Embed Size (px)
Citation preview
7/27/2019 Lung Ca (OPO)
http://slidepdf.com/reader/full/lung-ca-opo 1/8
Patient Summary
Patient RAB, 49 y/o male, diagnosed with Non-Small Cell Lung Cancer. Medical History shows
that he had wedge resection last November 2010 and Lobectomy last June 2011 because of Right
Adenocarcinoma. He also had a Segmentectomy due to Left Adenocarcinoma last December 2011. PET
scan performed last August 2012 reveals hypermetabolic pleural nodules at the Right Lower Lobe. Basedon his physical examination done last September 2012, he is negative EGFR (Epidermal Growth Factor
Receptor), Vital Signs Stable, Decreased Breath Sounds and NRRR. His initial recommendations are
Pemetrexed (Alimta) and Zoledronic Acid (Zometa). Patient undergone 2 cycles of Pemetrexed and
shifted to Gemcitabine HCL (Gemzar) last December 3, 2012.
Lung Cancer Overview
Lung Cancer is a disease characterized by uncontrolled cell growth in tissues of the lung, also
known as bronchogenic carcinomas.
There are two main types of lung cancer:
Non-small Cell Lung Cancer (NSCLC) is the most common type of lung cancer, accounts for
80%.
Squamous Cell Carcinoma (Epidermoid Carcinoma) – it is the most common type of
NSCLC and the most common type of lung cancer in men. This forms in the lining of the
bronchial tubes.
Adenocarcinoma - the most common type of lung cancer in women and in non-
smokers. It forms in the mucus-producing glands of the lungs.
Bronchioalveolar Carcinoma - this type of lung cancer is a rare type of
adenocarcinoma that forms near the lungs' air sacs.
Large-cell Undifferentiated Carcinoma - a rapidly growing cancer which form near the
outer edges or surface of the lungs. This is the least common type of NSCLC.
Small Cell Lung Cancer (SCLC) comprises about 20% of lung cancers. This is the most
aggressive and rapidly growing of all lung cancers. This is mostly related to cigarette smoking,
with only 1% of these tumors occurring in non-smokers.
If the lung cancer is made up of both types, it is called mixed small cell/large cell cancer.
If the cancer started somewhere else in the body and spread to the lungs, it is called metastatic cancer
to the lung.
7/27/2019 Lung Ca (OPO)
http://slidepdf.com/reader/full/lung-ca-opo 2/8
CAUSE SIGNS AND SYMPTOMS INCIDENCE PROGNOSIS
Smoking
Passive Smoking
Asbestos Fibers
Radon Gas
Familial
Predisposition
Lung Disease
(COPD)
Air Pollution
Persistent or intense coughing
Pain in the chest shoulder, or
back from coughing
Changes in color of the mucus
that is coughed up from the
lower airways (sputum)
Difficulty breathing and
swallowing
Hoarseness of the voice
Harsh sounds while breathing
(stridor)
Chronic bronchitis or
pneumonia
Coughing up blood, or blood in
the sputum
Lung cancer is the
deadliest type of
cancer for both men
and women. Each
year, more people
die of lung cancer
than of breast, colon,
and prostate cancers
combined. In 2008,
there were 1.61
million new cases,
and 1.38 million
deaths due to lung
cancer.
The overall prognosis
for lung cancer is poor
when compared with
some other cancers.
Survival rates for lung
cancer are generally
lower than those for
most cancers, with an
overall five-year
survival rate for lung
cancer of about 16%
Diagnosing Lung Cancer
Medical History and Physical Examination
Chest X-ray
CT Scan (Computerized Tomography)
MRI (Magnetic Resonance Imaging)
PET Scan (Positron Emission Tomography)
Bone Scan
Sputum Cytology
Bronchoscopy
Needle Biospy
Thoracentesis
Blood Tests
Staging Lung Cancer
The most common cancer staging method is called the TNM system.
T (1-4) indicates the size and direct extent of the primary tumor
N (0-3) indicates the degree to which the cancer has spread to nearby lymph nodes
M (0-1) indicates whether the cancer has metastasized to other organs in the body.
