-
2/29/2012
1
Gregg A Miller, MD
Balloon Assisted Angioplasty in AVF Maturation:
CHIEF MEDICAL OFFICER
Fresenius Vascular Care
ASSISTANT CLINICAL PROFESSOR
Columbia University Physicians & Surgeons
DISCLOSURE
Gregg A Miller, MDChief Medical OfficerFresenius Vascular
Care
I have no financial relationships to disclose.
www.GreggMillerMD.com
2009 Medicare $491 billion• 3.1% from 2008
2009 TOTAL MEDICARE COSTS
ESRD (5.9%)• $29 billion• 11%
non-ESRD (94.1%)
US Renal Data System: USRDS 2009 Annual Data Report. Bethesda,
MD: National Institute of Health, National Institute of Diabetes
and Digestive and Kidney Diseases, 2009
ANNUAL COST PER PATIENT
Based on 2007 ESRD data:
• $75,344 ($6278.66/mo) for Catheter
• $72,729 ($6060.75/mo) for AVG
• $55,112 ($4592.66/mo) for AVF
Miller GA et al: Percutaneous salvage of thrombosed immature
arteriovenousfistulas. Semin Dial. 2011;24(1): 107-114
AVF v AVG
Lee T, et al: Comparison of survival of upper arm arteriovenous
fistulas and grafts after failed forearm fistula. J Am Soc Nephrol.
2007;18(6):1936-41
-
2/29/2012
2
AVF Creation
AVF SUCCESS RATES
Unassisted Maturation
(40%)
Assisted Maturation;Requires Intervention
(60%)
Dember LM et al: Effect of clopidogrel on early failure of
arteriovenous fistulas for hemodialysis: a randomized controlled
trial. JAMA. 2008;299(18):2164-2171
Assisted Maturation
of AVF
AVF COMPARISONS
Mature AVF (unassisted)
Catheter
AVG
Peritoneal Dialysis
VS
FISTULA : PRO vs CON
Less cost PPPY -
Low infection rate -
- time to reach clinical success results
in prolonged catheter time
- Variable depth � More infiltrations
PRO vs CONUNASSISTED Maturation vs AVG
FISTULA MATURATION: PRO vs CON
AVF prevalence -
Less cost PPPY -
Low infection rate -
- time to reach clinical success results
in prolonged catheter time
- Variable depth � more infiltrations
- Requires multiple visits
- More procedures / PPY
- adv procedure skill & equip
PRO vs CONAssisted Maturation vs AVG
-
2/29/2012
3
TECHNIQUES
1) Flow Rerouting with Elimination of Competing Branch Veins
2) Staged Sequential Dilation
3) Long Length Balloon PTA
4) Limited Controlled Extravasation
Directional Guidance Rotate Guiding Catheter
Step 1: Find the Anastamosis
THROMBECTOMY MATURATION
Wire Guided Selective Catheterization
Step 2: Wire Guided Flow Re-routing
Demonstrate Basilic Vein Pathway
using 0.018 Guiding Catheter
THROMBECTOMY MATURATION
Find Point of Greatest Stenosis
Step 3: Confirm Basilic Outflow Vein
Confirm Lumen
THROMBECTOMY MATURATION
Step 4: Dilate in 1mm Increments until 6mm using Long Length
Balloons
THROMBECTOMY MATURATION
Step 5: Retrograde Access Using Balloon Puncture Technique
Dilate Inflow Stenosis Fully Efface all Stenoses & Restore
Flow
THROMBECTOMY MATURATION
-
2/29/2012
4
Step 6: Restore Flow / Troubleshoot
Forearm Flow-
Check for Perforations
Upper Arm Flow-
Check for Unimpeded Drainage
THROMBECTOMY MATURATION
Step 7: Eliminate Problematic Collateral Veins
Antegrade
Collaterals
Retrograde
Collaterals
THROMBECTOMY MATURATION
Step 8: Dilate Using Inflow Control
• Manual Pressure at anastamosis
• Protect torn distal vein segments
• Avoid exposing injured distal segments to high arterial
pressure
