Embed Size (px)
Citation preview
PRECOCIOUS PUBERTY
Definition of precocious puberty
Precocious puberty is defined as the onset of secondary
sexual characteristics before 8 yr of age in girls and 9 yr in
boys.
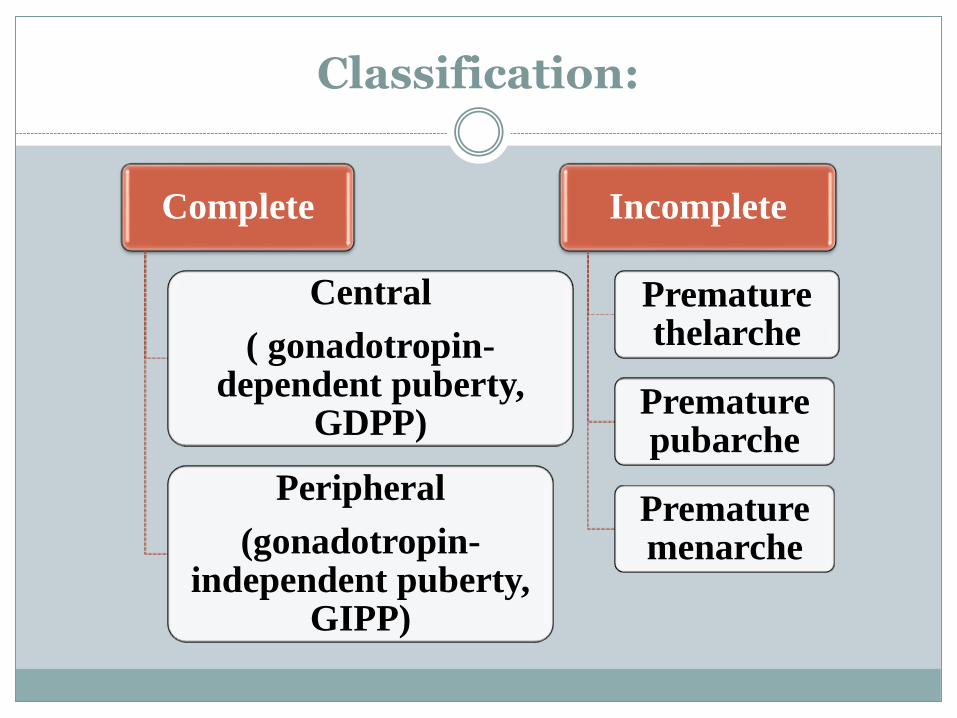
Classification:
Complete
Central
( gonadotropin-dependent puberty,
GDPP)
Peripheral
(gonadotropin-independent puberty,
GIPP)
Incomplete
Premature thelarche
Premature pubarche
Premature menarche
Gonadotropin-dependent precocious puberty ( GDPP)
also known as true precocious puberty
early activation of the entire hypothalamic-pituitary-gonadal (HPG) axis
is caused by the secretion of high-amplitude pulses ofgonadotropin-releasing hormone (GnRH) by thehypothalamus.
Although the onset is early, the pattern and timing ofpubertal events usually progresses in the normalsequence.
• Non- CNS lesion:- Idiopathic- Genetics-Prolonged, untreated severe hypothyroidism
• CNS lesion:-CNS tumour- CNS irradiation- hydrocephalus, cysts, trauma, CNS inflammatory disease,
Gonadotropin-dependent precocious puberty
condition occurs at least 5- to 10-fold more frequently in girls than in boys
Approximately 90% of sexual precocity in girls is idiopathic
75% of boys have a structural CNS abnormality
Causes of CNS lesion:
Hypothalamic hamartomas are the most commonbrain lesion causing true precocious puberty.
Hamartomas are non-malignant tumours of thetuber cinereum that consists of disorganized collection ofneurons and glias.
ectopically located neural tissue containing GnRH-secretory neurons and may function as an accessoryGnRH pulse generator
Other tumour: astrocytoma, optic and hypothalamicglioma
Causes of CNS lesion: (cont.)
