Embed Size (px)
Citation preview

AAMC Readiness for Reform
Association of American Medical Colleges1Association ofAmerican Medical Colleges
Learn
Serve
Lead
Maine Medical Center Case StudyPatient Safety: People, Processes, and Systems Leading to Positive Results
AAMC Readiness for Reform

AAMC Readiness for Reform AAMC Readiness for Reform
Association of American Medical Colleges Association of American Medical Colleges2 3
Background
“State and federal courts, state licensing boards, and accrediting bodies such as Joint Commission all function to maintain accountability and standards; however, the very fear of existing legal liability or its misapplication are the greatest hurdles to pioneering patient-safety efforts. The health care system needs to transform the existing culture of blame and punishment that suppresses information about errors and adverse events into a culture of safety that focuses on openness and information sharing to improve health care and prevent adverse outcomes. Education and leadership will be most important to creating and sustaining a strong safety culture and arguably the most important defense against preventable harms.”1
Maine Medical Center (MMC) is consistently ranked as one of the safest hospitals in America. It has won HealthGrades Excellence Awards™ in Cardiac Care, Coronary Intervention, Joint Replacement, and Prostatectomy.
MMC has worked hard for these achievements. The 637-bed tertiary hospital in Portland, Maine makes a deliberate and concerted effort to identify, assess, and address patient safety risk factors. A primary component of the patient safety strategy has been to create an institutional culture in which all team members identify and resolve safety issues without fear of retribution. Furthermore, MMC operates under the assumption that most safety issues are the result of systemic – not individual – failings and therefore must be remedied through a combination of infrastructural changes (e.g., processes, technologies, and training), and incentives that promote adoption and maintenance of safer practices. This case study details MMC’s efforts to develop both the culture and the technologies that enable a safer patient care experience.
Patient Safety Culture
Traditionally, medical errors were treated as ‘human errors’ made by clinicians and remediated by assigning blame and punishment. However, evidence suggests that the causes of errors are most often systemic. As a result, institutional culture plays a critical part in addressing such errors.2
The Agency for Healthcare Research and Quality (AHRQ) identifies four foundational features of a “Culture of Safety”:3
• Acknowledgment of the high-risk nature of an organization’s activities and the determination to achieve consistently safe operations
• A blame-free environment where individuals are able to report errors or near misses without fear of reprimand or punishment
The AAMC launched the Readiness for Reform (R4R) initiative in 2010 to support
the nation’s medical schools and teaching hospitals as they implement key elements
of health care reform. R4R began with a voluntary institution-wide survey to assess
members’ level of preparedness for eight key focus areas of health reform: education,
research/comparative effectiveness, payment reform, care delivery reform, community
and patient engagement, access, quality, and health information technology (HIT).
The AAMC now supports a number of projects aimed at identifying and sharing best
practices related to the R4R focus areas in member institutions. More information on
the R4R initiative can be found at: www.aamc.org/initiatives/r4r.
Preparing an organization to succeed under the rapidly shifting paradigms of the current
health care environment will require new leadership and management skills that extend
beyond the C-suite and into the very fabric of the organization. This case study is one in
a series that will highlight member success stories in the eight R4R focus areas.
AAMC Readiness for Reform Case Study Project Team:
Joanne Conroy, M.D.Chief Health Care OfficerAAMC
Michael Weitekamp, M.D.Robert G. Petersdorf Scholar-in-ResidenceAAMC
Meaghan QuinnSenior Program SpecialistAAMC
Tom EndersManaging DirectorManatt Health Solutions
Molly SmithManagerManatt Health Solutions
Jan NorrisAdvisorManatt Health Solutions
Maine Medical Center:
Douglas Salvador, M.D, M.P.H.Associate Chief Medical Officer and Patient Safety OfficerMaine Medical Center
1 Small SD, Barach P., “Patient safety and health policy: a history and review,” Hematol Oncol Clin North Am. 2002 Dec;16(6):1463-82.2 Anderson, James G., “The need for organizational change in patient safety initiatives,” RCHE Publications. 2006. Paper 40. http://docs.lib.
purdue.edu/rche_rp/403 Agency for Healthcare Research and Quality, “Patient Safety Primers: Safety Culture,” Accessed June 2012 at http://psnet.ahrq.gov/primer.
aspx?primerID=5

AAMC Readiness for Reform AAMC Readiness for Reform
Association of American Medical Colleges Association of American Medical Colleges4 5
Figure 1
How Healthy is Our Culture? Safety Attitudes Questionnaire Domain Scores
0
10
20
30
40
50
60
70
80
90
100
TeamworkClimate
2008
2009
SafetyClimate
JobSatisfaction
StressRecognition
WorkingConditions
Perceptions ofHospital Mgmt.
