Embed Size (px)
DESCRIPTION
Managing the Patient With MDS and Iron Overload. Aristoteles Giagounidis, MD, PhD Associate Professor of Medicine Head, Hematology/Oncology Clinical Research Unit St. Johannes Hospital Duisburg, Germany. Case History. 68-year-old financial advisor. - PowerPoint PPT Presentation
Citation preview
Managing the Patient With MDS and Iron Overload
Aristoteles Giagounidis, MD, PhDAssociate Professor of Medicine
Head, Hematology/Oncology Clinical Research Unit St. Johannes Hospital
Duisburg, Germany
Case History
• 68-year-old financial advisor
CABG = coronary artery bypass graft; NIDDM = noninsulin-dependent diabetes mellitus; PRBC = packed red blood cell
Past medical history
• NIDDM, coronary artery disease, CABG x 3 in 2001
• Developed macrocytic anemia in Jan 2003 (MCV 109 fl)
Transfusion frequency
• Initial transfusion frequency: 2 PRBC/month
• Over next 2 years: increasing transfusion dependence, reaching 3-4 U/wk in 2005

Clinical Examination
History and physical exam
• Reduced overall condition, peripheral edemas, dyspneic at little exertion, depressed
• Pulse 112/min, RR: 125/65 mm Hg
• No fever present
• No splenomegaly, hepatomegaly, or lymphadenopathy present
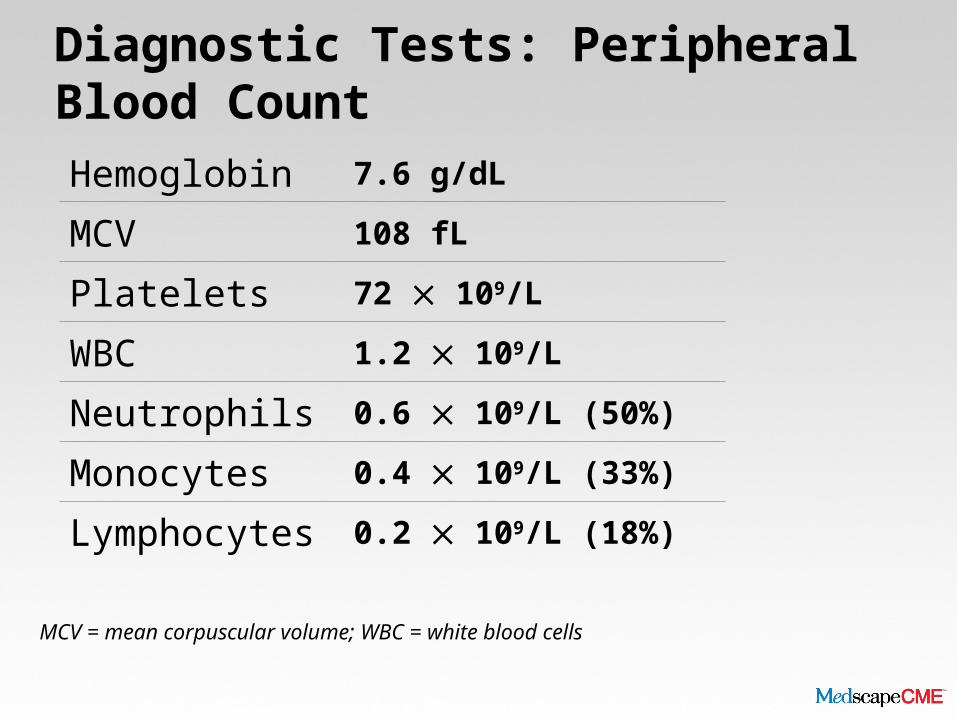
Diagnostic Tests: Peripheral Blood Count
MCV = mean corpuscular volume; WBC = white blood cells
Hemoglobin 7.6 g/dL
MCV 108 fL
Platelets 72 109/L
WBC 1.2 109/L
Neutrophils 0.6 109/L (50%)
Monocytes 0.4 109/L (33%)
Lymphocytes 0.2 109/L (18%)
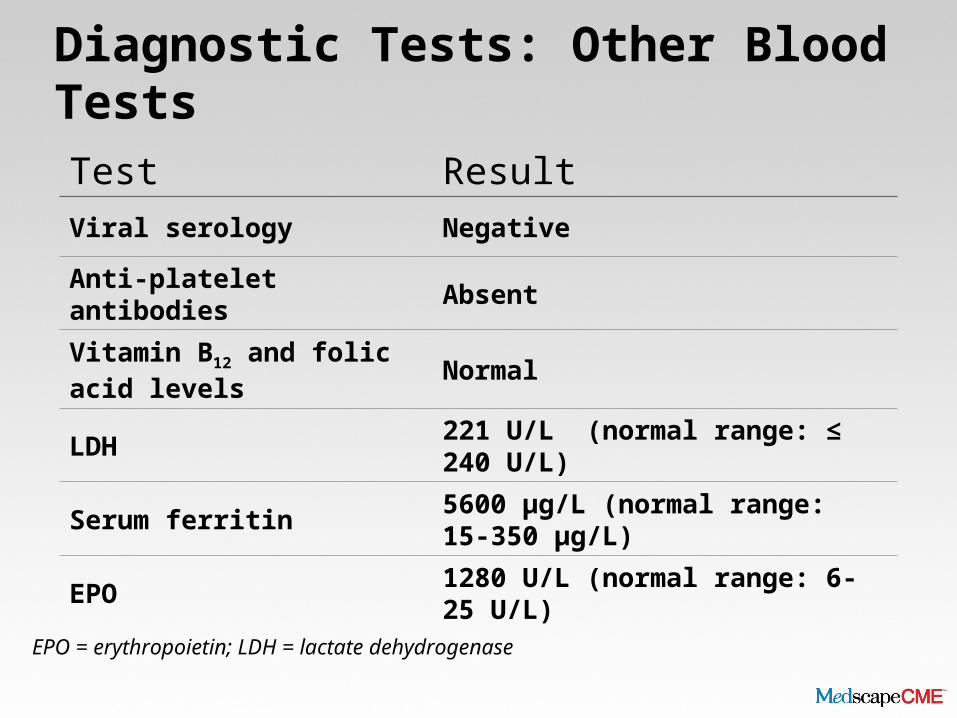
Diagnostic Tests: Other Blood Tests
EPO = erythropoietin; LDH = lactate dehydrogenase
Test ResultViral serology Negative
Anti-platelet antibodies Absent
Vitamin B12 and folic acid levels Normal
LDH 221 U/L (normal range: ≤ 240 U/L)
Serum ferritin 5600 µg/L (normal range: 15-350 µg/L)
EPO 1280 U/L (normal range: 6-25 U/L)
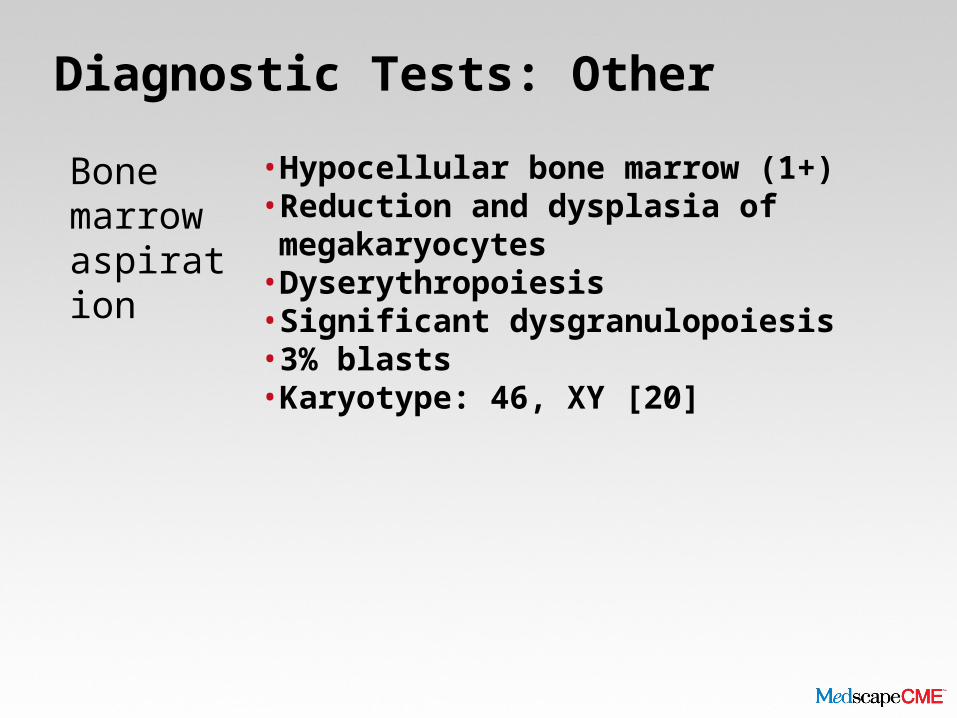
Diagnostic Tests: Other
Bone marrow aspiration
