Embed Size (px)
Citation preview
Linfoadenectomia e Linfoadenectomia e
nefrectomia citoriduttivaVincenzo FicarraDirettore Clinica di Urologia
Azienda Ospedaliera Universitaria di Udine
" ... to occlude the " ... to occlude the renalrenal arteryartery atat an an earlyearly stage of stage of
the procedure and the procedure and removeremove the the renalrenal tumortumor en en blocbloc
with the with the lymphaticslymphatics""
Radical nephrectomy for RCC: the
Robson criteria
"The para"The para--aorticaortic ((leftleft) and para) and para--caval (right) caval (right) lymphlymph
nodesnodes shouldshould be be removedremoved from the from the cruscrus of the of the
diaphragmdiaphragm distallydistally to the to the biforcationbiforcation of the aorta".of the aorta".
Robson CJ J Urol 1963; 89: 37Robson CJ J Urol 1963; 89: 37--4242
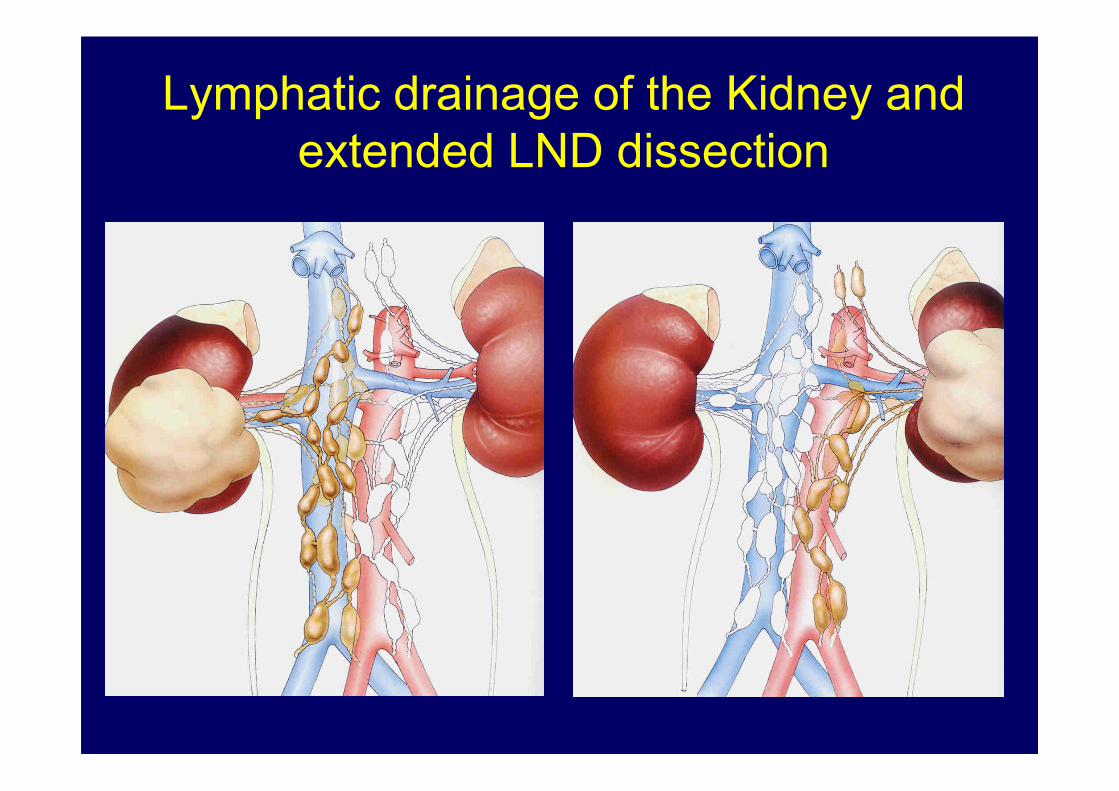
Lymphatic drainage of the Kidney and
extended LND dissection
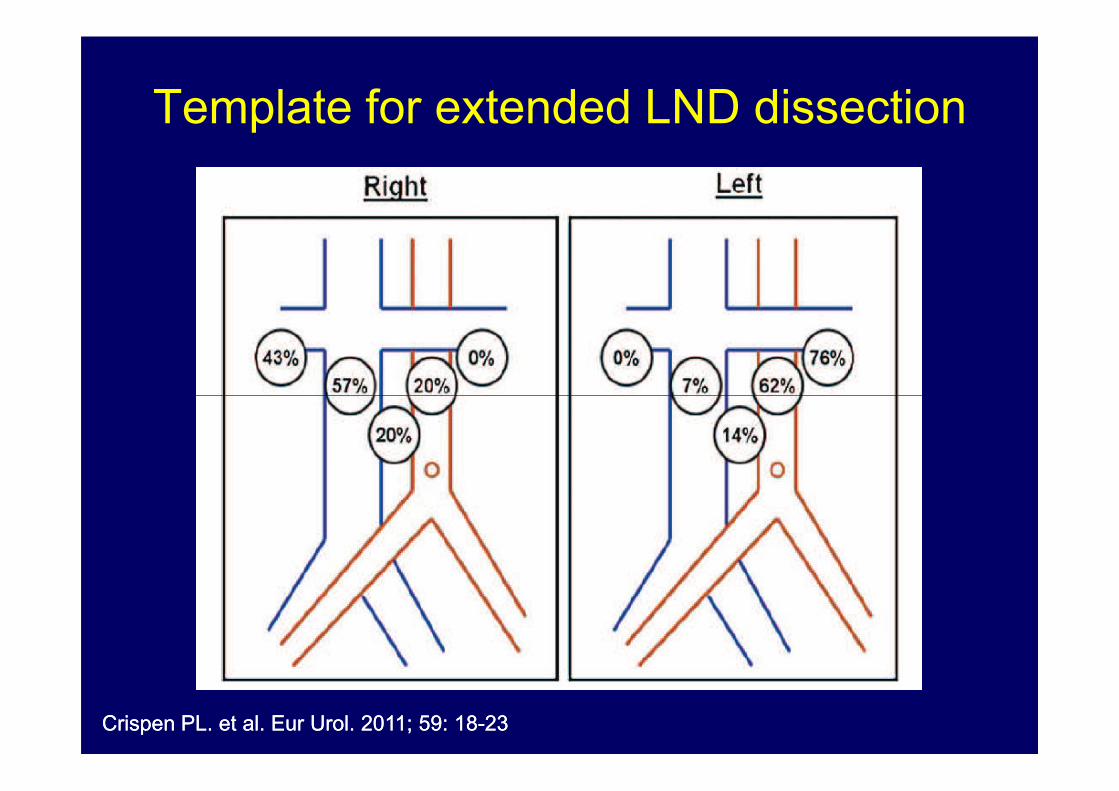
Template for extended LND dissection
CrispenCrispen PL. et al. PL. et al. EurEur UrolUrol. 2011; 59: 18. 2011; 59: 18--2323

•• The The availableavailable technologytechnology isis capablecapable of of
accuratelyaccurately identifyingidentifying onlyonly large large lymphlymph nodenode
metastasesmetastases
Imaging techniques and nodal
metastases staging
metastasesmetastases
•• PatientsPatients with (micro)with (micro)metastasesmetastases in in normalnormal--
sizedsized nodesnodes whowho mightmight benefit from LND benefit from LND
