Embed Size (px)
Citation preview

1
DISORDERS OF THYROID FUNCTION
HYPERTHYROIDISM
Hyperthyroidism is a condition in which there are increased levels of thyroid hormones in the blood and one for which surgical correction is frequently appropriate.Causes of thyrotoxicosisCommon causes: - diffuse toxic goiter (Grave’s disease) - toxic multinodular goiter (Plummer’s disease- toxic solitary nodule - nodular goiter with hyperthyroidism due to exogenous iodine.- exogenous thyroid hormone excess- thyroiditis
Rare causes:- metastatic thyroid carcinoma- pituitary tumour secreting TSH
Grave’s disease (Basedow’s disease)It is the most common cause of hyperthyroidism, it is an immunological disorder in which thyroid stimulating antibodies of the Ig G type bind to the TSH receptor and stimulate the thyroid cells to produce and secrete an excess of thyroid hormones.The thyroid gland hypertrophies producing diffuse enlargement.Most of the symptoms and signs of thyrotoxicosis result from excess thyroid hormones, stimulating metabolism, heat production and oxygen consumption.It is especially common in young women between 20 and 40 years of age.Ophthalmopathy has two major components:1- non infiltrating ophthalmopathy resulting from sympathetic activity leading to upper lid retraction, a stare and infrequent blinking.2- infiltrating ophthalmopathy causing oedema of the orbital contents, lids and periorbital tissues, cellular infiltration and deposition of mucopolysaccharide material within the orbit.Diplopia results from weakening and paralysis of the external ocular muscles.The cornea is vulnerable to damage and ulceration may occur.Investigations:- measurement of free T4, T3, TSH will confirm the diagnosis.- a radioactive iodine or technetium scan is not essential in patients with

2
Grave’s disease although it is necessary in the assessment of toxic solitary and multinodular goiter to determine the site of nodular overactivity.- radioactive iodine uptake studies are particularly appropriate revealing an increased uptake.- chest X ray- position of trachea- laryngoscopy- mobility of the vocal cords preoperatively- ecg- cardiac activity.
TreatmentIn Graves’s disease three treatment modalities can be used either alone or in combination to restore the euthyroid state:
- antithyroid drugs- radioactive iodine- surgery
Antithyroid drugsThese drugs interfere with the thyroid hormones synthesis.Medical treatment with antithyroid drugs has two principal roles:
- treatment of newly diagnosed patients with Grave’s disease in the hope of inducing a permanent remission
- render the toxic patient euthyroid in preparation for surgery.
Beta-adrenergic blockersMany of the manifestations of hyperthyroidism, particularly those relating to the cardiovascular system, can be ameliorated by the administration of beta-blockers such as metoprolol.Beta-blockers are usually used in combination with one of antithyroid drugs in patients who are severely toxic and in those patients being prepared for surgery.
Radioactive iodineI 131 used to control thyrotoxicosis achieves its effect by destruction of overactive thyroid tissue.There would appear to be no adverse effects of I 131 treatment with respect to leukemia, thyroid carcinoma, fetal damage or genetic mutation.An ablative dose will render more than 60% of patients hypothyroid in one year. Regular long-term surveillance is required and thyroxine replacement given as necessary.
SurgeryThyroidectomy in patients with Graves’s disease is safe and rapidly renders the patient euthyroid. The principal indications for surgery are:- relapse after an adequate course of antithyroid drugs- severe thyrotoxicosis with a large goiter

