Embed Size (px)
Citation preview

Precocious puberty
Dr. Mohit GoelJRIII23/6/14
From the radiologic pathology archives: precocious puberty: radiologic-pathologic correlation.Chung EM, Biko DM, Schroeder JW, Cube R, Conran RM.

Precocious puberty is defined as development of secondary sex characteristics before the age of 8 years in girls and 9 years in boys.
Two types: 1. central (true) precocious puberty (CPP) and 2. peripheral (pseudo-) precocious puberty (PPP) (or precocious
pseudopuberty).
CPP is caused by early activation of the hypothalamic-pituitary axis, with GnRH–stimulated gonadotropin secretion causing gonadal maturation.
Precocious puberty

In peripheral precocious puberty , serum sex steroid levels are elevated independent of gonadotropin secretion, and, because gonadotropin levels are low, the gonads do not undergo maturation.
Precocious puberty may be isosexual (involving secondary sex characteristics that are gender matched) or heterosexual (involving sex characteristics of the opposite gender).
CPP is always isosexual, whereas PPP may be isosexual or heterosexual.

CPP may be idiopathic or related to a CNS lesion such as a neoplasm, cyst, or hydrocephalus.
CPP in girls is usually idiopathic, whereas the vast majority of cases in boys are due to an intracranial lesion.
Isosexual PPP in girls is most commonly caused by an autonomously functioning ovarian cyst but may also be caused by a juvenile granulosa cell tumor (GCT) of the ovary.
Heterosexual PPP in girls (virilization) is most often related to androgen production by the adrenal glands due to a functioning ACN or congenital adrenal hyperplasia (CAH).

In boys, PPP is usually due to sex steroid hormone secretion by a sex cord–stromal tumor of the testis.
hCG secreting tumors such as hepatoblastoma, mediastinal teratoma, some testicular germ cell tumors, and suprasellar germinoma can stimulate testosterone production by Leydig cells of the testes because human chorionic gonadotropin is biologically similar to luteinizing hormone.

Imaging work-up depends on gender and the results of laboratory studies.
MR imaging of the CNS is essential in boys with CPP. For boys with PPP or unilateral testicular enlargement, testicular ultrasonography (US) is indicated.
For girls, pelvic US serves two purposes:
• evaluation for ovarian cyst or tumor and evaluation for estrogen-mediated ovarian and uterine maturation.
• US should also be used to screen for an adrenal mass
CNS imaging should be performed if CPP is suspected in girls younger than 6 years of age

Central Nervous System
CPP involves activation of the hypothalamic-pituitary-gonadal axis such that GnRH release from the hypothalamus causes gonadotropin secretion by the pituitary gland, leading to ovulation or spermatogenesis.
CPP may be further divided on the basis of etiology into idiopathic or organic types.
Organic causes have been found in 13%–42% of children with CPP and include tumors, trauma, infection, hydrocephalus, and midline anomalies.

CNS causes:
1. Hypothalamic Hamartoma2. Hypothalamic-Chiasmatic Astrocytoma3. Germ Cell Tumor4. Arachnoid Cyst5. Other Organic Causes of CPP- • Traumatic brain injury,• Empty sellaCongenital,• toxoplasmosis

Hypothalamic Hamartoma
Hypothalamic hamartoma is the lesion most commonly associated with CPP, being implicated in up to 60% of cases.
Hypothalamic hamartomas may be either • sessile (intrahypothalamic) or • pedunculated (parahypothalamic).
Imaging Features.—Sessile hypothalamic hamartomas may expand the hypothalamus. Pedunculated hypothalamic hamartomas usually arise from the floor of the hypothalamus and extend inferiorly.

Hypothalamic Hamartoma
Hypothalamic hamartoma is the lesion most commonly associated with CPP, being implicated in up to 60% of cases.
Hypothalamic hamartomas may be either • sessile (intrahypothalamic) or • pedunculated (parahypothalamic).
Imaging Features.—
Sessile hypothalamic hamartomas may expand the hypothalamus.
Pedunculated hypothalamic hamartomas usually arise from the floor of the hypothalamus and extend inferiorly.