cannotcannot be be visualizedvisualized by by anyany of the of the availableavailable
imagingimaging techniquestechniques (US, CT, MRI)(US, CT, MRI)
CapitanioCapitanio U. et al. U. et al. EurEur UrolUrol. 2011; 60: 1212. 2011; 60: 1212--12201220
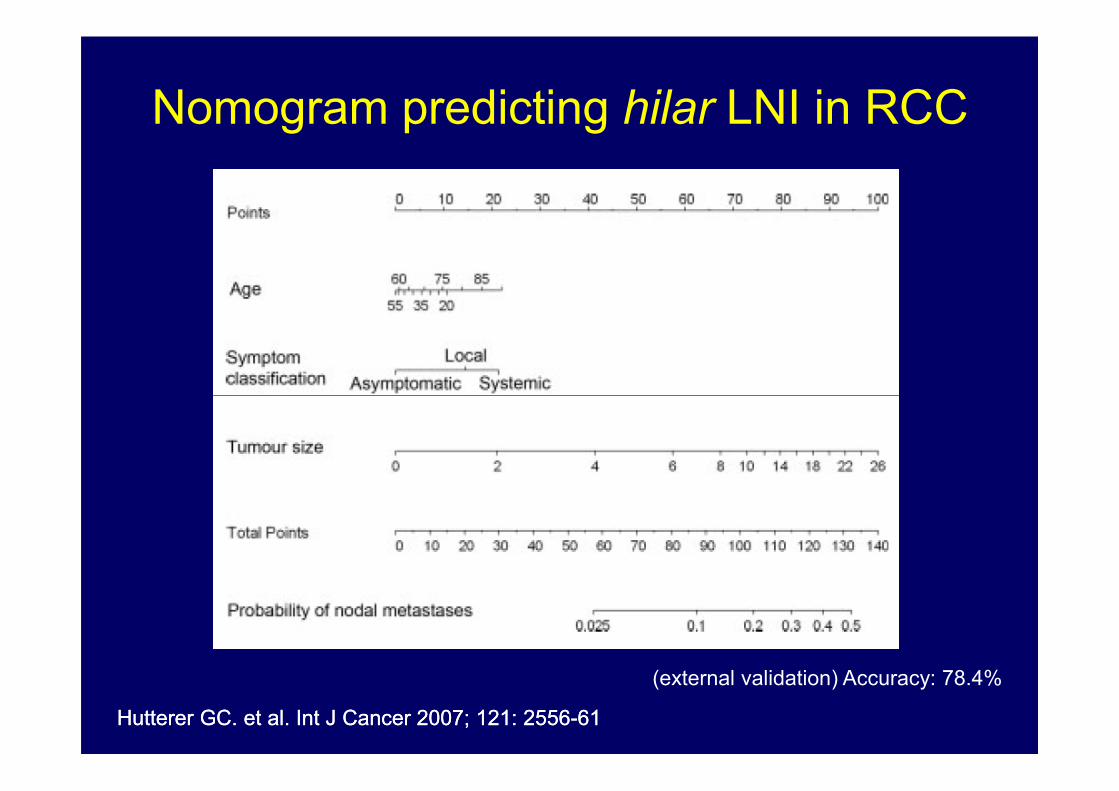
Nomogram predicting hilar LNI in RCC
HuttererHutterer GC. et al. GC. et al. IntInt J J CancerCancer 2007; 121: 25562007; 121: 2556--6161
(external validation) Accuracy: 78.4%

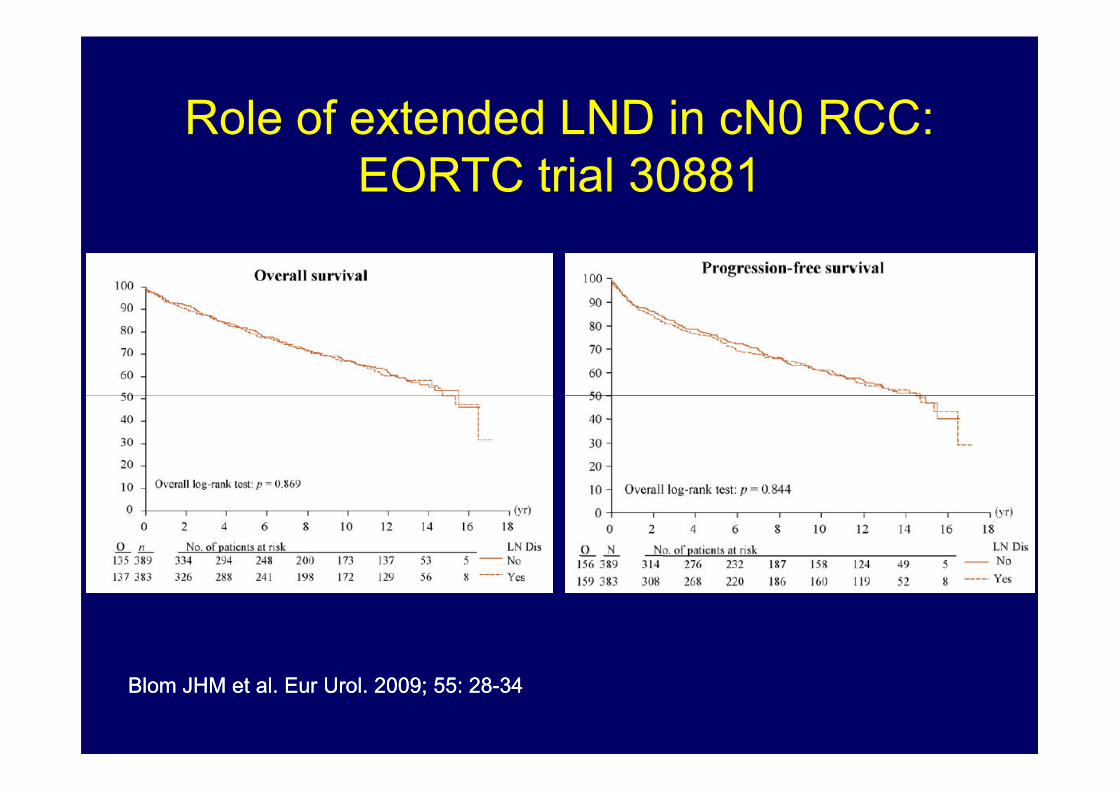
Role of extended LND in cN0 RCC:
EORTC trial 30881
772 cases
383 RN +
extended LND
1. Expected 5-year survival rate
85 %
BlomBlom JHM et al. JHM et al. EurEur UrolUrol. 2009; 55: 28. 2009; 55: 28--3434
772 cases
(T1-3, N0M0)389 RN
alone
1. Expected 5-year survival rate
70 %
Role of extended LND in cN0 RCC:
EORTC trial 30881
BlomBlom JHM et al. JHM et al. EurEur UrolUrol. 2009; 55: 28. 2009; 55: 28--3434
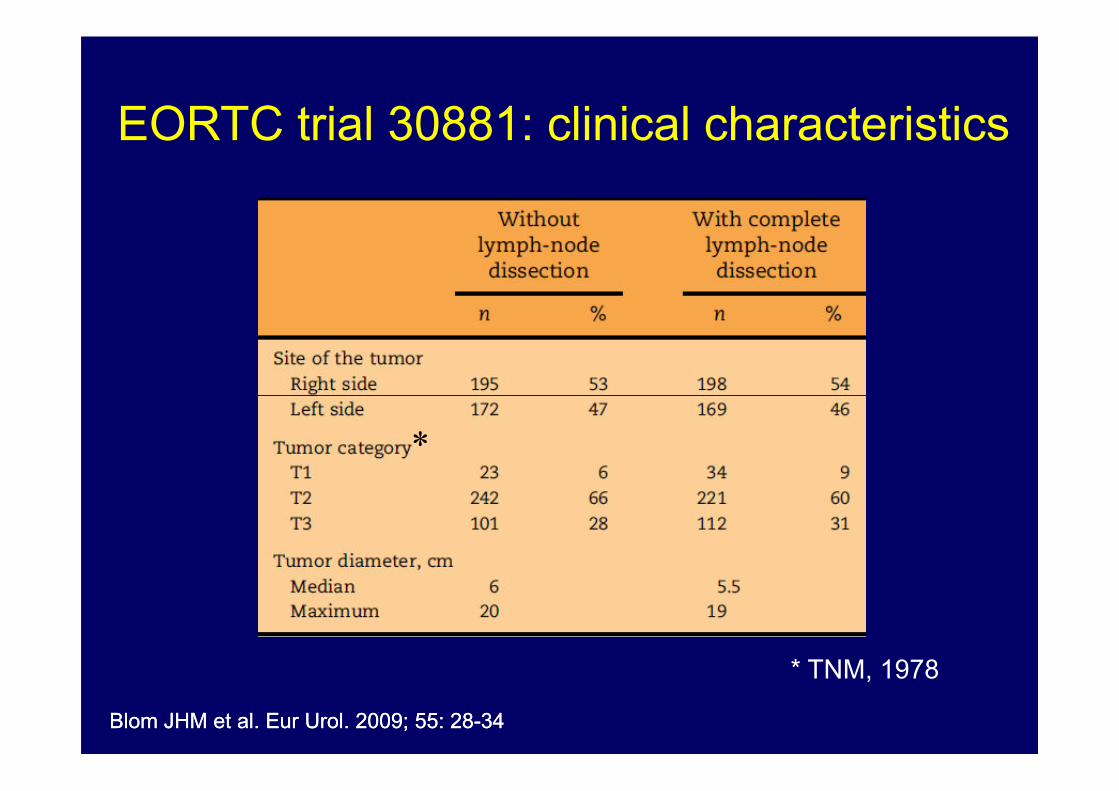
EORTC trial 30881: clinical characteristics
BlomBlom JHM et al. JHM et al. EurEur UrolUrol. 2009; 55: 28. 2009; 55: 28--3434
* TNM, 1978
*
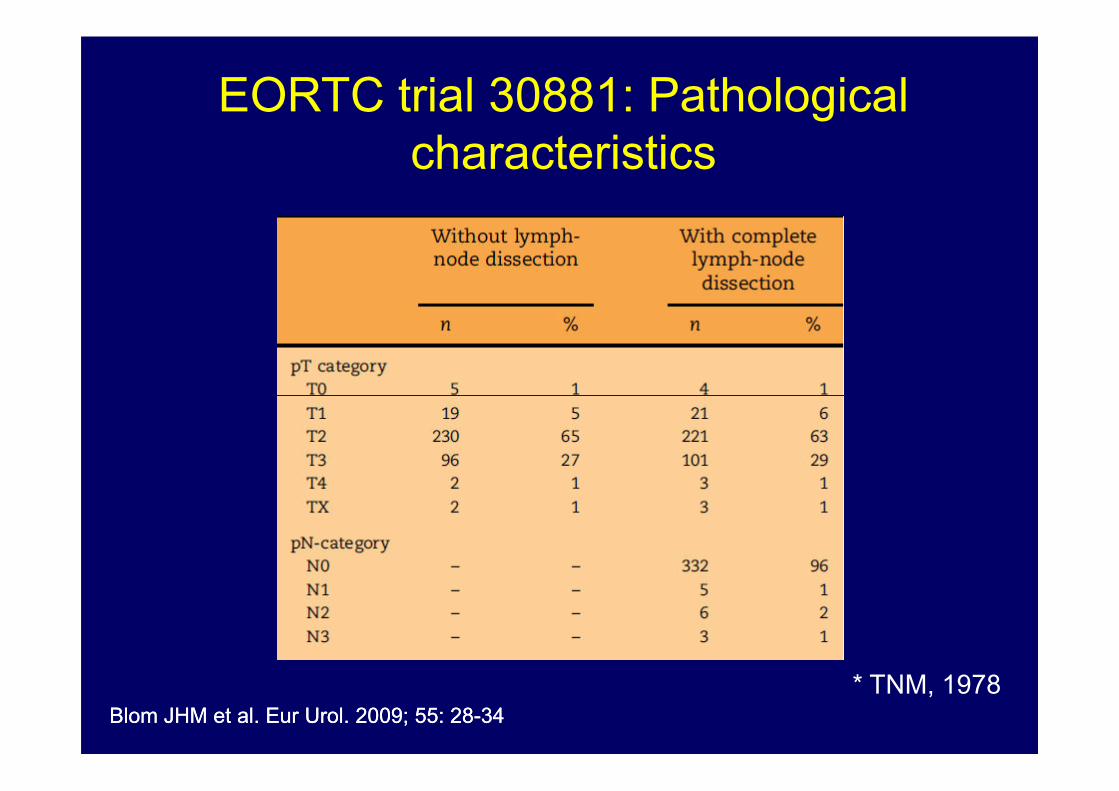
EORTC trial 30881: Pathological
characteristics
BlomBlom JHM et al. JHM et al. EurEur UrolUrol. 2009; 55: 28. 2009; 55: 28--3434
* TNM, 1978
*

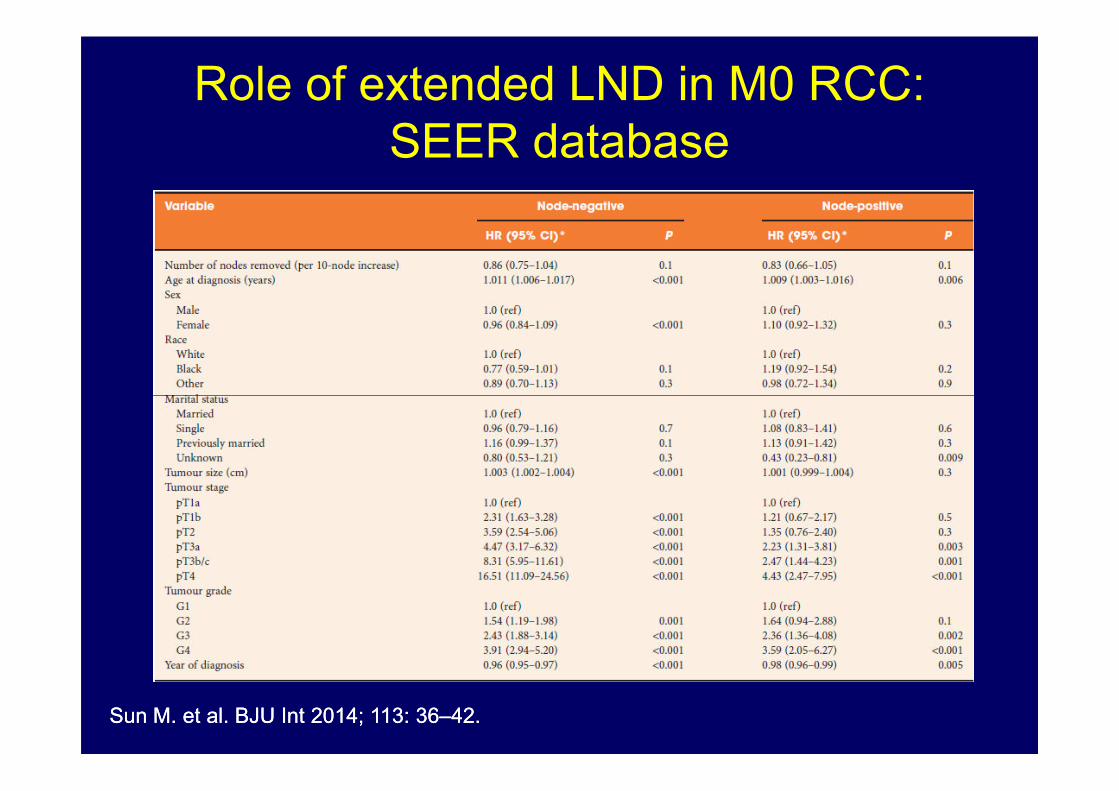
Role of extended LND in M0 RCC:
SEER database
SunSun M. et al. M. et al. BJU Int 2014; 113: 36BJU Int 2014; 113: 36––4242. .

