Embed Size (px)
Citation preview
DR. M.D. MAINA
MB.chB, Mmed(Int Medicine), MSc(Haem) London
IRON METABOLISM AND MANAGEMENT OF IRON OVERLOAD
DISCLOSURES
• The speaker has received logistical support from Novartis.
• Please note that my views and opinions do not necessarily reflect those of Novartis. Novartis only recommends the use of its products in accordance with the locally approved package insert.
INTRODUCTION
• Iron is a key element in all living organisms• Neither bacteria nor nucleated cells can
proliferate with an insufficient Iron supply• Much of the Iron in the human body is contained
in circulating red cells which contain 1mg of Iron per 1ml of packed cells.
• Smaller amounts of it are present in myoglobin and other enzymes.
• Iron is store in the form of ferritin or haemosiderin.
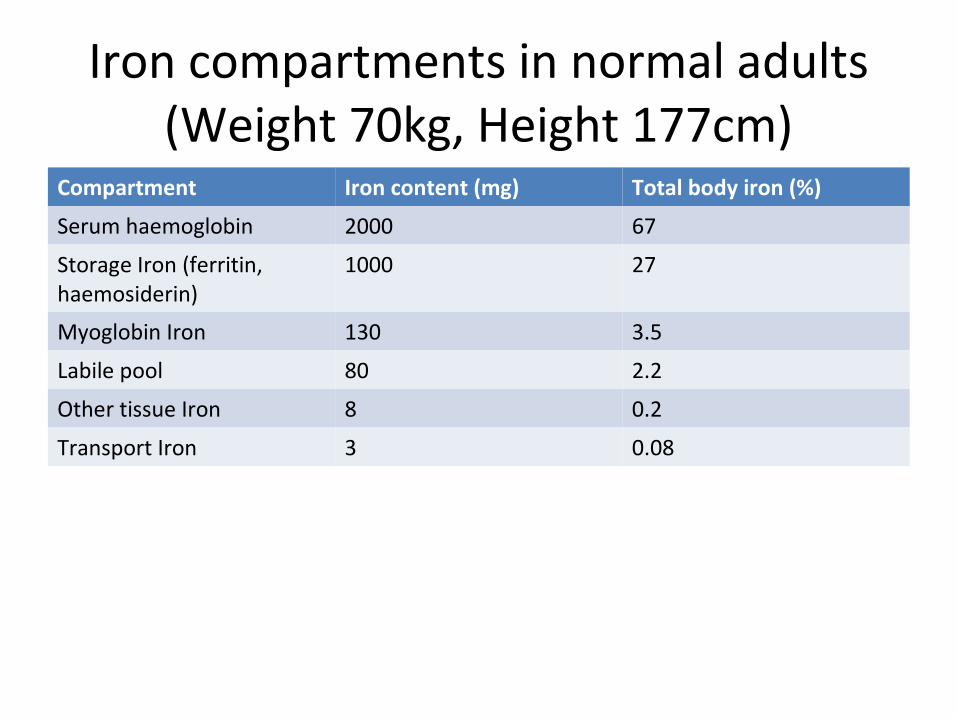
Iron compartments in normal adults (Weight 70kg, Height 177cm)
Compartment Iron content (mg) Total body iron (%)
Serum haemoglobin 2000 67
Storage Iron (ferritin, haemosiderin)
1000 27
Myoglobin Iron 130 3.5
Labile pool 80 2.2
Other tissue Iron 8 0.2
Transport Iron 3 0.08
Storage Compartment
• Iron is stored in either ferritin (water soluble) or haemosiderin (water insoluble.)
• Serum ferritin concentration usually correlates roughly with total body Iron stores.
• Serum ferritin levels are important in the diagnosis of Iron metabolism disorders i.e. Iron deficiency and Iron overload.
• Haemosiderin is found predominantly in macrophages.• Under pathological conditions it may accumulate in
large quantities in almost every tissue in the body.
Labile Iron Pool
• Iron leaves the plasma and enters the interstitial and intracellular fluid compartments before it is incorporated into heme or storage compounds.
• Labile pool Iron is considered equivalent to chelatable Iron pool.