They are typically isointense relative to gray matter with T1- and T2-weighted sequences, although they may be mildly hyper- or hypointense relative to gray matter with T2-weighted sequences



Hypothalamic-Chiasmatic Astrocytoma
Hypothalamic-chiasmatic astrocytomas represent up to 5% of all brain tumors in children, but they occur in 15%–20% of children with NF-1.
Imaging Features.—
• Enlargement or kinking of the affected optic nerve and chiasm are common.
• The lesion is classically T1 isointense and T2 hyperintense with homogeneous enhancement.
• Although cystic components may be seen, they are less common in patients with NF-1.




Germ Cell Tumor
Germ cell tumors of the CNS arise in the pineal region, sellar-suprasellar region, basal ganglia.
Imaging Features.—• The imaging characteristics of germ cell tumor are highly
variable, including T1 and T2 signal heterogeneity as well as a variable degree of contrast material enhancement of its solid elements.
• Germinomas may diffusely enhance.
• Heterogeneity is seen in nongerminomatous germ cell tumors and may be secondary to intratumoral hemorrhage.
• Cysts may be seen in both germinomas and nongerminomatous germ cell tumors.

• Synchronous tumors in the pineal and suprasellar regions may occur. • Dissemination is not uncommon in germ cell tumors, and screening of the
entire neuroaxis should be performed.



Arachnoid Cyst
Arachnoid cysts account for roughly 1% of intracranial masses, with nearly 10% occurring in the sellar-suprasellar region.
Imaging Features.—
• Arachnoid cysts are smooth, well-circumscribed lesions that classically follow the attenuation and signal characteristics of cerebrospinal fluid unless complicated by hemorrhage.
• There is no associated enhancement, although there may be associated mass effect or remodeling of the adjacent calvaria.




Adrenal Gland
The adrenal gland is made up of two distinct endocrine glands: 1. the medulla, which produces catecholamines, and 2. the cortex, which produces steroid hormones.
Cortex: G- Aldosterone (Mineralocorticoid)F- Cortisol (Glucocorticoid)R- Sex steroids (Androgen)
Medulla: Catecolamines (Norepinephrine, epinephrine, Dopamine)

The neonatal adrenal gland is large due to the presence of persistent fetal cortex, which rapidly involutes in the first few months of life.
The normal large glands are easily visualized at US in young infants.
A central echogenic stripe that representsthe medulla and prominent central veins is noted.
This is surrounded by a thicker hypoechoic region with a smooth or slightly undulating surface representing the fetal and definitive adrenal cortex.
Once involution of the fetal cortex has occurred, the normal adrenal gland is seen only at CT or MR imaging, and each limb is no greater in width than the adjacent diaphragmatic crus.

Adrenal Cortical Neoplasm
Although rare, pediatric adrenal tumors most commonly manifest with signs and symptoms of virilization.
Unlike similar tumors in adults, most pediatric ACNs (85%) are hyperfunctioning.
Overproduction of androgens may be accompanied by hypersecretion of cortisol or aldosterone.
ACNs are rarely feminizing.

Unlike with the adult tumors, which can be readily differentiated histologically into benign adenomas and malignant carcinomas, histologic classification of pediatric ACNs is not predictive of biologic behavior.
The malignant potential of a particular tumor is unknown, and the term adrenal cortical neoplasm is preferred.
ACNs are rare in children and account for only 0.2%–0.5% of pediatric cancers.
A bimodal age distribution - younger than 5 years of age. The peak age at diagnosis in the adolescent group is 10–16 years

Imaging Features.—In adults, benign and malignant ACNs are differentiated on the basis of findings of intracytoplasmic lipid and rapid contrast material washout, which are seen in adenomas but not in carcinomas.
The predictive value of these findings has not been studied in children, and imaging diagnosis is not as important in children as in adults.
Because the vast majority of childhood ACNs are functional, the diagnosis is known on the basis of laboratory findings.
Thus, the role of imaging in children with ACN is not diagnosis, but rather localization of the primary tumor and any metastases and determination of the local extent of the primary tumor for surgical planning.