• Hypocellular bone marrow (1+)• Reduction and dysplasia of megakaryocytes• Dyserythropoiesis • Significant dysgranulopoiesis• 3% blasts• Karyotype: 46, XY [20]
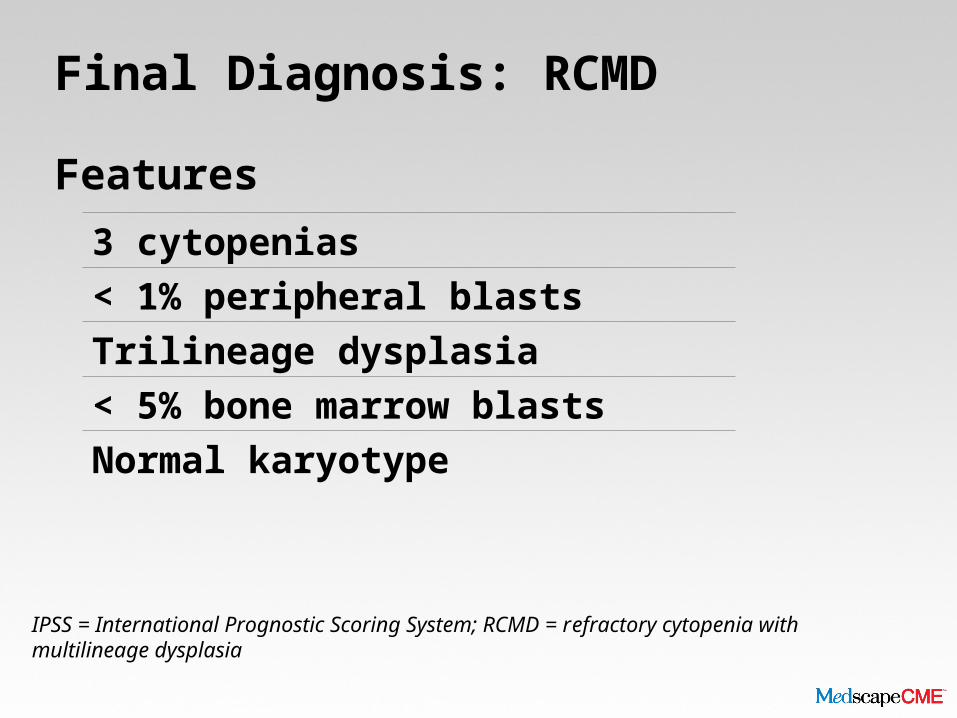
Final Diagnosis: RCMD
Features
IPSS = International Prognostic Scoring System; RCMD = refractory cytopenia with multilineage dysplasia
3 cytopenias< 1% peripheral blastsTrilineage dysplasia< 5% bone marrow blastsNormal karyotype
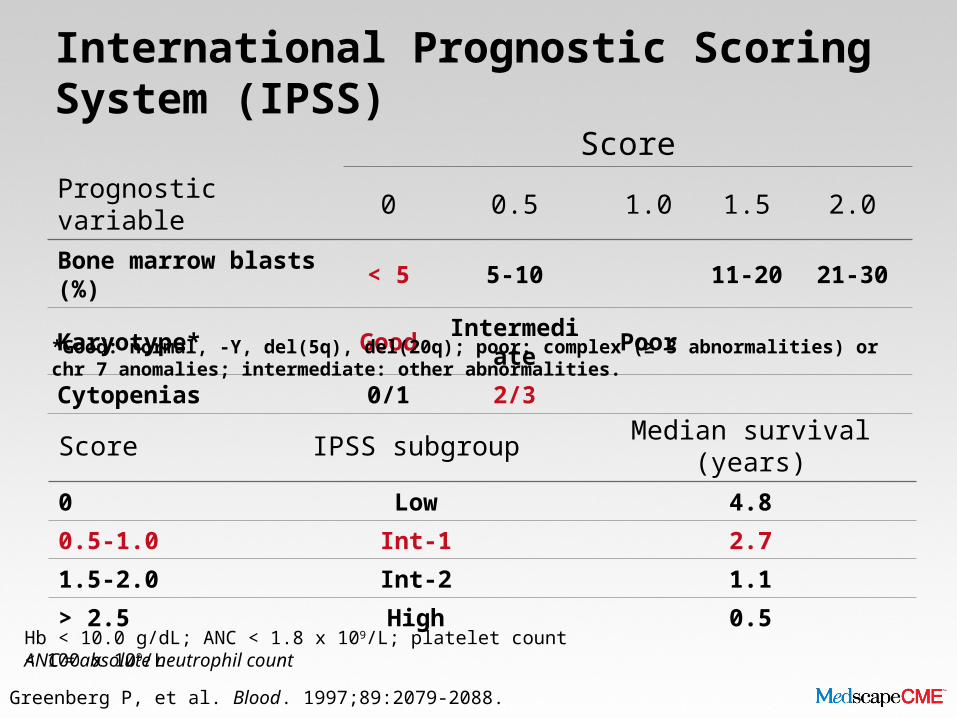
International Prognostic Scoring System (IPSS)
ScorePrognostic variable 0 0.5 1.0 1.5 2.0Bone marrow blasts (%) < 5 5-10 11-20 21-30
Karyotype* Good Intermediate Poor
Cytopenias 0/1 2/3
Score IPSS subgroup Median survival (years)0 Low 4.8
0.5-1.0 Int-1 2.7
1.5-2.0 Int-2 1.1
> 2.5 High 0.5
Greenberg P, et al. Blood. 1997;89:2079-2088.
*Good: normal, -Y, del(5q), del(20q); poor: complex (≥ 3 abnormalities) or chr 7 anomalies; intermediate: other abnormalities.
Hb < 10.0 g/dL; ANC < 1.8 x 109/L; platelet count < 100 x 109/LANC = absolute neutrophil count