Radiation therapy for leukemia or intracranialtumours irradiation is directed to thehypothalamic area or to areas of the brainanatomically distant from the hypothalamus
increases the risk of precocious puberty
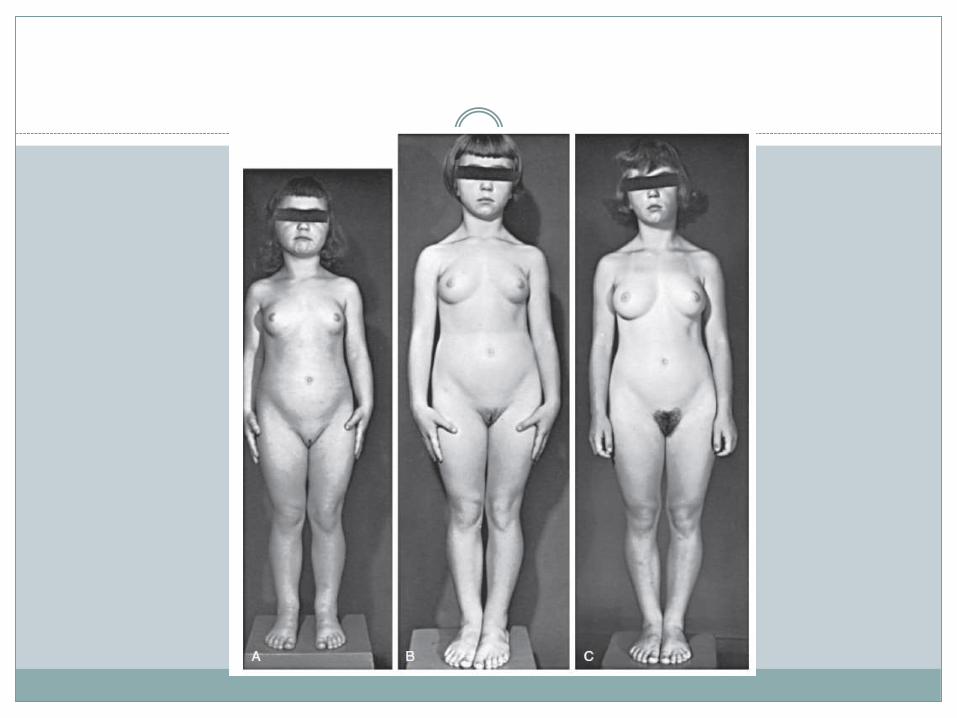
Clinical manifestations:
Begin at any age, follows the sequence observed in normalpuberty
In girls:
Breast enlargement comes first
Pubic hair may appear simultaneously but more oftenlaters
Menarche is a late event ( irregular cycle and usuallyanovulatory )
The pubertal growth spurt occurs early in female puberty
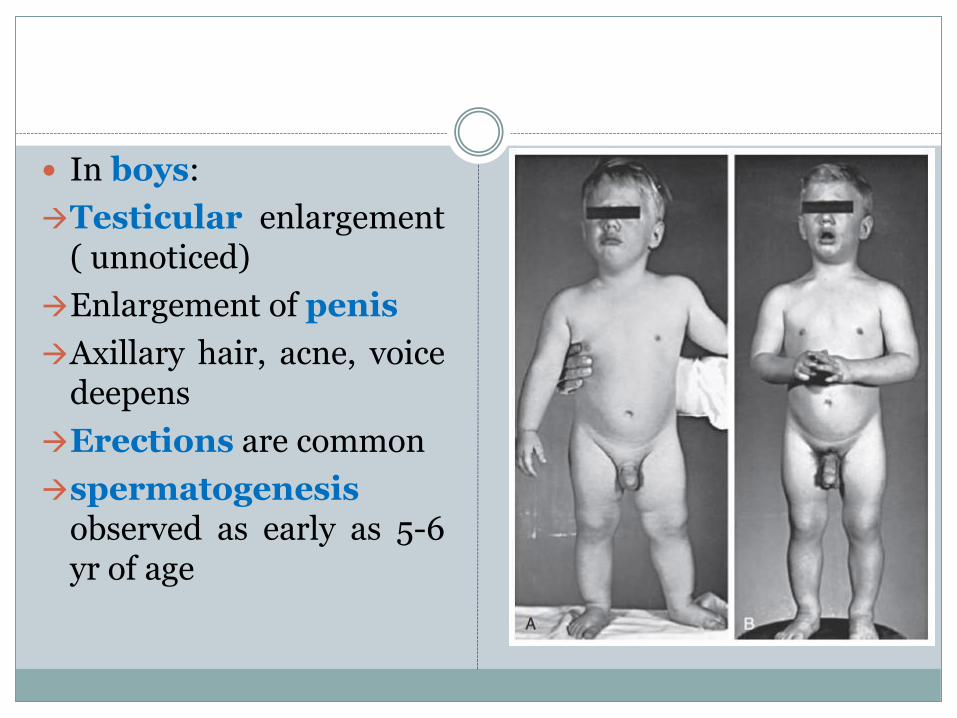
In boys:
Testicular enlargement( unnoticed)
Enlargement of penis
Axillary hair, acne, voicedeepens
Erections are common
spermatogenesisobserved as early as 5-6yr of age
In both gender:
Height, weight, and osseous maturation areadvanced
Without treatment, 30% early closure of theepiphyses > height less than the 5th percentile asadults
Emotional and mood swings are common
In intracranial lesion ( eg: hamartoma ) :
Hypothalamic signs:
diabetes insipidus
hyperthemia
unnatural crying or laughing(gelastic seizures)
cachexia
In optic glioma : proptosis
In irradiation of brain : signs of growth hormonedeficiency may present
Gonadotropin-independent precocious puberty ( GIPP)