3
- difficulty in controlling toxicity with antithyroid drugsThe surgical procedure: bilateral subtotal thyroidectomy leaving a posterior remnant of thyroid tissue on each side of the trachea or total thyroidectomy.
Toxic multinodular goitreAntithyroid drugs are of no value as a long-term treatment because thyrotoxicity is due to autonomy and will recur once any medication is discontinued.I 131 can be used for small goitres but usually a subtotal thyroidectomy is most appropriate after achievement of the euthyroid state or total thyroidectomy.
Toxic solitary noduleThis condition caused by a single autonomous thyroid can be treated by either a unilateral thyroid lobectomy or I 131
Follow-upBecause of the risk of developing postoperative hypothyroidism patients who have undergone any form of treatment for hyperthyroidism must be followed on a long-term basis with regular clinical and biochemical assessment.
Preparation for surgeryClassically the patient comes to surgery in the euthyroid state, controlled by a period of antithyroid drug therapy. Because the antithyroid drugs block the synthesis of thyroxine but do not inhibit the release of the hormone from existing colloid stores the time required for symptomatic improvement may vary widely from two weeks to as long as three months.There has been a lot of interest in carrying out the operation of thyroidectomy for thyrotoxicosis in patients prepared for operation by beta-adrenergic blockade with metoprolol. When the patient has become euthyroid, iodine given as Lugol’s solution is administered for ten days before surgery for the good reason to induce a firmity of the gland and reduce the hemorrhagic risk at operation.The operation is often made easier by avoidance of antithyroid drugs which are to a degree goitrogenic. Beta-blockers may be reduced after surgery and discontinued by 7 days after operation.
Postoperative complications
1. Postoperative bleedingThere is always a risk of postoperative bleeding after thyroid surgery.It is rare but sometimes dramatic and fatal. The bleeding may occur in one of two sites:

4
- deep to the myofascial layer in relation to the thyroid remnant or vessels. Evacuation must be done quickly but it will usually be possible to do this under general anesthesia in the operating theatre.- bleeding deep to the skin flaps is the more common and usually arises from veins. Bleeding is slow but a substantial hematoma may develop and produce pressure on the airway. Evacuation is mandatory. If hematoma is seen within 12 hours of operation it should probably be evacuated to prevent respiratory embarrassment developing. Little is to be gained by observation.
2. Postoperative thyrotoxic crisisThyrotoxic crisis is a serious complication but it should not be seen where there has been adequate preoperative preparation.It occurs within the first 24 hours of thyroidectomy with the patient becoming confused and hyperactive with a high temperature, profuse sweating and rapid heart rate.Treatment must be vigorous with beta-adrenergic blockade, intravenous hydrocortisone and iodine.
3. Postoperative voice changesRarely are voice changes due to any damage to recurrent laryngeal nerves since this occur in less than 1% of cases when thyroidectomy is carried out by experienced thyroid surgeons.Damage to the recurrent laryngeal nerve which may run between the bifurcation of the inferior thyroid artery as it enters the gland.Probably minor changes in the muscles around the cricoid and thyroid cartilages are the most important and it is to some extent, inevitable that there will be some changes with the mobilization of the gland.Trauma to the external laryngeal nerve supplying the cricothyroid muscle can lead to voice changes because of difficulty in achieving vocal cord tension if the muscle is paralysed.Damage to the internal laryngeal nerve is also serious and can occur where there is difficulty in mobilizing the superior pole. This leads to desensitization of the appropriate side of the larynx and spilling over, especially of liquids, during swallowing.
4. HypoparathyroidismThe commonly encountered hypocalcemia of the first few days after thyroidectomy probably has little to do with hypoparathyroidism and is more likely to be a consequence of the metabolic changes taking place with re-entry of calcium into bone demineralized by hyperthyroidism (“hungry bones”).The operation of thyroidectomy is designed to leave a large amount of thyroid capsule and with it the parathyroids.