Hematologist: Patient Prognosis
• Patient was told by general practitioner that he should be evaluated at a specialized hematology center
• Comments from hematologist:• No sensible treatment option at this stage for this lower-risk patient• Patient should remain on transfusions only• Iron chelation would not be indicated (probably due to short life
expectancy)
• Patient was severely depressed
Initial Treatment
• Patient had a hypoplastic bone marrow with normal karyotype• Was treated with antithymocyte globulin and cyclosporine A within a
clinical trial• Became transfusion independent within 3 months of therapy

Patient Developed Iron Overload
Overall transfusion load > 100 U without iron chelation
Cardiac EF 33% by echocardiography
ALT/AST (LFTs) 5X ULN
Direct bilirubin 1.4 mg/dL
• After 4 months of treatment, iron chelation was started after reduction of both corticosteroids and cyclosporine A
ALT/AST = alanine transaminase/aspartate transaminase; EF = ejection fraction; ULN = upper limit of normal
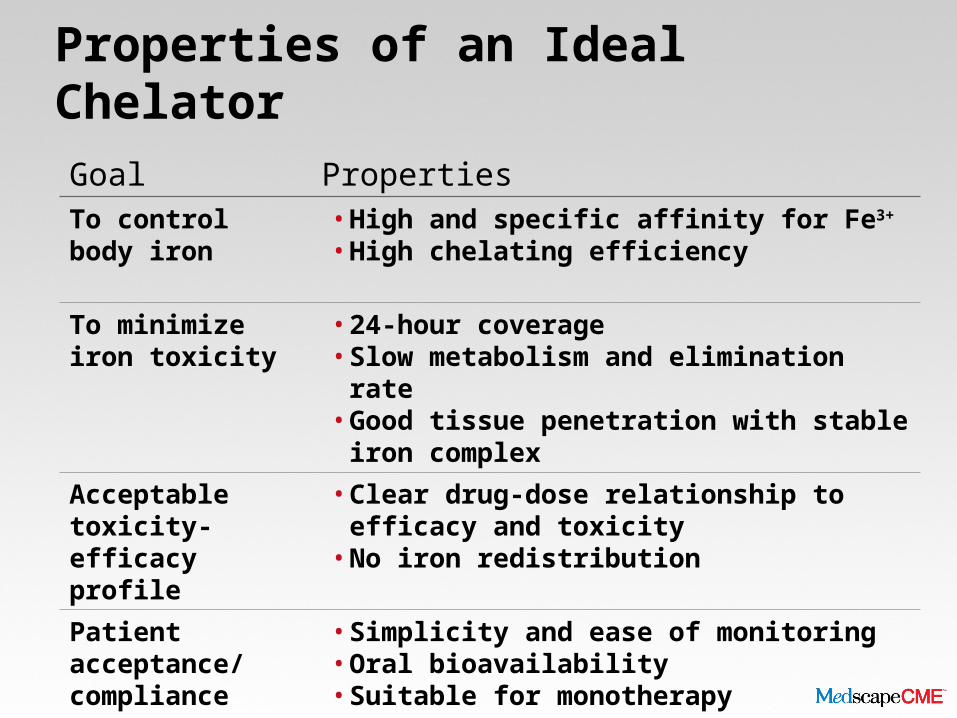
Properties of an Ideal Chelator
Goal PropertiesTo control body iron • High and specific affinity for Fe3+
• High chelating efficiency
To minimize iron toxicity
• 24-hour coverage• Slow metabolism and elimination rate• Good tissue penetration with stable iron complex
Acceptable toxicity-efficacy profile
• Clear drug-dose relationship to efficacy and toxicity• No iron redistribution
Patient acceptance/compliance
• Simplicity and ease of monitoring• Oral bioavailability• Suitable for monotherapy

Overview of Deferasirox
Property DeferasiroxUsual dose 20-30 mg/kg/d (to maximum of 40 mg/kg/d)
Route Oralonce daily
Half-life 8-16 h
Excretion Fecal
Adverse effects GI disturbances, rash, mild nonprogressive creatinine increase, ophthalmologic, auditory, elevated liver enzymes
Status Licensed
Approved indications Treatment of chronic iron overload due to frequent blood transfusions
Deferasirox Summary of Product Characteristics, 09/12/2009.