Perceptions ofUnit Mgmt.
Dan
ger
Zo
ne
Ave
rag
e Pe
rcen
t Po
siti
ve
Go
al Z
on
e
• Encouragement of collaboration across ranks and disciplines to seek solutions to patient safety problems
• Organizational commitment of resources to address safety concerns
Culture influences whether providers prioritize patient safety, whether errors are treated as evidence of systemic or personal failure, how solutions are developed and, in turn, whether solutions are adequately communicated and implemented by providers. Not surprisingly, the literature has increasingly found strong evidence of the close relationship between institutional culture and patient safety outcomes.4
At MMC, the issue of institutional culture was raised as the next step for improving patient safety. MMC had already worked to spread the tenets of Just Culture as well as embed a culture of patient centeredness. In 2008, MMC engaged Dr. Allan Frankel of Pascal Metrics to launch a patient safety culture improvement initiative. Pascal Metrics uses the following framework as part of its Safety Culture Program:5
Educate and Train
Educate and train staffat all levels of theorganization in thescience of safety andconceptualize it withinthe local environment.
Measure
Obtain safety culturesurvey data at the unit-level through staffsurveys and observation.
Analyze
Analyze culture toidentify and trackculture-driven risk andestablish performancebenchmarks.
Intervene
Develop action plansand tools and measureimplementation
This initiative led to dramatic improvements in MMC’s patient safety culture across the medical center and its practices. After implementing a formal team training program in surgical services, the Neonatal ICU and Family Birth Center, the patient safety culture was significantly improved in every domain of the Safety Attitudes Questionnaire (SAQ). Figure 1 shows the organization’s overall improvement on the SAQ domains from 2008 to 2009, and Figure 2 shows the improvement at the practice level using the example of the urology offices. Figure 3 shows the impact of the patient safety initiatives on clinical outcomes with decreases in surgical site infections rates.
4 1) Neily J, Mills PD, Young-Xu Y; et al. “Association Between Implementation of a Medical Team Training Program and Surgical Mortality,” JAMA 2010; 304(15):1693-1700. 2) Mazzocco J, Pettiti DB, Fong KT, et al. “Surgical Team Behaviors and Patient Outcomes,” Am J Surg 2008. 3) Pratt SD, Mann S, Salisbury M, et al. ”Impact of CRM-based team training on obstetric outcomes and clinicians’ patient safety attitudes,” Jt Comm J Qual Patient Saf 2007;33:720-725. 4) Hansen LO, Williams MV, Singer SJ. “Perceptions of Hospital Safety Climate and incidence of Readmission,” Health Services Research 2011;46(2):596-616.
5 Pascal Metrics, http://www.pascalmetrics.com/products_services/safety-culture.php

AAMC Readiness for Reform AAMC Readiness for Reform
Association of American Medical Colleges Association of American Medical Colleges6 7
Figure 3
Surgical Site Infection Rate
MMC quarterly cumulative SSI ratefor all surgical procedures included in surveillance plan
per 100 surgical procedures
Q12006
Q2 Q3 Q4
Rat
e o
f in
fect
ion
0
0.5
1
1.5
2
2.5
3
Q12007
Q2 Q3 Q4 Q12008
Q2 Q3 Q4 Q12009
Q2 Q3 Q4 Q12010
Q2
Quarter of the Year
While the Pascal Metrics program served to jumpstart improvements in the MMC’s patient safety culture, other factors – particularly technological adoptions and leadership priorities – consolidated this new culture and contributed to MMC’s long-term success. The next section offers a more detailed discussion of these and other factors that contributed to MMC’s success.