Iron Metabolism• Iron haemostasis in humans is maintained by strict regulation
according to body needs.• Approximately 1mg (10% of total dietary Iron) is absorbed daily
predominantly from the duodenum.• Fe3+ is reduced to Fe2+ that is transported into the cell by divalent
metal transporter (DMT-1) located in the apical brush border.• The Iron is then transported across the basolateral membrane by
ferroportin with the aid of ferroxidase hephaestin.• In circulation Fe2+ is bound to transferrin and is transported to the
liver and bone marrow.• In the liver transferrin receptors 1 and 2 mediate the endocytosis
of Iron which is then stored as ferritin and released by a ferroportin mediated mechanism when body needs increase.
• The presence of ferroportin on the cell membrane is regulated by hepcidin.
• Hepcidin is a 25-amino acid peptide produced in the liver.
• It acts by binding ferroportin transporter triggering its degradation.
• This reduces Iron absorption in the gut.• Low hepcidin levels increase Iron absorption
by increasing ferroportin levels.
Iron overload - Causes• Increased Absorption• Hereditary haemochromatosis. It results from mutation of HFE• gene is associated allel HLA-A3 and HLA-B8.This leads in decreace • In hepcidin levels and increases iron absorption.• Infective erythropoesis i.e. thallassemia intermedia, sideroblastic anaemia• Chronic liver diseaseIncreased Iron Intake• African siderosis (dietary and genetic)Repeated red cell transfusion• Transfusional siderosis i.e. Aplastic anaemia, sickle cell disease, sideroblastic
anaemia, red cell aplasia, myelodysplasia, primary myelofibrosis and thallassemia major
SICKLE CELL DISEASE• Sporadic blood transfusion• primary prevention of stroke in patients with abnormal transcranial Doppler
• velocities• prevention recurrence of stroke• short term transfusion programs in pregnancy
Mechanism of organ damage in Iron overload
• Saturation of transferrin by excess circulating Iron results in increased non-transferrin bound Iron (NTBI) and labile plasma iron (LPI.)
• NTBI and LPI tend to enter tissues more readily and form reactive oxygen species (ROS.)
• Excessive Iron deposits in hepatic parenchyma, endocrine organs and cardiac myocytes all leading to end organ damage by ROS-mediated lipid peroxidation.
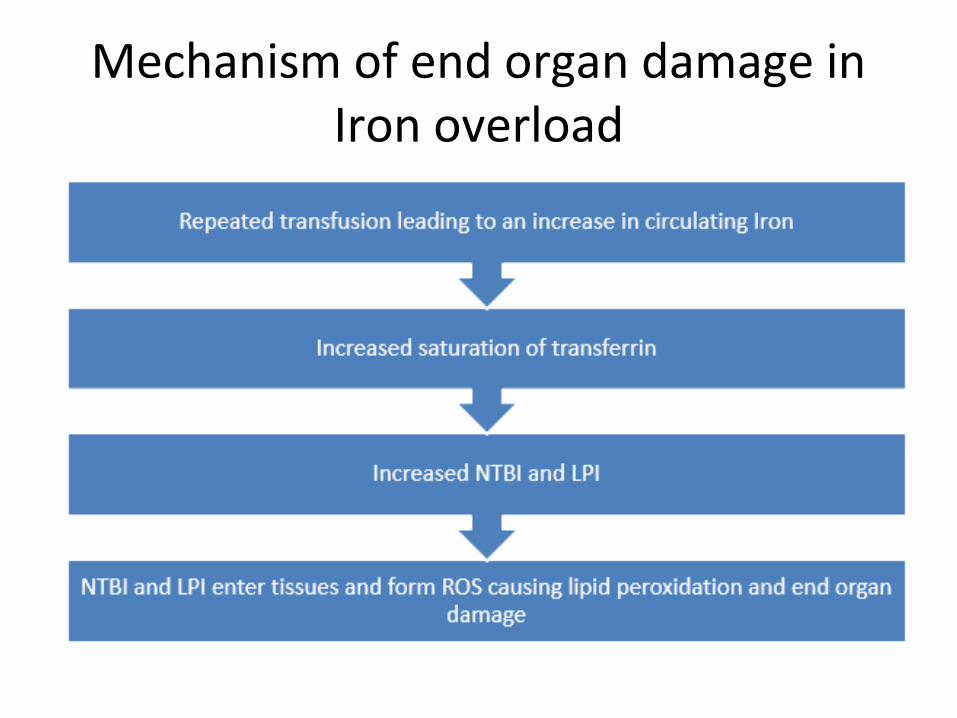
Mechanism of end organ damage in Iron overload
Assessment of Iron overload
Serum ferritin• Serum ferritin correlates roughly with total
body Iron stores, and can be used in assessing Iron overload.