Pathological LNI prevalence according to
pathological characteristics
CapitanioCapitanio U. et al. U. et al. EurEur UrolUrol. 2011; 60: 1212. 2011; 60: 1212--12201220
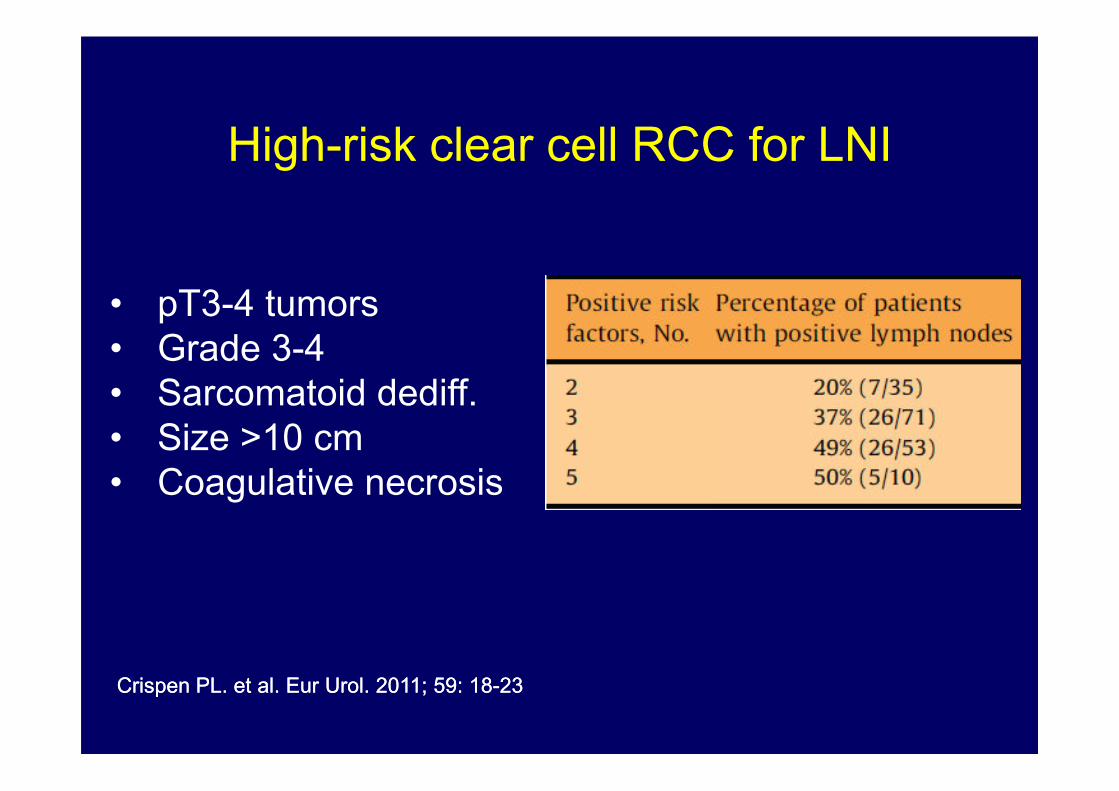
High-risk clear cell RCC for LNI
• pT3-4 tumors
• Grade 3-4
• Sarcomatoid dediff.
CrispenCrispen PL. et al. PL. et al. EurEur UrolUrol. 2011; 59: 18. 2011; 59: 18--2323
• Sarcomatoid dediff.
• Size >10 cm
• Coagulative necrosis

CapitanioCapitanio U. et al. BJU Inter. 2014; doi:10.1111/bju.12125U. et al. BJU Inter. 2014; doi:10.1111/bju.12125
*
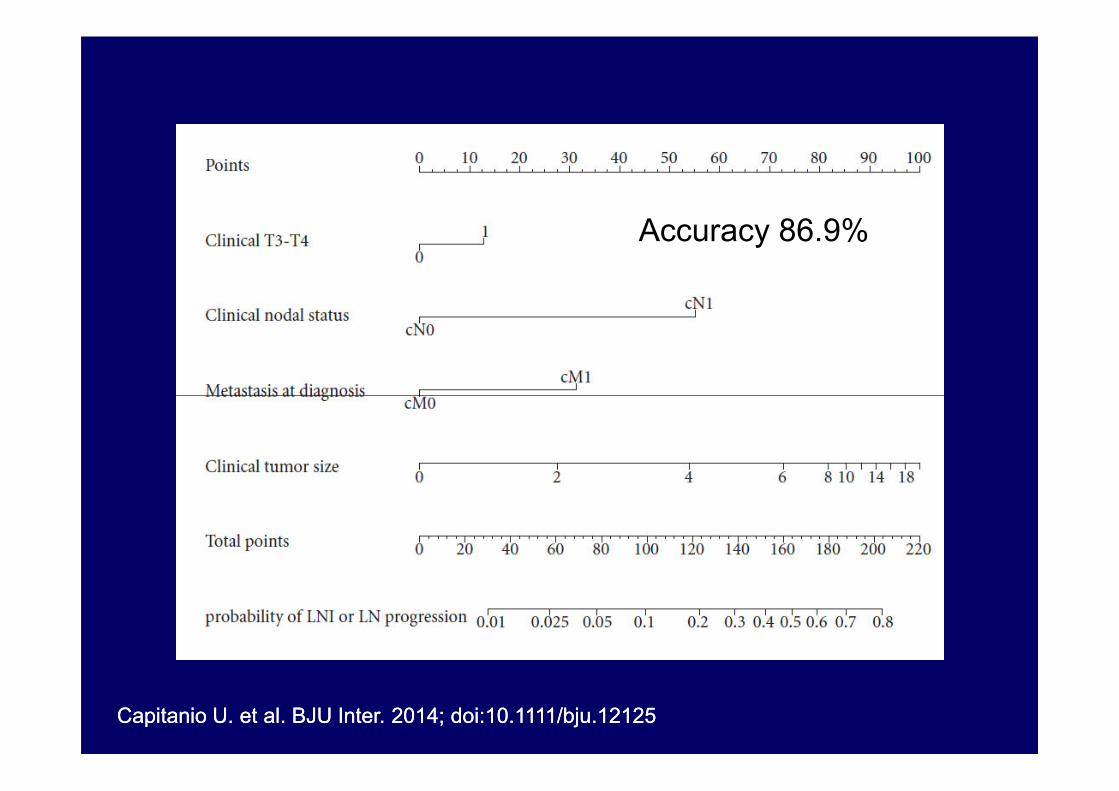
Accuracy 86.9%
CapitanioCapitanio U. et al. BJU Inter. 2014; doi:10.1111/bju.12125U. et al. BJU Inter. 2014; doi:10.1111/bju.12125
*

The use of a threshold of 3% would allow
the avoiding of ~50% of the LNDs
CapitanioCapitanio U. et al. BJU Inter. 2014; doi:10.1111/bju.12125U. et al. BJU Inter. 2014; doi:10.1111/bju.12125
*
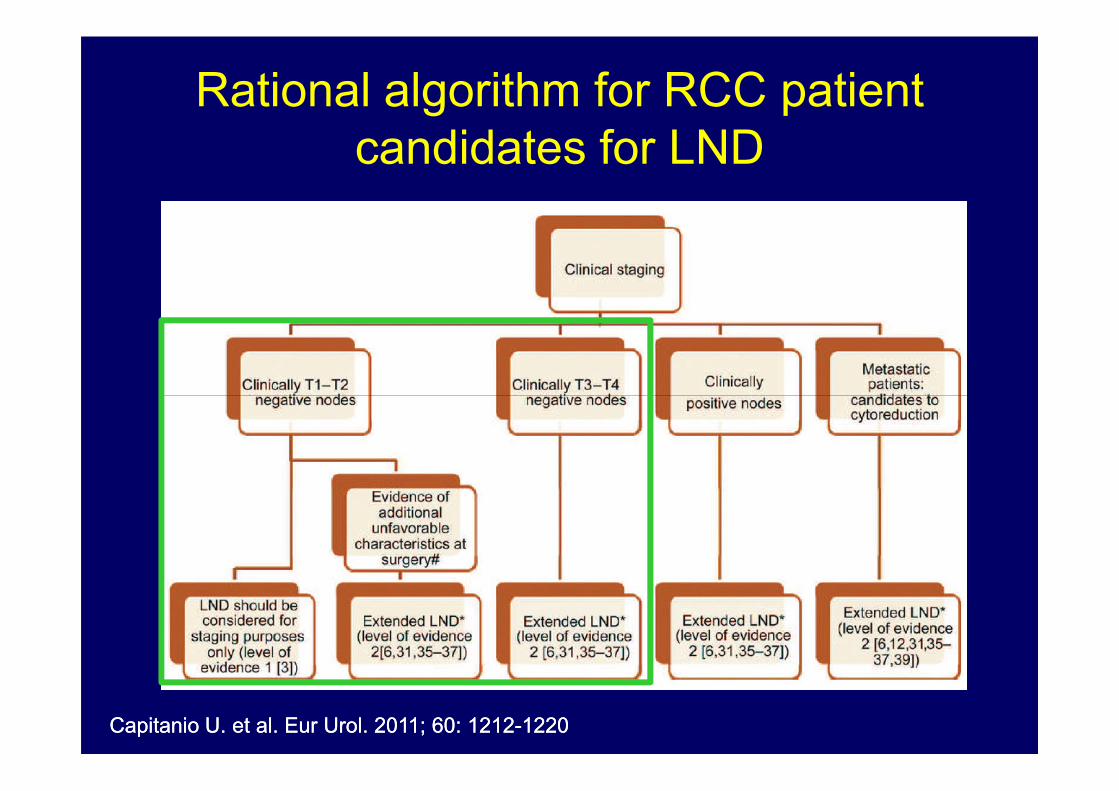
Rational algorithm for RCC patient
candidates for LND
CapitanioCapitanio U. et al. U. et al. EurEur UrolUrol. 2011; 60: 1212. 2011; 60: 1212--12201220