Figure 2
AHRQ Patient Safety Culture Office Survey Urology
0
10
20
30
40
50
60
70
80
90
100
Teamwork
2011
2012
Patient CareTracking
OrganizationalLearning
OverallPerceptions ofPatient Safety
and Quality
StaffTraining
Owner/ManagerPartner/Leader-
ship Supportfor Patient Safety
0
10
20
30
40
50
60
70
80
90
100
CommunicationAbout Error
2008
2009
CommunicationOpenness
Patient Safetyand Quality
issues
Office Processes& Standardization
InformationExchange
with OtherSettings
Work Pressure& Pace
AAMC Readiness for Reform AAMC Readiness for Reform
Association of American Medical Colleges Association of American Medical Colleges8 9
Factors for Success
Factor 1
Make PatientSafety Culturean Institutional
Priority
Factor 2
Conduct anInstitutionalAssessment
Factor 3
Educate theWhole Team
Factor 4
Make PatientSafety Culturean Institutional
Priority
Factor 5
UtilizeSupportingTechnology
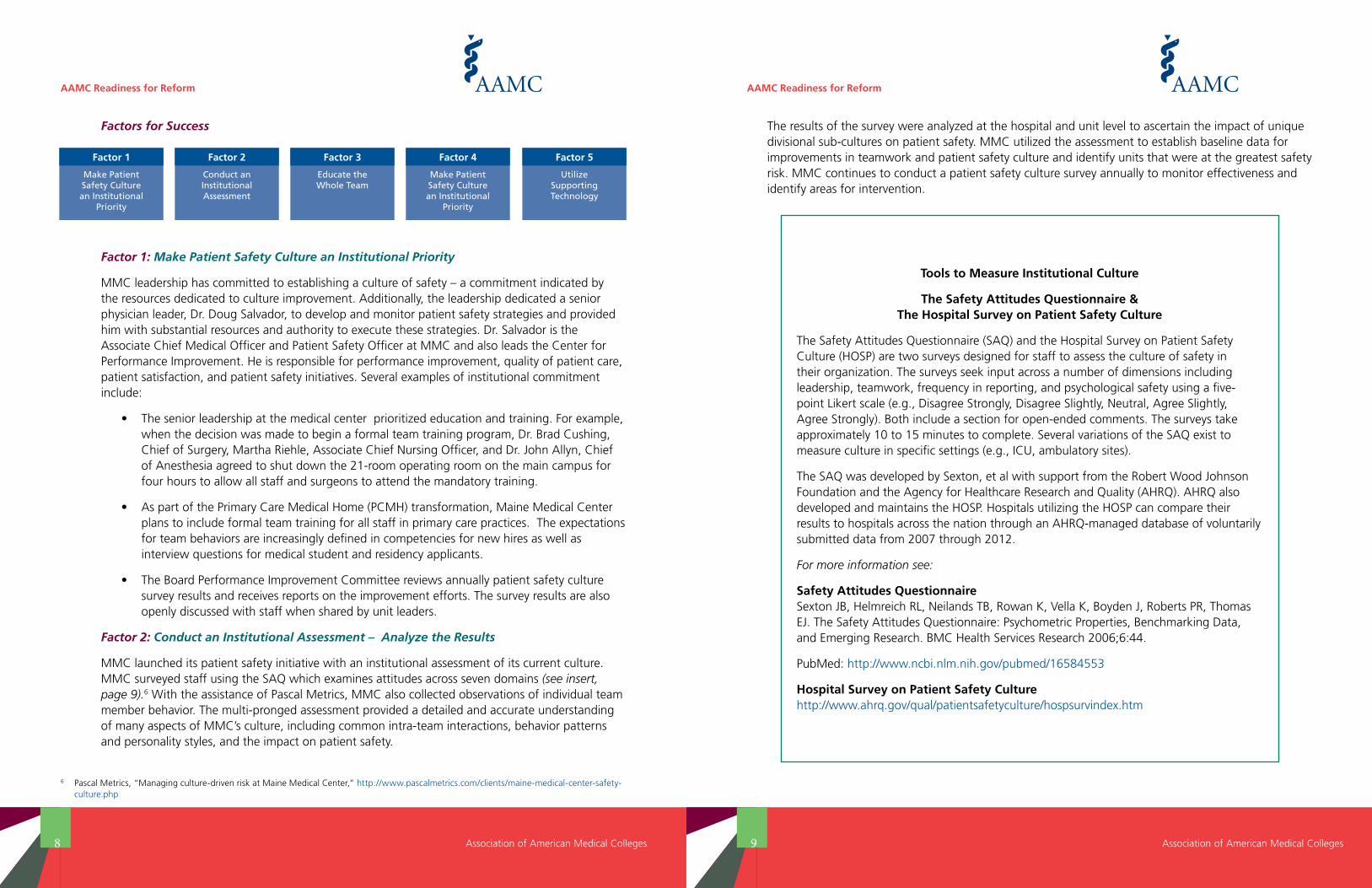
Factor 1: Make Patient Safety Culture an Institutional Priority
MMC leadership has committed to establishing a culture of safety – a commitment indicated by the resources dedicated to culture improvement. Additionally, the leadership dedicated a senior physician leader, Dr. Doug Salvador, to develop and monitor patient safety strategies and provided him with substantial resources and authority to execute these strategies. Dr. Salvador is the Associate Chief Medical Officer and Patient Safety Officer at MMC and also leads the Center for Performance Improvement. He is responsible for performance improvement, quality of patient care, patient satisfaction, and patient safety initiatives. Several examples of institutional commitment include:
• The senior leadership at the medical center prioritized education and training. For example, when the decision was made to begin a formal team training program, Dr. Brad Cushing, Chief of Surgery, Martha Riehle, Associate Chief Nursing Officer, and Dr. John Allyn, Chief of Anesthesia agreed to shut down the 21-room operating room on the main campus for four hours to allow all staff and surgeons to attend the mandatory training.