5
However, parathyroids are very small and are not always easy to identify at thyroidectomy. The incidence of hypoparathyroidism after surgery for thyrotoxicosis should be less than 1%.
5. HypothyroidismAll forms of treatment for thyrotoxicosis will produce a population of patients prone to develop hypothyroidism, greatest after radioiodine therapy but seen after all forms of treatment.
MALIGNANT DISEASE OF THE THYROID GLAND
Primary malignancies of the thyroid can be classified according to the element from which they arise:
Tumours of thyroid follicular epithelium1- papillary carcinoma2- follicular carcinoma3- anaplastic carcinoma
Tumours of parafollicular cells1- medullary carcinoma
Tumour of lymphoid element1- lymphoma
Papillary carcinomaThis is the commonest thyroid tumour which shows an increased incidence in iodine-rich areas and usually affects children and young adults. Previous neck irradiation particularly in the young may predispose to thyroid cancer.PathologyThis tumour which has a propensity for lymphatic spread both within the thyroid and to the paratracheal and cervical lymph nodes is usually a hard whitish lesion infiltrating the thyroid gland and presents as a thyroid nodule.The lesion is frequently multifocal, rarely encapsulated and blood-borne spread is usually a late feature.These tumours can be divided into three main types based on their size and extent: - minimal- these are lesions 1 cm. or less in size, usually not clinically obvious. They readily metastasise to regional lymph nodes.
- intrathyroidal- these lesions are larger than minimal tumours, have a less favourable prognosis, are situated totally within the thyroid.

6
- extrathyroidal- this a locally advanced condition extending through the thyroid capsule often involving adjacent structures as the trachea, oesophagus and recurrent laryngeal nerve.Clinical presentationThe commonest presentation of papillary carcinoma is a thyroid nodule frequently associated with enlarged cervical lymph nodes.Involvement of the adjacent structures by a locally invasive tumour may cause hoarseness of the voice due to recurrent laryngeal nerve palsy, airway symptoms because of tracheal involvement and dysphagia as a result of esophageal invasion.Less than 1% of patients at the time of initial presentation will show features of distant metastases.Diagnosis is based on a combination of careful clinical assessment and fine needle aspiration cytology.
Follicular carcinomaThis tumour, less common than papillary carcinoma, has a higher incidence in iodine-deficient areas due to chronic TSH stimulation and can also be caused by previous irradiation.
The disease has a female to male ratio of 3:1, affects an older age group (mean age 50 years) than papillary carcinoma.PathologyFollicular carcinoma is invariably encapsulated, solitary, readily exhibiting vascular invasion and spread via the bloodstream.Follicular carcinoma is classified into two types according to histopathological features: - minimally invasive- histology demonstrates only slight capsular or vascular invasion
- frankly invasive- histology demonstrates venous extension particularly into the middle thyroid and internal jugular veins.Clinical featuresFollicular thyroid cancer presents as a discrete solitary thyroid nodule increasing in size. Although many tumours are firm a follicular carcinoma is often soft because of hemorrhagy within the lesion.Metastatic disease may already be present at the time of diagnosis with bone and lung involvement.DiagnosisUnlike papillary thyroid carcinoma, follicular carcinoma cannot be diagnosed precisely by FNAC. The cytology report will describe a follicular tumour, usually showing a microfollicular pattern, the majority of such lesions being entirely benign.Only 20% of these will be subsequently identified as follicular carcinoma.

7
Treatment of differentiated thyroid cancerThere is general agreement that thyroidectomy is the treatment of choice.The treatment objectives are:- eradicate primary tumour- reduce the incidence of distant or local recurrence.Total thyroidectomy has been advocated because of its ability to treat multifocal tumour, decrease local and distal recurrence.In the case of papillary carcinoma there is a high incidence of multifocality which clearly would not be treated by a unilateral or even near total thyroidectomy.Retrospective studies of thyroidectomy for papillary tumours have demonstrated a reduced local recurrence rate when total thyroidectomy was performed compared with a subtotal resection.Thyroidectomy must always include clearance of pretracheal and paratracheal lymph nodes.
A unilateral lobectomy and isthmusectomy is adequate for minimal (less than 1 cm.) lesions.
Follicular tumours if minimal lesion then a unilateral lobectomy is all that is required.An invasive follicular tumour requires a total thyroidectomy.
Lymph node dissection is not routinely performed for follicular tumours. A decision to proceed to a total thyroidectomy can often be made at the time of surgery on the basis of the macroscopic appearance of the lesion and especially when the tumour size is in excess of 4 cm.
Postoperative treatmentThyroxineAny patient who has undergone total thyroidectomy will require replacement treatment with thyroxine.Thyroglobulin measurementIt is a sensitive indicator of residual or recurrent differentiated thyroid cancer when a total thyroidectomy has been performed and the patient is on full replacement thyroxine dosage.This measurement is now performed routinely and has markedly reduced the need for routine serial radioactive iodine scanning.Radioactive iodineRadioactive iodine is a most useful means of detecting metastatic disease when total thyroidectomy has been performed for differentiated cancer.Postoperatively, patients are initially placed on T3 and sent home to wait an I 131 scan six weeks later.