Independent of gonadotropin secretion and noactivation of the HPG axis
aka precocious pseudopuberty
caused by excess secretion of sex hormones(estrogens or androgens) derived either from thegonads or adrenal glands or from exogenoussources
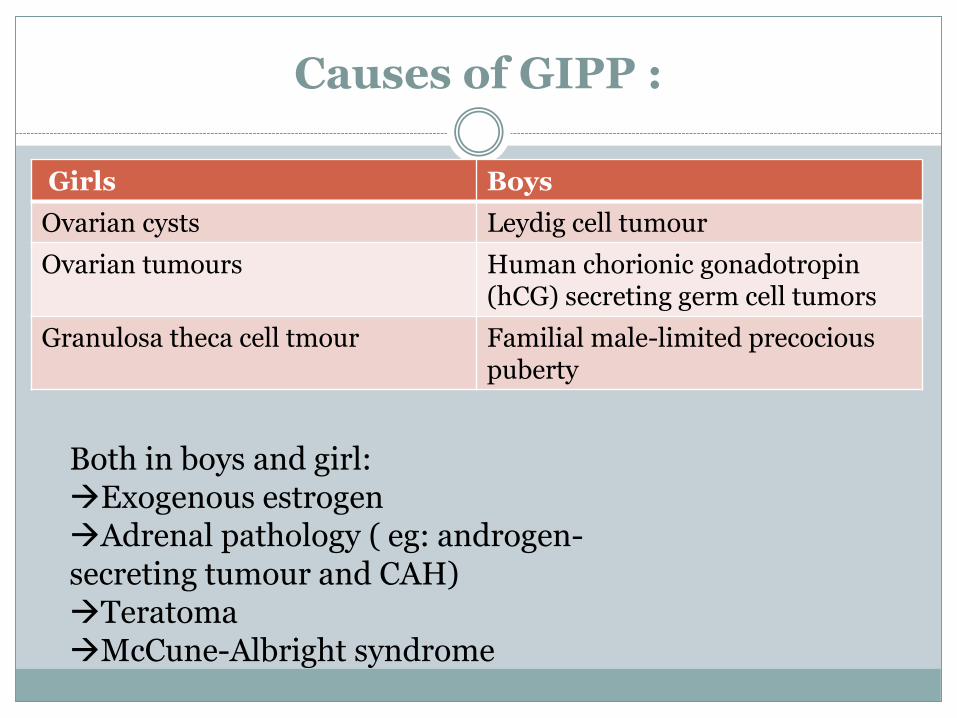
Causes of GIPP :
Girls Boys
Ovarian cysts Leydig cell tumour
Ovarian tumours Human chorionic gonadotropin(hCG) secreting germ cell tumors
Granulosa theca cell tmour Familial male-limited precocious puberty
Both in boys and girl:Exogenous estrogenAdrenal pathology ( eg: androgen-secreting tumour and CAH)TeratomaMcCune-Albright syndrome
How to approach:
Onset of age? Is the cause of precocity central or peripheral? Need to ask the
pattern of pubertal development in GDPP normal pubertaldevelopment but at an earlier age
How quickly is the puberty progressing?rapid bone maturation suggest either GDPP or GIPP
Presence of headaches or seizures ? CNS lesion Previous history of CNS disease or trauma? Are the secondary sexual characteristics virilizing or feminizing? feminizing in Sertoli cell tumorVirilization in CAH Any exposure to exogenous sex steroids?? (medicinal or cosmetic
sources) Timing of pubertal onset in his or her parents and siblings? family
history of similar symptoms?