• As part of the Primary Care Medical Home (PCMH) transformation, Maine Medical Center plans to include formal team training for all staff in primary care practices. The expectations for team behaviors are increasingly defined in competencies for new hires as well as interview questions for medical student and residency applicants.
• The Board Performance Improvement Committee reviews annually patient safety culture survey results and receives reports on the improvement efforts. The survey results are also openly discussed with staff when shared by unit leaders.
Factor 2: Conduct an Institutional Assessment – Analyze the Results
MMC launched its patient safety initiative with an institutional assessment of its current culture. MMC surveyed staff using the SAQ which examines attitudes across seven domains (see insert, page 9).6 With the assistance of Pascal Metrics, MMC also collected observations of individual team member behavior. The multi-pronged assessment provided a detailed and accurate understanding of many aspects of MMC’s culture, including common intra-team interactions, behavior patterns and personality styles, and the impact on patient safety.
The results of the survey were analyzed at the hospital and unit level to ascertain the impact of unique divisional sub-cultures on patient safety. MMC utilized the assessment to establish baseline data for improvements in teamwork and patient safety culture and identify units that were at the greatest safety risk. MMC continues to conduct a patient safety culture survey annually to monitor effectiveness and identify areas for intervention.
Tools to Measure Institutional Culture
The Safety Attitudes Questionnaire & The Hospital Survey on Patient Safety Culture
The Safety Attitudes Questionnaire (SAQ) and the Hospital Survey on Patient Safety Culture (HOSP) are two surveys designed for staff to assess the culture of safety in their organization. The surveys seek input across a number of dimensions including leadership, teamwork, frequency in reporting, and psychological safety using a five-point Likert scale (e.g., Disagree Strongly, Disagree Slightly, Neutral, Agree Slightly, Agree Strongly). Both include a section for open-ended comments. The surveys take approximately 10 to 15 minutes to complete. Several variations of the SAQ exist to measure culture in specific settings (e.g., ICU, ambulatory sites).
The SAQ was developed by Sexton, et al with support from the Robert Wood Johnson Foundation and the Agency for Healthcare Research and Quality (AHRQ). AHRQ also developed and maintains the HOSP. Hospitals utilizing the HOSP can compare their results to hospitals across the nation through an AHRQ-managed database of voluntarily submitted data from 2007 through 2012.
For more information see:
Safety Attitudes Questionnaire Sexton JB, Helmreich RL, Neilands TB, Rowan K, Vella K, Boyden J, Roberts PR, Thomas EJ. The Safety Attitudes Questionnaire: Psychometric Properties, Benchmarking Data, and Emerging Research. BMC Health Services Research 2006;6:44.