8
T3 is discontinued two weeks before the scan to allow a rise in TSH level before administering 2-5mCi of I 131.If there are no metastases and the total thyroidectomy has been successfully performed the uptake at 24h. should be less than 1%.When there is significant uptake in the thyroid bed this can be ablated with radioiodine and many metastatic disease subsequently treated with a therapeutic dose of 150-200mCi I 131.The maximum cumulative dose of I 131 should be no greater than 800-1000mCi.
Anaplastic carcinomaThis highly aggressive tumour usually affects the elderly with a peak incidence between 60 and 70 years of age.The tumour has a higher incidence in areas of endemic goitre. The tumour rapidly infiltrates local structures and metastases via the bloodstream and lymphatics.The frequent finding of foci of papillary or follicular carcinoma in anaplastic tumours suggests that this disease originates in an unrecognised or untreated differentiated tumour.The clinical findings are typically those of an elderly female often with a long history of goiter that suddenly starts to grow rapidly with hoarseness, dysphonia, dysphagia and a compromised airway.Confirmation of clinical diagnosis may be obtained by FNAC, the aspirate showing bizzare giant cells, multinucleated cells.Resection of the thyroid is rarely possible because of the local extent of disease.Incision biopsy for diagnostic purposes should be avoided for fear of infiltrating an uncontrollable local spread of the disease.If surgery is possible it should relieve an obstructed airway by excision of the of the isthmus.Radiotherapy and doxorubicin are the main modalities of treatment but invariably the tumour rapidly progresses usually leading to death of the patient within six months.
Medullary carcinomaThis is a tumour which arises from the C-cells, derived from neural ectoderm, and accounts for approximately 8% of malignant thyroid tumours.This is a solid non-follicular carcinoma that arises from the parafollicular C-cells which secretes calcitonin, a peptide capable of lowering the blood calcium and amenable to measurement by radioimmunoassay.PathologyMedullary carcinoma is a solid tumour located in the upper two thirds of the thyroid and is usually both multicentric and bilateral.

9
The tumour grows locally but readily spreads by lymphatics to regional nodes and via the bloodstream to distant sites such as liver, lungs, bones.This tumour produces and secretes calcitonin, a most valuable histochemical marker for medullary carcinoma. Carcinoembryonic antigen (CEA) is another tumour marker.Clinical featuresThe disease tipically presents as a mass in the neck often with enlarged cervical and mediastinal lymph nodes.Involvement of adjacent organs and the recurrent laryngeal nerve may cause respiratory or swallowing difficulties and voice changes.Sporadic disease has a peak incidence at 40-50 years of age whereas inherited familial disease is usually seen at a younger age.Diarrhea is often a prominent clinical feature but the ability of this tumour to secrete a range of hormones and peptides including calcitonin, prostaglandins, 5-hydroxytryptamine and ACTH can give rise to a range of clinical syndromes which may include Cushing’s syndrome.DiagnosisClinical assessment and the taking of a careful family history are fundamental to establishing a precise diagnosis and confirmation is obtained by FNAC and measurement of serum calcitonin.Because of the close association of phaeochromocytoma and MC in the MEN familial forms measurement of urinary VMA and metanephrines should be carried out in all patients with MC before progressing to any invasive measures such as surgery.TreatmentTotal thyroidectomy is the appropriate procedure to adequately treat multicentric and bilateral disease.The central and paratracheal lymph nodes are cleared from the level of the thyroid cartilage to the upper mediastinum.The lateral nodes in the carotid sheath are sampled and if involved with tumour a modified radical node dissection is performed preserving the internal jugular vein, sternomastoid muscle and spinal accessory nerve.Even when the primary tumour is extensive the recurrent laryngeal nerve can usually be preserved. Because of the multifocal nature of hereditary tumours a bilateral lymph node clearance is advised.PrognosisThe presence or absence of distant metastases and lymph node positivity are major factors in determining the ultimate prognosis.When lymph node metastases are present this survival rate is reduced to 45% at 10-years suevival.