• It is however increased in inflammatory conditions.
• Serum ferritin is not an accurate indicator of hepatic Iron concentration (HIC.)
Liver biopsy• This is the gold standard. It gives an accurate
estimation of Iron overload.• Normal HIC is 0.4 - 2.2mg per gram of liver dry weight.• HIC of more than 15mg/g liver dry weight is
consistently associated with liver fibrosis.
NB: Liver biopsy is an invasive procedure, has risks of complication (<1%), associated with sampling errors and lacks reproducibility.
T2*MRI
• It is a well validated predictor of HIC and cardiac complications from Iron overload.
• Increasing Iron content in the liver and the heart reduces relaxation times as measured by T2*.
Cardiac values < 20ms correlate with:• a decline in left ventricular ejection values• an increase in cardiac arrhythmias• a need for cardiac medication
Therapy of transfusional Iron overload
Pharmacological therapy• Chelation therapy to prevent or treat Iron overload in recurrent
transfusion• Chelation works by targeting unbound Iron, including NTBI and LPI that
causes tissue injury.
Indication of chelation therapy• Elevated HIC > 7mg/g liver dry weight has been used as a guide to start
therapy.• Serum ferritin > 1000ng/ml is used as a guide for patients with
thallassemia.• Transfusional overload: 20-30 unit packed cells should have chelation
therapy initiated.. Serum ferritin > 1000mg or 20 units packed cells transfused is
indication of chelation therapy .
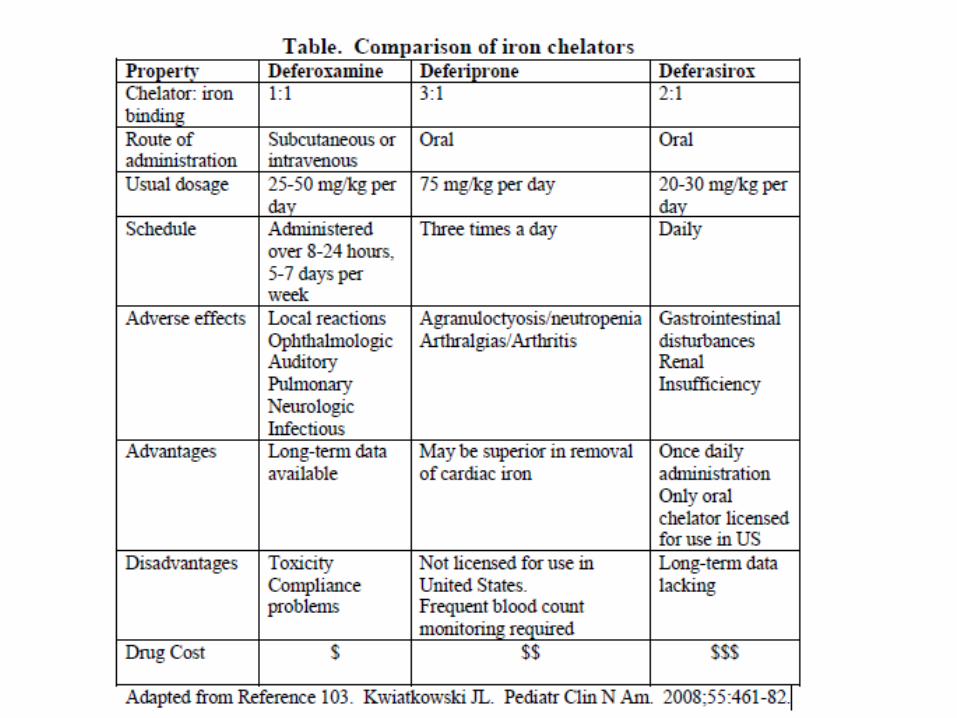
Chelation AgentDesferrioxamine (DFO) • It was introduced in the 1970s.• It is administered subcutaneously by infusion of 30-50ng/kg over
8-12 hours every night for 5-7 days a week.• With good compliance the drug can prevent or reverse cardiac
dysfunction and improves survival.