PubMed: http://www.ncbi.nlm.nih.gov/pubmed/16584553
Hospital Survey on Patient Safety Culture http://www.ahrq.gov/qual/patientsafetyculture/hospsurvindex.htm
6 Pascal Metrics, “Managing culture-driven risk at Maine Medical Center,” http://www.pascalmetrics.com/clients/maine-medical-center-safety-culture.php

AAMC Readiness for Reform AAMC Readiness for Reform
Association of American Medical Colleges Association of American Medical Colleges10 11
MMC is a medical school affiliate of Tufts University School of Medicine (TUSM). Every year, MMC graduates 36 students from the Maine Track of the TUSM. It is a unique program that includes a two-week orientation, a longitudinal preceptorship in the first and second year with rural practitioners in Maine, and the entire third and fourth year with clinical rotations in Maine including a Longitudinal Integrated Clerkship at several sites. The program was founded on the principles of providing unique training in team-based care, quality improvement, and rural medicine.
During the two-week summer orientation for all first-year medical students, two-and-a-half days are spent in innovative experiences designed to impart specific competencies in team leadership and team communication skills.7 The students camp out overnight and spend two days on an island in the Casco Bay doing team-building exercises. The debriefings are run by several clinicians and patient safety experts and are designed to relate their experience to clinical situations they will encounter. Additional time is spent at the end of the first year teaching negotiation and conflict resolution competencies.
MMC has learned several lessons with respect to its safety training program:
• Participation: The entire staff must be included to ensure risk reduction is systemically addressed.
• Emphasis: MMC chose a team training curriculum that emphasizes team leadership skills such as creating an environment of psychological safety where all team members are comfortable speaking up, and where leadership has responsibility for fostering an effective system of team communication. Emphasis is also placed in training on negotiation and conflict resolution.
• Trainer Qualifications: To be seen as credible by clinical staff, trainers must have familiarity with the unique clinical experience of providers.
Factor 3: Educate the Whole Team
MMC has implemented a number of training programs for physicians and other members of the care team. Hosted onsite to improve participation, MMC’s training programs are multi-disciplinary and emphasize team leadership competencies and team communication skills. The typical program begins with assessments of baseline team practice followed by a four-hour, off-site training. The training involves the entire range of staff, including unit secretaries, housekeeping, respiratory therapy, nursing, advanced practice professionals, physicians, and others. Staff are seated at tables of eight in assigned seats with at least one physician or advanced practice professional per table. Much of the training session is spent in discussion or the practice of communication skills related to real-world issues taken from their clinical areas. By summer 2012, more than 3,000 physicians, trainees, and staff had been trained at MMC.