10
Follow-upAfter surgery regular clinical and biochemical follow-up is carried out with measurement of the two tumour markers calcitonin and carcinoembryonic antigen (CEA).When raised levels of these agents persist after thyroidectomy or develop at a later stage this may signify persistent and recurrent disease.Ultrasonography, CT, MRI and scanning with other isotopes such as dimercaptosuccinic acid (DMSA) and meta-iodobenzyl guanidine (MIBG) can be utilised to detect this disease.For recurrence, external irradiation can occasionally produce some benefit but chemotherapy with doxorubicin is both toxic and disappointing.
The TNM stages of thyroid cancer“TNM” stands for Tumour, Node, Metastasis.
There are 4 main T stages for thyroid cancer
T1 - the tumour is entirely inside the thyroid and is less than 2cm across in any direction
T2 - The tumour is entirely inside the thyroid and is more than 2cm but no more than 4cm across in any direction T3 - The tumour is entirely inside the thyroid and is more than 4cm across in any direction T4a - The cancer has grown outside the covering of the thyroid gland into the surrounding tissues. T4b - The cancer has grown outside the thyroid gland into the area surrounding the bones of the spine, or one of the main blood vessels nearby.
N0- no lymph nodes contain cancer cells
N1 is divided into 2 groups
N1a - there are lymph nodes containing cancer cells on one side of the neck only (on the same side as the cancer) N1b - there are lymph nodes containing cancer cells anywhere else (usually the other side of the neck or in the chest)
M0- no metastases
M1- present distant metastases

11
Papillary and follicular thyroid cancerThe number stages for papillary and follicular thyroid cancer are the same. There are 4 number stages. These cancers are staged differently depending on age of the patient. These types of thyroid cancer tend to respond well to treatment, particularly in young patients.
Under 45years of age:
Stage 1 - cancer is only inside the thyroid, or the thyroid and the lymph glands Stage 2 - cancer has spread presenting metastases
Over 45:
Stage 1 - cancer is only inside the thyroid and is less than 2cm across Stage 2 - cancer is any size, but is only inside the thyroid Stage 3 - cancer has grown beyond the thyroid capsule, or there are cancer cells in the lymph nodes Stage 4 - cancer has spread to other parts of the body, such as lungs or bones
Medullary thyroid cancerThere are 4 number stages for medullary thyroid cancer. These are:
Stage 1 - cancer is less than 2cm across Stage 2 - cancer is between 2cm and 4cm across Stage 3 - There is spread to cervical lymph nodes Stage 4 - The cancer cells have spread to another part of the body
Staging for anaplastic thyroid cancerThere is no number staging system for anaplastic thyroid cancer. This is because there is a high risk of the cancer spreading.
Whether the cancer is only in the neck and so may be able to be completely removed
Whether the patient is fit enough to have treatments such as surgery or radiotherapy