For example, a small tumor that has not spread to lymph nodes or distant organs may be staged as (T1,
N0, M0).
7/27/2019 Lung Ca (OPO)
http://slidepdf.com/reader/full/lung-ca-opo 3/8
For non-small cell lung cancer, TNM descriptions lead to a simpler categorization of stages. These stages
are labeled from I to IV, where lower numbers indicate earlier stages where the cancer has spread less.
More specifically:
Stage I is when the tumor is found only in one lung and in no lymph nodes.
Stage II is when the cancer has spread to the lymph nodes surrounding the infected lung.
Stage III A is when the cancer has spread to lymph nodes around the trachea, chest wall, and
diaphragm, on the same side as the infected lung.
Stage III B is when the cancer has spread to lymph nodes on the other lung or in the neck.
Stage IV is when the cancer has spread throughout the rest of the body and other parts of the
lungs.
Small cell lung cancer has two stages: limited or extensive. In the limited stage, the tumor exists in one
lung and in nearby lymph nodes. In the extensive stage, the tumor has infected the other lung as well as
other organs in the body.
Treatment
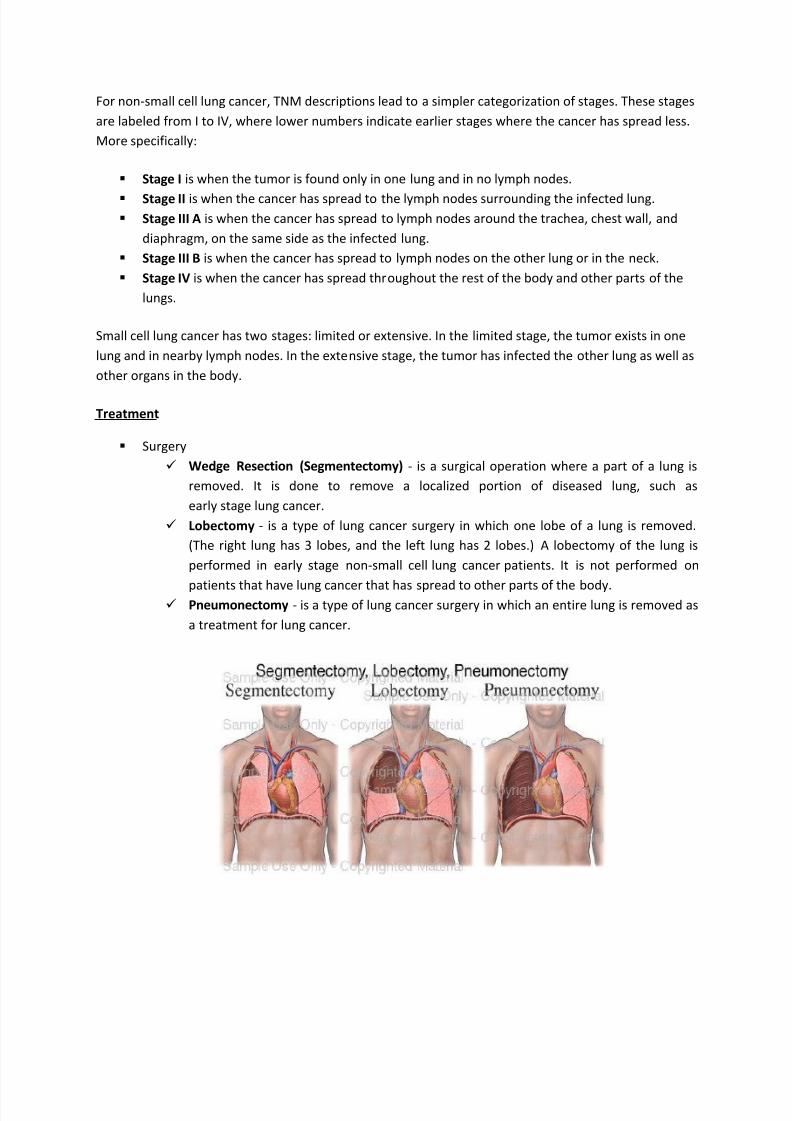
Surgery
Wedge Resection (Segmentectomy) - is a surgical operation where a part of a lung is
removed. It is done to remove a localized portion of diseased lung, such as
early stage lung cancer.