New residents (approximately 65 per year) receive three hours of training that stresses a patient safety culture on their first week of orientation. It is an interdisciplinary training experience that includes refresher training for recent hires.
7 Trowbridge RL, Varaklis K, Eddy V, Fritsch S, Skolfield J, Salvador D, Hillman R, Bing-You RG. “An Experiential Two-Week Orientation Designed to Introduce a Multi-Themed Curriculum,” J Gen Intern Med 25 (S3):S438, 2010.
AAMC Readiness for Reform AAMC Readiness for Reform
Association of American Medical Colleges Association of American Medical Colleges12 13
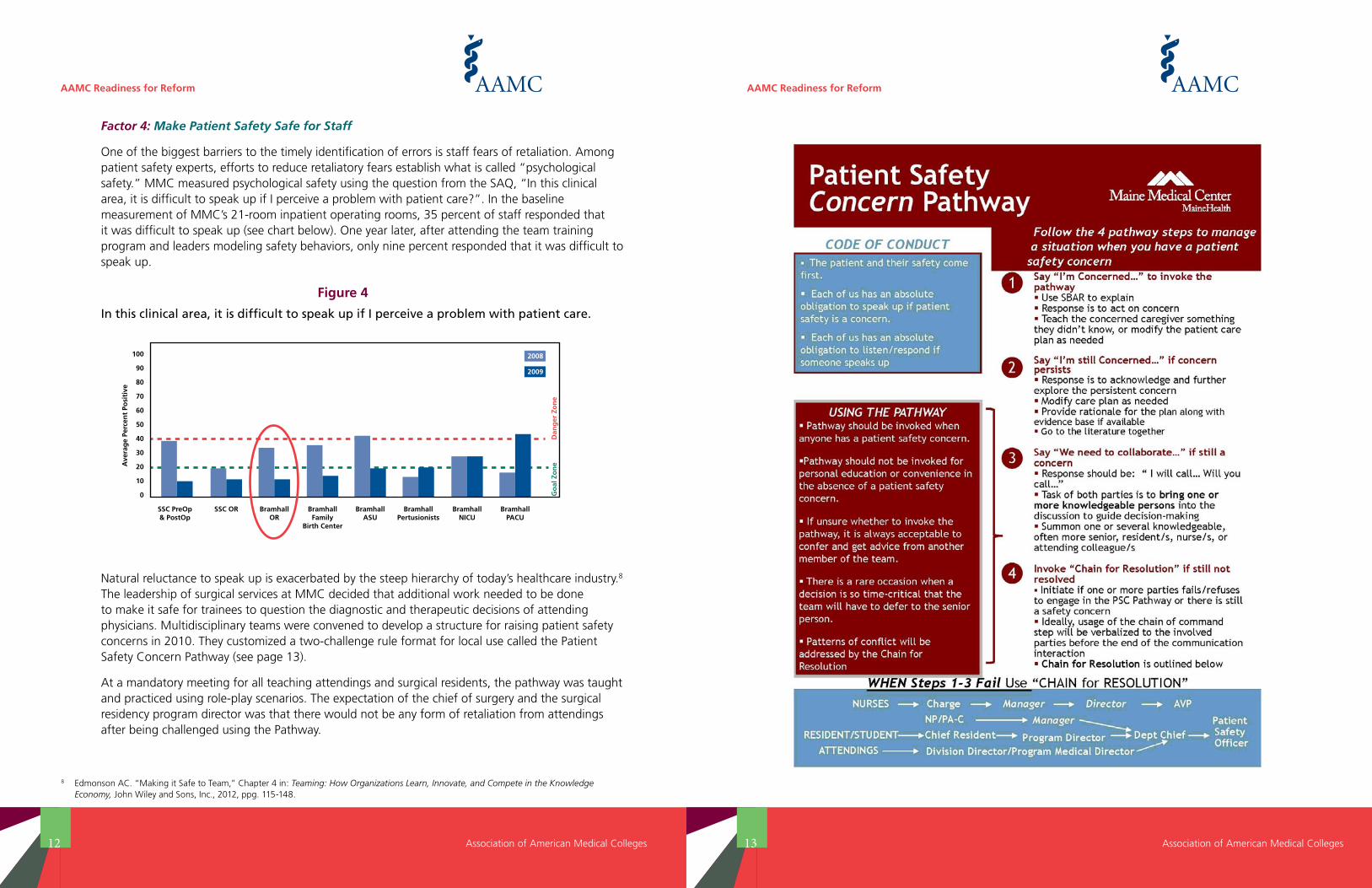
Factor 4: Make Patient Safety Safe for Staff
One of the biggest barriers to the timely identification of errors is staff fears of retaliation. Among patient safety experts, efforts to reduce retaliatory fears establish what is called “psychological safety.” MMC measured psychological safety using the question from the SAQ, “In this clinical area, it is difficult to speak up if I perceive a problem with patient care?”. In the baseline measurement of MMC’s 21-room inpatient operating rooms, 35 percent of staff responded that it was difficult to speak up (see chart below). One year later, after attending the team training program and leaders modeling safety behaviors, only nine percent responded that it was difficult to speak up.
Figure 4
In this clinical area, it is difficult to speak up if I perceive a problem with patient care.
0
10
20
30
40
50
60
70
80
90
100
SSC PreOp& PostOp
SSC OR BramhallOR
BramhallFamily
Birth Center
BramhallASU
BramhallPertusionists
BramhallNICU
BramhallPACU
2008
2009
Dan
ger
Zo
ne
Ave
rag
e Pe
rcen
t Po
siti
ve
Go
al Z
on
e
Natural reluctance to speak up is exacerbated by the steep hierarchy of today’s healthcare industry.8 The leadership of surgical services at MMC decided that additional work needed to be done to make it safe for trainees to question the diagnostic and therapeutic decisions of attending physicians. Multidisciplinary teams were convened to develop a structure for raising patient safety concerns in 2010. They customized a two-challenge rule format for local use called the Patient Safety Concern Pathway (see page 13).
At a mandatory meeting for all teaching attendings and surgical residents, the pathway was taught and practiced using role-play scenarios. The expectation of the chief of surgery and the surgical residency program director was that there would not be any form of retaliation from attendings after being challenged using the Pathway.
8 Edmonson AC. “Making it Safe to Team,” Chapter 4 in: Teaming: How Organizations Learn, Innovate, and Compete in the Knowledge Economy, John Wiley and Sons, Inc., 2012, ppg. 115-148.