BekemaBekema HJ et al. HJ et al. EurEur UrolUrol. 2013; 64: 799. 2013; 64: 799--810810
*
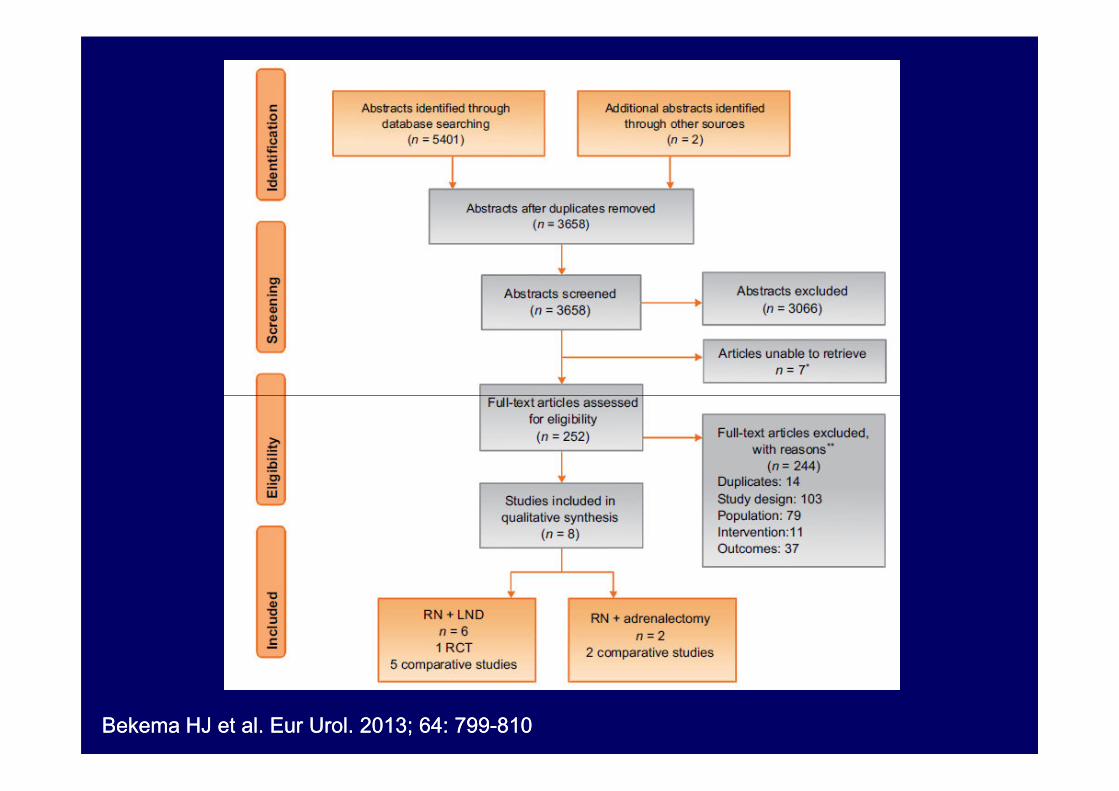
BekemaBekema HJ et al. HJ et al. EurEur UrolUrol. 2013; 64: 799. 2013; 64: 799--810810
*
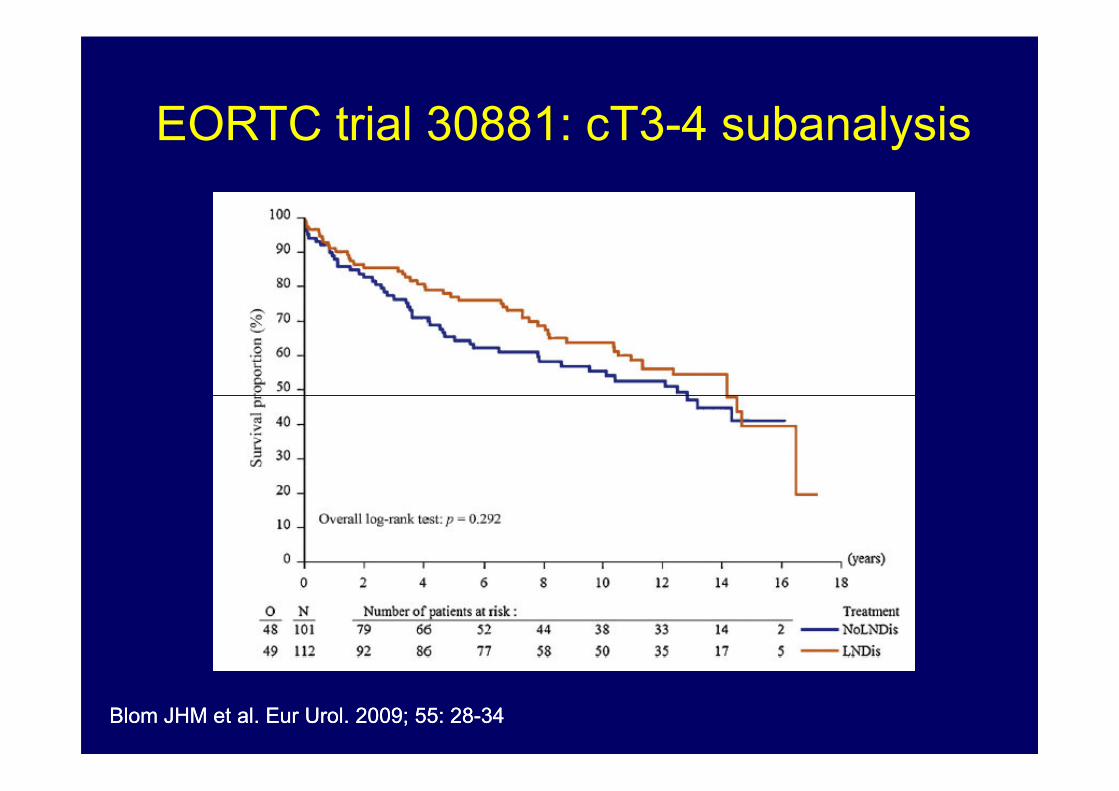
EORTC trial 30881: cT3-4 subanalysis
BlomBlom JHM et al. JHM et al. EurEur UrolUrol. 2009; 55: 28. 2009; 55: 28--3434
*
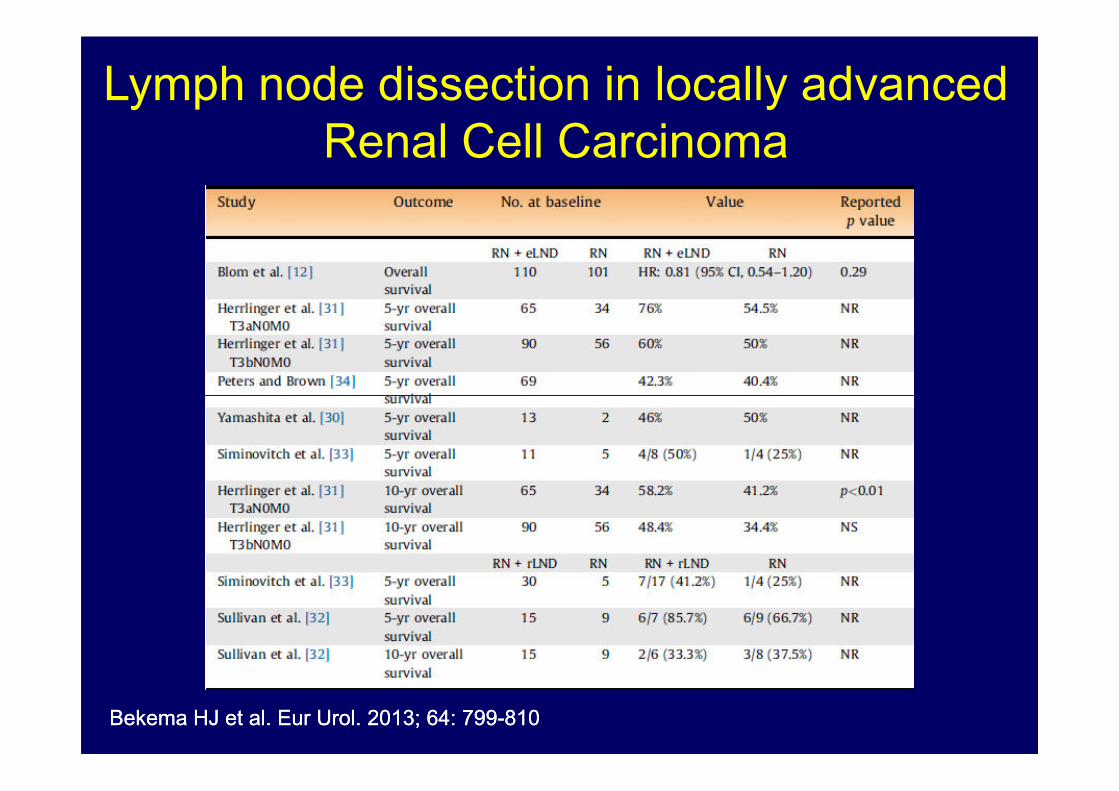
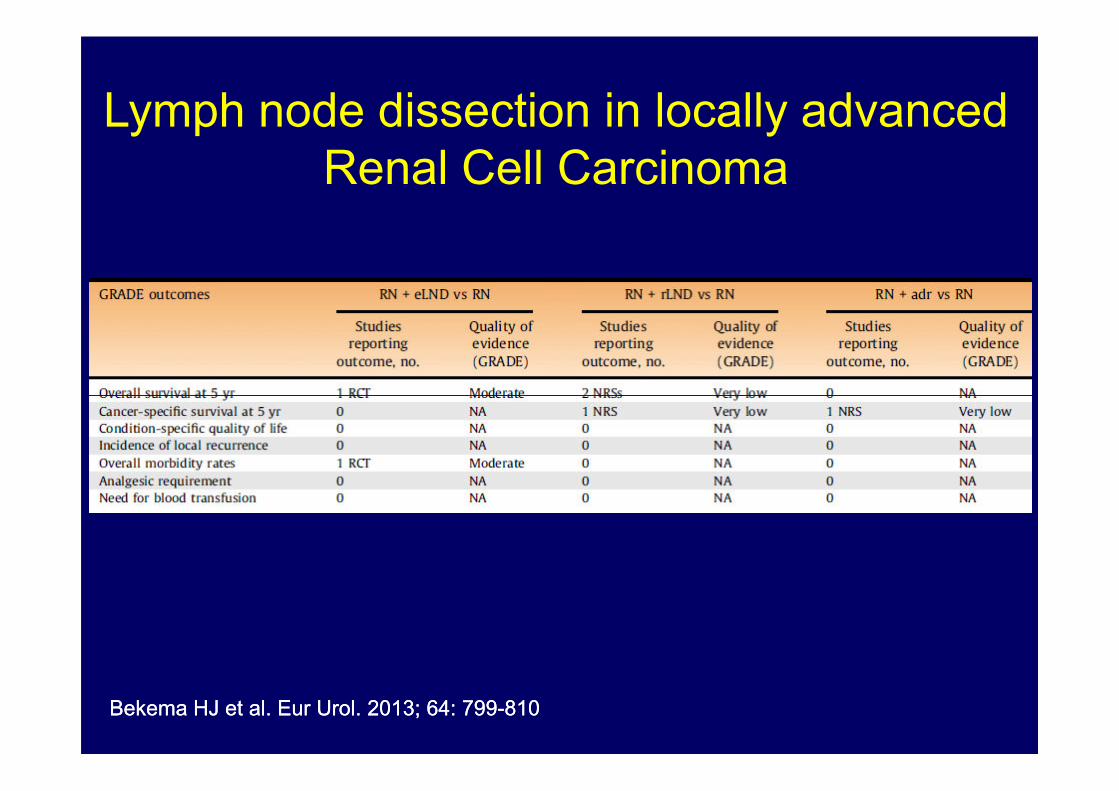
Lymph node dissection in locally advanced
Renal Cell Carcinoma
BekemaBekema HJ et al. HJ et al. EurEur UrolUrol. 2013; 64: 799. 2013; 64: 799--810810
*
Lymph node dissection in locally advanced
Renal Cell Carcinoma
BekemaBekema HJ et al. HJ et al. EurEur UrolUrol. 2013; 64: 799. 2013; 64: 799--810810
*

• There is insufficient evidence to draw any conclusions on
BekemaBekema HJ et al. HJ et al. EurEur UrolUrol. 2013; 64: 799. 2013; 64: 799--810810
*
• There is insufficient evidence to draw any conclusions on
oncologic outcomes for patients having concomitant LND
compared with patients having RN alone for cT3–T4N0M0
RCC
• The quality of evidence is generally low and the
results potentially biased.