Lobectomy - is a type of lung cancer surgery in which one lobe of a lung is removed.
(The right lung has 3 lobes, and the left lung has 2 lobes.) A lobectomy of the lung is
performed in early stage non-small cell lung cancer patients. It is not performed on
patients that have lung cancer that has spread to other parts of the body. Pneumonectomy - is a type of lung cancer surgery in which an entire lung is removed as
a treatment for lung cancer.
7/27/2019 Lung Ca (OPO)
http://slidepdf.com/reader/full/lung-ca-opo 4/8
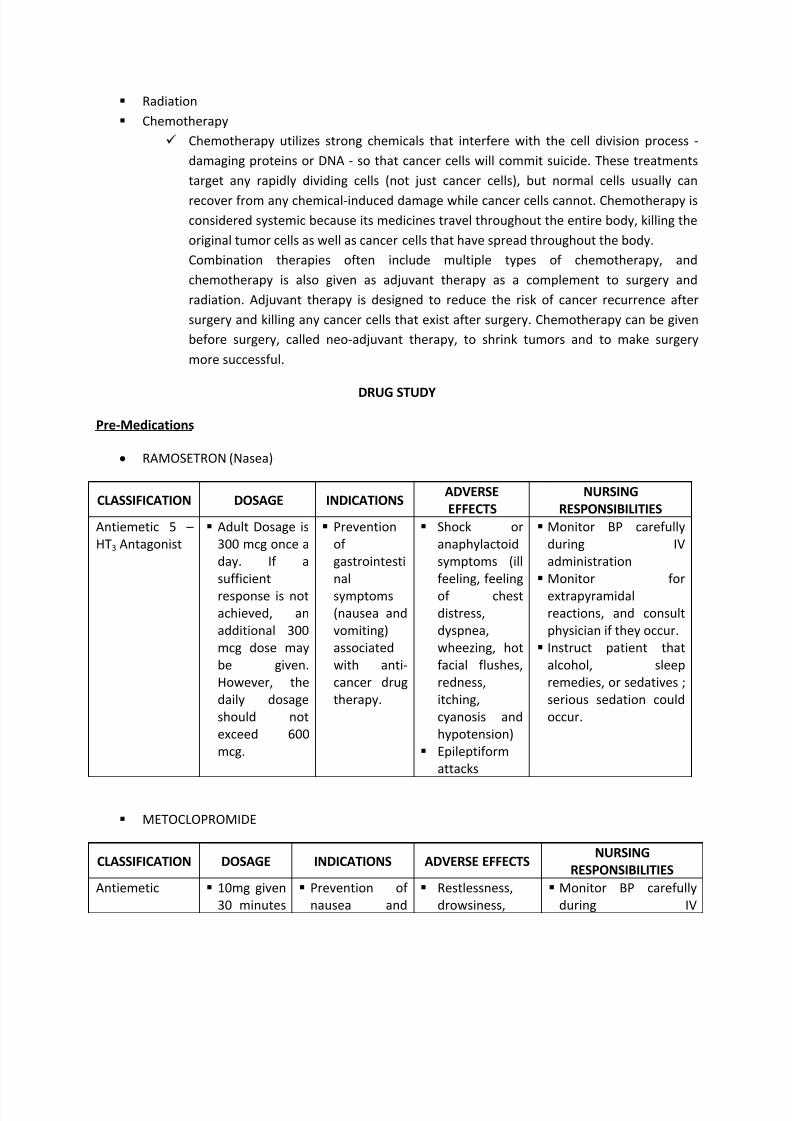
Radiation
Chemotherapy
Chemotherapy utilizes strong chemicals that interfere with the cell division process -
damaging proteins or DNA - so that cancer cells will commit suicide. These treatments
target any rapidly dividing cells (not just cancer cells), but normal cells usually can
recover from any chemical-induced damage while cancer cells cannot. Chemotherapy is
considered systemic because its medicines travel throughout the entire body, killing the
original tumor cells as well as cancer cells that have spread throughout the body.