12
THYROIDITIS
The thyroid gland may be subject to inflammatory change in a variety of conditions, the process being either focal or diffuse and often associated with thyroid dysfunction.
Subacute thyroiditisThis condition, often called granulomatous or de Quervain’s thyroiditis is probably of viral origin.It is characterised by painful swelling of one or both thyroid lobes with associated malaise and fever.Frequently there is a preceding history of sore throat or viral infection a week or two before the onset of thyroid symptoms.Approximately one third of patients are asymptomatic apart from enlargement of the thyroid gland but 15% have a more acute illness with symptoms and signs of hyperthyroidism.Thyroid hormone levels are raised but in contrast to Grave’s disease there is low uptake of radioactive iodine on scintigraphy. The ESR is raised.The disease process of subacute thyroiditis is usually self-limiting with resolution of local symptoms and thyroid dysfunction.A few patients, however, pass through a mild hypothyroid phase.Local symptoms can be controlled with aspirin but if severe and prolonged a course of steroids can be helpful.The transient hyperthyroidism does not require treatment with antithyroid drugs.
Autoimmune thyroiditisThis condition was described by Hashimoto and occurs as a diffuse process throughout the thyroid gland which usually enlarges to several times normal size.Although clasically the gland enlargement is diffuse there may be nodularity and lobulation making distinction from simple multinodular goitre or even malignant disease difficult.Histologically there is infiltration of the thyroid by lymphocytes and plasma cells, frequently secondary lymphoid nodules and adjacent stromal fibrosis.The condition is due to an immunological disorder characterised by thyroid antibodies in the serum.A positive family history of other autoimmune disease such as pernicious anaemia, gastritis, thyrotoxicosis is frequently obtained.As a result of destructive changes within the infiltrated thyroid, hypothyroidism usually ensues and when present requires treatment with thyroxine.This medication supresses TSH and leads to shrinkage of the thyroid gland with relief of any symptoms.

13
Surgery is not usually required since pressure symptoms and involvement of adjacent structures occurs rarely.Occasionally a satisfactory reduction in the size of the goiter can be achieved by the administration of steroids.When the thyroid, involved with autoimmune disease, is seen to rapidly enlarge or develop a firm asymmetrical nodular area, exclusion of lymphoma by FNAC is required.
Riedel’s thyroiditisThis condition, sometimes called invasive fibrous thyroiditis is characterised by a dense fibrous inflammatory infiltrate throughout the thyroid, sometimes extending through the capsule to involve adjacent structures.The condition is rare but is important because the clinical picture mimics thyroid malignancy.Needle biopsy is likely to be required to free a compromised airway.Steroid medication has been tried without much success and recently there have been reports of benefit from tamoxifen.
Acute suppurative thyroiditisThe thyroid can be infected by a variety of bacterial or fungal agents producing clinical features of an acute painfully inflamed gland.Confirmation of diagnosis and bacteriology is obtained by needle aspiration and appropriate antibiotics administered.
DISORDERS OF THE PARATHYROID GLANDS
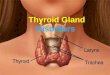
The parathyroid glands are important to surgeons for two reasons.First, because surgeons treat patients with symptomatic hyperparathyroidism they must know the cause and management of various hyperparathyroid conditions and second during operations in the neck, it is imperative that the intergrity of the parathyroids be preserved to avoid permanent hypoparathyroidism.There is no satisfactory replacement for endogenously produced parathyroid hormone and the patient with hypoparathyroidism is doomed to a lifelong process of episodic, symptomatic hypocalcemia despite calcium and vit. D therapy.AnatomyThe superior parathyroid glands usually lie at the junction of the upper and middle third of the thyroid gland on its posteromedial surface and in the tracheooesophageal groove.The inferior parathyroid glands lie close to the inferior poles of the thyroid gland.