Physical examination:
Measurements of height, weight, and calculation of height velocity (cm/yr)
Pubertal staging:
In girls :
- Breast staging, pubic hair,
In boys:
- Testicular volume? Penile size? Pubic hair?
Abdominal examination:
Palpate for mass ( in ovarian cyst and tumour)
Neurological examination (neurological deficit?)
Eye examination :
Fundoscopy :look for papilledema ( in CNS lesion)
Visual field
Look for signs of virilization in female? Ambigious genitalia? Hirsutism?
Dermatological exam to evaluate for cafe-au-lait spots( in McCune-Albrightsyndrome).
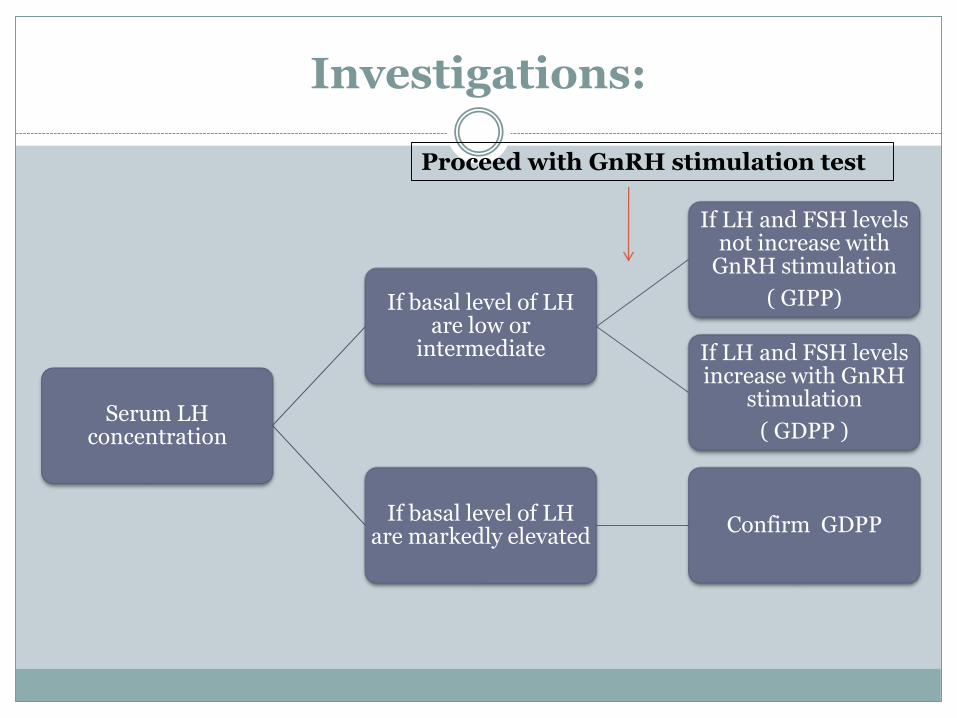
Investigations:
Serum LH concentration
If basal level of LH are low or
intermediate
If LH and FSH levels not increase with
GnRH stimulation
( GIPP)
If LH and FSH levels increase with GnRH
stimulation
( GDPP )
If basal level of LH are markedly elevated
Confirm GDPP
Proceed with GnRH stimulation test
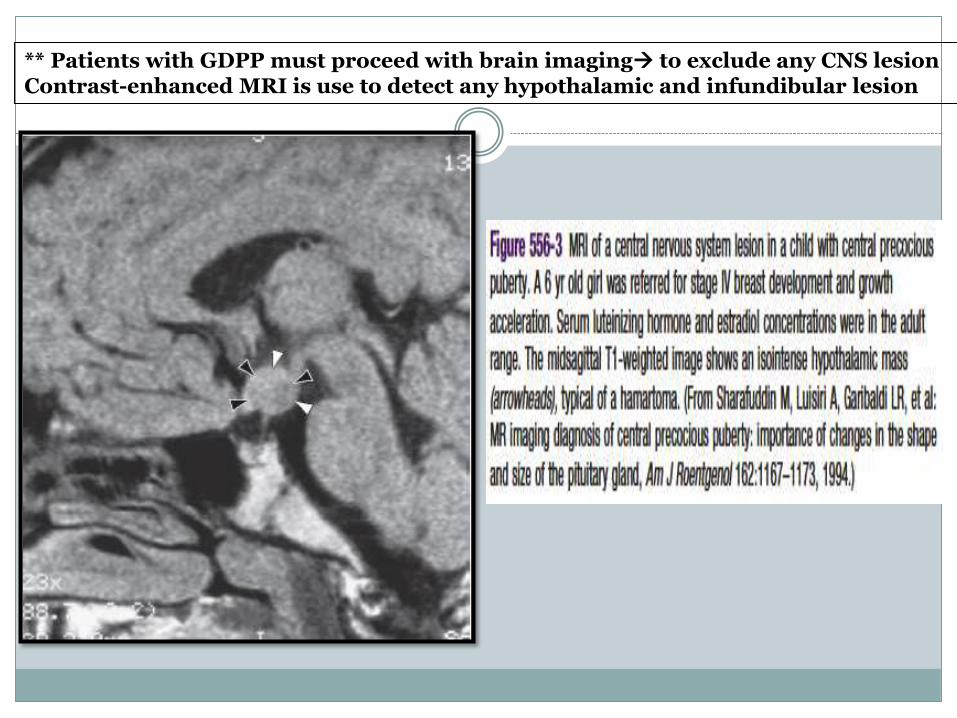
** Patients with GDPP must proceed with brain imaging to exclude any CNS lesionContrast-enhanced MRI is use to detect any hypothalamic and infundibular lesion
Other investigations:
Sex hormone
To establish degree of biochemical pubertal enhancement
Serum estradiol are low or undetectable in the early phase of sexualprecocity
Serum testosterone levels are detectable or clearly elevated
Thyroid function test
- To be done if there is any clinical evidence of hypothyroidism
Radiographic assessment of bone age:
- If the patient has a normal bone age, he or she is unlikely to haveGDPP
Several ix to identify the peripheral cause ofprecocious puberty ( GIPP ):
- Serum testosterone and estradiol- Serum LH and FSH- Renal profile (check on dehydration or electrolytes
imbalance) in aldosterone deficiency- Serum cortisol to screen for Cushing syndrome- Abdominal and pelvic ultrasound to identify
presence of ovarian cysts or tumour- Ultrasound of testes possibility of Leydig cell
tumour
Management of GDPP:
The treatment options depend upon the cause of theprecocious puberty
If (GDPP) is caused by an identifiable central nervoussystem (CNS) lesion therapy is directed toward theunderlying pathology