AAMC Readiness for Reform AAMC Readiness for Reform
Association of American Medical Colleges Association of American Medical Colleges14 15
Factor 5: Embed the Culture of Safety in Supporting Technology
Technology plays a significant role in patient safety. Technology systems can assist direct care by providing timely, accurate, and actionable patient information and decision support. These traditional technologies include bedside monitoring, computerized provider order entry, and bar-code systems for medications. Given the challenges of making durable and lasting changes in a system as large and complex as a hospital, MMC has taken specific steps to ensure that its underlying technical systems support and reinforce the cultural and procedural approaches. To enhance these traditional health IT systems, MMC also employs a suite of technology-enabled tools that collect and analyze data to identify areas at risk for systemic errors, mitigate risks,and facilitate provider adoption of protocols.
Protocol Development/Checklists: Structures can be successfully embedded into clinical practice to support teamwork behaviors and effective team communications. Just as systems can be created to ensure the use of evidence-based protocol as a pre-requisite for continuing care, checklists and protocols for teamwork can be embedded into the electronic health record (EHR). In that regard, MMC has implemented documentation of interdisciplinary care rounds as well as requirements for standard elements to be completed prior to allowing an order for specialist consultation.
Clinical Decision Support: Clinical decision support at the point of care is another technological intervention for improving care delivery and adherence to protocols. The Barbara Bush Children’s Hospital at MMC was an early adopter of an electronic version of the Bedside Pediatric Early Warning System (BPEWS) decision support system. The BPEWS uses seven clinical measures to assist providers in determining the appropriate placement of a patient. Ultimately, the system is designed to help providers monitor and intervene before a crisis point occurs with the patient. To that end, the system uses data collected by providers to recommend one of four next steps: (1) maintain current placement/treatment, (2) increase monitoring, (3) request an evaluation from the rapid response team, or (4) move the patient to the intensive care unit. The result has been a doubling in the use of the rapid response team, the development of a common provider language that is attributed to fewer miscommunications during crises, and a significant reduction in “code blue” calls.9
Performance Score Cards: MMC has developed multi-disciplinary scorecards to measure performance against clinical and financial objectives. MMC has invested in business intelligence software to make key performance elements transparent and available to all staff. These performance measures include important patient safety and communication measures including patient safety culture survey results.
Applying Its Approach to Patient Safety:10 Focus on Diagnostic Errors
Diagnostic error has not received the attention of other patient safety challenges, but research suggests the incidence and impact of such errors is high. A Harvard Medical Practice Study found that 17 percent of preventable errors in hospitalized patients were diagnostic. In reviewing its own data, MMC found that the largest category of malpractice is due to delayed identification of diagnostic errors. MMC sees the need to tackle diagnostic reliability and errors as the next frontier in patient safety.
MMC has taken an institutional approach to diagnostic errors. Multiple issues must be addressed to improve diagnostic reliability including education, measurement, error analysis, cognitive interventions, and clinical decision support.
• Measurement: Dr. Robert Trowbridge developed a diagnostic error reporting system at MMC. The reporting system can be accessed from the desktop of all clinical PC’s, and physicians can report suspected diagnostic errors by quickly answering three simple questions anonymously. The cases are then reviewed by content experts and classified according to Graber’s Diagnostic Error Evaluation Research (DEER) criteria.10
• Education: MMC has deliberately incorporated awareness training in diagnostic error into the grand rounds curriculum of all specialties as well as specific curricular elements for many residency specialties. A particularly innovative offering is the first year TUSM course in Clinical Reasoning, co-directed by Dr. Robert Trowbridge and Dr. Joseph Rencic in Boston.
• Error Analysis: Over the past several years, MMC has increasingly used the institutional Root Cause Analysis process to analyze diagnostic errors. Traditionally, many diagnostic errors have been considered cognitive in nature and directed towards institutional peer review processes. By reviewing diagnostic errors for systems causes, MMC has been able to implement actions designed to improve diagnostic reliability. These include interdisciplinary training in affective bias and an algorithm for the evaluation of a patient with a specific presenting complaint.
Cognitive Interventions: Individual departments have begun to test cognitive interventions including feedback of individual cases as well as diagnostic pauses or checklists.