14
Sometimes they are found some distance caudal to the thyroid gland in association with the inferior thyroid veins.
Parathyroid hormone (PTH)PTH is a major regulator of calcium metabolism. It acts in conjunction with calcitonin and activated vitamin D3 to regulate the plasma concentration of the ionized form of calcium.As serum calcium falls, the secretion of PTH increases.As serum calcium rises, the secretion of PTH decreases.PTH exerts its biologic effect on bone, intestine and kidney:- increases the mobilization of calcium and phosphate from bone.- acts synergistically with D3 to increase the absorbtion of calcium and phosphorus from the gut.- promotes the active reabsorbtion of calcium in the distal nephron.- inhibits phosphate reabsorbtion in the proximal tubule.Increased PTH secretion has the following clinical effects on bone, intestine and kidney:- hypercalcemia- hypocalciuria initially due to increased calcium reabsorbtion, then in a chronic state hypercalciuria-hypophosphatemia-hyperphosphaturia
Laboratory testsSerum PTH levels can be measured by radioimmunoassay.
HyperparathyroidismPrimary hyperparathyroidismIncidence. It may occur sporadically but may occur as:- part of a multiple endocrine adenomatosis syndrome- familial hyperparathyroidism- ectopic tumour
Etiology and pathology- 90% of primary HPT cases are due to a solitary adenoma of one of the four glands.- about 10% are due to four-gland hyperplasia- parathyroid carcinoma accounts for 1% of primary hyperparathyroidism cases.Clinical presentationMost patients with primary HPT are asymptomatic.When patients are symptomatic, the symptoms are:-renal lithiasis-osteitis fibrosa cystica

15
-psychiatric manifestations-peptic ulcer disease, usually associated with hypergastrinemia that results from hypercalcemia- cholelithiasis or pancreatitis may occur.- non-specific symptoms: weakness, easy fatigability, constipation, arthralgia.
DiagnosisLab. testsAn elevated serum calcium level is the cornerstone of diagnosis.While primary HPT is a relatively common cause of hypercalcemia, other causes must be excluded, such as metastatic bone disease, myeloma, sarcoidosis the use of thiazide diuretics, thyrotoxicosis and Addison’s disease.A serum PT hormone level is high, disproportionately.In patients with metastatic bone disease, ythypercalcemia occurs without a disproportionate elevation of PH.In patients with secondary HPT, the serum PTH level is high and the serum calcium is low.In patients with hypoparathyroidism the serum calcium and serum PTH are both low.The serum phosphorus level is decreased, hyperphosphaturia.
Radiographic studiesX-ray of the skull may show a “ ground-glass” appearance in the outer 2/3 of the skull. Skull X-rays are also obtained to search for enlargement of the sella turcica due to pituitary tumour.X-rays of the proximal ends of the long bones may demonstrate bony reabsorbtion.Indications for surgeryOnce the diagnosis of primary hyperparathyroidism is confirmed biochemically patients should be selected for operation.1. All symptomatic patients with biochemically proven HPT should be considered for surgery.2. Operation is also advised for an asymptomatic patient whose serum calcium levels exceed 11 mg/dl, especially if the patient has a decrease in bone density, hypercalciuria or a decrease in renal function due to other diseases such as hypertension or diabetes mellitus.Methods of preoperative localization- ultrasonography- scanning of the neck after administering Thallium 201
- thyrocervical angiography by Seldinger technique- CT and MRI