For most patients with GDPP primary treatmentoption gonadotropin-releasing hormone(GnRH) agonist
GnRH agonist administration slows acceleratedpuberty and improves final height
The decision of whether to treat GDPP with a GnRHagonist depends on:
- child’s age
- the rate of pubertal progression
- height velocity
- rate of bone age advancement.
Management for GIPP
GIPP does not respond to GnRH agonist therapy. Instead, treatment is directed at the underlying pathology:
Children with tumors of the testis, adrenal gland, and ovary treated by surgery.
Those with hCG-secreting tumors require some combination of surgery, radiation therapy, and chemotherapy depending upon the site and histologic type.
Management for GIPP (cont.)
A large functioning follicular cyst of the ovary Cysts develop and regress spontaneouslyconservative management
Children whose sexual precocity is caused by exposure to exogenous sex steroids exposure identified and removed
Children with identifiable defects in adrenal steroidogenesis ( CAH ) glucocorticoid therapy
Incomplete precocious puberty
Definition: isolated manifestations of precocity without development of other signs of puberty.
Inco
mp
lete Premature
thelarche
Premature pubarche
Premature menarche
Premature thelarche
Transient condition of isolated breast development that most often appears in the first 2 yr of life, often persists for 3-5 yr, and is rarely progressive
mostly idiopathic
either remit spontaneously or are very slowly progressive.
no other signs of pubertal development and their growth rate is normal.
Serum estradiol : usually normal
Mx: reassurance and monitoring regularly for any other sign of pubertal advancement
Premature pubarche
Appearance of sexual hair before the age of 8 yr in girls or 9yr in boys without other evidence of maturation
Slowly progressive condition that requires no therapy
Longitudinal observations suggest that ~50% of affectedgirls are at high risk for
Hyperandrogenism
Polycystic ovary syndrome
Metabolic syndrome
Premature menarche
Diagnosis of exclusion
Isolated vaginal bleeding in the absence of other secondary sexual characteristics
Very rare
Carefully exclude: Vulvovaginitis
Foreign body
Sexual abuse