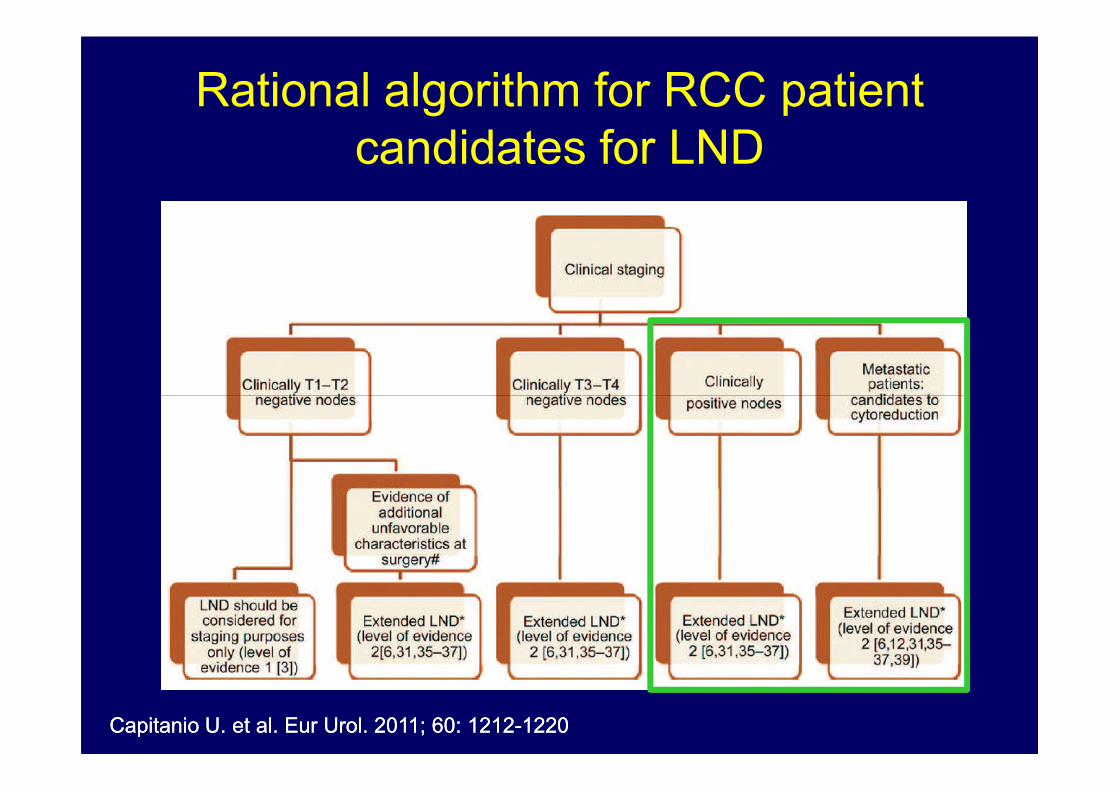
Rational algorithm for RCC patient
candidates for LND
CapitanioCapitanio U. et al. U. et al. EurEur UrolUrol. 2011; 60: 1212. 2011; 60: 1212--12201220

Role of extended LND in cN+ RCC
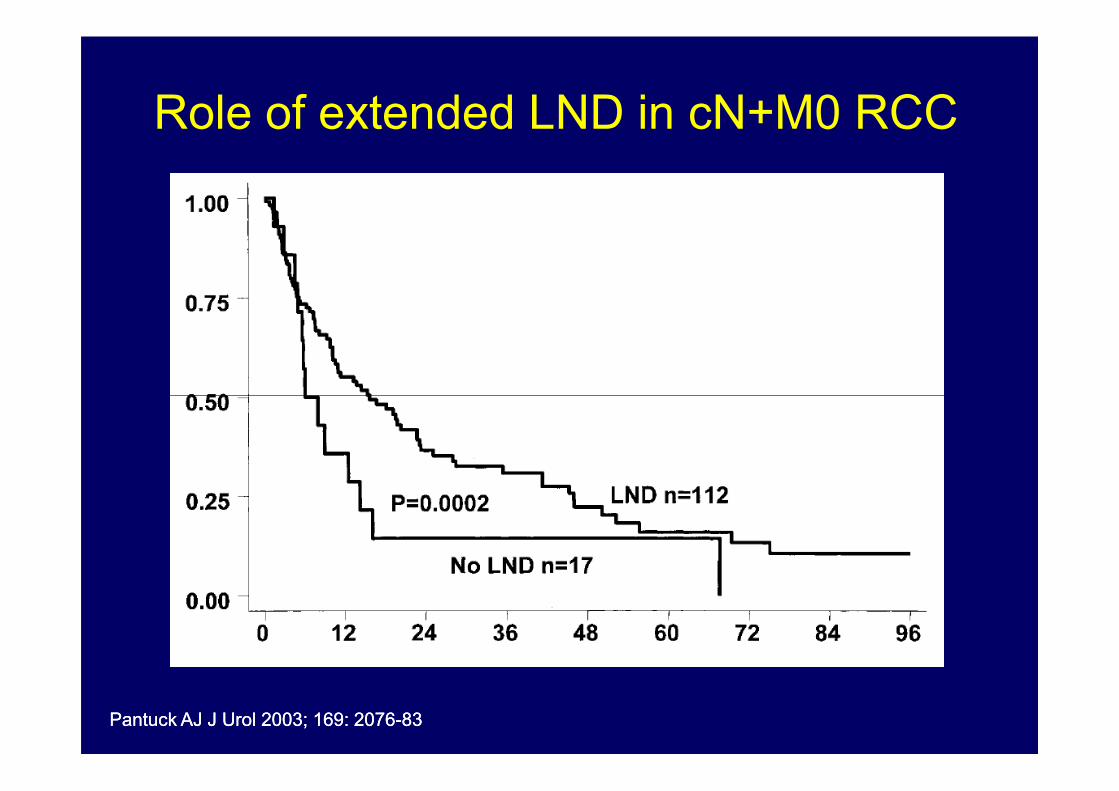
Role of extended LND in cN+M0 RCC
Pantuck AJ J Urol 2003; 169: 2076Pantuck AJ J Urol 2003; 169: 2076--8383
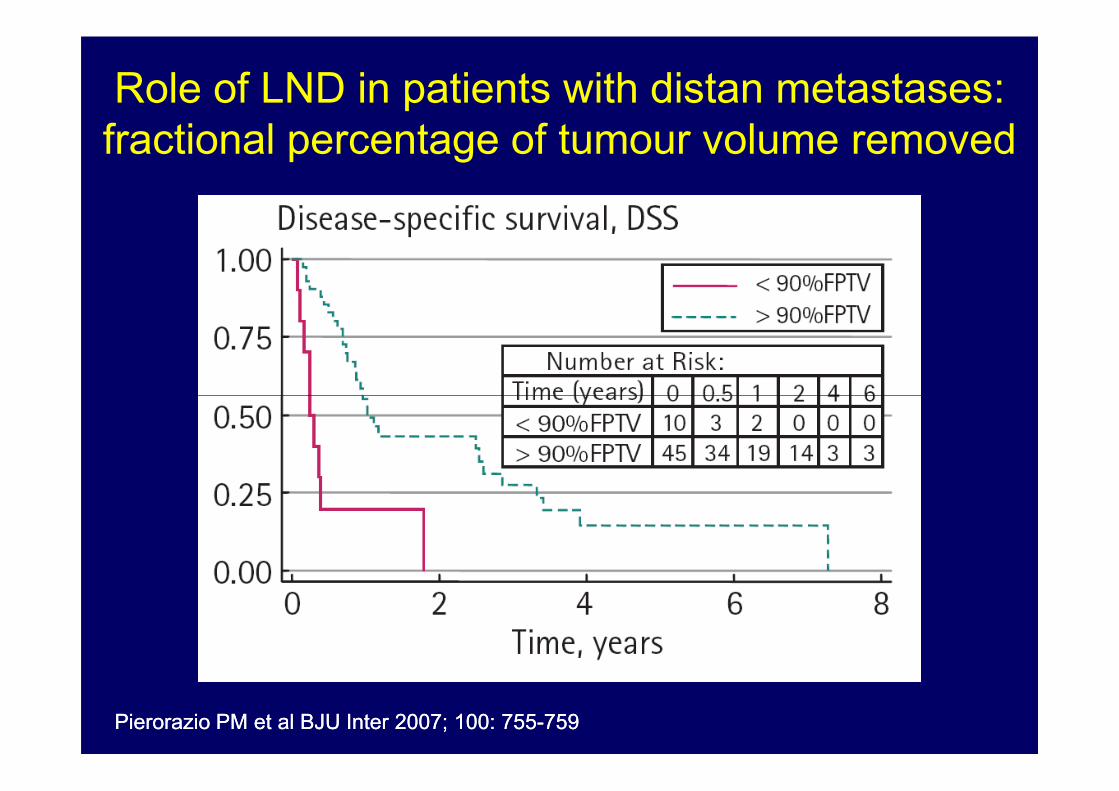
Role of LND in patients with distan metastases:
fractional percentage of tumour volume removed
PierorazioPierorazio PM et al BJU Inter 2007; 100: 755PM et al BJU Inter 2007; 100: 755--759759
Rational algorithm for RCC patient
candidates for LND
• cT2b (>10 cm); N0
• cT3-4; N0• cT3-4; N0
• cN+
• M+


Russell CM et al. J Russell CM et al. J UrolUrol. 2014; (in press). 2014; (in press)
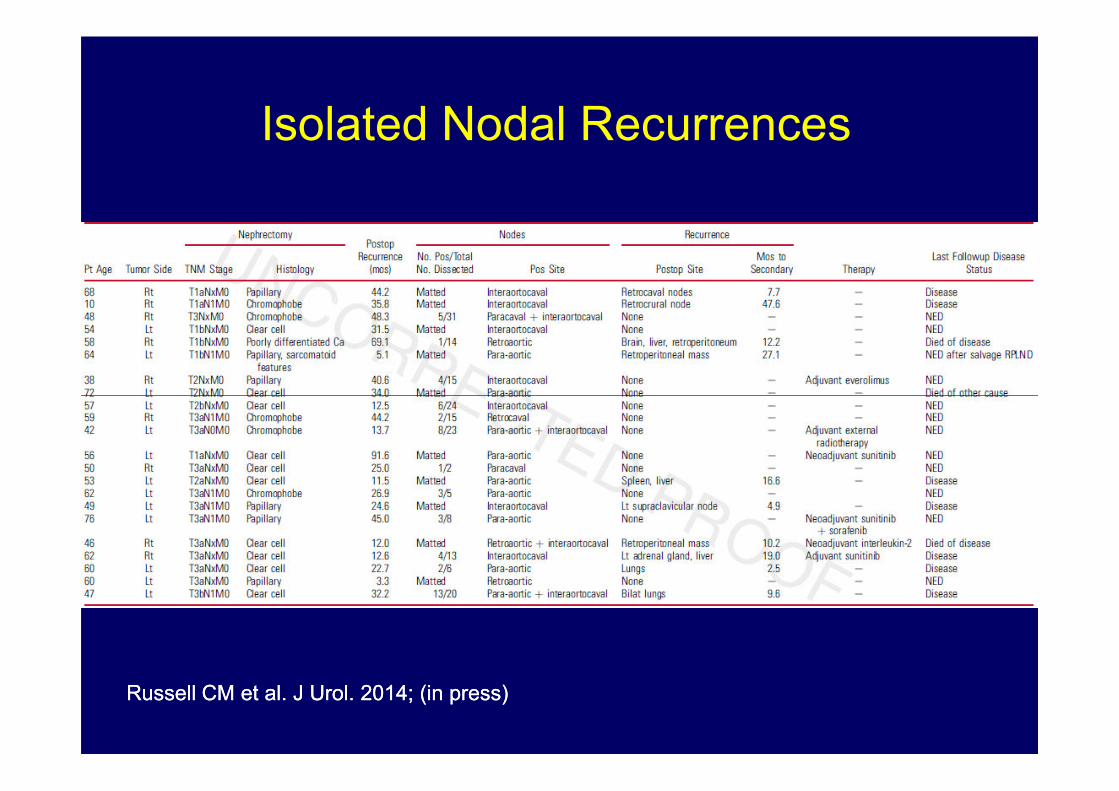
Isolated Nodal Recurrences
Russell CM et al. J Russell CM et al. J UrolUrol. 2014; (in press). 2014; (in press)
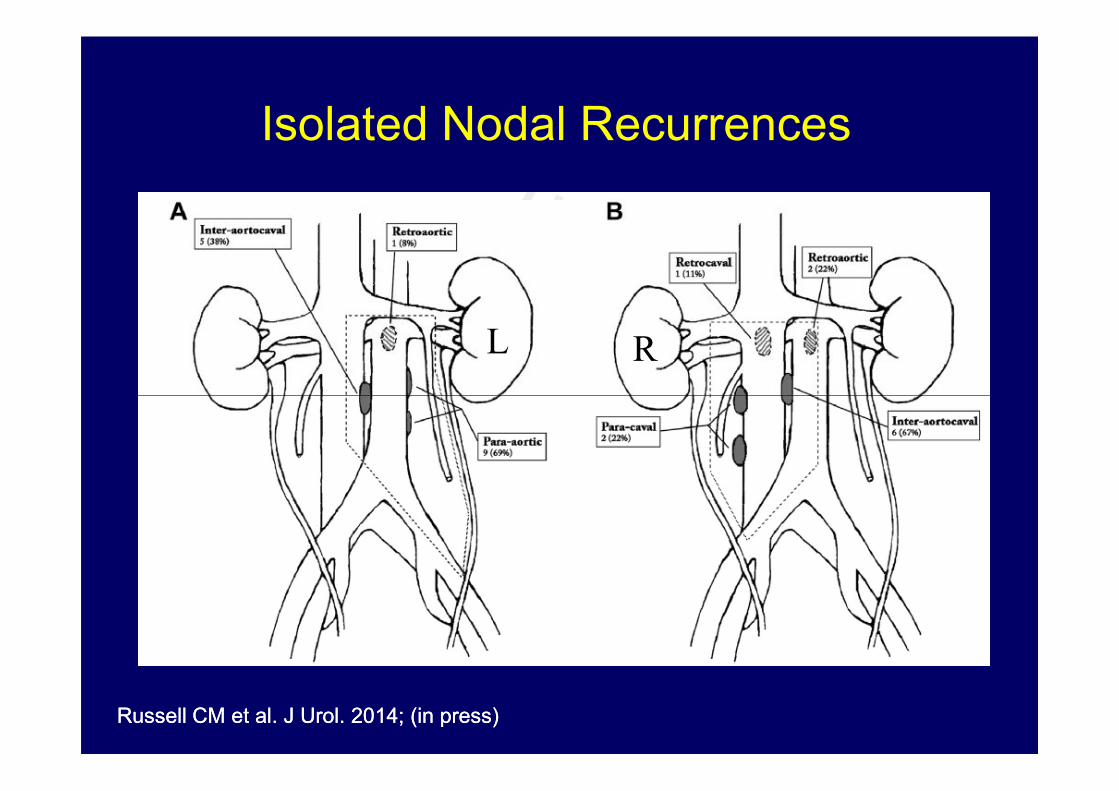
Isolated Nodal Recurrences
L R
Russell CM et al. J Russell CM et al. J UrolUrol. 2014; (in press). 2014; (in press)
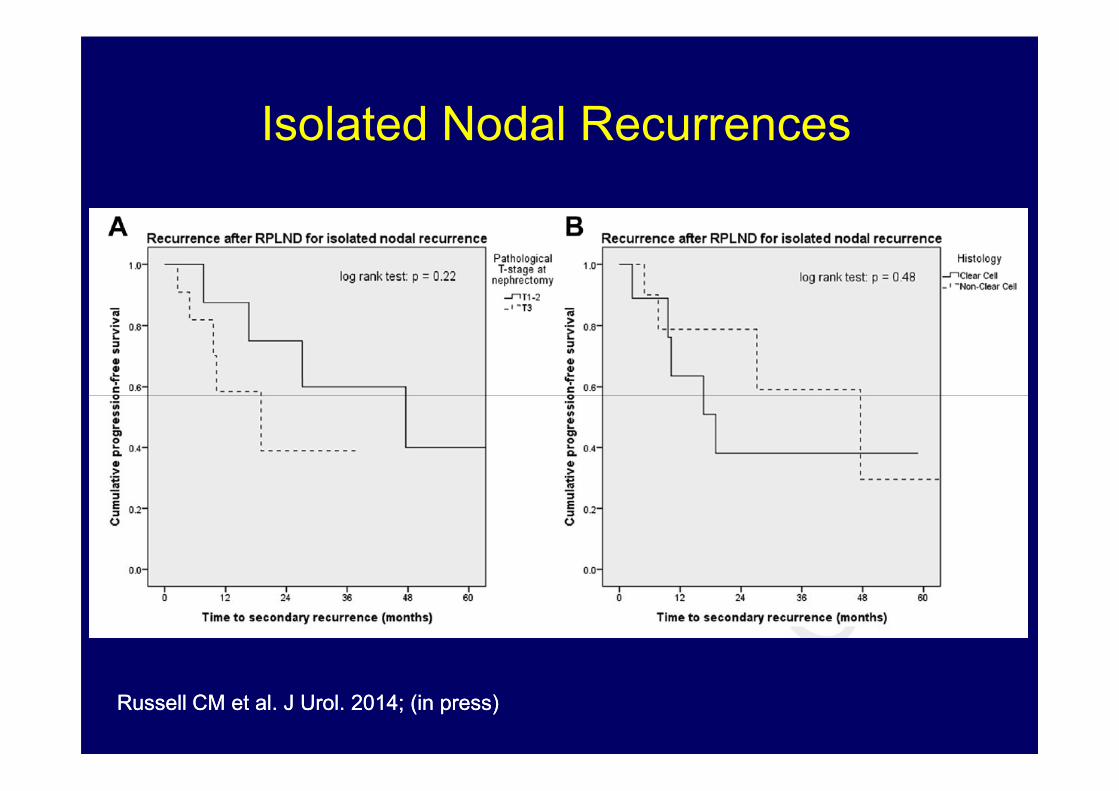
Isolated Nodal Recurrences
Russell CM et al. J Russell CM et al. J UrolUrol. 2014; (in press). 2014; (in press)

• Surgical resection represents the best curative
option for patients who present with isolated
retroperitoneal lymph node recurrence of RCC
Isolated Nodal Recurrences
Russell CM et al. J Russell CM et al. J UrolUrol. 2014; (in press). 2014; (in press)
• Durable postoperative progression-free survival
is attainable in many patients regardless of
histology or clinical TNM stage
Role of Nephrectomy in mRCC
• Curative (Nephrectomy + metastasectomy)
