sulem P, Gudbjartsson DF, Rafnar T, Holm H, Olafsdottir EJ,Olafsdottir GH, et al. Genome-wide association study identifiessequence variants on 6q21 associated with age at menarche. NatGenet. 2009;41:734–8.
76. Viswanathan SR, Daley GQ, Gregory RI. Selective blockade ofmicroRNA processing by Lin28. Science. 2008;320:97–100.
77. Nimmo RA, Slack FJ. An elegant miRror: microRNAs in stem cells,developmental timing and cancer. Chromosoma. 2009;118:405–18.
78. Hartge P. Genetics of reproductive lifespan. Nat Genet.2009;41:637–8.
79. Chesler EJ, Lu L, Shou S, Qu Y, Gu J, Wang J, et al. Complex traitanalysis of gene expression uncovers polygenic and pleiotropicnetworks that modulate nervous system function. Nat Genet.2005;37:233–42.
80. Hinney A, Vogel CI, Hebebrand J. From monogenic to polygenicobesity: recent advances. Eur Child Adolesc Psychiatry.2010;19:297–310.
81. Elks CE, Loos RJ, Sharp SJ, Langenberg C, Ring SM, TimpsonNJ, et al. Genetic markers of adult obesity risk are associated withgreater early infancy weight gain and growth. PLoS Med. 2010;7:e1000284.
82. Heerwagen MJ, Miller MR, Barbour LA, Friedman JE. Maternalobesity and fetal metabolic programming: a fertile epigenetic soil.Am J Physiol Regul Integr Comp Physiol. 2010;299:R711–22.
83. Barker DJ. Developmental origins of adult health and disease. JEpidemiol Community Health. 2004;58:114–5.
84. Waterland RA, Michels KB. Epigenetic epidemiology of the devel-opmental origins hypothesis. Annu Rev Nutr. 2007;27:363–88.
85. Jirtle RL, Skinner MK. Environmental epigenomics and diseasesusceptibility. Nat Rev Genet. 2007;8:253–62.
86. Reik W, Walter J. Genomic imprinting: parental influence on thegenome. Nat Rev Genet. 2001;2:21–32.
87. Egger G, Liang G, Aparicio A, Jones PA. Epigenetics in humandisease and prospects for epigenetic therapy. Nature. 2004;429:457–63.
88. McAllister EJ, Dhurandhar NV, Keith SW, Aronne LJ, Barger J,Baskin M, et al. Ten putative contributors to the obesity epidemic.Crit Rev Food Sci Nutr. 2009;49:868–913.
89. Baccarelli A, Bollati V. Epigenetics and environmental chemi-cals. Curr Opin Pediatr. 2009;21:243–51.
90. Ke X, Lei Q, James SJ, Kelleher SL, Melnyk S, Jernigan S, et al.Uteroplacental insufficiency affects epigenetic determinants ofchromatin structure in brains of neonatal and juvenile IUGR rats.Physiol Genomics. 2006;25:16–28.
91. Joss-Moore LA, Lane RH. The developmental origins of adultdisease. Curr Opin Pediatr. 2009;21:230–4.
92. Stoffers DA, Desai BM, DeLeon DD, Simmons RA. Neonatalexendin-4 prevents the development of diabetes in the intrauter-ine growth retarded rat. Diabetes. 2003;52:734–40.
93. Park JH, Stoffers DA, Nicholls RD, Simmons RA. Developmentof type 2 diabetes following intrauterine growth retardation in ratsis associated with progressive epigenetic silencing of Pdx1. J ClinInvest. 2008;118:2316–24.
94. Luo ZC, Low LC, Karlberg J. Critical growth phases for adultshortness in Hong Kong Chinese. J Pediatr Endocrinol Metab.2001;14:757–65.
95. Kappeler L, De Magalhaes Filho C, Leneuve P, Xu J, Brunel N,Chatziantoniou C, et al. Early postnatal nutrition determinessomatotropic function in mice. Endocrinology. 2009;150:314–23.
96. Fu Q, Yu X, Callaway CW, Lane RH, McKnight RA. Epigenetics:intrauterine growth retardation (IUGR) modifies the histone codealong the rat hepatic IGF-1 gene. Faseb J. 2009;23:2438–49.
97. Nativio R, Sparago A, Ito Y, Weksberg R, Riccio A, Murrell A.Disruption of genomic neighbourhood at the imprinted IGF2-H19locus in Beckwith-Wiedemann syndrome and Silver-Russell syn-drome. Hum Mol Genet. 2011;20:1363–74.
98. Netchine I, Rossignol S, Dufourg MN, Azzi S, Rousseau A, PerinL, et al. 11p15 imprinting center region 1 loss of methylation is acommon and specific cause of typical Russell-Silver syndrome:clinical scoring system and epigenetic-phenotypic correlations. JClin Endocrinol Metab. 2007;92:3148–54.
99. Demars J, Rossignol S, Netchine I, Syin Lee K, ShmelaM, Faivre L,et al. New insights into the pathogenesis of Beckwith-Wiedemannand Silver-Russell syndromes: Contribution of small copy numbervariations to 11p15 imprinting defects. Hum Mutat. 2011
100. Garcia-Bassets I, Kwon YS, Telese F, Prefontaine GG, Hutt KR,Cheng CS, et al. Histone methylation-dependent mechanismsimpose ligand dependency for gene activation by nuclear recep-tors. Cell. 2007;128:505–18.
101. Perera F, Herbstman J. Prenatal environmental exposures, epige-netics, and disease. Reprod Toxicol. 31:363–373
102. Anway MD, Leathers C, Skinner MK. Endocrine disruptor vin-clozolin induced epigenetic transgenerational adult-onset disease.Endocrinology. 2006;147:5515–23.