Smaller lesions are homogeneous, whereas larger lesions appear heterogeneous due to central necrosis, hemorrhage, and calcification.
Prominent radiating fibrous bands may create a nodular appearance or the appearance of a characteristic stellate scar.

At US, smaller lesions are generally homogeneously hypo- or hyperechoic.
Larger lesions may have a more heterogeneous nodular appearance or may contain central or diffuse hypoechoic areas corresponding to necrosis.
The mass may be surrounded by a hyperechoic, capsule-like rim. Use of color Doppler imaging is helpful in evaluating for caval extension of tumor

At CT, large ACNs show heterogeneous, predominantly peripheral enhancement.
The tumor may be surrounded by a thick, capsule-like rim that enhances. Fine or coarse calcification is seen at CT in about 30% of cases

MR imaging demonstrates the mass as iso- to slightly hypointense on T1WI and hyperintense on T2WI relative to the liver.
Functioning ACNs frequently show uniform signal loss at chemical shift imaging due to intracytoplasmic lipid.
(FDG) PET/CT is sensitive for the detection of ACNs due to their metabolic activity.
The main role of FDG PET in the evaluation of patients with ACN is detection of distant metastases.











Differential Diagnosis.—
In the presence of an endocrinopathy, there is no differential diagnosis.
Without these symptoms, adrenal medullary tumors should be considered first. Neuroblastoma is far more common than ACN.
The typical growth pattern of neuroblastoma is different from that of ACN in that neuroblastoma tends to surround rather than invade vessels, cross the midline, and extend into neural foramina.

Pheochromocytoma is another tumor of the adrenal medulla that may occur in older children.
Medullary tumors can be distinguished from ACN on the basis of laboratory findings of elevated catecholamine levels in the serum and urine and focal radiopharmaceutical uptake at scanning with metaiodobenzoguanidine.

Congenital Adrenal Hyperplasia
CAH, or adrenogenital syndrome, most often manifests in the perinatal period with ambiguous genitalia in girls or salt wasting in boys, but some patients may have delayed presentation with virilization at puberty.
Patients with Beckwith-Wiedemann syndrome are at increased risk for ACN and may also have cortical hyperplasia, with enlarged glands with a nodular or “cerebriform” surface due to adrenal cytomegaly involving most of the cells in the fetal cortex.




Imaging Features.—
CAH causes bilateral adrenal gland enlargement, which may be asymmetric.
An adrenal limb thicker than 4 mm is considered enlarged even in the neonatal period.
Adrenal gland enlargement alone is not sensitive or specific for CAH.
A normal-sized adrenal gland does not exclude the diagnosis of CAH, and some healthy babies have adrenal glands in the size range typical of CAH.



Testicular adrenal rest tumors in adrenogenital syndrome are very common in boys with CAH.
These tumors are small, generally multiple, and often bilateral.
The involved testis may be enlarged, but its contour is not distorted. The masses are eccentric and commonly surround the mediastinum testis.

Their appearance at US is variable and depends on size.
Smaller lesions (<2 cm) appear hypoechoic compared with the adjacent testicle, whereas larger lesions appear hyperechoic with posterior acoustic shadowing.
At color Doppler imaging, vessels may be seen coursing through the lesion without being deviated by it.

Female Reproductive Organs
The normal neonatal uterus is enlarged due to the influence of maternal hormones. The cervix is larger than the fundus, and the uterus is spade shaped.
Endometrium is readily visualized as a thin echogenic line in the uterine corpus.