• Cytoreductive (To resect primary tumor in the
prior to the initiation of systemic therapy for
unresectable metastases)unresectable metastases)
• Palliative (To improve symptoms)
- pain related to the kidney mass
- intractable hematuria
- paraneoplastic syndrome
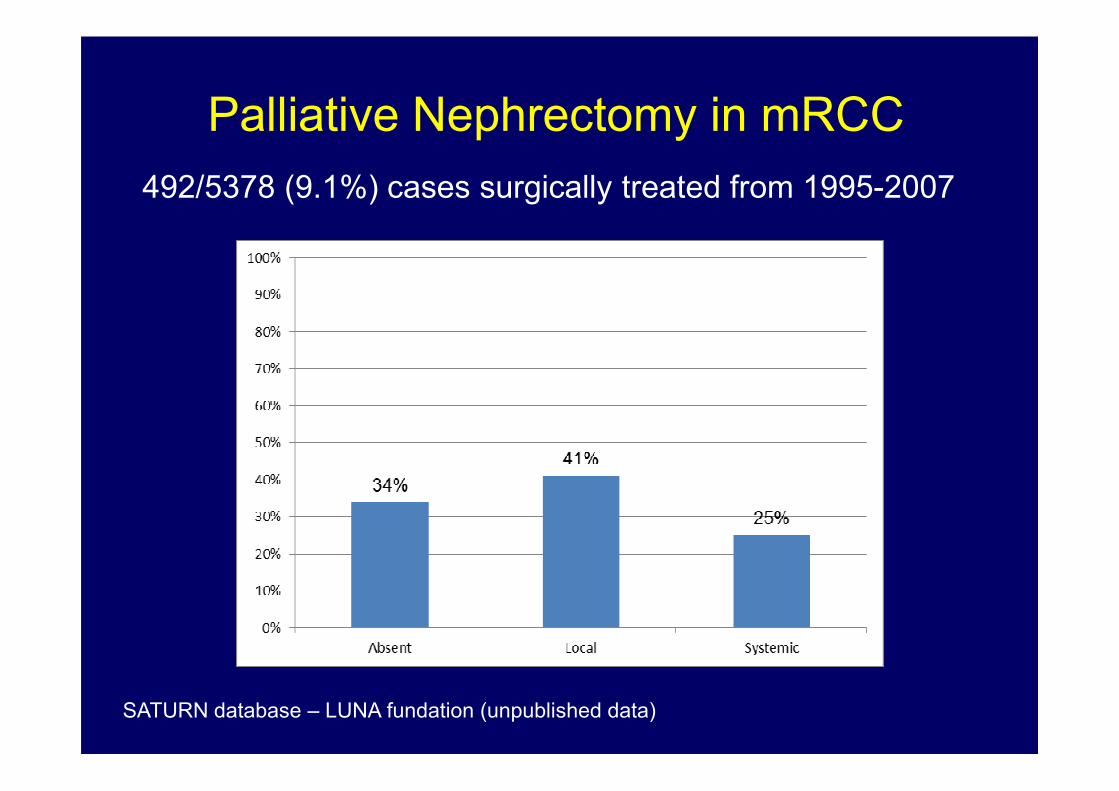
Palliative Nephrectomy in mRCC
492/5378 (9.1%) cases surgically treated from 1995-2007
SATURN database – LUNA fundation (unpublished data)
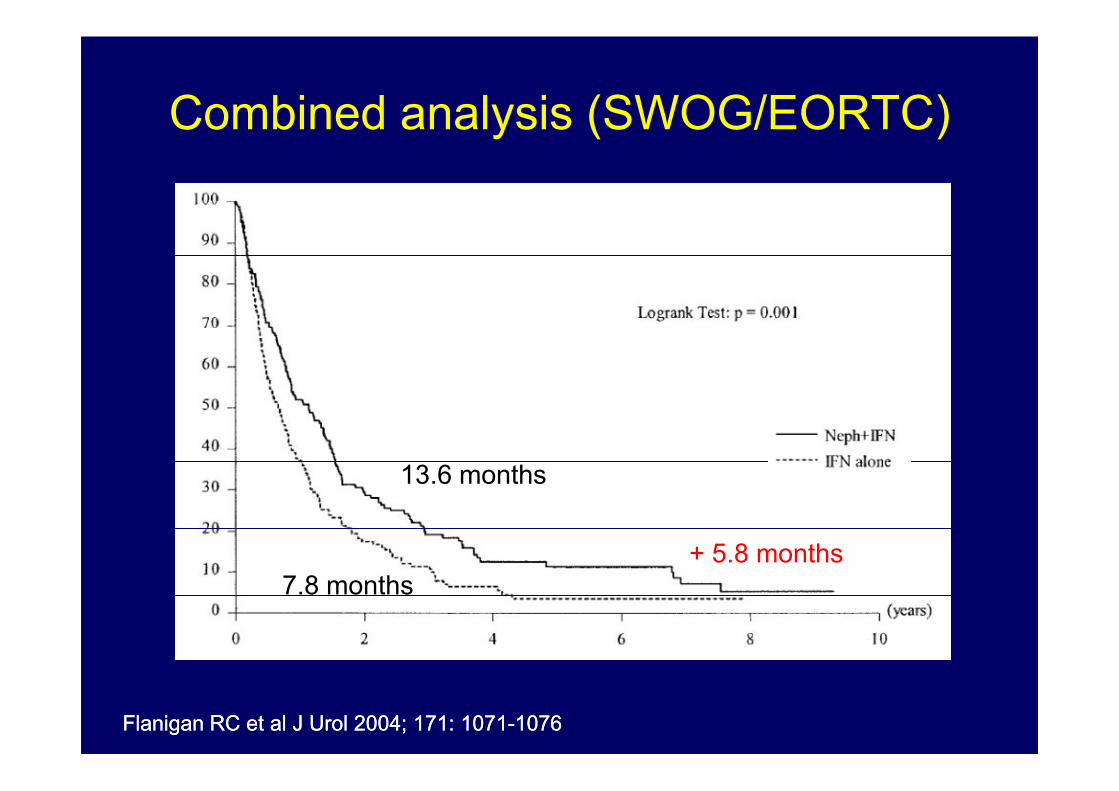
Combined analysis (SWOG/EORTC)
Flanigan RC et al J Urol 2004; 171: 1071Flanigan RC et al J Urol 2004; 171: 1071--10761076
13.6 months
7.8 months
+ 5.8 months
• Cytoreductive nephrectomy significantly improve
overall survival in patients with mRCC treated
with IFN-alpha independent of patients
Combined analysis (SWOG/EORTC)
- performance status
- site of metastasis (lung)
- presence of measurable disease
- (?) single Vs multiple metastases
Flanigan RC et al J Urol 2004; 171: 1071Flanigan RC et al J Urol 2004; 171: 1071--10761076
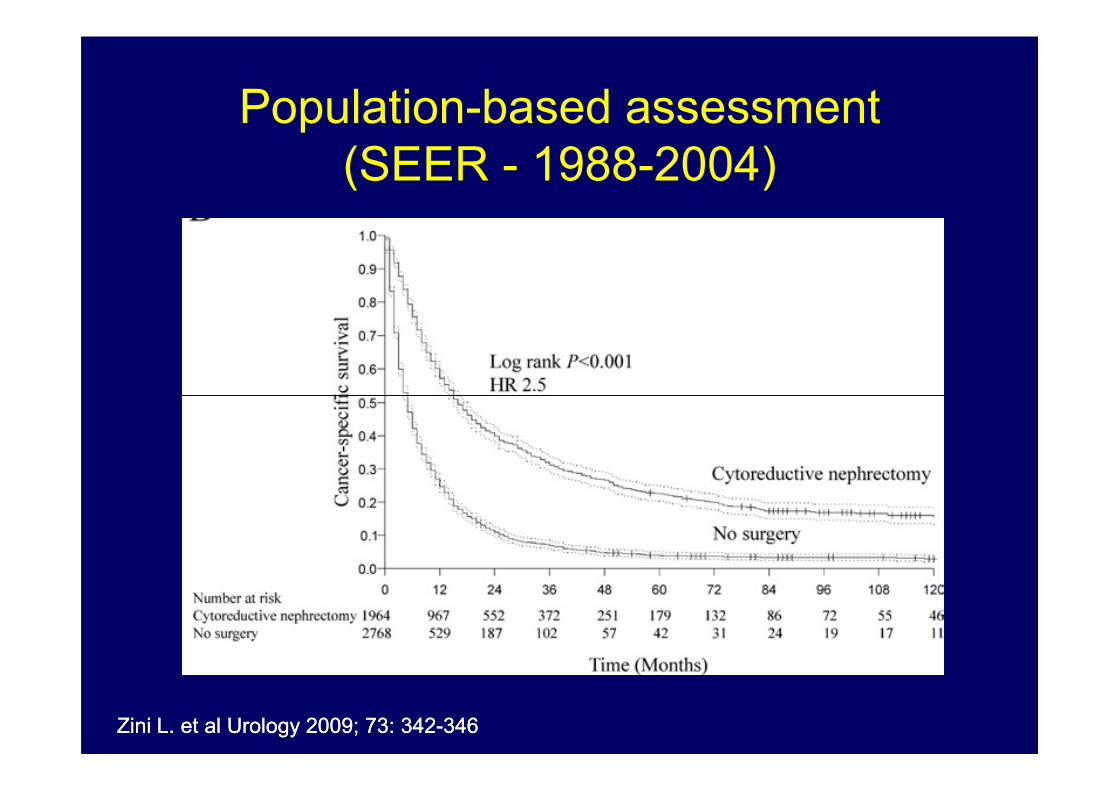
Population-based assessment
(SEER - 1988-2004)
Zini L. et al Urology 2009; 73: 342Zini L. et al Urology 2009; 73: 342--346346
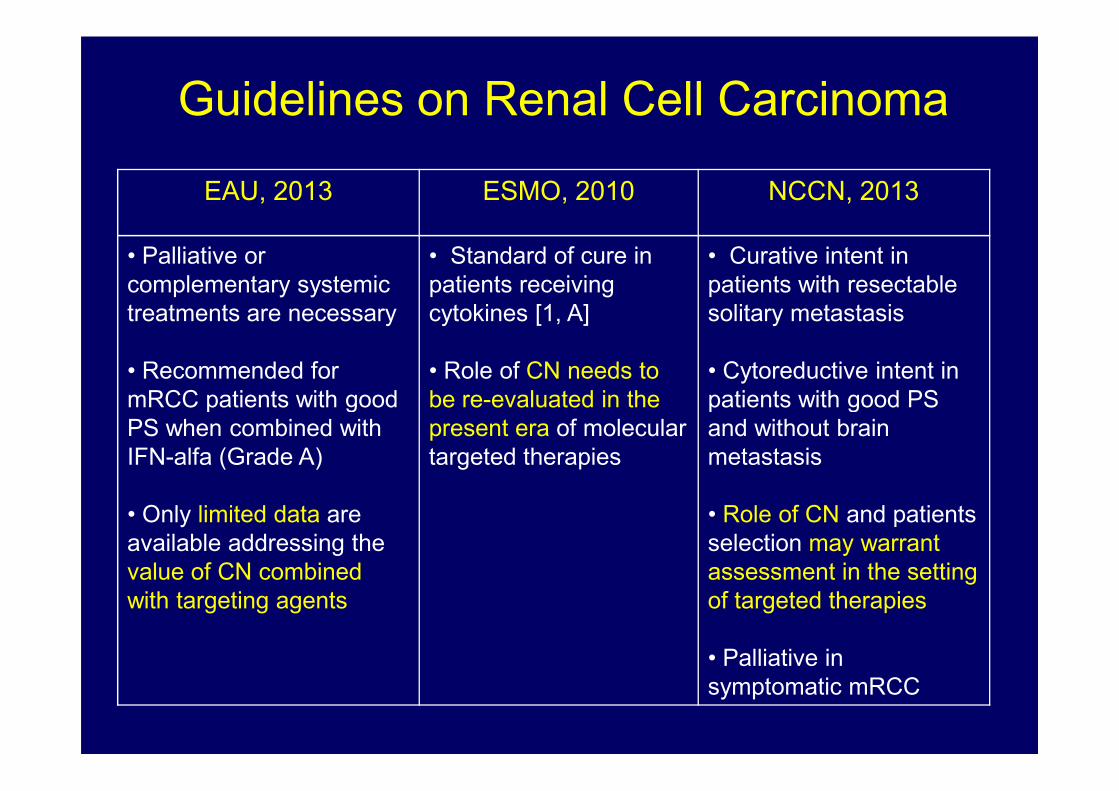
Guidelines on Renal Cell Carcinoma
EAU, 2013 ESMO, 2010 NCCN, 2013
• Palliative or
complementary systemic
treatments are necessary
• Recommended for
mRCC patients with good
• Standard of cure in
patients receiving
cytokines [1, A]
• Role of CN needs to
be re-evaluated in the
• Curative intent in
patients with resectable
solitary metastasis
• Cytoreductive intent in
patients with good PS mRCC patients with good
PS when combined with
IFN-alfa (Grade A)
• Only limited data are