Adverse effects• Reversible sensorineural deafness• Retinal damage• Growth retardation
NB: Compliance is poor
Deferiprone
• Orally active Iron chelator that causes predominantly urinary Iron excretion.
• It is given at 75mg/kg in three doses daily.• It is used alone or in combination with
desferrioxamine.• Deferiprone is more effective than desferrioxamine at
removing cardiac Iron.• Compliance is better.Side effects• Athropathy, neutropenia, G.I. Disturbance and Zinc
deficiency.
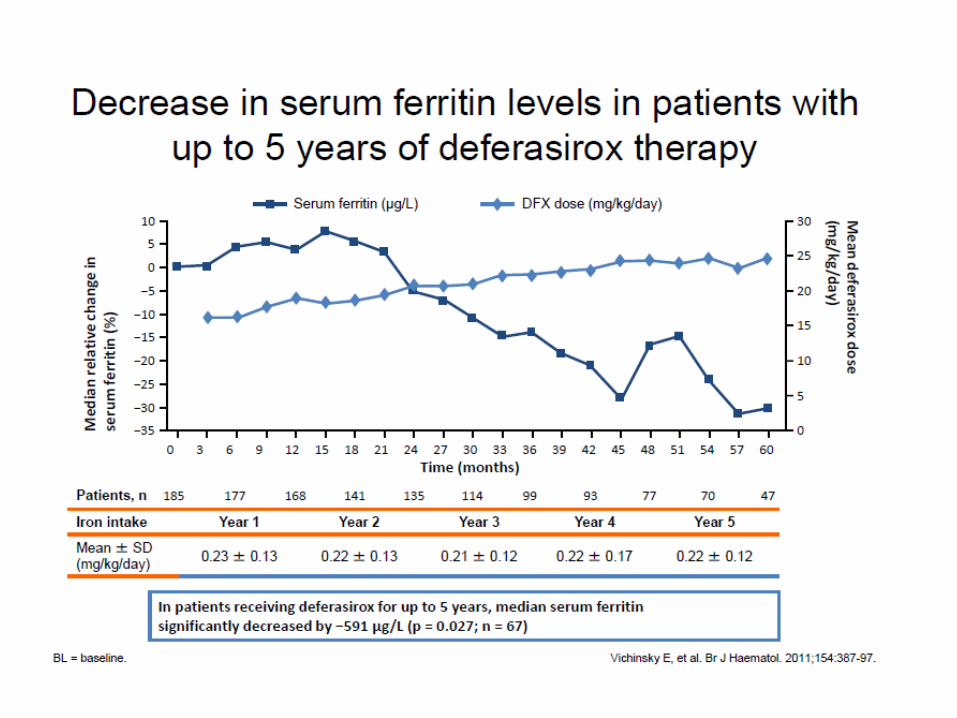
Deferasirox (Exjade/ Asunra)
• Newest oral chelating• Given at 20-40mg/kg• The dosing recommendation is pediatric >
2years is the same as for adults• The tablet is dispersed by stirring in a glass of
water or apple juice (100-200ml) until a fine suspension is obtained
• It is taken on an empty stomach 30 minutes before meals
Contraindications
1. Patients with creatinine clearance < 40ml/min
2. High risk myelodysplastic syndrome (MDS)
3. Non-haematological malignancies who are not expected to benefit from chelation therapy due to rapid progression of their disease.
4. Hypersensitivity to deferasirox.
Conclusion
• Life expectancy has increased dramatically for thallassemia major and other transfusion-dependent patients with chelation therapy.
• In many cases cardiac and liver damage caused by iron overload can be reversed and endocrine status may be improved.