Combination therapies often include multiple types of chemotherapy, and
chemotherapy is also given as adjuvant therapy as a complement to surgery and
radiation. Adjuvant therapy is designed to reduce the risk of cancer recurrence after
surgery and killing any cancer cells that exist after surgery. Chemotherapy can be given
before surgery, called neo-adjuvant therapy, to shrink tumors and to make surgery
more successful.
DRUG STUDY
Pre-Medications
RAMOSETRON (Nasea)
CLASSIFICATION DOSAGE INDICATIONSADVERSE
EFFECTS
NURSING
RESPONSIBILITIES
Antiemetic 5 –
HT3 Antagonist
Adult Dosage is
300 mcg once a
day. If a
sufficient
response is not
achieved, an
additional 300
mcg dose may
be given.
However, the
daily dosage
should not
exceed 600
mcg.
Prevention
of
gastrointesti
nal
symptoms
(nausea and
vomiting)
associated
with anti-
cancer drug
therapy.
Shock or
anaphylactoid
symptoms (ill
feeling, feeling
of chest
distress,
dyspnea,
wheezing, hot
facial flushes,
redness,
itching,
cyanosis and
hypotension)
Epileptiform
attacks
Monitor BP carefully
during IV
administration
Monitor for
extrapyramidal
reactions, and consult
physician if they occur.
Instruct patient that
alcohol, sleep
remedies, or sedatives ;
serious sedation could
occur.
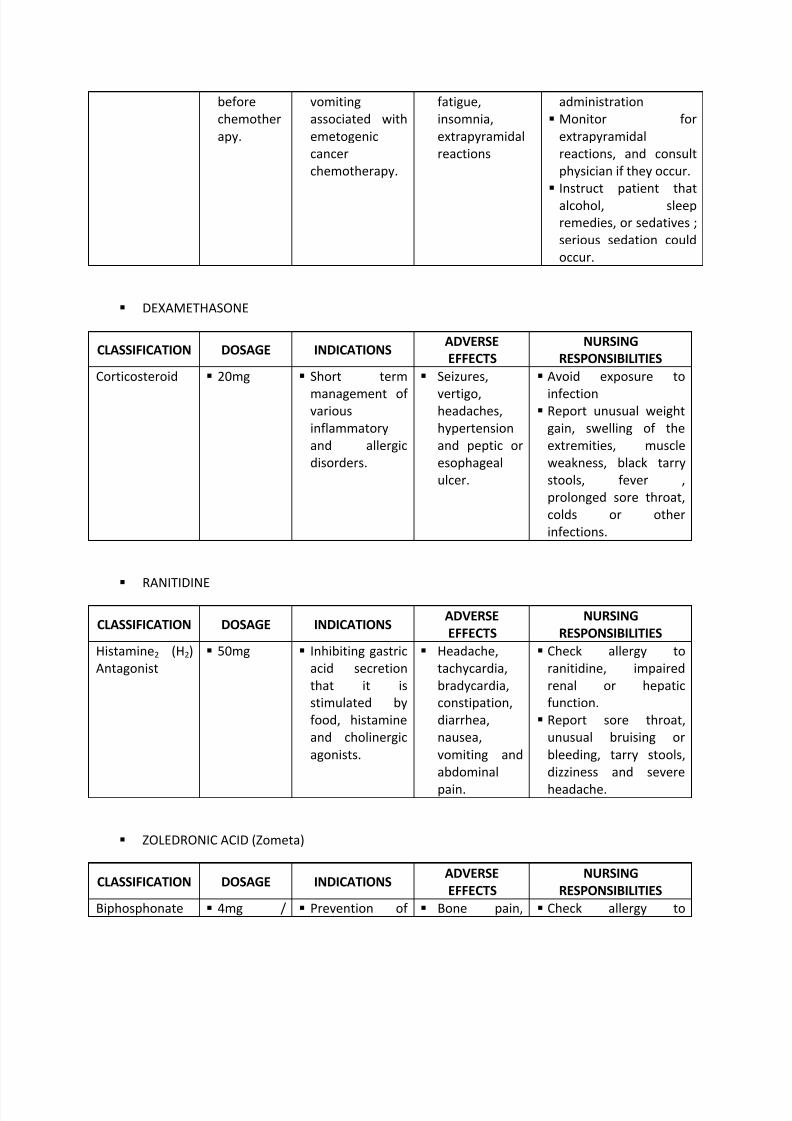
METOCLOPROMIDE
CLASSIFICATION DOSAGE INDICATIONS ADVERSE EFFECTSNURSING
RESPONSIBILITIES
Antiemetic 10mg given
30 minutes
Prevention of
nausea and
Restlessness,
drowsiness,
Monitor BP carefully
during IV
7/27/2019 Lung Ca (OPO)
http://slidepdf.com/reader/full/lung-ca-opo 5/8
before
chemother
apy.