available addressing the
value of CN combined
with targeting agents
be re-evaluated in the
present era of molecular
targeted therapies
patients with good PS
and without brain
metastasis
• Role of CN and patients
selection may warrant
assessment in the setting
of targeted therapies
• Palliative in
symptomatic mRCC

Cytoreductive Nephrectomy in the era of
Targeted molecular agents
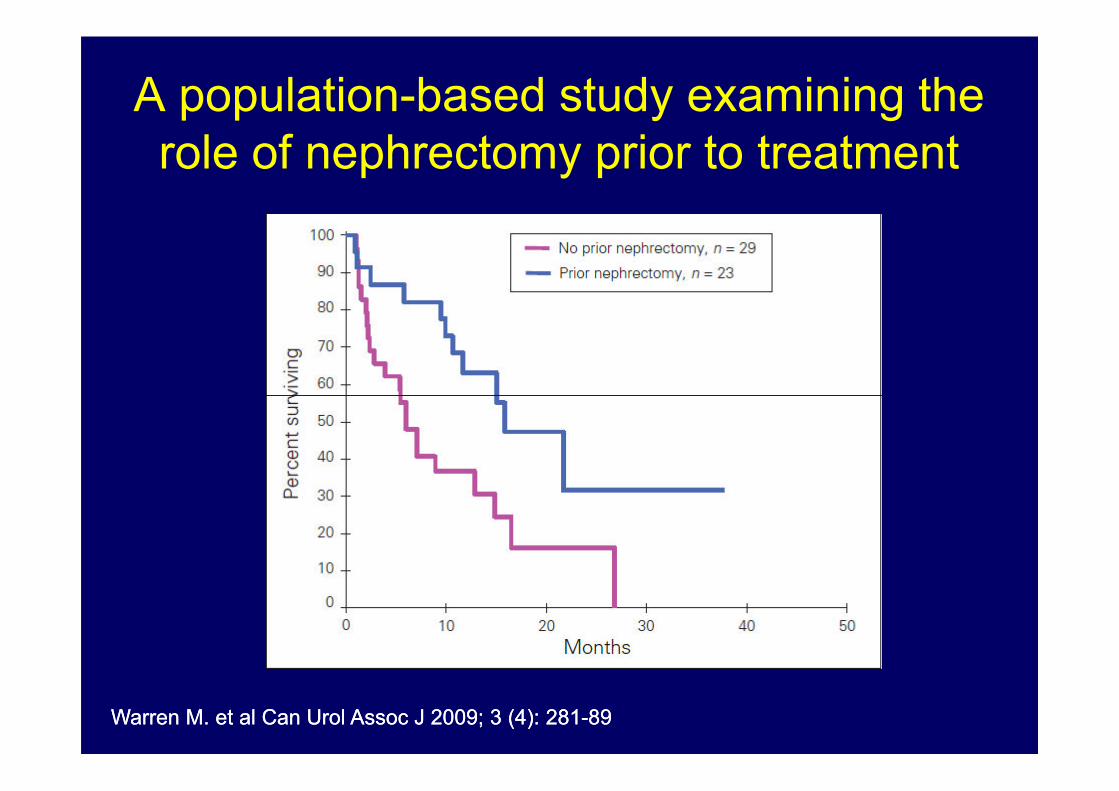
A population-based study examining the
role of nephrectomy prior to treatment
Warren M. et al Can Warren M. et al Can UrolUrol AssocAssoc J 2009; 3 (4): 281J 2009; 3 (4): 281--8989
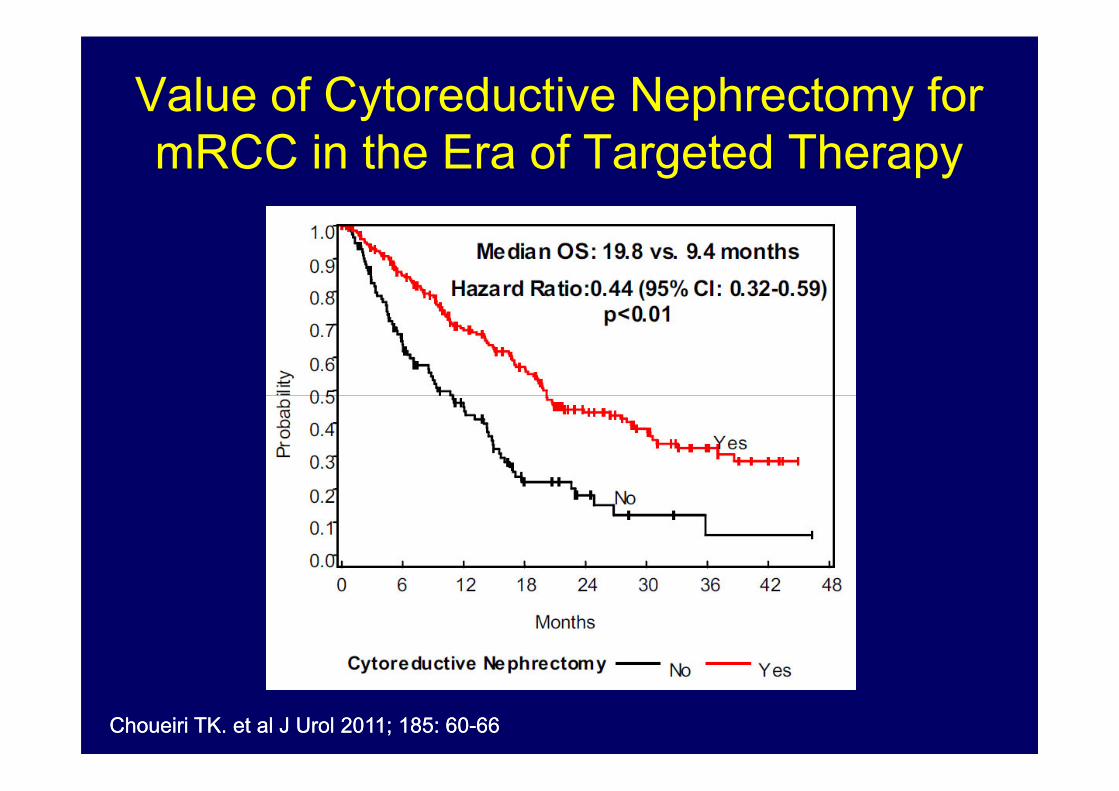
Value of Cytoreductive Nephrectomy for
mRCC in the Era of Targeted Therapy
ChoueiriChoueiri TK. et al J TK. et al J UrolUrol 2011; 185: 602011; 185: 60--6666
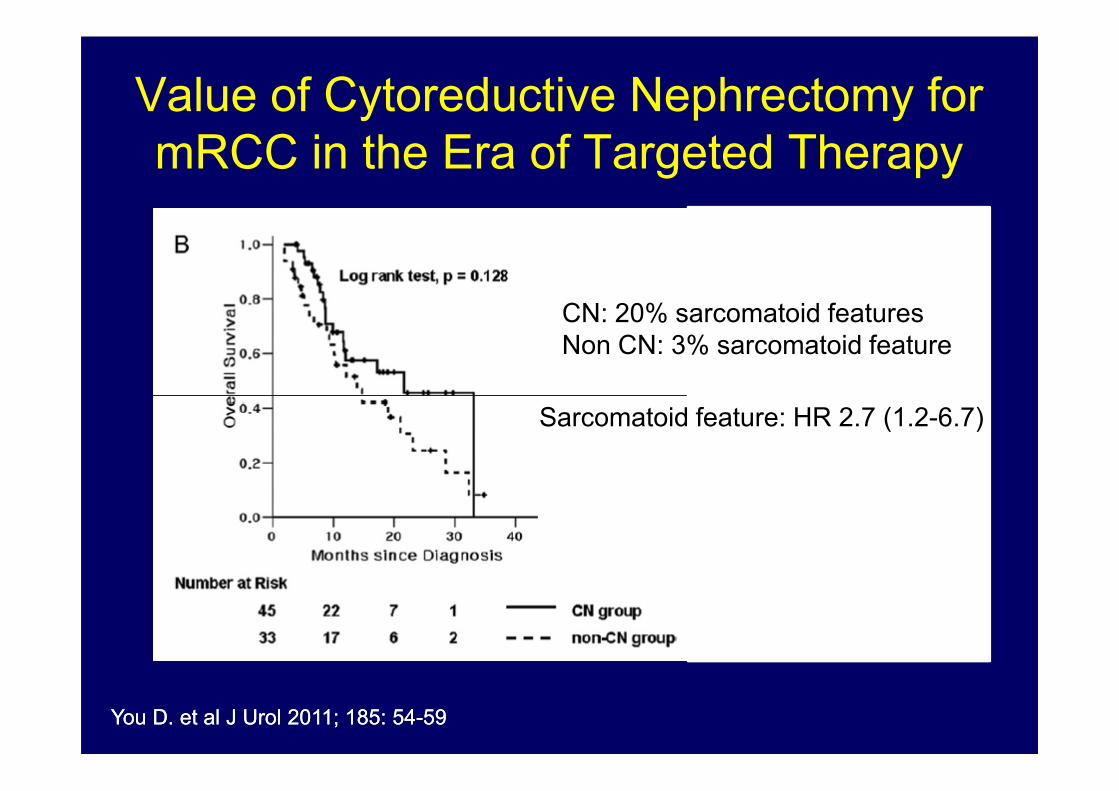
Value of Cytoreductive Nephrectomy for
mRCC in the Era of Targeted Therapy
CN: 20% sarcomatoid features
Non CN: 3% sarcomatoid feature
YouYou D. et al J D. et al J UrolUrol 2011; 185: 542011; 185: 54--5959
Sarcomatoid feature: HR 2.7 (1.2-6.7)
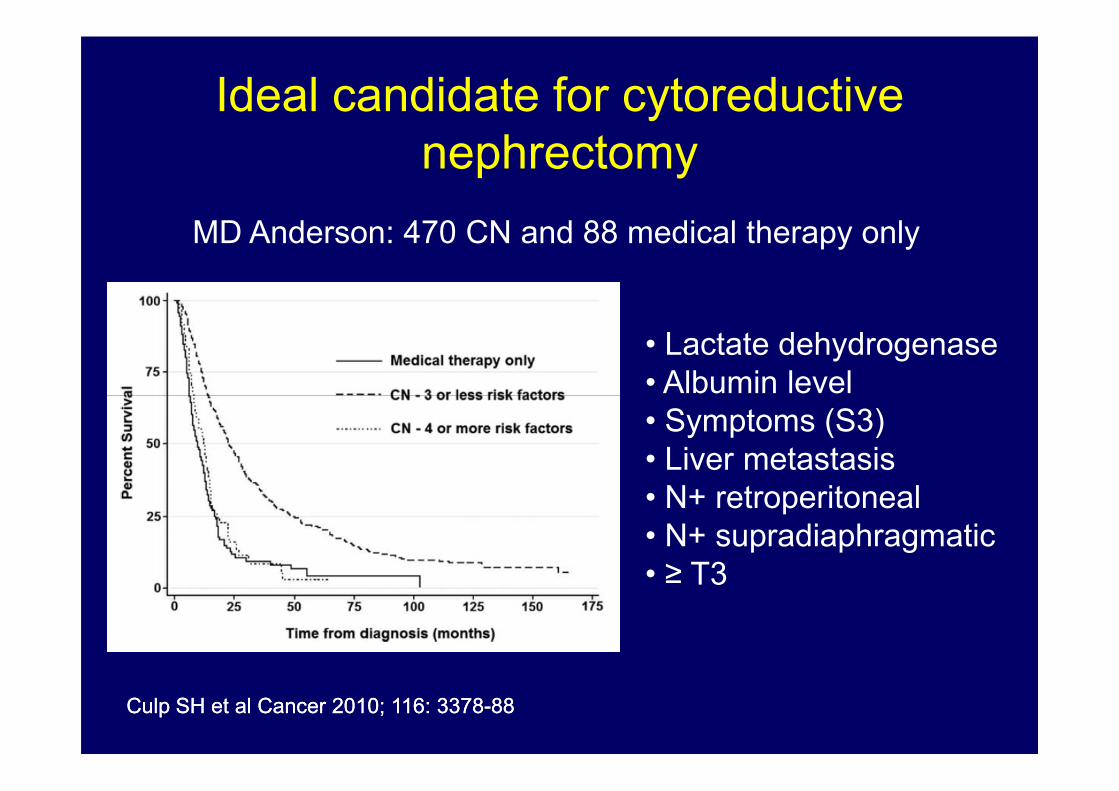
Ideal candidate for cytoreductive
nephrectomy
• Lactate dehydrogenase
• Albumin level
MD Anderson: 470 CN and 88 medical therapy only
• Albumin level
• Symptoms (S3)
• Liver metastasis
• N+ retroperitoneal
• N+ supradiaphragmatic
• ≥ T3
CulpCulp SH et al SH et al CancerCancer 2010; 116: 33782010; 116: 3378--8888
Candidate for cytoreductive nephrectomy
• Good surgical risk (good performance status)
• Limited metastatic tumor burden to lung or bone
• Extensive metastatic disease with systemic
therapy planned
• Symptoms related to the primary tumor