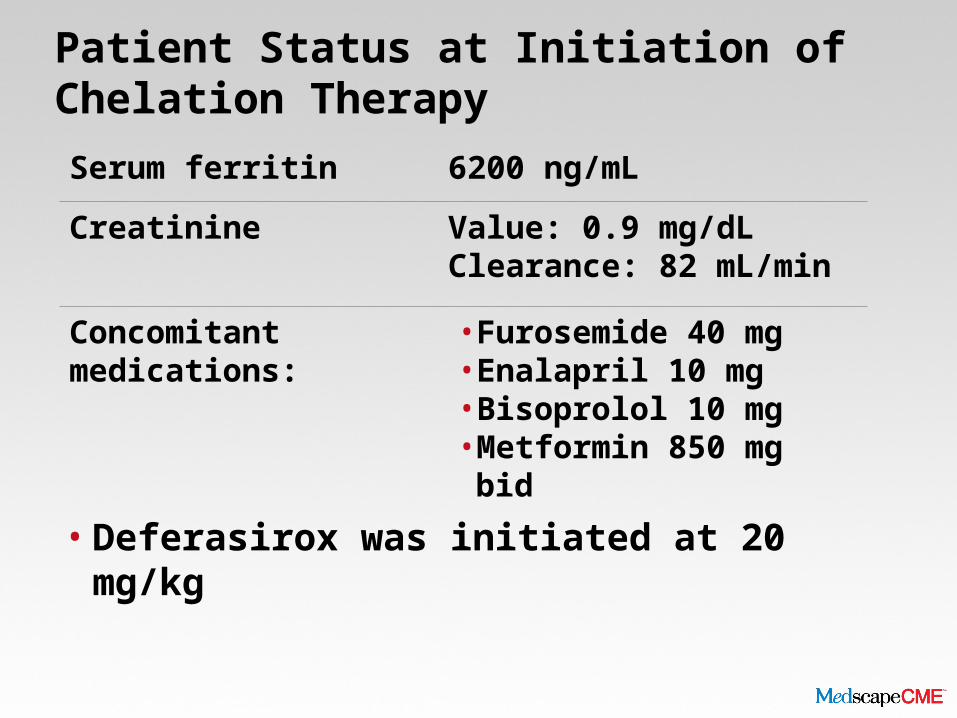
Patient Status at Initiation of Chelation Therapy
• Deferasirox was initiated at 20 mg/kg
Serum ferritin 6200 ng/mL
Creatinine Value: 0.9 mg/dL Clearance: 82 mL/min
Concomitant medications: • Furosemide 40 mg• Enalapril 10 mg• Bisoprolol 10 mg•Metformin 850 mg bid

Overview: Outcomes With Deferasirox
Transfusion burden No change
Serum ferritin Decreased from 6200 ng/mL to 2100 ng/mL
Creatinine Increased from 0.9 mg/dLto 1.3 mg/dL
Blood values • Platelets slightly increased to 95,000/µL•WBC slightly increased to
1700/µL
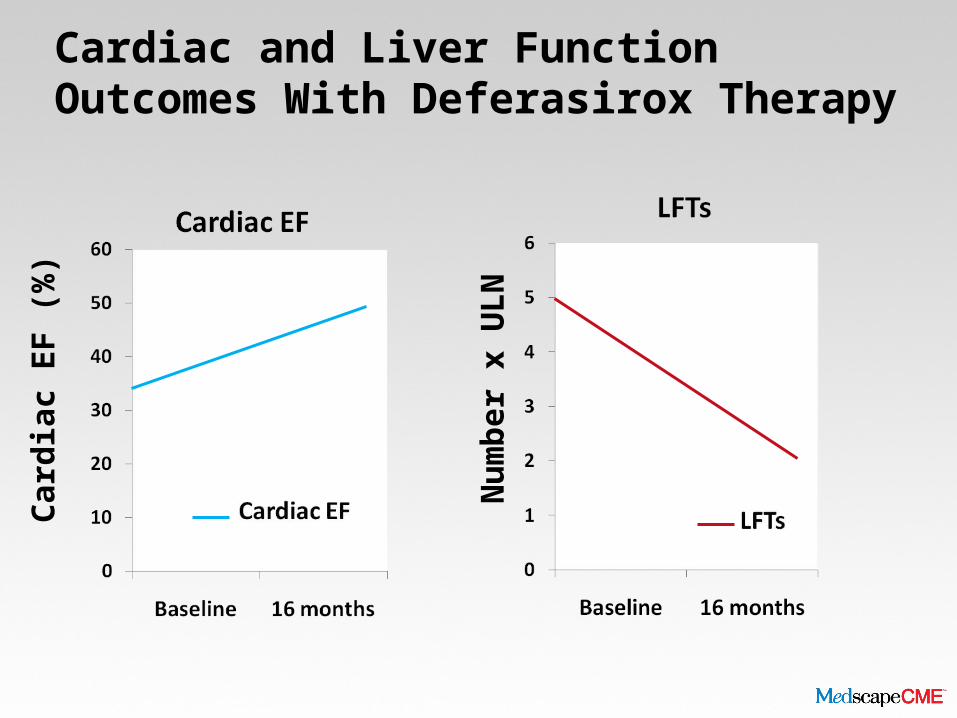
Cardiac and Liver Function Outcomes With Deferasirox Therapy
Num
ber x
ULN
Card
iac
EF (%
)
Disease Progression
• In 2007, the patient progressed to RAEB-II• Treatment with AZA was begun• Result: SD after 6 courses of therapy
• Deferasirox discontinued at this point due to short predicted OS
• AZA continued for another 7 courses• Patient ultimately developed frank AML and passed
away quickly