103. Janesick A, Blumberg B. Endocrine disrupting chemicals and thedevelopmental programming of adipogenesis and obesity. BirthDefects Res C Embryo Today 93:34–50
104. Newbold RR, Jefferson WN, Padilla-Banks E, Haseman J.Developmental exposure to diethylstilbestrol (DES) alters uterineresponse to estrogens in prepubescent mice: low versus high doseeffects. Reprod Toxicol. 2004;18:399–406.
105. Newbold RR, Padilla-Banks E, Jefferson WN. Environmentalestrogens and obesity. Mol Cell Endocrinol. 2009;304:84–9.
106. Rubin BS, Murray MK, Damassa DA, King JC, Soto AM.Perinatal exposure to low doses of bisphenol A affects bodyweight,patterns of estrous cyclicity, and plasma LH levels. Environ HealthPerspect. 2001;109:675–80.
107. Stahlhut RW, van Wijngaarden E, Dye TD, Cook S, Swan SH.Concentrations of urinary phthalate metabolites are associatedwith increased waist circumference and insulin resistance in adultU.S. males. Environ Health Perspect. 2007;115:876–82.
108. Verhulst SL, Nelen V, Hond ED, Koppen G, Beunckens C, VaelC, et al. Intrauterine exposure to environmental pollutants andbody mass index during the first 3 years of life. Environ HealthPerspect. 2009;117:122–6.
109. Somm E, Schwitzgebel VM, Toulotte A, Cederroth CR, Combes-cure C, Nef S, et al. Perinatal exposure to bisphenol a alters earlyadipogenesis in the rat. Environ Health Perspect. 2009;117:1549–55.
110. Sun Y, Nakashima MN, Takahashi M, Kuroda N, Nakashima K.Determination of bisphenol A in rat brain by microdialysis andcolumn switching high-performance liquid chromatography withfluorescence detection. Biomed Chromatogr. 2002;16:319–26.
111. Zoeller RT, Bansal R, Parris C. Bisphenol-A, an environmentalcontaminant that acts as a thyroid hormone receptor antagonist in
Rev Endocr Metab Disord (2012) 13:129–140 139

vitro, increases serum thyroxine, and alters RC3/neurogranin ex-pression in the developing rat brain. Endocrinology. 2005;146:607–12.
112. Savabieasfahani M, Kannan K, Astapova O, Evans NP,Padmanabhan V. Developmental programming: differential effectsof prenatal exposure to bisphenol-A or methoxychlor on reproduc-tive function. Endocrinology. 2006;147:5956–66.
113. Grun F, Blumberg B. Endocrine disrupters as obesogens. MolCell Endocrinol. 2009;304:19–29.
114. Itsuki-Yoneda A, Kimoto M, Tsuji H, Hiemori M, Yamashita H.Effect of a hypolipidemic drug, Di (2-ethylhexyl) phthalate, onmRNA-expression associated fatty acid and acetate metabolismin rat tissues. Biosci Biotechnol Biochem. 2007;71:414–20.
115. Dolinoy DC, Weidman JR, Waterland RA, Jirtle RL. Maternalgenistein alters coat color and protects Avy mouse offspring fromobesity bymodifying the fetal epigenome. Environ Health Perspect.2006;114:567–72.
116. Buck Louis GM, Gray Jr LE, Marcus M, Ojeda SR, Pescovitz OH,Witchel SF, et al. Environmental factors and puberty timing: expertpanel research needs. Pediatrics. 2008;121 Suppl 3:S192–207.
117. Parent AS, Rasier G, Gerard A, Heger S, Roth C, Mastronardi C,et al. Early onset of puberty: tracking genetic and environmentalfactors. Horm Res. 2005;64 Suppl 2:41–7.
118. Crews D, McLachlan JA. Epigenetics, evolution, endocrine dis-ruption, health, and disease. Endocrinology. 2006;147:S4–S10.
119. Ozen S, Darcan S: Effects of environmental endocrine disruptorson pubertal development. J Clin Res Pediatr Endocrinol. 3:1–6
120. Mouritsen A, Aksglaede L, Sorensen K, Mogensen SS, Leffers H,Main KM, et al. Hypothesis: exposure to endocrine-disruptingchemicals may interfere with timing of puberty. Int J Androl.33:346–359
121. Rasier G, Parent AS, Gerard A, Denooz R, Lebrethon MC, CharlierC, et al. Mechanisms of interaction of endocrine-disrupting chem-icals with glutamate-evoked secretion of gonadotropin-releasinghormone. Toxicol Sci. 2008;102:33–41.
122. Patisaul HB, Todd KL, Mickens JA, Adewale HB. Impact ofneonatal exposure to the ERalpha agonist PPT, bisphenol-A orphytoestrogens on hypothalamic kisspeptin fiber density in maleand female rats. Neurotoxicology. 2009;30:350–7.
123. Titus-Ernstoff L, Troisi R, Hatch EE, Palmer JR, Hyer M, KaufmanR, et al. Birth defects in the sons and daughters of women who wereexposed in utero to diethylstilbestrol (DES). Int J Androl. 33:377–384
124. Hatch EE, Troisi R, Wise LA, Titus-Ernstoff L, Hyer M, PalmerJR, et al. Preterm birth, fetal growth, and age at menarche amongwomen exposed prenatally to diethylstilbestrol (DES). ReprodToxicol. 31:151–157
125. Roth CL, Ojeda SR. Genes involved in the neuroendocrine con-trol of normal puberty and abnormal puberty of central origin.Pediatr Endocrinol Rev. 2005;3:7–16.
140 Rev Endocr Metab Disord (2012) 13:129–140