9 Caiazzo, K., “The Bedside Pediatric Early Warning System: A Clinical Nurse Leader’s Journey to Best Practice for Evaluating Patient Acuity,” CNL Summit 2011 Poster Presentations, January 20, 2011. Caiazzo, K., “CNL Outcomes in the Pediatric Inpatient Unit,” CNL Summit 2012 Abstract Presentations, January 20, 2012.
10 Reference for institutional approach to diagnostic error at MMC: Trowbridge RL, Salvador D. “Addressing Diagnostic Errors: An Institutional Approach,” in National Patient Safety Foundation (NPSF) Focus on Patient Safety Newsletter, Vol 13(3) 2010. Graber Reference: Schiff GD, Hasan O, Kim S, Abrams R, Cosby K, Lambert BL, et al. “Diagnostic error in medicine: analysis of 583 physician-reported errors,” Arch Intern Med 2009;169(20):1881-7.

AAMC Readiness for Reform AAMC Readiness for Reform
Association of American Medical Colleges Association of American Medical Colleges16 17
2. Let the data be your guide – mine existing data to identify triggers and implement error identification and tracking mechanisms. Encourage clinicians to report errors through anonymous systems. Dedicate resources to monitor and analyze data and turn errors into learning opportunities.
3. Take a team approach but be sure to obtain physician buy-in. Responsibility for patient safety should be shared across the institution – from the hospital executives to the specialists to the technicians – and opportunities for education and access to reporting tools should be available to all team members. However, physician buy-in is particularly critical for success. Physicians must see patient safety efforts as valuable and non-threatening. Organizations may want to start efforts on a pilot basis in particular units and expand more broadly as success is demonstrated.
4. Design quality and safety tools in response to identified areas of safety culture risk. Work with providers to embed these tools into the provider workflow.
Resources
AHRQ Patient Safety Network: http://psnet.ahrq.gov/default.aspx
Safety Attitudes Questionnaire: http://www.ncbi.nlm.nih.gov/pubmed/16584553
http://www.uth.tmc.edu/schools/med/imed/patient_safety/questionnaires/SAQBibliography.html
AHRQ Hospital Survey on Patient Safety Culture: http://www.ahrq.gov/qual/patientsafetyculture/hospsurvindex.htm
Pascal Metrics Safety Culture: http://www.pascalmetrics.com/products_services/safety-culture.php
Lessons Learned
1. Interventions must be sustained. When MMC relaxed education and training, results on patient safety culture measures and compliance with protocols fell.
2. Need to monitor. Organizations must develop a Just Culture where remediation of errors is applied fairly. This can be particularly challenging when certain risky behaviors do not frequently lead to errors, are missed, or not reported. Establishment of protocols and scorecards to track compliance can help support staff in adopting safer behaviors.
3. Engaging patients in safety improvement efforts is challenging. Despite significant discussion around how to include patients, it has been very difficult to put into practice. MMC has experimented with different patient engagement techniques such as including patients and families in morning rounds. However, MMC has not yet discovered a strategy that has significant impact on error rates.
4. Addressing patient safety helps prepare institutions for new payment models. Safety and quality are increasingly important under new payment methodologies across Medicare, Medicaid, and commercial payers (e.g., reimbursement penalties for unnecessary 30-day re-admissions). For example, starting later this year, if a patient has to be readmitted within 30 days for a cause that can be traced back to poor patient safety performance, the hospital will be penalized under Medicare. Therefore, patient safety initiatives are critical to both the health system’s quality and financial performance.
How Can Other AMCs Apply the MMC Patient Safety Framework?
MMC’s work in patient safety can serve as a road map for other AMCs. Many AMCs are at the forefront of incorporating evidence-based protocols and technology to predict and avert patient safety risk in hospitals. The steep hierarchy that exists across healthcare and within AMCs has not always been seen as elevating patient safety risk. Improving patient safety culture is not easy and requires different leadership from chiefs of service and program directors. The evidence is mounting that doing this work is necessary to achieving the highest levels of patient safety performance. As reimbursement from both government and commercial payers moves to pay for performance and value, those institutions that have begun to identify and address patient safety risks will be better prepared to succeed financially.
1. Leadership must commit to developing a patient safety culture and reflect this commitment through resource allocation, regular assessment of the safety culture within the organization, provider training, hiring practices, and identification of skilled patient safety personnel with an appropriate allocation of time.