NCCN NCCN GuidelinesGuidelines, 2013, 2013
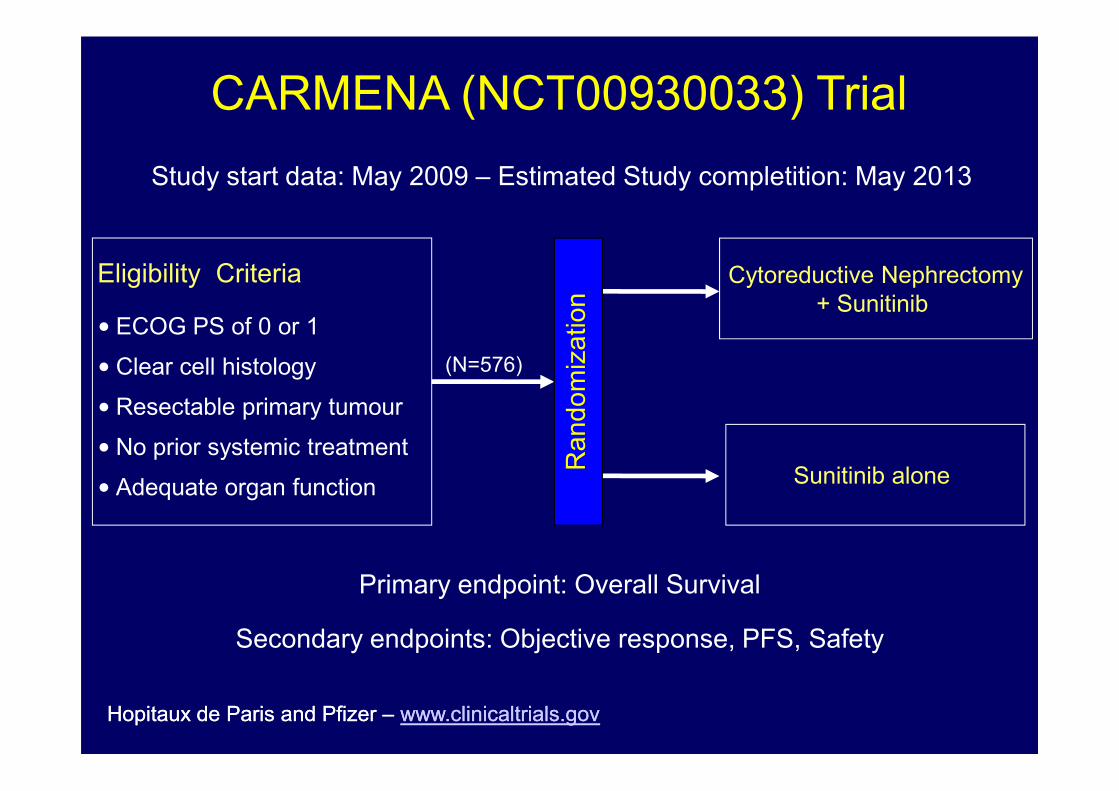
Eligibility Criteria
• ECOG PS of 0 or 1
• Clear cell histology
• Resectable primary tumour
Cytoreductive Nephrectomy
+ Sunitinib
Ra
nd
om
iza
tio
n
(N=576)
CARMENA (NCT00930033) Trial
Study start data: May 2009 – Estimated Study completition: May 2013
HopitauxHopitaux de Paris and Pfizer de Paris and Pfizer –– www.clinicaltrials.govwww.clinicaltrials.gov
Primary endpoint: Overall Survival
Secondary endpoints: Objective response, PFS, Safety
• Resectable primary tumour
• No prior systemic treatment
• Adequate organ functionSunitinib alone
Ra
nd
om
iza
tio
n
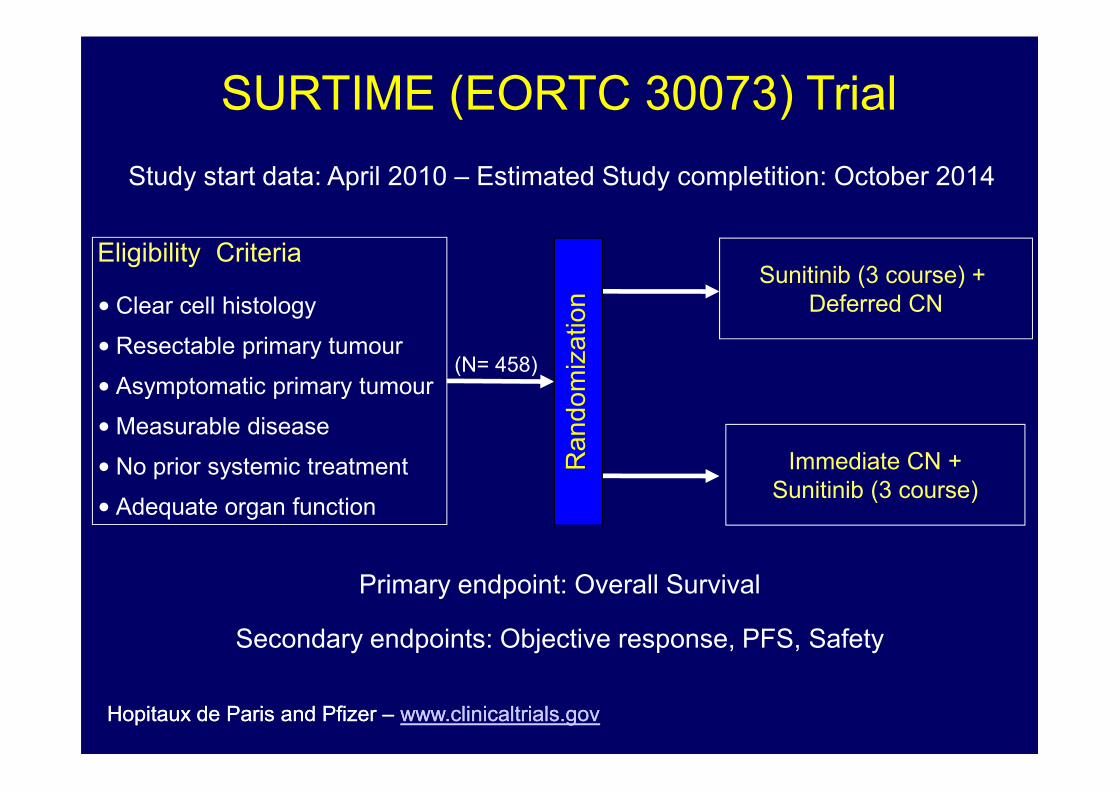
Eligibility Criteria
• Clear cell histology
• Resectable primary tumour
• Asymptomatic primary tumour
Sunitinib (3 course) +
Deferred CN
Ra
nd
om
iza
tio
n
(N= 458)
SURTIME (EORTC 30073) Trial
Study start data: April 2010 – Estimated Study completition: October 2014
HopitauxHopitaux de Paris and Pfizer de Paris and Pfizer –– www.clinicaltrials.govwww.clinicaltrials.gov
Primary endpoint: Overall Survival
Secondary endpoints: Objective response, PFS, Safety
• Asymptomatic primary tumour
•Measurable disease
• No prior systemic treatment
• Adequate organ function
Immediate CN +
Sunitinib (3 course)
Ra
nd
om
iza
tio
n
Conclusions
• Nephrectomy is still an important part of
the multidisciplinary treatment of RCC
• Targeted agents represent a substantial
improvement but since they are not
curative, the cytoreductive paradigm iscurative, the cytoreductive paradigm is
still relevant
• Today, the more relevant question should
address the timing of and appropriate
patient selection for cytoreductive
nephrectomy