THROMBECTOMY MATURATION
Step 9: Final Inspection
THROMBECTOMY MATURATION
Second Ballooning
BEFORE AFTER
THROMBECTOMY MATURATION
Follow-Up at Two Weeks
THROMBECTOMY MATURATION
-
2/29/2012
5
THROMBECTOMY MATURATION
Follow-Up at Four Weeks
THROMBECTOMY MATURATION
Aggressive Approach to Salvage Non-Maturing AVF: A Retrospective
Study with F/U (n=122)
All unusable AVFs underwent salvage procedures
BAM on AVF DIAMETER
Miller GA et al: Aggressive approach to salvage non-maturing
arteriovenous fistulae: a retrospective study with follow-up. J
Vasc Access. 2009;10:183-191
% PATENT
Aggressive Approach to Salvage Non-Maturing AVF: A Retrospective
Study with F/U (n=122)
Ave Access intvnt/yr= 1.5
Miller GA et al: Aggressive approach to salvage non-maturing
arteriovenous fistulae: a retrospective study with follow-up. J
Vasc Access. 2009;10:183-191
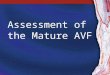
SECONDARY PATENCY
Kaplan-Meier Survival Analysis (n=122)
(mos)
INTERVENTIONS TO MATURATE
Lee T, et al: Decreased cumulative access survival in
arteriovenous fistulas requiring interventions to promote
maturation. Clin J Am Soc Nephrol. 2011;6(3):575-81
-
2/29/2012
6
VASCULAR REMODELING v VESSEL WALL THICKENING
Lee T, Roy-Chaudhury P: Advances and new frontiers in the
pathophysiology of venous neointimal hyperplasia and dialysis
access stenosis. Chronic Kidney Dis. 200;16(5):329-38
VASCULAR REMODELING v VESSEL WALL THICKENING
Lee T, Roy-Chaudhury P: Advances and new frontiers in the
pathophysiology of venous neointimal hyperplasia and dialysis
access stenosis. Chronic Kidney Dis. 200;16(5):329-38
HOW DO YOU PREDICT?
HOW DO YOU PREDICT?
Blood PressureTissue Integrity
First Failure Predicts Subsequent Failure
RADIAL ARTERY ANGIOPLASTY
Turmel-Rodrigues L et al: Percutaneous dilation of the radial
artery in nonmaturing autogenousradial-cephalic fistulas for
haemodialysis. Nephrol Dial Transplant2009; 24(12): 3782-3788
PREEMPTIVE PTA
Preemptive PTA allows for suboptimal veins
De Marco Garcia LP et al: Primary balloon angioplasty plus
balloon agioplasty maturation to upgrade small-caliber veins (
-
2/29/2012
7
SALVAGE FROM SALVAGE PROCEDURE
Table 3: Follow-up Stats for 108 Matured Fistulas
Miller GA et al: Percutaneous salvage of thrombosed immature
arteriovenousfistulas. Semin Dial. 2011;24(1): 107-114
IMMATURE FISTULA INTERVENTIONS
Miller GA et al: Percutaneous salvage of thrombosed immature
arteriovenousfistulas. Semin Dial. 2011;24(1): 107-
114
Miller GA et al: Aggressive approach to salvage non-maturing
arteriovenous fistulae: a retrospective study with follow-up. J
VascAccess. 2009;10:183-191
AVF
AVF SUCCESS RATES
Success (40%)
Failure (60%)
BAM (93%)
New Access (7%)
2.78 intvnt PPPY
0.06-0.57 intvnt PPPY
0-4.5% infections/yr
0.52% infections/yr
AVF/AVG COST COMPARISON
Success (40%)
Failure (60%)
2.78 intvnt PPPY
AVG
AVF
1.8-5.3 intvnt PPPY$72,729/yr
$55,112/yr
0.06-0.57 intvnt PPPY
0-4.5% infections/yr
0.52% infections/yr
6-22% infections/yr
+$5,487 (maintain)
=$60,599/yr
CONCLUSIONS
Though immature AVF requires more skill, initial procedures, and
time….
•Less infections
•Fewer interventions
•Costs less overall
Assisted Maturation AVF AVG>www.GreggMillerMD.com