vomiting
associated with
emetogenic
cancer
chemotherapy.
fatigue,
insomnia,
extrapyramidal
reactions
administration
Monitor for
extrapyramidal
reactions, and consult
physician if they occur.
Instruct patient that
alcohol, sleep
remedies, or sedatives ;
serious sedation could
occur.
DEXAMETHASONE
CLASSIFICATION DOSAGE INDICATIONSADVERSE
EFFECTS
NURSING
RESPONSIBILITIES
Corticosteroid 20mg Short term
management of various
inflammatory
and allergic
disorders.
Seizures,
vertigo,headaches,
hypertension
and peptic or
esophageal
ulcer.
Avoid exposure to
infection Report unusual weight
gain, swelling of the
extremities, muscle
weakness, black tarry
stools, fever ,
prolonged sore throat,
colds or other
infections.
RANITIDINE
CLASSIFICATION DOSAGE INDICATIONSADVERSE
EFFECTS
NURSING
RESPONSIBILITIES
Histamine2 (H2)
Antagonist
50mg Inhibiting gastric
acid secretion
that it is
stimulated by
food, histamine
and cholinergic
agonists.
Headache,
tachycardia,
bradycardia,
constipation,
diarrhea,
nausea,
vomiting and
abdominal
pain.
Check allergy to
ranitidine, impaired
renal or hepatic
function.
Report sore throat,
unusual bruising or
bleeding, tarry stools,
dizziness and severe
headache.
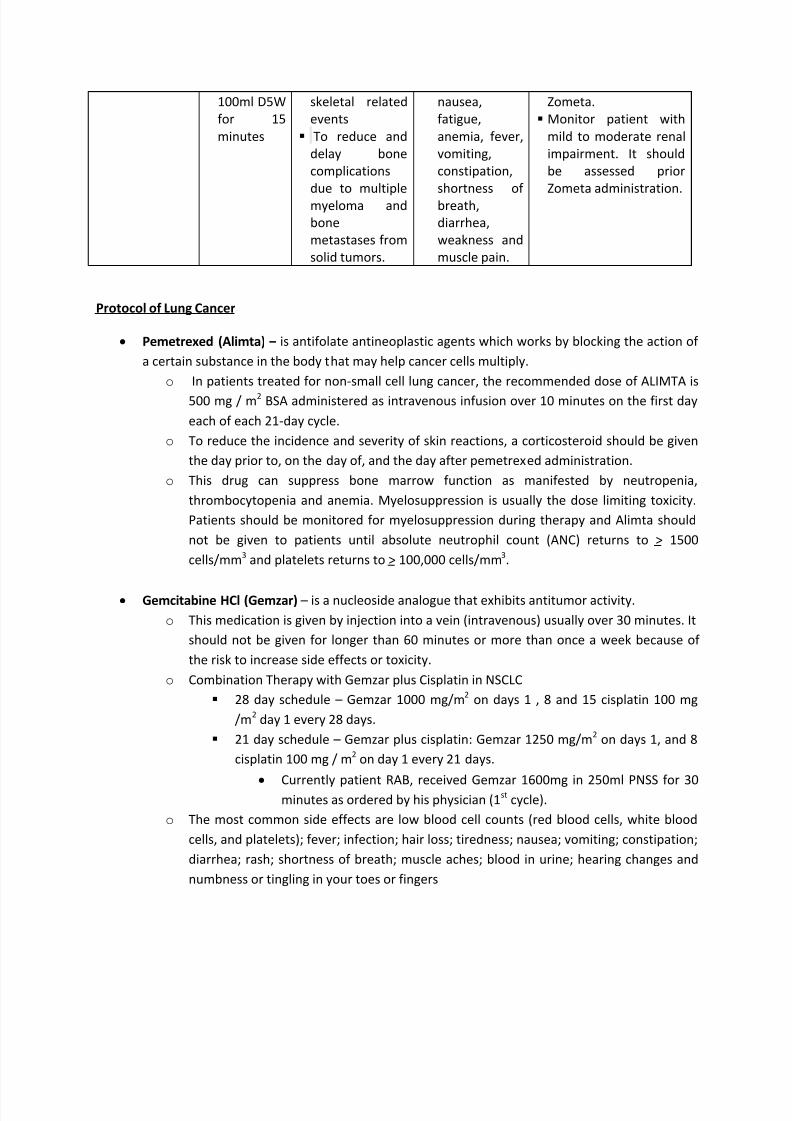
ZOLEDRONIC ACID (Zometa)
CLASSIFICATION DOSAGE INDICATIONSADVERSE
EFFECTS
NURSING
RESPONSIBILITIES
Biphosphonate 4mg / Prevention of Bone pain, Check allergy to
7/27/2019 Lung Ca (OPO)
http://slidepdf.com/reader/full/lung-ca-opo 6/8
100ml D5W
for 15
minutes
skeletal related
events
To reduce and
delay bone
complications
due to multiple
myeloma and
bone
metastases from
solid tumors.
nausea,
fatigue,
anemia, fever,
vomiting,
constipation,
shortness of