16
Surgical treatmentSolitary adenoma- removal of adenomaFour-gland hyperplasia- two options:
- subtotal parathyroidectomy- 5% recurrence rate after it- total parathyroidectomy with autotransplantation of minced parathyroid tissue into a well vascularized accessible forearm muscle.
THYMUS
The thymus gland has right and left lobes closely bound together which may overlap each other to some extent. It lies anteriorly in the superior mediastinum and extends both superiorly into the neck in front of the left brachiocephalic vein and also inferiorly into the anterior mediastinum where its lower poles are closely related to the pericardium.
After puberty the thymus undergoes fatty degeneration to a varying extent.Blood supply comes from the internal thoracic arteries and the venous drainage is into the left brachiocephalic vein.The function of the thymus gland has been the subject of an enormous amount of research over the last 20 years and has still not been completely clarified.Some aspects of its function are of considerable relevance to surgeons.The thymus, plays a vital role, particularly in childhood in determining the immunological competence of the individual. The thymic cells influence other lymphocytes, the B-cells to produce immunoglobulins in response to antigenic stimulation. The lymphocytes are from the bone marrow initially and develop into the two distinct populations, T-cells and B-cells.T-cells develop their identity in the neonatal period after passing through a thymic phase. The T-cells then migrate to colonize the T-cell area of the lymph nodes and spleen.T-cells have been identified: helper and suppressor, which influence the B-cell accordingly. The normal ratio of helper and suppressor T-cells is 2:1, this ratio is reversed in the immunocompromised patient
Myasthenia gravisMyasthenia gravis is an acquired autoimmune disorder which involves autoimmune blockage of postsynaptic nicotinic cholinergic receptors. The disease is related to the production of an antibody which blocks the effect of acetylcholine at the motor end-plate. The neuromuscular transmission is compromised the clinical result being muscular weakness and fatigability.The sourse of these autoantibodies is the abnormal thymus in the majority of cases.

17
The pathological appearance of the thymic gland in the majority of myasthenics shows some degree of hyperplasia of the lymphoid elements but 10-20% of myasthenics are reported to have thymomas.Affected patients experience weakness which worsens by exertion and improves by rest.Occular muscle involvement induces ptosis and diplopia, facial muscle involvement induces loss of facial expression and jaw drop. Bulbar muscle involvement induces nasal speech, choking on foods, dysphagia.Abnormal fatigability of the limb muscles causes difficulty in combing hair, lifting objects, climbing stairs, walking and running.
Diagnosis is based on the characteristic history of progressive weakness of the voluntary muscles, on physical examination which shows no neurological abnormality but impaired muscles strength and specific investigations.Anticholinesterase tests with edrophoniu or neostigmine which shows improvement of the muscle strength after injection.Electromyography- supramaximal stimulation of a motor nerve results in a 10% decrement of the amplitude of the evoked muscle action potential. In mysthenics the decrement is more than 10%.Assessment of the serum levels of autoantibodies to Acetyl choline receptors.CT of the thorax may show enlarged thymic gland or a thymic tumour located in anterior-superior mediastinum.
Thymectomy is an effective treatment for this disease in most patients.
Thymoma without myastheniaThe majority of such patients are asymptomatic.When symptoms occur they are often non-specific: chest pain, cough and occasionally breathlessness.Chest X-rays, lateral and antero-posterior views may depict an opacity retrosternally but CT scan represents the mainstay of diagnostic investigations.Thymic scintigraphy with 99mTc-tetrophosmin can show increased uptake at the site of thymoma.Any suspicion of a thymoma should be surgically excised.The contraindication of surgical treatment is clear-cut evidence of tumor invasion into the great vessels. Radiochemotherapy is useful in inoperable patients or in postoperative recurrence of a thymoma.

18
Study questions
1. A 35 years-old lady, underweight in spite of her good appetite went to her G.P. being concerned of sleeplessness, anxious state and palpitation. On physical examination her G.P. revealed a BP of 15/8 cm Hg, PR 90/min. and palpated a slightly enlarged painless thyroid gland. He prescribed sleeping tablets and tranquilizers (anti-anxiety agents). Did he manage well this patient?
2. What treatment should be done in the toxic solitary nodule ?
3. A 42 years-old lady complains of 2 weeks history of voice change and dysphagia along with a rapid growing painless neck lump. She is from Ukraine and it passed 10 years from Cernobil nuclear blast. How would you manage this patient?
4. How could you know that a total thyroidectomy for papillary carcinoma has been performed in the past by another surgeon if the patient cannot remember or lost her medical discharge form and now she came with a lateral neck lump?