After the first few months of life, the prepubertal uterus is straight and tubular in configuration, with the cervix the same size as or slightly larger than the fundus .

With the onset of puberty, the influence of estrogen causes enlargement of the uterine fundus more than of the cervix, the uterus assumes the pear shape
US image obtained in another healthy prepubertal girl shows small follicles within the ovaries

Ovarian Cyst
The most common cause of PPP in girls is an autonomously functioning follicular cyst.
Patients generally present with vaginal bleeding and breast development. Vaginal bleeding is due to withdrawal of estrogen stimulation when the cyst ruptures.
Imaging Features-The finding of an ovarian cyst 9 mm or larger in a girl with precocious puberty is strongly suggestive of PPP with autonomous ovarian estrogen secretion.
Uncomplicated follicular cysts are anechoic or hypoechoic unilocular cysts. Can be complicated by hemorrhage.
In PPP due to autonomous follicular cyst, the contralateral ovary is within normal size limits, but the uterus has a pubertal morphology and size due to estrogen stimulation. In contrast, girls with CPP often have bilateral small (<9-mm) cysts

Juvenile GCT of the Ovary
Juvenile GCT is a malignant primary ovarian neoplasm of children and young adults that is most often characterized by clinical manifestations of steroid hormone overproduction. The lesion is classified as a sex cord–stromal tumor.
Imaging Features.—As an ovarian tumor, juvenile GCT is usually initially identified at US, with demonstration of a large mixed cystic and solid mass.

US also shows uterine enlargement and pubertal morphology due to estrogen effect

At CT, the solid component of juvenile GCT may show iso- to hyperattenuation as well as contrast enhancement.
Hyperattenuating hemorrhage within cystic components of the mass is a characteristic finding. Calcifications are not a feature of juvenile GCT.

At MR imaging, the solid portion of the tumor demonstrates intermediate signal intensity with multiple hyperintense cystic spaces on T2-weighted images, creating a spongelike appearance


Male Reproductive Organs
Sex cord–stromal tumors of the testis are active endocrine tumors that secrete testosterone or estrogen, leading to precocious puberty in 10% of children.
This class of tumors includes Leydig cell, Sertoli cell, juvenile granulosa cell, and undifferentiated tumors.
Leydig Cell Tumors
Patients less than 10 years of age.
Imaging Features.—At US, Leydig cell tumors are usually homogeneous and hypoechoic but less commonly appear echogenic

At Doppler evaluation, Leydig cell tumors typically have prominent circumferential blood flow with a lack of internal vascularity.
At MR imaging- isointense on T1-weighted images and - hypointense on T2-weighted images compared with
surrounding testicle. - capsular high signal intensity on T2-weighted images- show marked homogeneous enhancement

Sertoli Cell Tumors
Although most Sertoli cell tumors occur under the age of 40 years, approximately 30% occur in children.
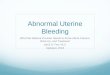
The most common histologic variant in children and adolescents is the large-cell calcifying subtype, which secretes testosterone and causes PPP in young boys.
Imaging Features.—At US, the appearance of Sertoli cell tumor is variable. The tumor may have the unusual appearance of an enlarged testicle with inhomogeneous increased echogenicity.
Sertoli cell tumor may also appear as multiple homogeneous nodules with surrounding thin hypoechoic rims
The large-cell calcifying subtype appears as an echogenic nodule with acoustic shadowing at gray-scale US

Conclusions
Sexual precocity has a wide range of causes involving multiple endocrine organs, and imaging plays an important role in the evaluation and diagnosis of children with symptoms of early sexual maturation.
CPP is usually idiopathic in girls but is most commonly related to a CNS lesion in boys, and brain MR imaging is essential for boys.
PPP may be caused by gonadal lesions or adrenal abnormalities, which are best initially evaluated with US.
Early diagnosis and treatment reverse the endocrine disorder with its physical changes, preserve adult height potential, and may be potentially life saving.

THANK YOU