breath,
diarrhea,
weakness and
muscle pain.
Zometa.
Monitor patient with
mild to moderate renal
impairment. It should
be assessed prior
Zometa administration.
Protocol of Lung Cancer
Pemetrexed (Alimta) – is antifolate antineoplastic agents which works by blocking the action of
a certain substance in the body that may help cancer cells multiply.
o In patients treated for non-small cell lung cancer, the recommended dose of ALIMTA is
500 mg / m2 BSA administered as intravenous infusion over 10 minutes on the first day
each of each 21-day cycle.
o To reduce the incidence and severity of skin reactions, a corticosteroid should be given
the day prior to, on the day of, and the day after pemetrexed administration.
o This drug can suppress bone marrow function as manifested by neutropenia,
thrombocytopenia and anemia. Myelosuppression is usually the dose limiting toxicity.
Patients should be monitored for myelosuppression during therapy and Alimta should
not be given to patients until absolute neutrophil count (ANC) returns to > 1500
cells/mm3 and platelets returns to > 100,000 cells/mm3.
Gemcitabine HCl (Gemzar) – is a nucleoside analogue that exhibits antitumor activity.
o This medication is given by injection into a vein (intravenous) usually over 30 minutes. It
should not be given for longer than 60 minutes or more than once a week because of
the risk to increase side effects or toxicity.
o Combination Therapy with Gemzar plus Cisplatin in NSCLC
28 day schedule – Gemzar 1000 mg/m2
on days 1 , 8 and 15 cisplatin 100 mg
/m2
day 1 every 28 days.
21 day schedule – Gemzar plus cisplatin: Gemzar 1250 mg/m2
on days 1, and 8
cisplatin 100 mg / m2 on day 1 every 21 days.