AML = acute myeloid leukemia; AZA = azacitadine; OS = overall survival; RAEB = refractory anemia with excess blasts; SD = stable disease
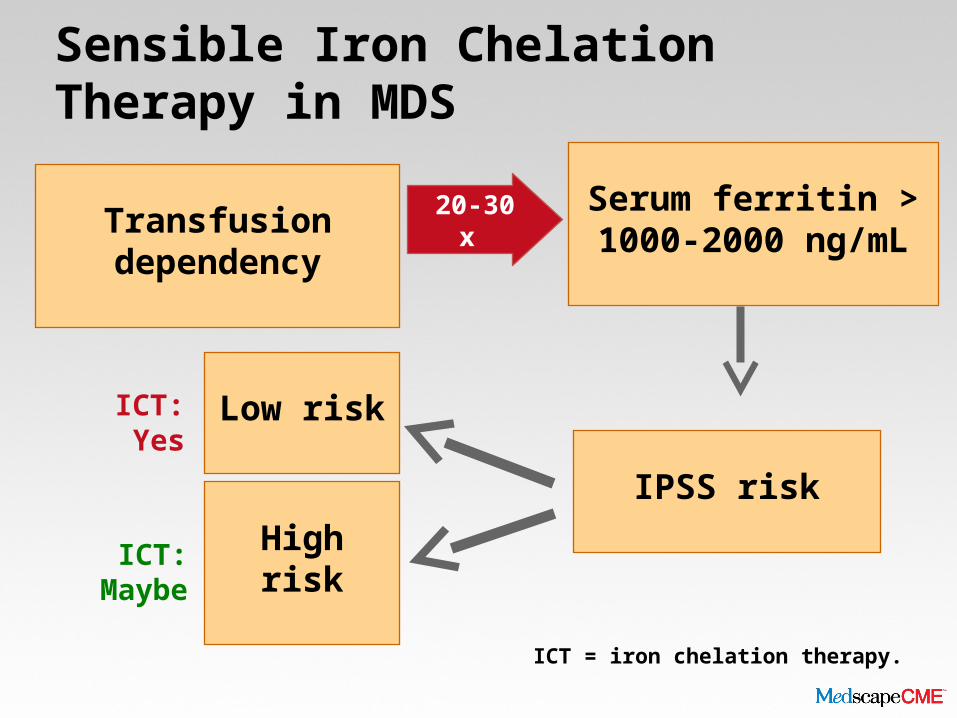
Serum ferritin > 1000-2000 ng/mLTransfusion
dependency 20-30 x
IPSS risk
Low risk
High risk
ICT: Yes
ICT: Maybe
Sensible Iron Chelation Therapy in MDS
ICT = iron chelation therapy.

Sensible Iron Chelation Therapy in MDS (cont)
High-risk IPSS
Palliative? Curative? Time gain?
Consider ICT in selected cases
Consider ICT in selected cases
No ICT
Conclusions: Lessons Learned
• Identifying candidates for ICT depends on risk scoring and goals of MDS treatment• Transfusion-dependent lower-risk patients with serum ferritin
>1000-2000 ng/mL are appropriate candidates
• Deferasirox therapy reduced serum ferritin, increased cardiac EF, and decreased LFTs in this lower-risk patient
• After progression to higher-risk disease:• Consider continuing ICT in patients whose treatment has potential
for cure and/or lengthened survival • Discontinue ICT in patients with higher-risk MDS whose treatment is
palliative