Currently patient RAB, received Gemzar 1600mg in 250ml PNSS for 30minutes as ordered by his physician (1
stcycle).
o The most common side effects are low blood cell counts (red blood cells, white blood
cells, and platelets); fever; infection; hair loss; tiredness; nausea; vomiting; constipation;
diarrhea; rash; shortness of breath; muscle aches; blood in urine; hearing changes and
numbness or tingling in your toes or fingers
7/27/2019 Lung Ca (OPO)
http://slidepdf.com/reader/full/lung-ca-opo 7/8
Lung Cancer
(Out Patient Oncology)
Submitted by:
Krizelle C. Natividad
ANSET II – Cluster C
7/27/2019 Lung Ca (OPO)
http://slidepdf.com/reader/full/lung-ca-opo 8/8
Cheats
history and physical examination may reveal the
presence of symptoms or signs that are suspicious
for lung cancer. In addition to asking about
symptoms and risk factors for cancer development
such as smoking, doctors may detect signs of
breathing difficulties, airway obstruction, or
infections in the lungs.Cyanosis, a bluish color of the
skin and the mucous membranes due to insufficient
oxygen in the blood, suggests compromised function
due to chronic disease of the lung. Likewise, changes
in the tissue of the nail beds, known as clubbing, also
may indicate chronic lung disease.
chest X-ray is the most common first diagnostic step
when any new symptoms of lung cancer are present.
Chest X-rays may reveal suspicious areas in the lungs
but are unable to determine if these areas are
cancerous. In particular, calcified nodules in the lungs
or benign tumors called hamartomas may be
identified on a chest X-ray and mimic lung cancer.
CT scans - may be performed on the chest, abdomen,
and/or brain to examine for both metastatic and lung
tumors. A CT scan of the chest may be ordered when
X-rays do not show an abnormality or do not yield
sufficient information about the extent or location of
a tumor. One advantage of CT scans is that they are
more sensitive than standard chest X-rays in the
detection of lung nodules, that is, they will
demonstrate more nodules. MRI - scans may be appropriate when precise detail
about a tumor's location is required.
PET scanning is a specialized imaging technique that
uses short-lived radioactive drugs to produce three-
dimensional colored images of those substances in
the tissues within the body. While CT scans and MRI
scans look at anatomical structures, PET scans
measure metabolic activity and the function of
tissues. PET scans can determine whether a tumor
tissue is actively growing and can aid in determining
the type of cells within a particular tumor
Bone scans are used to create images of bones on a
computer screen or on film. Doctors may order a
bone scan to determine whether a lung cancer has
metastasized to the bones
Sputum cytology: The diagnosis of lung cancer
always requires confirmation of malignant cells by a
pathologist, even when symptoms and X-ray studies
are suspicious for lung cancer. The simplest method
to establish the diagnosis is the examination of
sputum under a microscope. If a tumor is centrally
located and has invaded the airways, this procedure,
known as a sputum cytology examination, may allow
visualization of tumor cells for diagnosis. This is the
most risk-free and inexpensive tissue diagnostic
procedure, but its value is limited since tumor cells
will not always be present in sputum even if a cancer
is present. Also, noncancerous cells may occasionally
undergo changes in reaction to inflammation or
injury that makes them look like cancer cells.
Bronchoscopy: Examination of the airways by
bronchoscopy (visualizing the airways through a thin,
fiberoptic probe inserted through the nose or mouth)
may reveal areas of tumor that can be sampled
(biopsied) for diagnosis by a pathologist
Needle biopsy: (FNA) through the skin, most
commonly performed with radiological imaging for
guidance, may be useful in retrieving cells for
diagnosis from tumor nodules in the lungs. Needle
biopsies are particularly useful when the lung tumor
is peripherally located in the lung and not accessible
to sampling by bronchoscopy
Thoracentesis: Sometimes lung cancers involve the
lining tissue of the lungs (pleura) and lead to an
accumulation of fluid in the space between the lungs
and chest wall (called a pleural effusion). Aspiration
of a sample of this fluid with a thin needle
(thoracentesis) may reveal the cancer cells andestablish the diagnosis. As with the needle biopsy, a
small risk of a pneumothorax is associated with this
procedure.
Blood tests: While routine blood tests alone cannot
diagnose lung cancer, they may reveal biochemical or
metabolic abnormalities in the body that accompany
cancer. For example, elevated levels of calcium or of
the enzyme alkaline phosphatase may accompany
cancer that is metastatic to the bones. Likewise,
elevated levels of certain enzymes normally present
within liver cells, including aspartate
aminotransferase(AST or SGOT) and alanine
aminotransferase (ALT or SGPT), signal liver damage,
possibly through the presence of tumor metastatic to
the liver.